Embed Size (px)
Citation preview
Incidence of insulin-treated diabetes in Australia 1
Incidence of insulin-treated diabetes in Australia
Web report | Last updated: 25 Mar 2020 | Author: AIHW | Cat no: CDK 11
Citation: Australian Institute of Health and Welfare 2020. Incidence of insulin-treated
diabetes in Australia. Cat. no. CDK 11. Canberra: AIHW.
The Incidence of insulin-treated diabetes in Australia web report presents the
latest available data on new cases of type 1 diabetes and insulin-treated type
2 diabetes. It is part of the ongoing national reporting using the National
(insulin-treated) Diabetes Register (NDR). The NDR is a linked data set,
which includes data from the:
National Diabetes Services Scheme (NDSS)
Australasian Paediatric Endocrine Group (APEG)
National Death Index.
The data are presented by age, sex, trends, population groups and geographic areas.
Key findings 1. In 2018, about 31,300 people began using insulin to treat their diabetes in Australia.
2. Just over 2,800 people were diagnosed with type 1 diabetes—12 cases per 100,000
population.
3. 17,000 people started insulin to manage their type 2 diabetes—4,200 cases per
100,000 people with type 2 diabetes.
4. 1,700 (60%) people diagnosed with type 1 diabetes were aged under 25.
Incidence of insulin-treated diabetes in Australia 2
Incidence of insulin-treated diabetes in Australia Diabetes is a chronic condition marked by high levels of glucose (sugar) in the blood. This is
caused by the body being unable to produce insulin (a hormone made by the pancreas to
control blood glucose levels) or to use insulin effectively, or both.
An estimated 1 in 20 (4.9% or 1.2 million) Australians had diabetes in 2017–18, based on
self-reported data (ABS 2019).
All people with type 1 diabetes, and some with type 2, gestational or other forms of diabetes
will require insulin replacement therapy to manage their condition.
This web report presents the latest available data on new cases of insulin-treated diabetes,
with a focus on type 1 diabetes and insulin-treated type 2 diabetes, in Australia. Data are
from the 2018 National (insulin-treated) Diabetes Register (NDR).
New cases of insulin-treated diabetes in 2018
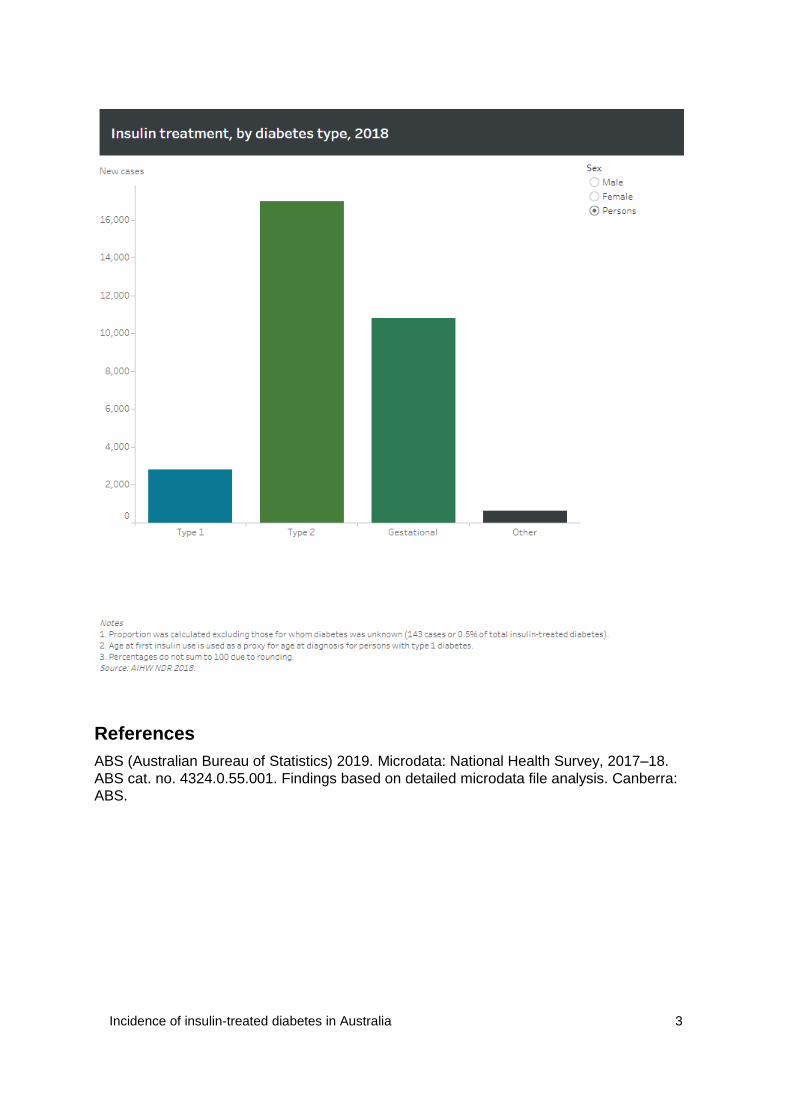
In 2018, about 31,300 people registered on the NDR began using insulin to treat their
diabetes. Of these:
just over 2,800 (9.0%) people were diagnosed with type 1 diabetes, and began using
insulin to treat it
17,000 (54%) people began using insulin to treat type 2 diabetes
10,800 (34%) females began using insulin to treat gestational diabetes
about 600 (2.0%) people began using insulin to treat other forms of diabetes.
Proportions were calculated excluding those for whom diabetes type was unknown (143
cases or 0.5% of total insulin-treated diabetes).
Due to rounding, percentages do not sum to 100.
Incidence of insulin-treated diabetes in Australia 3
References
ABS (Australian Bureau of Statistics) 2019. Microdata: National Health Survey, 2017–18.
ABS cat. no. 4324.0.55.001. Findings based on detailed microdata file analysis. Canberra:
ABS.
Incidence of insulin-treated diabetes in Australia 4
Type 1 diabetes incidence Type 1 diabetes is a lifelong autoimmune disease that often has onset in childhood or early
adulthood, but can occur at any age. The cause is unknown, but it is believed to be an
interaction of genetic and environmental factors. All people with type 1 diabetes need insulin
to manage their condition.
