Embed Size (px)
Citation preview

Incidence of Viral and Fungal Infections followingBusulfan-Based Reduced-Intensity versus
Myeloablative Conditioning in Pediatric AllogeneicStem Cell Transplantation Recipients
Prakash Satwani, I Leah Baldinger, I jason Freedman, I judith S. jacobson,2 jon Guerra, I
Carmel/a van de Ven,1 Erin Morris, I james Garvin, I Diane George, I M. Brigid Bradley, I
Monica Bhatia/ Bradford Tal/amy/ joseph Schwartz,3 Zhezhen jin,4 Mitchell S. Cairo 1,3,5
Reductions in the duration and nadir of neutropenia have translated into a significant decrease in bacteremia
in adult recipients of allogeneic stem cell transplantation (allo-SCT) with reduced-intensity conditioning(RIC) during the first 30 days after transplantation. It remains to be determined whether RIC allo-SCTalso will result in a decrease in systemic viral infections (SVls) and invasive fungal infections (IFls), whichare more dependent on alterations in cellular immunity. We compared the incidence of SVls and IFls in children receiving busulfan-based RIC allo-SCTand in children receiving myeloablative conditioning (MAC) alloSCT for various malignant and nonmalignant diseases. Allo-SCT recipients at risk for cytomegalovirus (CMV)received ganciclovir/foscarnet, and most of the patients received antifungal prophylaxis with liposomal amphotericin B until day + 100. Eighty-six patients (median age, 7.5 years; 70% with malignant disease, 30% withnonmalignant disease; 80% average risk, 20% poor risk) were evaluated. The probability of developing gradeII-IVacute graft-versus-host disease (aGVHD) was 29.1% (95% confidence interval [CI] = 16.7%-41.6%) inRIC allo-SCT versus 40.3% (95% CI=23.9%-56.6%) in MAC allo-SCT (P=.23), and that of chronic GVHD(cGVHD) was 28.9% (95% CI= 14.7%-43.0%) in RIC allo-SCT versus 28.4% (95% CI= 10.5%-46.3%) inMAC allo-SCT (P=.73). The overall probability of developing an SVI was 58%, and that of developing anIFIwas 15%.These probabilities did not differ significantly by conditioning intensity. In a multivariate Cox regression model, the following were identified as independent risk factors for invasive fungal infection: olderage (hazard ratio [HR]=1.3; 95% CI=I.I-1.6; P=<.OI), poor risk status (HR=6.5; 95% CI =1.1-37.4;P=.03), and CMV-positive recipient (high vs low CMV risk group, HR=26.7; 95% CI=3.4-210.8; P=<.OI).Overall infection-related mortality was only 1.1% (1/86) for SVls and 2.3% (2/86) for IFls. Our data indicatethat RIC allo-SCT does not carry a lower risk of SVls and IFls than MAC allo-SCT in pediatric recipients.
BioI Blood i'v1arrow Tmllsplant 15: 1587-1595 (2009) © 2009 Americall Societyfiir Blood alld Marrow Tmmpumtatioll
KEY WORDS: Reduced intensity, Infection, Myeloablative, Allogeneic stem cell transplantation
INTRODUCTION
From the lDeparnnem of Pediatrics; 2Dep'1rnnent of Epidemiology, :vlailman School ofPuhlic Health, Columbia University,New York, New York; 1.>athology; "Biostatistics; and 'Aledicinc,lvlorgan Stanley Children's Hospital of New York-Presbytelian.
Prcsented in part at the American Society of Blood and MarrowTransplantation's annual meeting, San Diego, Califomia,Fcbruary 2008.
Finrmcinl di.•.do.wre: See Acknowledgments on page 1594.Correspondence and reprint requests: ,\1itchell S. Cairo, MD,
Division of Pediatric Blood and Marrow Transplantation,
,\lorgan Stanley Children's Hospital of New York-Presbytelian,Columbia University, 3959 Broadway, CI-IN 10-03, New York,NY 10032 (e-mail: [email protected]).
Received April 21, 2009; accepted August 7, 2009© 2009 Amelican Society for Blood and ""'larrow Transplantation1083-8791/09/1512-0012$36.00/0
doi: 1D.l016/j.bbmt.20D9.08.006
Allogeneic hematopoietic stem cell transplantation(allo-SCT) as a treatment option for hematologic malih'11ancieshas long been based on the assumption thatmyeloablative (MA) doses of cytotoxic therapy are required for both disease eradication and host immunosuppression. But the last decade has seen a paradigmshift toward the curative potential of a graft-versusleukemia (GVL) or graft-versus-tumor (GVT) effect[I]. The concept behind reduced-intensity conditioning (RIC) allo-SCT is that instead of eradicating tumors through intensive/toxic chemoradiation, tumoreradication is done using the SCT donor's immunecells, relying on allogeneic GVT effects [2]. In patientswith nonmalignant disease, the aim of RIC allo-SCT isto create an immunologic platform of host and donor
1587

1588 P. Satwani et 01. BioI Blood Marrow Transplant 15:1587-1595.2009
tolerance using pre transplantation and posttransplantation immunosuppression.
Data on RIC allo-SCT in pediatric recipients arelimited [3,4]. We previously demonstrated the feasibility and safety of the RIC allo-SCT approach in children with malignant and nonmalignant diseases [5,6].We also demonstrated the safety of RIC allo-SCTand consolidation with gemtuzumab ozagamicin inchildren with average-risk acute myelogenous leukemia (AvIL) [7].
Following myeloablative conditioning (MAC) alloSCT, patient~ experience a period of profound neutropenia, severe mucositis, and immunodeficiency that canlead to serious infectious complications that may resultin significant morbidity and mortality. Theoretically,RIC allo-SCT could carry a lower risk of opportunisticinfections. The potential mechanism(s) that may beresponsible for this hypothetical reduced infectiousmorbidity following RIC allo-SCT includes shorterduration of severe neutropenia, lower grade of mucositis, enhanced immune reconstitution, decreased rate ofsevere acute graft-versus-host disease (aGVHD), andless use of immunosuppression compared with MACallo-SCT [8,9].Junghanss et a!. [10] reported a significantly reduced risk of bacterial infection during the first100 days posttransplantation in adult recipient~ ofRICallo-SCT. But, because of intense pretransplantationand/or posttransplantation immunosuppression, patients receiving RIC regimens actually may be at greaterrisk for systemic viral infections (SV1s) and invasivefungal infections (1FIs). Identified risk factors for developing SVIs after RIC allo-SCT include lymphopenia,cytomegalovims (CMV), serologic status of the donorand recipient, in vivo T cell depletion using antithymocyte globulin (ATG) oralemtuzumab, and exvivo T celldepletion [11,12].
