Embed Size (px)
Citation preview

Diffuse Interstitial (Infiltrative, Restrictive) DiseasesM .Sibanda MBChB 5

Obstructive Versus Restrictive Pulmonary Diseases
Such a classification is based on pulmonary function tests.A critical part of the initial workup of patients. 1. obstructive disease (airway disease)- limitation of airflow. 2. restrictive disease-reduced expansion of lung parenchyma.Obstructive disease: hallmark is a decreased expiratory flow rate (FEV1 it follows that the ratio of FEV1 to FVC ).Diffuse restrictive diseases FVC is reduced and the expiratory flow rate is normal or reduced proportionately (ratio of FEV1 to FVC is near normal).

Focus on restrictive defect
Occurs in two general conditions1. Chest wall disorders in the presence of normal lungs (e.g in diseases of the pleura, Guillain-Barre syndrome.2. Acute or chronic interstitial lung diseases (classic acute restrictive disease is ARDS, Chronic restrictive diseases pneumoconiosis, interstitial fibrosis of unknown aetiology, and most of the infiltrative conditions (e.g., sarcoidosis). THE SECOND CONDITION IS WHAT WE WILL FOCUS ON.

Diffuse Interstitial (Infiltrative, Restrictive) Diseases
Heterogeneous group of disorders characterised by diffuse usually chronic involvement of pulmonary connective tissue. Principally the most peripheral and delicate interstitium in alveolar walls

DEFINITION cont.…Many of the entities are of unknown cause and pathogenesis.Some have an intra-alveolar as well as an interstitial component.Account for about 15% of non-infectious diseases.Clinical and pulmonary functional changes. Patients have dyspnoea, tachypnea, end-inspiratory crackles, and eventual cyanosis, without wheezing. Classic physiologic features: reductions in carbon monoxide diffusing capacity, lung volume, and compliance.CXR-picture and the term infiltrative.Early stages-can often be distinguished .Advanced forms- hard to differentiate becoz, of end-stage lung.

DEFINITION cont.…
Categorized either as clinicopathologic syndromes or as having characteristic histology . Frequency of disease: most common associations are -Environmental diseases (approximately 25%) -Sarcoidosis (approximately 20%) -Idiopathic pulmonary fibrosis (approximately 15%) -the collagen vascular diseases (approximately 10%) more than 100 different causes and associations account for the remaining interstitial disease.

Pathogenesis

Pathogenesis cont.…
Earliest common manifestation of most of the interstitial diseases is alveolitis.In mild and self-limited injury, resolution with restoration of normal architecture follows. Accumulation of leukocytes has two consequences. -1. Distorts the normal alveolar structures . -2. Release of mediators that can injure parenchymal cells and stimulate fibrosisTHESE RESULT IN END STAGE LUNG

Pathogenesis cont.…
initial stimuli for alveolitis are as heterogeneous, ROS, directly toxic to endothelial cells, epithelial cells etc.Compliment and macrophage mediated accumulation of inflammatory cells is seen I most diseases .CMI is seen in disease like sarcoidosis with formation of granulomas .

Major Categories of Chronic Interstitial Lung Disease Fibrosing Usual interstitial pneumonia (idiopathic pulmonary fibrosis) (IPF ) Nonspecific interstitial pneumonia (NSIP) Cryptogenic organizing pneumonia (COP) Associated with collagen vascular diseases Pneumoconiosis Drug reactions Radiation pneumonitis Granulomatous Sarcoidosis Hypersensitivity pneumonitis Eosinophilic Smoking-Related Desquamative interstitial pneumonia Respiratory bronchiolitis-associated interstitial lung disease Other Pulmonary alveolar proteinosis

Fibrosing Category1. Idiopathic Pulmonary Fibrosis (cryptogenic fibrosing alveolitis)Diffuse interstitial fibrosis (usual interstitial pneumonia (UIP)), which in advanced cases results in severe hypoxemia and cyanosis.Males are affected more often than are females.Approx. two-thirds of patients are older than 60 years of age at presentation.similar pathologic findings in the lung may be noted with well-defined entities such as asbestosis

