Embed Size (px)
Citation preview

Hit the road Jack!
W. FRANK PEACOCK, MD, FACEP, FACC

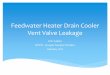
Visits130,000,000annually
6.24 Msuspected or actual
cardiac4.1 Msent home non-cardiac
50,000 MIs
3.1 Mnon-cardiac
(50%)
10.4 M chest pain (8.0%)
1.2 MAMI(20%)
1.5 MUA
(24%)
374,400sudden death
(6%)

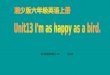
Myocardial Pain
PneumoniaPneumothorax
Sickle cell
Anemia
Pulmonary Embolus
Musculoskeletal Pain
Aortic Dissection
Mondor’s
SyndromeTietze’s
disease
Herpes
Zoster
Blunt Chest Trauma
Breast
Cancer
Breast Abcess
Contact
Dermatitis
GERD
Boerhave’s
Mallory-
Weiss
Mediastinitis
Lung
Cancer
Anxiety Panic Attack
Breast Implant
Thoracic
Spine Ds
Subdiaphrag
Abcess
Empyema
Amniotic Fluid
Embolus
IVDA Pulm Infarction
Asthma

HsTn (STATISTICAL)DefinitionYoucan’thaveitbothways
Sensitivity
TP/(TP+FN)
Specificity
TN/(TN+FP)

How often is the EKG diagnostic?
2%
N=10,869Pope JH, et al. Missed Diagnosis of Acute Cardiac Ischemia in the ED, NEJM 2000;342:1163-70
10.4 million annual ER CPSTEMI = 208,000
3500 ER’s = 59 STEMI/ER/yr
No ECG ∆ = 10,192,000/yr= 2,912/ER/yr= to find 59

How good are the parts?Than M. Lancet, 2011. DOI:10.1016/S0140-6736(11)60310-3
Sensitivity NPVECG 35.2 89.3POC markers 82.9 96.1TIMI 96.7 97.5POC + ECG 88.8 96.7TIMI + ECG 98.1 98.3ADP 99.3 99.1

How often is the Tn diagnostic?
8%
N=10,869Pope JH, et al. Missed Diagnosis of Acute Cardiac Ischemia in the ED NEJM 2000;342:1163-70
10.4 million annual ER CPTotal NSTEMI = 822,0003500 USA ER’s = 238/ER/yr
9,568,000 –Tn/yr2733 -Tn/ER to find 238

What is the fastest troponin? POC vs the central lab.Locale Hosp
TypeTransp POC
TnCL
CKMBDiff
(mins)ED Univ Pneumo
tube21±0.2(n=1879)
107±2.3(n=1744)
86±2.3
ED Univ Courier 22±0.5(n=855)
72±1.7(n=689)
50±1.5
CCU Rural Nurses 12±0.5(n=471)
147±64.1(n=150)
135±64.1
ED Muni Pneumotube
22±0.8(n=706)
90±0.5(n=185)
68±1.1
ED Univ Pneumo tube
18±0.5(n=698)
52±1.4(n=679)
34±1.4
All 20±0.2(n=4609)
85±1.5(n=3447)
65±1.5
Gaze D et al. Point of Care: The Journal of Near-Patient Testing & Technology. 2004;3:156–158.
5 hospitals4609 Tn POC samples
3447 split and sent to lab for CKMB

How good are the parts?Than M. Lancet, 2011. DOI:10.1016/S0140-6736(11)60310-3
Sensitivity NPVECG 35.2 89.3POC markers 82.9 96.1TIMI 96.7 97.5POC + ECG 88.8 96.7TIMI + ECG 98.1 98.3ADP 99.3 99.1

Howsensitivedoesithavetobe?
• 100,000AnnualERvisits• 8%CP=8k/yr =22/day
• Sn=95%– Miss5outof100– Miss1AMIevery4.5days
• Miss81AMI/yr
• Sn=99.5%– Miss1outof200– Miss1every9days

OK it has to go to the lab, but how about one and done???

