Embed Size (px)
Citation preview

Arq Neuropsiquiatr 2008;66(2-B):385-390
385
ImmunohIstochemIcal expressIon of markers ki-67, neun, synaptophysIn, p53 and her2 In medulloblastoma and Its correlatIon wIth clInIcopathologIcal parameters
Rosalva Thereza Meurer1, Daniele Tondolo Martins2, Arlete Hilbig3, Marlise de Castro Ribeiro4, Adriana Vial Roehe5, Ligia Maria Barbosa-Coutinho6, Marilda da Cruz Fernandes7
Abstract – Medulloblastoma (MB) is the most common malignant brain tumor in childhood. The alterations found include: presence of oncoproteins p53 and HER2, elevated mitotic index, and presence of neuronal differentiation. The aim of this study was to determine the immunohistochemical expression of markers Ki-67, NeuN, synaptophysin, HER2 and p53 in 40 MB samples and their correlation with clinicopathologic parameters and survival. In 29 patients (72.5%), ≥20% of cells were positive for Ki-67. Males showed greater ki-67 expression (p=0.02) and smaller survival rates (p=0.002). NeuN and synaptophysin were negative in 16 (40%) and 8 (20%) cases, respectively. P53 was positive in 18 (45%) cases, with 11 (61%) weakly positive and 7 (39%) strongly positive. HER2 was positive in 23 (57.5%) of the samples and did not show statistical association with survival (p=0.07).
KEy woRds: medulloblastoma, immunohistochemistry, Ki-67, NeuN, synaptophysin, HER2, p53, survival analysis.
expressão imunoistoquímica dos marcadores ki-67, neun, sinaptofisina, p53 e her2 em meduloblastoma e sua correlação com os parâmetros clínico-patológicos
Resumo – Meduloblastoma (MB) é o tumor maligno encefálico mais freqüente na infância. dentre as alterações encontradas estão: a presença das oncoproteínas p53 e HER2, elevado índice mitótico e presença de diferenciação neuronal. o objetivo deste estudo foi determinar a expressão imunoistoquímica (IMQ) dos marcadores Ki-67, NeuN, sinaptofisina, HER2 e p53 em 40 amostras de MB, correlacionando-as com parâmetros clinicopatológicos e com a sobrevida. Vinte e nove pacientes (72,5%) apresentaram 20% ou mais das células positivas para Ki-67. os pacientes do sexo masculino apresentaram maior expressão do Ki-67 (p=0,02) e também menor sobrevida (p=0,002). NeuN e sinaptofisina foram negativos em 16 (40%) e 8 (20%) casos, respectivamente. P53 foi positivo em 18 (45%) casos, sendo 11 (61%) fracamente positivos e 7 (39%) fortemente positivos. HER2 foi positivo em 23 (57,5%) das amostras e não demonstrou associação estatística com a sobrevida (p=0.07).
PAlAVRAs-cHAVE: meduloblastoma, imunoistoquímica, Ki-67, NeuN, sinaptofisina, HER2, p53, sobrevida.
1Postgraduate Program in Pathology, Fundação Faculdade Federal de ciências Médicas de Porto Alegre Rs, Brazil (FFFcMPA): 1Master student, Graduate Program in Pathology, FFFcMPA; 2Undergraduate Medical student of the FFFcMPA; 3Neurologist; M.d. and Phd: Medical clinic by UFRGs. Adjunct Pro-fessor of Human Anatomy, FFFcMPA; 4Neurologist, Md, Phd, substitute Professor of Neurology at FFFcMPA; 5Pathologist, Md, Phd, FFFcMPA, substitute Professor, department of Pathology, FAMEd - UFRGs; 6Professor Emeritus, Reader in Pathologic Anatomy, FFFcMPA, Neuropathologist, Full Professor of Pathologic Anatomy, FFFcMPA; 7Biologist, Master in Neuroanatomy by UFRGs, doctor in cellular and Tissue Biology by UsP, Adjunct Professor ofAdjunct Professor of Histology, FFFcMPA. Financial support provided by cAPEs, PRoAP and Fundação Faculdade Federal de ciências Médicas de Porto Alegre, Rs.
