Embed Size (px)
Citation preview

COMMUNITY HEALTH STUDIES VOLUME V f f f , NUMBER I. 1984
INCOME FROM PRIVATE MEDICAL PRACTICE IN AUSTRALIA 1966-1978. AN ANALYSIS OF TAXATION STATISTICS
Richard Taylor
Deportment of Social and Preventive Medicine, Monosh University Medical School, Alfred Hospitol, Rohron 3181.
Summary The evidence from taxation statistics indicates
that private medical practitioners in Australia have improved their income relative to most other professions since 1966/67, receiving three to four times the income of salary and wage earners by the late 1970s. Evidence concerning the frequency distribution of high income earners in various occupation groups also suggests that private medical practitioners are the highest paid group in Australia.
Data on average net and estimated average gross annual income per doctor indexed for the Consumer Price Index, Average Weekly Earnings and the Medical Fees Index indicate a peak income in 1975/76, mainly as a result of medical fee rises.
There has been a secular decline during the period under review in net income as a proportion of gross income of private doctors as a result of increases in practice "expenses". This increase in "expenses" was not accompanied by increases in the proportion of expenses accounted for by wages paid, and this phenomenon may be partly a result of the increased application of tax avoidance schemes which enable personal consumption expenditure to be subsumed with "business expenses".
Introduction The level of medical incomes in Australia is of
interest because, collectively, these incomes comprise a significant proportion of expenditure on medical care and because such incomes are either paid directly from the public purse or result from business activity in a heavily subsidized medical 'market". Income in private practice is of particular interest in view of extensive government and health insurance subsidies, claims of widespread and endemic fraudulent practicesl and because it appears that private doctors are one of the highest paid occupations in Australia. There
TAYLOR I
has been disquiet concerning the justification for such high medical incomes and an increasing appreciation of the ethical conflicts which inevitably involve the doctor/ businessman.2
Methods This article uses taxation statistics to trace the
incomes of private medical practitioners from the mid 1960s to the late 1970s, and relates these incomes to other occupational groups in Australia. The average annual income of doctors in private medical practice (1966/67-1977/ 78) was calculated from information contained in the taxation statistics published as supplements to reports by the Commissioner of Taxation to the Australian (Commonwealth) Parliament.3 This analysis includes individual medical practitioners who are in business (private medical practice) and who were subject to or actually paid provisional tax. Where possible, calculations have been based on doctors who paid provisional tax since this group does not include certain part-time or marginal practitioners who are not in full-time private practice (for example, married women, semi- retired, etc.).
Unfortunately, there have been successive changes in the way the taxation statistics have been calculated and tabulated over the period covered by the study. The change in tabulation from those subject to provisional tax, to those actually paying provisional tax, occurred in 1971/72. In some of the early years actual income is given in the schedules rather than net income - both measures, however, are very closely related. For some years certain figures were not published and, in some instances, these have been obtained or estimated by Dr Richard Scotton from tabulations specially requested from the Taxation Department and other data.* Since 1978/79 changes have been *Division of Planning and Rescarch, Huhh Commission of Victoria. Dr Scotton assisted in providing unpublished figures for this analysis. Data obtained from Scotton arc indicated in the cabkr.
COMMUNITY HEALTH STUDIES

made in the way the taxation statistics have been partnerships and trusts schedule and the net tabulated which precludes analysis of the kind income from partnerships and trusts from the which has been undertaken in this study. The individual schedule. It was assumed that the ratio reasons for these changes are not stated in the of gross business income to net business income in taxation statistics supplement and are not obvious. the partnerships and trusts schedule could be Total net income of all individual medical applied as an inflating factor to the net income practitioners was given in the individual schedule from partnerships and trusts in the individual of the taxation statistics and the average annual net schedule, thus yielding an estimate of annual gross income per doctor was obtained by simply dividing partnership and trust income for the total of this figure by the number of doctors included in individual medical practitioners (c), (see Table I ) . this schedule.
