-
8/11/2019 Healthcare - Managed Care 2013.12
1/64
Please see General Disclaimers on the last page of this
report.
Current Environment
............................................................................................
1
Industry Profile
....................................................................................................
22
Industry Trends
...................................................................................................
24
How the Industry Operates
...............................................................................
41
Key Industry Ratios and Statistics
...................................................................
47
How to Analyze a Managed Care Company
.................................................. 49
Glossary
................................................................................................................
55
Industry References
...........................................................................................
57
Comparative Company Analysis
......................................................................
59
This issue updates the one dated May 2013.
The next update of this Survey is scheduled for May 2014.
Industry SurveysHealthcare: Managed Care
Phillip M. Seligman, Managed Health Care Equity Analyst
NOVEMBER 2013
CONTACTS:
INQUIRIES & CLIENT RELATIONS
800.852.1641
clientrelations@
standardandpoors.com
SALES
[email protected]
MEDIA
Marc Eiger
212.438.1280
[email protected]
S&P CAPITAL IQ
55 Water Street
New York, NY 10041
mailto:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]
-
8/11/2019 Healthcare - Managed Care 2013.12
2/64
Topics Covered by Industry Surveys
Aerospace & Defense
Airlines
Alcoholic Beverages & Tobacco
Apparel & Footwear:Retailers & Brands
Autos & Auto Parts
Banking
Biotechnology
Broadcasting, Cable & Satellite
Chemicals
Communications Equipment
Computers: Commercial Services
Computers: Consumer Services &the Internet
Computers: Hardware
Computers: Software
Electric Utilities
Environmental & Waste Management
Financial Services: Diversified
Foods & Nonalcoholic Beverages
Healthcare: Facilities
Healthcare: Life SciencesTools & Services
Healthcare: Managed Care
Healthcare: Pharmaceuticals
Healthcare: Products & Supplies
Heavy Equipment & Trucks
Homebuilding
Household Durables
Household Nondurables
Industrial Machinery
Insurance: Life & Health
Insurance: Property-Casualty
Investment Services
Lodging & Gaming
Metals: Industrial
Movies & Entertainment
Natural Gas Distribution
Oil & Gas: Equipment & Services
Oil & Gas: Production & Marketing
Paper & Forest Products
Publishing & Advertising
Real Estate Investment Trusts
Restaurants
Retailing: General
Retailing: Specialty
Semiconductor Equipment
Semiconductors
Supermarkets & Drugstores
Telecommunications: Wireless
Telecommunications: Wireline
Thrifts & Mortgage Finance
Transportation: Commercial
Global Industry Surveys
Airlines: Asia
Autos & Auto Parts: Europe
Banking: Europe
Food Retail: Europe
Foods & Beverages: Europe
Media: Europe
Oil & Gas: Europe
Pharmaceuticals: Europe
Telecommunications: Asia
Telecommunications: Europe
S&P Capital IQ Industry Surveys
55 Water Street, New York, NY 10041
EXECUTIVE EDITOR:EILEEN M. BOSSONG-MARTINES ASSOCIATE
EDITOR:CHARLES MACVEIGH STATISTICIAN:SALLY KATHRYN NUTTALL
CLIENT SUPPORT:1-800-523-4534. ISSN0196-4666.
VISIT THE S&P CAPITAL IQ WEBSITE:www.spcapitaliq.com
S&P CAPITAL IQ INDUSTRY SURVEYS (ISSN 0196-4666) is
published weekly. Reproduction in whole or in part (including
inputting into a computer) prohibitedexcept by permission of
S&P Capital IQ. To learn more about Industry Surveysand the
S&P Capital IQ product offering, please contact our Product
Specialist team
at 1-877-219-1247 or visit getmarketscope.com. Executive and
Editorial Office: S&P Capital IQ, 55 Water Street, New York, NY
10041. Officers of McGraw HillFinancial: Douglas L. Peterson,
President, and CEO; Jack F. Callahan, Jr., Executive Vice
President, Chief Financial Officer; John Berisford, Executive
Vice
President, Human Resources; D. Edward Smyth, Executive Vice
President, Corporate Affairs; Charles L. Teschner, Jr., Executive
Vice President, Global Strategy;
and Kenneth M. Vittor, Executive Vice President and General
Counsel. Information has been obtained by S&P Capital IQ
INDUSTRY SURVEYS from sources
believed to be reliable. However, because of the possibility of
human or mechanical error by our sources, INDUSTRY SURVEYS, or
others, INDUSTRY SURVEYS
does not guarantee the accuracy, adequacy, or completeness of
any information and is not responsible for any errors or omissions
or for the results obtained from
the use of such information.