Received 21 November 2007, received in final form 14 April 2008. Accepted 29 April 2008.
Dra. Rosalva Thereza Meurer – Rua Sarmento Leite 245 - 90050-170 Porto Alegre RS - Brasil. E-mail: [email protected]
Medulloblastoma (MB) is the most common malignant brain tumor in children, accounting for about 20% of all primary tumors of the central nervous system (cNs), with a peak of incidence at 5-7 years-old. These tumors have an aggressive behavior and despite treatment, the 5-year survival rate is 60%1,2. For therapeutic and prognostic pur-
poses, patients are divided in groups of high and low risk, according to the staging proposed by chang et al. (1969)3, age at the time of diagnosis, and presence of residual tu-mor4,5. A more accurate assessment of risk in children with MB can be done using a combination of clinical, histo-pathologic, and molecular prognostic factors4,6,7.

Arq Neuropsiquiatr 2008;66(2-B)
386
Medulloblastoma: Immunohistochemical markersMeurer et al.
MBs are among the intracranial tumors with fastest cellular proliferation6. studies show that the Mitotic In-dex (MI) determined by Ki-67 (MIB-1) above 20% is corre-lated with a worse prognosis8. NeuN and synaptophysin are commonly used as markers of neuronal differentia-tion in brain tumors, mainly in heterogeneous tumors such MBs9,10. HER2 is a proto-oncogene that has been largely studied and related with bad prognosis in cancer. In MB, investigations of HER2 expression have demonstrated a consistent association between the expression of this gene and a worse prognosis11-13 . TP53 gene mutations are one of the most frequent genetic alterations observed in tumors. Increased immunohistochemical expression of p53, particularly when staining is intense, has been associ-ated with a worse prognosis in MB14,15.
This study was designed to evaluate the immunohisto-chemical expression of Ki-67, NeuN, synaptophysin, HER2 and p53 in patients with MBs and to establish their corre-lation with clinicopathologic markers as histological sub-type, presence of residual tumor, gender, age, and over-all survival.
methodStudied sample
A retrospective study carried out using 40 samples of tu-
mor tissue collected from patients between 1 and 44 years of
age who had been submitted to total or partial resection of cer-
ebellar MB at hospitals santo Antônio of the complexo Hospi-
talar santa casa of Porto Alegre, and são lucas of PUcRs, with
anatomopathological diagnosis of MB from Jan 1996 to Jan 2005.
The anatomopathological records were reviewed and reassessed
by two researchers. The cases were classified into classic MB or
desmoplastic MB based on hematoxylin-eosin (HE) and reticulin
staining. The samples used in this study were obtained from the
first surgical procedure of the patients. Patient records were re-
viewed as for gender, age at the time of diagnosis, partial or to-
tal tumor resection, post-operative treatment, presence of me-
tastasis, recurrence, and death. Patients with incomplete data
regarding these variables were excluded from the study. Knowl-
edge of the death cases was obtained through the death certif-
icates provided by the responsible agency.
Immunohistochemical reactions
For the immunohistochemical studies we used tumor tissue
fixed in formalin and included in paraffin. The blocks were cut
into 3 mm thick sections, deparaffinized and rehydrated for the
performance of the technique. The streptoavidin-biotin-peroxi-
dase method (kit lsAB + Peroxidase dakocytomation®) was used
for detection of proteins Ki-67, synaptophysin, NeuN, HER2 and
p53. The antigenic recuperation was performed with sodium ci-
trate (pH 6.0) heated in double boiler (95-98ºc) for 30 min. En-
dogenous peroxidase activity was blocked using two baths of 10
min in hydrogen peroxide (H2o2) 30V, at 5%, in methanol. Un-
specific proteins were blocked using normal horse serum for 30
min. Incubation with primary antibodies (Table 1) was performed
overnight at 4ºc. Incubation with secondary antibody and tertia-
ry antibody was performed for 30 min at room temperature. As
negative control we used the same tissues, incubated with the
same antibodies except for the primary one, which was replaced
by normal horse serum. The antigen-antibody binding was visual-
ized with the dAB chromogen (diaminobenzidin). counterstain-
ing was with Harris hematoxylin; the slides were dehydrated and
mounted in synthetic resin.
