Embed Size (px)
Citation preview
5/22/2020
RECOGNITION AND MANAGEMENT
OF POSTPARTUM DEPRESSION IN THE
PEDIATRIC OFFICE VISIT
MEREDITH SPADA, MD
ASSISTANT PROFESSOR OF
PSYCHIATRY
UNIVERSITY OF PITTSBURGH
SCHOOL OF MEDICINE
EYDIE MOSES-KOLKO, MD
ASSOCIATE PROFESSOR OF
PSYCHIATRY
UNIVERSITY OF PITTSBURGH
SCHOOL OF MEDICINE
OBJECTIVES
Describe the rationale for screening for postpartum depression
Describe a screening tool that is appropriate for identifying postpartum depression in the pediatrics office visit
Describe appropriate disposition planning for moms who present to a newborn/infant visit with postpartum depression
2
1
2
5/22/2020
PART 1
Why screen for postpartum depression?
3
QUESTION 1
Which of the following is a potential consequence of
postpartum depression?
A. Fewer reports of child abuse and neglect
B. Improved parental adherence to safety guidelines
C. Increased rates of breastfeeding
D. Inappropriate medical care
4
3
4
5/22/2020
QUESTION 2
Which of the following is more likely in the offspring of
mothers with postpartum depression?
A. Impaired social interaction
B. Delays in language, cognitive, and social-emotional development
C. ADHD, anxiety, depression, and conduct disorder
D. All of the above
5
QUESTION 3
Are you currently conducting screening for postpartum
depression in your practice?
A. yes
B. no
6
5
6
5/22/2020
QUESTION 4
What year did the American Academy of Pediatrics recommend