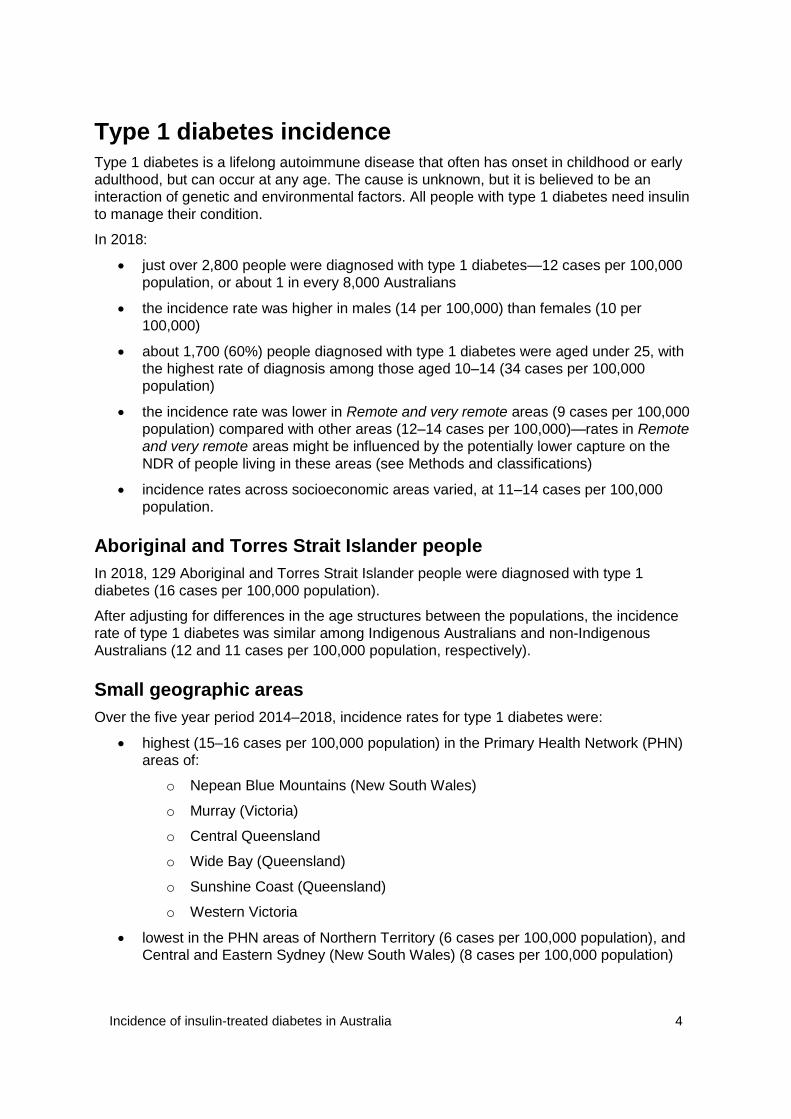
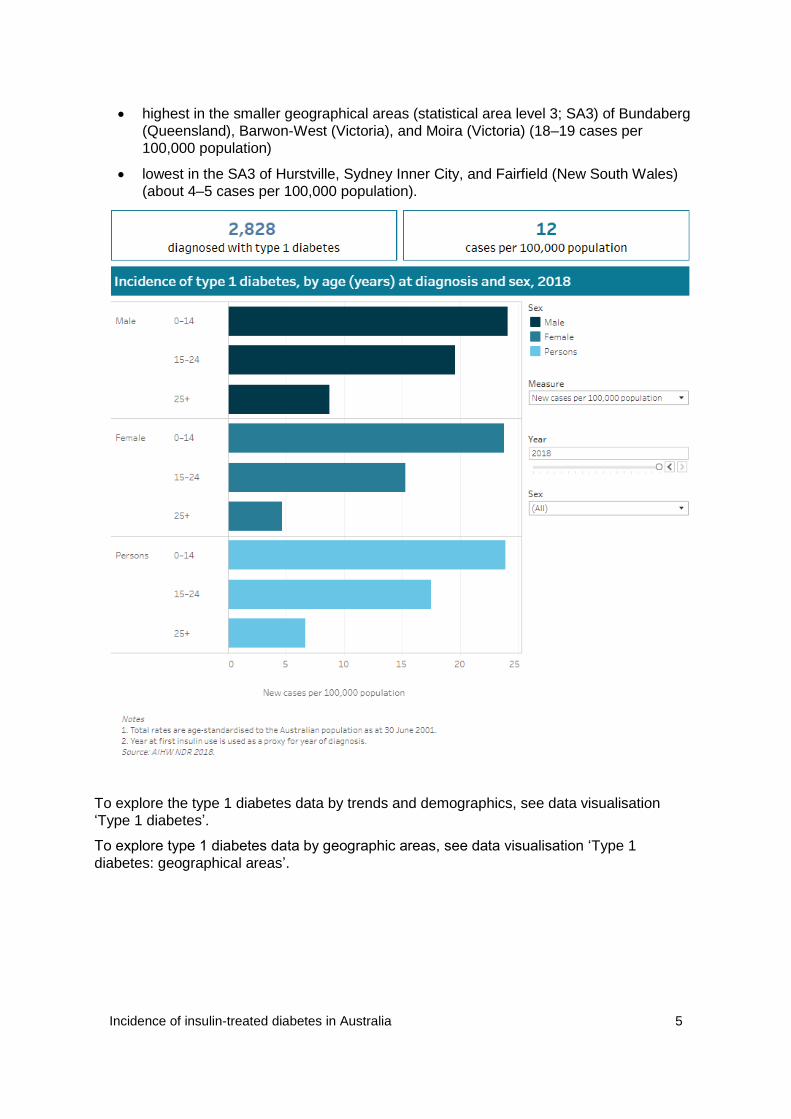
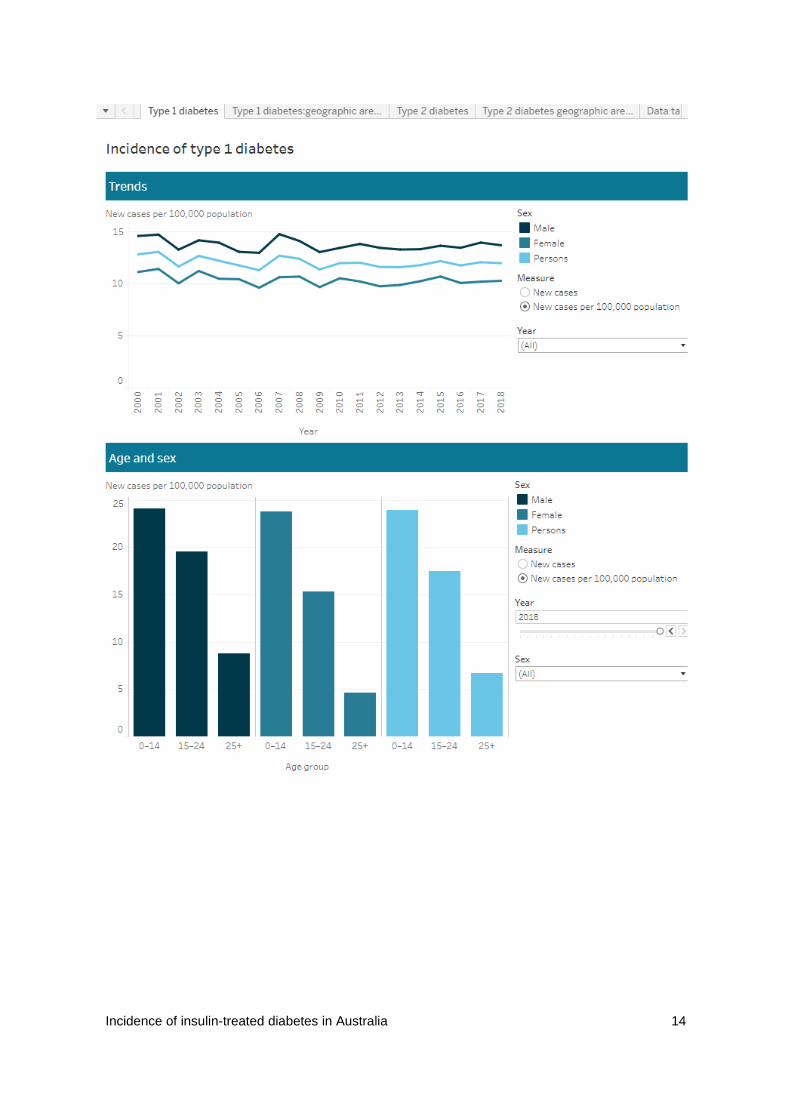
In 2018:
just over 2,800 people were diagnosed with type 1 diabetes—12 cases per 100,000
population, or about 1 in every 8,000 Australians
the incidence rate was higher in males (14 per 100,000) than females (10 per
100,000)
about 1,700 (60%) people diagnosed with type 1 diabetes were aged under 25, with
the highest rate of diagnosis among those aged 10–14 (34 cases per 100,000
population)
the incidence rate was lower in Remote and very remote areas (9 cases per 100,000
population) compared with other areas (12–14 cases per 100,000)—rates in Remote
and very remote areas might be influenced by the potentially lower capture on the
NDR of people living in these areas (see Methods and classifications)
incidence rates across socioeconomic areas varied, at 11–14 cases per 100,000
population.
Aboriginal and Torres Strait Islander people
In 2018, 129 Aboriginal and Torres Strait Islander people were diagnosed with type 1
diabetes (16 cases per 100,000 population).
After adjusting for differences in the age structures between the populations, the incidence
rate of type 1 diabetes was similar among Indigenous Australians and non-Indigenous
Australians (12 and 11 cases per 100,000 population, respectively).
Small geographic areas
Over the five year period 2014–2018, incidence rates for type 1 diabetes were:
highest (15–16 cases per 100,000 population) in the Primary Health Network (PHN)
areas of:
o Nepean Blue Mountains (New South Wales)
o Murray (Victoria)
o Central Queensland
o Wide Bay (Queensland)
o Sunshine Coast (Queensland)
o Western Victoria
lowest in the PHN areas of Northern Territory (6 cases per 100,000 population), and
Central and Eastern Sydney (New South Wales) (8 cases per 100,000 population)
Incidence of insulin-treated diabetes in Australia 5
highest in the smaller geographical areas (statistical area level 3; SA3) of Bundaberg
(Queensland), Barwon-West (Victoria), and Moira (Victoria) (18–19 cases per
100,000 population)