The indexes of markers Ki-67 and p53 were calculated as
percentage of stained nuclei in 1,000 cells. The counting was
performed by 2 researchers under light microscopy. cells were
considered positive if their nucleus was stained brown. For p53
the positive samples were divided into 2 groups according to
the intensity of staining: weak or strong. For the evaluation of
NeuN and synaptophysin the following key was used: (+) 1-10%,
(++) 11-50%, (+++) >50% of tumor cells stained. As regards HER2,
positive samples were considered as those which showed reac-
tivity in either the membrane or the cytoplasm. If the counts
by the two researchers differed by over 20%, a third research-
er was summoned to do a new count and the mean of the three
counts was used.
Statistical analysis
comparisons between the groups were calculated by ANo-
VA parametric test, student’s t test and Fisher’s exact test. For
survival the Kaplan-Meier test was used. The magnitude of asso-
ciation among the variables death versus clinical aspects and im-
munohistochemical markers was measured by Hazard Ratio (HR),
Table 1. Immunohistochemistry in medulloblastomas.
Antibody (clone) dilution Manufacturer catalog No. Positive control
Ki-67 (MIB-1) 1/300 dakocytomation® M 7240 Palatine tonsil
NeuN (MAB77) 1/1000 chemicon® MAB377 Nervous tissue (brain)
synaptophysin sy38 1/200 dakocytomation® M0776 Adrenal gland
HER2 (cB11) 1/40 Novocastra® Ncl-l-cB11 Breast
P53 (do-7) 1/100 dakocytomation® M7001 Breast
Arq Neuropsiquiatr 2008;66(2-B)
387
Medulloblastoma: Immunohistochemical markersMeurer et al.
obtained by cox Regression model and 95% confidence intervals (cI). The level of significance used was α ≤ 0.05. The data were analyzed with the sPss 12.0 software package (chicago, Il, UsA).
Ethical aspects The project was approved by the Research Ethic committee
of the santa casa de Porto Alegre (protocol number 205/04).