Redistribution or reproduction is prohibited without written
permission. Copyright 2013 Standard & Poors Financial Services
LLC. All rights reserved.
STANDARD & POORS, S&P, S&P CAPITAL IQ, S&P 500,
S&P MIDCAP 400, S&P SMALLCAP 600, and S&P EUROPE 350
are registered trademarks of Standard &
Poors Financial Services LLC.
-
8/11/2019 Healthcare - Managed Care 2013.12
3/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 1
CURRENT ENVIRONMENT
Evolution in managed care
The federal government, through passage of the Patient
Protection and Affordable Care Act (ACA) in 2010,is attempting to
strengthen the overall US healthcare system by setting regulations
that will govern theindustry. The first set of provisions took
effect on September 23, 2010, with more implemented in 2011
andsubsequent years. As these new rules have begun to take effect,
managed care organizations (MCOs) arebeing forced to evolve and
adapt to the changing conditions. S&P Capital IQ (S&P)
believes that all sectorsof the healthcare industry are being
affected, but the managed care group will see the greatest
impact.
The cloud of uncertainty surrounding the legality of the
healthcare reform law was removed by the June2012 decision of the
US Supreme Court to uphold the individual mandate provision of the
law, while alsogiving states the choice to opt out of the Medicaid
expansion plan. (The decision is discussed in more
detailbelow.)
Until late 2007, a confluence of trends helped the managed care
industry thrive: a strong economy, pricing
discipline, moderating medical cost trends, enrollment gains
(including an influx of Medicare and Medicaidbeneficiaries into
private managed care programs), geographic expansion, and ongoing
consolidation.Disciplined control of administrative
functionsincluding above-average cost cuts and information
systemupgradeswas another positive driver.
Then, a recession began in December 2007. Although it officially
ended in June 2009, unemployment ratesrose until October 2009
before trending down, albeit slowly. This rise in unemployment
created obstacles to
growth for MCOs, as commercialmembership rolls dropped
meaningfully.However, the number and percentage ofthose insured
increased in 2012, to263.2 million and 84.6%, respectively,from
260.2 million and 84.3% in 2011.According to the US Census
Bureau,2011 was the first year in 10 years thatthe percentage of
those insured did notdecline, and 2012 showed furtherprogress.
The Henry J. Kaiser Family Foundation(KFF), a nonprofit
healthcare researchand analysis firm, attributed this reversalof
trend mainly to the provisions of theACA, and to the decline in
income levelsin 2011, making more Americans
eligible for coverage. We think that this reversal was due
primarily to the ACA requiring insurers to allowparents to keep
adult children on their plans until age 26. Such gains have more
than offset the continued
loss of employer-sponsored coverage (at least so far),
particularly among adults aged 45 to 64. Moreover,we believe the
gains were more profitable for the insurers as the newly insured
younger members tend to behealthier, as a group, than the existing
or lost enrollment.
According to the Census Bureau, the percentage and number of
people covered by Medicaid in 2012 werenot statistically different
from 2011, at 16.4% and 50.9 million, while the percentage and
number of peoplecovered by Medicare increased in 2012 to 15.7% and
48.9 million, from 15.2% and 46.9 million in 2011.We believe the
trend in Medicaid is as expected, given the declining unemployment
rates and that realmedian family and nonfamily household incomes in
2012 were not statistically different from 2011 levels.