lowest in the SA3 of Hurstville, Sydney Inner City, and Fairfield (New South Wales)
(about 4–5 cases per 100,000 population).
To explore the type 1 diabetes data by trends and demographics, see data visualisation
‘Type 1 diabetes’.
To explore type 1 diabetes data by geographic areas, see data visualisation ‘Type 1
diabetes: geographical areas’.
Incidence of insulin-treated diabetes in Australia 6
Insulin-treated type 2 diabetes incidence Type 2 diabetes is a progressive condition that occurs when the body becomes resistant to
insulin, or insulin production is inadequate. The cause is unknown, but it is believed to be an
interaction of genetic and environmental factors.
Type 2 diabetes tends to develop over a long period of time, and generally has onset later in
life. When blood glucose levels can no longer be maintained at optimum levels through diet,
exercise and other medications, insulin replacement might be required. Some people newly
diagnosed with type 2 diabetes need insulin replacement from diagnosis.
Change in method for insulin-treated type 2 diabetes
The method used to calculate the incidence rates of insulin-treated type 2 diabetes has changed in recent years.
In reports before 2019, incidence rates of insulin-treated type 2 diabetes were calculated based on the Australian Bureau of Statistics (ABS) estimated resident population.
For this web update, incidence rates were calculated based on the population including all people with type 2 diabetes who have never used insulin, and are registered with the National Diabetes Services Scheme.
This change means that results presented in this report and cannot be compared with earlier publications or results based on earlier NDR data.
As the NDR potentially underestimates the number of Aboriginal and Torre Strait Islander registrants with diabetes, the incidence of insulin-treated type 2 diabetes based on the prevalent type 2 diabetes population by Indigenous status has not been reported. This is an important data gap for future development. For more information, see the Methods and classifications.