screening for postpartum depression?
A. 1995
B. 2010
C. 2013
D. 2019
7
QUESTION 5
How much more likely are pediatricians to detect postpartum
depression when a screening tool is utilized?
A. 2X
B. 4X
C. 8X
D. 20X
8
7
8
5/22/2020
PART 2
IMPLEMENTING THE Edinburgh Postnatal
Depression Scale (EPDS)
9
SCREENING FOR POSTPARTUM DEPRESSION
Edinburgh Postnatal Depression Scale
Widely used and validated
Ten-items; item 10 assesses suicidality
Score by summing items (3 items reverse scored)
AAP recommends screening at 1, 2, 4, and 6- month visits
10
Earls 2010 Pediatrics
9
10
5/22/2020
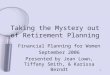
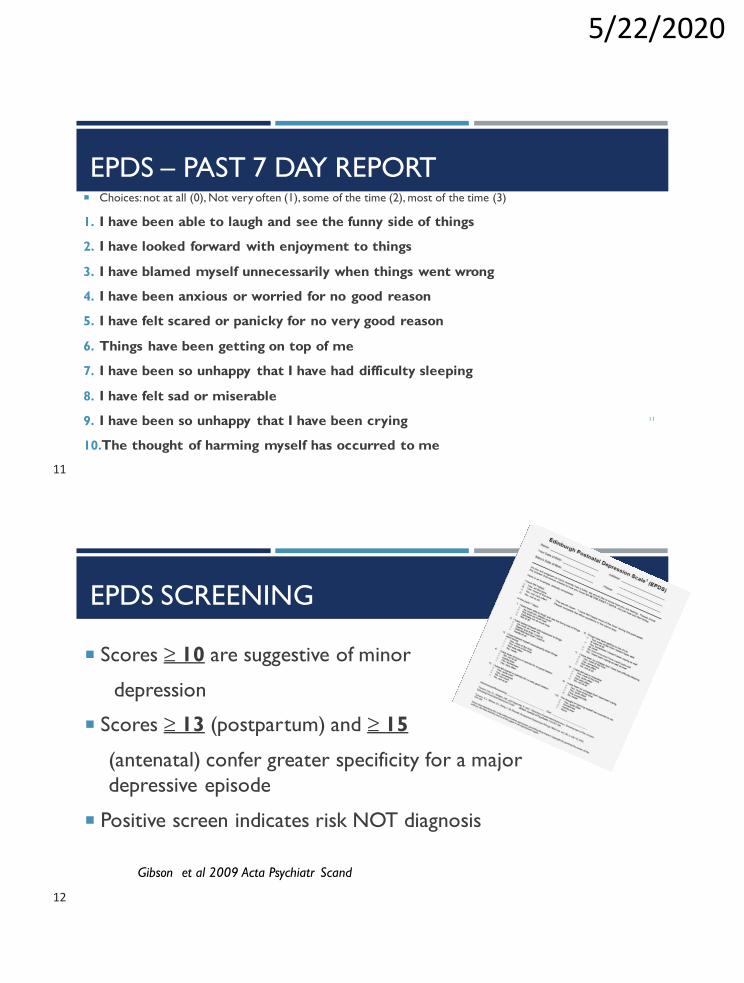
EPDS – PAST 7 DAY REPORT
11
Choices: not at all (0), Not very often (1), some of the time (2), most of the time (3)
1. I have been able to laugh and see the funny side of things
2. I have looked forward with enjoyment to things
3. I have blamed myself unnecessarily when things went wrong
4. I have been anxious or worried for no good reason
5. I have felt scared or panicky for no very good reason
6. Things have been getting on top of me
7. I have been so unhappy that I have had difficulty sleeping
8. I have felt sad or miserable
9. I have been so unhappy that I have been crying
10.The thought of harming myself has occurred to me
EPDS SCREENING
Scores ≥ 10 are suggestive of minor
depression
Scores ≥ 13 (postpartum) and ≥ 15
(antenatal) confer greater specificity for a major