Estimated total gross income for the total of Gross income for all individual medical all individual medical practitioners was obtained practitioners was more difficult to obtain. It is the by the addition of (a), (b) and (c) above, and the sum of (a) total individual business income, average annual estimated gross income per doctor (b) individual income from salary and wages and was obtained by dividing this figure by the number (c) gross income from partnerships and trusts. (a) of medical practitioners included in the individual and (b) are given in the individual schedule but (c) schedule. Both net and estimated gross annual is not. Estimated gross income from partnerships income per doctor has been deflated by the and trusts for the total of individual practitioners Consumer Price Index (CPI), Average Weekly had to be estimated from data available in the Earnings (AWE), and the Medical Fees Index
TABLE 1
Estimation of Gross Partnership and Trust Income for the Total of Individual Medic81 Practitioners, 1966/67 - 1977/78
Year Estimation of Gross Partnership & Trust
Income for the Total of Individual Medical Practitioners
From the Partnership and Trusts Table
(c x d) Estimated Gross
Income Income (alb) Partnership & Trusts Partnership & Trusts Income for the Total of Individual Medical Practitioners
(a) (b) ( 4 ( 4 Net Income from
(Individual Table)
Gross Business Net Business Factor
19781793 1977178 1976177 1975176 19741 75 1973174 1972173 I971 I 72 1970171 1969170 I968 I 69 I9671 68 1966167
376840 369245 371512 339732 245341 I96566 176233 157916 137157 I I5728 104860 92834 97041
I82563 192178 198314 196181 I39287 1 13623 104678 96738 870 I8 73467 67276 59988 57540
2.064 1.921 1.873 1.732 1.761 1.730 1.684 1.684 1.576 1.575 1.559 1.548 1.513
- 1681 18+ I7 1487+ I55654+ 1 I5422+ 103087+§ (978850)+# 84 103+ 80148* 68389* 63285* 58068* 53520.
- 322955 321 195 269593 203258 1 7 8 3 q ( 164780)g 137256 126313 107713 98661 89889 80976
AII income figures arc in s x 10' * subject to provisional tax + paid provisional tax 0 supplied by Scotton. ( ) = estimated t it is no longer possible to obtain (d)
TAYLOR 2 COMMUNITY HEALTH STUDIES

(MFI). This allows evaluation of secular trends in income: in relationship to the earnings of others (AWE); taking into account the effect of general price inflation (CPI); and adjusting for the effect of the level of medical fees (MFI). The year 1966/67 was used as the base year in which all indices were set at 100 by the following calculation:
(Given index in each year)
lndcx in 1966167
Standardized (on 1966167) = x index for each year
The indices for the various years were obtained from the Australian Bureau of Statistics (CPIgL AWE)4andapaperbyDeeble(MFI).5The standard index was then applied to the data to yield an income index deflated by the CPI, AWE or MFI, with 1966167 as the base year, as follows:
(Income per doctor for year) x (1oooo)
each year (Standardidized index for each year) x
(income per doctor 1966/67)
Deflated income index for I
In 1977/78 certain tabulations of taxation statistics were published which enabled calculations to be made of the frequency of high income earners in the various occupational groups. These figures are based on taxable income. Private medical practice is subsumed within the section Health, Educatio? and Welfare, but doctors comprise half of this group and thus certain conclusions can be drawn.
A comparison of the incomes of certain other professional and occupational groups in relation to private medical practitioners over the years 1966/67-1977/78 was undertaken. The average annual net income (per taxpayer) in these groups was expressed as a proportion of average annual net income of doctors. Net income was used because it was readily obtainable for all groups and was a comparable measure over time. It should be noted that net income underestimates disposable income for medical practitioners (and others in business) since personal consumption spending can be subsumed within business expenses. This poses a problem when comparisons of net income are made with wage and salary earners who have little opportunity to engage in such practices. However, it can probably be assumed safely that lawyers, accountants, dentists and certain other professions in business are as adept as doctors in minimizing their net income for taxation purposes so the comparison of these groups with doctors is valid.