Whyisn’t1troponinenough?
• ADAPTandAPACEhadpresentationsat~4hours………….
• Yourcutpoint is?Letssay13pg/mL– Mrs Jonesnormallylivesat4– Shepresents45minutesafterCPonset– Tn is12(300%increasefrombaseline)

Oneanddone?• Metaanalysisof23papers– Elecsys hs TnT atEDpresentation– LOD=5ng/L,LOQ=13ng/L
(thelowestTnT thathasCVof≤10%)
– 99th%ile ofhealthypop=14ng/L• Results
– N=9428– Pre-testprobabilityofAMI21%– Mostpatientspresentedwithin12hrs ofsymptomonset• studymedians3.5-6.3hrs
• Using14ng/Lcutpoint– Sn=89.5%
• (95%CI86.3%to92.1%),
– Sp=77.1%(68.7%to83.7%).
• Cutpoints determinemissrate– For100consecutivepatients– 5ng/Lwillmiss2-3AMI– 3ng/Lwillmiss0AMI
BMJ

Reichlin T. N Engl J Med 2009;361:858-67.
718 consecutiveED suspect AMI
MI/USA 238 (33.1%)

Chest Pain Protocol VS. ADP
A CHEST PAIN PROTOCOL
A series of activities to identify a patient as:
1) Having an event
2) Being at risk for having an event
AN ACCELERATED DIAGNOSTIC PROTOCOL
A series of activities to identify the patient as:
1) NOT having an event
2) Being at low risk for having an event

WhyanADP?AcceleratedDiagnosticProtocol
• ReasonforanADP• ERdocsvsriskscores
–Docsareriskadverse–Docsalwaysadmitmorethanscores

Whydoweadmitsooomany?
LAWYER
ER Dr.

ADP is for discharging! Maybe that is a good idea?
ADP1) Non-Dx ECG2) (-) Tn x23) Low Risk Score
Risk Scores▪TIMI▪HEART▪EDACS▪CRUSADE▪GRACE

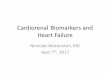
TIMI Risk Score: 2 week MACE
4.78.3
13.2
19.9
26.2
40.9
051015202530354045
0/1 2 3 4 5 6/7
▪ Risk factors:▪ Age ≥65 years▪ ≥3 risk factors for CAD▪ Prior coronary stenosis ≥50%
▪ ST-segment deviation on ECG
▪ ≥2 anginal events in last 24 hours
▪ Use of ASA in last 7 days▪ Elevated serum cardiac
markers CK-MB or troponin
Each risk factor is = 1 point, and total represents TIMI Risk ScoreEvent rates (all-cause mortality, MI, or UTVR) increase with each 1-point increase in score
Number of Risk Factors1R
ate
of C
ompo
site
En
dpoi
nt
(Day
s 1-
14),
%
Antman EM et al. JAMA. 2000;284:835-842.

How good are the parts?Than M. Lancet, 2011. DOI:10.1016/S0140-6736(11)60310-3
Sensitivity NPVECG 35.2 89.3POC markers 82.9 96.1TIMI 96.7 97.5POC + ECG 88.8 96.7TIMI + ECG 98.1 98.3ADP 99.3 99.1

HEART Score for 6 week MACE
Hx: Hi =2, Mod =1, Slight =0
ECG: Sig ST dep =2, NS repol =1, Nl =0
Age: ≥65 =2, 45-65 =1, ≤ 45 =0
Risks: ≥3 =2, 1-2 =1, 0=0
Tn: ≥3x ULN =21-3 ULN =1≤ ULN =0
Low risk = 0-3; <2% MACE risk
RISKSHyperchole, HTN, DMTobbacco(+) FH, Obesity
MACE = AMI, PCI, CABG, (+) cath, death

HEART Pathway Randomized Trial
▪ 282 ED suspected ACS patients, randomized to HEART or standard tx
▪ HEART N=141, with score < 4, negative Tn at 0 and 3 hours▪ 75 low risk, 56 discharged
▪ Standard care N=141, per ACC/AHA guidelines▪ X low risk, 26 discharged.
▪ Results: No MACE in either arm▪ HEART lower objective cardiac testing; 68.8 vs 56.7% (P=0.048)▪ lower LOS; 9.9 vs 21.9 hours (P=0.013)▪ higher early discharges by 21.3% (39.7% versus 18.4%; P<0.001).
Mahler S. Circ Cardiovasc Qual Outcomes. 2015 March ; 8(2): 195–203