depressive episode
Positive screen indicates risk NOT diagnosis
Gibson et al 2009 Acta Psychiatr Scand
11
12
5/22/2020
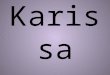
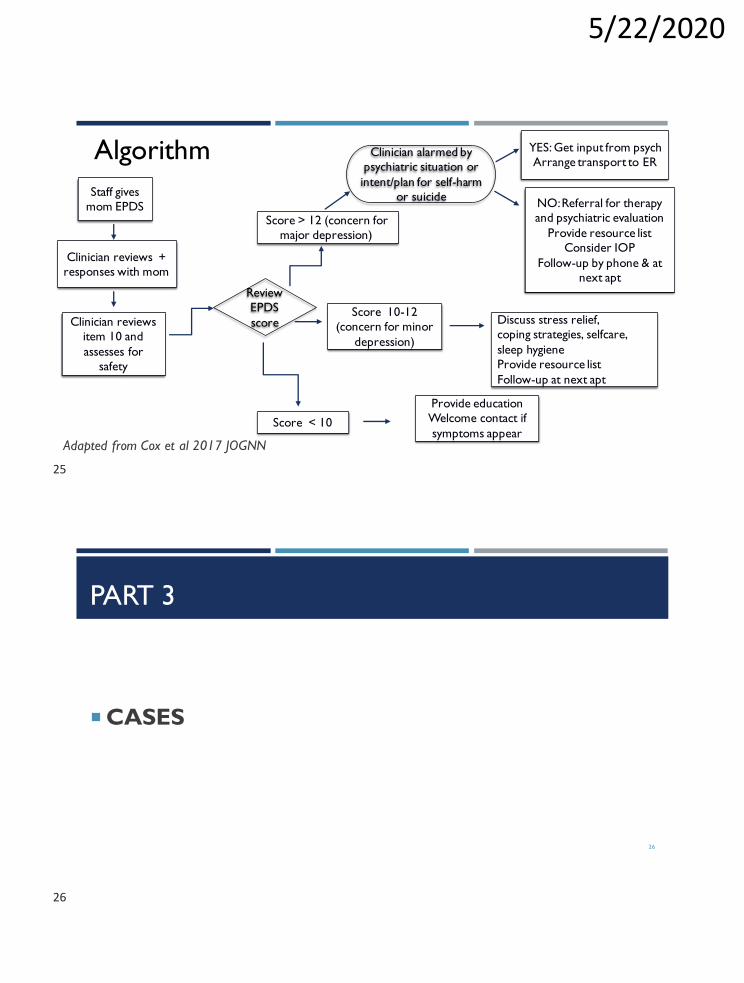
Staff gives
mom EPDS
Adapted from Cox et al 2017 JOGNN
Algorithm
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Adapted from Cox et al 2017 JOGNN
Algorithm
13
14
5/22/2020
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Adapted from Cox et al 2017 JOGNN
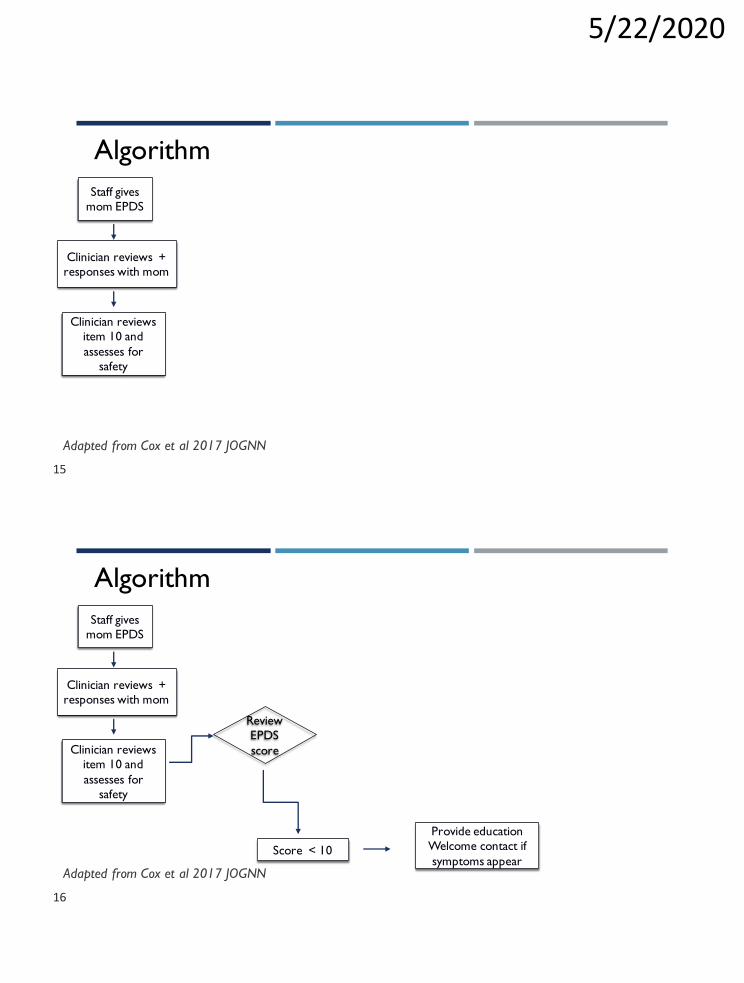
Algorithm
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Review
EPDS
score
Score < 10
Provide education
Welcome contact if
symptoms appearAdapted from Cox et al 2017 JOGNN
Algorithm
15
16
5/22/2020
17
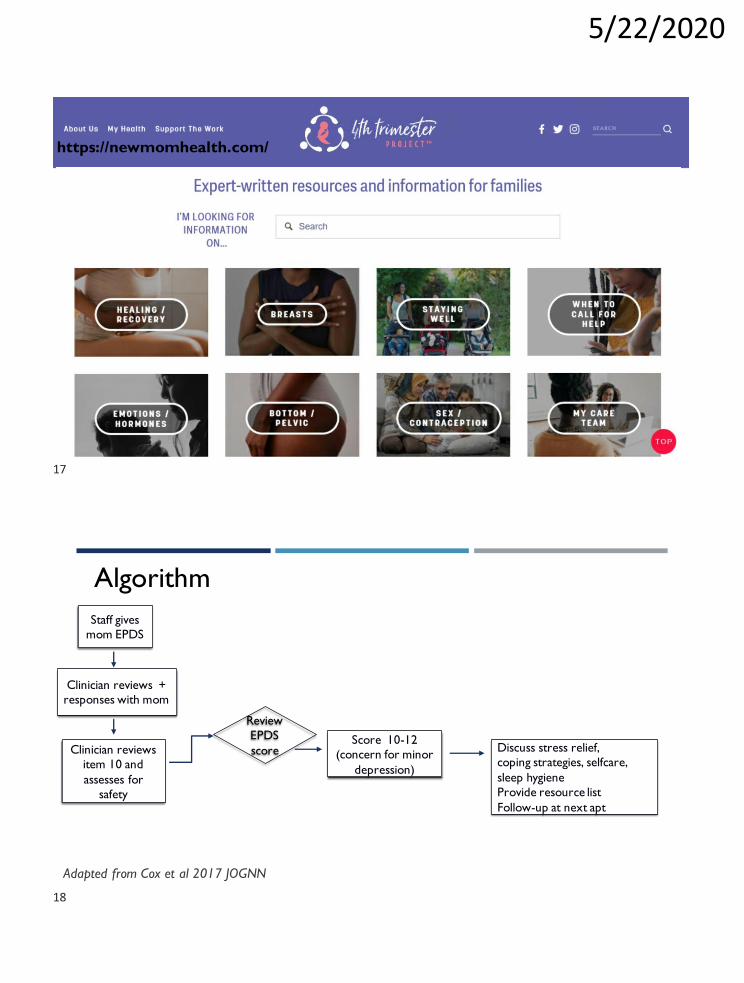
https://newmomhealth.com/
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Review
EPDS
scoreScore 10-12
(concern for minor
depression)
Discuss stress relief,
coping strategies, selfcare,
sleep hygiene
Provide resource list
Follow-up at next apt
Adapted from Cox et al 2017 JOGNN
Algorithm
17
18
5/22/2020
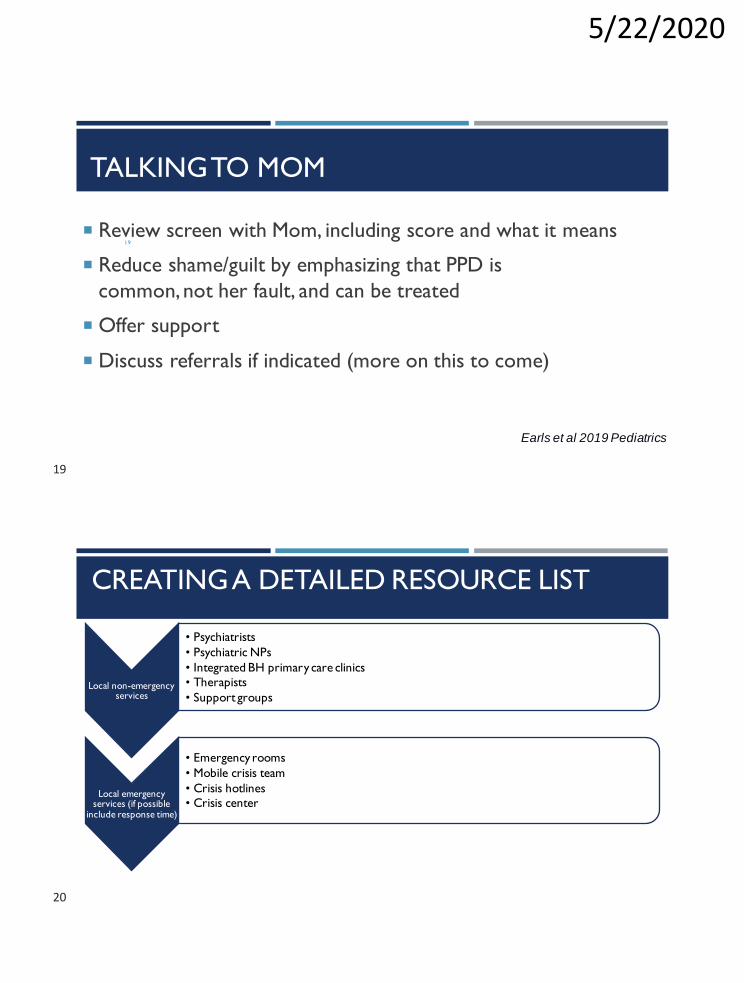
TALKINGTO MOM
19
Review screen with Mom, including score and what it means
Reduce shame/guilt by emphasizing that PPD is
common,not her fault, and can be treated
Offer support
Discuss referrals if indicated (more on this to come)
Earls et al 2019 Pediatrics
CREATING A DETAILED RESOURCE LIST
Local non-emergency services
• Psychiatrists
