Embed Size (px)
Citation preview

HNF 470 Diet Therapy and Coronary Heart Disease (CHD)
I. Risk Factors for Developing CHD
II. Diet-Responsive Risk Factors for CHD
A. American Heart Association “Step” DietsB. Role for Dietary Supplements?
III. Diet Therapy in the Secondary Prevention of IHD
IV. Diet Therapy in the Primary Prevention of IHD
V. Are AHA Step I and II Guidelines Enough?
http://www.msu.edu/course/hnf/470

Definitions andTerminologies

The Burden
Deaths due to CVD are the #1 cause of death in the u.s.
(#1 = Coronary heart Disease; #3 = Stroke)
Mortality has dropped DRAMATICALLY in thepast two decades--
• 1˚ ly due to advances in treatment• Incidence has not changed.

Coronary Heart Disease
Cause: Formation of Atherosclerotic Plaques
Risk Factors: Maleness (>45 yo), Femaleness (>55 yo)High LDL (>160 mg/dl); Low HDL (<35 mg/dl)Hypertension (Diastolic >90 mm Hg)SmokerDMFamily Hx
Etiology: Current hypothesis: Oxidation of the apolipoproteincomponent of LDL leads to injury of cells liningthe artery (intima). Damage leads to plateletactivation, excessive clotting, and atherogenesis.Narrowing of the artery leads to a hypoxic (ischemic)condition in target organs.

Risk Factors for CHD:The Framingham Heart Study
Major Risk Factors “Important” Risk Factors
Cigarette Smoking Obesity*Hypertension* Physical InactivityHigh Total Serum Cholesterol* Family Hx of Premature CHDLow HDL Cholesterol* Hypertriglyceridemia*Diabetes Mellitus* Increased Lipoprotein [a]
Increased serum homocysteine*Abnormal levels of various
coagulation factors
*Dietary factors contribute strongly to the control of or in the etiology of these risk factors.

Diet-Related Risk Factors
High LDL Cholesterol High LDL Cholesterol
Begin treatment LDL Cholesterol (mg/dl)
With CHD: >100Without CHD + one risk factor: >160 Without CHD + > 2 risk factors: >130
Low HDL CholesterolLow HDL Cholesterol
HypertensionHypertension
Diabetes MellitusDiabetes Mellitus

Blood Lipid Fraction Desirable Borderline High
LDL Cholesterol (mg/dl) <130 130-159 >160
Total Cholesterol (mg/dl) <200 200-239 >240
Triglycerides (Fasting; mg/dl) <200 200-400 >400
HDL Cholesterol= “Low” (Bad) if 35 mg/dl
LDL:HDL ratio: > 5 indicates risk for men >4.5 indicates risk for women

Diastolic Pressure (mm Hg)
< 85 = Normal
80-89 = High-Normal
90-99 = Mild
100-109 = Moderate
110-119 = Severe
>120 = Very Severe

Source: http://www.bmj.com
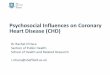
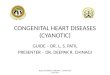
Figure 1: Annual trends in incidence and case fatality rate of CHD by country.
United States Russia, E. Europe, China

Source: http://www.bmj.com

Role of Diet in the Modification of Blood Cholesterol Levels
Assumptions:
• Blood cholesterol [ ] is an important and modifiable risk factor for coronary heart disease. • Sustained reduction of total cholesterol [ ] of 1% is associated with a 2-3% reduction in the incidence of coronary heart disease.

Total Cholesterol Levels (mg/dl) in the U.S.(National Health and Nutrition Examination Surveys)
Age Group 1976-80 1988-1994
Adults 213 203
Adolescents (ages 12-17) 167 160

Role of Diet in the Modification of Blood Cholesterol Levels-3
Tang et al. (1998) BMJ 316: 1213-1220Systematic review of dietary intervention trials to lower blood total cholesterol in free-living subjects.
Efficacy of Dietary Intervention Trials to Lower Total Cholesterol
Diet Types % Reduction inTotal Cholesterol
AHA Step 2
Lower Total Fat 6.0
Raise PUFA:SFA Ratio
AHA Step 1 3.0


Tang et al. (1998) BMJ 316: 1213-1220Systematic review of dietary intervention trials to lower blood total cholesterol in free-living subjects.
Role of Diet in the Modification of Blood Cholesterol Levels-4
How Do These Results Compare to Metabolic Ward Studies?
• Dietary change results in decreases of total cholesterolup to 15%.
• Difficulties in complying with the prescribed dietary changemay explain the failure to achieve the expected reductionsin cholesterol concentrations.
• Even so, diets low in saturated fat and cholesterol areimportant adjunctive therapies for lowering populationrisk of CHD.


