Embed Size (px)
Citation preview
Gastroenterology 2017;152:1588–1598
AGASECTION
Hepatitis C Virus Infection Care Pathway—A Report From theAmerican Gastroenterological Association Institute HCV CarePathway Work Group
Fasiha Kanwal,1 Bruce R. Bacon,2 Lauren A. Beste,3 Joel V. Brill,4 Allen L. Gifford,5Stuart C. Gordon,6 Michael A. Horberg,7 Jacob G. Manthey,8 Nancy Reau,9
Vinod K. Rustgi,10 and Zobair M. Younossi11
1Baylor College of Medicine and Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas; 2Saint Louis UniversitySchool of Medicine, St. Louis, Missouri; 3VA Puget Sound Health Care System, Seattle, WA and University of WashingtonSchool of Medicine and 4Predictive Health LLC, Paradise Valley, Arizona; 5Boston University and VA Center for HealthcareOrganization and Implementation Research, Boston, Massachusetts; 6Henry Ford Health System, Detroit, Michigan;7Mid-Atlantic Permanente Research Institute, Kaiser Permanente Mid-Atlantic States, Rockville; 8American GastroenterologicalAssociation, Bethesda, Maryland; 9Rush University Medical Center, Chicago, Illinois; 10Robert Wood Johnson School ofMedicine, New Brunswick, New Jersey; and 11Virginia Commonwealth University and Inova Fairfax Hospital,Falls Church, Virginia
hronic hepatitis C virus (HCV) infection is a common
Most current article
© 2017 by the AGA Institute0016-5085/$36.00
http://dx.doi.org/10.1053/j.gastro.2017.03.039
Ccondition that affects more than 2.7 millionindividuals in the US.1 New direct acting antiviral (DAA)treatments offer an unprecedented opportunity to cure HCV.In clinical trials as well as clinical practice, DAA treatmentshave resulted in sustained virological response (SVR–asurrogate for virological cure) in 90-100% of patients.2–8
The population-level effectiveness of DAA remains limitedby low rates of HCV case screening and identification9.However, recent updates in HCV screening guidelinesrecommend one-time testing for all persons born between1945 and 1965,10 which is expected to increase the numberof individuals diagnosed with and subsequently treated forHCV.
The goal of the HCV Clinical Pathway is to provideguidance on the cascade of care and best practices formanaging US-based patients with HCV in order to delivervalue-based, efficient, safe, and effective care. The Pathwayencompass the entire care spectrum of patients withHCV—from outreach and screening, to initial evaluation,antiviral treatment, and post treatment follow up care(Figure 1 outlines the scope of HCV Clinical Pathway). Thetarget audience includes clinicians involved in managingpatients with HCV (internists, infectious disease specialists,gastroenterologists and hepatologists, advanced practiceproviders, and others) as well as healthcare systems andplans in the US. Given the diversity in healthcare deliverysystems across the world, this pathway may not be gener-alizable to patients and clinicians outside of the US.
Outreach and ScreeningThe first section of the HCV clinical pathway addresses
active outreach and screening of individuals at risk for HCV.Approximately 50% of Americans with chronic HCV areunaware of their infection status, and far fewer havereceived curative antiviral therapy.11 Therefore, needs existboth for increased screening to identify people with un-recognized infections, as well as for better processes to link
diagnosed patients to antiviral treatment. Taskforce mem-bers recommend tailoring HCV outreach strategies to a va-riety of populations (Figure 2).
HCV screening is recommend for all persons bornbetween 1945-1965, and for anyone with transmission riskfactors (eg, history of injection drug use, transfusion ororgan transplant before 1992, received clotting factorsbefore 1987, history of long-term dialysis, HIV infection,persistently elevated liver enzymes, healthcare and publicsafety workers after needle sticks, sharps, or mucosalexposure to HCV-positive blood, and children born to HCV-positive women).12–15 A large body of work supports theuse of one-time HCV screening for at-risk patients, meritingits inclusion as a core measure in the Centers for Medicareand Medicaid Services quality reporting programs.16 Addi-tionally, HCV antibody testing is a covered service under theAffordable Care Act and is available without financial pen-alty to all insured patients in the 1945–1965 birth cohort.
