Embed Size (px)
Citation preview

13 Effect of Glucose Managementon Coronary Heart Disease Risk in
Downl
Patients with DiabetesKasia J. Lipska and Silvio E. Inzucchi
CHANGING EPIDEMIOLOGY OFDIABETES AND CORONARY HEARTDISEASE, 155
EPIDEMIOLOGIC RELATIONSHIP OFGLUCOSE WITH CORONARY HEARTDISEASE, 155
TRIALS OF GLUCOSE-LOWERINGINTERVENTIONS, 157
TRIALS OF GLUCOSE-LOWERINGINTERVENTIONS IN PREDIABETESAND EARLY DIABETES, 159
oaded for Aman Shah (a.shah.1@elsevFor personal use only. N
THE “HOW” OF GLUCOSELOWERING: THE EVIDENCE FORSPECIFIC MEDICATIONS ANDMEDICATION CLASSES, 161Metformin, 162Sulfonylureas, 163Thiazolidinediones, 163Insulin, 164Incretin-Based Therapies, 165Other Agents, 165
ier.com) at Elsevier - Demonstration Account from ClinicalKeyo other uses without permission. Copyright ©2017. Elsevier Inc
RISKS ASSOCIATED WITHANTIHYPERGLYCEMICMEDICATIONS, 167Hypoglycemia, 167Other Adverse Effects of
Medications, 168
IMPLICATIONS FOR CLINICALPRACTICE, 168
REFERENCES, 169
Coronary heart disease (CHD) is the most common vascularcomplication of diabetes. Because elevated glucose definesdiabetes and because diabetes is a well-recognized risk fac-tor for CHD, strategies that lower glucose should theoreti-cally reduce the risk of CHD events in diabetes. In reality,the relationship between glucose-lowering strategies andcardiovascular outcomes is complex and suggests that theimpact of interventions on patient outcomes cannot be eas-ily predicted from the effects of interventions on surrogatemeasures (such as glucose or hemoglobin A1c, HbA1c).Indeed, CHD can precede the development of diabetes,and some have suggested that both conditions (CHD anddiabetes) have common genetic and environmental rootsand spring from a “common soil” (Fig. 13-1) (see also Chap-ters 2, 8, and 9).1 This chapter describes the epidemiologicrelationship between glucose and CHD, reviews clinical trialevidence of the effects of glucose lowering on CHD out-comes, discusses the benefits and risks of glucose loweringwith specific medications and in specific patient popula-tions, and concludes with implications for clinical practice.
CHANGING EPIDEMIOLOGY OF DIABETESAND CORONARY HEART DISEASE
The general incidence and prevalence of CHD havedeclined in the United States in the last several decades,and this decline has been accompanied by a decline inCHD-related mortality.2 These trends have been attributedto better cardiovascular risk factor control and treatmentduring and after acute coronary syndromes over time, pri-marily with the use of statin medications, blood pressuremanagement, and anti-platelet therapies. In contrast toCHD trends, the incidence and prevalence of diabetes havebeen steadily increasing over time, with the disease nowaffecting close to a third of older U.S. adults (65 years orolder) (see also Chapter 1).3,4 In addition, adults with diabe-tes are living longer.5 As a result, the burden of CHD attrib-utable to diabetes is increasing (see also Chapter 7).6 These
changes in the epidemiology of diabetes and CHD haveimportant implications. First, strategies that mitigate the riskof CHD in diabetes patients will be of growing importancebecause heart disease is increasingly a complication of dia-betes. Second, these strategies will be applied to an agingpopulation with a high comorbidity burden and at higherrisk for adverse effects of therapy.
EPIDEMIOLOGIC RELATIONSHIP OF GLUCOSEWITH CORONARY HEART DISEASE
Multiple studies have assessed the relationship between var-ious glucose parameters—fasting glucose, 2-hour glucoseduring an oral glucose tolerance test, or HbA1c levels—and the risk of CHD in populations with and without diabe-tes. Most of this work suggests a continuous relationshipbetween measures of glycemia and CHD risk.
Several studies and a metaregression analysis have shownthat in nondiabetic populations, there is a graded relation-ship between initial fasting and postprandial glucose levelsand subsequent occurrence of cardiovascular events over12 years of follow-up.7 The association is apparent even atlevels below the diabetic thresholds. However, becauseHbA1c is the preferred test for monitoring blood glucosecontrol during the chronic management of diabetes, datasummarized here will be predominantly based on this glyce-mic parameter.
In the large prospective population study of Norfolk, in theUnited Kingdom, HbA1c and cardiovascular risk factorswere assessed from 1995 to 1997, and cardiovascular diseaseevents and mortality were examined during the next 6 to8 years of follow-up.8 The relationship between HbA1cand cardiovascular disease and total mortality was continu-ous and apparent even among persons without diabetes.The risk was lowest among persons with HbA1c below 5%and increased thereafter throughout the range of nondia-betic HbA1c levels up to 6.9%. Each one percentage pointincrease in HbA1c above 5% was associated with a 20% to
155.com by Elsevier on December 21, 2017.. All rights reserved.

HypertensionDyslipidemia
HyperglycemiaHyperinsulinemia
InflammationImpaired Fibrinolysis
Endothelial DysfunctionGenetic Predisposition
Insulin ResistanceInsulin ResistanceInsulin Resistance
DiabetesDiabetes CHDCHDDiabetes CHD
FIGURE 13-1 The “common soil” hypothesis of diabetes and coronary heart disease (CHD).
156
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
25% increase in the relative risk for CHD among men andwomen in age- and risk-factor adjusted models. Moreover,when known diabetes status and HbA1c concentration wereincluded in the same model, diabetes was no longer a signif-icant independent predictor of CHD, suggesting that theincreased risk of CHD in dysglycemic states is mediatedthrough hyperglycemia itself.
The prognostic value of HbA1c was also assessed in theAtherosclerosis Risk in Communities (ARIC) study of U.S.adults without a prior history of diabetes or cardiovasculardisease and with up to 15 years of follow-up.9 Similar tothe observations from the Norfolk study, the risk for CHDincreased with higher HbA1c values in a continuous fashionindependent of classic cardiovascular risk factors. Whencompared with study participants with HbA1c of 5% to lessthan 5.5% (the reference range), the hazard ratio (HR) forCHD was increased 23% in those with HbA1c of 5.5% to lessthan 6%, 78% for HbA1c of 6% to less than 6.5%, and 95% forHbA1c of 6.5% or higher. Although, clearly, the causal role ofglucose in the development of CHD could not be evaluatedin this epidemiologic study, the findings suggest that HbA1c,even in the nondiabetic range, can be a useful independentmarker of cardiovascular risk.
Although the association between HbA1c level and CHDmay be prognostically important in nondiabetic individuals,to understand the effect of glucose lowering on CHD risk wemust examine data in patients with diabetes. A prospectiveobservational study of type 2 diabetes patients enrolled inthe United Kingdom Prospective Diabetes Study (UKPDS)
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
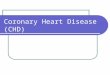
examined the relationship between HbA1c and cardiovas-cular complications. They found that each 1% increase inthe updated HbA1c was associated with a 14% relative riskincrease for myocardial infarction (MI; Fig. 13-2).10 A meta-analysis of 13 prospective cohort studies of HbA1c and car-diovascular disease in persons with diabetes (type 1 or 2)suggested that chronic hyperglycemia is associated withan increased risk for cardiovascular disease. The pooled rel-ative risk for cardiovascular disease associated with a 1%increase in HbA1c was 1.18. In a subgroup of six studies con-ducted in patients with type 2 diabetes, a 1% increase inHbA1c was associated with a 13% increased relative riskfor CHD.11 The inclusion criteria for the meta-analysis didnot specify pharmacologic treatment for diabetes; rather,these were observational studies involving patients on bothmedication and diet therapy. These results suggest a moder-ate increase in cardiovascular risk with increasing HbA1c indiabetic adults. However, the meta-analysis relied on smallstudies with some suggestion of heterogeneity of effects thatcould not be explored in detail.
One large analysis examined data from the U.K. GeneralPractice Research Database (GPRD) on 27,965 patients withtype 2 diabetes whose oral monotherapy was intensified tooral combination therapy, and 20,005 whose oral therapywas intensified to include insulin.12 The primary and second-ary outcomes for the two cohorts were all-cause mortalityand major cardiovascular events, respectively, over themean follow-up of 4.5 years. HbA1c in the study was basedon themean of any values recorded between the therapeutic
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

0
5 6 7 8
Updated mean hemoglobin A1c concentration (%)
9 10 11
80A
djus
ted
inci
denc
e of
myo
card
ial i
nfar
ctio
npe
r 10
00 p
erso
n-ye
ars
(%)
40
60
20
FIGURE 13-2 Epidemiologic relationship between hemoglobin A1c andcardiovascular events. (Modified from Stratton et al. BMJ 2000.10)
157
13EffectofGluco
seMan
agem
entonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
switch and death or date of censor. In combined cohortanalysis, the HbA1c decile with a median value of 7.5%(interquartile range 7.5% to 7.6%) was associated with thelowest mortality and the lowest progression to large-vesseldisease among those without prior history of cardiovascularevents. Higher and lower HbA1c values were associatedwith an increased risk, and the pattern of risk was U shaped.In the oral combination therapy group, a wider range ofHbA1c values was safe with respect to mortality risk (medianHbA1c 6.9% to 8.9%), whereas this range was narrower forpatients on insulin (median HbA1c 7.5% to 8.1%). In addi-tion, the use of insulin was associated with an approximately50% higher hazard of mortality comparedwith the use of oralagents. Although no evidence supports a direct cardiotoxiceffect of insulin in type 2 diabetes, it is certainly possible thatage, comorbidities, and diabetes duration may be related tothe decision to initiate insulin as well as to the higher mor-tality risk. The findings from this study differ significantlyfrom the graded, continuous epidemiologic relationshipsbetween HbA1c and cardiovascular outcomes in individ-uals without diabetes. In nondiabetic populations, lowerHbA1c values predict better outcomes without a clearthreshold, but the data from treated patients with diabetessuggest that there may be a risk associated with achievingnear-normal glycemia.Another retrospective cohort study, this time performed in
the United States, confirmed the results of the GPRD analysis.Here, data from 71,092 patients with type 2 diabetes age60 years or older within the Kaiser Permanente Northern Cal-ifornia system were analyzed to examine the associationbetween baseline HbA1c level and subsequent nonfatalcomplications (metabolic, microvascular, and cardiovascu-lar events) and mortality.13 The authors found a similarU-shaped relationship between HbA1c level and mortality,with higher risk in those with HbA1c below 6% and 10%
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
or higher in the adjusted models. In contrast, however, therelationship between HbA1c and cardiovascular eventswas continuous with increasing risk above HbA1c of 6%.Integrating all of the outcomes together, the “optimal”HbA1c range identified by this study lay somewhere in the6% to 7.9% range. As in the GPRD study, the analysis addedimportant information about optimal glycemic targets in dia-betes, suggesting that achievement of low glycemic levelsmay provide benefits (such as lower risk of CHD), but thatvery low levels of glycemia may be associated with harm(e.g., higher mortality risk). A third study, this involving alladults with type 2 diabetes drawn from the Kaiser Perma-nente Southern California system, showed a U-shaped rela-tionship between HbA1c and cardiovascular events, withHbA1c levels of 6% or lower and greater than 8% associatedwith an increased risk of cardiovascular events.14Whether ornot low HbA1c levels are a marker of sicker patients or amediator of harm remains highly debatable. Moreover,whether this phenomenon is actually directly attributableto lower than desirable glycemia or to adverse effects ofthe medications clinicians use to achieve this range is notclear. Randomized clinical trials can test the effects of inter-ventions directly on patient outcomes and may be able toprovide greater insight into the effect of glucose loweringon CHD events.
TRIALS OF GLUCOSE-LOWERINGINTERVENTIONS
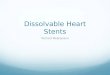
The landmark trial in type 2 diabetes that investigated theeffect of intensive glucose lowering on microvascular andmacrovascular outcomes was the UKPDS. The trial wasbegun in 1977 and the results were published in 1998. In thistrial, 3867 patients with newly diagnosed type 2 diabetes(median age 54) were randomized to intensive treatmentwith sulfonylureas (chlorpropamide, glibenclamide (glybur-ide in the U.S.), or glipizide) or with insulin, versus conven-tional therapy with diet alone.15 The median HbA1c level inthe intensive group during the course of the trial was 7%, ver-sus 7.9% in the conventional arm. Three separate aggregateendpoints were studied over the 10 years of follow-up. Therisk in the intensive group was 12% lower for any diabetes-related endpoint (P¼0.03), which included both macrovas-cular and microvascular events as well as metabolic compli-cations; not significantly lower for any diabetes-related death(�10%, P¼0.34); and not significantly lower for mortality(�6%, P¼0.44), compared with patients treated with dietonly. The reduction in diabetes-related endpoints was drivenby a 25% risk reduction in microvascular events, and thereduction in MI did not reach statistical significance(�16%, P¼0.052). A subgroup of UKPDS patients who wereoverweight (>120% ideal body weight) were randomizedeither to intensive therapy with metformin (n¼342, medianHbA1c 7.4%) or conventional diet therapy (n¼411, medianHbA1c 8%).16 In this subset of patients, treatment withmetformin was associated with a 32% reduction in anydiabetes-related endpoint (P¼0.002), 42% reduction indiabetes-related death (P¼0.017), and 36% reduction inmortality (P¼0.011). In this cohort of patients treatedwith metformin, there was a significant 39% reduction inMI (P¼0.01) (Fig. 13-3). In summary, the UKPDS trialestablished that intensive glucose control reduces the riskof microvascular complications in patients with newly
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