TAYLOR 3
Results Total net income and estimated total gross
income for all medical practitioners included in the individual schedule for each year 1966167 to I977/ 78 are set out in Table 2. The average annual net income per doctor and the average annual (estimated) gross income per doctor for the period under review are set out in Table 3. Also included in this table are income indices deflated for CPI, AWE and MFI.
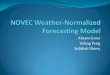
Secular changes in annual net income index and annual estimated gross income index, deflated by CPI, AWE and MFI, are displayed graphically in Figs. I and 2. The CPI deflated indices (both net and gross) peaked in 1975/76, the year of the introduction of Medibank and considerable rises in medical fees. The CPIdeflated net income index declined rapidly in the next two years but the drop in the CPIdeflated gross income index was less marked.
The AWEdeflated income indices generally followed the movements of the income indices deflated by the CPI. However, whereas the net income deflated by the AWE is less than 100, except in 1975176, the AWE deflated estimated gross income is greater than 100 (except in 1974/75). This suggests that private practitioners were doing better in relation to others than would be deduced from consideration of only AWE- deflated net income. This is because, as mentioned previously, gross income is a better measure than net income of actual medical incomes.
The income index deflated for MFI is a measure of medical "activity" or volume since the effect of changing costs of medical fees is held constant. Secular movements of the MFI-deflated income index provide no evidence of increased utilization of medical services in 1975/76, and it is deduced that the increase in CPI and AWE- deflated indices in that year is a result of the rise in medical fees.
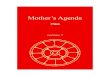
It can be calculated from Table 3 that net, as a proportion of estimated gross, income per doctor (for those included in the schedule for individual medical practitioners) declined from 62 per cent in 1966/67 to 54 per cent in 1977/78. This phenomenon can be investigated more closely by looking at the figures for medical partnerships. since more detailed data on the relationship of net and gross income are available from this schedule (Fig. 3). For medical partnerships, net income as a proportion of gross business income dropped from
COMMUNITY HEALTH STUDIES

TABLE 2
Total Net and Estimated Total Gross Income for Medical Practitioners
Included in the Individual Table, 1966/77 - 1977/78
(a) (b) ( 4 (a+b+c) ( 4
Year Doctors Business Income from Salary Income from Gross Income Income Number of Total Individual Individual Income Estimated Gross Estimated Total
and Wages Partnerships
Total Net
and Tusts
19771 78+ I5237 639442 87282 322955 1049679 562082 1976/77+ 14153 558635 79957 321 195 960787 534944 1975 / 76+ 13185 472324 63513 269593 805430 477493 1974/75+ 1 1736 31 I428 34544 203258 549230 305977 19731 74+$ 11289 226850 25115 178340 441594 239327 19721730 NA NA NA ( 164780) NA NA 1971 I 72+ 10122 176612 15546 137256 329414 189133 19701 71 I0434 150555 15578 126313 292446 171755 19691 70* 9894 I24227 12072 107713 2440 I 2 1450253 1968/69* 9849 114326 I1015 9866 I 224002 133635$ 19671 68. 9582 I04639 9483 89889 20401 1 1230941 19661 67* 9184 94994 8566 80976 I84536 113913%
All income figures are in S x lo3 8 supplied by Scotton, ( ) = estimated (a), (b) and (d) from individual tables (c) estimated from partnership/trusts and individual table figures (see Table I ) + taxpayers charged provisional tax * taxpayers subject to provisional tax % actual Income
I
-I FIGURE 1
Net income (per doctor) in private practice, deflated by the consumer price index (CPI), average weekly earnings (AWE) and the medical fees index (MFI) - 1966/6? to 1977/78
TAYLOR 4 COMMUNITY HEALTH STUDIES