Role of Diet in the Modification of Blood Cholesterol Levels-2
Chief Determinants of Blood Cholesterol Levels
1. Certain saturated fatty acids cause a linear increasein low-density lipoprotein (LDL) cholesterol concentration.(Total SFA in U.S. Diet: 11-12 % of total energy)
2. Trans unsaturated fatty acids increase LDL cholesterol[ ]; not quite as atherogenic as certain SFA.(Total trans FA in U.S. Diet: ~ 3 % of total energy)
3. Polyunsaturated fatty acids derived from plant oils doNOT raise LDL cholesterol [ ].(Total PUFA in U.S. Diet: ~ 6 % of total energy)
4. Monounsaturated fatty acids derived from high oleic acid(cis-18:1) oils (e.g., olive, peanut, canola) do NOT raiseLDL cholesterol [ ].


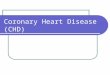
Deciles of PUFA:SFA Ratio and Risk of CHD in Women (Hu et al. AJCN 70: 1001-8, 1999)


The eating plan is based on these AHA dietary guidelines:
* Total fat intake should be less than 30 % of calories.
* Saturated fatty acid intake should be less than 10 % of calories.
* Polyunsaturated fatty acid intake should be no more
than 10 percent of calories.
* Monounsaturated fatty acids make up the rest of the total fat intake, about 10 to 15 % of total calories.
* Cholesterol intake should be no more than 300 mG per day.
* Sodium intake should be no more than
2400 milligrams (3 grams) per day.

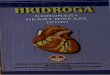
Fruit and Vegetable Intake in the Nurses Health Study and Relative Risk of CHD

To control the amount and kind of fat, saturated fatty acids, and dietary cholesterol you eat:
Eat up to 6 ounces (cooked) per day of lean meat, fish and skinless poultry.
The approximately 5 to 8 teaspoon servings of fats and oils per day may be used for cooking and baking, and in salad dressings and spreads.
Use cooking methods that require little or no fat — boil, broil, bake, roast, poach,
steam, sauté, stir-fry or microwave.
Trim off the fat you can see before cooking meat and poultry. Drain off all fat after browning.
The 3 to 4 egg yolks per week included in your eating plan may be used alone or in cooking and baking (including store-bought products).
Choose skim or 1% fat milk and nonfat or low-fat yogurt and cheeses.

Physicians Health StudyHennekens et al. (1996) N Engl J Med 334:1145.
•• 22,071 male physicians randomized to alternate-day22,071 male physicians randomized to alternate-dayß-carotene (50 mg), aspirin (325 mg), both activeß-carotene (50 mg), aspirin (325 mg), both activetreatments, or both placebos.treatments, or both placebos.
•• Aspirin component terminated early (1988) due toAspirin component terminated early (1988) due tostatistically extreme 44% reduction in risk of firststatistically extreme 44% reduction in risk of firstmyocardial infarction.myocardial infarction.
•• After 12 years of treatment with ßC, there was noAfter 12 years of treatment with ßC, there was noeffect on any CA endpoint, MI, stroke, or CHDeffect on any CA endpoint, MI, stroke, or CHDdeaths.deaths.

Vitamin E Supplementation and CHD
•• Evidence from prospective trials (Physicians HealthEvidence from prospective trials (Physicians HealthStudy, Nurses Health Study) showed ~40% reductionStudy, Nurses Health Study) showed ~40% reductionin CHD incidence with > 2 yrs intake of >100 I.U. AT.in CHD incidence with > 2 yrs intake of >100 I.U. AT.
•• The Iowa Women’s Health Study showed that vitamin EThe Iowa Women’s Health Study showed that vitamin Econtent in FOOD, not supplements, was inverselycontent in FOOD, not supplements, was inverselyassociated with risk of death from CHD (lowest vs.associated with risk of death from CHD (lowest vs.highest quintile of consumption: RR= 0.38;p=0.004)highest quintile of consumption: RR= 0.38;p=0.004)

Cambridge Heart Antioxidant StudyCambridge Heart Antioxidant Study (Stephens et al. (1996) Lancet 347: 781-86)(Stephens et al. (1996) Lancet 347: 781-86)
** Double-blinded study of the prevention of CVD death Double-blinded study of the prevention of CVD death and non-fatal MI in patients with angiographically proven and non-fatal MI in patients with angiographically proven coronary atherosclerosis receiving alpha tocopherol or coronary atherosclerosis receiving alpha tocopherol or a placebo.a placebo.
** 2002 patients2002 patients 546 (800 I.U.) 546 (800 I.U.)
489 (400 I.U.)489 (400 I.U.)
967 (placebo)967 (placebo)
** Median follow-up: Median follow-up: 510 days (range 3-981)510 days (range 3-981)