resultsClinicopathologic findings The studied sample comprised 40 patients between 1
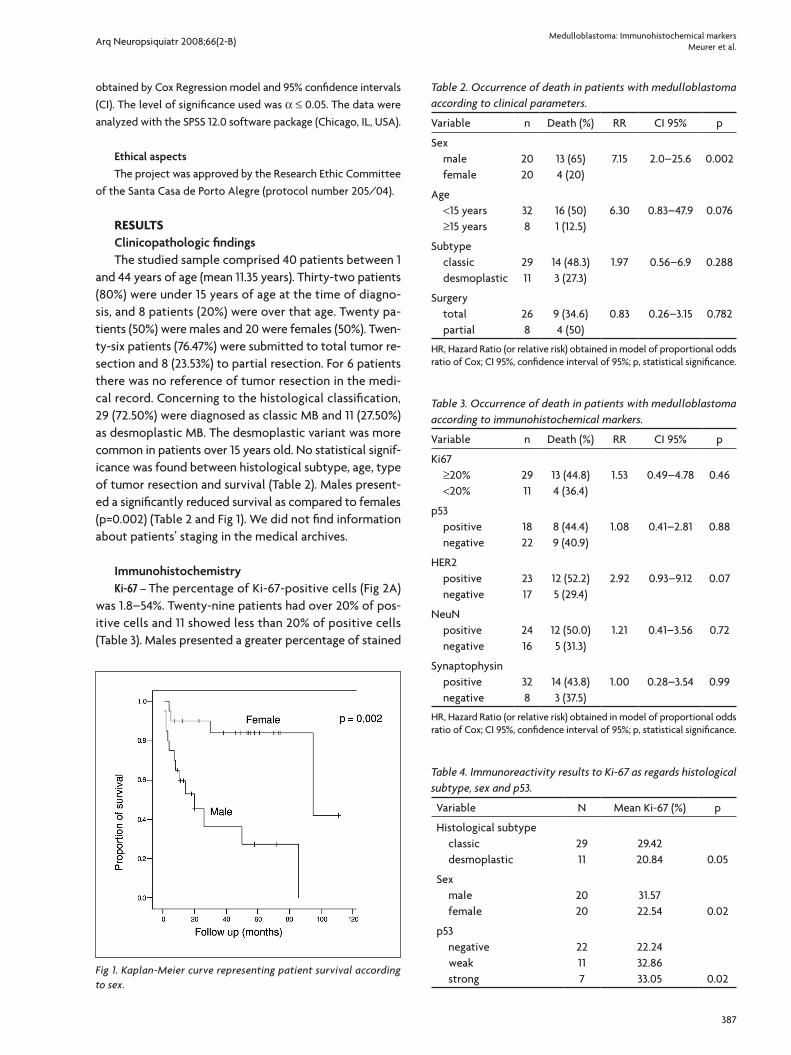
and 44 years of age (mean 11.35 years). Thirty-two patients (80%) were under 15 years of age at the time of diagno-sis, and 8 patients (20%) were over that age. Twenty pa-tients (50%) were males and 20 were females (50%). Twen-ty-six patients (76.47%) were submitted to total tumor re-section and 8 (23.53%) to partial resection. For 6 patients there was no reference of tumor resection in the medi-cal record. concerning to the histological classification, 29 (72.50%) were diagnosed as classic MB and 11 (27.50%) as desmoplastic MB. The desmoplastic variant was more common in patients over 15 years old. No statistical signif-icance was found between histological subtype, age, type of tumor resection and survival (Table 2). Males present-ed a significantly reduced survival as compared to females (p=0.002) (Table 2 and Fig 1). we did not find information about patients’ staging in the medical archives.
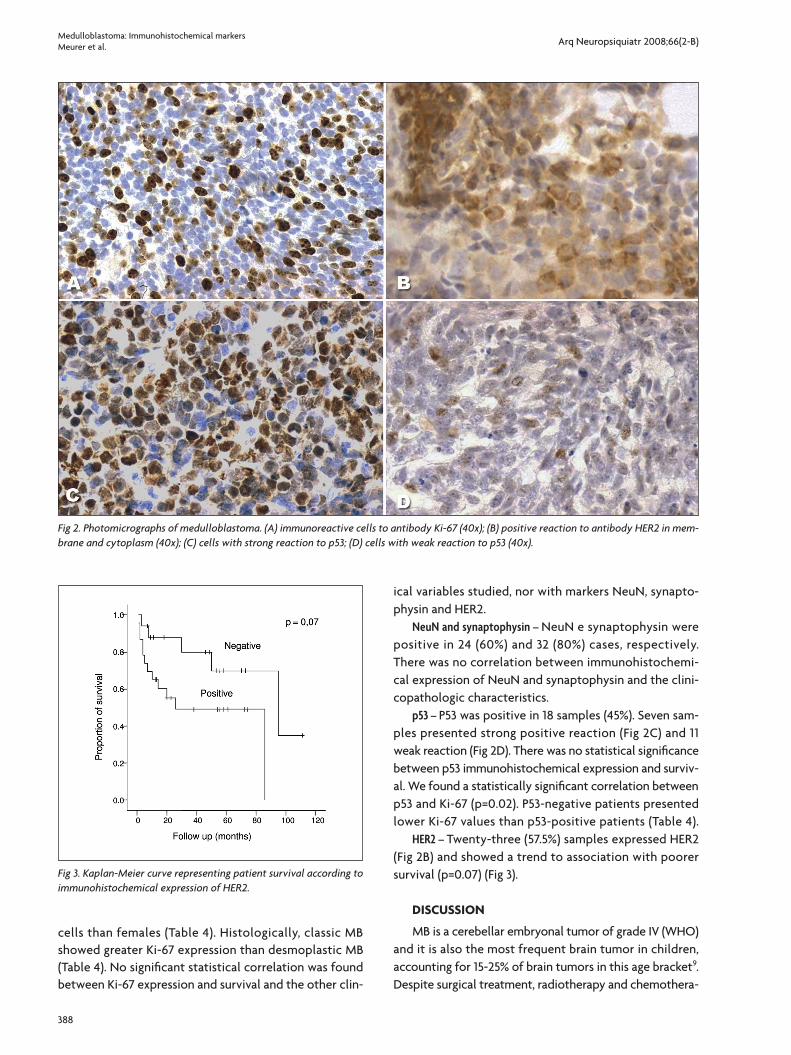
Immunohistochemistry Ki-67 – The percentage of Ki-67-positive cells (Fig 2A)
was 1.8–54%. Twenty-nine patients had over 20% of pos-itive cells and 11 showed less than 20% of positive cells (Table 3). Males presented a greater percentage of stained
Table 2. Occurrence of death in patients with medulloblastoma according to clinical parameters.
Variable n death (%) RR cI 95% p
sex male female
2020
13 (65)4 (20)
7.15 2.0–25.6 0.002
Age <15 years ≥15 years
328
16 (50)1 (12.5)
6.30 0.83–47.9 0.076
subtype classic desmoplastic
2911
14 (48.3)3 (27.3)
1.97 0.56–6.9 0.288
surgery total partial
268
9 (34.6)4 (50)
0.83 0.26–3.15 0.782
HR, Hazard Ratio (or relative risk) obtained in model of proportional odds ratio of cox; cI 95%, confidence interval of 95%; p, statistical significance.
Table 3. Occurrence of death in patients with medulloblastoma according to immunohistochemical markers.