EDACS-ADPEmergency Department Assessment Chest Pain Score -Accelerated Diagnostic Procedure
Characteristic Parameter Points
History 18-50 yo with CAD, or >2 risk factors
+4
Age 18-45 +2
46-50 +4
51-55 +6
56-60 +8
61-65 +10
66-70 +12
71-75 +14
76-80 +16
81-85 +18
>85 +20
Characteristic Parameter Points
Sex Male +6
Signs and Symptoms
Diaphoresis +3
Arm or shoulder radiation
+5
Painoccurred or worsened with inspiration
-4
Pain is reproduced with palpation
-6
Low Risk Criteria§EDACS Score <16§No new ECG ischemia §Negative 0 and 2h Tn

PEARLComparing Scores
▪ PEARL data set: 7 EdsN=458
▪ Patient with suspected ACS
▪ Dr documented risk of MI before Tn results asLow, Moderate, or High
TIMI
GRACE
HEART-2
EDACS
HEART-1
Singer A. Am JEM, 2017, Jan 5. pii: S0735-6757(17)30003-7. doi: 10.1016/j.ajem.2017.01.003. [Epub ahead of print]

Scores: standard cutpointLow risk
definition
N % with AMI Sensitivity
Clinical Low 136 5.9 (3.0-11.2) 88.7 (78.5-94.7)
HEART 0-3 146 4.1 (1.9-8.7) 91.5 (81.9-96.5)
TIMI 0 26 0 (0-12.9) 100 (93.6-100)
GRACE <51 14 7.1 (1.3-31.5) 98.6 (91.4-99.9)
EDACS <16 195 1.0 (0.2-4.1) 97.1 (89.1-99.5)
Singer A. Am J EM. 2017 Jan 5. pii: S0735-6757(17)30003-7. doi: 10.1016/j.ajem.2017.01.003.

Performance: Sensitivity set at 99% Sensitivity set at 99%
Cutoff % Low Risk Clinical -- --HEART-1 0 1HEART-2 0-2 18.9TIMI 0 7GRACE 49 3.2EDACS 12 34.3
Singer A. Am J EM. 2017 Jan 5. pii: S0735-6757(17)30003-7. doi: 10.1016/j.ajem.2017.01.003.

How many will the ADP D/C?10.4 million annual ER CP 3500 USA ER’s
ED D/C rate # of patients7.0 (TIMI) 728,000
18.9 (HEART) 1,965,60034.3 (EDACS) 3,567,20077% (TRAPID) 8,008,000

HighSensitivityTroponinintheUSA
• FDAclearsbloodtesttohelpdiagnosepatientswithasuspectedMI
• Jan19,2017– TheFDAgranteda510(k)clearancefortheElecsys TroponinTGen5STATbloodtestforpatientswithasuspectedMI.

Patie
nts
Dis
char
ged
Early
(%)
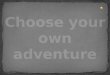
1) Than M, Cullen L, Reid C, et al. Lancet. 2011;377:1077-84. 2) Than M, Cullen L, Aldous S, et al. J Am Coll Cardiol. 2012;59(23):2091-8.3) Cullen L, Mueller C, Parsonage WA, et al. J am Coll Cardiol. 2013;62(14):1242-9. 4) Mueller C, Giannitsis E, Christ M, et al. Ann Emerg Med. 2016;68(1):76-87.
TRAPID-AMI4cTnT ≤ 12 ng/L; Δ1 hour ≤ 3 ng/L
APACE3
cTnI ≤ 26.2 ng/LASPECT1
cTnI ≤ 50 ng/LADAPT2
cTnI ≤ 30 ng/L
70
60
50
40
30
20
10
0
Increased Troponin Sensitivity = More ED Discharges
38.6
20.0
63.4
9.8

2015 ESC Guidelines
▪ The NPV for MI in patients assigned ‘rule-out’ exceeded 98% in several large validation cohorts
Eur Heart J. 2016Jan 14;37(3):267-315.

Will the ESC guidelines work in the US?
▪ hscTnT and I at 0 and 3 h post-presentation
▪ Purpose: validate the ESC Working Group on Acute Cardiac Care rule-in algorithm
1061 hsTnI985 hsTnT
Sn of 99th %ileto R/O AMIHsTnI 93.2%HsTnT 94.8%
Pickering JW, et al. Heart 2016;0:1–9.

How quickly can I make a decision?
▪ECG… 10’▪Tn (central lab)… 90’
▪Risk Score (EDACS)▪Some admitted
▪Repeat Tn @ 3 hrs▪Returns for decision…. ~4 hours