Embed Size (px)
Citation preview
HISTORICAL RESEARCH REPORTResearch Report TM/89/06
1989
Ergonomic studies of keyboard operators with soft tissue disorders Love RG, Symes AM, Soutar CA

Copyright © 2006 Institute of Occupational Medicine. INSTITUTE OF OCCUPATIONAL MEDICINE No part of this publication may be reproduced, stored Research Avenue North, Riccarton, Edinburgh, EH14 4AP or transmitted in any form or by any means without Tel: +44 (0)870 850 5131 Fax: +44 (0)870 850 5132 written permission from the IOM e-mail [email protected]
Ergonomic studies of keyboard operators with soft tissue disorders
Love RG, Symes AM, Soutar CA This document is a facsimile of an original copy of the report, which has been scanned as an image, with searchable text. Because the quality of this scanned image is determined by the clarity of the original text pages, there may be variations in the overall appearance of pages within the report. The scanning of this and the other historical reports in the Research Reports series was funded by a grant from the Wellcome Trust. The IOM’s research reports are freely available for download as PDF files from our web site: http://www.iom-world.org/research/libraryentry.php
HISTORICAL RESEARCH REPORTResearch Report TM/89/06
1989

ii Research Report TM/89/06
Report No. TM/89/06UDC 616.74
Ergonomic studies ofkeyboard operators withsoft tissue disorders
LOVE RCSYMES AMSOUTAR CA
November 1989
Price:£40.00 (UK)£45.00 (Overseas)
(iii)
Report No. TM/89/06HSE Contract 1/MS/126/585/85
INSTITUTE OF OCCUPATIONAL MEDICINE
ERGONOMIC STUDIES OF KEYBOARD OPERATORSWITH SOFT TISSUE DISORDERS.
by
R.G. Love, A.M. Symes, C.A. Soutar
Institute of Occupational Medicine8 Roxburgh PlaceEDINBURGHEH8 9SU
Tel: 031 667 5131Telex: 9312100237=TD GFax: 031 667 0136 November 1989
This report is one of a series of Technical Memoranda (TM) published by theInstitute of Occupational Medicine. Current and earlier lists of these reports, andof other Institute publications are available from the Librarian/Information Officerat the address overleaf.
For further information about the Institute's facilities for research, service/consultancy and teaching please contact the Librarian/Information Officer in thefirst instance.
(iv)
CONTENTS
SUMMARY
1. INTRODUCTION 1
2. METHODS 3
2.1 Subjects 32.2 Ergonomic assessments 3
3. RESULTS 5
4. DISCUSSION 7
ACKNOWLEDGEMENTS 9REFERENCE 11TABLE 12APPENDIX 13
(v)
SUMMARY
We have carried out a descriptive ergonomic case study of a small group ofkeyboard operators with soft tissue disorders of the upper limb, identified in anearlier epidemiological study, of the influence of work activities on risk of softtissue disorders.
The aims of the study were to determine (1) what activities at work required thespecific movements we found in our earlier study to be associated with risk of softtissue disorders; (2) what ergonomic factors might have contributed to the risk, and(3) what, if any, modifications to equipment or working practices were suggested bythese observations.
Out of seventeen cases invited, nine agreed to participate, three of whom werestudied at their place of work. Subjects were observed at work or interviewed athome. In only one case did it appear that operating the keyboard itself requiredone of the movements previously found to be associated with risk of soft tissuedisorder (in this case, keeping the thumb flexed); instead these risky movementsappeared to be required by other activities that keyboard operators do, such asturning the roller on a manual typewriter, turning pages, operating a hole punchingmachine, gripping a pen tightly, and lifting heavy files above the head. Falls ontothe hands outside work also sometimes preceded the chronic condition.Ergonomically unsound postures related to poor positioning of seats and equipmentwere common in the group.
This small case study has generated the hypothesis that the excess of soft tissuedisorders in keyboard operators is partly the result of the ancillary, non-keyboard,activities that keyboard operators do, possibly initiating some tissue damage whichmay then be exacerbated by keyboard operation. If this is true, modifying oravoiding some of the ancillary activities might be beneficial. Additionally, it maybe helpful to determine the benefit of a period of rest after falls on the hands,before manual work is resumed. Lastly, attention to ergonomic principles in theprovision of seats and positioning of equipment is likely to be advantageous.

1
1. INTRODUCTION
A case-control study of the influence of occupation on upper limb soft tissuedisorders was recently reported (English et al, 1989). Jobs significantlyover-represented among these cases compared with controls were cleaners,hairdressers, butchers, musicians, machine operators, VDU operators and otherkeyboard users. Cleaners and keyboard users were the occupations most frequentlyreporting upper limb disorders.