Interventions to promote HCV awareness and appro-priate viral testing have shown promise in both outpatientand inpatient settings.17 Leveraging data resources, such aselectronic health records, has been associated withincreased testing rates.18–21 HCV disproportionately affectspersons who inject drugs, and homeless or incarceratedindividuals. Emergency Department-based HCV screening,HCV testing in incarcerated populations, and outreach topeople who inject drugs are potential means to reachunderserved individuals.22–24 HCV-related educationalresources are readily available for both patients andclinicians on the AGA website (www.gastro.org).
Once HCV infection is recognized, linkage-to-careinterventions are important to ensure that patients are

Figure 1.Overview of HCVcare pathway.
May 2017 HCV Infection Care Pathway 1589
afforded access to antiviral treatment.25–27 Linkage to caremayrequire the establishment or expansion of treatment referralnetworks and multidisciplinary teams. The use of supportservices, such as patient navigators, may reduce treatmentbarriers in selected circumstances.17 Primary-care based HCVtreatment, with appropriate specialty mentorship and support,may be a viable alternative for patients with limited specialtycare access (see Organization of HCV Care Team section).28
AGASE
CTION
Organization of HCV Care TeamSuccessful antiviral treatment requires coordination of
clinical, behavioral, and administrative management activ-ities. Significant public health impact requires outreach toengage populations that need treatment (as described in theprevious section), followed by patient evaluation and pre-scribing, negotiation of prior authorizations, and treatmentmonitoring.
A multidisciplinary, patient-centered team approach isthe optimal model for addressing these needs. Integrated
multidisciplinary care has proven effective in improvingHCV treatment initiation and SVR.29 Examples of effectiveclinical team approaches are also found in HIV care, whichsimilarly to HCV requires a high level of adherence andinvolves patients with complex behavioral and social prob-lems.30 Multidisciplinary teams for HCV care shouldencourage strong communication among team members,and place the patient at the center (Figure 3).
Practices will vary in their HCV caseloads, and thus thecapacities of individual practices to dedicate staff to eachrole will likely vary. Some larger, more urban or safety-netpractices may require larger teams, while smaller practicesmay access mental health or pharmacy clinical servicesthrough well-developed referral or “warm-handoff”arrangements. The size and configurations of patient-centered care teams depend on individual patient prefer-ences and healthcare needs.31 Connecting “spokes” of thisteam model may, in some circumstances, be createdthrough use of remote telemedicine or related technologies(eg, Project Extension for Community Healthcare Outcomes

Figure 2. Outreach to patients not in treatment.
1590 Kanwal et al Gastroenterology Vol. 152, No. 6
AGASECTION
[ECHO]) to enable delivery of HCV care to remotesettings.28
Within teams, pre-treatment evaluation and prescribingof HCV treatment is in the hands of an appropriatespecialist, who may be trained in hepatology, gastroenter-ology, or infectious diseases, but in some cases withappropriate training and support, could be a general inter-nist, or other primary care provider. The role of care coor-dinator is essential, generally serving as the principal pointof contact for the patient, and assuring continuity of allaspects of treatment care. Care coordination may be done by
Figure 3. Composition of a clinical team.
a nurse, social worker, health technician, or anotherappropriate team member depending on the clinic config-uration. Care coordination may involve case management,including prior authorization and benefits management. Theclinical pharmacist can play an essential role in pre-treatment assessment for drug interactions, monitoringadherence, and preventing waste and diversion of expensivemedications. Finally, access to mental health and substanceabuse treatment is important, to help address the highprevalence of behavioral and mental health problems.
Initial Evaluation of Patients With HCVThe initial assessment of an individual infected with HCV
requires clinicians to efficiently gather data to weigh the riskof disease progression against the benefit of viral eradication.Although HCV eradication is considered beneficial in virtuallyall infected persons a patientmust be physically andmentallyready for treatment. Conditions that could compromisetreatment success must be carefully considered.
The first visit is an opportunity to assess medical con-ditions that may contribute to progression, risk of compli-cations or impact the selection of treatment regimen(Figure 4). Physical examination and laboratory testingshould be targeted to evaluate for conditions that impacttreatment decisions, identify patients at risk for progressionof liver fibrosis or advanced liver disease, and screen forHCV extra-hepatic manifestations. Some laboratory testsmay be necessary to meet the requirements of the patient’shealth insurance provider.