Estimated gross income (per doctor) in private practice, deflated by the consumer price index (CPI), average weekly earnings (AWE) and the medical fees index (MFI) - 1%6/67 to 1977/78
TABLE 3
Net 8nd Estimated Total Grosa Annual Income per Doetor, 1%6/67 - 1977/78
((0 (b) fithated Gross Deflated Gross Income
Year Income per Index using: Doctor
1977pa+ 19761 77+ 1975/76+ 1974/75+ 1973/74+4 1972/73+# 1971/72' 1970/71* 1969/70* 19681 69. 19671 68. 1966/67*
fl)
68894 67886 6 I087 46799 39117 (35050) 32544 28028 24663 22744 21291 20093
CPI
I42 154 I57 I36 I33 134 I32 1 22 I12 I 07 I03 100
A WE
101 I10 111 97 I02 I 0 6 I08 I02 100 100 100 100
MFI
107 115 114 118 I20 1 I7 I10 100 104 NA NA 100
(C) ( 4 Net Income Deflated Net Income Per
Doctor Index using:
0) CPI , A W E MFI
36889 37797 362 I 5 26072 21200 ( 19890) 18685 16461 14658f 13568f
124031 12846f
I23 139 IS1 I23 I17 1 24 I23 I16 I08 I03 100 100
88 99
I07 88 90 98 100 97 96 96 98 100
93 I03 I10 106 106 I08 102 95
100 NA NA 100
f actual income * subject to provisioapt tax + paying provisional tax 0 supplied by Scotton, ( ) = estimated (a) TOW estimsted gross income/number of doctors (scc Tabk 2) (c) Total net income/namber of doctors (see Tabk 2) (c) and (d) see methods section.
CPI: Consumer Price Index; AWE Average Weekly Earnings; MFI: Medical Fee Index.
TAYLOR 5 COMMUNITY HEALTH STUDIES

70
FIGURE 3
Net income, d r i e s and otber expense8 88 8 proportion of gross business income, medical partnerships (1%6/67 - 1978/79)
66 per cent in 1966/67 to 43 per cent in 1978/79. As expected, this was accompanied by a rise in expenses. However, the expenses that increased were not related to salaries paid, for this component actually declined (as a proportion of gross business income) after 1974/75.
The average annual net income per individual in various professional, business and occupational groups was compared with private medical practitioner income over the period 1966/67 to 1977/78. This was accomplished by expressing the net income of these other groups as a proportion of the net income of doctors (Fig. 4). It can be seen from Fig. 4 that most professions have suffered a decline in income relative to private medical practitioners from the mid 1970s onwards. Only wage and salary earners have managed to increase their relative position (from 21 per cent of private medical practitioner income in 1966/67 to 27 per Cent in 1977/ 78) but this change may be spurious kcause of possible increasing use of tax avoidance schemes by doctors.
Tabulations were produced in the 1977/78 taxation statistics which permitted an analysis of the Occurrence of high income earners in the various occupational categories (Table 4). The
TAYLOR 6
frequency distributions of taxable income for various Occupational groups were given. The values of $32,OoO, $50,000 and $ 100,OOO per annum were selected as cut-off points for computing the frequency of high-income earners.
It can be seen from Table 4 that although those who have an income from business and are classified as Health, Education and Welfare make up only 0.7 per cent of total tax payers, they comprise 24 per cent of those earning over $32,000 per annum and approximately 34 per cent of those earning over S50,OOO per annum or $100,000 per annum. Half of the category Health, Education and Welfare is composed of medical practitioners, and it is likely that the proportions mentioned above would be higher if doctors could be isolated in one group.
An examination of frequency of high-income earners amongst the various occupational groups also reveals intersting findings. Whereas the frequency of high-income earners amongst all taxpayers was 6.7/1000,1.8/1000andO.2/1OOOfor the income groups >$32.000, >$SO,OOO and >$100,OOO respectively, for the category Health, Education and Welfare the frequency was 239.7/ 1000, 90.8/ 1000 and 1 l.O/ 1OOO.
COMMUNITY HEALTH STUDIES

I
-.,;.=v ..... .... - - - ”... --_.