• Psychiatric NPs
• Integrated BH primary care clinics
• Therapists
• Support groups
Local emergency services (if possible
include response time)
• Emergency rooms
• Mobile crisis team
• Crisis hotlines
• Crisis center
19
20
5/22/2020
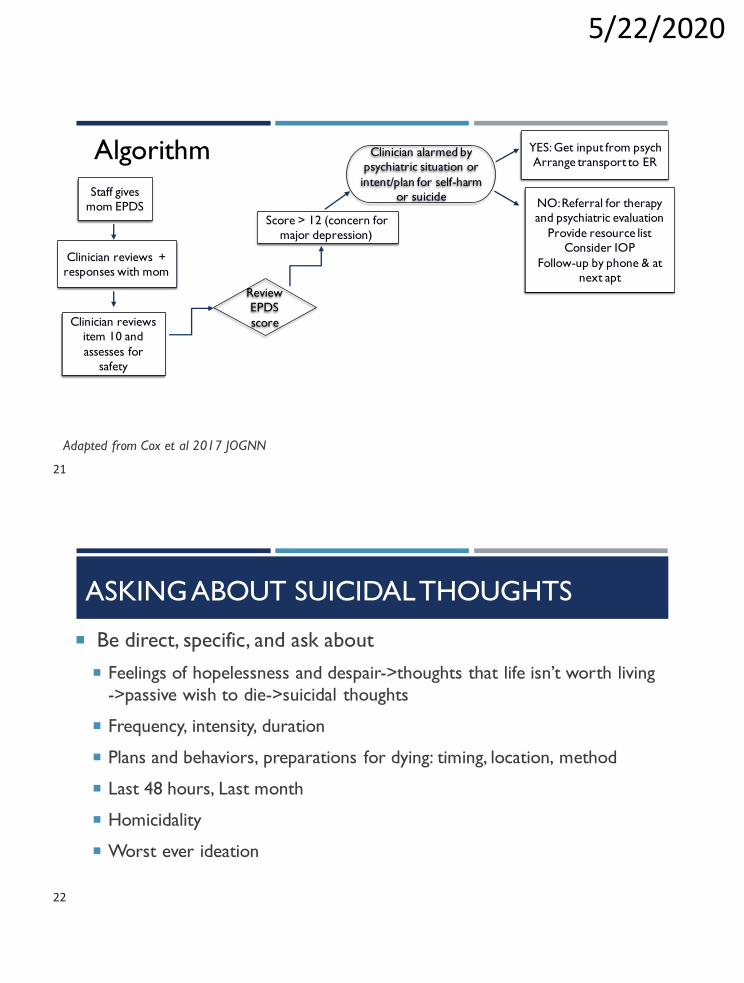
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Review
EPDS
score
Score > 12 (concern for
major depression)
Clinician alarmed by
psychiatric situation or
intent/plan for self-harm
or suicide
YES: Get input from psych
Arrange transport to ER
NO: Referral for therapy
and psychiatric evaluation
Provide resource list
Consider IOP
Follow-up by phone & at
next apt
Adapted from Cox et al 2017 JOGNN
Algorithm
ASKING ABOUT SUICIDAL THOUGHTS
22
Be direct, specific, and ask about
Feelings of hopelessness and despair->thoughts that life isn’t worth living
->passive wish to die->suicidal thoughts
Frequency, intensity, duration
Plans and behaviors, preparations for dying: timing, location, method
Last 48 hours, Last month
Homicidality
Worst ever ideation
21
22
5/22/2020
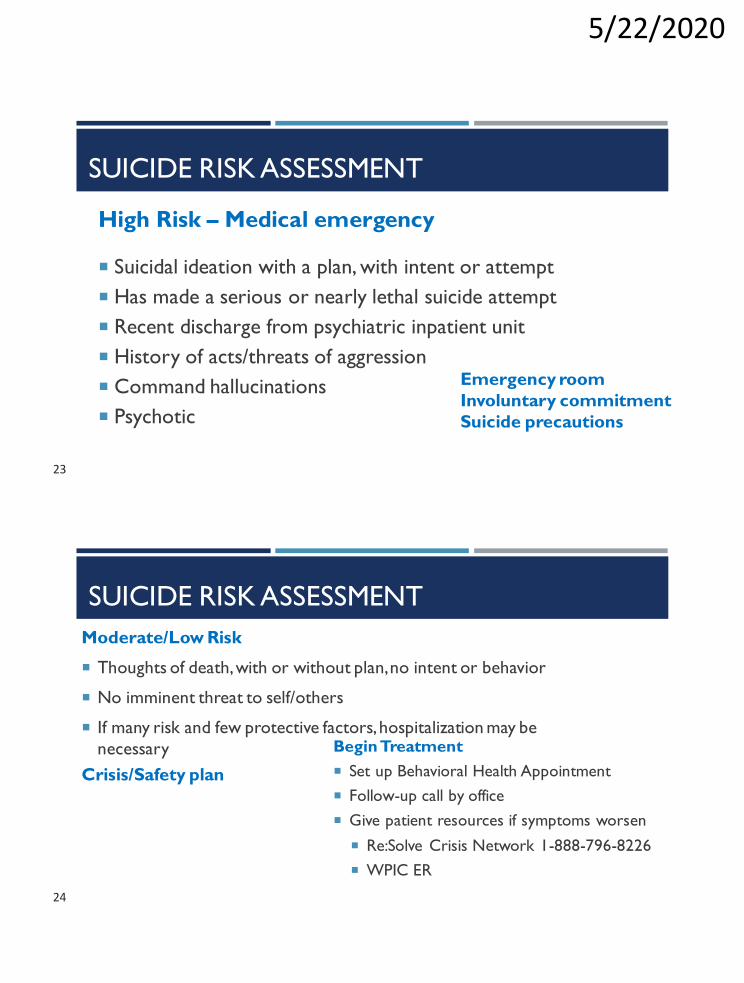
SUICIDE RISK ASSESSMENT
High Risk – Medical emergency
Suicidal ideation with a plan, with intent or attempt
Has made a serious or nearly lethal suicide attempt
Recent discharge from psychiatric inpatient unit
History of acts/threats of aggression
Command hallucinations
Psychotic
Emergency room
Involuntary commitment
Suicide precautions
SUICIDE RISK ASSESSMENT