CHAOS ResultsCHAOS Results
1.1. Alpha tocopherol treatment decreased risk of CVD deathAlpha tocopherol treatment decreased risk of CVD deathand non-fatal MI:and non-fatal MI:
Relative Risk (RR):Relative Risk (RR): 0.53 (95% CI 0.34-0.83; p=0.005)0.53 (95% CI 0.34-0.83; p=0.005)
2.2. Most of this benefit was due to decreased risk of non-fatalMost of this benefit was due to decreased risk of non-fatalMI:MI:
RR:RR: 0.23 (95% CI 0.11-0.47; p=0.005)0.23 (95% CI 0.11-0.47; p=0.005)
3.3. Non-significant INCREASE or excess in cardiovascular Non-significant INCREASE or excess in cardiovascular deaths in the treatment group compared to the placebo group.deaths in the treatment group compared to the placebo group.

Vitamin E: A ReviewFunction: Cell Membrane AntioxidantFunction: Cell Membrane Antioxidant
(prevents lipid peroxidation/free radical generation)(prevents lipid peroxidation/free radical generation)
Alpha-TocopherolAlpha-Tocopherol Gamma-TocopherolGamma-Tocopherol
• • higher vitamin E activityhigher vitamin E activity • principal form of • principal form of • • more potent antioxidantmore potent antioxidant vitamin E in U.S. diet vitamin E in U.S. diet• • primary form of supplemental vitamin Eprimary form of supplemental vitamin E • more rapid uptake and• more rapid uptake and• • low plasma levels are strong predictors oflow plasma levels are strong predictors of cellular turnover cellular turnover risk of certain cancers and CHDrisk of certain cancers and CHD • traps mutagenic• traps mutagenic• • displaces gamma-T in plasma/other tissuesdisplaces gamma-T in plasma/other tissues electrophiles like NOx electrophiles like NOx• • 5-fold higher plasma levels than gamma-T5-fold higher plasma levels than gamma-T

Dietary Effectors of Endothelial Cell Function (“NOT ready for prime time”)
• Arginine: substrate for endothelial nitric oxidesynthase
HeartBar®: 3 grams arginine per barPurports “Heart Healthy” benefits
• Pharmacologic Doses of Vitamins A and C
• Negative Effector: High Fat Diets

Frequent nut consumption and risk ofcoronary heart disease in women: prospective cohort study
Frank B Hu et al. Harvard University School of Public HealthBMJ 1998;317:1341-1345 ( 14 November )

After adjusting for age, smoking, and other known risk factors for CHD:
Women consuming > five ounces of nuts a week (frequent consumption)
vs.
women who never ate nuts or who ate < one ounce a month (rare consumption)
had a significantly lower risk of total coronary heart disease (RR = 0.65, 95% confidence interval 0.47 to 0.89, P for trend=0.0009).

The magnitude of risk reduction was similar for both
fatal coronary heart disease (0.61, 0.35 to 1.05, P for trend=0.007)
& non-fatal MI (0.68, 0.47 to1.00, P for trend=0.04).
Further adjustment for intakes of dietary fats, fibre, vegetables, and fruits did not alter these results. The inverse association persisted in subgroups stratified by levels of smoking, use of alcohol, use of multivitamin and vitamin E supplements, body mass index, exercise, and intake of vegetables or fruits.

Key messages
Nuts are high in fat, but most of the fatty acids are unsaturated
This study suggests that frequent consumption of nuts, including peanuts, may reduce the risk of coronary heart disease
This protective effect may be partly mediated through serum lipids because unsaturated fats have benefical effects on serum lipids. Other potentially protective constituents include vegetable protein, magnesium, vitamin E, fibre, and potassium
Nuts can be included as part of a healthy diet

Lyon Diet Heart Study(de Lorgeril et al., Arch Int Med 158: 1181-1187)
• Randomized secondary prevention trial;• 605 patients with coronary artery disease
randomized to either a Meditarranean-type diet or control (A.H.A. Step 1-like) diet;
• After ~ 4 years of follow-up, Cox proportional hazards model was used to estimate risk ratios for cancer, total or cardiac death, combined total death, nonfatal cancer, and nonfatal MI.

Table 1: Number of Events and Risk Ratios
de Lorgeril et al. (1998) Arch. Int. Med. 158: 1181-1187.

Table 2: Characteristics of patients who developed cancer in the two groups

Figure 1: Cumulative survival without nonfatal cancer among patients in the experimental and control groups.

Figure 2: Cumulative survival without nonfatal cancer and recurrent acute MI among patients in the experimental and control groups.


Eat a variety of foods.
Choose most foods from plant sources.
Eat at least 5 servings of fruits and vegetables every day.
Eat at least 6 servings of whole grain foods each day.
Minimize the consumption of high-fat foods, especially those from animals.
Choose low-fat, low-cholesterol foods.
Limit the amount of simple sugars in the diet.