Embed Size (px)
Citation preview

Evolution of HER2+ breast cancer
Prof. Dr. med. Sibylle Loibl
Chair of the German Breast Group
Centre for Haematology and Oncology, Bethanien, Frankfurt/Germany

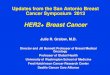
Increase in pCR in HER2+
Long CHT + duale anti-
HER2 therapy
Long CHT +Trastuzumab similar to short CHT+duale anti-
HER2
Short CHT +Trastuzumab
CHT allone
20%
48%
74%
38%
15%
25%
45%
65%
Loibl S et al. Curr Opin Obstet Gynecol. 2015 ;27:85-91.

Cortazar P, et al.
Lancet 2014

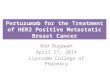
Increase in pCR by trastuzumab correlates with better prognosis (NOAH – trial)
Gianni L, et al. NOAH study Lancet Oncol
2014 and Lancet 2010
HER2-positive (Techno – Phase II)
87%
Untch M et al., J Clin Oncol 2011

Figure 2
Source: The Lancet Oncology 2014; 15:640-647 (DOI:10.1016/S1470-2045(14)70080-4)
Terms and Conditions
Gianni L, et al. NOAH study Lancet Oncol
2014
10 year update NOAH study

Figure 3
Source: The Lancet Oncology 2014; 15:640-647 (DOI:10.1016/S1470-2045(14)70080-4)
Terms and Conditions
Gianni L, et al. NOAH study Lancet Oncol
2014
10 year update NOAH

NeoSphere: Study Design
S
U
R
G
E
R
Y
Study dosing: q3w x 4
THP (n=107) Docetaxel (75100 mg/m2) Trastuzumab (86 mg/kg) Pertuzumab (840420 mg)
HP (n=107) Trastuzumab (86 mg/kg) Pertuzumab (840420 mg)
TP (n=96) Docetaxel (75100 mg/m2) Pertuzumab (840420 mg)
TH (n=107) Docetaxel (75100 mg/m2) Trastuzumab (86 mg/kg)
3xFEC +Trastuzumab for 1 year every 3 weeks
3xFEC +Trastuzumab for 1 year every 3 weeks
3xFEC +Trastuzumab for 1 year every 3 weeks
4xDoc - 3xFEC +Trastuzumab for 1 year every 3 wks
Primary Endpoint: pCR =ypT0/is
FDA-requested Endpoint: pCR =ypT0/is ypN0
Gianni L, et al. Lancet Oncol 2012

29.0
45.8
16.8 24.0 21.5
39.3
11.2 17.7
0
10
20
30
40
50
60
Arm AHT (n = 107)
Arm BPHT (n = 107)
Arm CPH (n = 107)
Arm DPT (n = 96)
NeoSphere: pCR Rates
p = 0.0141
p = 0.0198
p = 0.003
ypT0/is (primary endpoint)
ypT0/is ypN0
pC
R, %
Gianni L, et al. Lancet Oncol 2012

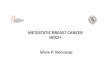
PFS by pCR
Gianni L, et al. Lancet Oncol 2016; 6:791–800.
PFS was substantially better in patients achieving a pCR
NeoSphere: At 5-year analysis, 14% of patients had relapsed or died
Overall population
No tpCR (n = 323)
tpCR (n = 94)
5-year PFS, % (95% CI) 76 (71–81) 85 (76–91)
Stratified HR = 0.54 (95% CI: 0.29, 1.00)
0
10
30
50
70
80
90
100
20
40
60
0 12 24 36 48 60 Time (months)
PFS
(%
)

D+T+P
D+T
T+P; D+P
NeoSphere: PFS
Gianni L et al. Lancet Oncol 2016; 17:791-800

OTHER STUDIES INVESTIGATING THE DUAL BLOCKADE WITH TRASTUZUMAB AND PERTUZUMAB

Neoadjuvant Therapy mit Trastuzumab and Pertuzumab in HER2+ primary b.c.
39.3
63.6
56
66.2
0
10
20
30
40
50
60
70
Neosphere DTP Tryphaena DcbTP Kristin DCbTP G7 P/nab-P TP-ECTP
ypT0/is ypN0
ypT0/is ypN0