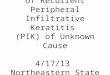
MorphologyPleural surfaces of the lung have the appearance of cobblestones .The cut surface shows fibrosis (firm, rubbery white areas).Patchy interstitial fibrosis. Earliest lesions appear as fibroblastic foci .Temporal heterogeneity.Honeycomb fibrosis occurs.The interstitial inflammation is usually patchy and consists of an alveolar septal infiltrate of mostly lymphocytes . Foci of squamous metaplasia and Intimal fibrosis and medial thickening of pulmonary arteries often present.

Usual interstitial pneumonia. The fibrosis, which varies in intensity, is more pronounced in the sub-pleural region

Usual interstitial pneumonia. Fibroblastic focus with fibres running parallel to surface and bluish myxoid extracellular matrix.

Clinical Course
IPF usually presents insidiously Gradual onset of a non-productive cough and progressive dyspnoea. O/E "dry" or "Velcro"-like crackles during inspiration.Cyanosis, cor pulmonale, and peripheral oedema .Investigations: Surgical lung biopsy remains the gold standard for diagnosing IPF .Prognosis is poor mean survival of 3 years or less.

Nonspecific Interstitial Pneumonia
Unknown aetiology, affects mostly 45 to 55 year olds. Lung biopsies fail to show diagnostic features of any of the other well-characterized interstitial diseases."wastebasket" type of diagnosis, it is important to differentiate non-specific interstitial fibrosis from UIP.Divided into cellular and fibrosing patterns.Fibroblastic foci are typically absent.Clinical course : Patients present with dyspnoea and cough of several months' duration cellular pattern have a better outcome

Cryptogenic Organizing Pneumonia
Synonymous with "bronchiolitis obliterans organizing pneumonia.Clinical coursecough and dyspnoea . Radiographically have subpleural or peribronchial patchy areas of airspace consolidationSome individuals recover spontaneously, but most require treatment HistologicallyPolypoid plugs of loose organizing connective tissue within alveolar ducts, alveoli, and often bronchioles .Organizing pneumonia with intra-alveolar fibrosis. There is no interstitial fibrosis/ honeycomb

Cryptogenic organizing pneumonia. Alveolar spaces are filled with balls of fibroblasts (arrow).

Pulmonary Involvement in Collagen Vascular Diseases
systemic lupus erythematous, rheumatoid arthritis, systemic sclerosis, and dermatomyositis-polymyositis are examples.Histologic variants , with NSIP, UIP-pattern (similar to what is seen in IPF), vascular sclerosis, organizing pneumonia, and bronchiolitis (small airway disease, with or without fibrosis) being the most common.Pulmonary involvement in these diseases is usually associated with a poor prognosis.

Pneumoconiosis
Non neoplastic lungs reaction to inhalation of mineral dusts in the work place and organic as well as inorganic particles, fumes and vapours.

Mineral Dust-Induced Lung Disease Agent Disease: Exposure Coal dust exposure: Simple coal workers' pneumoconiosis: macules and nodules Complicated coal workers' pneumoconiosis: PMF- Coal mining Silica exposure: Silicosis -Sandblasting, quarrying, mining, stone cutting, foundry work, ceramics Asbestos exposure: Asbestosis pleural effusions, pleural plaques, or diffuse fibrosis; mesothelioma; carcinoma of the lung and larynx- Mining, milling, and fabrication of ores and materials; installation and removal of insulation

Pathogenesis Size, shape, solubility, and reactivity of the particles etc determine the reaction of the lung to mineral dusts .The amount which cause disease depends on the factors above.Coal dust is relatively inert (large amounts must deposit).Silica, asbestos, and beryllium are more reactive than coal dust (fibrotic reactions at lower concentrations)Macrophages accumulate and endocytose the trapped particulatesMore reactive particles trigger the macrophages to release inflammatory mediators.Tobacco smoking worsens the effects of all inhaled mineral dusts, more so with asbestos than with any other particle. Larger particles resist dissolution these tend to evoke fibrosing collagenous pneumoconiosis (characteristic of silicosis).