A
0
15
20
Inci
denc
e pe
r 10
00 p
atie
nt-y
ears
10
5
Conventionaldiet
Insulinor
Sulfonylurea
MYOCARDIAL INFARCTION
NS
39%reduction
50%reduction
P � 0.01
Metformin0
6
8
10
Inci
denc
e pe
r 10
00 p
atie
nt-y
ears
4
2
Conventionaldiet
CORONARY DEATHS
P � 0.02
Metformin
BFIGURE 13-3 Results of the UKPDS trial with respect to myocardial infarction and coronary deaths. NS¼Non significant. (Modified from Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes [UKPDS 34]. UK Prospective Diabetes Study [UKPDS] Group, Lancet 352:854, 1998).
158
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
diagnosed type 2 diabetes, but suggested that macrovascularbenefits may be confined to overweight patients treated withmetformin therapy.
After the UKPDS trial was completed, study participantsand their clinicians were advised to lower levels of blood glu-cose as much as possible, and patients returned to commu-nity or hospital-based diabetes care according to theirclinical needs without any attempts to maintain previouslyrandomized therapies. In the 10-year post-trial monitoringstudy of patients who survived to the end of the UKDPS trial,HbA1c levels were no longer different between theoriginal intensive and conventional arms (approximately8% at the end of the post-trial monitoring period).17 In thesulfonylurea-insulin group, relative risk reductions fordiabetes-related endpoints persisted, whereas significant riskreductions for MI (15%, P¼0.010) and mortality (13%,P¼0.007) emerged over time. In the metformin group, rela-tive risk reductions persisted for any diabetes-related end-point, MI (33%, P¼0.005), and mortality (27%, P¼0.002).These observations suggest a modest but sustained effect ofintensiveglucose loweringoncardiovascular events,butonlyafter many years of follow-up. Whether the effect is confinedto patientswith newly diagnosed type 2 diabetes orwhether itreflects the long period of time required to significantly affectsubsequent atherosclerotic outcomes is not entirely clear.
Even before the cardiovascular benefits of intensive glu-cose therapy emerged in the long-term follow-up of theUKPDS trial, guidelines recommended a target HbA1c levelof 7% or less in most patients. This was primarily driven bythe expectation of microvascular benefits, albeit with uncer-tainty over the effects on macrovascular events. To settle thequestions about the role of intensive glucose therapy in type2 diabetes, three randomized controlled trials were specifi-cally designed to examine the impact of targeting near-normal glycemia on cardiovascular risk. The HbA1c targetswere set low because of the continuous epidemiologic rela-tionship of glucose with cardiovascular risk, suggesting thatperhaps much lower glucose levels need to be achieved fora significant benefit to emerge. The three trials all recruited
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
participants with type 2 diabetes who had either a history ofor multiple risk factors for cardiovascular disease, thusensuring adequate event rates to study the effects of the inter-ventions. Participants were therefore quite distinct frompatients in the UKPDS trial—they were older, had a longerduration of diabetes, and had a greater comorbidity burden.
The Action to Control Cardiovascular Risk in Diabetes(ACCORD) trial enrolled 10,251 patients (mean age 62,median baseline HbA1c 8.1%, 35% with history of prior car-diovascular event) to intensive glucose therapy (targetingHbA1c <6%, median achieved HbA1c 6.4%) versus con-ventional therapy (targeting HbA1c 7% to 7.9%, medianachieved HbA1c 7.5%).18 This trial was stopped prematurelyafter a mean follow-up of 3.5 years because of a higher mor-tality rate in the intensive therapy group compared with thecontrol arm (HR 1.22, P¼0.04). The primary endpoint of thetrial, major cardiovascular events, was not significantlyreduced (HR 0.90, P¼0.16), although the rate of nonfatalMI was lower in the intensive therapy group (HR 0.76,P¼0.004). To date, analyses have not identified any clearexplanation for the higher mortality risk associated withthe intensive glucose-lowering strategy. In the intensive ther-apy group, a median HbA1c level of 6.4% was rapidlyachieved andmaintained, but subsequent post hoc analysesimplicated factors associated with persistently higherHbA1c, rather than low HbA1c, as likely contributors tothe increased mortality risk.19 In addition, rates of serioushypoglycemia requiring medical assistance were threefoldhigher in the intensive group than during standard therapy(10.5% versus 3.5%, P<0.001). Subsequent retrospective epi-demiologic analyses of ACCORD have suggested, however,that severe hypoglycemia may not, in fact, account for thedifference in mortality between the two study arms.20
Although hypoglycemia was associated with increased mor-tality within each randomized group, the risk of death wasactually lower in participants experiencing hypoglycemiain the intensive arm than in participants with hypoglycemiain the standard arm. Other explanations, such as the partic-ular medication combinations or undetected medication
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

159
13EffectofGluco
seMan
agem
entonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
interactions, have also been proposed, but no particularmedication class has been implicated thus far. In the end,the explanation for the increased mortality may never beknown, but the findings have led to a growing recognitionthat intensive glucose loweringmay be associatedwith somebenefits but also important risks.Subsequent follow-up of the participants from the
ACCORD trial, up to the originally planned 5 years, showedpersistently increased mortality rates in the intensive therapygroup (HR 1.19, P¼0.02), but still lower rates of nonfatal MI(HR 0.82, P¼0.01).21 Given these findings, strategies used inthe ACCORD study targeting an HbA1c below 6% are notrecommended for patients with advanced type 2 diabetesand established macrovascular complications or multiplerisk factors for cardiovascular events.At the same time the ACCORD study was published,
results from the Action in Diabetes and Vascular Disease:Preterax and Diamicron Modified Release Controlled Evalu-ation (ADVANCE) trial also became available.22 In this trial,11,140 patients with type 2 diabetes (mean age 66, medianbaseline HbA1c 7.2%, 32%with history of major macrovascu-lar disease) were randomized to intensive therapy (preferen-tially with the sulfonylurea gliclazide, targeting HbA1c�6.5%, with mean achieved HbA1c 6.5%) or to standardtherapy (HbA1c goal according to local guidelines, meanachieved HbA1c 7.3%). After a median follow-up of 5 years,there was a reduction in the primary outcome of the study,which was a composite of microvascular andmacrovascularevents (HR 0.90, P¼0.01), and this was almost entirelydriven by effects on intermediate markers of nephropathy.There was no significant effect with respect to major cardio-vascular events (HR 0.94, P¼0.32) in ADVANCE, but also noincrease in mortality (HR 0.93, P¼0.28) as in ACCORD.Investigators of ADVANCE specifically examined varioussubgroups at potentially increased risk of death, but nonewere identified. Overall, the trial findings suggest a modestimprovement in markers of microvascular complicationswith intensive treatment, but no significant benefit gainedwith respect to CHD endpoints.One additional trial confirmed the lack of significant ben-
efit of intensive glucose lowering on major cardiovascularevents, the Veterans Affairs Diabetes Trial (VADT). In thisstudy of 1791 U.S. military veterans with type 2 diabetes(mean age 60, median baseline HbA1c 9.4%, 40% with priorhistory of cardiovascular events), participants were random-ized to intensive glucose or standard therapy using a combi-nation of agents, with a goal of achieving an absolutereduction in HbA1c of 1.5% in the intensive versus the stan-dard arm. Median HbA1c levels achieved were 6.9% versus8.4% in the intensive and standard groups, respectively, overa median follow-up of 5.6 years. There was no significantbenefit with respect to the primary composite outcome, ofcardiovascular events (HR 0.88, P¼0.14), the individual out-come of death from any cause, nor any difference withrespect to most microvascular complications (no changesin retinopathy, new neuropathy, or doubling of creatinine,but reduction in some albuminuria-based endpoints). In thisstudy of patients with advanced type 2 diabetes, other car-diovascular risk factors were well controlled, and differ-ences in HbA1c levels between the two groups weremaintained. However, overall, the benefit of decreasingHbA1c from 8.4% to 6.9% was minimal, except in the pro-gression of albuminuria, an intermediate marker with uncer-tain implications for long-term renal risk.
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
Multiple meta-analyses have followed the three random-ized controlled trials described earlier to determine whetherpooling results of existing studies will illuminate our under-standing of these relationships (Fig. 13-4). Although theseanalyses sometimes included studies of different intent(not necessarily glucose-lowering per se) and with variablepatient characteristics (newly diagnosed versus advanceddiabetic patients), they consistently show a modest,although significant, reduction of approximately 15% inthe risk for nonfatal MI, but no impact on mortality or cardio-vascular death.23–28 Moreover, all of these studies show thatthe risk for severe hypoglycemia with intensive glucose ther-apy is more than doubled.
Why have these large randomized controlled trials failedto show that intensive glucose lowering improves cardiovas-cular outcomes when the epidemiologic relationshipbetween glycemia and cardiovascular events is so convinc-ing? Many of the expectations for reduction in risk may havearisen from the effects of statin medications on majoradverse cardiovascular events (MACEs) in early trials. Astrong epidemiologic association between cholesterol andCHD exists, and interventional studies show a 23% relativereduction in risk achieved for every 1 mmol/L (38 mg/dL)of cholesterol lowering. Glycemia is a much weaker risk fac-tor for CHD than cholesterol, but the assumption has beenthat some degree of risk reduction should result from glu-cose lowering. However, it is clear that the simple arithmetic(lower the level of a risk factor and cardiovascular eventswill naturally follow) does not apply in the case of glycemia.There may be a modest reduction in nonfatal MI, but overalldisappointing results with respect to mortality and the com-posite of major cardiovascular events. Several potentialexplanations can be proposed: significant adverse effectsof glucose therapy may counterbalance possible benefits,effects of glucose lowering applied in advanced diabetesmay be too late to prevent atherosclerotic events, or theimpact of glucose lowering may take a longer time to mate-rialize than the 5 to 7 years assessed in most clinical trials.Regardless of the reasons, currently available therapiestested in these studies do not appear to constitute a “magicbullet” for the increased cardiovascular morbidity ofdiabetes.
TRIALS OF GLUCOSE-LOWERINGINTERVENTIONS IN PREDIABETES AND EARLYDIABETES
Because one potential reason for the lack of benefit of inten-sive glucose lowering on cardiovascular disease is that it isapplied too late to prevent atherosclerosis, it is worthwhileto examine studies that have investigated glucose loweringbefore diabetes actually develops or very early in the diseasecourse.
One such study was the Diabetes Prevention Program thatrandomly assigned 3234 nondiabetic persons at high risk fordiabetes (with elevated body mass index and fasting andpostload glucose values) to intensive lifestyle therapy, met-formin monotherapy, or placebo.29 Lifestyle interventionand metformin both significantly reduced the incidence ofsubsequent diabetes. In follow-up studies of the trial popula-tion, the lifestyle intervention also improved cardiovascularrisk factors compared with metformin or placebo treatment,but the number of cardiovascular events was too small
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