Some specific movements associated with soft tissue disorders were identified,suggesting opportunities for task modification or equipment redesign to reduce therisks of injury: Notably, repetitive pinching between thumb and finger, sustainingthe thumb in a bent position, and higher rates of flexion/extension of the wristwere associated with thumb conditions; repetitive gripping in the palm with fingerconditions; keeping the thumb bent, repeated wrist supination/pronation and forcefulelbow flexion, with wrist or forearm conditions, and rotation of the shoulder witharm raised, with shoulder conditions.
We have now carried out ergonomic studies of some of the keyboard operatorswith soft tissue disorders, identified in our previous study, in order to determine;(1) what activities at work required the specific movements we found to beassociated with risk of soft tissue disorders; (2) what ergonomic factors might havecontributed to the risks, and (3) what, if any, modifications to equipment orworking practices were suggested by these observations.
3
2. METHODS
A descriptive ergonomic case study was carried out as follows:
2.1 Subjects
All cases of upper limb disorder, who had satisfied the diagnostic criteria of ourprevious study, had attended the orthopaedic clinic in Edinburgh and were currentlyor had recently been keyboard users, formed the study group. There wereseventeen cases in Edinburgh who worked in jobs likely to involve use ofkeyboards (sixteen women and one man). These were secretary (8), typist (5),and computer operator (4). They were invited by post to participate in theseadditional studies. Consent was sought for agreement to approach their employer,so that an ergonomist could make observations at their workplace. We specifiedthat an individual's name would not be revealed to an employer without consent.It had been hoped that the local Employment Medical Adviser would be able toapproach individual employers to obtain consent for access to their premises butthis did not prove to be possible. We therefore contacted employers directly,usually through the personnel department.
Eight subjects were willing for us to contact their employers; five were unwilling,one had left the area and four either did not reply or were unobtainable (notknown at last address). Two of the subjects were unwilling because they did notwant to risk being identified by their employers.
Eight employers were contacted and only three agreed to take part, in spite ofrepeated contacts from ourselves. In addition to the three subjects whoseemployers were willing to take part, six subjects (five of whom had consented tous approaching their employers) were willing to be interviewed. In total nine ofthe original seventeen cases (all women) were seen at or away from theirworkplace.
2.2 Ergonomic assessments
Subjects seen at their workplace were informed of the nature of the study. Videorecordings of the tasks they currently performed were made or, where the subject'sjob had changed since her interview at the orthopaedic clinic, of other workersundertaking similar duties. These subjects were interviewed in more detail abouttheir current and past work activities, the nature of their working environment anddesign of the workstation, relevant pastimes and hobbies and their own assessmentof the possible association between their injury and work activities or other events.
Subjects who agreed to be interviewed away from work were asked a similar rangeof questions, which were designed to allow the subject to volunteer as muchrelevant information as possible. Where appropriate video recordings were. used toassess postures, use of equipment (for repetitive or forceful movements) and in onecase observation of a workplace similar to the one used by a subject who hadchanged jobs.
Information reported by the subjects at their clinic interview on specificmovements, repetition rates and postures was used to supplement this further data.In particular question 4, which asked about finger tapping movements, establishedthe number of finger keystrokes per minute by multiplying the subject's knowntyping speed by five (the average number of letters per word). The presence orabsence of movements, which had been found to be significant risk factors for thetype of disorder reported by these subjects, was also noted. These were:repetitive pinching, sustained bent thumb and high rates of flexing/extending thewrist for thumb conditions; repetitive gripping in the palm for finger conditions;sustained bent thumb, repetitive wrist supination/pronation and forcefullyflexing/extending the elbow for wrist conditions.
5
3. RESULTS
Three subjects were examined at their place of work, though only one of thesewas carrying out the same job in the same organisation as that performed at thetime of recruitment into the earlier study 21-32 months previously. Another sixsubjects were interviewed away from their place of work. They were all stillemployed in the same jobs as at the time of interview, except one who had leftto have a baby. All subjects were female, and all were right handed. Their agesranged from 19 to 59 years, and when they first developed symptoms had workedin their current job for between 1 and 19 years. Their injuries consisted of deQuervain's tenovaginitis of the extensor tendons of the thumb in three subjects(bilateral in one), carpal tunnel syndrome in two subjects, ganglia (one wrist andone middle finger) in two, trigger thumb, and osteoarthritis of the firstmetacarpophalangeal joint.