Figure 5 displays the algorithm to evaluate patients forthe degree of liver disease severity, including fibrosis andcirrhosis). The presence of stigmata of decompensatedcirrhosis on physical examination (ascites, encephalopathy,
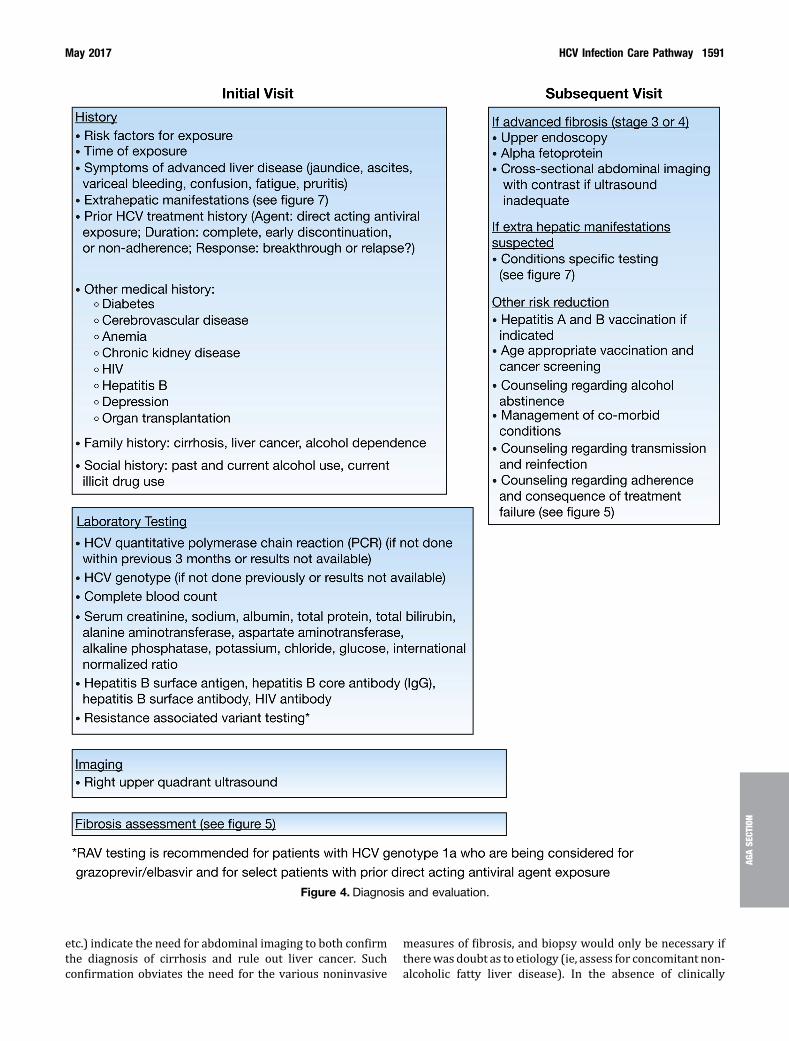
Figure 4. Diagnosis and evaluation.
May 2017 HCV Infection Care Pathway 1591
AGASE
CTION
etc.) indicate the need for abdominal imaging to both confirmthe diagnosis of cirrhosis and rule out liver cancer. Suchconfirmation obviates the need for the various noninvasive
measures of fibrosis, and biopsy would only be necessary iftherewas doubt as to etiology (ie, assess for concomitant non-alcoholic fatty liver disease). In the absence of clinically

Figure 5. HCV fibrosis assessment algorithm.
1592 Kanwal et al Gastroenterology Vol. 152, No. 6
AGASECTION
apparent cirrhosis, there is the need to assess degree of liverfibrosis. Such assessment can be done noninvasively viaelastography (usually “vibration-controlled” or Fibroscan®),serum biomarkers (FIB4 or aspartate aminotransferase to
platelet ratio index), or various proprietary markers.32 Theroutine use of the invasive gold standard liver biopsy hasbecome less popular, recognizing that even liver biopsy maymiss the presence of cirrhosis. The results of non-invasive

Figure 6. Assess diseaseseverity.