Moderate/Low Risk
Thoughts of death, with or without plan, no intent or behavior
No imminent threat to self/others
If many risk and few protective factors, hospitalization may be
necessary
Crisis/Safety plan
Begin Treatment
Set up Behavioral Health Appointment
Follow-up call by office
Give patient resources if symptoms worsen
Re:Solve Crisis Network 1-888-796-8226
WPIC ER
23
24
5/22/2020
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Review
EPDS
score
Score > 12 (concern for
major depression)
Clinician alarmed by
psychiatric situation or
intent/plan for self-harm
or suicide
Score 10-12
(concern for minor
depression)
Score < 10
YES: Get input from psych
Arrange transport to ER
NO: Referral for therapy
and psychiatric evaluation
Provide resource list
Consider IOP
Follow-up by phone & at
next apt
Discuss stress relief,
coping strategies, selfcare,
sleep hygiene
Provide resource list
Follow-up at next apt
Provide education
Welcome contact if
symptoms appearAdapted from Cox et al 2017 JOGNN
Algorithm
PART 3
CASES
26
25
26
5/22/2020
CASE 1
Ms. B is a 32 yo G1P1 who presents to her son's 2 month
visit.The son is overall healthy and growth is appropriate
EPDS =14 (0 for item 10)
27
CASE 1 CONTINUED
When following up on the EPDS, Ms. B bursts into tears, stating that she has been having trouble getting out of bed. She has had difficulty sleeping, extreme anxiety, poor appetite, tearfulness, and difficulty coping.