0.5 1.0
Relative risk (95% CI)
2.0
Early trialsUKPDS 33 564/2729 259/1138
Trial
Primary Composite Cardiovascular Outcome
Intensive
Events/Total, n/ N
Conventional
UKPDS 34 57/342 105/411
Subtotal 621/3071 364/1549
Recent trials
ACCORD 352/5128 371/5123
ADVANCE 557/5571 590/5569
VADT 113/892 131/899
Subtotal 1022/11,591
A
B
1092/11,591
Total 1643/14,662 1456/13,140
(95% CI) (95% CI)
Relative risk ratio Risk difference
0.79 (0.57 to 1.09) �25 (�56 to 5)
0.94 (0.86 to 1.02) �7 (�12 to �2)
0.90 (0.83 to 0.98) �15 (�24 to �5)
Heterogeneity P � 0.20; I 2 � 33.3%
0.5 1.0
Relative risk (95% CI)
2.0
Early trialsUKPDS 33 276/2729 126/1138
Trial
Cardiovascular Mortality
Intensive
Events/Total, n/ N
Conventional
UKPDS 34 25/342 53/411
Subtotal 301/3071 179/1549
Recent trials
ACCORD 135/5128 94/5123
ADVANCE 253/5571 289/5569
VADT 40/892 33/899
Subtotal 528/11,591 416/11,591
Total 729/14,662 595/13,140
(95% CI) (95% CI)
Relative risk ratio Risk difference
0.75 (0.48 to 1.19) �15 (�36 to 6)
0.13 (0.79 to 1.63) 4 (�9 to 17)
0.97 (0.76 to 1.24) �3 (�14 to 7)
Heterogeneity P � 0.002; I 2 � 76.3%
FIGURE 13-4 Relative risk and risk differences estimates (per 1000 patients over 5 years of treatment), with 95% confidence intervals (CI), for the main studyoutcomes in the UKPDS, ACCORD, ADVANCE, and VADT. A, Primary composite cardiovascular outcome. B, Cardiovascular mortality. (Modified from Kelly TN, BazzanoLA, Fonseca VA, et al. Systematic review: glucose control and cardiovascular disease in type 2 diabetes, Ann Intern Med 151:394-403, 2009.)
160
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
(n¼89 at 3 years) to allow any meaningful examination ofthe differences among groups.30 After 10 years of follow-upof the Diabetes Prevention Program, the cumulative inci-dence of diabetes was still lowest in the former lifestyle inter-vention group.31 Cardiovascular disease risk factorsimproved in all three treatment groups, but averaged over
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
all follow-up, systolic and diastolic blood pressure and tri-glyceride levels were lower in the lifestyle than in the othergroups (even though the use of antihypertensive medica-tions was less frequent). However, the number of clinicalevents remained too small to determine the effect of diabe-tes prevention strategies on actual cardiovascular events.
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

161
13EffectofGluco
seMan
agem
entonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
In the Study to Prevent Non–Insulin-Dependent DiabetesMellitus (STOP-NIDDM), investigators examined the effectof postprandial glucose lowering on the incidence of diabe-tes in 1429 participants with impaired glucose tolerance, ele-vated fasting glucose, and overweight or obesity.32 As asecondary outcome, investigators specifically examinedthe effect of intervention on major cardiovascular eventsand hypertension, although the trial was not adequatelypowered to answer that question. The participants were ran-domized to receive either acarbose or placebo and were fol-lowed for a mean of 3.3 years. In the course of the trial,almost one quarter of participants discontinued participa-tion prematurely (including significantly greater numbersrandomized to acarbose). Moreover, concerns about incon-sistencies, failure to follow intention-to-treat analysis, andchanges in the trial endpoints have been raised. Neverthe-less, the trial reported an unanticipated 49% relative riskreduction (P¼0.03) in major cardiovascular events (includ-ing revascularization procedures, congestive heart failure,and peripheral vascular disease in addition to the conven-tional major cardiovascular events) associated with acar-bose therapy. This composite endpoint was primarilydriven by an incredible 91% reduction in MI (P¼0.02).Clearly, these trial findings will need to be confirmed infuture studies before acarbose therapy can be recom-mended for cardiovascular risk reduction. One such trial,the Acarbose Cardiovascular Evaluation (ACE) study, is cur-rently ongoing and testing the impact of acarbose on cardio-vascular outcomes in persons with impaired glucosetolerance and established cardiovascular disease or acutecoronary syndromes.Encouraged by the STOP-NIDDM results, investigators of
the Nateglinide and Valsartan in Impaired Glucose Toler-ance Outcomes Research (NAVIGATOR) trial decided to testan alternative postprandial glucose-lowering approach witha short-acting insulin secretagogue, nateglinide, in additionto lifestyle modification. They randomized 9306 persons(mean age 64) with impaired glucose tolerance (baselineHbA1c 5.8%) at high risk for cardiovascular disease (24%had a prior history of cardiovascular events) to nateglinideor placebo and followed participants for amedian of 5 years.Nateglinide did not reduce the occurrence of the three co-primary outcomes—incident diabetes (HR 1.07, P¼0.05),cardiovascular outcome (death from cardiovascular causes,nonfatal MI, nonfatal stroke, or hospitalization for heart fail-ure, HR 0.94, P¼0.43), or the extended cardiovascular out-come (which in addition included unstable angina orarterial revascularization, HR 0.93, P¼0.16). The trial resultscontrast sharply with the findings of the STOP-NIDDM studyand show that targeting postprandial hyperglycemia withnateglinide in participants with impaired glucose tolerancedoes not lead to cardiovascular benefits.Another potential approach is to test whether early provi-
sion of basal insulin to normalize fasting plasma glucosemay reduce cardiovascular outcomes in persons with mildlyelevated glucose levels or early diabetes. This strategy doesnot specifically target postprandial hyperglycemia, butrather postulates that insulin, which has been demonstratedto have anti-inflammatory effects, may actually be cardiopro-tective and that it may also preserve pancreatic beta cellfunction over time. The Outcome Reduction with Initial Glar-gine Intervention (ORIGIN) trial randomized 12,537 people(mean age 64; 82% with early diabetes, 6% with new diabe-tes, and 12% with impaired fasting glucose or impaired
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
glucose tolerance; median baseline HbA1c 6.4%; 59% withprior cardiovascular disease) to insulin glargine or standardcare.33 The target in the insulin group was to achieve a fast-ing glucose level of 95 mg/dL or lower. After amedian 6 yearsof follow-up, HbA1c levels were 6.2% versus 6.5% in the insu-lin and standard arms, respectively. The trial found no signif-icant reduction in two co-primary outcomes, majorcardiovascular events (HR 1.02, P¼0.63) and major cardio-vascular events plus revascularization and heart failure (HR1.04, P¼0.27). However, there was an increased risk of hypo-glycemia with insulin therapy and some weight gain (+1.6 kgversus �0.5 kg in the two groups). Although diabetes inci-dence was decreased (a finding of questionable clinicalapplication), the trial findings were generally disappointing.The ORIGIN trial did not support the original hypothesis thatnormalizing glucose with early insulin therapy would lead tobetter cardiovascular outcomes.
These studies illustrate the impact of glucose loweringwith a variety of different approaches in persons with predi-abetes or early diabetes on cardiovascular outcomes. Withthe exception of the STOP-NIDDM study, which had impor-tant limitations, the studies to date have not supported thenotion that glucose lowering is beneficial for cardiovascularoutcomes at the prediabetic stage. Despite the epidemio-logic association of glucose with cardiovascular events thatextends well into the nondiabetic range, interventions target-ing glycemia have thus far failed to deliver an effective strat-egy to reduce this risk.
THE “HOW” OF GLUCOSE LOWERING: THEEVIDENCE FOR SPECIFIC MEDICATIONS ANDMEDICATION CLASSES
Perhaps one of the most important lessons in cardiovascularrisk reduction in type 2 diabetes has been the growing rec-ognition that the exact strategy used to reduce glucosemay actually matter with respect to outcomes. For severaldecades now, the thrust of clinical research has been to testapproaches that target specific degrees of glucose lowering.Less attention was previously paid to the different ways inwhich glycemia is actually improved and how that mayaffect downstream events. The early UKPDS experience,albeit based on a small subgroup (n¼342) of patients,has given metformin a preferred place in the diabetic regi-men for type 2 diabetes. In most subsequent trials (ACCORD,ADVANCE, VADT), combinations of various medications,including insulin use, had to be used to lower glucose levels,and there was no particular advantage to one strategy versusanother. However, these glucose-lowering trials were notdesigned to test the effects of specific medications onoutcomes.
Interest in the effects of specific antihyperglycemic medi-cations on outcomes was boosted by the publication of ameta-analysis by Nissen and colleagues in 2007 that showedan adverse effect of the thiazolidinedione rosiglitazone onMI risk.34 In the analysis of 42 trials that was performed, therewere 86 MI events in the rosiglitazone group compared with71 in the comparator arm (including placebo, metformin,sulfonylurea, or insulin), resulting in an increased odds ratioof 1.43 (P¼0.03). Although the methodology and the resultsof this meta-analysis have been debated, and some havenoted no increase in risk associated with rosiglitazoneuse,35,36 there is no doubt that the study provided a
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

TABLE 13-1 Major Randomized Controlled Trials inType 2 Diabetes
UKPDS ACCORD ADVANCE VADT
Study Participants
Mean age, yearsDiabetes duration,
yearsPrior
macrovasculardisease
53NewExcluded*
621035%
66832%
6011.540%
Duration of Study
Number of years 11 3.5 5 5.6
HbA1c Goal
Intensive therapyStandard therapy
†
{<6%7%-7.9%
�6.5%Standard
<6%8%-9%
HbA1c Achieved
Intensive therapyStandard therapy
7.0%7.9%
6.4%7.5%
6.4%7.0%
6.9%8.5%
Severe Hypoglycemia
Annual events per100 patients
Intensive therapyStandard therapyP value
0.710.20Not
reported
4.61.5<0.001
0.560.30<0.001
12.04.0<0.001
Primary Outcome}
HR (95% CI) forintensive versusstandardtherapy
0.88(0.79-0.99)
0.90(0.78-1.04)
0.90(0.82-0.98)
0.88(0.74-1.05)
All-Cause Mortality
HR (95% CI) forintensive versusstandardtherapy
0.94(0.80-1.10)
1.22(1.01-1.46)
0.93 (0.83-1.06)
1.07(0.81-1.42)
Cardiovascular Mortality
HR (95% CI) forintensive versusstandardtherapy
0.94(0.66-1.30)
1.35(1.04-1.76)
0.88 (0.74-1.04)
1.32(0.81-2.14)
HR¼Hazard ratio; CI¼confidence intervalBolded results represent HR reaching statistical significance, P<0.05.*Excluded myocardial infarction (MI) within 1 year prior, heart failure, angina, or
more than one vascular event.†Based on fasting plasma glucose (FPG) <108 mg/dL.{Based on FPG <270 mg/dL.}An aggregate endpoint of any diabetes-related endpoint (UKPDS); a composite of
nonfatal myocardial infarction, nonfatal stroke, and fatal myocardial infarction andstroke (ACCORD); combined microvascular and macrovascular disease (ADVANCE);and time to occurrence of a composite of major cardiovascular events (VADT).(Data from Ismail-Beigi F, Moghissi E, Tiktin M, et al. Individualizing glycemic targets intype 2 diabetes mellitus: Implications of recent clinical trials, Ann Intern Med 154:554–559, 2011.)
162
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
cautionary tale for glucose lowering. Most important, thestudy suggested that even though a medication may reduceglucose levels, and thus appear to treat diabetes effectively,it may in fact increase the risk of clinical events that are thetarget of glucose lowering in the first place. After the rosigli-tazone experience, however, the U.S. Food and Drug Admin-istration (FDA) mandated that glucose-loweringmedications must have data that support their safety withrespect to cardiovascular events before they are approvedfor use in diabetes.37
Despite the intense interest in the specific effects of med-ication classes (and individual agents) that followed, there isa paucity of data to guide choice of therapy in diabetes withrespect to long-term outcomes. Indeed, a recent compara-tive effectiveness analysis of 140 trials and 26 observationalstudies of medications for type 2 diabetes concluded thatevidence on long-term clinical outcomes, including mortal-ity, cardiovascular disease, nephropathy, and neuropathy,was of low strength and insufficient.38 Evidence supportedmetformin as a first-line agent in treatment of diabetes, butthis evidence was primarily based on its efficacy to lowerHbA1c levels, safety, adverse effect profile, and cost. Weshall now review the available evidence for themajor classesof antihyperglycemic therapy. These results are summarizedin Table 13-1.
MetforminMetformin, which works primarily by reducing hepatic glu-cose production, remains the first-line agent in the treatmentof type 2 diabetes because it effectively reduces HbA1c levels,is weight-neutral, and does not lead to hypoglycemia whenused as monotherapy. It is also inexpensive, has a favorablesafety profile, and may have potential benefit with respect tocardiovascular disease, based on the UKPDS substudy.16
Despite the many advantages of metformin, data withrespect to cardiovascular risk reduction with metformin arenot entirely consistent. In addition to the UKPDS substudy,16
only one prior randomized controlled trial was conducted onthis subject. In the trial, 390 patients treated with insulin wererandomized to receive either metformin or placebo as add-ontherapy.39 The primary endpoint, an aggregate of microvascu-lar and macrovascular outcomes, did not differ between thetwo groups after 4.3 years of follow-up (HR 0.92, P¼0.33), butthere was a significant reduction in the secondary endpoint ofmacrovascular events (HR 0.60, P¼0.04). In addition, metfor-min usewas associatedwith beneficial effects on bodyweightand insulin requirements.
In observational studies, metformin use (either as mono-therapy or in combination with another oral agent) hasbeen associated with reduced mortality,40–42 cardiovasculardeaths,40 and cardiovascular events.41–43 Because metfor-min is generally the preferred initial agent for diabetes treat-ment and remains contraindicated in patients withadvanced chronic kidney disease, patients who are not trea-ted with this medication in an observational study may differin important ways from those who are. These analyses eitheradjusted for potential confounders ormatched patient popu-lations for the propensity to be prescribed metformin versusanother medication (usually a sulfonylurea). However,these investigations were observational in nature, so unmea-sured factors may potentially still have contributed to the dif-ferences in outcomes.
Alongside the evidence that supports the safety and effec-tiveness of metformin, there are data that provide a less
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
reassuring picture. Although the UKPDS substudy showedbenefits of metformin in overweight participants, the trialalso reported an increased death rate in nonoverweightpatients who took metformin and a sulfonylurea comparedwith those who took a sulfonylurea alone (relative risk 1.60,P¼0.04).16 Combined analysis of the two UKPDS studies didnot reveal an increased risk for mortality in patients treatedwith this combination, and the increased mortality in theUKPDS substudy has not been fully explained. In a subse-quent meta-analysis of 13 randomized controlled trialsinvolving more than 13,000 type 2 diabetes patients, com-pared with other treatments, metformin therapy had no sig-nificant effect on the risk for mortality (relative risk 0.99 withwide 95% confidence intervals that could not exclude a 25%
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