Table 1.Clinical Assessment and Diagnosis of Extrahepatic Manifestation of HCV
Clinical presentation Diagnostic investigation Diagnosis
Orthostatic purpura, skin ulcers, ischemicdigits, arthralgia, peripheral neuropathy
� Serum cryoblobulins, low C4, RFþ� Skin biopsy showing leukocytoclastic vasculitis
Mixed Cryoglobulinemia
Mono/oligo-arthritis � Non-erosive synovitis (x-ray)� RFþ, anti-CCP-,
Arthritis
XerostomiaXeroftalmia
� Schirmer’s testþ, mild salivary gland involvement� Absent or low titer autoAntibody (ANA/ENA)
Sicca Syndrome
Skin hyperpigmentation, erosions atsun-exposed areas and bullae
� Elevated serum & urinary porphyrins,URO-D deficiency
Porphyria Cutanea Tarda
Hypothyroidism � Increased TSH, anti-Tg/TPO Ab� Ultrasonographic alterations, FNA
Thyroiditis
Peripheral sensory/moto neuropathy fatigue,depression, cognitive disorder, stroke
� EMG alterations� Doppler-US of cranial vessels� Brain MRI/PET, CT� Neuropsychiatric evaluation
Neuropathy and centralnervous system involvement
Edema and/or hypertension � Proteinuria, increased serum creatinine� Glomerulonephritis at renal biopsy
Glomerulonephritis
Arterial ischemic disease or heart failure � Arterial and cardiac Doppler- US studies� EKG� Cardiac stress test� ?angiogram
Cardiovascular disease
Adenopathy, splenomegaly, cytopenias,lymphocytosis, monoclonal components,systemic symptoms
� Nodal or extranodal biopsy, bone marrow biopsy,CT/PET scan
Non-Hodgkin’s B-cellLymphoma
Chronic fatigue and impaired quality of life � Rule out other chronic diseases (hypothyroidism, fattyliver, rheumatologicdisorders)- medical evaluation
� Rule out psychiatric disorders (depression),psychological evaluation
HCV –related chronic fatigue
ANA, anti-nuclear antibody; anti-CCP, cyclic citrullinated peptide antibodies; anti-Tg/TPO, anti-thyroid antibodies; C4, com-plement 4; CT, computerized tomography; RF, rheumatoid factor; EKG, electrocardiogram; EMG, electromyogram; ENA,extractable nuclear antigen; FNA, fine needle aspiration; MRI, magnetic resonance imaging; PET, Positron emission tomog-raphy; TSH, thyroid stimulating hormone; URO-D, uroporphyrinogen decarboxylase (URO-D); US, ultrasound.
May 2017 HCV Infection Care Pathway 1593
AGASE
CTION

Figure 7. Algorithmassessing extrahepaticmanifestation of HCV.
1594 Kanwal et al Gastroenterology Vol. 152, No. 6
AGASECTION
studies provide helpful information to patient and clinicianregarding fibrosis stage, though all may suffer from occa-sional false readings and must be tempered by clinical judg-ment. Concordant results on two non-invasive studies (such aFIB-4 and Fibroscan) may preclude the need for invasive orexpensive testing to assess liver fibrosis.
Figure 8.Monitoring while
Patients should be assessed for signs and symptoms ofextrahepatic manifestations, which may indicate a compel-ling need for treatment. Some EHMs have mild or moderateclinical presentations (sicca syndrome, arthralgia, periph-eral neuropathy) while others present with life-threateningcomplications such as intestinal vasculitis and malignant
on antiviral treatment.

Figure 9. Long-term follow-up.
May 2017 HCV Infection Care Pathway 1595
AGASE
CTION

1596 Kanwal et al Gastroenterology Vol. 152, No. 6
AGASECTION
complications. Occasionally, extrahepatic manifestationshave no or minimal clinical manifestation and are discov-ered during routine laboratory testing of HCV infectedpatients. In this context, it is important to note that testingand management should be focused on the symptomaticpatients with extrahepatic manifestations (Figure 6).
Diagnostic testing for various extrahepatic manifesta-tions will depend on the clinical presentation and will bebased on the established diagnostic modalities of the spe-cific condition (Table 1). Once diagnosed, both extrahepaticmanifestation-specific and HCV-specific treatment must beconsidered.