Variable n death (%) RR cI 95% p
Ki67 ≥20% <20%
2911
13 (44.8)4 (36.4)
1.53 0.49–4.78 0.46
p53 positive negative
1822
8 (44.4)9 (40.9)
1.08 0.41–2.81 0.88
HER2 positive negative
2317
12 (52.2)5 (29.4)
2.92 0.93–9.12 0.07
NeuN positive negative
2416
12 (50.0)5 (31.3)
1.21 0.41–3.56 0.72
synaptophysin positive negative
328
14 (43.8)3 (37.5)
1.00 0.28–3.54 0.99
HR, Hazard Ratio (or relative risk) obtained in model of proportional odds ratio of cox; cI 95%, confidence interval of 95%; p, statistical significance.
Table 4. Immunoreactivity results to Ki-67 as regards histological subtype, sex and p53.
Variable N Mean Ki-67 (%) p
Histological subtype classic desmoplastic
2911
29.4220.84 0.05
sex male female
2020
31.5722.54 0.02
p53 negative weak strong
22117
22.2432.8633.05 0.02
Fig 1. Kaplan-Meier curve representing patient survival according to sex.
Arq Neuropsiquiatr 2008;66(2-B)
388
Medulloblastoma: Immunohistochemical markersMeurer et al.
cells than females (Table 4). Histologically, classic MB showed greater Ki-67 expression than desmoplastic MB (Table 4). No significant statistical correlation was found between Ki-67 expression and survival and the other clin-
ical variables studied, nor with markers NeuN, synapto-physin and HER2.
NeuN and synaptophysin – NeuN e synaptophysin were positive in 24 (60%) and 32 (80%) cases, respectively. There was no correlation between immunohistochemi-cal expression of NeuN and synaptophysin and the clini-copathologic characteristics.
p53 – P53 was positive in 18 samples (45%). seven sam-ples presented strong positive reaction (Fig 2c) and 11 weak reaction (Fig 2d). There was no statistical significance between p53 immunohistochemical expression and surviv-al. we found a statistically significant correlation between p53 and Ki-67 (p=0.02). P53-negative patients presented lower Ki-67 values than p53-positive patients (Table 4).