..._. ............... ~ ........ ........... ..........................
1-7 ow u mrn WI nm TIP, IM. ww wx I.npl .,%.
FIGURE 4
Mean annual net income in various profdonal and occupational groups, expressed as a proportion of private medical practitioner income.
TABLE 4
High Income Eunem in the Vuioua Occupationd Group. 1977/78
Occupational Proportion of Frquency (per 1OOO) of Proportion (96) of all Groups all Taxpaycrs High Income Earners+ Taxpaycrs with various
232 250 5100 1 3 2 150 a00
by Occupational Group: Annual Incomes- (%)
occupation 1 Income from Salary 69.8 and Wages Occupation 2 Income from PrOPcf iY (+ salary) 12.0
1.4 0.1 < 0.1 14.3 5. I 1.3
13.8 3. I 0.4 24.7 20.8 21.5
occupation 3 Income from Business: Rimry production Mining < Manufacturing Construction Trarapoa&comrmnuniCaton Wholesale/ Retail Finance/ Insurance Health, Education Welfare Otherhot stated
4.9 : 0.1 0.9 2.8 1.2 3.8 1.6
8.7 19.3 11.1 3.4 3.2
11.5 55.7
2.0 5.5 3.1 0.8 0.5 2.9
19.7
0.3 6.3 NA 0.9 0.6 1.5 0. I 1.4 NA 0.6 0.4 6.5 2.6 13.5
5.4 0.1 1.5 1.3 0.3 6.2
18.0
6.7 NA 2.2 I .4 NA 6.3
18.6
0.7 2.3
239.7 29.2
90.8 5.0
11.0 24.4 0.8 6.7
34.9 6.5
33.4 8.1
Totals 100.0 6.7. 1.8. 0.25 100;0 100.0 100.0
+ Declared Taxable Income in S x 101 per annum. * Frquency of High Income Earners amongst all Taxpayers. NA: Not Available.
TAYLOR 7 COMMUNITY HEALTH STUDIES

Discussion The data concerning income in private
practice presented ip this article are derived from taxation statistics published by the Australian (Commonwealth) Government.' Changing definitions and methods of calculation and tabulation have sometimes caused difficulty in interpretation and the most recent published statistics preclude further analysis of the kind presented in this report. However, care has been taken to provide the most complete and comparable figures on income in private practice from 1966/67 to 1977/78.
Although data on average annual net income per doctor in private practice was readily obtainable, the extent to which this is a measure of real income, given the current prevalence of tax avoidance, is difficult to determine. It seems that tax avoidance schemes have been pursued with greater determination and vigour by the medical profession in recent years, and medical conferences even give star billing to tax consultant (avoidmce) experts.+
For this reason average annual gross income per private doctor was estimated using a combination of information from the partnerships and trusts schedule and the individual schedule. This effort proved worthwhile since there were differences in the secular movements of indices derived from the two income measures (that is, net income and estimated gross income).
Both the net and estimated gross income indices, deflated for the Consumer Price Index (CPI), peaked in 1975/76 - although the gross income index was higher. The decline in the CPI- deflated income index was more marked for net income than for gross. This may have been a result of the success of measures designed to subsume part of actual income into "business expenses".
The AWEdeflated net and estimated gross income indices followed similar secular trends as the CPIkflated indices. However, whereas the AWEdeflated net income index was nearly always less than 100 (except in 1975/76), the AWE- deflated gross income index was almost always above 100 (except in 1974/75). Consideration of only AWEdeflated average annual net income per doctor might invite the conclusion that there has +The Third International General Medical Conference in Bali (April, 1981) devoted 25 per cent of lecture time to "investment" and had a "brilliant investmentltax advisor" as one of the "outstanding guest lecturers" (see brochure, AMA travel service, 1981).
TAYLOR 8
been an erosion of private medical practitioner incomes relative to average weekly earnings since 1966/67. However, the movements in AWE- deflated estimated average gross annual income per doctor during the 1970s suggests that, for most of the period, medical practitioners had improved their position relative to the income of others in the community.