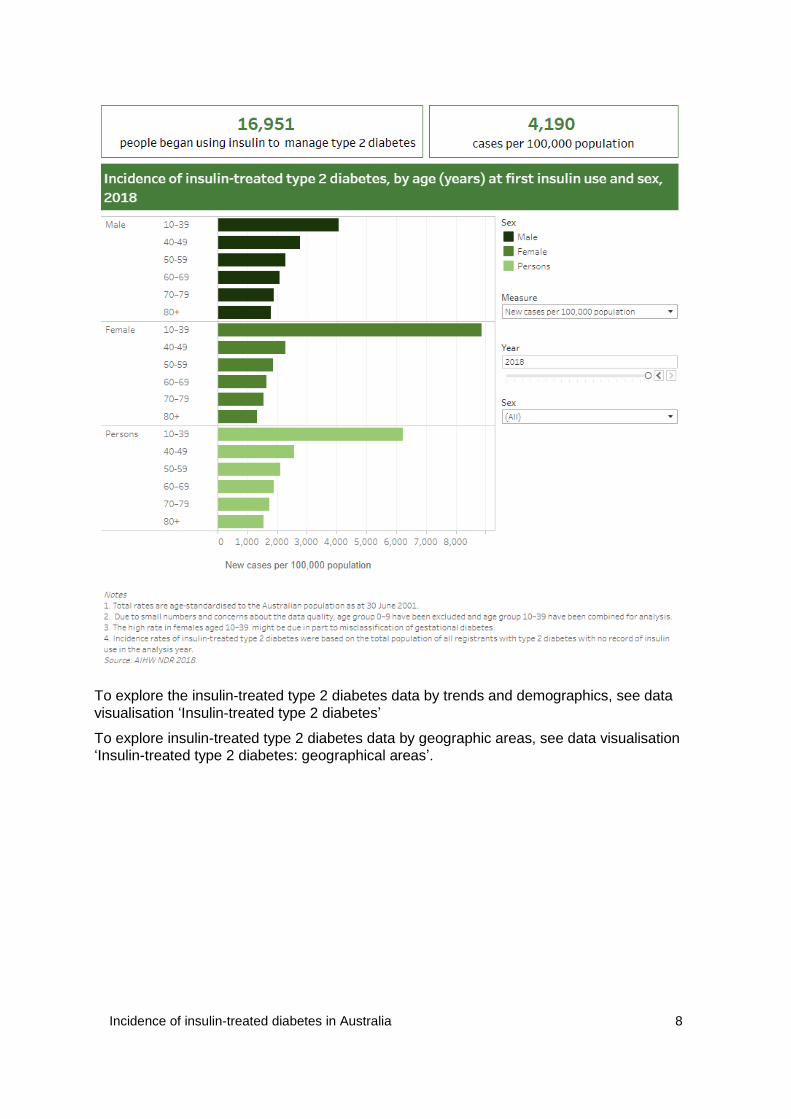
In 2018:
about 17,000 people began using insulin to manage their type 2 diabetes—4,200
cases per 100,000, or about 1 in every 24 registrants with type 2 diabetes not
previously using insulin
the incidence rate was 1.7 times higher in females (5,400 per 100,000) than in males
(3,200 per 100,000)
incidence rates for insulin-treated type 2 diabetes were twice as high among those
living in Major cities (4,300 cases per 100,000 registrants with type 2 diabetes not
previously using insulin) as those in the Remote and very remote areas (2,000 cases
per 100,000)—rates in Remote and very remote areas might be influenced by the
potentially lower capture on the NDR of people living in these areas (see Methods
and classifications)
incidence rates across socioeconomic areas varied, at 4,000–4,500 per 100,000 type
2 diabetes registrants
Incidence of insulin-treated diabetes in Australia 7
Small geographic areas
– Over the five year period 2014–2018, incidence rates for insulin-treated type 2
diabetes were:
highest (5,400–6,000 per 100,000 NDR registrants with type 2 diabetes not
previously using insulin) in the Primary Health Network (PHN) areas of:
o Western Queensland (Queensland)
o Hunter New England (New South Wales)
o Central Coast (New South Wales)
o Darling Downs (Queensland)
o West Moreton (Queensland)
o Tasmania
lowest incidence in the PHN areas of Northern Territory (2,100 cases per 100,000
NDR registrants with type 2 diabetes not previously using insulin), Country Western
Australia (3,700), and Perth North (Western Australia) (3,900).
highest in the smaller geographical areas (statistical area level 3; SA3) of Botany
(New South Wales) (8,100 cases per 100,000 NDR registrants with type 2 diabetes
not previously using insulin), Port Stephens (New South Wales) (8,400) and Huon–
Bruny Island (Tasmania) (9,600)
lowest in the Northern Territory SA3 of Daly-Tiwi West Arnhem (965 cases per
100,000 NDR registrants with type 2 diabetes not previously using insulin) and
Katherine (412).
The coverage of the National Diabetes Services Scheme may be lower in SA3 areas with
remote communities or communities with large Aboriginal and Torres Strait Islander
populations. This might influence estimates on the number of people with insulin-treated
diabetes in these areas on the NDR. For more information, see Methods and classifications.
Incidence of insulin-treated diabetes in Australia 8
To explore the insulin-treated type 2 diabetes data by trends and demographics, see data
visualisation ‘Insulin-treated type 2 diabetes’
To explore insulin-treated type 2 diabetes data by geographic areas, see data visualisation
‘Insulin-treated type 2 diabetes: geographical areas’.
Incidence of insulin-treated diabetes in Australia 9
Time to first insulin use The majority of type 2 diabetes cases can be initially managed through a combination of diet,
exercise, and medication (RACGP 2016).
However, some people newly diagnosed with type 2 diabetes need insulin replacement from
diagnosis. While insulin treatment in a newly diagnosed patient is less common, it might be
used in patients with type 2 diabetes in hyperglycaemic emergencies.
When blood glucose levels can no longer be maintained at optimum levels through diet,
exercise, and other medications, insulin replacement might be required (RACGP 2016).
Eventually, many people with type 2 diabetes will need insulin as well as other treatments.
Between 2012 and 2018, the median time to first insulin use for people with insulin-treated
type 2 diabetes remained relatively unchanged, at about 7–8 years after diagnosis.
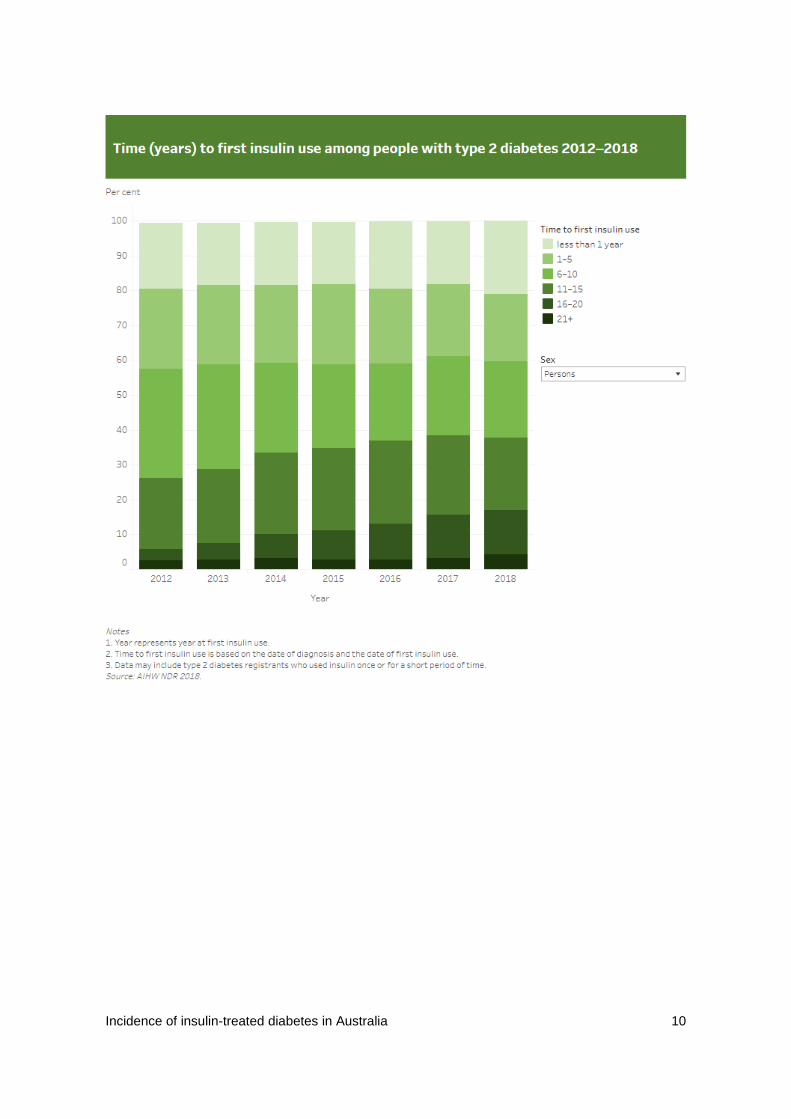
The proportion of people with insulin-treated type 2 diabetes, who began using insulin
immediately (that is, less than a year) after diagnosis remained relatively unchanged
between 2012 and 2017 at around 18–19%, with a slight rise to 21% in 2018.