0
20
40
60
80
TCH+P T-DM1+P
pC
R (
%)a
Difference: -11.3
95% CI: -20.5, -2.0
Stratified 2-sided P−value: 0.0155b
Kristin Study: pCR (ypT0/is, ypN0)
Presented by: Dr Sara Hurvitz
123/221 99/223
apCR rate and 95% CI are shown. Patients with missing or unevaluable pCR status were considered nonresponders: TCH+P, 7 (3.2%); T-DM1+P, 18 (8.1%). Treatment
discontinuation in the neoadjuvant phase for progressive disease: TCH+P, 0% of patients; T-DM1+P, 7% of patients. bCochran-Mantel-Haenszel Chi-square.
56% 44%

pCR Rates in subgroups of GeparSepto
Loibl S, et al. Annals Oncol 2016
HER2+ HER2-


APHINITY: Randomization Stratification Factors by Treatment
Pertuzumab
n=2400 Placebo n=2404*
Nodal status, n (%)
0 positive nodes and T ≤1 cm*
0 positive nodes and T >1 cm*
1–3 positive nodes
≥ 4 positive nodes
90 (3.8)
807 (33.6)
907 (37.8)
596 (24.8)
84 (3.5)
818 (34.0)
900 (37.4)
602 (25.0)
Adjuvant chemotherapy regimen (randomised), n (%)
Anthracycline-containing regimen
Non-anthracycline-containing regimen
1865 (77.7)
535 (22.3)
1877 (78.1)
527 (21.9)
Hormone receptor status (central), n (%)
Negative (ER- and PgR-negative)
Positive (ER- and/or PgR-positive)
864 (36.0)
1536 (64.0)
858 (35.7)
1546 (64.3)
Geographical region, n (%)
USA
Canada/Western Europe/Australia – New Zealand/South Africa
Eastern Europe
Asia Pacific
Latin America
296 (12.3)
1294 (53.9)
200 (8.3)
550 (22.9)
60 (2.5)
294 (12.2)
1289 (53.6)
200 (8.3)
557 (23.2)
64 (2.7)
Protocol Version, n (%)
Protocol A
Protocol Amendment B
1828 (76.2)
572 (23.8)
1827 (76.0)
577 (24.0)
* One patient was excluded from the ITT population due to her falsification of personal information

APHINITY:Intent-to-Treat Primary Endpoint Analysis Invasive Disease-free Survival
Number needed to treat: at 3 years 112 at 4 years 59
expected: 89.2%

APHINITY: Node-positive Subgroup
Number needed to treat: at 3 years 56 at 4 years 32

APHINITY: Hormone Receptor-negative Subgroup
Number needed to treat: at 3 years 63 at 4 years 44

* 1st interim analysis at 26% of the target events for the final overall survival analysis
3-year Pertuzumab
n=2400 Placebo n=2404 Hazard ratio (95% CI) p value
IDFS (primary endpoint), % 94.1 93.2 0.81 (0.66, 1.00) 0.045
Secondary efficacy endpoints, %
IDFS incl. second primary non-BC events (STEEP definition)
93.5 92.5 0.82 (0.68, 0.99) 0.043
Disease-free interval 93.4 92.3 0.81 (0.67, 0.98) 0.033
Recurrence-free interval 95.2 94.3 0.79 (0.63, 0.99) 0.043
Distant recurrence-free interval 95.7 95.1 0.82 (0.64, 1.04) 0.101
Overall survival (first interim analysis)*
97.7 97.7 0.89 (0.66, 1.21) 0.467
APHINITY: Secondary Efficacy Endpoints

APHINITY: Cardiac Endpoints
N (%) Pertuzumab n=2364
% Treatment difference (95% CI)
Placebo n=2405
Primary cardiac endpoint 17 (0.7) 0.4 (0.0, 0.8) 8 (0.3)
• Heart failure NYHA III/IV + LVEF drop* • Cardiac death**
15 (0.6) 2 (0.08)
6 (0.2) 2 (0.08)
• Recovered according to LVEF 7 4
Secondary cardiac endpoint Asymptomatic or mildly symptomatic LVEF drop*
64 (2.7) -0.1 (-1.0, 0.9) 67 (2.8)
*LVEF drop = ejection fraction drop ≥10% from baseline AND to below 50%; **Identified by the Cardiac Advisory Board for the trial according to a prospective definition
von Minckwitz G, et al. New Engl J Med 2017