Coal Workers' Pneumoconiosis ("black lung" )
Findings range from: 1.asymptomatic anthracosis, 2.simple coal workers' pneumoconiosis (CWP),3. complicated CWP or progressive massive fibrosis (PMF).Fewer than 10% of cases of simple CWP progress to PMF.PMF is a generic term that applies to a confluent fibrosing reaction in the lung; this can be a complication of any one of the three pneumoconiosis discussed here. Anthracite mining has been associated with a higher risk of CWP.

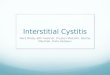
MorphologyPulmonary anthracosis: innocuous coal-induced pulmonary lesion -Inhaled carbon pigment is engulfed by alveolar or interstitial macrophages. -Which then accumulate in the connective tissue along the lymphatics, including the pleural lymphatics, or in lymph nodes. Linear streaks and aggregates of anthracotic pigment are seen.Simple CWP: coal macules and the somewhat larger coal nodule are seen. -The upper lobes and upper zones of the lower lobes are more heavily involved.C -Centrilobular emphysema can occur.Complicated CWP (PMF)Occurs on a background of simple CWP by coalescence of coal nodules characterized by intensely blackened scars larger than 2 cm, sometimes up to 10 cm in greatest diameter

Progressive massive fibrosis superimposed on coal workers' pneumoconiosis. The large blackened scars are principally in the upper lobe. Note the extensions of scars into surrounding parenchyma and retraction of adjacent pleura.

Clinical Course Usually a benign disease that produces little decrement in lung function.Increasing pulmonary dysfunction, pulmonary hypertension, and cor pulmonale, seen if PMF develops. Progression from CWP to PMF has been linked to a variety of conditions including coal dust exposure level and total dust burden Once smoking-related risk has been taken into account, there is no increased frequency of bronchogenic carcinoma in coal miners.

Silicosis
Currently the most prevalent chronic occupational disease in the world. Slowly progressive.Caused by inhalation of crystalline silica.(quartz is most commonly implicated in silicosis)After inhalation the particles interact with epithelial cells and macrophages.Ingested silica particles cause activation and release of mediators by pulmonary macrophages, including IL-1, TNF.When mixed with other minerals, quartz has a reduced fibrogenic effect.

Morphology
Silicotic nodules .Microscopically, the silicotic nodule demonstrates concentrically arranged hyalinized collagen fibers surrounding an amorphous center. "whorled" appearance of the collagen fibres.Polarized microscopy reveals weakly birefringent silica particles, primarily in the center of the nodules.Fibrotic lesions may occur in the hilar lymph nodes and pleura."eggshell" calcification .

Advanced silicosis seen on transection of lung. Scarring has contracted the upper lobe into a small dark mass (arrow). Note the dense pleural thickening

Several coalescent collagenous silicotic nodules

Clinical Course
Usually detected in routine chest radiographs performed on asymptomatic workers.(fine nodularity in the upper zones of the lung is seen)After PMF is present the disease may be progressive, even if the person is no longer exposed.Many individuals with PMF develop pulmonary hypertension and cor pulmonale,Disease is slow to kill, but impaired pulmonary function may severely limit activity.Silicosis is associated with an increased susceptibility to tuberculosis.

Asbestosis and Asbestos-Related Diseases
occupational exposure to asbestos is linked to : (1) parenchymal interstitial fibrosis (asbestosis) (2) localized fibrous plaques or, rarely, diffuse fibrosis in the pleura (3) pleural effusion (4) bronchogenic carcinoma. (5) malignant pleural and peritoneal mesothelioma (6) laryngeal carcinoma.

PathogenesisThere are two distinct forms of asbestos Serpentine and amphibole.Amphibole are more pathogenic than the serpentine chrysotile.Asbestos causes fibrosis by interacting with lung macrophages.Asbestos probably also functions as both a tumor initiator and a promoter.Potentially toxic chemicals adsorbed onto the asbestos fibers undoubtedly contribute to the pathogenicity of the fibres.