She reports that she has been having the thought that it would be better if she didn’t wake up or if she died, however she denies SI/HI/intent/plan. She adamantly denies any thoughts to harm herself, baby, or anyone else.
28
27
28

5/22/2020
CASE 1
29
DISCUSS WITH YOUR GROUP
BABY BLUES
Self-limited
Maternal role functioning not affected
Within 10 days of delivery
50-80% of new mothers
Symptoms: tearfulness, irritability, anergia,
overwhelmed feelings30
29
30
5/22/2020
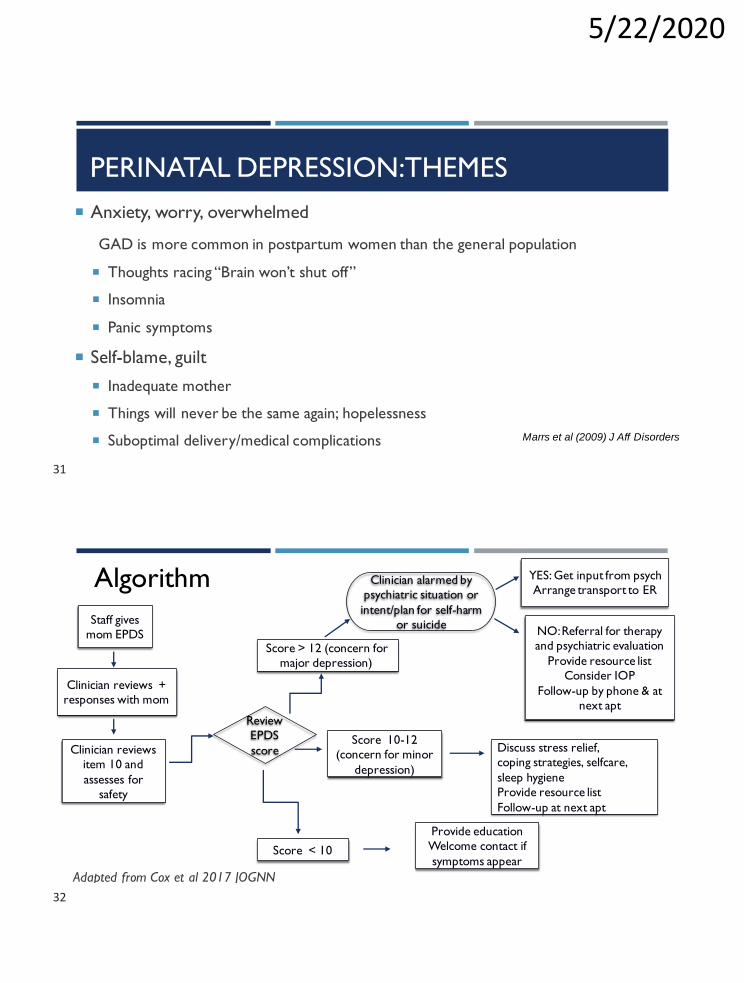
PERINATAL DEPRESSION: THEMES
Anxiety, worry, overwhelmed
GAD is more common in postpartum women than the general population
Thoughts racing “Brain won’t shut off”
Insomnia
Panic symptoms
Self-blame, guilt
Inadequate mother
Things will never be the same again; hopelessness
Suboptimal delivery/medical complications Marrs et al (2009) J Aff Disorders
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Review
EPDS
score
Score > 12 (concern for
major depression)
Clinician alarmed by
psychiatric situation or
intent/plan for self-harm
or suicide
Score 10-12
(concern for minor
depression)
Score < 10
YES: Get input from psych
Arrange transport to ER
NO: Referral for therapy
and psychiatric evaluation
Provide resource list
Consider IOP
Follow-up by phone & at
next apt
Discuss stress relief,
coping strategies, selfcare,
sleep hygiene
Provide resource list
Follow-up at next apt
Provide education
Welcome contact if
symptoms appear
Adapted from Cox et al 2017 JOGNN
Algorithm
31
32
5/22/2020
33
DOCUMENTATION IN INFANT'S CHART
Type of screening tool used
Discussion with mother/parents (whether positive or negative)
If indicated: followup and referral plan
There is no reason to open a chart on the mother because she
is not receiving treatment
Earls et al 2019 Pediatrics
CASE 2
Ms. C is 21 year old G3. She presents with her 1 month old
daughter
She lives with her mom and 3 children
She scores a 15 on the EPDS and responds "yes, quite often" to
question 10 regarding thoughts of harming self
She reports a history of severe postpartum depression
following the birth of her first child34
33
34
5/22/2020
You followup the EPDS and perform a suicide screen
What questions would you ask to assess for suicidality?