The second visit is an ideal time for continued patienteducation and obtaining follow-up data for conditionsidentified at the first assessment. This visit offers anopportunity to initiate treatment or treatment planning.This visit is particularly important for individuals withcirrhosis who require ongoing management and surveil-lance for cirrhosis complications (see Section on follow-upcare) and those with extrahepatic manifestations whorequire treatment of both HCV and specific extrahepaticmanifestations.
Figure 7 displays the characteristics that guide selectionof appropriate type and duration of DAA regimen. Thesefactors are determined from patient history and laboratoryassessment discussed in the previous section. Figure 7 alsoshows the laboratory tests that should be performed priorto the initiation of DAA treatment. HCV treatment recom-mendations are changing at a fast pace. Given the scope ofthe HCV Pathway, the Taskforce recommended referring tothe American Association for the Study of Liver Disease andInfectious Diseases Society of America guidance on antiviraltreatment. Figure 8 presents the frequency of laboratorymonitoring as well as clinic visits for patients who are ontreatment.
Post Treatment Monitoring andFollow-up Care
Appropriate follow up recommendations and ongoinglinkage to liver-related care is important for excellent HCVcare (Figure 9). Patients who do not achieve SVR afterantiviral treatment should continue to receive ongoingmonitoring for progressive liver fibrosis. Alternative anti-viral treatments should be considered. At this point, patientsmay be referred to an experienced HCV provider, preferablyone with access to clinical trials for patients who did notrespond to the current DAAs.
Follow up recommendations for patients who achieveSVR vary based on the stage of liver fibrosis. In patients withfibrosis stage of �2, the care course can be consideredcomplete. However, prior to discharge from liver care,patients with ongoing high-risk behaviors (eg, street druguse or high risk sexual exposure) should be educated aboutthe risk of re-infection. Patients should be educated aboutrisk of progressive disease in the presence of other potentialcauses of liver disease, such as excessive alcohol use andnonalcoholic fatty liver disease. Liver-related care should
continue for patients with advanced fibrosis (fibrosis stage3 or 4) at the time of SVR and should include liver cancerscreening and monitoring of liver function every 6 months.Annual follow-up with liver/GI specialty care is recom-mended. Patients with established cirrhosis should beperiodically screened for gastroesophageal varices inaccordance with AGA guidelines.
Antiviral treatment can be deferred for many reasons,including: viral resistance to available agents, patientrefusal, drug-drug interactions which cannot be overcome,or other biopsychosocial issues. Regular monitoring toassess liver function is necessary. Also, periodic physicalexamination and consultation with the experienced HCVspecialist is recommended. Treatment should be consideredas soon as the underlying reason for deferring treatment isresolved.
SummaryThe HCV Clinical Pathway provides guidance regarding
the best practices for managing patients with HCV. Byimplementing HCV Care Pathway in practice settings, clini-cians and healthcare systems will be able to provide carethat is consistent with evidence based guidelines andavailable performance measures in the 2016 CMS PQRS HCVMeasures Group.33 The HCV Care Pathway will promotereduce variation in clinical practice and improve patientoutcomes.
References
1. Denniston MM, Jiles RB, Drobeniuc J, et al. Chronichepatitis C virus infection in the United States, NationalHealth and Nutrition Examination Survey 2003 to 2010.Ann Intern Med 2014;160:293–300.
2. Feld JJ, Jacobson IM, Hezode C, et al. Sofosbuvir andvelpatasvir for HCV genotype 1, 2, 4, 5, and 6 infection.N Engl J Med 2015;373:2599–2607.
3. Lawitz E, Gane E, Pearlman B, et al. Efficacy and safetyof 12 weeks versus 18 weeks of treatment with grazo-previr (MK-5172) and elbasvir (MK-8742) with or withoutribavirin for hepatitis C virus genotype 1 infection inpreviously untreated patients with cirrhosis and patientswith previous null response with or without cirrhosis(C-WORTHY): a randomised, open-label phase 2 trial.Lancet 2015;385:1075–1086.
4. Naggie S, Cooper C, Saag M, et al. Ledipasvir andsofosbuvir for HCV in patients coinfected with HIV-1.N Engl J Med 2015;373:705–713.
5. Poordad F, Hezode C, Trinh R, et al. ABT-450/r-ombi-tasvir and dasabuvir with ribavirin for hepatitis C withcirrhosis. N Engl J Med 2014;370:1973–1982.
