Embed Size (px)
Citation preview
C S R M A N A G E M E N T
I H A B A B D E L A Z I Z , M D F R C S A L - M A S H R E Q E Y E C E N T E R M E M O R I A L I N S T I T U T E O F O P H T H A L M O L O G Y
CSR To understand the way of management we have to understand the disease.
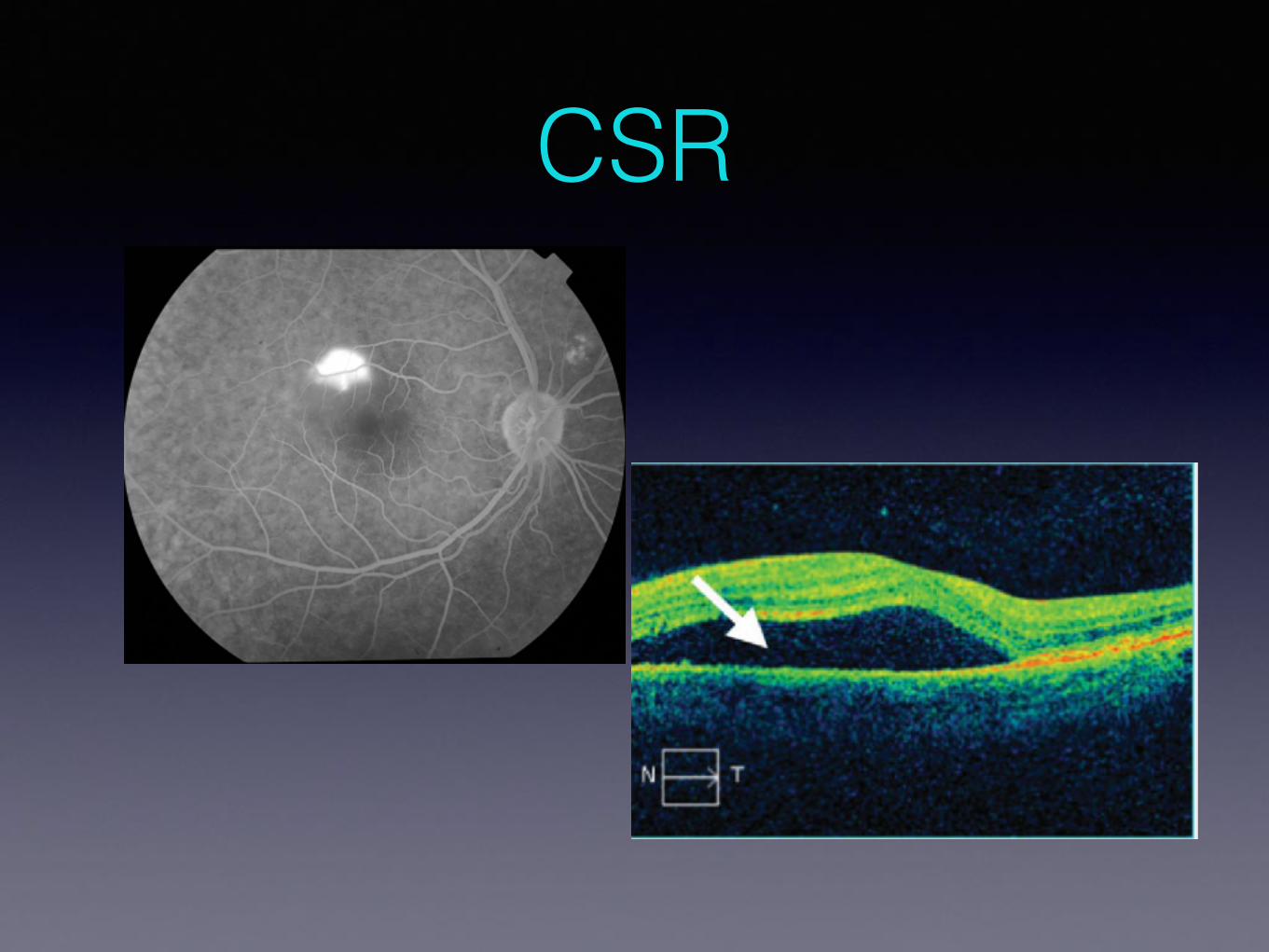
• The Central serous retinopathy (CSR) is reversible condition characterized by
• NSD• PED• blurred or distorted central vision.