163
13EffectofGluco
seMan
agem
reduction or 31% increase in risk), cardiovascular mortality(relative risk 1.05), or rates of MI (relative risk 0.90 with 95%confidence intervals that could not exclude 26% risk reduc-tion or 9% harm).23 Similar findings were reported in a meta-analysis that specifically examined the effects of metforminwith insulin compared with insulin alone in 23 trials withover 2000 participants.44 The study found that metforminadded to insulin did not significantly change mortality risk(relative risk 1.30, with 95% confidence intervals 0.57 to2.99) or cardiovascular mortality risk (relative risk 1.70, with95% confidence intervals 0.35 to 8.30) but provided littlereassurance with regard to each of these endpoints giventhe wide confidence intervals.
entonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
SulfonylureasSulfonylureas, insulin secretagogues, are the oldest oral agentclass for treatment of hyperglycemia. Whereas sulfonylureasare effective at glucose lowering, they increase the risk ofhypoglycemia, are associated with a modest weight gain,and likely result in less durable effects on glucose controlcompared with metformin or thiazolidinediones.45
Questions about cardiovascular safety of sulfonylureasdate back to 1970 when the University Group DiabetesProgram (UGDP) trial reported an increased risk for cardio-vascular death associated with the use of tolbutamide com-pared with placebo or insulin.46 Subsequently the FDAmandated a boxed warning for all sulfonylureas. Sulfonyl-ureas inhibit the adenosine triphosphate (ATP)–dependentpotassium channels that are present within cardiomyocytesand coronary vascular endothelial cells, and it has been pos-tulated that the presence of sulfonylureas at the time of anacute coronary event prevents adequate coronary vasodila-tion and thus may result in a larger area of myocardial dam-age. However, the risk of cardiovascular death noted by theUGDP group was not supported by the subsequent UKPDSstudy, which showed no difference in cardiovascular riskbetween the use of sulfonylureas (chlorpropamide, gliben-clamide, or glipizide) or insulin therapy15 (but a benefit withthe use of metformin, as noted earlier16). The large A Diabe-tes Outcome Prevention Trial (ADOPT) study comparedmetformin, rosiglitazone, or glyburide therapy with respectto glycemic control, but again found no difference withrespect to cardiovascular events (which were not frequentand were collected as adverse events during the trial) acrossthe treatment groups after 4 years of treatment.45 Finally, theADVANCE study of intensive glucose lowering primarilyused gliclazide in its intensive glucose control arm andfound no risk associated with this strategy.22
Subsequent observational studies have, however, mostlysuggested harmwith sulfonylurea treatment, especially com-pared with metformin therapy.40,41,47,48 Whether sulfonyl-ureas are associated with adverse effects or metforminis protective remains debatable. Sulfonylureas are stillconsidered a viable option for second-line therapy in diabe-tes, primarily based on their effectiveness in loweringglucose and extensive accrued experience with the use ofthese agents.
ThiazolidinedionesThiazolidinediones, which lower glucose by activatingthe nuclear transcription factor peroxisome proliferator-activated receptor gamma (PPAR-γ), are insulin sensitizers.
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
They do not increase the risk of hypoglycemia and mayresult in more durable blood glucose control than sulfonyl-ureas or metformin.45 Although these agents improve manyintermediate markers of cardiovascular risk (e.g., C-reactiveprotein and markers of endothelial function), they areassociated with substantial weight gain, lower-extremityedema, heart failure, bone fractures, and possibly bladdercancer risk.
Rosiglitazone, but not pioglitazone, has actually beenassociated with an increased risk of MI,34 which led to itsrestricted use in diabetes. Therefore the two members ofthe thiazolidinediones class need to be considered sepa-rately if their individual risks and benefits are to be under-stood. It is worth noting that most analyses of the effects ofglucose-lowering therapies on clinical outcomes grouptogether medications of the same class and perform class-based comparisons. This practice is based on the assump-tion that medications in the same class have a similar modeof action and therefore will have a similar effect on clinicaloutcomes. The experience with rosiglitazone and pioglita-zone, both members of the thiazolidinedione class, suggestthat individual medications within the same class can affectclinical outcomes in different ways.
As already mentioned, the effect of rosiglitazone on car-diovascular events was analyzed in a highly publicizedmeta-analysis, which showed an increased risk of MI associ-ated with its use.34 Several other meta-analyses confirmedadverse effects associated with rosiglitazone,49,50 but notall found harm.35,36 However, observational studies compar-ing rosiglitazone with other oral diabetes medications51 orwith pioglitazone52–54 have consistently shown increasedrisk of mortality and heart failure with rosiglitazone use.The only trial specifically designed to evaluate cardiovascu-lar outcomes associated with rosiglitazone was the Rosiglita-zone Evaluated for Cardiovascular Outcomes in Oral AgentCombination Therapy for Type 2 Diabetes (RECORD)study.55 RECORD randomized 4447 diabetes patients withinadequately controlled hyperglycemia treated with metfor-min or sulfonylurea monotherapy to receive, in addition, asulfonylurea, metformin, or rosiglitazone. In the final analy-sis of the trial, there was no difference in the primary end-point (cardiovascular hospitalization or cardiovasculardeath) among the groups, but the event rate was lower thanexpected and the dropout rate in the trial was high, decreas-ing the power to detect significant differences in outcomes.Notably, the risk of heart failure was increased approxi-mately twofold with rosiglitazone.
Finally, in the Bypass Angioplasty Revascularization Inves-tigation 2 Diabetes (BARI 2D) trial, 2368 patients with type 2diabetes and obstructive coronary artery disease were facto-rially randomized to a) medical therapy with insulin provi-sion [insulin or sulfonylurea] versus insulin sensitization[metformin or rosiglitazone]); and b) randomized to medi-cal treatment versus coronary revascularization (a prioridetermined to be percutaneous coronary intervention[PCI] or coronary artery bypass grafting [CABG]), evaluatingthe effects on death and major cardiovascular events.56 Therewas no difference in the rates of death and cardiovascularevents between patients undergoing revascularization ormedical therapy, or between strategies of insulin provisionand insulin sensitization. However, in the CABG stratum, riskof major cardiovascular events was significantly lower withrevascularization and insulin sensitization (18.7%) comparedwith insulin sensitization therapy alone (32%, P¼0.002).
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

25
20
15
10
5
00 6 1812 24 30 36
2,488 2,373 2,2182,302 2,146 3482,530 2,413 2,2152,317 2,122 345
Time from randomization (months)
A
B
0.15
Kaplan-Meier event rate N events: 3-year estimate:
Placebo 358/2,633 14.4%Pioglitazone 301/2,605 12.3%
0.10
0.05
0.0N at risk:
0 6 1812 24
Pioglitazonevs placebo
0.841 0.722, 0.981 0.0273
HR 95% CI P value
30 36
5,238 5,102 4,8774,991 4,752 4,651 786 (256)
Time from randomization (months)
Pro
port
ion
of e
vent
s (%
)
Pioglitazone (514 events)Placebo (572 events)
HR=0·90 (95% CI 0·80–1·02)p=0·095
Numbers at riskPioglitazone
Placebo
FIGURE 13-5 PROactive study. Time to primary composite endpoint (all-causemortality, nonfatal myocardial infarction, stroke, acute coronary syndrome,revascularization, and above-knee amputation) and time to secondary endpoint(major cardiovascular events).
164
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
Because rosiglitazone was the primary thiazolidinedioneused for insulin sensitization, there did not appear to be harmassociated with its use in the setting of this trial. However, thetrial was not designed to specifically address rosiglitazone’ssafety.
Given the weight of the evidence, in 2011 the FDA placedrestrictions on prescription and use of rosiglitazone-containing medications through a Risk Evaluation and Miti-gation Strategy (REMS).57 The use of rosiglitazone was lim-ited to patients already successfully treated with thismedication, or patients whose blood glucose levels couldnot be controlled with other antihyperglycemia medicinesand who did not wish to use pioglitazone instead. In June2013, the FDA reviewed readjudicated data from theRECORD trial and concluded that the trial had not foundan elevated risk of MI or death associated with rosiglitazone.Therefore in November 2013 the FDA lifted its earlier restric-tions on rosiglitazone use. Given the highly publicizeddebates over the safety of rosiglitazone, it is unclear if thismedication will ever become widely used again in patientswith type 2 diabetes.
In contrast to rosiglitazone, data with pioglitazone appearto be more reassuring with respect to cardiovascular out-comes.48,52–54,58 The largest completed trial investigatingeffects of pioglitazone on cardiovascular outcomes wasthe Prospective Pioglitazone Clinical Trial in MacrovascularEvents (PROactive) study, in which 5238 patients with type 2diabetes and established macrovascular disease receivedpioglitazone or placebo, added to their baseline diabetestherapy.59 After an average follow up of 2.9 years, therewas a 10% relative risk reduction in the primary endpoint(including all-cause mortality, nonfatal MI, stroke, acute cor-onary syndrome, revascularization, and above-knee amputa-tion), but this did not reach statistical significance(P¼0.095) (Fig. 13-5). The secondary, and more conven-tional, outcome of major cardiovascular events was signifi-cantly decreased with pioglitazone (HR 0.84, P¼0.03).Concerns have been raised about the late definition of thesecondary endpoint after the trial was under way, the largenumber of secondary endpoints (more than eight), and theincreased risk of heart failure in the intervention group (16%versus 11.5%), which may have, over time, negativelyaffected study results.
In summary, the cardiovascular benefits of thiazolidine-diones are not entirely clear. The association of rosiglitazonewith MI, heart failure, and mortality is concerning, and mostguidelines recommend against the use of rosiglitazone forthose reasons. The potential benefits of pioglitazone in thePROactive study must be weighed against the increased riskof heart failure and fractures.
InsulinAs type 2 diabetes progresses, beta cell function declinesand the effectiveness of oral agents for glucose controldiminishes. However, endogenous insulin secretion is notentirely lost in type 2 diabetes, and strategies for insulinuse can be less complex than those used in the treatmentof type 1 diabetes. The main side effects of insulin use areweight gain and hypoglycemia. Given that insulin has beenused in clinical practice for decades and is a naturally occur-ring peptide hormone, fewer concerns have been previouslyraised about its cardiovascular safety. However, insulin mayobviously induce hypoglycemia, whichmay in turn promote
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
adrenergic discharges and arrhythmia, promotes fluid reten-tion, and may result in hypokalemia (especially whenadministered intravenously) as a result of potassium shiftsfrom the extracellular to intracellular space. Recent con-cerns about the cardiovascular safety of insulin use in type2 diabetes have been raised.60 These concerns are primarilybased on observational studies that show an increased riskof mortality, cardiovascular mortality, and cardiovascularevents in diabetes patients treated with insulin comparedwith other agents.12,61–63 In one such recent analysis, dataon over 84,000 patients with type 2 diabetes in the GPRDwere used to determine the risk of the primary outcome (firstmajor adverse cardiac event, first cancer, or mortality) asso-ciated with five different glucose-lowering regimens (metfor-min monotherapy, sulfonylurea monotherapy, insulinmonotherapy, metformin plus sulfonylurea, and insulin plusmetformin).63 When compared with all other regimens, insu-lin monotherapy was associated with an increased risk of theprimary outcome and all-cause mortality. The observationalnature of the study does not permit conclusions about thecausal nature of these associations; the risk of harms maybemediated by insulin itself or by the clinical characteristicsof patients who require and are prescribed insulin. Indeed,there were important differences in baseline characteristics
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