Morphology Marked by diffuse pulmonary interstitial fibrosis.Asbestos bodies distinguish it from diffuse interstitial fibrosis. Asbestosis begins in the lower lobes and subpleurally ( In contrast to CWP and silicosis) Contraction of the fibrous tissue distorts the native architecture, creating enlarged airspaces enclosed within thick fibrous walls.(honeycombed formation).Pulmonary hypertension and cor pulmonale may result.Pleural plaques (well-circumscribed plaques of dense collagen often containing calcium.)Uncommonly, asbestos exposure induces pleural effusions, which are usually serous but may be bloody.

High-power detail of an asbestos body, revealing the typical beading and knobbed ends (arrow)

Asbestosis. Markedly thickened visceral pleura covers the lateral and diaphragmatic surface of lung. Note also severe interstitial fibrosis diffusely affecting the lower lobe of the lung

Clinical Course
Dyspnea (exertion then at rest)Productive coughThe disease may remain static or progress to CHF, cor pulmonale, and deathDisease manifestations more common 20 years after exposure.The relative risk for mesotheliomas, normally a very rare tumor , is more than 1000-fold greater.Concomitant cigarette smoking, has no association with increased risk of mesothelioma.

Drug- and Radiation-Induced Pulmonary Diseases
Acute and chronic alterations in respiratory structure and function can result from drugs.e.gBleomycin, an anticancer agent, causes pneumonitis and interstitial fibrosisAmiodarone, an anti-arrhythmic agent, is also associated with pneumonitis and fibrosis Radiation pneumonitis .Acute radiation pneumonitis-fever, dyspnea out of proportion to the volume of irradiated lung, pleural effusion, and pulmonary infiltrates. Progress to chronic radiation pneumonitis may occur, associated with pulmonary fibrosis.

Granulomatous Diseases
Sarcoidosis -bilateral hilar lymphadenopathy or lung involvement (or both), visible on chest radiographs, is the major presenting manifestation . The prevalence of sarcoidosis is higher in women than in men, BLACKS than whites .Sarcoidosis is one of the few pulmonary diseases with a higher prevalence among nonsmokers.

Aetiology and PathogenesisUnknown but evidence points to the1. immune dysregulation in 2. genetically predisposed individual 3. exposed to certain environmental agentsCell mediated response to unidentified antigen driven by CD4= helper T cells. CMI. These accumulate In the Intra-alveolar and interstitial space. IL -2 and IFN-GAMMA etc from TH-1 cells, result in T-cell expansion and macrophage activation, respectively, this eventually lead to recruitment of additional T cells and monocytes and contribute to the formation of granulomas.Polyclonal hypergammaglobulinemia and anergy to common skin test antigens occur. (TH-cell dysregulation)Familial and racial clustering of cases and association with certain human leukocyte antigen (HLA) genotypes (e.g., class I HLA-A1 and HLA-B8) Viruses, mycobacteria, Borrelia, pollen have been proposed as the inciting agent for sarcoidosis .

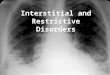
Morphologynoncaseating epithelioid granuloma.Central necrosis unusual Granulomatous fibrous and hyaline with chronicity.Schaumann bodies and Asteroid bodies are also seen (not pathognomonic of sarcoidosis) .The granulomas predominantly involve the interstitium rather than airspaces, with some "lymphangitic" distribution tendency.The bronchoalveolar lavage (BAL) contains abundant CD4+T cells.Diffuse interstitial fibrosis resulting in a honeycomb lung in 5-15%.hilar and paratracheal lymph nodes are enlarged in 75% to 90% of patients.