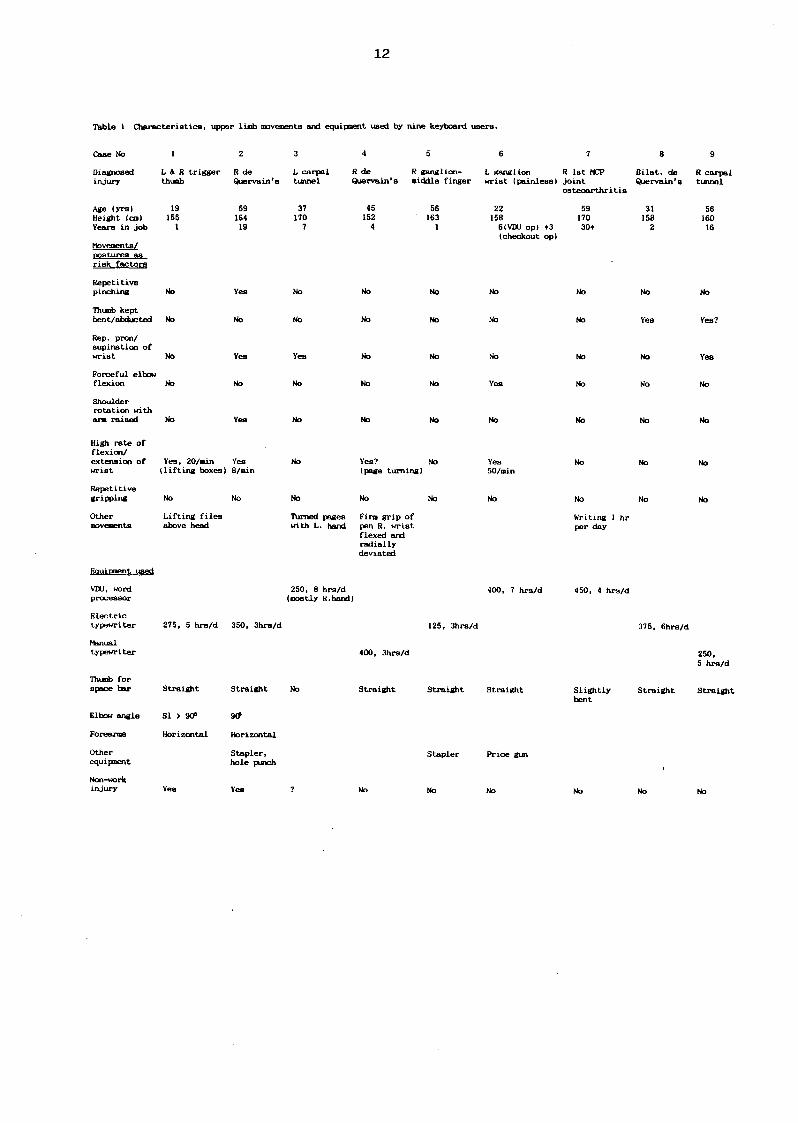
At the time symptoms commenced, three were using word processors or othervideo display terminal, four were using an electric typewriter, and two a manualtypewriter. Characteristics of these subjects and their work related movements aregiven in Table 1. More detailed descriptions are given for each case in theAppendix.
Thumb conditions
In our earlier study we showed that conditions of the thumb were in generalassociated with repetitive pinching between thumb and forefinger, sustaining thethumb in a flexed position, and with higher rates of repetitive flexion/extension ofthe wrist. Of the five subjects in the present study with conditions of the thumb,two performed pinching movements repetitively. In neither of these was pinchingassociated directly with keyboard use; in one the handle of a hole punchingmachine (for papers) had to be screwed up forcibly using a pinch grip, for up to3 hours a day; in the others, pinching was associated with writing with a ball pointpen up to three hours per day, gripping the pen tightly with the wrist flexed andradially deviated. One sustained a flexed thumb while operating the space bar onthe keyboard, and two flexed the wrists, one at high rates of repetition, whileperforming non-typing activities (stacking file boxes, hole punching).
All subjects used their thumb (usually straight) to depress the space bar, and thiswas brought about by abduction of the right thumb rather than by rotating thewrist.
Two of these subjects reported that a fall on the outstretched thumbs precededsymptoms, which were subsequently exacerbated by activities at work.
Wrist conditions
The earlier study also showed that conditions of the wrist and forearm wereassociated with keeping the thumb flexed, repeated supination/pronation of thewrist, and forceful repetitive elbow flexion. Of the three subjects with wristconditions in the present study, two repetitively pronated/extended the wrist. Inone this was while turning the typewriter roller to insert paper, in the other whileturning pages with the left hand while entering data with the right hand (theinjury was on the left). One flexed her elbow forcibly while doing a second jobas supermarket checkout operator, pulling purchases past her with her left hand.
Finger conditions
The earlier study showed that finger conditions were associated with repetitivepalmar gripping. The one subject with a finger condition (ganglion) in the presentstudy did not report any gripping activities at work.
