-
Tuberculosis is one of the well-described infectiousdiseases,
which has a worldwide occurrence and is asso-ciated with various
clinical manifestations (1). Hepatictuberculosis is one of the
uncommon forms of extrapul-monary tuberculosis (1-4). In
tuberculosis, involve-ment of liver is usually seen in association
with pul-monary or miliary tuberculosis (1, 2, 5). Occurrence
ofisolated hepatic tuberculosis without extrahepatic
mani-festations is very rare (1-5). In both, isolated hepaticand
systemic tuberculosis, hepatic involvement tends tobe multiple
micro- or macronodular, whereas the singlenodule or mass form is
rare (1-3, 6). Hence, hepatic tu-berculosis can mimic primary or
metastatic liver malig-nancies (1). In the present study, we have
reported someunusual findings on isolated hepatic tuberculosis,
whichwas revealed to be infiltrative type of hepatic tuberculo-sis
from CT scans and ultrasonograms.
Case Report
A 49-year-old female patient was admitted to our hos-pital with
abdominal pain and fever from past 20 days.During the past four
years, the patient had undergonerepeated intrahepatic biliary stone
removals by chole-dochoscopy. Physical examination revealed neither
he-patomegaly nor splenomegaly. Laboratory tests showedan elevated
level of C-reactive protein (CRP), howeverher other tests were
normal, including alkaline phos-phatase, erythrocyte sedimentation
rate (ESR), α-feto-protein, and CA 19-9. Plain chest radiography
was unre-markable. Abdominal CT revealed a very hypoattenuat-ing
lesion in the right lobe of the liver (Fig. 1A). Therewas less
enhancement of lesion when compared withrest of the liver
parenchyma. There was neither lym-phadenopathy nor calcification in
the abdomen.Abdominal ultrasonography revealed a very
ill-defined,heterogenous, subtle low echogenicity in the right
lobeof the liver. CT and ultrasonographic findings revealedthe
presence of cholangiohepatitis associated with intra-hepatic
biliary stones. The patient’s symptoms were re-lieved after
administration of antibiotics, and after dis-charging she had no
specific symptoms. Two months
J Korean Radiol Soc 2005;53:269-272
─ 269 ─
Hepatic Tuberculosis: Unusual CT and Sonographic Findings1
Jihyeon Cha, M.D., Jae Ho Byun, M.D., Seong Eon Yoon, M.D., Ye
Ri Lee, M.D., Hyung Jin Won, M.D., Ah Young Kim, M.D., Yong Moon
Sin, M.D., Pyo Nyun Kim, M.D.,
Hyun Kwon Ha, M.D., Moon-Gyu Lee, M.D.
A case of infiltrative type of hepatic tuberculosis is
presented. Ultrasonography re-vealed a very ill-margined,
heterogenously low echoic lesion in the right hepatic lobe.CT scans
demonstrated a very ill-defined, geographic, hypodense lesion with
minimalcontrast enhancement mimicking cholangiohepatitis or
infiltrative tumor in the righthepatic lobe.
Index words : TuberculosisLiverComputed tomography
(CT)Ultrasound (US)
1Department of Radiology, Asan Medical Center, University of
UlsanCollege of MedicineReceived June 15, 2005 ; Accepted July 21,
2005Address reprint requests to : Jae Ho Byun, M.D., Department
ofRadiology, Asan Medical Center, University of Ulsan College
ofMedicine, 388-1 Poongnap-dong, Songpa-gu, Seoul 138-736,
Korea.Tel. 82-2-3010-4400 Fax. 82-2-476-4719 E-mail:
[email protected]
-
later, follow-up CT revealed the expansion of a very
ill-defined, geographic, hypodense lesion with subtle con-trast
enhancement in the right lobe of the liver and anew, ill-defined,
low-attenuating lesion in the left lobe ofthe liver (Figs. 1B and
C). There was neither lym-phadenopathy nor calcification and no
abnormal find-ings were observed on the CT scans. The patient
wasreadmitted and underwent sonographically guided per-cutaneous
liver biopsy of a very ill-margined, heteroge-
neously low echoic lesion in the right lobe of the liver(Fig.