It results from idiopathic leakage at the level of the RPE
CSR
CSR Pathophysiology The underlying pathophysiology is not completely understood but their are many
theories which involve :
1.functional or structural defect in the fluid-pumping capabilities (RPE).
2.Abnormalities of choroidal circulation including venous congestion, lobular ischemia (blood flow reduction by OCT-A) and multiple areas of hyper-permeability have been seen by (ICGA) might indicate increased hydrostatic pressure in the choroid.
3. OCT EDI showed increased choroidal thickness.
4.Patients with systemic inflammatory disease receiving steroids are at an increased risk to develop this condition.
5.Increased endogenous or exogenous glucocorticoid levels are an important risk factor.
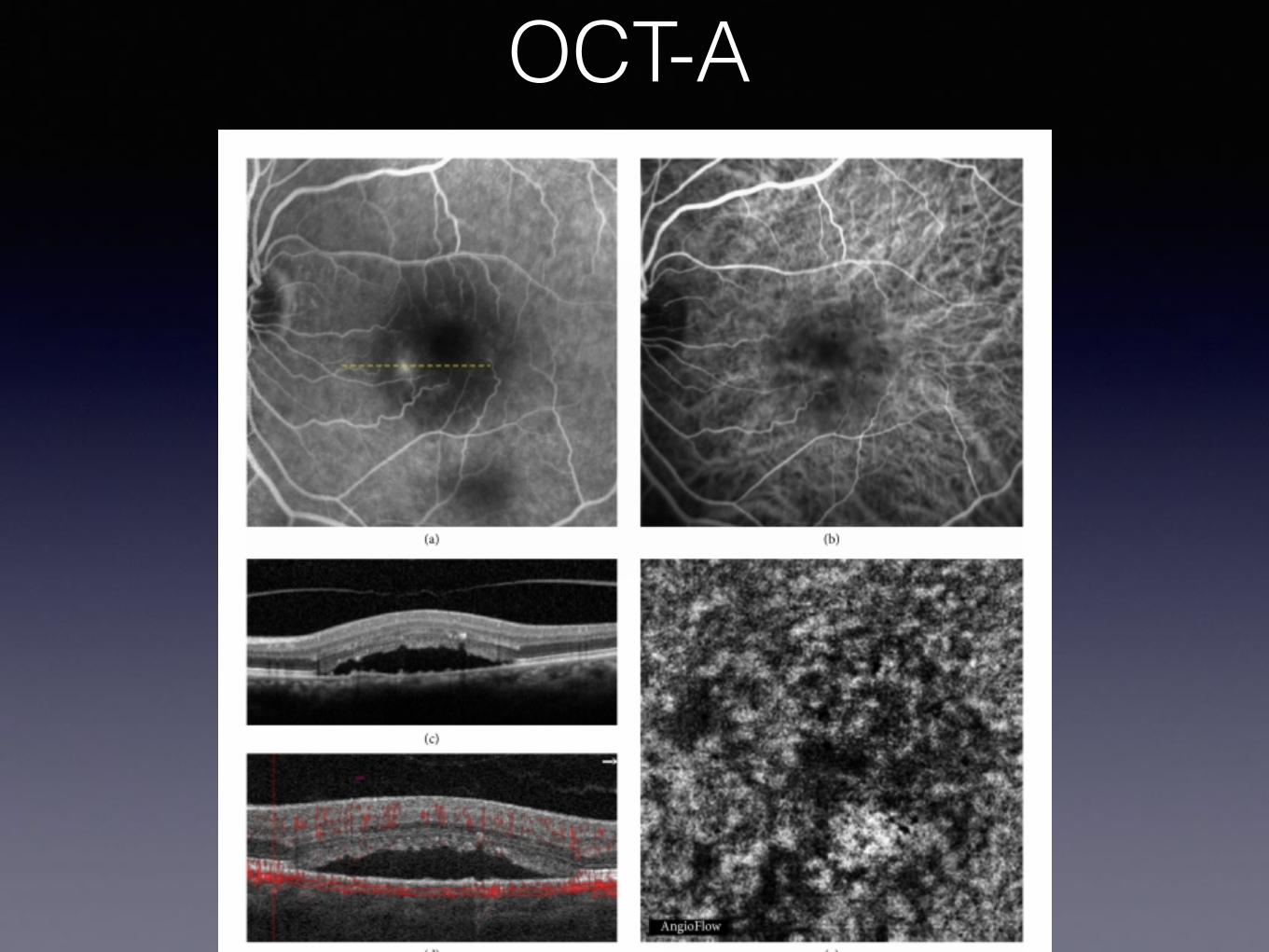
OCT-A
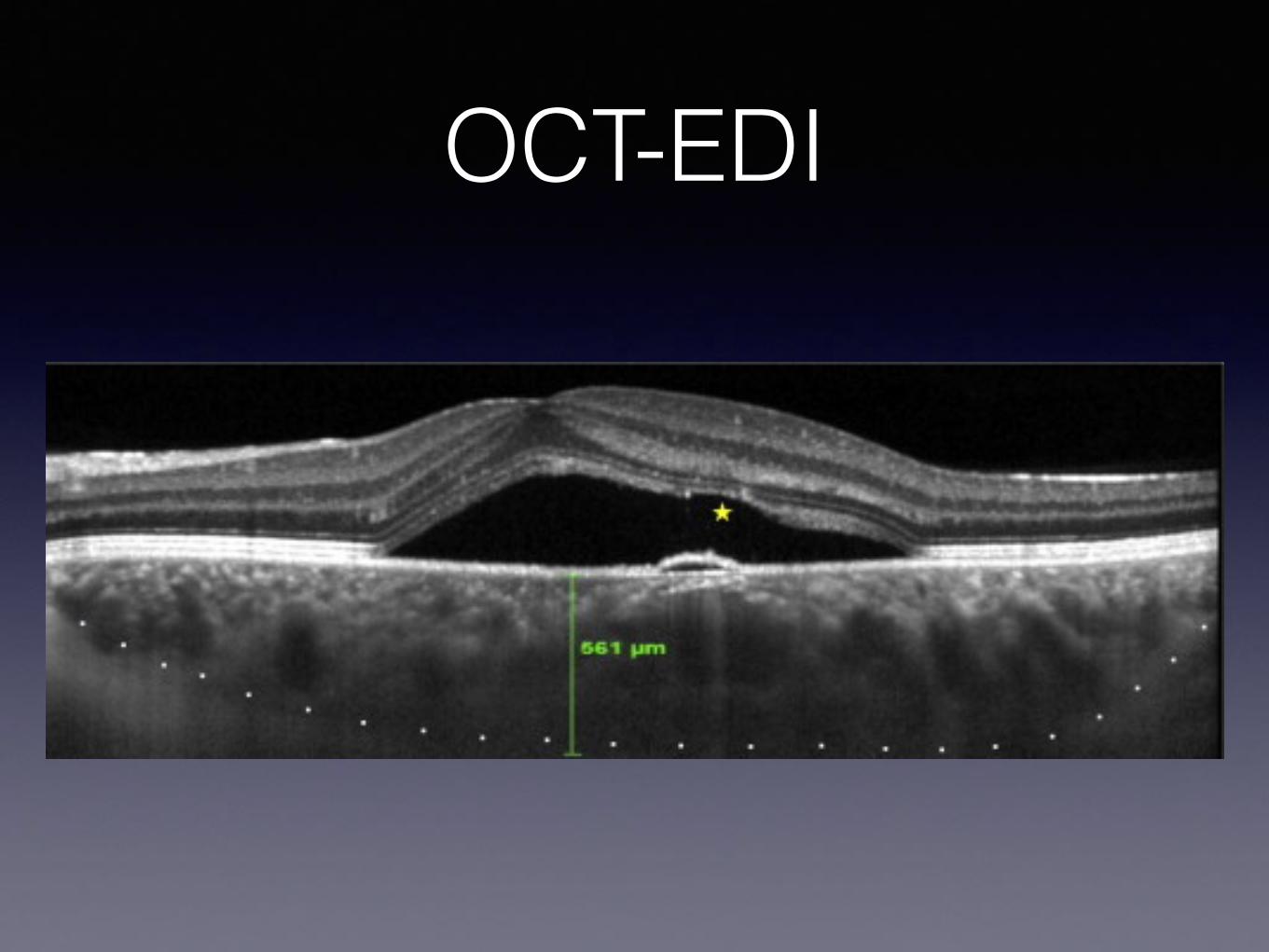
OCT-EDI
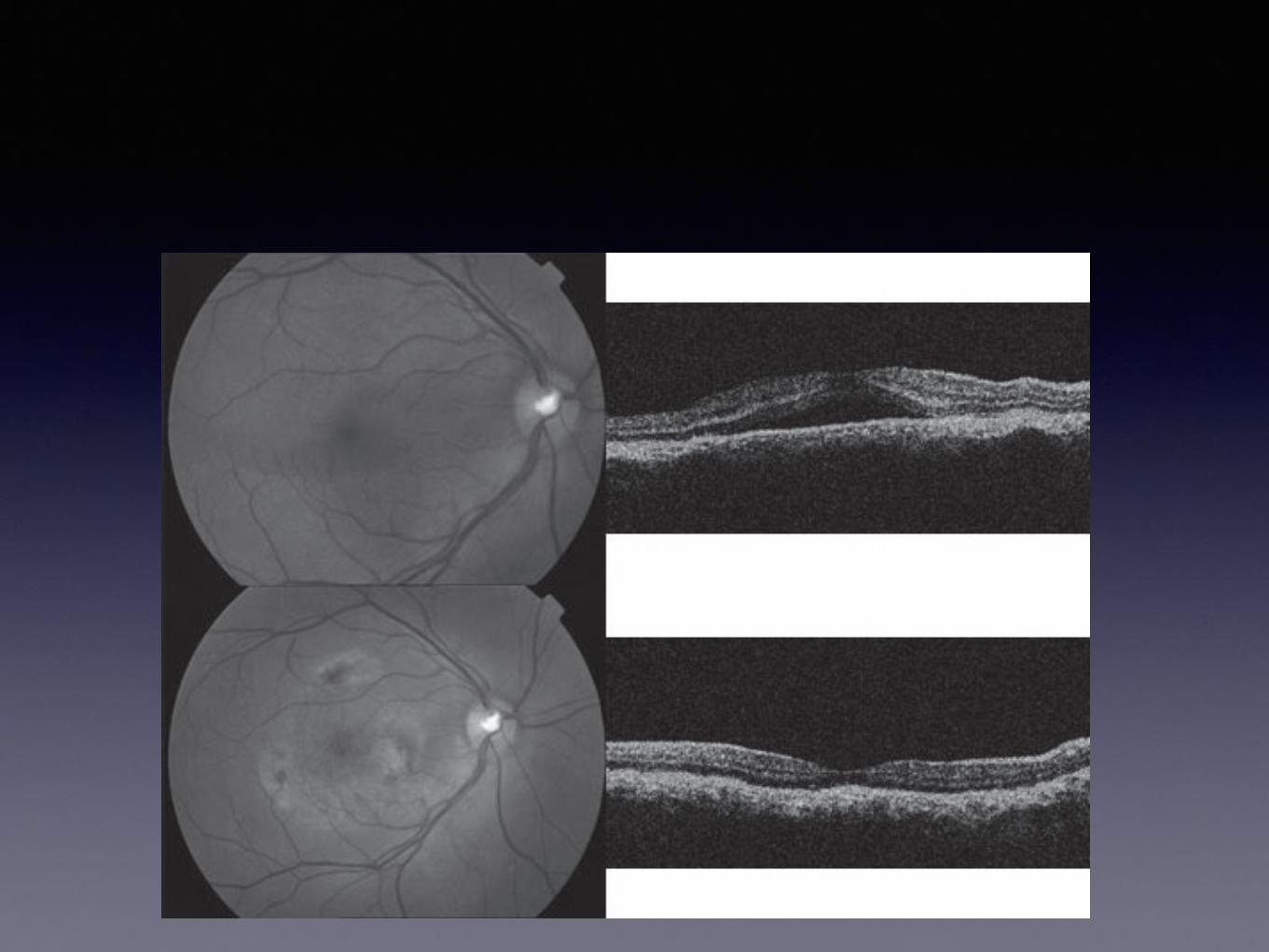
Chronic CSR• Fluid persists more than 6 month
• Occasionally, the NSD persists and leads to pigment epithelial and photoreceptor damage with visual impairment.