Summary of results
The study has explained in part what operations performed by keyboard operatorsrequire the movements found in our earlier study to be associated with risk ofinjury. These operations mostly did not include direct operation of the keyboard,except for keeping the thumb flexed when depressing the space bar. We note thatdepressing the space bar with the thumb requires abduction of the thumb at thefirst metacarpophalangeal joint, a movement which was not studied in our previousresearch. Thus the high risk activities were mostly other tasks that keyboardoperators do, turning the roller on a manual typewriter, operating a hole punch,turning pages, using a ball-point pen with an uncomfortable grip, lifting heavy filesoverhead, or doing a second job as checkout operator (also suspected of beingassociated with increased risk of soft tissue disorders). In two subjects, fallsoutside work appeared to have caused the initial injury.
7
4. DISCUSSION
Participation in the study was incomplete, and we do not know what additionalinformation would have been provided by the non-responders. Since this was adescriptive case study, not an epidemiological study, the observations made on theparticipants nevertheless provide useful, if incomplete, information.
This study of a small group of keyboard operators with soft tissue disorders of theupper limb has gone some way to explaining what activities at work require thespecific movements which we had earlier shown to be in general associated withsoft tissue disorders. In only one case did it appear that operating the keyboarditself required one of these risky movements (in this case keeping the thumbflexed); instead, these risky movements appeared to be required by other activitiesthat keyboard operators do, such as turning the roller on a manual typewriter,turning pages, operating a hole punching machine, gripping a pen tightly and liftingheavy files above the head. Falls onto the hands outside work may also initiatean injury which is subsequently exacerbated by work. Ergonomically unsoundpostures related to poor positioning of seats and equipment were common in thisgroup, and probaly contributed to the risks of injury.
Since we previously confirmed (English et al, 1989) an excess of soft tissuedisorders in keyboard operators, the present results tend to suggest either; that thisis the result, not of operating a keyboard, but of the ancillary activities thatkeyboard operators do; or that a combination of trauma from ancillary activities(and non-work activities) with repetitive movements during keyboard operationprecipitates these disorders.
Incidentally, and in view of the frequency with which the thumb is affected bythese disorders, we note that the thumb is used repetitively to depress the spacebar or the keyboard, by abduction of the thumb at the first metacarpophalangealjoint. We do not know whether this movement is associated with risk of injurysince in our previous work we studied many movements but not this one, and wehope to remedy this omission in due course.
Thus the results of this small study have generated some hypotheses, which couldbe tested in future studies; (1) keyboard users' ancillary activities may contributeto risk of injury, and some benefit may be obtained by studying how theseactivities might be modified or avoided: (2) Injuries sustained outside work may insome cases predispose to chronic soft tissue disorders in keyboard operators.Possibly a period of rest after such injuries, before normal work is resumed, couldbe beneficial. Lastly we note that the postures of these workers were frequentlyincorrect, according to standard ergonomic principles, and attention to the seatingand positioning of equipment used by keyboard operators is likely to help preventthese disorders.
9
ACKNOWLEDGEMENTS
We thank the Health and Safety Executive for their continued financial support,the subjects who participated and the employers who allowed us to visit theirpremises. We also thank Mr R J Graves and Dr R A Graveling for usefuldiscussions and other contributions and Miss A Lobban for typing the report.

10
11REFERENCE
English CJ, Maclaren WM, Court-Brown C, Hughes SPF, Porter RW, WallaceWA, Graves RJ, Pethick AJ, Soutar CA. Clinical epidemiological study ofrelations between upper limb soft tissue disorders and repetitive movements atwork. Edinburgh: Institute of Occupational Medicine (IOM Report No. TM/88/19).
12
Table 1 Characteristics, upper limb movements and equipment used by nine keyboard users.
Case No
Diagnosedinjury
Age (yrs)Height (cm)Years in job
Movements/postures asrisk factors
Repetitivepinching
Thumb keptbent/abducted
Rep. pron/aupination ofwrist
Forceful elbowflexion
Shoulderrotation witham raised
High rate offlexion/extension ofwrist
Repetitivegripping
Othermovements
Equipment used
VDU, wordprocessor
Electrictypewriter
Manualtypewriter
Thumb forspace bar
Elbow angle
Forearms
Otherequipment
Non-workinjury
L & R trigger R de L carpal R de R ganglion-thumb Quervain'a tunnel Quervain's middle finger
19 59 37 45 56155 164 170 152 163
1 1 9 7 4 1
No Yes No No No
No No No No No
No Yes Yes No No
No No No No No
No Yea No No No
Yea, 20/min Yes No Yes? No(lifting boxes) 8/min (page turning)
No No No No No
Lifting files Turned pages Firm grip ofabove head with L. hand pen R. wrist
flexed andradiallydeviated
250, 8 hrs/d(mostly R.hand)
275, 5 hrs/d 350, 3hrs/d 125, 3hrs/d
400, 3hrs/d
Straight Straight No Straight Straight
SI > 90* 90»
Horizontal Horizontal
Stapler, Staplerhole punch
Yes Yes ? No No
L ganglion R 1st MCPwrist (painless) joint
osteoarthritis
22 59158 1706(VDU op) +3 30+(checkout op)
No No
No No
No No
Yes No
No No
Yes No50/min
No No
Writing 1 hrper day
400, 7 hrs/d 450, 4 hra/d
Straight Slightlybent
Price gun
No No
Bilat. de R carpalQuervain's tunnel
311582
No
5616016
No
Yes?