Between 2012 and 2018, the proportion of people with insulin-treated type 2 diabetes who
began using insulin:
decreased from 23% to 19% for those who started insulin 1–5 years after diagnosis
decreased from 31% to 22% for those who started insulin 6–10 years after diagnosis
peaked in 2016 at 24% for those who started using insulin 11–15 years after
diagnosis, before falling to 21% in 2018
increased from 3% to 13% for those who started insulin 16–20 years after diagnosis
remained similar at about 3%–4% for those who started insulin 21 years or more after
diagnosis.
Data should be interpreted with caution. Many factors influence the timing of insulin initiation.
They include the benefits of early effective glycaemic control, the number of non-insulin
treatments available, glycaemic target used for individual patients, and the availability of
insulin supplies and monitoring equipment (RACGP 2015).
Data presented for time to first insulin use might include people who are prescribed insulin
treatment only once or for a short period of time, who might no longer be using insulin.
Incidence of insulin-treated diabetes in Australia 10
Incidence of insulin-treated diabetes in Australia 11
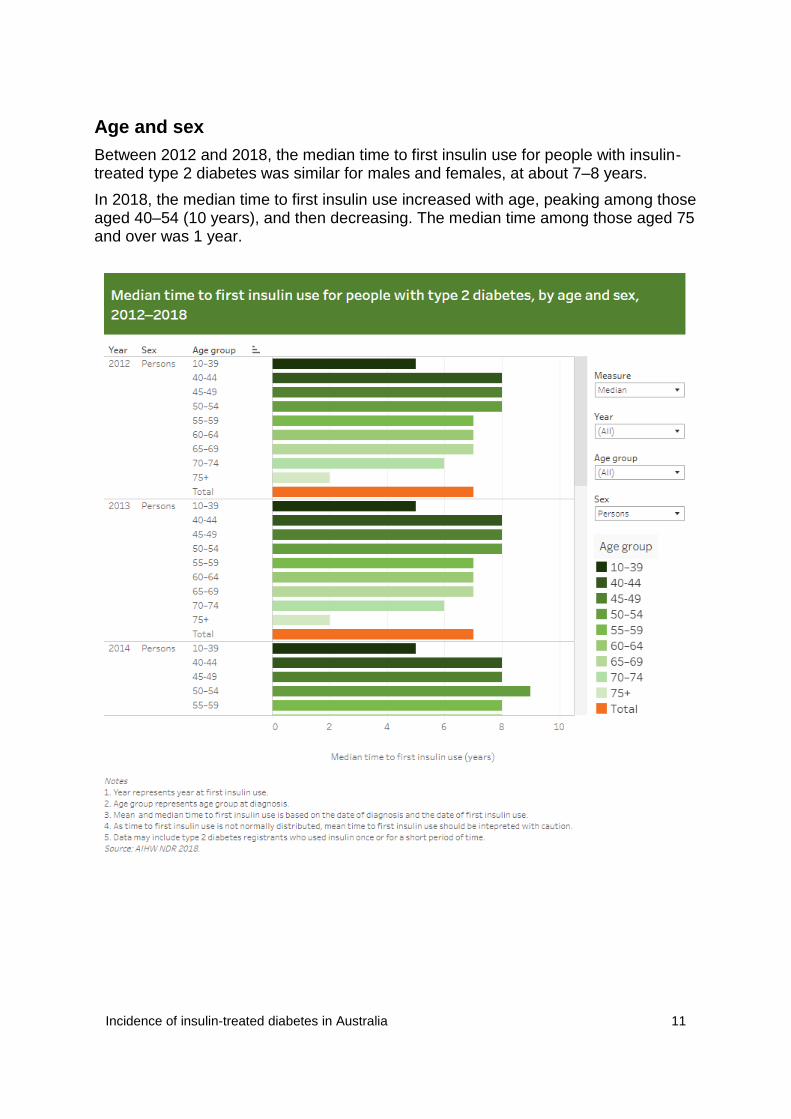
Age and sex
Between 2012 and 2018, the median time to first insulin use for people with insulin-treated type 2 diabetes was similar for males and females, at about 7–8 years.
In 2018, the median time to first insulin use increased with age, peaking among those aged 40–54 (10 years), and then decreasing. The median time among those aged 75 and over was 1 year.