• Chronic cases of CSC may yield further complications such as descending atrophic tracts, dependent retinal detachment, cystoid macular edema,cystoid, secondary CNV, and fibrous scarring
CSR TTT
Fortunately, the disorder is self-limited in the majority of patients so observation and discontinuation or marked tapering of corticosteroids is the treatment of choice in most patients, as the natural history is one of spontaneous resolution with the regain of excellent vision
TTT modalities
• Photodynamic therapy (PDT)• Mineralocorticoid receptor (MR) antagonist eg.
Spironolactone • Intra vitreal injection of anti-VGEF• Argon laser photocoagulation• Micropulse laser
PDT • Choriocapillaris thrombosis, changes in the vascularization
pattern and decreased vascular permeability have been demonstrated
• Verteporfin may be deposited within the serous fluid under the macula and its activation may release free radicals and pro-inflammatory factors that induce a permanent adhesion between the neurosensory retina and RPE.
• Less destructive
PDT• 82 eyes in 72 patients treated with PDTcomplete disappearance of SRF in all cases, demonstrated by OCT
and FA with success rates of 100%.
• BCVA had improved in 67% of eyes at the end of follow-upTwo eyes in our series had recurrent CSC after PDT during follow-up69 eyes required a single PDT session.
• None of the patients showed adverse events after PDT or severe vision loss,
• The reduction in macular thickness was also statistically significant falling from 330 lm (SD 91) before PDT to 187 lm (SD 52) at the end of followup.
Francisco L. Lugo et al 2009
Reduced dose PDT • Pilot study by Lai et al. using half dose verteporfin for chronic CSCR has
demonstrated both efficacy and safety.
• Chan et al. have shown in an RCT that included patients that half dose PDT was also effective both anatomically and functionally in treating acute symptomatic CSCR.
• A comparative case series by Lim et al. have shown that half dose PDT facilitated earlier resolution of SRF and earlier recovery of visual function when compared to focal laser.
• Ratanasukon et al. concluded that about 45% of CSCR patients treated with half dose PDT had photoreceptor disruption at 1-year follow-up.
• Availability.
Spironolactone • Anti-Glucocorticoid
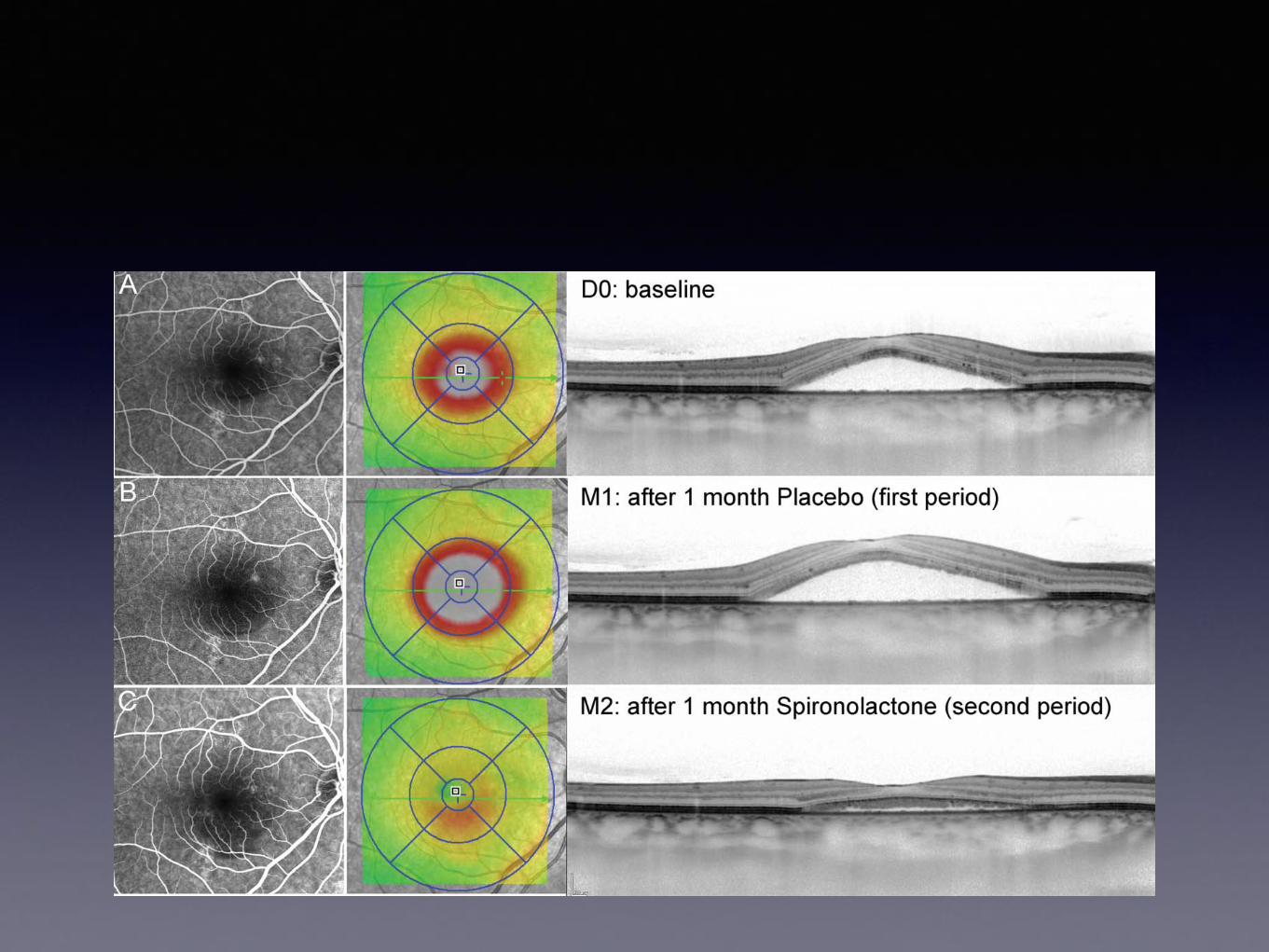
• Sixteen eyes of 16 patients evaluate the effect of MR antagonist spironolactone administered orally, against placebo on SRF in nonresolving CSCR.