Morphology cont…Skin lesions : approximately 30-50% of cases of patients. -Erythema nodosum, the hallmark of acute sarcoidosis ( Sarcoidal granulomas are uncommon in these lesions). -Lupus pernio.Involvement of the eye and lacrimal glands occurs in about one-fifth to one-half of patients -ocular involvement: takes the form of iritis or iridocyclitis (Corneal opacities, glaucoma, and (less commonly) total loss of vision may then develop. -Posterior uveal tract is also affected. -Ocular lesions are frequently accompanied by inflammation in the lacrimal glands sicca syndrome may occur.. Unilateral or bilateral parotitis with painful enlargement of the parotid glands in < 10%. Mikulicz syndrome, is also seen.

Morphology cont… -The spleen In about three-fourths of cases it contains granulomas, in approximately 10% it becomes clinically enlarged. The liver demonstrates microscopic granulomatous lesions, usually in the portal triads.Bone marrow is reported in as many as 40% of patients, although it rarely causes severe manifestations. Sometimes there is hypercalcemia and hypercalciuria.Muscle involvement : is often underdiagnosed, since it may be asymptomatic.muscle weakness, aches, tenderness, and fatigue should prompt consideration of occult sarcoid myositis.Muscle biopsy could be a useful tool in the diagnosis of sarcodosis.

Characteristic sarcoid noncaseating granulomas in lung with many giant cells

Clinical Course.In many individuals the disease is entirely asymptomatic, discovered on routine chest films . bilateral hilar adenopathy or as an incidental finding at autopsyIn others, lesion to other tissues may be presenting manifestations.In about two-thirds of symptomatic cases there is a gradual appearance of respiratory symptoms .Lung or lymph node biopsy are often used.Sarcoidosis follows an unpredictable course . 65% to 70% of affected individuals recover with minimal or no residual manifestations.20% develop permanent lung dysfunction or visual impairment.Of the remaining 10% to 15%, most succumb to progressive pulmonary fibrosis and cor pulmonale. Patients presenting with hilar lymphadenopathy alone have the best prognosis, followed by those with adenopathy and pulmonary infiltrates.

Hypersensitivity PneumonitisAn immunologically mediated inflammatory lung disease (allergic alveolitis).Results from heightened sensitivity to inhaled antigens such as moldy hay .Immunologically mediated injury occurs at the level of alveoli. Occupational exposures are diverse, probably have very similar pathophysiology.Several lines of evidence suggest that hypersensitivity pneumonitis is an immunologically mediated disease.Increased numbers of T lymphocytes of both CD4+ and CD8+ phenotype, also indication of a type III hypersensitivity and type IV hypersensitivity against the implicated antigen(s). hypersensitivity pneumonitis is an immunologically mediated response to an extrinsic antigen that involves both immune-complex and delayed-type hypersensitivity reactions. progression to serious chronic fibrotic lung disease can be prevented by removal of the environmental agent.

Selected Causes of Hypersensitivity Pneumonitis Syndrome – Exposure - Antigens Fungal and Bacterial Antigens -Farmer's lung - Moldy hay - Micropolyspora faeni . -Bagassosis - Moldy pressed sugar cane (bagasse ) - Thermophilic actinomycetes. -Maple bark disease - Moldy maple bark - Cryptostroma corticale . -Humidifier lung - Cool-mist humidifier -Thermophilic actinomycetes, Aureobasidium pullulans -Malt worker's lung - Moldy barley - Aspergillus clavatus . -Cheese washer's lung - Moldy cheese - Penicillium casei . Insect Products -Miller's lung - Dust-contaminated grain - Sitophilus granarius (wheat weevil) . Animal Products -Pigeon breeder's lung - Pigeons - Pigeon serum proteins in droppings . Chemicals -Chemical worker's lung - Chemical industry - Trimellitic anhydride, isocyanates .

MorphologyPatchy mononuclear cell infiltrates, demonstrated in both acute and chronic forms of hypersensitivity pneumonitis. Lymphocytes predominate, but plasma cells and epithelioid cells are also present.In acute forms of the disease, variable numbers of neutrophils also may be seen.Interstitial noncaseating granulomas are present in more than two-thirds of cases.In advanced chronic cases, diffuse interstitial fibrosis occurs.Interstitial fibrosis and obliterative bronchiolitis (late stages)Intra-alveolar infiltrates in over 50%

Hypersensitivity pneumonitis, histologic appearance. Loosely formed interstitial granulomas and chronic inflammation are characteristic.