165
13EffectofGluco
seMan
agem
entonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
ete
among treatment groups; despite adjustment for a variety ofvariables, residual confounding remains an importantlimitation.Although few trials have specifically focused on the effec-
tiveness and safety of insulin for prevention of cardiovascu-lar events, several trials have tested the use of insulin duringand after an acute MI for secondary prevention of cardiovas-cular disease and mortality. The first Diabetes Mellitus, Insu-lin Glucose Infusion in Acute Myocardial Infarction(DIGAMI) study showed significant reduction in mortality(absolute reduction of 11%) associated with the use ofinsulin-glucose infusion during admission and subcutane-ous insulin after hospitalization for glycemic control com-pared with standard therapy in diabetic patients.64
Because it was unclear whether the mortality benefit wasthe result of inpatient or outpatient glycemic control inDIGAMI, the DIGAMI-2 study tested three different strategies,including combinations of insulin-based inpatient and out-patient glycemic control regimens.65 However, the studystruggled with patient recruitment and did not achieve differ-ences in glycemic control among the three groups. Therewere no differences in mortality among the three groups.However, in the post hoc analysis of the DIGAMI-2 trial, insu-lin treatment was actually associated with an increased riskfor nonfatal cardiovascular events, but not mortality.66
The previously described ORIGIN trial provided morereassuring evidence on the use of insulin glargine in adultswith prediabetes or early diabetes but did not suggest cardio-vascular benefits.33 The use of insulin in this trial was asso-ciated with a very modest reduction in already low HbA1clevels (6.3% versus 6.0% in the standard versus insulin group,respectively) at the end of 2 years, no significant reduction inthe cardiovascular endpoints, but increase in weight gainand hypoglycemic events. Moreover, there was no effectof glargine on the incidence of various cancers, a concernraised because of insulin’s role in cell growth, differentia-tion, and proliferation and because of epidemiologic studiespointing to the increased risk of cancer associated with itsuse.67,68
s
Incretin-Based TherapiesMedications that work through the incretin system havebeen relatively recently introduced into the type 2 diabetespharmacopeia. These agents either mimic or increase thecirculating concentrations of endogenous glucagon-likepeptide 1 (GLP-1), thereby stimulating pancreatic insulinsecretion in a glucose-dependent fashion, suppressing pan-creatic glucagon output, slowing gastric emptying, anddecreasing appetite. The main advantage of the injectableGLP-1 agonists is weight loss, which is modest in mostpatients but can be significant in some. A limiting side effectis nausea and vomiting, particularly early in the course oftreatment. Concerns regarding an increased risk of pancrea-titis remain unresolved. The oral dipeptidyl peptidase 4(DPP-4) inhibitors work predominately through effects onthe endocrine pancreas and appear to be weight neutral.Typically, neither of the incretin-based classes causes hypo-glycemia as monotherapy.Give the recent introduction of these agents to the market
and limited long-term experience, results of trials evaluatingcardiovascular outcomes are only beginning to be reported,and many are still under way (Table 13-2). GLP-1 analoguesare effective in improving glycemic control and reduce
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
several cardiovascular risk factors. Based on animal studies,GLP-1–based therapy may mitigate ischemia-induced car-diac injury,69 but more data will be needed to assess long-term cardiovascular outcomes in humans.70
More information is currently available on the cardiovas-cular effects of DPP-4 inhibitors, and so far they appear toneither increase nor decrease cardiovascular events.71,72
These effects are disappointing, given that several industry-sponsored pooled cardiovascular analyses of DPP-4 inhibi-tors described risk ratios well below 1 for cardiovascularevents,73–75 raising hopes for a class of agents that couldactually reduce cardiovascular risk. However, two largerandomized controlled trials showed that saxagliptin andalogliptin had an overall neutral effect on major cardiovas-cular events. In the Saxagliptin Assessment of VascularOutcomes Recorded in Patients with Diabetes Mellitus–Thrombolysis in Myocardial Infarction 53 (SAVOR-TIMI 53)trial, 16,492 patients with type 2 diabetes who had risk factorsor a history of cardiovascular events were assigned toreceive saxagliptin or placebo in addition to their existingdiabetes medication therapy.71 After a median of 2.1 years,there was no difference in the primary endpoint (MI, ische-mic stroke, or cardiovascular death) between the twogroups (HR 1.0, 95% CI 0.89-1.12). However, more patientsin the saxagliptin group reported hypoglycemic events(15.3% versus 11.7%, P<0.001), and, somewhat unexpect-edly, more patients on saxagliptin were hospitalized forheart failure (3.5% versus 2.8%, P¼0.007). The findings ofincreased heart failure risk are concerning and warrant addi-tional investigation. In the Examination of CardiovascularOutcomes with Alogliptin Versus Standard of Care (EXAM-INE) trial, 5380 patients with type 2 diabetes who had hadan acute coronary event in the preceding 15 to 90 days wererandomly assigned to receive either alogliptin or placebo inaddition to an existing antihyperglycemic regimen.72 Similarto the findings of the SAVOR trial, there was no difference inthe primary endpoint (MI, stroke, or cardiovascular death)between the two groups (HR 0.96, upper boundary of theone-sided CI 1.16). Heart failure hospitalization was not aprespecified endpoint in EXAMINE, but when it was exam-ined in a post hoc fashion (including those events thatoccurred after a primary endpoint), there were numerically,but not statistically, more events in the alogliptin group (106versus 89, HR 1.19, P¼0.22).76 Three other DPP-4 inhibitorcardiovascular trials are currently ongoing (TECOS [saxa-gliptin], CAROLINA [linagliptin] and CARMELINA (linaglip-tin)). Several others involving GLP-1 receptor agonists(LEADER [liraglutide], EXSCEL [exenatide once weekly exe-natide], ELIXA (lixisenatide), SUSTAIN 6 [semaglutide]) willprovide additional data needed to assess cardiovasculareffects of these therapies.69
In summary, incretin-based therapies reduce HbA1clevels, do not lead to hypoglycemia (at least, as monother-apy), and are not associated with weight gain or MI, stroke,or cardiovascular death. Therefore they appear to be attrac-tive agents for the management of type 2 diabetes. On theother hand, they are very expensive, they may increasethe risk of heart failure in the case of saxagliptin, and theirother long-term risks and benefits are not yet known.
Other AgentsAcarbose is an alpha-glucosidase inhibitor that delays gutcarbohydrate absorption. Acarbose is infrequently used in
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

TABLE 13-2 Summary of Cardiovascular Effects Associated with Various Classes of Glucose-Lowering Agents
AGENT MECHANISM OF ACTION
EXPECTEDHBA1C
REDUCTION ADVERSE EFFECTS CARDIOVASCULAR EFFECTS
Sulfonylureas
Glyburide (akaglibenclamide)
GlipizideGlimepirideGliclazideTolbutamideChlorpropamide
Bind to sulfonylurea receptors onpancreatic islet cells, closingKATP channels, stimulatinginsulin release. Relatively longduration of action.
Approximately1%-2%
HypoglycemiaWeight gain
Hypoglycemia may precipitate ischemia,arrhythmia.
Cardiac KATP channel closure may impairischemic preconditioning.
Observational studies suggest worse CVDoutcomes compared with metformin.
Glinides
RepaglinideNateglinide
Bind to sulfonylurea receptors onpancreatic islet cells, closingKATP channels, stimulatinginsulin release. Relatively shortduration of action.
Approximately1%-2%
HypoglycemiaWeight gain
Hypoglycemia may precipitate ischemia,arrhythmia.
Cardiac KATP channel closure may impairischemic preconditioning.
Few CVD outcome studies exist.
Biguanide
Metformin Activates AMP-kinase and reduceshepatic glucose production.
Approximately1%-2%
Diarrhea, nauseaLactic acidosisDecreases B12 levels
May improve CVD outcomes (UKPDS 34).Favorable CVD outcomes in most
observational studies.Should not be used in patients with acute or
unstable HF because of lactic acidosis risk.
α-Glucosidase Inhibitors
VogliboseAcarboseMiglitol
Slow gut carbohydrate absorption. Approximately0.5%-1.0%
Gas, bloating May reduce MI risk (STOP-NIDDM).
Thiazolidinediones
PioglitazoneRosiglitazone
Activate the nuclear receptorPPAR-γ, increasing peripheralinsulin sensitivity. Also reducehepatic glucose production.
Approximately1%-1.5%
Weight gainEdema, HFFractures? Bladder cancer
(pioglitazone)
Contraindicated in NYHA Class III or IV HF(because of fluid retention); notrecommended in Class II HF.
Pioglitazone may reduce MI, stroke risk(PROactive) but increases HF risk.
Rosiglitazone may increase MI risk.
GLP-1 ReceptorAgonists
ExenatideLiraglutideAlbiglutide
Increase glucose-dependentinsulin secretion, decreaseglucagon secretion, and delaygastric emptying.
Approximately1%-1.5%
Approximately0.6%-0.8%
Nausea, vomiting—
Long-term outcomes not known.
DPP-4 Inhibitors
SitagliptinSaxagliptinLinagliptinVildagliptinAlogliptin
Inhibit degradation ofendogenous GLP-1 (and GIP-1),thereby enhancing incretin levels.
Alogliptin and saxagliptin have a neutraleffect on cardiovascular outcomes, butsaxagliptin may increase risk of HF.
Amylin Analogue
Pramlintide Decreases glucagon secretion anddelays gastric emptying.
Approximately0.4%-0.6%
Nausea, vomiting Long-term outcomes not known.
Insulins
Glargine, detemir,degludec
NPHRegularLispro, aspart, glulisinePremixed
Increase insulin supply. Theoreticallylimitless
HypoglycemiaWeight gainEdema (at high doses)
Few randomized controlled trials showneutral effects on cardiovascularoutcomes, but observational studiessuggest increased risk of cardiovascularevents and mortality compared with oralantihyperglycemic agents.
SGLT-2 Inhibitors
CanagliflozinDapagliflozinEmpagliflozin
Blocks reabsorption of filteredglucose load in the proximaltubule, leading to glucosuria
Approximately0.5%-1.0%
Genital mycotic infectionsUrinary tract infectionsReversible decrease in GFRHemodynamic side effectsIncrease in LDL-cholesterol
Reduction in systolic blood pressureWeight lossNo long-term data on CV outcomes
AMP ¼ Adenosine monophosphate; CVD ¼ Cardiovascular disease; GFR ¼ glomerular filtration rate; GIP-1 ¼ Gastric inhibitory polypeptide-1; GLP-1 ¼ Glucagon-like peptide-1;HF ¼ Heart failure; KATP¼adenosine triphosphate (ATP) sensitive potassium channel; NYHA¼New York Heart Association; SGLT-2 ¼ sodium-glucose co-transporter 2.Data from Inzucchi and McGuire.
166
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
Downloaded for Aman Shah ([email protected]) at Elsevier - Demonstration Account from ClinicalKey.com by Elsevier on December 21, 2017.For personal use only. No other uses without permission. Copyright ©2017. Elsevier Inc. All rights reserved.