Income indices deflated by the MFI adjust for changes in medical fees over time and thus, provide a measure of private medical "activity". It can be seen from the results presented that there was no significant increase in utilization of medical services in 1976/76, the year of the introduction of Medibank, and that the rise in doctor incomes in that year was principally due to medical fee increases. The gross income index per doctor even declined in 1975/76, compared to the previous year, when deflated for MFI. This is in line with other estimates of use of medical services in the Medibank year: these estimates also point firmly to the dominant influence of medical fee increases in the escalation of medical costs and doctor incomes during this period, rather than the direct effect of Medibank (through 'over-utilization").6,7
The decline in net, as a proportion of estimated gross, income per doctor over the period of study is an interesting phenomenon. These declines in net income in relation to gross income are ostensibly due to increases in practice expenses. The Australian Medical Association has claimed that a "major cause has been the movement to equal pay for female employees".8 However, an examination of the information available on medical partnerships quite clearly shows that salaries paid as a proportion of gross income have declined in recent years and that it is other expenses which have increased.
Compared to other professionals and businessmen it appears that private medical practitioners are doing nicely. When the average net income per individual in various occupational groups engaged in private business is expressed as a proportion of private medical practitioner income, it is apparent that doctors have improved their position relative to other groups since 1966/67 and, particularly, since the mid-1970s.
Another way of examining the income of private practitioners in relation to other occupational groups is through an analysis of the frequency of high income earners in the various occupational categories. Amongst all taxpayers
COMMUNITY HEALTH STUDIES

the frequency of taxable incomes L$32,000, >$50,000 and >$100,O00 per annum was 6.7, 1.8 and 0.2 per 1,OOO respectively. However, amongst the Health, Education and Welfare (private business) group, containing private medical practitioners, the rates were 239.7, 90.8 and 11.00 per 1,OOO for the three income groups. This frequency of high income earners is more than four times that of the closest group, Finance and Insurance. As Powles has pointed out, since doctors earn as much, or more, than senior management in business, or financiers, private medical practitioners are doing as well, or better, than “those who are in the business of making money”.9
What the appropriate level of private medical practitioner income should be is a matter for debate. According to the tenets of the free market system - a philosophy subscribed to by many doctors - the present high income of private practitioners is evidence of a significant shortage of doctors in private practice.10 Yet is is almost universally agreed that there are sufficient, if not excess numbers of doctors in relation to patients in Australia, particularly in urban areas. Furthermore, in a market system the price of goods or services should fall with increased volume of sales because of the effect of additional competition.5 However, this phenomenon has not been observed in the Australian medical “market”. The anomalies described above and the current level of incomes in private practice have been ascr ibed t o “. . . the monopol i s t ic and institutionalized system of medical price setting**.lo
The dependence of high incomes in private practice on insurance and government subsidies of medical fees cannot be overemphasised. Most people would be unable to afford doctors’ fees at current levels if it was not for medical insurance and many would be unable to afford insurance if it was not for the Commonwealth Medical Benefit which keeps premiums down to reasonable levels. If medical practice were conducted in a free market it is likely that medical fees and private doctor incomes would be much less.
The Australian Medical Association appears to be most interested in maintaining income relativities between private practitioners and wage earners. At least this is the approach they take in their submissions to enquiries into medical fees for medical benefit purposes.II However, the level of medical income in private practice depends on how it is calculated and to what extent personal
TAYLOR 9
consumption expenditure is subsumed within practice expenses. Furthermore, it has been claimed that the maintenance of income relativities between doctors and other similar professions, rather than salary and wage earners, would be a more appropriate yardstick.