HER2 – Twenty-three (57.5%) samples expressed HER2 (Fig 2B) and showed a trend to association with poorer survival (p=0.07) (Fig 3).
dIscussIon
MB is a cerebellar embryonal tumor of grade IV (wHo) and it is also the most frequent brain tumor in children, accounting for 15-25% of brain tumors in this age bracket9. despite surgical treatment, radiotherapy and chemothera-
Fig 2. Photomicrographs of medulloblastoma. (A) immunoreactive cells to antibody Ki-67 (40x); (B) positive reaction to antibody HER2 in mem-brane and cytoplasm (40x); (C) cells with strong reaction to p53; (D) cells with weak reaction to p53 (40x).
Fig 3. Kaplan-Meier curve representing patient survival according to immunohistochemical expression of HER2.

Arq Neuropsiquiatr 2008;66(2-B)
389
Medulloblastoma: Immunohistochemical markersMeurer et al.
py, 50-60% of the affected individuals survive 5 years after the diagnosis16. currently, there are no accurate clinical prognostic markers except for tumor dissemination via liquor at the time of diagnosis4,5,17, hence the need for vali-dating new indicators of MB biological behavior. In order to assess the prognostic potential of Ki-67, NeuN, syn-aptophysin, HER2 and p53 in MB we have analyzed these proteins in 40 samples using the immunohistochemical technique and have correlated the results with clinico-pathological parameters such as: age, sex, histological subtype, presence of residual tumor, and survival. In our study, sex showed a great impact on survival rate. Male patients presented significantly reduced survival as com-pared to females (p=0.002). This finding was also reported by Jaros et al. and weil et al.14,18. As previously described by other authors2,15, the variables age, histological subtype, and presence of residual tumor did not have a statistically significant correlation with survival.
The immunohistochemical expression of protein Ki-67 is strongly associated with cellular proliferation and it is a widely used marker to evaluate the mitotic index in tumors. MBs are rapidly proliferating tumors, and they have a quite elevated Ki-67 expression7,15,19-21. In our study, the mean number of Ki-67-positive cells was 27.05%. This finding was not statistically significant concerning patient survival, even after stratification of the sample (Table 3), as suggested by Ito et al.8. These authors, studying a pop-ulation of 32 patients, have noted a significant associa-tion between the mitotic index and the prognosis. In this study, Ki-67-positive cells above 20% was associated with a worse prognosis. Miralbell et al.22 and Urberuaga et al.19
suggested that Ki-67 expression is probably not a deter-minant factor of prognosis in MB. In the present study, Ki-67 expression was greater in male patients (p=0.02), who also presented shorter survival (p=0.002). These data could suggest a possible connection between high mitotic index and shorter survival.
NeuN and synaptophysin are markers of neuronal dif-ferentiation6,9. The prognostic value of these markers is conflicting in the literature14. In our study, immunohisto-chemical expression of NeuN and synaptophysin were not correlated with prognosis.
TP53 is a gene that plays a key role in the regulation of the cell cycle and apoptosis. In normal cells, protein p53 is present in low levels and is generally undetectable through immunohistochemistry. High levels of p53 ex-pression in immunohistochemical reactions are related with deletions or genetic mutation points23. Expression and mutation of protein p53 are rare events in MBs9,14. In our study, 18 cases showed p53-positive cells, but, nei-ther the percentage of stained cells, nor the intensity of
staining were correlated with survival (p=0.88). studies conducted by Jaros et al.14 and woodburn et al.15 showed that strong immunohistochemical expression of protein p53 is associated with bad prognosis, yet there is no con-nection between prognosis and number of stained cells. An interesting finding observed in this study was a correla-tion between immunohistochemical expression of Ki-67 and p53. Patients with p53-negative cells presented lower Ki-67 values than patients with p53-positive cells. This may be related to the functional loss of mutated p53, which would allow a greater proliferation of neoplastic cells.