Incidence of insulin-treated diabetes in Australia 12
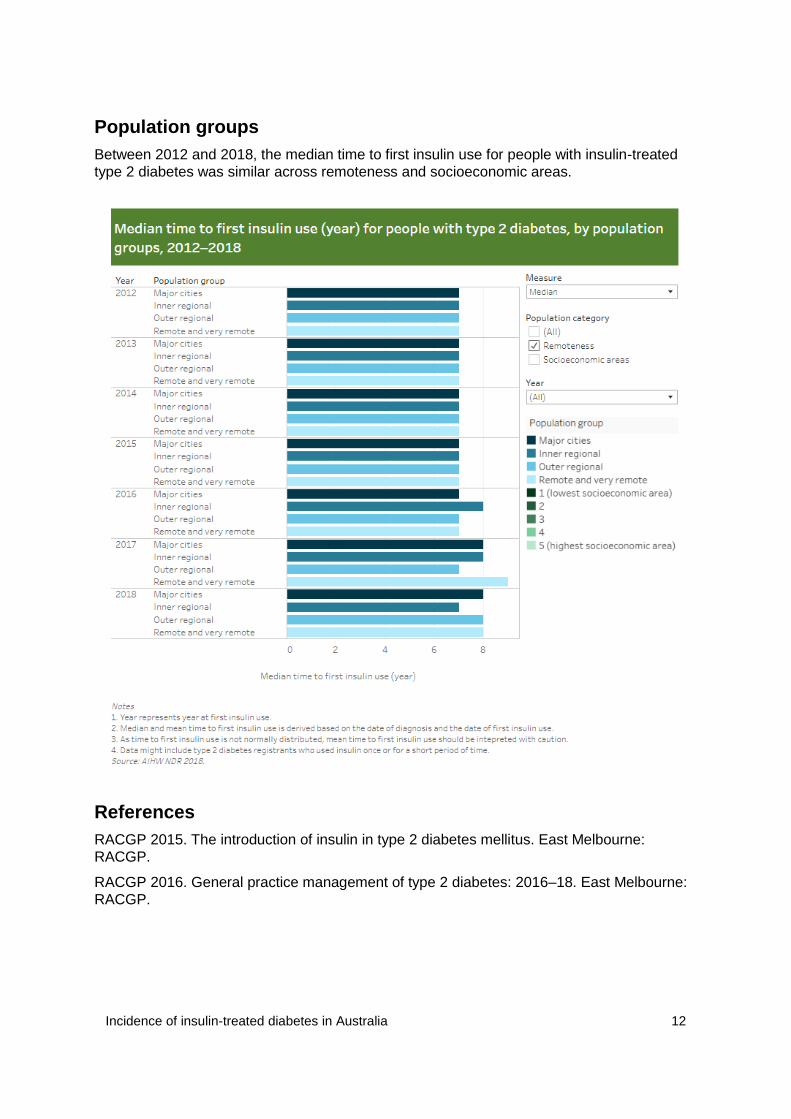
Population groups
Between 2012 and 2018, the median time to first insulin use for people with insulin-treated
type 2 diabetes was similar across remoteness and socioeconomic areas.
References
RACGP 2015. The introduction of insulin in type 2 diabetes mellitus. East Melbourne:
RACGP.
RACGP 2016. General practice management of type 2 diabetes: 2016–18. East Melbourne:
RACGP.
Incidence of insulin-treated diabetes in Australia 13
Incidence of insulin-treated diabetes data
visualisation In this visualisation, you can explore the data for type 1 diabetes and insulin-treated type 2
diabetes by:
trends (calendar years)
age at first insulin use
population groups (Indigenous status, remoteness area, and socioeconomic area)
geographic areas (state and territory, Primary Health Network, and statistical area
level 3).
Incidence of insulin-treated diabetes in Australia 14

Incidence of insulin-treated diabetes in Australia 15
Incidence of insulin-treated diabetes in Australia 16
Data sources
National (insulin-treated) Diabetes Register
The National (insulin-treated) Diabetes Register (NDR) collects information about people
who began using insulin as part of their treatment for diabetes since 1999.
The register includes most people diagnosed with type 1 diabetes since this time, as well as
those with type 2 diabetes, gestational diabetes, and other less common forms of diabetes
who use insulin to manage their condition.
The Australian Institute of Health and Welfare (AIHW) maintains the NDR, which is derived
from 2 primary data sources:
The National Diabetes Services Scheme (NDSS)
Established in 1987, the NDSS is an initiative of the Australian Government,
administered with the assistance of Diabetes Australia. People with a diagnosis of
diabetes by a health professional can register with the scheme. Once registered, they
can access diabetes self-management information, services, and subsidised
products—such as pens and needles to administer insulin, blood glucose test strips,
insulin pump consumables, and continuous glucose monitoring products.
Australasian Paediatric Endocrine Group (APEG) state-based registers
The APEG is a professional body that represents health professionals involved in
managing and researching disorders of the endocrine system, including diabetes in
children and adolescents. The APEG maintains clinic-based state and territory
diabetes registers of children.
The capture of insulin-treated diabetes on the NDR depends on the coverage of these 2
primary data sources.
For more information see the NDR data quality statement.
Incidence of insulin-treated diabetes in Australia 17
Methods and classifications
Comparison with previous reports
The methods to create the National (insulin-treated) Diabetes Register (NDR) have changed
in recent years. These include:
the way data are processed
how eligibility for the NDR is determined
changes to the method used to calculate the incidence of insulin-treated type 2
diabetes.
The derivation of the register applied these new methods retrospectively across all years.
Because of these changes, results presented in this report and based on the NDR 2018
cannot be compared with earlier publications, or with results based on earlier NDR data.
Diabetes type on the NDR
A health practitioner classifies diabetes type at the time of NDSS registration. But
misclassification can occur, as the symptoms of type 1 and type 2 diabetes can be similar,
particularly in young adults.
Further, changes in the classification of diabetes type in the NDSS data in 2002–2003 might
have resulted in people with insulin-treated type 2 diabetes being misclassified as having
type 1 diabetes.
So, as part of processing information from the primary data sources to create the NDR, the
reported diabetes type is checked against a set of criteria, and revised where necessary.
This algorithm (a method of calculation) assesses and reclassifies diabetes type for some
registrants on the NDSS. The reclassified diabetes type has been used to calculate
estimates by diabetes type for the NDR 2018.
The algorithm is based on age at diagnosis and the period between diagnosis and first
insulin use, because of the correlation with diabetes type. The algorithm has been
periodically updated in consultation with the AIHW Diabetes Expert Advisory Group. But with
or without the algorithm, there will always be some level of misclassification.
More information on the algorithm is available on request.
Incidence
Incidence is the number of new cases (of an illness or event) occurring in a population during
a given period. Incidence can be described as either a whole number or rate relative to the
total number of people at risk.
Incidence should not be confused with prevalence, which refers to the total number or
proportion of cases (of an illness or event) in a population at a given point in time.
In this report incidence of insulin-treated diabetes is described over the calendar year—that
is, the number of new cases from 1 January to 31 December in the year being reported.
Incidence of insulin-treated diabetes in Australia 18
Incidence rates
Throughout this report, incidence rates are calculated and presented based on the number of
cases per 100,000 population.
For example, the incidence rate of:
type 1 diabetes among males is calculated as a rate per 100,000 males in the
Australian population
insulin use among people with type 2 diabetes is calculated as a rate per 100,000
NDR registrants with type 2 diabetes not previously using insulin.
The denominator population used to calculate the incidence rates for insulin-treated type 2
diabetes has changed in recent years. As a result, the incidence rates presented in this web
report cannot be compared with earlier publications or results based on earlier NDR data.
For more information see Type 2 diabetes population.