14
Placebo
Hazard ratio, 1.00 (95% CI, 0.89–1.12)P � 0.001 for noninferiorityP � 0.99 for superiority
Saxagliptin
Pat
ient
s w
ith e
ndpo
int (
%) 12
8
6
4
2
10
00 180 540360 720 900
DaysA
24
Placebo
Hazard ratio, 0.96 (upper boundaryof the one-sided repeated CI, 1.16)
Alogliptin
Cum
ulat
ive
inci
denc
e of
prim
ary
endp
oint
s (%
)
18
6
12
0
167
13EffectofGluco
seMan
agem
entonCoronary
Heart
Disease
Risk
inPa
the United States because of gastrointestinal side effects. Posthoc analyses of the STOP-NIDDM trial showed a reduction incardiovascular endpoints, but, as mentioned earlier, therewere problems with the trial design and conduct.32 Anotheragent, colesevelam, a bile acid sequestrant, is typically usedto lower low-density lipoprotein (LDL) levels, but also mod-estly reduces glucose. The dopamine agonist bromocriptinereduces glucose levels, but very modestly, and is available inthe United States only for antihyperglycemic therapy. A 52-week trial evaluated the short-term overall and cardiovascu-lar safety of bromocriptine in type 2 diabetes.77 The fre-quency of serious adverse events was comparablebetween treatment arms, but fewer patients experienced car-diovascular events in the bromocriptine compared with theplacebo group (HR 0.60, 95% CI 0.35-0.96). Future studieswill need to confirm whether bromocriptine is indeed asso-ciated with cardiovascular risk reduction in the long-term.Newer agents, such as the SGLT-2 inhibitors, that lower
glucose by inhibiting a renal cotransporter and therebydecrease glucose reabsorption in the kidney, have beenrecently approved by the FDA, but studies are under wayto determine their long-term safety and efficacy.78,79 Short-term studies suggest that these agents lower HbA1c by0.5% to 1%, do not lead to hypoglycemia (in monotherapy),and lower blood pressure and weight, but are associatedwith mycotic genital infections and adverse events relatedto osmotic diuresis.80–85 Other glucose-loweringmedicationsthat stimulate glucose-dependent insulin secretion are beingtested for their efficacy and safety, as well.86 It will take sometime to understand the cardiovascular impact of these neweragents on patients with type 2 diabetes.
0 6 1812 24 30MonthsB
FIGURE 13-6 Summary of results from A, SAVOR and B, EXAMINE trials, in whichsaxagliptin and alogliptin were compared against placebo with respect to majorcardiovascular outcomes (myocardial infarction, stroke, or cardiovascular death).71
(Modified from NEJM.)
tients
with
Diab
etes
RISKS ASSOCIATED WITHANTIHYPERGLYCEMIC MEDICATIONS
If efforts to reduce glucose levels were not associated withany risk, there might be less hesitation to normalize themin diabetic patients. In reality, the benefits of glucose lower-ing must be weighed against the burden of treatment andknown, as well as potential, risks of therapy. Because dataon the impact of various anti-hyperglycemic agents onlong-term clinical outcomes are limited, clinical decisionsabout the type and intensity of glucose lowering must bemade with some uncertainty in mind (Fig. 13-6). We willnow review data on the known risks associated with antihy-perglycemic agents. This information is critical to informeddecision making and should be discussed with patients asstrategies for treatment are considered.
HypoglycemiaThe pursuit of strict glucose control is frequently hamperedby concerns over hypoglycemia. Hypoglycemia requiringthird-party assistance is common in the course of type 2 dia-betes therapy and occurs with a frequency of approximately35 episodes per 100 patient-years among insulin-treatedpatients.87 Hypoglycemia occurring during treatment hasbeen associated with several adverse events, includingincreased mortality,88,89 higher risk of dementia,90 falls,91 fall-related fractures,92 cardiovascular events,89,93,94 and poorhealth-related quality of life.95,96
In particular, the relationship between hypoglycemia andsubsequent cardiac events warrants attention. There are a
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
number of plausible mechanisms by which acute hypogly-cemia may trigger ischemia, arrhythmia, and cardiovascularevents (Fig. 13-7). Hypoglycemia increases the levels ofcounterregulatory hormones, such as epinephrine and nor-epinephrine, which may induce increased cardiac rate and/or contractility, heightening myocardial oxygen consump-tion, while also precipitating vasoconstriction and plateletaggregation. Acute hypoglycemia in the presence of hypoka-lemia prolongs cardiac repolarization, increases the QTinterval, favoring a proarrhythmic state. One study of type1 and type 2 diabetic patients who presented to the hospitalwith severe hypoglycemia documented frequent hypokale-mia, QT prolongation, and severe hypertension during thehypoglycemic events.97 Although animal studies have veri-fied the effect of hypoglycemia on myocardial ischemicinjury,98 the data in humans are less clear, and debates con-tinue on whether hypoglycemia is a mediator or merely amarker of such adverse outcomes—that is, does the propen-sity toward hypoglycemia simply identify sicker individualswho have lost the ability to counterregulate?
Clinical trial data consistently show that assignment to anintensive glucose control strategy is associated with a two-fold to threefold higher risk of hypoglycemia compared withstandard care.15,18,22,99,100 In trial settings, hypoglycemiarequiring third-party assistance occurred with a frequency
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

Hypoglycemia
Myocardial ischemiaArrhythmia
Hemodynamic changes
Increased heart rateIncreased systolic blood pressureIncreased cardiac output
ECG changes
QT prolongationIncreased QT dispersion
Inflammation and coagulation
Endothelial dysfunctionPlatelet aggregation/activationThrombosis
Sympathoadrenal activation:catecholamine, glucagon release
Hypokalemia
Increase in endothelin, CRP,vascular endothelial growth factor
FIGURE 13-7 Proposed mechanisms linking hypoglycemia with cardiovascular events. CRP¼C-reactive protein; EKG¼Electrocardiogram.
168
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
of 0.6 to 12 events annually per 100 patients in the intensivetherapy group and 0.2 to 4 events in the standard therapygroup—much less frequently than in the community setting.Although the relationship between intensive therapy andhypoglycemia appears clear, the relationship betweenachieved level of glycemic control and hypoglycemia is morecomplex. In the Diabetes Control and Complications Trial(DCCT) of type 1 diabetes patients, an inverse relationshipbetween HbA1c level and serious hypoglycemia was noted,with thenumber of events logically increasingwithdecreasingHbA1c.100 In contrast, however, detailed post hoc analyses ofACCORD participants with type 2 diabetes showed thatpatients with poorer glycemic control had a higher risk ofhypoglycemia, irrespective of treatment assignment.101 In fact,a greater drop in HbA1c level during the first 4 months of thetrial was not associated with increased hypoglycemia risk.Rather, patients who started out with higher baseline HbA1clevels and were unable to reduce their blood glucose levelsappeared to be at the highest risk for this complication. More-over, participants with persistently elevated HbA1c levelsabove 7% after initiation of the intensive strategy had a highermortality risk than those achieving lower glycemic levels(<7%).19What is actuallymediating thehigher riskof hypogly-cemia and mortality in this setting is unclear, but the findingssuggest that aggressive attempts to intensify treatment inpatients who remain hyperglycemic may confer a very highrisk for subsequent hypoglycemia.
Other apparent risk factors for hypoglycemia, aside fromintensive glucose lowering, include treatment with insulinor sulfonylurea medications,102 older age,101 lower healthliteracy level,103 longer duration of diabetes,101 renal impair-ment,102 polypharmacy,104baselinecognitive impairment,105
and recent admission to the hospital within 30 days.104
Other Adverse Effects of MedicationsIntensive glucose control usually requires polypharmacy toachieve HbA1c targets, and adverse effects of medicationsrequire careful consideration. Even in patients who do not
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
choose tight glycemic targets, multiple medications to lowerglucose are often required with increasing duration of thedisease, as beta cell function declines.
The relative importance of various adverse effects of med-ications may vary from patient to patient. Weight gain is typ-ically associated with the use of insulin, sulfonylureas, andthiazolidinediones. Heart failure, edema, and fractures areassociated with the use of thiazolidinediones. Gastrointesti-nal side effects complicate treatment with metformin, acar-bose, and some of the incretin-based therapies. In general,drug reactions increase in frequency with the use of multiplemedications. Addition of another medication to lower glu-cose may also pose a financial burden and significantlyincrease time and effort required to manage diabetes(including, potentially, capillary blood glucose monitoring).
IMPLICATIONS FOR CLINICAL PRACTICE
What is the effect of glucose management on CHD events inpatients with type 2 diabetes? Based on the available data,intensive glucose lowering appears, at best, to modestlydecrease the risk of CHD by approximately 15% when com-pared with standard glucose strategies. Assuming a 10-yearrisk of CHD of 17.4% (control arm of UKPDS), the numberneeded to treat (NNT) ranges on the order of 41 to 46 over10 years to prevent one CHD event.106 What about type ofantihyperglycemic therapy? Our understanding of the impli-cations of the specific type of therapy on these outcomes isonly beginning to emerge. Best cardiovascular outcomesappear to be associated with the use of metformin, but thesedata are based only on a small subgroup of UKPDS patientsand observational data. Sulfonylureas compared with met-formin appear to be associated with inferior results, andthe impact of thiazolidinediones remains somewhat unclear(with a suggestion of better outcomes for CHD with pioglita-zone, but an increase in heart failure). The effect of newerincretin-based therapies on cardiovascular outcomesappears neutral so far.
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.