Adenovirus (ADV) and CMV are serious causes ofmorbidity and mortality in patients undergoing alloSCT. CMV infection is one of the most devastatinginfectious complications associated with allo-SCT.CNIV reactivation occurs in 60%-80% of allo-SCT
recipients who are CMV-seropositive and/or havea seropositive donor and do not receive CMV prophylaxis and/or preemptive therapy [13]. The rate of ADVinfection in allo-SCT recipients is 5%-27%, and mortality ranges from 8% to 54%. The mortality rate ishigher in patients with ADV pneumonia (73%) anddisseminated disease (61%) [14]. The rate of ADVinfection is 4%-6% in adult allo-SCT recipients, butas high as 47% in pediatric allo-SCT recipients [IS].
IFI is another leading cause of infectious mortalityfollowingallo-SCT (10%-20%) [16]. The incidence ofIFIs has increased from 5.7% to 11.2% over the last
decade [17]. Risk factors for developing an 11'1 includeprolonged neutropenia, unrelated or mismatcheddonor source, and aGVHD or chronic GVHD(cGVHD) and its treatment. Adult RIC allo-SCT
and MAC allo-SCT recipients have equivalent risbfor aspergillosis; however, there was a trend towardincreased I-year survival in RIC alIo-SCT recipientsfollowing invasive aspergillosis [18].
There have been a few prospective ,md retrospective studies in adults regarding the incidence andoutcome of SVIs and IFIs following RIC allo-SCT[10-12]. Some of tl10se studies have suggested thatRIC allo-SCT is associated with increased risk of
0\1V, Epstein-Barr virus (EEV) , ADV, and IFIs[14-18]. Children undergoing allo-SCT may be atgreater risk for primary viral infections; however, thereis a paucity of data on SVIs and IFIs in children following RIC and MAC alIo-SCT. In the present study, wecompared the incidence and risk factors for SVIs andIFIs following busulfan-based RIC allo-SCT versusMAC allo-SCT.
PATIENTS AND METHODS
Patients
Patients included consecutive children and adolescents who underwent busulfan (Bu)-based RIC aIloSCT at the Morgan Stanley Children's Hospital ofNew York-Presbyterian, between January 2001 andDecember 2007. Indications for transplantation included various malignant and nonmalignant conditions. Allogeneic stem cell sources included bonemarrow (BM), peripheral blood stem cells (PBSCs),and umbilical cord blood (VCB). Poor-risk malignantpatients were defined as those with chemoresistant malignant disease, in third complete remission (CR3) orgreater, induction failure, progressive disease, and/orreceiving a second allograft. All other patients with malignant and nonmalig'nant diseases were defined as average risk. All patients were on clinical protocols forallo-SCT approved by the Institutional Review Boardat Columbia University Medical Center, and all research protocols were in compliance with the Declaration of Helsinki.
Conditioning Regimens
The conditioning regimens were protocol-drivenand disease-specific. Patients with comorbid featuresbefore undergoing allo-SCT were prioritized forRIC regimens; prioritization of the remaining patientswas protocol-driven and disease-specific. All patientswithout c0l110rbid features were offered MAC. The
RIC am1 included patients who received Bu (6.4-8mg/kg), Rudarabine (Flu; 150-180 mg/m2) ± rabbit
antithymocyte globuli~ (ATG; 8 m¥/kg) or Eu (12.816 mg/kg), and Flu (bO-180 mg/m-) ± alemtuzumab(54 mg/m2). The MAC arm included patients whoreceived Eu (12.8-16 mg/kg), cyclophosphamide (Cy)(120-200 mg/kg) ± rabbit ATG (8 mg/kg) or Bn

BioI Blood Marrow Transplant 15:1587-1595,2009 Viral and Fungal Infections following RIC allo-SCT 1589
(12.8-16 mg/kg), and melphalan (Mel; 135 mg/nl) ±rabbit ATG (8 mglkg). Forty-four children receivedrabbit ATG (MAC allo-SCT, n=21; RIC allo-SCT,n=23), and 16 children received alemtuzumab(54 mg/m2) (MAC allo-SCT, n =0; RIC allo-SCT,n= 16). Patients with acute lymphoblastic leukemia(ALL) were excluded because they were treated witha total body irradiation (TBI)-based MAC regimen.
GVHD Prophylaxis and Grading
aGVHD prophylaxis in the majority of patients(93%) consisted of tacrolimus starting at 0.03 mg/kg/day in a continuous i.v. infusion or 0.12 mg/kgorally twice a day with dosage adjustment to maintainblood levels between 5 and 20 ng/mL, and mycophenolate mofetil (MMF) at 15-30 mg/kg every 6-12hours either orally or i.v., as described previously[19J. Tacrolimus was started either on the first day ofthe conditioning regimen or day -1 pretransplantation, and M.MF was started on day + 1 posttransplantation. Tacrolimus and i\L\1F doses were taperedin patients with :S grade II aGVHD on day + 30 formalignant disease and on day + 180 for nonmalignantdisease [19J. Acute GVHD and cGHVD were gradedaccording to the Seattle criteria [20J. The 8 patientswho received unrelated PBSCs also received metho
trexate (MTA} 15 mg/m2 i.v. on day + 1, followed byMTX 10 mg/m2 via slow i.v. push on days +3, +6,and + 11. Six patients who did not receive tacrolimus/i\:lMF received cyclosporine (CsA) 1.5 mg/kgi.v. from day -3 to day -5, along with MTX as describedabove.