Yes
No
No
No
No
375, 6hrs/d
250,5 hrs/d
Straight Straight
No
13
APPENDIX
Case Descriptions
Subjects examined at the workplace.
Case 1: Secretary
This worker is a 19 year old secretary in the commercial department of a largebrewing company. She is 155cm tall. Since leaving school four years ago, shehas worked for the same company as a secretary but at the time of the clinicinterview 32 months earlier had worked in a different department. At the timeshe had attended the orthopaedic clinic, trigger thumb of the left hand wasdiagnosed.
Her work tasks were typing on an electric typewriter (at 275 keystrokes perminute) for five hours per day, occasionally lifting and carrying files and generalclerical work.
She revealed that she had also had trigger thumb of the right hand but had onlybeen treated for the left thumb surgically. She stated that the condition originatedfrom an accident on a skateboard three years ago, in which she had fallen offbackwards and taken the weight of her fall on her thumbs.
However, (additional to lighter lifting activities) she had to lift heavy file boxes andpiles of folders to about 50cm above head height twice a day. This necessitated apalmar grip, sometimes changed so that she took the weight on her thumbs in apinch grip. This occurred during a six month period and caused soreness in boththumbs after she had the injury because of the firm grip she had to adopt. Shehad found her workplace (desk and surrounding office layout) restricted hermovements, causing her to stretch backwards or forwards to reach the telephoneand other objects on and around her desk. Her seat was not adjustable. In herpresent job her seat is adjustable and her working environment, an open planoffice, is more comfortable than before. In her present job as a secretary/typistshe was observed on the video recording to adopt an upright sitting posture duringtyping, her elbow angle was slightly greater than 90°, her forearms horizontal andhands held slightly ulnar-deviated. She only abducted her straight right thumb tooperate the space bar without force and the left thumb was kept straight and notused at all.
She has recently been treated for a back problem which resulted, she thinks, fromcarrying cardboard trays of two dozen beer cans from time to time. It is possiblethat, as a result of her thumb injuries, she had adopted an unsatisfactory posturewhile lifting, in which she had been given no specific training.
Re: identifed risk factors, she did not use repetitive pinching movements more thanonce per minute nor sustain a bent thumb position but she did flex and extendher wrists 20 times per minute for two hours per day when lifting file boxes.
14
We conclude that she may have acquired her disorder as the result of anon-occupational accident and that occupational activities (lifting heavy boxes)aggravated it because of the height to which she had to raise her arms whenlifting boxes and sustaining a pinch grip. The mode of operation of the keyboardof her typewriter did not suggest that this activity contributed to her disorder,except for flexion/extension of the wrist, an identified risk factor for these injuries.
Case 2: Secretary
She is a 59 year old secretary in an office in a public library, where she hasworked for nineteen years. She is 164cm tall. Two and a half years previouslyshe had attended the orthopaedic clinic, where she was diagnosed as having chronictenosynovitis of the right thumb and wrist (De Quervain's disease). Her rightforefinger was slightly deformed and she stated that the clinic's radiograph of herwrist had shown several small fractures in the first metacarpal of the rightforefinger, which she thought could have been caused by constant use of thetelephone dial. Her work tasks involve mostly typing on an electric typewriter,answering the telephone, using a stapler and a hole punch as well as collating andgeneral clerical work.
A few months before her symptoms were reported she had fallen outside and takenthe weight of her fall on her hands. Nevertheless there are a number of featuresof her work which are potentially relevant to her condition.
She was observed to use a device for punching three holes through thick files ofpaper. Its operation requires her to stand bent forward over a desk and, using herright arm with elbow raised, to grip the operating handle between thumb andforefinger (pinch grip), forcibly turning the handle as if using a tap. This requiredabout sixteen turns for each hole but could be more for thicker files. Each holewas punched in turn and the handles released by reverse turning using left or righthand. Once the handle was partially loosened she used her right forefinger tocontinue to release the hole punchers. This task was performed several timesduring a week and could at times continue all morning. She occasionally used ahand-pressure operated two-hole punch with her left hand for 1-2 hours per day.