Clinical Course
May present either :As a may present either as an acute reaction with fever, cough, dyspnea, and constitutional complaints 4 to 8 hours after exposure .As a chronic disease with insidious onset of cough, dyspnea, malaise, and weight loss.Temporal relationship of symptoms to exposure to the incriminating antigen in acute rxn makes diagnosis obvious.

Pulmonary Eosinophilia These diverse diseases are generally of immunologic origin but are incompletely understood .characterized by an infiltration and activation of eosinophils, the latter by elevated levels of alveolar IL-5.Pulmonary eosinophilia is divided into the following categories: 1. Acute eosinophilic pneumonia with respiratory failure. -characterized by: rapid onset of fever, dyspnea, hypoxia, and diffuse pulmonary infiltrates on chest radiograms. 2. Simple pulmonary eosinophilia (Löffler syndrome). -characterized by transient pulmonary lesions, eosinophilia in the blood, and a benign clinical course. -The alveolar septa are thickened by an infiltrate containing eosinophils and occasional giant cells

Pulmonary Eosinophilia 3. Tropical eosinophilia -caused by infection with microfilariae, a parasite. 4. Secondary eosinophilia, - Seen, for example, in association with asthma, drug allergies, and certain forms of vasculitis.1.Idiopathic chronic eosinophilic pneumonia. -Characterized by aggregates of lymphocytes and eosinophils within the septal walls and the alveolar spaces, typically in the periphery of the lung fields . -accompanied by high fever, night sweats, and dyspnea. -Good response to corticosteroids

Smoking-Related Interstitial Diseases
Desquamative interstitial pneumonia (DIP) and respiratory bronchiolitis are the two eg.Accumulation of large numbers of macrophages with abundant cytoplasm containing dusty brown pigment (Smoker's macrophages ) in the airspaces in DIP. - The alveolar septa are thickened by a sparse inflammatory infiltrate (usually lymphocytes), and interstitial fibrosis, when present, is mild. - good prognosis with excellent response to steroid therapy and smoking cessation.Respiratory bronchiolitis .characterized by the presence of pigmented intraluminal macrophages akin to DIP, but in a "bronchiolocentric" distribution (first- and second-order respiratory bronchioles).

Clinical course DIPpresents in the fourth or fifth decade of life, more common males than females 2 : 1.Virtually all patients are cigarette smokers.

Desquamative interstitial pneumonia. Medium-power detail of lung to demonstrate the accumulation of large numbers of mononuclear cells within the alveolar spaces with only mild fibrous thickening of the alveolar walls

PULMONARY ALVEOLAR PROTEINOSIS
Pulmonary alveolar proteinosis (PAP) is a rare disease Characterized : -Radiologically by bilateral patchy asymmetric pulmonary opacification . -Histologically by accumulation of acellular surfactant in the intra-alveolar and bronchiolar spaces. Three distinct classes of this disease. acquired, congenital, and secondary PAP. 1. Acquired PAP is of unknown etiology. -Without any familial predisposition; it represents 90% of all cases of PAP. -Now considered to be autoimmune disorder and can occur post double lung transplant 2. Congenital PAP is a rare cause of immediate-onset neonatal respiratory distress. -Cause unclear

PULMONARY ALVEOLAR PROTEINOSIS
1. SecondaryUncommonCauses include acute silicosis Other inhalational syndromesImmunodeficiency disordersMalignancy Hematopoietic disorders

Morphology.
Characterized by a peculiar homogeneous, granular precipitate within the alveoli.Minimal inflammatory reactionCausing focal-to-confluent consolidation of large areas of the lungs with minimal inflammatory reaction.On section, turbid flud exudes from these areas.Marked increase in the size and weight of the lung

Pulmonary alveolar proteinosis, histologic appearance. The alveoli are filled with a dense, amorphous, protein-lipid granular precipitate, while the alveolar walls are normal.