6. Sulkowski MS, Gardiner DF, Rodriguez-Torres M, et al.Daclatasvir plus sofosbuvir for previously treated oruntreated chronic HCV infection. N Engl J Med 2014;370:211–221.
7. Backus LI, Belperio PS, Shahoumian TA, et al. Real-world effectiveness of ledipasvir/sofosbuvir in 4,365

May 2017 HCV Infection Care Pathway 1597
AGASE
CTION
treatment-naive, genotype 1 hepatitis C-infectedpatients. Hepatology 2016;64:405–414.
8. Ioannou GN, Beste LA, Chang MF, et al. Effectiveness ofsofosbuvir, ledipasvir/sofosbuvir, or paritaprevir/ritona-vir/ombitasvir and dasabuvir regimens for treatment ofpatients with hepatitis C in the Veterans Affairs NationalHealth Care System. Gastroenterology 2016;151:457–471.
9. Kanwal F, Lok AS, El-Serag HB. CDC and USPSTF 2012recommendations for screening for hepatitis C virusinfection: overview and take-home messages.Gastroenterology 2013;144:478–481.
10. Smith BD, Morgan RL, Beckett GA, et al. Hepatitis Cvirus testing of persons born during 1945-1965: recom-mendations from the Centers for Disease Control andPrevention. Ann Intern Med 2012;157:817–822.
11. Holmberg SD, Spradling PR, Moorman AC, et al.Hepatitis C in the United States. N Engl J Med 2013;368:1859–1861.
12. AASLD/IDSA/IAS–USA. HCV Guidance: Recommenda-tions for Testing, Managing, and Treating Hepatitis C.Available at: http://hcvguidelines.org/. Last accessedOctober 2016.
13. Screening for Hepatitis C Virus Infection in Adults: U.S.Preventive Services Task Force RecommendationStatement. Ann Intern Med 2013;159:349–357.
14. Centers for Disease C, Prevention. Testing for HCVinfection: an update of guidance for clinicians and labo-ratorians. MMWR Morb Mortal Wkly Rep 2013;62:362–365.
15. Smith BD, Morgan RL, Beckett GA, et al. Recommen-dations for the identification of chronic hepatitis C virusinfection among persons born during 1945-1965. MMWRRecomm Rep 2012;61:1–32.
16. Decision Memo for Screening for Hepatitis C Virus (HCV)in Adults (CAG-00436N) In: Services CfMaM, ed, 2014.Available at: https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=272.Last accessed October 2016.
17. Ramirez G, Cabral R, Patterson M, et al. Early Identifi-cation and Linkage to Care for People with Chronic HBVand HCV Infection: The HepTLC Initiative. Public HealthRep 2016;131 Suppl 2:5–11.
18. Sidlow R, Msaouel P. Improving Hepatitis C virusscreening rates in primary care: a targeted interventionusing the electronic health record. J Healthc Qual 2015;37:319–323.
19. Shahnazarian V, Karu E, Mehta P. Hepatitis C: improvingthe quality of screening in a community hospital byimplementing an electronic medical record intervention.BMJ Qual Improv Rep 2015 May 20;4(1).
20. Reilley B, Leston J, Hariri S, et al. Birth cohort testing forhepatitis C Virus - Indian Health Service 2012-2015.MMWR Morb Mortal Wkly Rep 2016;65:467–469.
21. Southern WN, Norton B, Steinman M, et al. A Birth-cohort testing intervention identified hepatitis c virusinfection among patients with few identified risks: across-sectional study. BMC Infect Dis 2015;15:553.
22. Allison WE, Chiang W, Rubin A, et al. Hepatitis C virusinfection in the 1945-1965 birth cohort (baby boomers)
in a large urban ED. Am J Emerg Med 2016;34:697–701.
23. Rich JD, Beckwith CG, Macmadu A, et al. Clinical care ofincarcerated people with HIV, viral hepatitis, or tubercu-losis. Lancet 2016;388:1103–1114.
24. Rich JD, Allen SA, Williams BA. Responding to hepatitisC through the criminal justice system. N Engl J Med2014;370:1871–1874.
25. Turner BJ, Taylor BS, Hanson JT, et al. Implementinghospital-based baby boomer hepatitis C virus screeningand linkage to care: Strategies, results, and costs.J Hosp Med 2015;10:510–516.