Pertuzumab n=2364
Placebo n=2405
Neutropenia 385 (16.3%) 377 (15.7%)
Febrile Neutropenia 287 (12.1%) 266 (11.1%)
Anaemia 163 ( 6.9%) 113 ( 4.7%)
Diarrhoea 232 (9.8%) 90 ( 3.7%) - with chemotherapy and targeted therapy 232 ( 9.8%) 90 ( 3.7%)
- with targeted therapy (post-chemotherapy)
12 ( 0.5%) 4 ( 0.2%)
- with AC->T (N=1834; 1894) 137 ( 7.5%) 59 ( 3.1%)
- with TCH (N= 528; 510) 95 (18.0%) 31 ( 6.1%)
APHINITY: Common Grade ≥ 3 Adverse Events
von Minckwitz G, et al. New Engl J Med 2017

A. Schneeweiss et al. Ann Oncol 2013;24:2278-2284
TRYPHAENA - Mean change in LVEF from baseline during the treatment period

APHINITY: Health-related Quality of Life
Plot of Mean EORTC QLQ-C30 global health status by treatment regimen, ITT population

OTHER ADJUVANT STUDIES INVESTIGATING SINGLE OR DUAL HER2+ THERAPY IN BREAST CANCER

ALTTO update DFS
Moreno-Aspitia M et al. on behalf of the ALTTO investigators

HERA 11 Year Update
3 Types of patients:
1.Patients who needed more to be cured
2.Patients who had just enough
3.Patients who did not need trastuzumab to be cured
Cameron D, Lancet Oncol 2017

BCIRG 006: Node positive subgroup
1. Slamon D, et al. SABCS 2015 (Abstract S5-04; oral presentation); 2. Slamon D, et al. N Engl J Med 2011; 365:1273–1283.
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60 72 84 96 108 120 132
Pro
po
rtio
n d
ise
ase
-fre
e
Time (months)
80%2
78%2
71%2
69.6%
68.4%
62.2% ACT
AC-HT
TCH
Relapse rate still 30% Within 10 years
Relapse rate 20% in 5 years

Tolaney et al, et al. New Engl J M 2015
HER2+
ER+ or ER-
Node Negative
< 3 cm
Enroll
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
PACLITAXEL 80 mg/m2 + TRASTUZUMAB 2 mg/kg x 12
T T T T T T T T T T T T T
FOLLOWED BY 13 EVERY 3 WEEK DOSES
OF TRASTUZUMAB (6 mg/kg)*
N=406
*Dosing could alternatively be 2 mg/kg IV weekly for 40 weeks ** Radiation and hormonal therapy was initiated after completion of paclitaxel
APT Trial Design

Patient Characteristics
N %
Age
<50
50-70
≥70
132
233
41
33
57
10
Size of Primary Tumor
T1a ≤0.5 cm
T1b >0.5-≤1.0
T1c >1.0-≤2.0
T2 >2.0-≤3.0
77
124
169
36
19
31
42
9
Histologic Grade
I Well differentiated
II Moderately differentiated
III Poorly differentiated
44
131
228
11
32
56
HR Status (ER and/or PR)
Positive
Negative
272
134
67
33
50% 91%
Tolaney et al, et al. New Engl J M 2015

Paclitaxel + Trastuzumab for small tumours
Tolaney S et al. New Engl J Med. 2015
3-year rate of 98.7% (95% confidence interval [CI], 97.6 to 99.8).

Invasive Disease-Free Survival
Tolaney et al, et al. New Engl J M 2015 and ASCO 2017

APT: Small node-negative, HER2-positive tumours treated with
1 year of adjuvant trastuzumab are more likely to recur if HR-negative
Tolaney SM, et al. ASCO 2017 (Abstract 511; poster presentation).
HR-positive
HR-negative