Estimated resident populations
Population data were used to derive incidence rates of type 1 diabetes. Population data are
sourced from the Australian Bureau of Statistics (ABS), and updated when revised or new
estimates become available.
All population estimates that the ABS currently produces are based on area of usual
residence. These estimated resident populations are derived from the ABS Census of
Population and Housing, and adjusted for deaths, births and net migration.
The estimated resident populations used in this report are based on the population estimates
for 30 June 2018.
The Aboriginal and Torres Strait Islander population is calculated from the Census. Because
of the smaller Indigenous population, it is difficult to measure population changes accurately
between Census years using the same methods as for the Australian population. As a result,
the ABS has developed experimental estimates and projections based on the 2016 Census.
All calculations of rates for Aboriginal and Torres Strait Islander people use:
the estimated resident populations derived from the 2016 Census for 2005–2016
the Series B projected Indigenous populations for 2017 and 2018.
Type 2 diabetes population
All registrants with type 2 diabetes with no record of insulin use were used as the
denominator population to derive the incidence rates of insulin-treated type 2 diabetes.
The NDR derived data from the NDSS and APEG was used to identify the population with
diagnosed type 2 diabetes. As most people with type 2 diabetes registered with APEG are
also registered with the NDSS, the combined NDSS and APEG data are referred to in the
web report as NDSS data.
The population data included all people with type 2 diabetes who were diagnosed between
2000 and 2018 and were still alive on 31 December of each year of analysis.
The coverage of the Australian population with type 2 diabetes registered with the NDSS is
unknown, as not all people with type 2 diabetes need insulin treatment or register with the
NDSS. The NDSS might underestimate people with type 2 diabetes who manage their
diabetes primarily through diet, exercise, and medication.
Incidence of insulin-treated diabetes in Australia 19
The population for each year of the analysis was derived based on the diagnosis date of the
registrants recorded on the NDSS and APEG. Although NDSS data are available from 1987,
many people who registered with the NDSS in the early years of operation have a missing
diagnosis date. Where diagnosis date was missing, registration date was used as a proxy to
derive the population.
Due to concerns with the Aboriginal and Torres Strait Islander population derived from the
NDSS, incidence data for insulin-treated type 2 diabetes by Indigenous status have been
excluded from this report.
The NDSS might underestimate the number of Indigenous registrants because:
identifying as being Aboriginal or Torres Strait Islander is voluntary
people might access diabetes-related products through other programs
the coding of Indigenous status on the NDSS has changed.
For more information, see Indigenous status.
Age-specific rates
Age-specific rates provide information on incidence in an age group relative to the total
number of people at risk in the same age group.
All age-specific rates in this report are presented as new cases per 100,000 population.
Rates were not reported if the number of new cases of insulin-treated diabetes was less than
5.
Age-standardised rates
Age-standardisation is a method used to eliminate the effect of differences in population age
structures when comparing populations with different age structures, and where age affects
the variable being compared.
All incidence rates presented in this report are age-standardised to the 2001 Australian
population, and presented as age-standardised new cases per 100,000 population.
Age-standardised rates were not reported if the number of new cases of insulin-treated
diabetes was less than 20. Age groups were combined where there were less than 30 cases
in any age group to calculate age-standardised rates.
Time to first insulin use
Time to first insulin use is reported for 2012–2018. It was derived from the date of diagnosis
and date of first insulin use recorded on the NDR for people with insulin-treated type 2
diabetes.
Many registrants in the early years of operation of the NDSS have a missing date of
diagnosis. This affects the derivation of the time to first insulin use for people with insulin-
treated type 2 diabetes, as they might have been diagnosed long before starting insulin
treatment and registering with the NDSS.
Looking at missing data for diagnosis date from 2000–2018 showed that the percentage with
a missing date of diagnosis fell from 27% to 10%, stabilising at about 10%–13% in 2012–
2018. So, the analysis for time to first insulin use was restricted to 2012–2018.
Incidence of insulin-treated diabetes in Australia 20
Geography
Statistical area level 3
Data presented for smaller geographical areas are based on the area of usual residence,
using the statistical area level 3 (SA3) units defined in the Australian Statistical Geographical
Standard (ASGS) 2016. SA3 are geographical areas built from whole statistical areas level 2
(SA2).
In general, the SA3s are designed to have populations of 30,000–130,000. There are 358
spatial SA3 regions covering the whole of Australia without gaps or overlaps. SA3
correspondence files are sourced from the ABS.
Due to the small number of new cases of insulin-treated diabetes in some SA3s, incidence
rates have been calculated for a combined 5-year reference period (2014–2018).
Data for a SA3 were not reported if the number of new cases of insulin-treated diabetes was
less than 5 for an area.
Incidence rates were not reported if the number of new cases of insulin-treated diabetes was
less than 20 in the reference period; this affected 18% of SA3s for type 1 diabetes, and 1.8%
of SA3s for insulin-treated type 2 diabetes.
Primary Health Network
Primary Health Network (PHN) organisations connect health services across a specific
geographic area (a PHN area). The Australian Government Department of Health defines
the boundaries.
There are 31 PHN areas that cover the whole of Australia. PHNs replaced the previous 61
Medicare Locals on 1 July 2015. The boundaries align with Local Hospital Network (LHN)
boundaries (or equivalent), and take into account population size, LHN alignment, state and
territory borders, patient flow, stakeholder input and administrative efficiencies. Not all PHNs
directly align with the ABS ASGS structure.
Statistical area level 2 (SA2) data was combined up to the PHN area levels, using
concordance files sourced from ABS for the analysis of type 1 diabetes.
PHN correspondence files are sourced from the ABS for the analysis of insulin-treated type 2
diabetes. For this update, statistical information is presented using the 2017 boundaries of
the 31 PHNs.