1D). Histologic examination showed chronic granu-lomatous
inflammation with caseous necrosis, whichwas consistent with
tuberculosis (Fig. 1E). Ziehl-Neelsenstain of the specimen for
Mycobacterium tuberculosiswas negative. Culture for Mycobacterium
tuberculosisby employing the specimen was not performed.
Anti-tu-berculous treatment with isoniazid, rifampin, ethambu-tol,
and pyrazinamide was started, and the patient was
Jihyeon Cha, et al : Hepatic Tuberculosis
─ 270 ─
C D
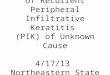
Fig. 1. A 49-year-old woman with he-patic tuberculosis.A.
Enhanced CT scan shows a very ill-defined, hypodense lesion
(arrows) inthe right lobe of the liver. There ispneumobilia in the
left intrahepaticbile duct of the liver due to previous re-moval of
biliary stone by chole-dochoscopy.B, C. Follow-up enhanced CT scans
ob-tained two months after the initial CT,reveal the expansion of a
very ill-de-fined, geographic, hypodense lesion (ar-rows) with
minimal contrast enhance-ment in the right lobe of the liver and
anew ill-defined, low-attenuating lesion(arrows) in the left lobe
of the liver.D. Ultrasonogram shows a very ill-mar-gined,
heterogenously low echoic lesion(arrows) in the right lobe of the
liver.E. Photomicrograph of the lesion showschronic granulomatous
inflammation(arrows) with caseous necrosis (aster-isk). (H & E
stain, ×100)F. Thirteen weeks after initiation of an-ti-tuberculous
treatment, a follow-upenhanced CT scan shows reduction
ofhypoattenuating lesion (arrows) in theright lobe of the
liver.
A B
E F
-
discharged from the hospital six days after initiation ofthe
anti-tuberculous medication. Thirteen weeks afterinitiation of the
anti-tuberculous treatment, follow-upabdominal CT revealed
reduction of the hypoattenuat-ing lesions in both the lobes of
liver (Fig. 1F). Wethought that the hypoattenuating lesion in the
left lobeof the liver was also hepatic tuberculosis.
Discussion
Tuberculosis can affect virtually any organ system inthe body
and can be devastating if left untreated. In re-cent years, the
prevalence of tuberculosis in both im-munocompetent and
immunocompromised individualshas increased, and this disease has
become a subject ofuniversal concern. Isolated hepatic tuberculosis
withoutextrahepatic involvement and the macronodular orpseudotumor
forms are rare (1-3). Kok and Yapp (1) re-ported that only 5 (0.3%)
of 1678 new cases of tubercu-losis represented isolated hepatic
tuberculosis withoutextrahepatic involvement of tuberculosis.
Hepatic tuber-culosis can be classified as follows (3): a) primary
acutepulmonary tuberculosis with liver involvement; b) mil-iary
tuberculosis; c) primary tuberculosis; d) tuberculo-ma (abscess);
e) chronic pulmonary tuberculosis withliver involvement; and f)
tuberculous cholangitis.
Hepatic tuberculosis can be diagnosed on CT scans asmicronodular
(miliary) or macronodular (7). The micron-odular type manifests on
CT scans as multiple, tiny, low-attenuation foci, each a few
millimeters in diameter andit spreads throughout the liver. The
macronodular type israre and manifests as diffuse liver enlargement
withmultiple, hypodense lesions measuring from 1- to 3-cmin
diameter or as a single tumor-like mass (1, 3, 6, 7).Contrast
enhancement occurs in peripheral granuloma-tous tissue, and the
central low density of caseationnecrosis shows less enhancement or
homogenous mini-mal enhancement (5). As the time progresses,
calcifica-tion of the lesion occurs and occasionally may
becomeextensive (1). The ultrasonograms reveals the presence ofthe
miliary form is that of a homogenous enlarged liveror a bright echo
pattern, which is indistinguishable fromthat observed in liver
cirrhosis or other cases of in-creased hepatic echogenicity (1, 8).
The macronodularform is seen as multiple round hypoechoic nodules
(1, 8).
In our case, CT revealed a very ill-defined,
geographic,low-attenuation lesion with minimal contrast
enhance-ment. There were some penetrating vessels through
thehypoattenuating lesion. These CT findings were neither
micronodular nor macronodular. Ultrasonography alsorevealed a
very heterogeneously hypoechoic lesion withill margin. The cause of
cholangitis was unclear becauseeither tuberculosis or biliary stone
could be the cause ofcholangitis.