ExteNET: study design
Chan et al. Lancet Oncol 2016 Clinicaltrials.gov identifier: NCT00878709
• HER2+ breast cancer
– IHC 3+ or ISH amplified (locally determined)
– Prior adjuvant trastuzumab + chemotherapy
– Lymph node +/–, or residual invasive disease after neoadjuvant therapy
• Stratified by: nodal status, hormone receptor status, concurrent vs sequential trastuzumab
Ran
do
miz
atio
n (1
:1)
Neratinib x 1 year
240 mg/day
Placebo x 1 year
2-y
ear
fo
llow
-up
for
iDFS
5-y
ear
fo
llow
-up
for
iDFS
Ove
rall
surv
ival
Part A Part B Part C
N=2840
Primary endpoint: invasive disease-free survival (iDFS)
Secondary endpoints: DFS-DCIS, time to distant recurrence, distant DFS, CNS recurrences, OS, safety
Other analyses: biomarkers, health outcome assessments (FACT-B, EQ-5D)
Endocrine adjuvant therapy given to patients with HR-positive tumors according to local practice
34

EXTENET 5-year analysis: iDFS
35
Neratinib
Placebo
50
60
70
Two-sided P = 0.008
HR (95% CI) = 0.73 (0.57–0.92)
80
90
0 6 12 18 24 30 36 42 48 54 60
No. at risk
Neratinib
Placebo
1420
1420
1316
1354
1272
1298
1225
1248
1106
1142
978
1029
965
1011
949
991
938
978
920
958
885
927
Months after randomization
Inva
sive
dis
ease
-fre
e s
urv
ival
(%
)
100
95.5%
∆ 2.4%
97.9%
91.7%
∆ 2.6%
94.3%
90.2%
∆ 2.0%
92.2%
89.1%
∆ 2.1%
91.2%
87.7%
∆ 2.5%
90.2%
0
Intention-to-treat population. Cut-off date: March 1, 2017
Treatment

EXTENET iDFS by hormone receptor status
36
Neratinib
Placebo
50
60
70
80
90
0 6 12 18 24 30 36 42 48 54 60
No. at risk
Neratinib
Placebo
816
815
757
779
731
750
705
719
642
647
571
581
565
567
558
556
554
551
544
542
523
525
Months after randomization
HR-positive subgroup In
vasi
ve d
isea
se-f
ree
su
rviv
al (
%)
100
96.1%
98.1%
91.7%
95.4%
89.8%
93.6%
88.5%
92.6%
86.8%
91.2%
0
50
60
70
Two-sided P = 0.762
HR (95% CI) = 0.95 (0.66–1.35)
80
90
0 6 12 18 24 30 36 42 48 54 60
No. at risk
Neratinib
Placebo
604
605
559
575
541
548
520
529
464
495
407
448
400
444
391
435
384
427
376
416
362
402
Months after randomization
HR-negative subgroup
100
94.7%
97.5%
91.8%
92.8%
90.4%
90.8%
89.3%
89.9%
88.8%
88.9%
0
Inva
sive
dis
ease
-fre
e s
urv
ival
(%
)
Neratinib
Placebo
Two-sided P = 0.002
HR (95% CI) = 0.60 (0.43–0.83)
Intention-to-treat population. Cut-off date: March 1, 2017


GUIDELINES

Recommendation of anti-HER2 therapy in high risk HER2+ breast cancer
1. Curigliano G, et al. Ann Oncol 2017; 28:1700–1712; 2. NCCN Breast Cancer Guidelines. Version 4, 2017 – February 7, 2018.
St. Gallen Expert Consensus1 NCCN Breast Cancer Guidelines2
Adjuvant systemic treatment recommendations:
Dual blockade with pertuzumab and trastuzumab improves outcome among patients who are at high risk of relapse due to lymph node involvement or hormone receptor negativity†
Adjuvant systemic treatment recommendations: If HER2-positive, node-positive, HR-positive or HR-negative receive adjuvant chemotherapy with trastuzumab ± pertuzumab (plus endocrine therapy if HR-positive)


© AGO e. V. in der DGGG e.V.
sowie
in der DKG e.V.
Guidelines Breast
Version 2018.1
www.ago-online.de
Subtype-specific Strategies for Systemic Treatment
AGO If chemotherapy is indicated due to tumor biology consider
systemic treatment before surgery (neoadjuvant) ++
HR+/HER2- and „low risk” Endocrine therapy without chemotherapy ++
HR+/HER2- and „high risk” Conventionally dosed AT-based chemotherapy ++ Dose dense chemotherapy ++ Followed by endocrine therapy ++
HER2+ Trastuzumab (plus Pertuzumab neoadjuvant at high risk) ++
Sequential A/T-based regimen with concurrent T + H ++ Anthracycline-free, platinum-containing regimen + Anthracycline-free, taxane-containing regimen +
Triple-negativ (TNBC) Conventionally dosed AT-based chemotherapy ++ Dose dense chemotherapy ++ Neoadjuvant platinum-containing chemotherapy +