During typing she was observed on the video recording to lean forward because thedesk was too low. When typing her forearms were horizontal and her elbow anglewas about 90°. She kept her fingers in a bent position while typing and she usedher right thumb, held in a straight position, to operate the space bar at the frontof the keyboard. She typed at a rate of 350 keystrokes per minute for threehours each day on average, and for up to 3 hours at a time. Her desk layoutwas in the shape of a left handed L which required her to twist backwards in herseat to answer the telephone. She also had to apply considerable force downwardswith her arms when operating a stapler repetitively during collation of papers,which she did on average twice a week. In order to do this she had to raise hershoulders and arms, while bent over the stapler to provide sufficient downwardforce.
Re: identified risk factors, she used repetitive pinching movements when operatinga hole punch but did not sustain a bent thumb. She flexed and extended herwrist eight times per minute for an hour each day.
We conclude that, although she had a non-occupational fall onto her hands, whichmight have weakened the more distal joints and soft tissues of her arm, therepetitive and forceful right-handed action of the hole punch is most likely to havebeen associated with the chronic tenosynovitis in her thumb and wrist. Using her
15
thumb to operate the space bar on the typewriter conceivably could haveexacerbated the damage, as well as repeated flexion/extension of the wrist.
Case 3: Computer operator.
At the time of her injury this worker, aged 37 and 170cm tall, had beenemployed as a computer operator in a large modern office buiding of aninternational financial organisation for nearly seven years. She had carpal tunnelsyndrome of the left wrist, which had resolved by the time of her clinic interview.
Her job involved two tasks, which were carried out all day and rotated monthly:transferring information from cards onto a computer via 'soft-touch1 keyboard, anda similar task of putting information onto punch cards which, she stated, needed amore forceful key depression. She punched data in at a rate of 250 strokes perminute for eight hours per day but did not use her thumbs. The data entry taskwas observed to be mostly right-handed (numeric keys) with some left handed(alpha key) operation and page turning. The punch card task was nearly all righthanded with only one or two left handed keystrokes per card. Although thesubject no longer did this job, observation of the workplace (which was in nearlyall respects identical to the computer room she had worked in previously inanother building) indicated the presence of potential ergonomic problems. Otheroperators said that this computer room became very warm, which was notsatisfactorily relieved by opening windows. Most of their seats, which were meantto be adjustable, could not be adjusted because of damaged mechanisms; VDUsreflected a lot of light from windows and strip lighting, which was parallel to thescreens; many operators were slightly bent forward because of low work surfacesand had their heads and bodies turned slightly to the left to read stacks of cards.Consequently they did not need to turn their necks. Their work tasks werecontinuous except for mid-morning and afternoon coffee breaks and a lunch break.
The subject herself did not report any specific work related problems, except beingtoo warm. Her condition had come on unexpectedly when she was not at work.Although she was absent from work until the symptoms resolved, she said that shedid not experience discomfort doing any of her duties at work.
Re: identified risk factors, she did not keep her thumb bent, repetitively rotate herwrist or forcefully bend her elbow.
We conclude that her history and mostly right handed keyboard tasks do notsuggest a directly work related upper limb disorder. However, repeated pageturning, involving slight outward rotation (supination) of the left wrist might havecontributed to her wrist disorder.
Subjects examined away from the workplace.
Case 4: Secretary.
This 45 year old woman is employed as a secretary in a small hospital, where shehas worked for two and a half years. She is 152cm tall. At the time of herorthopaedic clinic interview two years ago she had been diagnosed as having DeQuervain's disease in the right hand, six months after starting her present job.
However, until nine months before attending the clinic she had worked for fouryears part-time in a travel agency, where her duties involved typing, sorting andlifting piles of brochures and writing. Three hours were spent hand writing andturning pages of brochures and she had a fixed period (three hours) on a manual
16
typewriter every day. Although the amount varied from day to day, each travelbooking consisted of about one third handwriting with a ballpoint pen for up tothree hours per day. She typed at 400 finger strokes and 80 thumb strokes perminute and when using the manual machine she exerted force with her fingers andabducted her thumb. If she had done much handwriting during the day, she feltmore soreness in her right hand on returning home than if she had done less,irrespective of the amount of typing. She had a very firm writing grip, which hadweakened after her condition started. She was observed to hold a pen with tightlybunched fingers, wrist flexed and radially deviated.