Infection Prophylaxis and Supportive Care
All patients were hospitalized in protectiveisolation, defined as a single hospital room witha high-efficiency particulate air filtration system andreverse-isolation requiring strict hand sanitizationand mask use by staff for patients undergoing unrelated hematopoietic SCT. All patients received sargramostim 250 ~lg/m2/day i.v. from day 0 until the whiteblood cell count reached:::::300/mm3 for 2 days, followed by filgrastim 10 ~lg/kg/day i.v. or s.c. until an,lbsolute neutrophil count (Al"JC) of:::::2500/mm3 wasachieved for 3 days, as described previously [21J. Herpes simplex virus (HSV) prophylaxis consisted of acyclovir 250 mg/m2 i.v. every 8 hours from day -5 untilthe development of engraftment and :S grade II mucositis. Pneumocystis carinii prophylaxis consisted oftrimethoprim/sulfamethoxazole until day -2 and then3 times weekly after myeloid engraftment. Patientsunable to tolerate trimethoprim/sulfamethoxazolereceived i.v. pentamidine prophylaxis every 2 weeks.Fungal prophylaxis consisted of Iiposoma 1amphotericin B 3 mg/kg/day i.v. from day 0 through day + 100, asdescribed previously [221. CMV prophylaxis was
administered as described previously [23J. In brief,patients at risk of acquiring CMV infection (ie,a CMV-positive donor and/or recipient) after achieving an Al'JC> 750/mm3 after allo-SCT receivedfoscarnet 90 mg/kg every other day, alternating Witllganciclovir 5 mg/kg every other day up to day + 100.
Systemic Viral Infections
CMV Infection and CMV Disease
CMV infection was defined as isolation of the
CMV virus or detection of viral nucleic acid in anybody fluid or tissue specimen. CMV systemic diseasewas defined as the isolation of the CMV virus or detec
tion of nucleic acid in any body fluid or tissue specimenalong with evidence of end-organ disease. Low risk forCMV infection was defined as a CMV IgG-negativedonor and recipient; intermediate risk, as CMVIgG-positive donor and CMV IgG-negative recipient;and high risk, as CMV IgG-positive donor and recipient or CMV IgG-positive recipient and CMV IgGnegative donor. [24J
ADV Colonization and Infection
Recovery of ADV from stool culture was defined ascolonization. Patients who were culture- or polymerase chain reaction (PCR)-positive for ADV with corresponding clinical signs and symptoms were consideredto have ADV infection involving tllOse site(s). Disseminated ADV disease was defined as clinical evidence of
ADV infection involving 2 or more organ sites.
Other Viral Infections
BK/]C virus infection was defined as hemorrhagiccystitis with a positive urine PCR. Human herpesvirus-6 (HHV-6) infection was defined as a positivePCR from blood and/or cerebrospinal fluid. Upperrespiratory illness was defined as the acute onset ofany rhinorrhea, sinusitis, pharyngitis, or cough withno clinical or radiologic evidence of lower respiratorytract involvement and/or hypoxia, combined withdetection of the virus in upper respiratory secretions.Lower respiratory illness was defined as clinical signsand symptoms of lower respiratory involvement withradiologic evidence of new pulmonary infiltrates withor without hypoxia associated with detection ofthe virus in nasal washings or broncoalveolar lavagespecimens [25J.
Invasive Fungal Infections
IFIs were divided into candidemia, invasive aspergillosis, and other fungi. Invasive aspergillosis was defined as possible (based on clinical signs and symptomsplus a compatible thoracic computed tomography scanor X-ray), probable (based on clinical signs and symptoms, compatible X-ray findings, plus a positive

1590 P. Satwani et 0/. Bia/ Blood Marrow Transp/ant /5:/587-/595, 2009
respiratolY tract culture for A.pergillu.f spp or positiveg,11actomannan assay), and definite (based on positivehistology for an invasive mold infection by Aspe1-gillus)
infections. Candida infection was defined as a positivefungal blood or urine culture or evidence of infectionin any organ system on radiographic evaluation orproven by biopsy.
Statistical Analysis
The "I: and t-tests were used to compare the characteristics of the 2 groups with respect to categoricaland continuous variables, respectively. Continuousvariables were categorized when not normally distributed. Univariate and multivariate Cox regressionmodels were used to evaluate the association of differ
ent risk factors for posttransplantation SVIs and IFIs.The endpoint was time to diagnosis of SVIs and IFlsseparately. Patients were censored at relapse, death,subsequent transplantation, or end of follow-up. Forpatients who received more than 1 Bu-based conditioning regimen during the specified time period,only the first transplantation was evaluated. Onepatient whose exact date of death was unknown wascensored at the date of last contact. In patients withmultiple infectious outcomes posttransplantation,only the first incident that met one or both of the foregoing definitions was included in the analysis. Timedependent variables, such as GVHD, were consideredpotential risk factors only if they occurred before infection was diagnosed. Assumptions for proportionalhazards over time were checked for each model used.
Kaplan-Meier statistics and log-rank tests were usedto compare time to infection and survival betweengroups. All reported P values are 2-sided and usea significance level of .05. All statistical calculationswere performed using SAS 9.1 (SAS Institute, CalY,NC). The multivariate model controlled for recipientage, sex, diagnosis, conditioning type, stem cell source,donor type, GVI-ID, and risk.
RESULTS
Patients and Demographic Data
A total of86 patients (52 males, 34 females; medianage, 7.5 years) received a Bu-based conditioning regimen during the study period. One patient who diedof progressive disease on day + 1 was deemedineligible for analysis. The RIC arm comprised 53patients, 39 of whom (74%) underwent transplantationfor a malignant condition (AML, n= 13; neuroblastoma, n=9; Hodgkin lymphoma [HL], n=8; chronicmyelogenous leukemia [CML], n=4; non-Hodgkinlymphoma, n=4; and biphenotypic leukemia, n= 1)and 14 of whom (26%) underwent transplantationfor a nonmalignant condition (sickle cell disease,
n=7; myelodysplastic syndrome [MDS], n=2; thalassemia, n=2; severe aplastic anemia [SAA], n=2; andscleroderma, n = 1). Of the 33 patients in the MACarm, 21 (64%) ill1derwent transplantation for a malignant condition (AML, n = 18; ALL, n = 1; undifferentiated leukemia, n= 1; and neuroblastoma, n= 1) and 12(36%) 1mderwent transplantation for a nonmalignantcondition (sickle cell disease, n=6; thalassemia, n=2;and hemophagocytic lymphohistiocytosis, n=4) (Table 1). The patients in the RIC and MAC arms hadsimilar performance status (95.31 ± 1.6 vs 93 .8± 1.8;P=not significant).
Donor Sources
The donor sources in the RIC arm included UCB
in 28, PBSCs in 20 (14 related and 6 unrelated), andBNl in 5 (4 related and 1 unrelated). In the MACarm, the donor source was UCB in 18, PBSCs in 7(4 related and 3 unrelated), and BM in 8 (7 relatedand 1 unrelated).
Engraftment
The median time to neutrophil and plateletengraftment was 17 days and 30 days, respectively inthe RIC arm and 14 days and 44 days, respectively,in the MAC arm.