© AGO e. V. in der DGGG e.V.
sowie
in der DKG e.V.
Guidelines Breast
Version 2018.1
www.ago-online.de
Adjuvant Treatment with Trastuzumab +/- Pertuzumab
Oxford LoE GR AGO
Trastuzumab 1a A ++ Trastuzumab + Pertuzumab
N+ and / or HR- 1b B + • N- and HR+ 1b B +/-
Trastuzumab in node-negative disease (if
chemotherapy is indicated) 10 mm 1a A ++ > 5–10 mm 2b B + ≤ 5 mm 2b B +/-

© AGO e. V. in der DGGG e.V.
sowie
in der DKG e.V.
Guidelines Breast
Version 2018.1
www.ago-online.de
Adjuvant Systemic Therapy after Neoadjuvant Systemic Therapy
Oxford LoE GR AGO
Endocrine treatment in endocrine responsive disease 1a A ++
Complete trastuzumab treatment for 1 year in HER2-positive disease
2b B ++
Complete pertuzumab treatment for 1 year in HER2-positive disease
1b B +/-
if N+ or HR- 2b B +
If insufficient response in case of non-pCR (invasive residual tumor in the breast and / or axillary nodes) after adequate NACT (antracyclines, taxanes, 18 weeks)
Capecitabine adjuvant in TNBC 2b B + Capecitabine adjuvant in HR+/Her-2- BC 2b B +/- Experimental therapies in controlled trials 5 D +

Options for HER2+ Primary Breast Cancer
12 -18 weeks Paclitaxel plus Trastuzumab -1 year of Trastuzumab
EC x4 q3/2w weeks - 12 weeks Paclitaxel plus Trastuzumab-1 year anti-HER2 therapy
18 weeks Paclitaxel plus Trastuzumab plus Pertuzumab – 1 year of Trastuzumab/Pertuzumab
EC x4 q3/2w weeks - 12 weeks Paclitaxel plus Trastuzumab/Pertuzumab -1 year anti-HER2 therapy
EC x4 q3/2w weeks - 12 weeks Paclitaxel plus Trastuzumab -1year Trastuzumab -1 year Neratinib
EC x4 q3/2w weeks - 12 weeks Paclitaxel plus Trastuzumab/Pertuzumab: no pCR – T-DM1
Standard for the majority
increasing risk

Proposed Treatment Algorithm
Low risk Intermdiate risk High risk Super high
Surgery PT or PTPer EC-PT-T EC-Taxane plus Trastuzumab+Pertuzumab
NACT none EC-Taxane plus Trastuzumab+Pertuzumab or EC-Taxane plus Trastuzumab
EC-Taxane plus Trastuzumab +Pertuzumab
EC-Taxane plus Trastuzumab+Pertuzumab
After surgery Trastuzumab for up to one year
Trastuzumab +Pertuzumab for up to one year
1. Trastuzumab +Pertuzumab for up to one year irrespective of pCR
2.Trastuzumab ± Pertuzumab for up to one year – Neratinib for another year for HR+ and no pCR?

Summary - HER2+ breast cancer
Early Breast Cancer All patients with HER2+ primary breast cancer recieve trastuzumab for 1 year – either adjuvant or part of the
neoadjuvant therapy
– Low risk: Paclitaxel plus Trastuzumab
– Intermediate risks: EC-Paclitaxel weekly plus Trastuzumab
– High risk tumours: EC-Paclitaxel plus Trastuzumab and Pertuzumab
The majority of women with high risk HER2+ breast cancer scheduled for neoadjuvant therapy recieve the dual blockade with pertuzumab in addition to EC-Paclitaxel for up to six cycles preoperatively
– Treatment effect could be maximised with pCR rate in HR- of >70%
Patients achieving a pCR have a significantly better outcome than pts without
– Non-pCR patients might need a better anti-HER2 treatment – KATHERINE trial
Higher pCR rate in:
– HR-pts
– PIK3CA wild-type

Greetings from Frankfurt