169
13EffectofGluco
seMan
agem
entonCoronary
Heart
Disease
Risk
inPatien
tswith
Diab
etes
Who is the patient, andwhat are his or her goals for care? Tohelp patients make the best decisions about their care, clini-cians must consider the clinical characteristics of a patientand thecontext inwhichheorshe lives todeterminehowthesevarious factors may influence the relationship between treat-ment and outcomes. Data to guide this type of individualizedtreatment are lacking, and future research is critically neededto provide better information to guide personalized decisions.Basedonexistingdata, patientswithhigh levelsof comorbiditymay derive less cardiovascular benefit from intensive glucosecontrol,107andmostguidelinessuggesthigherglycemic targetsfor older patients with longer duration of diabetes, establishedcardiovascular disease, and high risk of hypoglycemia. Natu-rally, these patients are at higher underlying risk of CHD, butthey appear to benefit less from tight glycemic control. In con-trast, thebenefitsof aggressive lipidandbloodpressurecontrolappear to be greatest based on high underlying CHD risk,although the relative benefits will clearly depend also on com-peting mortality risk and current medications.107
As already suggested, central to the decision makingabout treatment are patient’s preferences and goals for care.Patient-centered care needs to begin by eliciting these pref-erences and goals, because understanding them is indis-pensable for providing care that is responsive to andrespectful of patients’ needs. A shared decision-making pro-cess stresses a partnership between the patient’s values andpreferences and the physician’s knowledge of clinical evi-dence and judgment. Decisions are highly individualized,based on available evidence, and uncertainty must beacknowledged when it exists. As an example, more intensiveglycemic control in a patient already struggling with a com-plex regimen may lead to an overburdened patient who isunable to cope with his or her disease. Indeed, somewhatparadoxically, pushing forward with intensive antihypergly-cemic therapy may decrease adherence to other moreevidence-based therapies. In such a circumstance, it maybe reasonable to liberalize glycemic targets to some degree.On the other hand, a patient whose most important goal isprevention of diabetes complications may choose to takeon the additional burden of insulin therapy or multiple med-ications to control blood glucose levels with high intensity.How to prioritize glucose lowering within the patient’s
overall diabetes care plan is also critically important. Clearly,statin therapy, smoking cessation, aspirin for appropriatepatients, and blood pressure control are the central pillarsof cardiovascular risk reduction. On a population level,based on UKPDS data, fewer persons would need to be trea-ted with tight blood pressure control (NNT 23) than intensiveglucose control (NNT 46) to prevent one MI event.108 Simi-larly, lipid therapy for primary prevention (NNT 34 or 35)and secondary prevention (NNT 13 or 14) appears to bemore effective for cardiovascular events than intensive glu-cose control.109 However, for individual patients, the opti-mal strategy is still unknown. It is also unclear whetherpatients will do better if each problem is addressed sequen-tially or if they are addressed simultaneously, and how thisvaries based on degree of out-of-range risk factor levels.Despite decades of study, we remain largely ignorant of the
benefits and risks of antihyperglycemic therapy as it relates tocardiovascular disease risk. Research in the coming decadeneeds to provide us with better information so that patientscan make decisions about glucose targets and antihypergly-cemic strategies that optimize their outcomes.
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstraFor personal use only. No other uses without permission.
References1. Stern MP: Diabetes and cardiovascular disease. The “common soil” hypothesis, Diabetes
44:369–374, 1995.
2. Roger VL, Go AS, Lloyd-Jones DM, et al: Heart disease and stroke statistics–2012 update: a report
from the American Heart Association, Circulation 125:e2–e220, 2012.
3. Cowie CC, Rust KF, Ford ES, et al: Full accounting of diabetes and pre-diabetes in the U.S. pop-
ulation in 1988–1994 and 2005–2006, Diabetes Care 32:287–294, 2009.
4. National diabetes fact sheet: general information and national estimates on diabetes in the
United States, 2011.
5. Gregg EW, Cheng YJ, Saydah S, et al: Trends in death rates among U.S. adults with and without
diabetes between 1997 and 2006: findings from the national health interview survey, DiabetesCare 35:1252–1257, 2012.
6. Fox CS, Coady S, Sorlie PD, et al: Increasing cardiovascular disease burden due to diabetes mel-
litus: the Framingham Heart Study, Circulation 115:1544–1550, 2007.
7. Coutinho M, Gerstein HC, Wang Y, et al: The relationship between glucose and incident cardio-
vascular events. A metaregression analysis of published data from 20 studies of 95,783 individ-
uals followed for 12.4 years, Diabetes Care 22:233–240, 1999.
8. Khaw KT, Wareham N, Bingham S, et al: Association of hemoglobin A1c with cardiovascular
disease and mortality in adults: the European Prospective Investigation into Cancer in Norfolk,
Ann Intern Med 141:413–420, 2004.
9. Selvin E, Steffes MW, Zhu H, et al: Glycated hemoglobin, diabetes, and cardiovascular risk in
nondiabetic adults, N Engl J Med 362:800–811, 2010.
10. Stratton IM, Adler AI, Neil HA, et al: Association of glycaemia with macrovascular and microvas-
cular complications of type 2 diabetes (UKPDS 35): prospective observational study, Br Med J(Clin Res Ed) 321:405–412, 2000.
11. Selvin E, Marinopoulos S, Berkenblit G, et al: Meta-analysis: glycosylated hemoglobin and car-
diovascular disease in diabetes mellitus, Ann Intern Med 141:421–431, 2004.
12. Currie CJ, Peters JR, Tynan A, et al: Survival as a function of hba(1c) in people with type 2 dia-
betes: a retrospective cohort study, Lancet 375:481–489, 2010.13. Huang ES, Liu JY, Moffet HH, et al: Glycemic control, complications, and death in older diabetic
patients: the diabetes and aging study, Diabetes Care 34:1329–1336, 2011.
14. Colayco DC, Niu F, McCombs JS, et al: A1c and cardiovascular outcomes in type 2 diabetes: a
nested case-control study, Diabetes Care 34:77–83, 2011.
15. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional
treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective
Diabetes Study (UKPDS) group, Lancet 352:837–853, 1998.16. Effect of intensive blood-glucose control with metformin on complications in overweight
patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group, Lan-cet 352:854–865, 1998.
17. Holman RR, Paul SK, Bethel MA, et al: 10-year follow-up of intensive glucose control in type 2
diabetes, N Engl J Med 359:1577–1589, 2008.
18. Gerstein HC, Miller ME, Byington RP, et al: Effects of intensive glucose lowering in type 2 diabe-
tes, N Engl J Med 358:2545–2559, 2008.
19. Riddle MC, Ambrosius WT, Brillon DJ, et al: Epidemiologic relationships between a1c and all-
cause mortality during a median 3.4-year follow-up of glycemic treatment in the accord trial,
Diabetes Care 33:983–990, 2010.
20. Bonds DE, Miller ME, Bergenstal RM, et al: The association between symptomatic, severe hypo-
glycaemia andmortality in type 2 diabetes: retrospective epidemiological analysis of the accord
study, Br Med J (Clin Res Ed) 340:b4909, 2010.21. Gerstein HC, Miller ME, Genuth S, et al: Long-term effects of intensive glucose lowering on car-
diovascular outcomes, N Engl J Med 364:818–828, 2011.
22. Patel A, MacMahon S, Chalmers J, et al: Intensive blood glucose control and vascular outcomes
in patients with type 2 diabetes, N Engl J Med 358:2560–2572, 2008.
23. Boussageon R, Supper I, Bejan-Angoulvant T, et al: Reappraisal of metformin efficacy in the treat-
ment of type 2 diabetes: a meta-analysis of randomised controlled trials, PLoS Med 9:e1001204,
2012.
24. Hemmingsen B, Lund SS, Gluud C, et al: Intensive glycaemic control for patients with type 2
diabetes: systematic review with meta-analysis and trial sequential analysis of randomised clin-
ical trials, Br Med J (Clin Res Ed) 343:d6898, 2011.25. Kelly TN, Bazzano LA, Fonseca VA, et al: Systematic review: glucose control and cardiovascular
disease in type 2 diabetes, Ann Intern Med 151:394–403, 2009.
26. Marso SP, Kennedy KF, House JA, et al: The effect of intensive glucose control on all-cause and
cardiovascular mortality, myocardial infarction and stroke in persons with type 2 diabetes mel-
litus: a systematic review and meta-analysis, Diab Vasc Dis Res 7:119–130, 2010.27. Ray KK, Seshasai SR, Wijesuriya S, et al: Effect of intensive control of glucose on cardiovascular
outcomes and death in patients with diabetesmellitus: ameta-analysis of randomised controlled
trials, Lancet 373:1765–1772, 2009.28. Turnbull FM, Abraira C, Anderson RJ, et al: Intensive glucose control and macrovascular out-
comes in type 2 diabetes, Diabetologia 52:2288–2298, 2009.
29. Knowler WC, Barrett-Connor E, Fowler SE, et al: Reduction in the incidence of type 2 diabetes
with lifestyle intervention or metformin, N Engl J Med 346:393–403, 2002.
30. Ratner R, Goldberg R, Haffner S, et al: Impact of intensive lifestyle and metformin therapy on
cardiovascular disease risk factors in the diabetes prevention program, Diabetes Care28:888–894, 2005.
31. Knowler WC, Fowler SE, Hamman RF, et al: 10-year follow-up of diabetes incidence and weight
loss in the diabetes prevention program outcomes study, Lancet 374:1677–1686, 2009.32. Chiasson JL, Josse RG, Gomis R, et al: Acarbose treatment and the risk of cardiovascular disease
and hypertension in patients with impaired glucose tolerance: the STOP-NIDDM trial, JAMA290:486–494, 2003.
33. ORIGIN Trial Investigators, Gerstein HC, Bosch J, Dagenais GR, et al: Basal insulin and cardio-
vascular and other outcomes in dysglycemia, N Engl J Med 367:319–328, 2012.
34. Nissen SE, Wolski K: Effect of rosiglitazone on the risk of myocardial infarction and death from
cardiovascular causes, N Engl J Med 356:2457–2471, 2007.
35. Richter B, Bandeira-Echtler E, Bergerhoff K, et al: Rosiglitazone for type 2 diabetes mellitus,
Cochrane Database Syst Rev, 2007, CD006063.36. Diamond GA, Bax L, Kaul S: Uncertain effects of rosiglitazone on the risk for myocardial infarc-
tion and cardiovascular death, Ann Intern Med 147:578–581, 2007.
37. US Department of Health and Human Services, Food and Drug Administration Center for Drug
Evaluation and Research (CDER), guidance for industry; diabetes mellitus—evaluating cardio-
vascular risk in new antidiabetic therapies to treat type 2 diabetes, 2008.
38. Bennett WL, Maruthur NM, Singh S, et al: Comparative effectiveness and safety of medications
for type 2 diabetes: an update including new drugs and 2-drug combinations, Ann Intern Med154:602–613, 2011.
39. Kooy A, de Jager J, Lehert P, et al: Long-term effects of metformin on metabolism and microvas-
cular and macrovascular disease in patients with type 2 diabetes mellitus, Arch Intern Med169:616–625, 2009.
40. Johnson JA, Majumdar SR, Simpson SH, et al: Decreased mortality associated with the use of
metformin compared with sulfonylurea monotherapy in type 2 diabetes, Diabetes Care25:2244–2248, 2002.
tion Account from ClinicalKey.com by Elsevier on December 21, 2017.Copyright ©2017. Elsevier Inc. All rights reserved.