GVHD
The probability of developing aGVHD gradeII-IV was 29.1 % (95% confidence interval [CI]=16.7%-41.6%) in the RIC arm versus 40.3% (95%CI=23.9%-56.6%) in the MAC arm (P=.23 [not significant]). The probability of developing cGVHDwas 28.9% (95% CI=14.7%-43.0%) in the RIC armversus 28.4% (95% CI= 10.5%-46.3%) in the MACarm (P=.73 [not significant]).
Infections
SVls
A total of 50 patients developed an SVI (RIC,n=29; l\1AC, n=21) a median of 37 days (range,10-449 days) after allo-SCT. In the RIC arm, the median time to onset of SVI was 70 days (range, 10-252days), and the infectious organisms identified includedHSV (n=3), CMV (n=4), ADV (n=4), respiratorysyncytial vims (RSV; n=4), polyomavims (n=6), parainfluenza (n=3), rotavirus (n=2), varicella zoster virus(VZV; n= 1), and calicivirus (n= 1). In the MAC arm,the median time to onset of SVI was 33 days (range,11-449 days), and the following viral organisms wereidentified: polyomavirus (n=8), CMV (n=5), RSV(n=3), lISV (n=2), parainfluenza (n=1), HlIV-6(n=I), rotavirus (n=I), and ADV (n=I). The overallprobability of developing an Sv'I was 58%. This probability did not differ significantly by conditioning

BioI Blood Marrow Transplant 15:1587-1595,2009 Viral and Fungal Infections following RIC allo-SCT 1591
Table I. Demographic and Clinical Characteristics Table 2. Multivariate Analysis of the Risk Factors for SVls andIFls
100_L_ Reduced Inlensity
Myeloablative
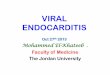
Figure I. Kaplan-Meier probability of developing an SVI in children inthe RIC arm versus those in the MAC arm.
oo 300 600 900 120015001800210024002700 3000
Day
IFls
A total of 13 patients developed an 11'1 (RIC arm,n=10; MAC arm, n=3), occurring a median of 160days (range, 8-630 days) after alIo-SCT. In the RICarm, the median time to onset of 11'1 was 135 days(range, 8-630 days), and the species associated withinfection were Candida spp (n = 7), AJ1Je"rgi//uJ" spp(n = 2), and mucor (n = 1). In the NIAC am1, the mediantime to onset of infection after alIo-SCT was 167 days(range, 41-260 days). Of the 3 infections in this group,2 resulted from Candida spp and 1 frin ScedoJporium
spp. Most (62%) ofthe fungal infections occurred before day + ISO. The overall probability of developingan 11'1 was 15%. This probability did not differsignificantly between the RIC and MAC anns(P= .24) (Figure 2). In univariate analysis, only agewas significantly related to 11'1; children age<7.5 yearsappeared to have a lower risk than older children(HR=O.2; 95% CI=0.04-0.74; P=.(2). In a multivariate Cox regression model, the following were identified as independent risk factors for 11'1; older age(HR=1.3; 95% CI=1.1-1.6; P < .01), poor risk
a seronegative donor (hazard ratio [HR] =2.9; 95%CI=1.2-7.2; P=.02) (rable 2). RabbitATG and alemtuzumab were not associated with a significant increasein SVIs in the univariate and multivariate analyses.
RIC indicates reduced intensity conditioning; SVls, systemic viral infec
tions; IFls, invasive fungal infections; MAC, myeloablative conditioning;
PBSCs, peripheral blood stem cells; BM, bone marrow; UCB, umbilical
cord blood; CMV, cytomegalovirus; GVHD. gralt-versus-host disease.
SVlsIFls
Risk Factor
HR (95% CI)PHR (95% CI)P
RegimenRIC
1.00 (reference)1.00 (reference)MA
1.28 (0.67-2.42).460.12 (0.02-0.77) .03
CMV risk group Low1.00 (reference)1.00 (reference)
Intermediate1.15 (0.44-3.02).797.25 (0.75-69.73) .07
High2.83 (1.14-6.98).0326.73 (3.39-210.78)< .01
GVHD Acute grade 0-'1.00 (reference)1.00 (reference)
Acute grade II-IV1.63 (0.87-3.04).132.25 (0.46-10.97) .31
Any chronic0.89 (0.43-1.85).750.76 (0.18-3.20) .71
Donor type Matched related1.00 (reference)1.00 (reference)
Alternative donor1.53 (0.70-3.35).690.77 (0.13-4.57) .78
Age :$7.5 years
1.00 (reference)1.00 (reference)> 7.5 years
1.05 (0.99-1.11).111.33 (1.13-1.56) < .01Sex Female
1.00 (reference)1.00 (reference)Male
1.05 (0.56-1.97).900.72 (0.16-3.20) .67Stem cell source PBSCs/BM
1.00 (reference)1.00 (reference)UCB
0.86 (0.36-2.0 I).726.26 (0.90-43.58) .06Risk Average
1.00 (reference)1.00 (reference)Poor
0.89 (0.38-2.07).786.54 (1.14-37.36) .03
1tJ __ .J __ '__ t". LJ'-1. .&...11....1 __ U __ .J __ J __ I I
,r,
tI..I
80
20-
c:o""u,S,!
.s 60e:>'0g 40:D\1)
.Qe
Q.
RIC indicates reduced intensity conditioning; MAC, myeloablative con
ditioning; PBSCs, peripheral blood stem cells; BM, bone marrow;
UCB, umbilical cord blood; CMV. cytomegalovirus; ANC, absolute neu
trophil count; GVHD. gralt-versus-host disease.