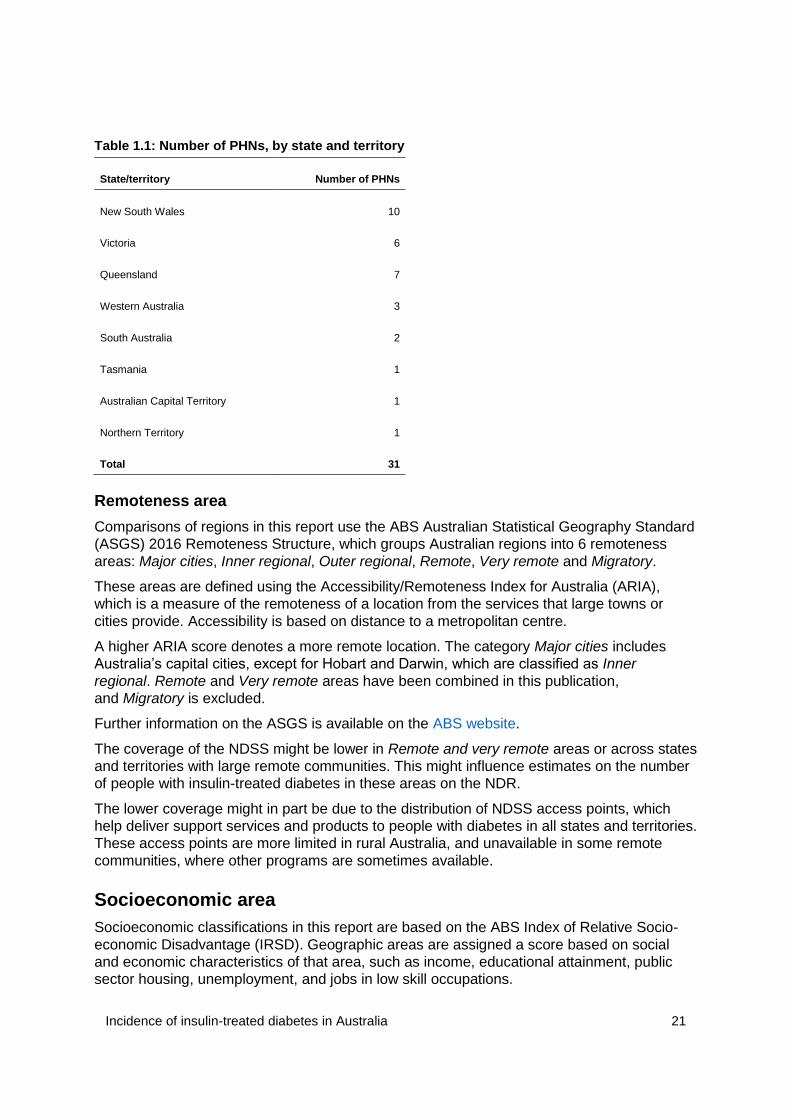
Table 1.1 shows the number of PHNs by state and territory. Three jurisdictions (Tasmania,
the Northern Territory, and the Australian Capital Territory) are single PHNs. Their size,
particularly in jurisdictions with large Indigenous populations (such as the Northern Territory
and Western Australia), might mask important inter-area variation.
Incidence rates for PHNs with less than 20 new cases of insulin-treated diabetes in the
reference period were not reported. In 2018, this affected the Northern Territory and Western
Queensland PHNs.
Incidence of insulin-treated diabetes in Australia 21
Table 1.1: Number of PHNs, by state and territory
State/territory Number of PHNs
New South Wales 10
Victoria 6
Queensland 7
Western Australia 3
South Australia 2
Tasmania 1
Australian Capital Territory 1
Northern Territory 1
Total 31
Remoteness area
Comparisons of regions in this report use the ABS Australian Statistical Geography Standard
(ASGS) 2016 Remoteness Structure, which groups Australian regions into 6 remoteness
areas: Major cities, Inner regional, Outer regional, Remote, Very remote and Migratory.
These areas are defined using the Accessibility/Remoteness Index for Australia (ARIA),
which is a measure of the remoteness of a location from the services that large towns or
cities provide. Accessibility is based on distance to a metropolitan centre.
A higher ARIA score denotes a more remote location. The category Major cities includes
Australia’s capital cities, except for Hobart and Darwin, which are classified as Inner
regional. Remote and Very remote areas have been combined in this publication,
and Migratory is excluded.
Further information on the ASGS is available on the ABS website.
The coverage of the NDSS might be lower in Remote and very remote areas or across states
and territories with large remote communities. This might influence estimates on the number
of people with insulin-treated diabetes in these areas on the NDR.
The lower coverage might in part be due to the distribution of NDSS access points, which
help deliver support services and products to people with diabetes in all states and territories.
These access points are more limited in rural Australia, and unavailable in some remote
communities, where other programs are sometimes available.
Socioeconomic area
Socioeconomic classifications in this report are based on the ABS Index of Relative Socio-
economic Disadvantage (IRSD). Geographic areas are assigned a score based on social
and economic characteristics of that area, such as income, educational attainment, public
sector housing, unemployment, and jobs in low skill occupations.
Incidence of insulin-treated diabetes in Australia 22
A low score means an area has, on average, more low-income families, people with less
training, and higher unemployment, and might be considered disadvantaged relative to other
areas with higher scores.
High scores reflect a relative lack of disadvantage, rather than advantage, and the IRSD
relates to the average disadvantage of all people living in a geographical area. It cannot be
presumed to apply to all individuals living in the area.
For this report, the population is divided into 5 socioeconomic groups, with roughly equal
populations (each about 20% of the total), based on the level of disadvantage of the
statistical local area of their usual residence.
The first group includes the 20% of the population living in areas with the highest levels of
relative disadvantage (referred to as Group 1, lowest).
The last group includes the 20% of the population living in areas with the lowest levels of
relative disadvantage (referred to as Group 5, highest).
The IRSD values used in this report are based on the 2016 Census. Further information is
available on the ABS website.
Indigenous status
The NDR might underestimate the number of Aboriginal and Torres Strait Islander registrants
with insulin-treated diabetes. Reasons are as follows:
Indigenous status can only be reported for people who registered on the NDSS after
2005, due to changes in the way this variable is coded. Before 2005, data entry of
Indigenous status coded all ‘unknown’ or ‘not stated’ responses to the Indigenous
status question as ‘non-Indigenous’. In 2005, an extra value was added to indicate
‘inadequate/not stated’ where Indigenous status was not known. As a result,
Indigenous status cannot be determined for 98% of people registered on the NDSS
before 2005.
Identifying as being of Indigenous origin on both data sources of the NDR (NDSS and
APEG) is voluntary.
Other programs that give Indigenous Australians access to diabetes-related products
might result in lower registration rates for the NDSS, and subsequently the NDR,
among Aboriginal and Torres Strait Islander people. For example, programs such as
Aboriginal Medical Services and the National Aboriginal Community Controlled Health
Organisation—provide Indigenous Australians access to free and subsidised products
that people with insulin-treated diabetes need. In addition, NDSS access points are
not always available in remote areas.
These factors might lead to an underestimation of the incidence of type 1 diabetes among
Aboriginal and Torres Strait Islander people.
As a result of the classification changes in 2005 on the NDSS, it is not possible to derive the
prevalent type 2 diabetes population for Aboriginal and Torres Strait Islander people. So the
rates of insulin use among Indigenous type 2 diabetes have not been reported. The reporting
of insulin-treated type 2 diabetes in Aboriginal and Torres Strait Islander people is an
important data gap that requires future data development work.