35
CASE 2 CONTINUED
CASE 2 CONTINUED
She reports that she has had suicidal thoughts to overdose on
over the counter medications. She feels hopeless.
She denies that she has taken steps to move forward with this
plan including googling how much she would need to take.
What is your plan?
36
35
36
5/22/2020
CASE 2
37
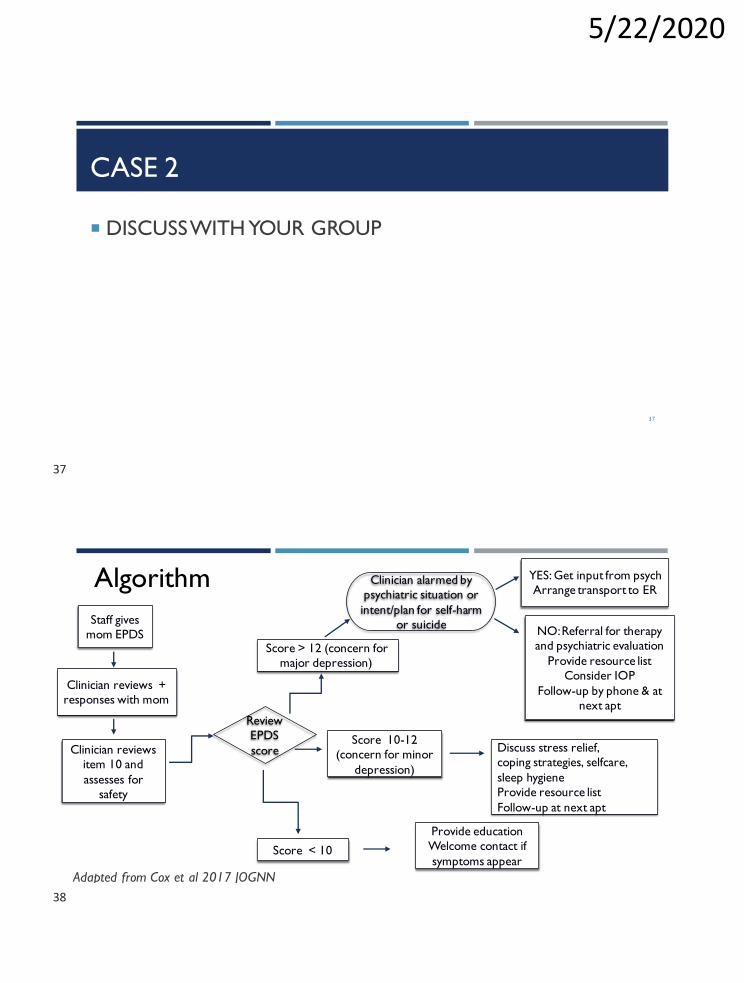
DISCUSS WITH YOUR GROUP
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Review
EPDS
score
Score > 12 (concern for
major depression)
Clinician alarmed by
psychiatric situation or
intent/plan for self-harm
or suicide
Score 10-12
(concern for minor
depression)
Score < 10
YES: Get input from psych
Arrange transport to ER
NO: Referral for therapy
and psychiatric evaluation
Provide resource list
Consider IOP
Follow-up by phone & at
next apt
Discuss stress relief,
coping strategies, selfcare,
sleep hygiene
Provide resource list
Follow-up at next apt
Provide education
Welcome contact if
symptoms appear
Adapted from Cox et al 2017 JOGNN
Algorithm
37
38
5/22/2020
CASE 3
27 yo MF presents with her 2 year old son and 6 mo old
daughter who she is breastfeeding
She reports fears that something horrible could happen to her
children
Has panic attacks, very poor sleep, low energy and difficulty
functioning
She scores a 22 on the EPDS and responds "yes, quite often" to
question 10 39
CASE 3 (CONT’D)
You dig deeper:
She refuses to leave children for fear of their safety despite her husband’s suggestion that she should visit with a friend to help relax
She is having both children sleep in her room at night so that she can check on their breathing
She is fearful of using the stairs because she is worried she will drop her children
She has stopped cooking and is ordering takeout because she has repeated distressing images of stabbing her children with a knife. This is extremely distressing for her.