intensity (P=.44) (Figure 1). In both univariate andmultivariate analyses, the only statistically significantrisk factor for SVI was CMV risk; subjects who wereseropositive ancllor had a seropositive donor hadnearly 3 times the risk of seronegative subjects with
RIC Arm,MAC Arm.Total,Characteristic
n (%)n (%)n (%)P
Patients
53 (62)33 (38)86 (100)Sex Male
33 (62)19 (58)52 (40)Female
20 (38)14 (42)34 (60),67
Age >7.5 years
26 (49)17 (52)43 (50).82
Ethnicity White19 (36)9 (27)28 (33)
Black10 (19)4 (12)14 (16)
Hispanic15 (28)9 (27)24 (28)
Other9 (17)II (34)20 (23).334
Diagnosis Malignant39 (74)21 (64)60 (70)
Nonmalignant14 (26)12 (36)26 (30).33
Risk status Poor risk10 (19)7 (21)17 (20).79
Average isk
43 (81)26 (79)69 (80)
Previous transplantation
19 (36)0(0)19 (22)< .01
Stem cell source PBSCs/BM25 (47)15 (45)40 (47).88
UCB28 (53)18 (55)46 (53)
Matched related donor16 (30)II (33)27 (31).76
CMV risk group Low17 (32)6 (19)23 (27)
Intermediate13 (25)7 (22)20 (24)
High
23 (43)19 (59)42 (49).30
Hematopoietic recovery ANC recovery < 17 days
21 (49)26 (64)47 (55).19
Platelet engraftment <32 days8 (15)5 (IS)13 (15).99
GVHD status Acute grade II-IV
16 (30)13 (39)29 (34).38Chronic
12 (23)6 (18)18 (21).62

1592 P. Satwani et 0/. BioI Blood Marrow Transplant 15:/587-1595.2009
100, Table 3. Multivariate Analysis of Risk Factor for Mortality_.L. Reduced Intensity --------------------------
Myeloablative
Figure 2. Kaplan-Meier probability of developing an IFI in children inthe RIC arm versus those in the MAC arm.
Figure 3. Kaplan-Meier probability for as in children in the RIC armversus those in the MAC arm.
':] ""o 300 600 900 1200 1500 1800 2100 2400 2700
Day
RIC indicates reduced intensity conditioning; SVls, systemic viral infec
tions; IFls. invasive fungal infections: MAC. myeloablative conditioning;
PBSCs, peripheral blood stem cells; BM. bone marrow; UCB. umbilical
cord blood; CMV. cytomegalovirus; GVHD. graft-versus-host disease.
in terms of overall survival (OS) (P=.4) (Fig'ure 3).Factors significantly associ<Jted with mortality in themultivariate model included poor risk (HR=3.5;95% CI=1.3- 9.5; P=.OI), IFI (HR=2.6; 95%CI = 1.1-6.0; P= .02) and previous transplantation(HR=4.5; 95% CI=1.2-16.7; P=.02) (Table 3). Themultivariate model controlled for conditioning type,diagnosis, age, sex, stem cell source, CMV risk group,<JndGVHD. Having an SVI W<JSnot associated withpoor survival (P=.87), but having an IFI significantlyreduced OS (P < .01). This difference persistedwhen the analysis was stratified by conditioning type.Overall infection-related mortality was only 1.1%(1/86) for SVIs and 2.3% (2/86) for IFk The onlydeath likely related to an SVI was secondary to RSVpneumonia in a patient with induction failure ANlLon day + 144 after an HLA-matched sibling RIC<Jllo-SCT; during administration of aerosolized ribav<Jrin, the patient relapsed and died of A.ML. Twodeaths were related to IF!. One patient had SAA andgrade III aGVHD and subsequently developed
Risk Factor HR (95% CI)P
RegimenRIC
1.00 (reference)MAC
1.12 (0.40-3.57).75
CMV risk group Low1.00 (reference)
Intermediate0.17 (0.04-0.98).05
High0.80 (0.29-2.32).69
GVHD Acute grade 0-1
1.00 (reference)
Acute grade II-IV
1.93 (0.76-4.95).17
Any chronic0.60 (0.18-2.02).41
Diagnoses Nonmalignant1.00 (reference)
Malignant
2.79 (0.73-0.70).13
Donor type Matched related1.00 (reference)
Alternative donor0.98 (0.28-3.48).98
Age 0:;7.5 years
1.00 (reference)
>7.5 years
1.03 (0.95-1.12).53Sex Female
1.00 (reference)Male
0.68 (0.29-1.56).36
Stem cell source PBSCs/BM1.00 (reference)
UCB3.23 (1.00-10.42).05
Risk Average
1.00 (reference)Poor
3.53 (1.31-9.51).01
Previous transplantation No1.0 (reference)
Yes4.53 (1.23-16.77).02
IFls No1.0 (reference)
Yes4.66 (1.52-14.35)< .01
SVls No1.0 (reference)
Yes0.65 (0.27-1.53).31
Reduced Intensity
-'- Myeloablatlve
't_.J.JL1- J. •••
, -t_I_~~~_~IoUJ.&..&.U ~~~~J
300 600 900 1200150018002100240027003000
Day
t_.L. _ J.II.FltI.JIW_U Io••.• .a.-IU 1..\"1..1 _1. __ .JJ. _ J. 1.1
~'L~UI'I
100
_ 80~.~'"
U)
~ 60
~'0g 40:isco.0e
c..
oo
Survival/Mortality
Some 70% of the patients in the RIC arm and 61%of those in the MAC arm were alive at the end of
follow-up, with a median survival of 812 days (range,15-2328 days) and 429 days (range, 39-2808 days),respectively. The 2 groups did not differ significantly
(HR=6.5; 95% CI=1.1-37.4; P=.03), and CMVpositive recipient (high vs low CMV risk group:HR=26.7; 95% CI=3.4-210.8; P < .01) (T<Jble 2).In addition, in the multivariate model, patients in theMAC arm appeared to have a significantly lower riskof IFI than those in the RIC arm (HR=O.I; 95%CI=0.02-0.8; P=.03). Rabbit ATG and alemtuzumabwere not associated with a sihrnificant increase in IFI inthe univariate and multivariate analyses.
c 80o=u~.sro 600>C::JU.'0g 40:arn.ceQ.. 20

BioI Blood Marrow Transplant 15:1587·1595,2009 Viral and Fungal Infections following RIC allo.sCT 1593
Candida lusitallia, and the other had Hodgkin lymphoma and extensive cGVHD, and later died of A:,per
gillus fumigatl/s.