Her current job, which was originally full time and a year ago became part time,mostly involved use of an electric typewriter, which she preferred to the manualtype, and general clerical duties but very little handwriting. She now only usedher right thumb in a straight position to operate the space bar without force.This job requires less writing, the typewriter is easier to operate and her seat isadjustable.
Re: identified risk factors, she did not use repetitive pinching movements, sustain abent thumb or flex/extend her wrist at high rates.
Although the subject was unable to make a direct connection with any activity thatmight have induced her condition, we conclude that it may have been associatedwith the amount of handwriting at work, in the absence of any other positivehistory, such as the presence of hazardous movements found from the earlier studyto be related to thumb condition.
Case 5: Typist/receptionist.
This subject was a 56 year old woman (height 163cm) currently employed full timeas a receptionist in a law firm, where she was working at the time of her clinicinterview. Fourteen months before the interview she had worked part time as atypist/receptionist in a language school for a year where her medical problems hadbegun. She was diagnosed as having a ganglion and a mucous cyst on the middlefinger of her right hand.
She had learnt to type in her late thirties and experienced a lot of discomfortwhen typing, due, she thought, to taking up typing relatively late in life. She alsostated that she had arthritic problems with her finger joints.
At the language school her duties were typing on an electric typewriter, collatingand a small amount of translating. She spent three hours per day typing forspells of up to two and a half hours at a time. Her typing rate was 125keystrokes per minute. She used her straight thumb 25 times per minute tooperate the space bar without force. She also used a pen and stapler, the formerfor up to three hours per day. Her work environment there was poorly ventilatedand sometimes stuffy. Five months after leaving this job she started work with thelaw firm, where her duties are answering the telephone and light paper work butno typing. During the last two weeks she had begun to use a word processor athome for 2-3 hours each evening and was again experiencing soreness in theinjured finger.
Re: identified risk factors, she did not use gripping movements repetitively.
Her only hobby was drawing and painting very occasionally, she did not performany sport except running and did not recall having any falls.
17
We conclude that although lacking the potentially hazardous movements related toher condition, the pains in her finger were clearly associated .with the onset oftyping and her taking up typing again recently.
Case 6: VDU operator.
This 22 year old woman (height 158cm) has worked full time as a VDU operatorwith an insurance company for six years and three evenings each week as asupermarket check-out operator for the last two years. Prior to this she had hada part time job for a year as a supermarket shelf-packer. She was diagnosed ashaving a ganglion on her left wrist.
As a shelf-packer she performed a lot of heavy lifting and also made frequent useof a price gun, which was squeezed between thumb and forefinger of her righthand up to 60 times per minute. As a check-out operator she operates a cashregister and moves groceries from in front to behind her with her left hand. Indoing this she grasps individual items and, while pushing these behind her, wristand elbow bending 50-60 times per minute for 3 hours is involved. At theinsurance company she spends all day (7 hours) key typing at 400 finger strokesand 80 thumb strokes per minute for up to 4 hours per day. She was unable togive any further information about her work tasks.
She had never experienced discomfort in her wrist during any of her jobs.Although she had noticed the swelling (ganglion) on her wrist, she did not realisethat it was unusual, until she was recommended to see a doctor about it. Herhobbies are aerobics, swimming and knitting.
Re: identified risk factors, she did not keep her thumbs bent, rotate her wristsrepetitively or forcefully bend her elbow.
In conclusion we suspect that the combination of being a full-time VDU operatorand a part time check-out operator has led to her mild disorder and, in theabsence of other precipitating factors, the left-handed movement of groceriesappears to be a principal risk factor.
3.2.4 Case 7: Shorthand typist.
This 59 year old woman (height 170cm) had worked as a shorthand typist all herworking life. She is currently employed part-time by a firm of solicitors. At theorthopaedic clinic 21 months ago she was diagnosed as having early osteo-arthritisof the first metacarpophalangeal joints of the thumb and forefinger of her righthand.
Her work tasks are mainly typing, writing, answering the telephone, stapling andother light paper work. She types at 450 finger strokes and 90 thumb strokes perminute for up to four hours at a time (the length of her shift). She uses aslightly bent right thumb to operate the space bar without force. She also uses aballpoint pen for up to an hour a day but did not bend her thumb. Prior to1983 she used an electric typewriter but, since then and at the time of her injury,she has been using a word processor. Although she could not be certain that anyone of her work tasks had directly caused her medical problem, her work didaggravate the condition.
Before acquiring this medical condition she often experienced discomfort across hershoulders, in the neck and along both forearms when typing and at home afterwork. She had also contracted tennis elbow which she associated with gardening
18
activities, as she was a keen gardener. She had also broken her left wrist whilehome decorating and suffered from cervical spondylitis.