26. Younossi ZM, LaLuna LL, Santoro JJ, et al. Imple-mentation of baby boomer hepatitis C screening andlinking to care in gastroenterology practices: amulti-center pilot study. BMC Gastroenterol 2016;16:45.
27. Linas BP, Barter DM, Leff JA, et al. The hepatitis Ccascade of care: identifying priorities to improve clinicaloutcomes. PLoS One 2014;9:e97317.
28. Arora S, Thornton K, Murata G, et al. Outcomes oftreatment for hepatitis C virus infection by primary careproviders. N Engl J Med 2011;364:2199–2207.
29. Ho SB, Bräu N, Cheung R, et al. Integrated careincreases treatment and improves outcomes of patientswith chronic hepatitis C virus infection and psychiatricillness or substance abuse. Clin Gastroenterol Hepatol2015;13:2005–2014.e1–3.
30. Wilson IB, Landon BE, Hirschhorn LR, et al. Quality of HIVcare provided by nurse practitioners, physician assistants,and physicians. Ann Intern Med 2005;143:729–736.
31. Schottenfeld L, Petersen D, Peikes D, et al. Creatingpatient-centered team-based primary care. AHRQ Pub.No. 16-0002-EF. Rockville, MD: Agency for HealthcareResearch and Quality, March 2016.
32. Asrani SK. Incorporation of noninvasive measures of liverfibrosis into clinical practice: diagnosis and prognosis. ClinGastroenterol Hepatol 2015;13:2190–2204.
33. Center for Medicare and Medicaid Services. QualityIncentives Patient Assessment Instruments. Avail-able at: https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/pqrs/measurescodes.html. Accessed: Ocotber 13, 2016.
Reprint requestsAddress requests for reprints to: Jacob Manthey, Practice and QualityManager, AGA National Office, 4930 Del Ray Avenue, Bethesda, Maryland,20814. e-mail: [email protected].
AcknowledgmentsDisclaimers: Any mention of specific pharmaceuticals, devices, diagnostics, orcompanies is for informational purposes only, and does not representendorsement by the American Gastroenterological Association.Any mention of specific HCPCS or CPT codes does not constitute coding
advice or recommendations by the American GastroenterologicalAssociation. Inclusion or exclusion of a procedure or service does not implyany health insurance coverage or reimbursement policy.This care pathway framework is not intended to impose requirements on
practices or to establish a local, regional, or national legal standard of care.There are various appropriate treatment modalities for each patient, and thephysician must use his or her judgement in selecting from among feasibletreatment options. The ultimate judgement regarding appropriateness of anyspecific procedure or course of action must be made by the physician alongwith the patient, in light of all the circumstances presented. All that shouldbe expected is that the physician will follow a reasonable course of action

1598 Kanwal et al Gastroenterology Vol. 152, No. 6
AGASECTION
based on current knowledge, available resources, and the needs of the patient,in order to deliver effective and safe medical care.CPT codes, descriptions and other data only are copyright 2016 American
Medical Association (AMA). All rights reserved. CPT is a registered trademarkof the American Medical Association.
Conflicts of interestThe authors disclose the following: Bruce R. Bacon has completed promotionallectures for AbbVie, BMS, Gilead, Merck, and Salix; paid on a per lecture basis.Joel V. Brill personally owns shares in Endochoice and is a consultant for
GeneNews. Stuart C. Gordon sits on the advisory board for Gilead, Merck,AbbVie, Intercept, and BMS; provides grant and research support for Gilead,Merck, AbbVie, Intercept, CymaBay, Exalenz, Conatus, and BMS; is amember of the speaker’s bureau for Gilead; and is a scientific advisor forCVS-Caremark. Nancy Reau is a member of the US National AdvisoryBoards for Abbvie, Gilead, Merck, and BMS. Vinod K. Rustgi sits on theadvisory boards of Gilead, Merck, and AbbVie and the speaker’s bureau forGilead, AbbVie, BMS, and Salix. Zobair M. Younossi provides consultingservices or has received research funds from Intercept, Gilead, BMS, GSK,and Tobira. The remaining authors disclose no conflicts.





