When hepatic tuberculosis is present in the macron-odular form,
it is often confused with metastasis, lym-phoma, sarcoidosis, and
liver abscess (1, 2, 6, 8). In ourcase, because of the patient’s
underlying biliary stonedisease, her hepatic lesion was initially
mistaken fornonspecific cholangiohepatitis associated with
biliarystones. It could also have been considered to be
anotherinfiltrative disease such as lymphoma, amyloidosis orfatty
deposition.
Because the radiologic and clinical findings of
hepatictuberculosis have a low specificity, microbiological
orhistopathologic examination of such specimens is need-ed in order
to make a diagnosis. Histologically, a tuber-culous lesion is
composed of central caseating necrosiswith surrounding epitheloid
and giant cells and border-ing lymphohistiocytic cells (3, 8). The
more unequivocalconfirmation is the discovery of tuberculous
bacilli afterthe use of special stains and/or on subsequent
cultures.Because the frequency of positive acid-fast smears islow,
ranging from 0to 45%, the caseating necrosis canbe considered to be
very suggestive and sufficient forthe diagnosis (8). The proper
clinical setting and follow-up of liver recovery, under specific
anti-tuberculosismedication, leads to final diagnosis (8).
This rare case shows the infiltrative type of hepatic
tu-berculosis without extrahepatic involvement of tubercu-losis. In
patients who are presented with protracted ill-ness and have an
unusual lesion in the liver on cross-sectional images, biopsy must
be performed for correctdiagnosis and suitable treatment must be
given.
Acknowledgments
The authors thank Bonnie Hami, MA, Department ofRadiology,
University Hospitals Health System,Cleveland, Ohio, for her
editorial assistance in prepar-ing the manuscript.
References
1. Kok KYY, Yapp SKS. Isolated hepatic tuberculosis: report of
fivecases and review of the literature. J Hepatobiliary Pancreat
Surg1999;6:195-198
2. Kawamori Y, Matsui O, Kitagawa K, Kadoya M, Takashima
T,Yamahana T. Macronodular tuberculoma of the liver: CT and
MRfindings. AJR Am J Roentgenol 1992;158:311-313
J Korean Radiol Soc 2005;53:269-272
─ 271 ─
-
3. Levine C. Primary macronodular hepatic tuberculosis: US and
CTappearances. Gastrointest Radiol 1990;15:307-309
4. Achem SR, Kolts BE, Grisnik J, MacMath T, Monteiro
CB,Goldstein J. Pseudotumoral hepatic tuberculosis. J
ClinGastroenterol 1992;14:72-77
5. Hayashi M, Yamawaki I, Okajima K, Tomimatsu M, Ohkawa
S.Tuberculous liver abscess not associated with lung
involvement.Intern Med 2004;43:521-523
6. Tritou I, Prassopoulos P, Daskalogiannaki M, Charoulakis
N,
Papakonstantinou O, Gourtsoyiannis N. Miliary hepatic
tubercu-losis not associated with splenic or lung involvement.
ActaRadiologica 2000;41:479-481
7. Harisinghani MG, McLoud TC, Shepard JO, Ko JP, Shroff
MM,Mueller PR. Tuberculosis from head to toe. RadioGraphics
2000;20:449-470
8. Blangy S, Cornud F, Sibert A, Vissuzaine C, Saraux JL,
BenacerrafR. Hepatitis tuberculosis presenting as tumoral disease
on ultra-sonography. Gastrointest Radiol 1988;13:52-54
Jihyeon Cha, et al : Hepatic Tuberculosis
─ 272 ─
대한영상의학회지 2005;53:269-272
비특이적 간 결핵1
1울산대학교의과대학서울아산병원진단방사선과
차지현·변재호·윤성언·이예리·원형진·감아영·신용문·김표년·하현권·이문규
본 증례는 복부 초음파상 간 우엽에 경계가 불분명하고 불균질한 에코로 보이고 컴퓨터 전산화 촬영상 경계가
불분
명한 저음영의 조영증강이 미미한 소견을 보여 간 종괴로 오인했던 침윤적 간 결핵에 대한 예를 보고하고자
한다.