On the other side of the argument the Doctors’ Reform Society believes that private practitioners, particularly radiologists and pathologists, are over-paid and has made statements to this effect.12
Although there are no specific guidelines for determining if a certain group is over-paid, the high income of private practitioners relative to others, in the context of a heavily subsidized and monopolistic medical “market”, suggests that the remuneration of private doctors is excessive. The inflated incomes in private practice are particularly noteworthy in view of the adequate (and probably excessive) supply of doctors and the desirability of medicine as a profession, not requiring extraordinary remuneration in order to attract suitable candidates. It is also worth observing that a public opinion survey revealed that approximately 30 per cent of those polled by the Age newspaper in 1979 thought that doctors are paid “far too mucW.13
Rather than continue public subsidy of private practice in these circumstances, one would think that a quality medical system could be organized which does not involve the public provision of such an affluent way of life for those who have such intrinsically rewarding jobs as doctors. The Scheme proposed by Opit is a feasible alternative4
1. Publicly-funded, salaried, specialist and hospital services for those in need of care; and private practice and private insurance, at market rates, for those who prefer to seek care outside of the public system.
2. Universal insurance for primary care, coupled with a much reduced medical benefits schedule, and adequate monitoring to detect and prevent abuse.
Opit’s suggestions are based on the premise that essential medical services should be regarded as a public utility, rather than private consumption, and that most resources should be directed towards the most essential services, even though they may not be the most profitable for private medicine.
COMMUNITY HEALTH STUDIES

Aeknorledgcrncnts 1 would like to thank Dr Richard Scotton (Division of
Planning & Research, Health Commission of Victoria) for his invaluabk assistance in providing unpublished figuresand for his guidance in the analysis of the data. Dr John Deeble (Health Research Project, Australian National Univmity). and Dr John Powles (Department of Social & Preventive Medicine, Monash University Medical School) also provided valuable advice. However. the inferences made from the data and the conclusions drawn in this article do not necessarily represent the views of those who provided assistance.
References
1. Grattan M, Metherell M. “Clamp on health 8. Passmore L. (Assistant Secretary-General, Australian Medical Association). “Doctors incomes and the AMA.” Letter to the editor, Age, 11 September 1981.
Powles J. “Are our doctors overpaid?“ Age, 20 September 1979.
cheats. AMA says $lOOm milked each year”. Age, 4 February 1982.
Knopfelmacher F. Letter to the editor. Age, 5 March 1981.
9. 2.
3. Commissioner of Taxation. Taxatfon 10. Scotton R. “Medical manpower - some Statistics. Supplements to the reports to policy issues” in Tatchell, P.M. (ed.) parliament (parliamentary papers), Economics and Health: Proceedings of the Australian Taxation Office, Canberra, First Australian Conference of Health Australian Capital Territory, 1966/ 67 - Economists, Health Research Project, l977/ 78. Technical Paper No. 3, Australian National
University, Canberra, 1980.
11. Ludeke J.T. 1979 Enquiry on Medical Fees for Medical Benefit Purposes Report. Document 565/ I /79. Commonwealth Department of Health, July 1979.
4. Cameron R. Year Book Australia, No. 64, 1980. Australian Bureau of Statistics, Canberra, Austalia. ABS Catalogue NO. 1301.0.
5. Deeble J. “Medical fees under insurance” in 12. Walsh G. “Doctors to get $80,000. Average Tatchell P.M. (4.) Economics and Health, income increases 70 per cent since 1981, Health Research Project, Technical Paper No. 6, Australian National University, Canberra, 1982, pp. 24-56.
6. Scotton R. “Costs and use of medical 14. Opit L.J. Submission to the Enquiry into the services”. Australian Economic Review. NO. Efficiency and Management of Hospitals. 42, p.72-76, 1978. Commonwealth Department of Health.
Department of Social and Preventive 7. Deeble J. “Financing health care in a static Medicine, Monash University Medical
School, 1980. Reprinted in New Doctor No.
1975.”Age, 23 July 1979.
13. “Doctors head the overpaid list“. Age, 10 January 1979.
economy*, Social Science and Medicine, V. 19, pp. 28-35, 1981. 16, 1982, pp. 713-724.
TAYLOR 10 COMMUNITY HEALTH STUDIES