DISCUSSION
Regimen-related mortality after MAC allo-SCT inpediatric recipients can be as high as 20%-40%[26-28]. In our experience with RIC allo-SCT in pediatric recipients, the day + 100 nonrelapse mortality(NRM) was only 1.3% [29]. This decrease in day+ 100 NRM may result in part from the decreasedrisk of early life-threatening infections. However,these 2 different conditioning regimens (RIC andMAC) have not been compared with respect to therates of SVIs and IF Is in pediatric allo-SCT recipients.Here, we report the incidence ofSvls and IFls in children and adolescents who received a Bu-based MAC or
RIC regimen when undergoing allo-SCT. We did notinclude patients who received TEl-based conditioningbecause (1) the most common indication for a TBIbased conditioning regimen is ALL, and we have notperfonned any RIC allo-SCT for ALL, and (2) wehave not used TBI as a part of the conditioning regimen for RIC allo-SCT. The literature on the use ofRIC in children and adults with ALL is limited; however, a recent study by Kennedy-Nasser et a!. [30] ofchildren with ALL who received a TBI-containingMAC regimen found a 16% incidence ofCMV reactivation (14/83), a 19% incidence of adenovirus reactivation (16/83), and a 4.8% incidence of IFls (4/83)[30]. In our study, the incidence of C,\I1V reactivationwas 15%, that of adenovirus reactivation was 3%,and that ofIFI was 9.0% in the MAC arm.
We found no significant difference between pediatric RIC allo-SCT and MAC allo-SCT recipients interms of incidence ofSVI or OS. However, the patientsin the MAC arm appeared to have a significantly lowerrisk of IF!. These results are not surprising given that38% of the patients in the RIC arm received an l'\1ACautologous transplantation before undergoing a RICallo-SCT; their underlying risk of infection may haveinitially been greater because of previous chemotherapy. In addition, while several studies have reporteda similar risk of IFI in RIC allo-SCT and MAC allo
SCT recipients, our findings are more consistent withthose of Fukuda et a!., who found a trend towarda higher risk of invasive aspergillosis among nonmyeloablative (NMA) recipients [18, 31, 32]. In that study,the cumulative incidence rates of proven or probableIFI, invasive mold infections, invasive aspergillosis,and invasive candidiasis during the first year afterallo-SCT with NMA conditioning were 19%, 15%,14%, and 5%, respectively, and 39% deaths were related to a mold infection. In contrast, in our studyonly 2 deaths (2.3%) were related to IF!.
Despite the lower risk ofIFI in the MAC arm, the19% overall risk of developing IFI in the RIC arm wasnot significantly different from the 17% incidencereported in a recent study of adult RIC allo-SCTrecipients [33]. A possible reason for the higher incidence of IFls in RIC allo-SCT recipients may besecondary to the need for prolonged immunosuppression and greater risk of graft failure in RIC allo-SCTrecipients. The use of alemtuzumab in immunosuppressive conditioning has been associated with delayedimmune reconstitution.
Our failure to detect a significant difference in incidence of SVIs is consistent with the result~ of other
studies. In one matched case-controlled study of 168adult allo-SCT recipients, the I-year incidence ofCMV disease was similar in those receiving RIC andthose receiving NlAC [10]. Likewise, a study by Schetelig et a!. [34] comparing aBu-based RIC allo-SCT regimen to MAC allo-SCT conditioning found nosignificant difference in the incidence ofCMV infection[34].
The risk factors for SVls and IFls identified in this
study, including CMV seropositivity and patient age,are similar to tllOse reported previously, with the majorexception of GVHD [35,36]. Our failure to detect anassociation between infection and GVHD in the present study may be from the lower incidence of GVIIDin this population than has been reported previouslyin RIC allo-SCT recipients, and might be linked tothe different GVHD prophylaxis regimens used inour cohort [37].
One potential concern following RIC allo-SCT isthe possible increase in the incidence ofEBV reactivation and Iymphoproliferative disorder, which appearsto be higher in patients receiving ATG as a part ofthe allo-SCT conditioning regimen [38]. In our seriesof 86 patients, 44 received ATG (MAC arm, n=21;RIC arm, n=23) and 16 received alemtuzumab. Noneof the children experienced EBV reactivation, andonly 1 child had EBV-negative lymphoproliferativedisorder. In addition, alemtuzumab has been associatedwith a significant risk of CMV reactivation. Chakrabarti et a!. [39] found a 50% incidence of CMV reactivation in adult patients receiving alemtuzumab as a partof RIC allo-SCT, but a 84.8% probability of developing a CMV reactivation in those patients at intermediate and high risk for Cl\:1V [39]. Similarly in a study byShenoy et a!. [40] of children receiving Flu, Mel, andalemtuzumab RIC, 6 of 7 CMV-positive recipientsand 1 CMV-negative recipient reactivated CNlV. Inour study, 36 of 53 children (68%) in the RIC armwere at intermediate or high risk for CMV infection,but only 4 of these children developed CMV reactivation, including 2 of16 children who received alemtuzumah. This low incidence of CMV reactivation in our
patient population could be due to the aggressiveCl\:1V prophylaxis instituted at our center [23]. \Ve

1594 P. Satwanl et 01. Bioi Blood Marrow Transplant 15:1587-1595.2009
also found no significant difference in the incidence ofSVIs and IFls in children who received ATG and thosewho received alemtuzumab.
The major limitation of this retrospective study isthe small sample size of both groups. Our proportionalhazards assumptions were not met, most likely due tothe small sample size. ""''hen we ran these same analyses using a simple logistic regression model, CMVhigh-risk status was the only significant risk factorfor SVI. ClVIVhigh-risk status, older age, and malignant condition remained significant risk factors forIFI. In addition, CMV intermediate risk, malignantdisease, poor risk disease status, and IFI remained significant risk factors for mortality. These results areconsistent "Tith those from the Cox regression models.Because the subjects were heterogeneous in terms ofunderlying disease and donor source, these preliminary analyses should be replicated in additional studiesof children with more homogenous diagnoses and cellsources.
Despite these limitations, however, we believe thatour central conclusions are valid. The fact that this
study was conducted at a single institution ensuresconsistent policies and protocols in terms of prophylaxis, isolation precautions, and diagnosis of infection.Furthemore, the fact that all conditioning regimenswere busulfan-based allows for grcater comparabilitybetween subjects in the 2 groups.
\\'hen assessing the risk of SVIs and lFrs in childrenundergoing allo-SCT, we need to consider variousothcr factors beyond the conditioning regimcn. Compared with heavily pretreated patients, patients whoundergo allo-SCT for nonmalignant disease (otherthan immunodeficiency) have a lower risk of infectionfollowing allo-SCT due to an intact immune system, absence of chemotherapy-related thymic injury, and lackof significant end organ damage. Patients with ex vivoor in vivo T cell depletion related to alemtuzumab areat risk for SVls due to delayed immune reconstitution.Donor sourcc also may have an impact on the risk ofSVls and IFrs. Compared to with children undergoingallo-SCT with DCB (delayed immune reconstitution)or an unrelated donor (increased risk of GVHD), children undergoing HL\-matched sibling allo-SCT havea lower risk of GyTID and relatively faster immunereconstitution, which may lead to a decreased incidenceof SVIs and lFls. One of the most critical risk factors forSVIs and lFls is GVI-ID and its treatment with steroids
and other immunosuppressive therapy. In our statisticalanalysis, although we controlled for all of these riskfactors, we were unable to demonstrate the individualimpacts of these factors on the risk of SVls and lFls,likely due to the small number of subjects.