Proto-oncogen HER2 is located on chromosome 17 and codes for a membrane receptor glycoprotein, p185, which is thus called HER2 protein or receptor10. Immunohistochem-ical expression of this receptor is associated with worse prognoses in several human neoplasias, including MB11-13, 17.
Gilbertson et al.11 have demonstrated that protein HER2 is expressed in most MBs. In a retrospective study of 55 cases of MB, the prognostic value of HER2 expres-sion was dependent on the percentage of positive tumor cells. Patients with more than 50% of positive tumor cells presented a lower survival rate (p=0.0049). These findings were confirmed later by Gilbertson et al.24. In a study with 41 patients with MB, Herms et al.12 detected a smaller im-munohistochemical expression of HER2 (13%) in 45 cases of MB, but they also found a smaller survival rate for pa-tients with positive HER2, particularly in those diagnosed before 3 years of age. Gajjar et al.2 analyzed 81 cases of MB by the western blot technique and detected HER2 expres-sion in 40% of cases. HER2 expression in this study proved to be an independent factor of bad prognosis (p=0,031), showing a greater impact if combined with clinical charac-teristics of the patients. In our study, all patients who were clinically considered as “low risk and HER2-negative” were alive within 5 years, as compared to 54% of the patients considered as “low risk and HER2-positive” (p=0.001).
The immunohistochemical expression of HER2 in this study was positive in 23 (57.5%) of the samples and pre-sented a trend to association with poorer survival (p=0.07). some discrepancies about HER2 immunoreactivity found in the literature may be related to the morphological char-acteristic of MB cells, which have a scarce cytoplasm, mak-ing it difficult to ascribe the immunohistochemical stain-ing to the membrane or to the cytoplasm. In our study, staining in either cytoplasm or membrane was considered as positive. The same approach was used by Herms et al., Nam et al. and Gilbertson RJ et al.12,25,23. concerning to the survival rate, the results obtained in this study are in agreement with those by Nam et al.25 and Ray et al.17.
In conclusion, in our study, the only variable that showed influence in patients’ survival rate and which might

Arq Neuropsiquiatr 2008;66(2-B)
390
Medulloblastoma: Immunohistochemical markersMeurer et al.
be considered as a potential prognostic factor in MB, was the greatest proliferative index measured for Ki-67 in male patients, who presented a statistically significant shorter survival. P53 also was associated with a greater prolifera-tive index. considering the other immunohistochemical markers studied, particularly HER2, we suggest that fur-ther investigations are needed, with larger samples, based on the tendency towards an association found by us.
references 1. EllisonDW,CliffordSC.,GajjarA,GilbertsonJR.What’snewinneu-
ro-oncology?Recentadvancesinmedulloblastoma.EurJPaediatNeu-rol2003;7:53-66.
2. GajjarA,HernanR,KocakM,etal.Clinical,histopathologic,andmo-lecular markers of prognosis: toward a new disease risk stratification systemformedulloblastoma.JClinOncol2004;22:984-993.
3. ChangCH,HousepianEM,HerbertCJR.Anoperativestagingsys-temandamegavoltageradiotherapeutictechnicforcerebellarmedul-loblastomas.Radiology1969;93:1351-1359.
4. GilbertsonJR.Medulloblastoma:signallingachangeintreatment.Lan-cetOncol2004;5:209-218.
5. RutkauskienéG,LabanauskasL,JaruseviciusL.Theresultsofthetreat-mentofchildhoodmedulloblastomawithradiotherapyatKaunasUniversityofMedicineHospitalin1994-2000.Medicina(Kaunas)2006;42(1).
6. EllisonD.Classifyingthemeduloblastoma;insightsfrommorphologyandmoleculargenetics.NeuropatholAppNeurobiol2002;28:257-282.
7. Grotzer MA, Geoerger B, Janss AJ, et al. Prognostic significance of Ki-67(MIB-1)proliferationindexinchildhoodprimitiveneuroectodermaltumorsofthecentralnervoussystem.MedPediatOncol2001;36:268-273.