• The results demonstrated a significant reduction of SRF in treated eyes.
• The limitations of this study are the non optimal dosage per patient
• (ELODIE BOUSQUET,et al 2015)
Other anti-glucocroticoid
Epelernone, Finasteride, Rifpmacin
IV AntiVegf Injetion 9 of the 12 patients (response group) show absorption of SRF
• Twelve eyes in 12 patients (Chih-Hsin Chen, et al 2013) 9 of the 12 patients (responder group) show absorption of SRF.
There were three cases showing increased SRF after intravitreal bevacizumab injection (nonresponder group)
In the responsonder group, six patients showed stable CMT for_6months . However, three of the nine patients in the response group had a relapse of SRF at 3months follow-up.
Two of the three patients with recurrences received secondary intravitreal bevacizumab injection, and SRF was absorbed within 1 month after the secondary injection.
3 months later, recurrences with SRF accumulation was noted again in these two patients.
In conclusion:• Intravitreal bevacizumab injections provide only short-term effects in SRF
absorption in some cases, even if they are sensitive to the treatment.• Bevacizumab injection is not always an effective treatment modality for all patients
with chronic CSCR
Argon Laser Treatment 9 of the 12 patients (response group) show absorption of SRF• Applying laser photocoagulation to the leaking RPE guided by FA has been enhance
resolution of the neurosensory detachment in CSCR.
• Argon laser is more widely used. Many studies have demonstrated faster resolution of SRF in patients who underwent laser photocoagulation compared to control eyes.
• Nevertheless laser photocoagulation does not influence the final visual outcome or rate of recurrence.
In conclusion:• Therefore, argon laser photocoagulation is an effective treatment for
acute CSCR with clearly defined focal leakage point as seen on FA given that the leakage is not subfoveal or juxtafoveal.
• Side effects such as permanent scotoma, laser scar enlargement, and laser induced CNV .
To My opinion
• When their are focal dye leakage at the level of RPE (extra foveall) consider laser treatment, PDT.
• When the fovea is involved consider PDT, AntiVEGF injection,• When their are pachychoroid, use either PDT , antiVegf, are the TTT of
choice.• PDT has good influence in Visual outcome more than Laser treatment.• Argon laser has significant side effects more than PDT.• Medical TTT is coming.