In summary, our findings indicate that in children,RlC ,llIo-SCT is not associated with a higher risk ofSVIs compared with MAC allo-SCT, but might beassociated with a greater incidence of IFls. Moreover,
due to the availability of sophisticated monitoring andnewer antibiotics and other therapeutic strategies,both SVIs and lFls are not associated with mortalityin pediatric allo-SCT recipients.
ACKNOVVLEDGMENTS
Financial di.rclo.wre: This work was supported inpart by grants from the Pediatric Cancer ResearchFoundation, Marisa Fund, Dream Discovery andCure Fund, Paul Luisi Foundation, Brittany BaronFund, and Sonia Scaramella Fund. The authors thankthe nurses and infectious disease team for providingexcellent care to the allo-SCT recipients, and LesliePariag for her assistance with manuscript preparation.
REFERENCES
1. Champlin R, Khouri 1, Shimoni A, er al. Harnessing graftversus-malignancy: non-myeloablative preparative regimens forallogeneic haematnpoietic transplantation, an evolving strategyfor adoptive immunotherapy. Br] Hat:motol. 2000;111:18-29.
2. Satwani P, Harrison L, iVlorris E, et al. Reduced-intensityallogeneic stem cell tmnsplantation in adults and children withmalignant and nonmalignant diseases: end of the beginning:md future challenges. Bioi Blood lHmnr.:.' Tromplimt. 2005;11:403-422.
3. Satwani P, Cooper N, Rao K, et al. Reduced-intensity conditioning and allogeneic stem cell transplant:ttion in childhoodmalignant and nonmalignant diseases. Blme lHcl/1'011'Ti·ompI1l11t.2008;41: 173-182.
4. Satwani P, Morris E, Bradley ,'I'lll, et al. Reduced-intensity andnonmyeloahlative allogeneic stem cell transplantation in children and adolescents with malignant and nonmalignant diseases.Pediatr Blood Callcer. 2008;50: 1-8.
5. Bradley MB, Cairo IvlS. Stem cell transph1l1tation for pediatriclymphoma: past, present and future. Balle lV!fI11'ov! Ti·allsplmlt.
2008;41:149-158.6. Del Toro G, Satwani 1', Harrison L, et al. A pilot study of
reduced-intensity conditioning and allogeneic stem cell transplantation from unrelated cord hlood :U1d matched familydonors in children and adolescent recipient~. Bone il1mTIT':"
T1-rI11Jpll/nt. 2004;33:6\3-622.7. Roman E, Cooney E, IIa rrison L, et a1. Preliminary results of
the safety of immunothempy with gemtuzumab ozogamicinfollowing reduced-intensity allogeneic stem cell transplant inchildren with CD33 + acute myeloiJ leukemia. Clill Callce,- Re.\'.2005;11:7164s-7170s.
8. Chalmwerty R, Peggs 1(, Chopra R, et a1.Limiting tl'Jnsph11ltation-related mortality following unrelateJ donor stem cell transphmDttion hy using a nonmyeloahlative conditioning regimen.Blood. 2002;99:1071-1078.
9. N"gler A, Aker M, Or R, et al. Low-intensity conditioning issufficient to ensure engraftmenr in matched unrelated honemarrow transplant"tion. R'(p Hnncltol. 2001;29:362-370.
10. Junghanss C, Boeckh M, Carter RA, et al. Incidence and outcome of cytomeg"lovirus infections following nonmyelo"hlativecompared with myeloablative :lllogeneic stem cell transplant"tion," m:ltched control study. Blood. 2002;99:1978-1985.
II. Boeckh M. Current antiviral strategies for controlling cytomegalovirns in hematopoietic stem cell rransphmt recipient" prevention and therapy. Tt'lImpllnFtt Di.r. 1999;1:165-178.
12. Einsele H, EhningerG, SteidleM, et al. Lymphocytopenia as anunfavorahle prognostic fJctor in patients with cytomegalovirusinfection after hone marrow transplantation. Blood. 1993;82:1672-1678.

BioI Blood Marrow Transplant 15:1587-1595, 2009 Viral and Fungollnfections following RIC allo-SCT 1595
13. \Vinsron DJ, YoungJA, Pullarkat V,etal.lvlarihavirprophylaxis fi)rprevention of tytomegalovims infection in allogeneic stem celltransplant recipients: amulticenter, randomized, douhle-hlind, p1.1ceho-controlled. dose-r:mging study. Blood. 2008;111:5403-5410.
14. Ljungman P. Treatment of adenovirus infections in the immunocompromised host. En/".7 Clin J1;IicrobioIII~{ect Dis. 2004;23:583-588.
15. HoffmanJA, Shah AJ, Ross LA, et al. Adenovirn! infections anda prospective trial of cidofovir in pediatric hematopoietic stemcell transplantation. Bioi Blood jHamJ11' Tm1/.\1>lllllt. 20()!;7:388-394.
16. \Vingard JR. Fungal infections after bone marrow transplant.Bioi Blood l'Hl/rrow Tral1J1Jltmt. 1999:5:55-68.
17. \-Vald A, Leisenring \'1, van Burik JA, et al. Epidemiology ofAspergillu.r infections in a large cohort of patients undergoinghone marrow transplantation.] Infea Dis. 1997:175:1459-1466.
18. Junghanss C, "hrr KA, Carter RA, et ai. Incidence and outcomeof bacterial and fungal infections following nonmyeloablativecompared with myeloablative allogeneic hematopoietic stemcell transplantation: a matched control study. Bioi Blood jHllrrow
']"msplalll.2002;8:512-520.
19. Osunkwo I, 13essmerrny 0, Harrison L, et al. A pilot study oftacrolimus and mycophenolate mofetil graft-vetsus-host diseaseprophylaxis in childhood and adolescent allogeneic stem cell transplant recipients. Bioi Blood Marrow Tmmpltmt. 2004;10:246-258.