Re: identified risk factors, she did not use repetitive gripping or pinchingmovments, sustain a bent thumb or flex/extend her wrist repetitively.
We conclude that, although the association between her original condition(osteoarthritis) and work activities is not clear, the upper limb soreness shereported during and after typing is likely to be work related.
3.2.5 Case 8: Typist.
Eight months before the original interview at the orthopaedic clinic this 31 yearold woman, who is 158cm tall, had left her job as a typist at the headquarters ofa bank, in order to have a child. She had De Quervain's disease in bothwrists/thumbs.
Her job, which she had had for one and three quarter years, involved mostlytyping on an electric typewriter but included some writing and stapling. Onaverage her typing involved 375 finger strokes but only ten thumb movements perminute, both with force, for six hours per day for as long as an hour at a time.Since her right thumb was abducted to operate the space bar after each word it ismore likely that she used her thumb at a rate of 75 movements per minute. Indoing this she used a straight thumb without force. The typing load varied fromday to day but on days when the load was high or she had to do a lot of fasttyping she had felt soreness in her hands, wrists and arms. After leaving this jobshe had no problems with either wrist nor did she have any soreness. However,following the birth of her child she experienced pains when holding and lifting thebaby. This has temporarily resolved but has recently recurred now that the childis heavier to pick up.
At her place of work she had a properly adjustable seat but the desk top was toohigh. Consequently her feet did not always reach the floor. Footrests and wristrests were not provided.
Re: identified risk factors, she did not use a pinch grip repetitively but she didsustain an abducted thumb and originally said that she flexed/extended her wrists370 times per minute for six hours per day. She subsequently stated that she kepther wrists in a slightly bent position during typing.
In conclusion, in addition to keeping her thumb and wrists bent her historysuggests that typing, particularly after a session of fast typing, was the maincontributory factor to her condition, which temporarily resolved after she left herjob, possibly because of the awkward arm posture induced by her high desk.
Case 9: Secretary
This 56 year old woman has been employed as a part-time secretary in a studenthall of residence for over sixteen years. She is 160cm tall. At the time of herclinic she had carpal tunnel syndrome diagnosed in her right wrist and during thetwo and a half years since then she has developed the same condition in her otherwrist as well as pains in her neck and back.
Her work is mostly typing and general clerical work on her own in an office. Shenormally types at a rate of 250 finger strokes per minute and uses her right thumbheld in a straight position 50 times per minute to operate the space bar for five
19
hours each day and for as long as one and a half hours continuously. Herthumbs are kept abducted and her wrists are kept in a bent position for more thana minute at a time. She had experienced discomfort in her right wrist a yearbefore attending the clinic and at that time she was using a manual typwriter,which required a more forceful operation with her fingers and right thumb. Shecommented that underlining caused a problem because of the repeated operation ofthe same key in rapid succession with the middle finger of her right hand, afunction superseded in her present electric machine. She could not say how muchunderlining she carried out each day. She also inserted paper and turned thetypewriter roller with her right hand up to seven times per minute.
Her working environment was excessively hot, because the office was locateddirectly above a boiler room. Although her seat was adjustable it wasuncomfortable and did not give adequate back support: she was not supplied with afootrest. She has to turn her head to the left and back again repeatedly(unquantified) to check her scripts and she believed that this, her uncomfortableseating and typing tasks had led to her back and neck problems.
She was a regular participant in Scottish Country dancing and lawn green bowls.
Re: identified risk factors, she sustained a bent thumb and rotated her wrist seventimes per minute for an hour each day but did not forcefully bend her elbow orrepeatedly flex and extend her wrist.
In conclusion the carpal tunnel syndrome in both her wrists is likely, consideringthe presence of two movements identified as being risk factors, to have beenbrought on by manual typing activities and the posture adopted during typing isprobably also associated with her back and neck discomfort.

HEAD OFFICE:
Research Avenue North,Riccarton,Edinburgh, EH14 4AP, United KingdomTelephone: +44 (0)870 850 5131Facsimile: +44 (0)870 850 5132
Email: [email protected]
Tapton Park Innovation Centre,Brimington Road, Tapton,Chesterfield, Derbyshire, S41 0TZ, United KingdomTelephone: +44 (0)1246 557866Facsimile: +44 (0)1246 551212
Research House Business Centre,Fraser Road, Perivale, Middlesex, UB6 7AQ,United KingdomTelephone: +44 (0)208 537 3491/2Facsimile: +44 (0)208 537 3493
Brookside Business Park, Cold Meece, Stone, Staffs, ST15 0RZ,United KingdomTelephone: +44 (0)1785 764810Facsimile: +44 (0)1785 764811
(A20115) IOM (R) ReportCov art 3/15/06 12:32 PM Page 2