8. ItoS,HoshinoT,PradosMD,EdwardsMSB.Cellkineticsofmedullo-blastoma.Cancer1992;70:671-678.
9. LantosPL,LouisDN,RosenblumMK,KleihuesP.Tumoursofthener-vous system. In Graham DI, Lantos PL (eds). Greenfield’s neuropathol-ogy.London:Arnold2002;2:882-894.
10. PreusserM,LaggnerU,HaberlerC,etal.ComparativeanalysisofNeuNimmunoreactivityinprimarybraintumours:conclusionsforra-tionaluseindiagnostichistopathology.Histopathology2006;48:438-444.
11. Gilbertson RJ, Pearson ADJ., Perry RH, et al.. Prognostic significant of
thec-erbB2oncogeneproductinchildhoodmedulloblastoma.BrJCan-cer1995;71:473-477.
12. HermsJW,BehnkeJ,BergmannM,etal.PotentialprognosticvalueofC-erbB-2ExpressioninMedulloblastomasinveryyoungchildren.JPe-diatHematol/Oncol1997;19:510-515.
13. GilbertsonRJ.ERBB2inpediatricCancer:innocentuntilprovenguilty.TheOncologist2005;7:508-517.
14. Jaros E, Lunec J, Perry RH, et al. P53 protein overexpression identifies agroupofcentralprimitiveneuroectodermaltumourswithpoorprog-nosis.BrJCancer1993;68:801-807.
15. WooburnRT,AzzarelliB,MontebelloJ.F,GossIE.Intensep53stainingisavaluableprognosticindicatorforpoorprognosisinmedulloblasto-ma/centralnervoussystemprimitiveneuroectodermaltumors.JNeu-ro-Oncol2001;52:57-62.
16. BrandesAA,ParisMK.Reviewoftheprognosticfactorsinmedulloblas-tomaofchildrenandadults.CritRevOncol/Hematol2004;50:121-128.
17. RayA,HoM,MaJ,etal.Aclinicobiologicalmodelpredictingsurviv-alinmedulloblastoma.ClinCancerRes2004;10:7613-7620.
18. Weil MD, Lamborn K, Edwards MS, Wara WM. Influence of a child’s sexonmedulloblastomaoutcome.JAMA1998;13:279:1474-1476.
19. UrberuagaA,NavajasA,BurgosJ,PijoánJI.AreviewofclinicalandhistologicalfeaturesofSpanishpaediatricmedulloblastomasduringthelast21years.ChildsNervSyst2005;22:466-474.
20. FerrariAF,AraújoMBM,AguiarPH,PleseJPP.Medulloblastoma:eval-uationofproliferativeindexbymonoclonalantibodyMib-1,itsprog-nosticcorrelationandtherapeuticimplications.ArqNeuropsiquiatr2003;61:3A.
21. KayaselçukF,ZorludemirS,GümürdülüD,etal.PCNAandKi-67incentralnervoussystemtumors:correlationwiththehistologicaltypeandgrade.JNeuro-Oncol2002;57:115-121.
22. MiralbellR,TolnayM,BieriS,etal.Pediatricmedulloblastoma:prog-nosticvalueofp53,bcl-2,Mib-1,andmicrovesseldensity.JNeuro-Oncol1999;45:103-110.
23. SoussiT.Thep53tumorsuppressorgene:frommolecularbiologytoclinicalinvestigation.AnnNYAcadSci2000;910:121-137;discussion137-139.
24. GilbertsonRJ,WickramasingheC,HermanR,etal.Clinicalandmo-lecular stratification of disease risk in medulloblastoma. Br J Cancer 2001;85:705-712.
25. NamDH,WangKC,KimYM,etal.Theeffectofisochromosome17qpresence,proliferativeandapoptoticindices,expressionofC-erbB-2,bcl-2andp53proteinsontheprognosisofmedulloblastoma.JKoreanMedSci2000;15:452-456.





