20. Glucksberg H, Srnrb R, Fefer A, et al. Clinical manifestations ofgraft-versus-host disease in human recipients of marrow fromHLA-matched sibling donors. ·!i-aJ1.fpltlllffltioll. 1974;18:295-304.
21. \Vaxman I, Nlilitano 0, Baldinger L, et ai. Sequential administration of sargramostim and filgrastim in pediatric allogeneicstem cell transplantation recipients undergoing myeloablativeconditioning. Pediatr T'nJ1/spiaut. 2009: 13:464-474.
22. Roman E, Osun\':wo I, NIilitano 0, ct ai. Liposomal amphotcricin 13prophylaxis of invasivc mold infcctions in children postallogcncic stem cell transplantation. Peditltr Blood Cmu:rl'. 2008;50:325-330.
23. Shereck E13. Cooney E, van de Yen C, et al. A pilot phase IIstudy of alternate-day ganciclovir and foscarnet in preventingcytomegalovims (C\IV) infections in at-risk pedi,uric and adolescent allogeneic stern cell transplant recipients. Prdilltr BloodCancrr.2007;49:306-312.
24. 130eckh M, Nichols \VG. The impact of cytomegalovirus serostatus of donor and recipient before hematopoietic stcrn celltransplantation in the era of antiviml prophybxis and preemptive therapy. Blood. 2004;103:2003-2008.
25. Ljungman P, \Vard KN, Crooks BN, et ai. Respiratoryvims infections after stem cell transplantation: a prospective study fromthe Infcctious Discases \Vorking Party of the European Groupfor Blood ,md '\-hrro\\' Transplantation. Bonr All11'11J1v'Trtm.l'
plont.2001;28:479-484.
26. KurtzhergJ, Laughlin M, Graham ML, et ai. Placent:1! blood asa source of hematopoietic stcm cells for transplantation into unrclated rccipients. N Eugl] Aled. 1996;335:157-166.
27. Locatelli F, Rocha V, Chastang C, et aI. Factors associated withoutcome after cord blood transplantation in children with acuteleukemia. Eurocord-Cord mood Tr-ansplant Group. Blood.1999;93:3662-3671.
28. \Vagner JE, Barkcr IN, DcForTE, et al. Transplantation of unrelated donor umhilical cord hlood in 102 patients with malig-
nant and nonmalignant diseases: influence of CD34 cell doseand HLA disparity on treall11ent-related mortality and survival.Blood. 2002;100:1611-1618.
29. Satw,mi P,Tallamy 13,Kohl V, et a!. Reduced-intensity conditioning (RlC) allogeneic stem cell transplantation in pediatric rccipicnts is associated with very low carly mortality and high donorchimerism [ahstrnctJ. l'edifltr Blood C'tmm'. Puhlished online
(0.149) at, wwwI43.imersciencc.wiley.com/joumaIIl17935000/grouphomelhome.html; 2008. Accessed.
30. Kennedy-Na."er AA, Bollard C\I, Myers GD, et ai. Comparable outcome of altern,uive donor and matched sihling donorhematopoietic stem cell tmnsplant for children with acutelymphoblastic leukemia in first or second remission using alcmrnzumah in a myeloablative conditioning regimen. Bioi BloodMfl17'{J1VJ;,({ll.<plallt. 2008;14:1245-1252.
31. Fukuda '1', Boeelffi M, Carter RA, et aI. Risks ,md outcomcs of
invasive fungal infections in recipients of allogeneic hematopoietic stern cell transplants aftcr nonmyeloablative conditioning.BWod.2003;102:82i-833,
32. iVlartino R, Cahallero MD, Canals C, et al. Reduced-intensityconditioning reduces rhe risk of severe infections afrer allogeneicperipheral hlood stem cell transplantation. Bone Afarrow 'TrtJ1l.\·
plllT/t.2001;28:341-347.
33. Niederwicser D, Maris NI, Shizum JA, et al. Low-dose totalhody irradiation (1'131)and fludarabine followcd hy hematopoietic cell transplantation (HCT) from HLA-matched ormismatched unrelated donors and postgrafting immunosupprcssion with cyclosporine and mycophcnolatc lIlofetil (1\-IM1')can induce durahle complete chimerism and sustained remissions in p,uient~ with hematological diseases. Blood. 2003;101:1620-1629.
34. Schetelig], Oswald 0, Steuer N, et ai. Cytomegalovims infectifms in allogencic stem cell rccipients aftcr reduced-intensityor myeloablative conditioning assessed by quantitative PCRand pp65-antigcnemia. Bom ,111111'071.'']'·fI/ljpla1/t. 2003;32:695-701.
35. Busca A, Locatelli F. Barhlli A. et ai. Infectious complicationsfollowing nonmyeloa blative allogeneic hem,uopoietic stem celltransplantation. TmTl.lpi Infect Dis. 2003;5:132-139.
36. Frcre P, Baron F, Bonnet C, et al. Infcctions after allogeneichematopoietic stem cell transplantation with a nonmyeloahlati\-econditioning regimen. Boll<' Marr071.' Ji·awplant. 2006;37:411-418.
37. Pctersen SL, Madsen HO, Ryder LP, et :11. Haematopoicticstem cell transplantation with non-mycloahlativc conditioningin the outpatient setting: results, complic'ltions ami admissionrequirements in a single institution. B1'] Haernl/tol. 2004;125:225-231.
38. Cohen J, Gandhi M, Naik P, et ai. Increased incidence ofE13V-rel'lted diseasc following paediatric stem cell transplantation with reduced-intensity conditioning. Br] llflemfltol. 2005;129:229-239.
39. Chakraharti S, Mackinnon S, Chopra R, et a1.High incidence ofcytomegalovims infection after nonmycloablative stern celltransplantation: potential rolc of Campath-lI-I in dela)~ngimmune reconstirntion. Blood. 2002;99:4357-4363.
40. Shenoy S, Grossman \VJ, DiPersio], et a1. A novel reducedintensity stcm ccll transplant regimcn for nonmalignantdisorders. B01/e lV1a71'07J)T'm1l.lpltmt. 2005;35:345-352.









![An Unusual Presentation of Fungal Mass in Concha BullosaThe incidence of concha bullosa in vari-ous studies is 14% to 53.6% [1]. The most common content is air. Fungal mass in concha](https://img.pdfslide.us/doc/110x75/5e560abca18caf60756b98cf/an-unusual-presentation-of-fungal-mass-in-concha-bullosa-the-incidence-of-concha.jpg)


