PCP recommended Zoloft, but she was too fearful about side effects, on self, nursing infant, and fear if she were to become pregnant and how it would affect fetus
40
39
40
5/22/2020
CASE 3
41
DISCUSS WITH YOUR GROUP
OBSESSIVE-COMPULSIVE SYMPTOMS
Obsessions = Irrational, intrusive thoughts
25% of perinatal women have obsessions; 3-9% of perinatal women have OCD
Examples: Aggressive, harm befalling loved ones, contamination
Obsessions are ego-dystonic, very distressing, and mothers try to resist them or avoid
danger
Compulsions = Irresistible urges
Checking repeatedly on infant “won’t let child out of my sight”
Breastfeeding/pumping schedule
Preventing contact with germsWisner, Hudak et al AJP; Fairbrother and Woody AWMH 2008
41
42
5/22/2020
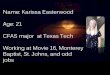
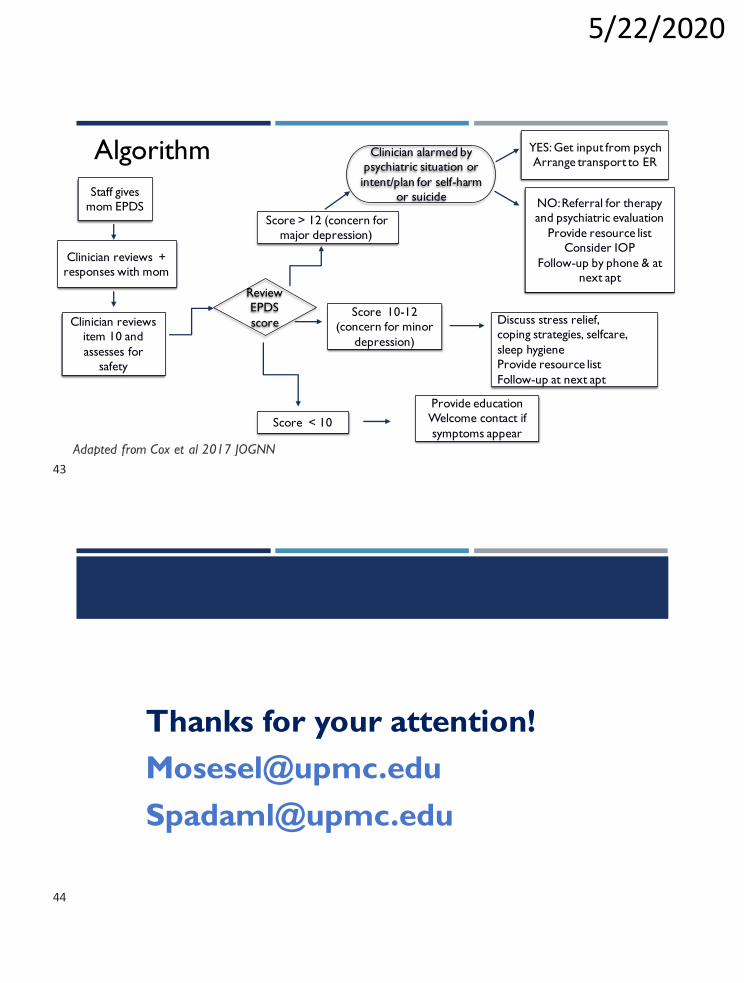
Staff gives
mom EPDS
Clinician reviews +
responses with mom
Clinician reviews
item 10 and
assesses for
safety
Review
EPDS
score
Score > 12 (concern for
major depression)
Clinician alarmed by
psychiatric situation or
intent/plan for self-harm
or suicide
Score 10-12
(concern for minor
depression)
Score < 10
YES: Get input from psych
Arrange transport to ER
NO: Referral for therapy
and psychiatric evaluation
Provide resource list
Consider IOP
Follow-up by phone & at
next apt
Discuss stress relief,
coping strategies, selfcare,
sleep hygiene
Provide resource list
Follow-up at next apt
Provide education
Welcome contact if
symptoms appear
Adapted from Cox et al 2017 JOGNN
Algorithm
Thanks for your attention!
43
44