170
III
MANAGEM
ENTOFCORONARYH
EARTD
ISEA
SERISK
ANDD
ISEA
SEINPA
TIEN
TSWITHD
IABET
ES
41. Tzoulaki I, Molokhia M, Curcin V, et al: Risk of cardiovascular disease and all cause mortality
among patients with type 2 diabetes prescribed oral antidiabetes drugs: retrospective cohort
study using UK general practice research database, Br Med J (Clin Res Ed) 339:b4731, 2009.42. Roumie CL, Hung AM, Greevy RA, et al: Comparative effectiveness of sulfonylurea and metfor-
min monotherapy on cardiovascular events in type 2 diabetes mellitus: a cohort study, AnnIntern Med 157:601–610, 2012.
43. McAfee AT, Koro C, Landon J, et al: Coronary heart disease outcomes in patients receiving anti-
diabetic agents, Pharmacoepidemiol Drug Saf 16:711–725, 2007.44. Hemmingsen B, Christensen LL, Wetterslev J, et al: Comparison of metformin and insulin versus
insulin alone for type 2 diabetes: systematic review of randomised clinical trials with meta-
analyses and trial sequential analyses, Br Med J (Clin Res Ed) 344:e1771, 2012.45. Kahn SE, Haffner SM, Heise MA, et al: Glycemic durability of rosiglitazone, metformin, or glybur-
ide monotherapy, N Engl J Med 355:2427–2443, 2006.
46. A study of the effects of hypoglycemia agents on vascular complications in patients with adult-
onset diabetes. Vi. Supplementary report on nonfatal events in patients treated with tolbuta-
mide, Diabetes 25:1129–1153, 1976.47. Simpson SH, Majumdar SR, Tsuyuki RT, et al: Dose-response relation between sulfonylurea
drugs and mortality in type 2 diabetes mellitus: a population-based cohort study, CMAJ174:169–174, 2006.
48. Morgan CL, Poole CD, Evans M, et al: What next after metformin? A retrospective evaluation of
the outcome of second-line, glucose-lowering therapies in people with type 2 diabetes, J ClinEndocrinol Metab 97:4605–4612, 2012.
49. Singh S, Loke YK, Furberg CD: Long-term risk of cardiovascular events with rosiglitazone: ameta-
analysis, JAMA 298:1189–1195, 2007.
50. Cobitz A, Zambanini A, Sowell M, et al: A retrospective evaluation of congestive heart failure and
myocardial ischemia events in 14,237 patients with type 2 diabetes mellitus enrolled in 42 short-
term, double-blind, randomized clinical studies with rosiglitazone, Pharmacoepidemiol Drug Saf17:769–781, 2008.
51. Lipscombe LL, Gomes T, Levesque LE, et al: Thiazolidinediones and cardiovascular outcomes in
older patients with diabetes, JAMA 298:2634–2643, 2007.
52. Winkelmayer WC, Setoguchi S, Levin R, Solomon DH: Comparison of cardiovascular outcomes
in elderly patients with diabetes who initiated rosiglitazone vs pioglitazone therapy, Arch InternMed 168:2368–2375, 2008.
53. Juurlink DN, Gomes T, Lipscombe LL, et al: Adverse cardiovascular events during treatment with
pioglitazone and rosiglitazone: population based cohort study, Br Med J (Clin Res Ed) 339:b2942,2009.
54. Graham DJ, Ouellet-Hellstrom R, MaCurdy TE, et al: Risk of acute myocardial infarction, stroke,
heart failure, and death in elderly medicare patients treated with rosiglitazone or pioglitazone,
JAMA 304:411–418, 2010.
55. Home PD, Pocock SJ, Beck-Nielsen H, et al: Rosiglitazone evaluated for cardiovascular out-
comes in oral agent combination therapy for type 2 diabetes (record): a multicentre, rando-
mised, open-label trial, Lancet 373:2125–2135, 2009.56. Frye RL, August P, Brooks MM, et al: A randomized trial of therapies for type 2 diabetes and cor-
onary artery disease, N Engl J Med 360:2503–2515, 2009.
57. FDA drug safety communication: updated risk evaluation and mitigation strategy (REMS) to
restrict access to resiglitazone containing medicines including Avandia, Avandamet, and Avan-
daryl, 2011. http://fda.gov/Drugs/DrugSafety/ucm2555005.htm. Accessed January 09, 2013.
58. Lincoff AM, Wolski K, Nicholls SJ, et al: Pioglitazone and risk of cardiovascular events in patients
with type 2 diabetes mellitus: a meta-analysis of randomized trials, JAMA 298:1180–1188, 2007.
59. Dormandy JA, Charbonnel B, Eckland DJ, et al: Secondary prevention of macrovascular events
in patients with type 2 diabetes in the PRoACTIVE study (prospective pioglitazone clinical trial in
macrovascular events): a randomised controlled trial, Lancet 366:1279–1289, 2005.60. Currie CJ, Johnson JA: The safety profile of exogenous insulin in people with type 2 diabetes:
justification for concern, Diabetes Obes Metab 14:1–4, 2012.
61. Gamble JM, Simpson SH, Eurich DT, et al: Insulin use and increased risk of mortality in type 2
diabetes: a cohort study, Diabetes Obes Metab 12:47–53, 2010.
62. Anselmino M, Ohrvik J, Malmberg K, et al: Glucose lowering treatment in patients with coronary
artery disease is prognostically important not only in established but also in newly detected dia-
betes mellitus: a report from the euro heart survey on diabetes and the heart, Eur Heart J29:177–184, 2008.
63. Currie CJ, Poole CD, EvansM, et al: Mortality and other important diabetes-related outcomeswith
insulin vs other antihyperglycemic therapies in type 2 diabetes, J Clin Endocrinol Metab, 2013.64. Malmberg K: Prospective randomised study of intensive insulin treatment on long term survival
after acute myocardial infarction in patients with diabetes mellitus. Digami (diabetes mellitus,
insulin glucose infusion in acute myocardial infarction) study group, BMJ 314:1512–1515, 1997.65. Malmberg K, Ryden L, Wedel H, et al: Intense metabolic control by means of insulin in patients
with diabetes mellitus and acute myocardial infarction (digami 2): effects on mortality and mor-
bidity, Eur Heart J 26:650–661, 2005.66. Mellbin LG, Malmberg K, Norhammar A, et al: Prognostic implications of glucose-lowering treat-
ment in patients with acute myocardial infarction and diabetes: experiences from an extended
follow-up of the diabetes mellitus insulin-glucose infusion in acute myocardial infarction
(digami) 2 study, Diabetologia 54:1308–1317, 2011.
67. Currie CJ, Poole CD, Gale EA: The influence of glucose-lowering therapies on cancer risk in type
2 diabetes, Diabetologia 52:1766–1777, 2009.
68. Li C, Zhao G, Okoro CA, et al: Prevalence of diagnosed cancer according to duration of diag-
nosed diabetes and current insulin use among U.S. adults with diagnosed diabetes: findings
from the 2009 behavioral risk factor surveillance system, Diabetes Care, 2013.69. Jose T, Inzucchi SE: Cardiovascular effects of the dpp-4 inhibitors, Diab Vasc Dis Res 9:109–116,
2012.
70. Shyangdan DS, Royle P, Clar C, et al: Glucagon-like peptide analogues for type 2 diabetes mel-
litus, Cochrane Database Syst Rev, 2011, CD006423.71. Scirica BM, Bhatt DL, Braunwald E, et al: Saxagliptin and cardiovascular outcomes in patients
with type 2 diabetes mellitus, N Engl J Med 369:1317–1326, 2013.
72. WhiteWB, Cannon CP, Heller SR, et al: Alogliptin after acute coronary syndrome in patients with
type 2 diabetes, N Engl J Med 369:1327–1335, 2013.
73. Schweizer A, Dejager S, Foley JE, et al: Assessing the cardio-cerebrovascular safety of vildaglip-
tin: meta-analysis of adjudicated events from a large phase iii type 2 diabetes population, Dia-betes Obes Metab 12:485–494, 2010.
74. Frederich R,Alexander JH, Fiedorek FT, et al: A systematic assessment of cardiovascular outcomes
in the saxagliptin drug development program for type 2 diabetes, Postgrad Med 122:16–27, 2010.
Downloaded for Aman Shah ([email protected]) at Elsevier - DemonstrFor personal use only. No other uses without permission
75. Williams-Herman D, Engel SS, Round E, et al: Safety and tolerability of sitagliptin in clinical stud-
ies: a pooled analysis of data from 10,246 patients with type 2 diabetes, BMC Endocr Disord 10:7,
2010.
76. WhiteWB: Cardiovascular outcomes with alogliptin in patients with type 2 diabetes mellitus and
recent acute coronary syndromes. In 49th Annual meeting of the European Association for theStudy of Diabetes (EASD) meeting, September 26, 2013, ; 2013.
77. Gaziano JM, Cincotta AH, O’Connor CM, et al: Randomized clinical trial of quick-release bromo-
criptine among patients with type 2 diabetes on overall safety and cardiovascular outcomes,
Diabetes Care 33:1503–1508, 2010.
78. Neal B, Perkovic V, de Zeeuw D, et al: Rationale, design, and baseline characteristics of the Cana-
gliflozin Cardiovascular Assessment Study (CANVAS)–a randomized placebo-controlled trial, AmHeart J 166:217–223, 2013. e11. http://dx.doi.org/10.1016/j.ahj.2013.05.007. Epub 2013 Jun 24.
79. BI 10773 (Empagliflozin) Cardiovascular outcome event trial in Type 2 diabetes mellitus
patients. http://clinicaltrials.gov/show/NCT01131676. Accessed April 21, 2014.
80. Clar C, Gill JA, Court R, Waugh N: Systematic review of sglt2 receptor inhibitors in dual or triple
therapy in type 2 diabetes, BMJ Open 2:2012.
81. Cefalu WT, Leiter LA, Yoon KH, et al: Efficacy and safety of canagliflozin versus glimepiride in
patients with type 2 diabetes inadequately controlled with metformin (cantata-su): 52 week
results from a randomised, double-blind, phase 3 non-inferiority trial, Lancet 382:941–950, 2013.82. Lavalle-Gonzalez FJ, Januszewicz A, Davidson J, et al: Efficacy and safety of canagliflozin com-
pared with placebo and sitagliptin in patients with type 2 diabetes on background metformin
monotherapy: a randomised trial, Diabetologia 56:2582–2592, 2013.
83. Schernthaner G, Gross JL, Rosenstock J, et al: Canagliflozin comparedwith sitagliptin for patients
with type 2 diabetes who do not have adequate glycemic control with metformin plus sulfonyl-
urea: a 52-week randomized trial, Diabetes Care 36:2508–2515, 2013.
84. Jabbour SA, Hardy E, Sugg J, Parikh S: Dapagliflozin is effective as add-on therapy to sitagliptin
with or without metformin: a 24-week, multicenter, randomized, double-blind, placebo-
controlled study, Diabetes Care, 2013.85. Vasilakou D, Karagiannis T, Athanasiadou E, et al: Sodium-glucose cotransporter 2 inhibitors for
type 2 diabetes: a systematic review and meta-analysis, Ann Intern Med 159:262–274, 2013.
86. Determination of safety, tolerability, pharmacokinetics, food effect & pharmacodynamics of sin-
gle & multiple doses of P11187. http://clinicaltrials.gov/ct2/show/NCT01874366. Accessed April
21, 2014.
87. Donnelly LA, Morris AD, Frier BM, et al: Frequency and predictors of hypoglycaemia in type 1
and insulin-treated type 2 diabetes: a population-based study, Diabet Med 22:749–755, 2005.
88. McCoy RG, Van Houten HK, Ziegenfuss JY, et al: Increased mortality of patients with diabetes
reporting severe hypoglycemia, Diabetes Care 35:1897–1901, 2012.
89. Hsu PF, Sung SH, Cheng HM, et al: Association of clinical symptomatic hypoglycemia with car-
diovascular events and total mortality in type 2 diabetes mellitus: a nationwide population-
based study, Diabetes Care, 2012.90. Whitmer RA, Karter AJ, Yaffe K, et al: Hypoglycemic episodes and risk of dementia in older
patients with type 2 diabetes mellitus, JAMA 301:1565–1572, 2009.
91. Schwartz AV, Vittinghoff E, Sellmeyer DE, et al: Diabetes-related complications, glycemic con-
trol, and falls in older adults, Diabetes Care 31:391–396, 2008.
92. Johnston SS, Conner C, Aagren M, et al: Association between hypoglycaemic events and fall-
related fractures in medicare-covered patients with type 2 diabetes, Diabetes Obes Metab14:634–643, 2012.
93. Johnston SS, Conner C, Aagren M, et al: Evidence linking hypoglycemic events to an increased
risk of acute cardiovascular events in patients with type 2 diabetes, Diabetes Care 34:1164–1170,2011.
94. Desouza C, Salazar H, Cheong B, et al: Association of hypoglycemia and cardiac ischemia: a
study based on continuous monitoring, Diabetes Care 26:1485–1489, 2003.
95. Laiteerapong N, Karter AJ, Liu JY, et al: Correlates of quality of life in older adults with diabetes:
the diabetes & aging study, Diabetes Care 34:1749–1753, 2011.
96. Williams SA, Shi L, Brenneman SK, et al: The burden of hypoglycemia on healthcare utilization,
costs, and quality of life among type 2 diabetes mellitus patients, J Diabetes Complications26:399–406, 2012.
97. Tsujimoto T, Yamamoto-Honda R, Kajio H, et al: Vital signs, qt prolongation, and newly diag-
nosed cardiovascular disease during severe hypoglycemia in type 1 and type 2 diabetic patients,
Diabetes Care 2013.
98. Libby P, Maroko PR, Braunwald E: The effect of hypoglycemia on myocardial ischemic injury
during acute experimental coronary artery occlusion, Circulation 51:621–626, 1975.
99. DuckworthW, Abraira C, Moritz T, et al: Glucose control and vascular complications in veterans
with type 2 diabetes, N Engl J Med 360:129–139, 2009.
100. The effect of intensive treatment of diabetes on the development and progression of long-term
complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications
Trial Research Group, N Engl J Med 329:977–986, 1993.
101. Miller ME, Bonds DE, Gerstein HC, et al: The effects of baseline characteristics, glycaemia treat-
ment approach, and glycated haemoglobin concentration on the risk of severe hypoglycaemia:
post hoc epidemiological analysis of the accord study, BMJ 340:b5444, 2010.102. Davis TM, Brown SG, Jacobs IG, et al: Determinants of severe hypoglycemia complicating type 2
diabetes: the fremantle diabetes study, J Clin Endocrinol Metab 95:2240–2247, 2010.
103. Sarkar U, Karter AJ, Liu JY, et al: Hypoglycemia is more common among type 2 diabetes patients
with limited health literacy: the diabetes study of Northern California (distance), J Gen InternMed 25:962–968, 2010.
104. Shorr RI, Ray WA, Daugherty JR, et al: Incidence and risk factors for serious hypoglycemia in
older persons using insulin or sulfonylureas, Arch Intern Med 157:1681–1686, 1997.
105. Punthakee Z, Miller ME, Launer LJ, et al: Poor cognitive function and risk of severe hypoglycemia
in type 2 diabetes: post hoc epidemiologic analysis of the accord trial,Diabetes Care 35:787–793,2012.
106. Yudkin JS, Richter B: Intensive glucose control and cardiovascular outcomes, Lancet 374:522,2009, author reply 524.
107. Greenfield S, Billimek J, Pellegrini F, et al: Comorbidity affects the relationship between glyce-
mic control and cardiovascular outcomes in diabetes: a cohort study, Ann Intern Med151:854–860, 2009.
108. Vijan S, Hayward RA: Treatment of hypertension in type 2 diabetes mellitus: blood pressure
goals, choice of agents, and setting priorities in diabetes care, Ann Intern Med 138:593–602,
2003.
109. Vijan S, Hayward RA: Pharmacologic lipid-lowering therapy in type 2 diabetes mellitus: back-
ground paper for the american college of physicians, Ann Intern Med 140:650–658, 2004.
ation Account from ClinicalKey.com by Elsevier on December 21, 2017.. Copyright ©2017. Elsevier Inc. All rights reserved.