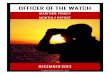
Chart H06: THEUNEMPLOYMENTSITUATION
(1,250)
(1,000)
(750)
(500)
(250)
0
250
5004
5
6
7
8
9
10
11
2008 2009 2010 2011 2012 2013
Net change in nonfarm employees (thousands, right scale)
Unemployment rate (%, left scale)
THE UNEMPLOYMENT SITUATION
Source: US Bureau of Labor Statistics.
(Inverted scale, thousands)(%)
-
8/11/2019 Healthcare - Managed Care 2013.12
4/64
2 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
The rise in the number and percentage of Medicare beneficiaries
is also unsurprising, as seniors account foran increasing
percentage of the US population.
Impact of the ACA on employers in 2014
The reforms set to take effect in 2014 under the ACA would
impose a penalty on large employers (thosewith 500 or more
employees) that do not offer affordable health insurance to their
employees. Further, the
reforms would provide premium tax credits to lower-income
persons in order to enable them to buyinsurance in state exchanges
if affordable employer coverage is unavailable to them.
According to the National Institute for Health Care Reform
(NIHCR), a nonprofit health policy researchorganization, the ACA
provides large firms with a strong economic incentive (averaging
$2,503 peremployee) to provide insurance to employees. However,
small firms (with fewer than 50 employees) willhave less economic
incentive (averaging $990 per employee), in large part because
these employers will beexempt from the penalty. The NIHCR defines
the economic incentive or disincentive as the amountcalculated by
adding the dollar value of the employer-sponsored insurance tax
subsidy and the value ofavoiding the penalty for not offering
insurance, and then subtracting the value of the premium tax
creditsthat eligible workers could use in an exchange if their
employer does not offer coverage.
Hence, we would not be surprised if some small businesses opt
for the healthcare penalty if the total cost ofthe penalties is
below that of the cost of their premiums, as noted in an April 2013
Wall Street Journal
article. We are also not surprised by the findings of the US
Chamber of Commerces Q2 2013 SmallBusiness Outlook Survey,
published in July 2013. In the survey, 79% of respondents said that
the ACAwill make coverage for their employees more expensive, while
71% felt that the law will make it harder forthem to hire; in
addition, 27% indicated that they will cut hours to reduce their
number of full-timeemployees and 23% will replace full-time
employees with part-timers.
The Wall Street Journalreported on May 27, 2013, that small
businesses seeking to avoid the ACAsprovisions at least for a while
are considering offers by some insurers to allow them to renew
theircontracts in December 2013, rather than in January, when they
would normally renew. The article went onto note that some state
regulators and benefits lawyers question the tactic, highlighting
that Illinois andRhode Island are disallowing early health plan
renewals for small businesses. Separately, a Wall Street
Journalarticle published on May 28 noted that some insurers have
begun to offer small companies theopportunity to self-insure. Under
self-insurance, employers pay benefits firms or health insurers a
fee to
administer the plans, but the employers are fully responsible
for paying for their employees medical costs.Under the ACA,
companies that self-insure do not have to offer the richer benefits
that will be required oftraditional health insurance, in which the
insurer is paid a premium and absorbs the medical cost risks.
Self-insurance has long been a popular practice among large
employers. They absorb the risks, but it gives themmore control
over their benefit offerings, is less costly than traditional
insurance, and the costs are broadlyspread over a large employee
base. The risk to a small firm is that it will have to more fully
absorb thesizable medical bills of an employee who has a serious
accident or disease.
HEALTHCARE REFORM ARRIVES
Healthcare reform, as defined by the Patient Protection and
Affordable Care Act, which was signed into lawby President Obama on
March 23, 2010, requires most US citizens and legal residents to
have minimumessential health insurance coverage. Accompanying that
bill was the Health Care and Education Reconciliation
Act of 2010, which was signed into law on March 30, 2010. (To
simplify, both Acts will be referred to asthe ACA in this
Survey.)
In February 2013, the nonpartisan Congressional Budget Office
(CBO), a research arm of Congress, and thestaff of the Joint
Committee on Taxation (JCT) estimated that the ACA (including only
those provisionsrelated to healthcare in the Reconciliation Act)
would have a gross cost of around $1.6 trillion (about $60billion
lower than the projection in August 2012) and would increase the
deficit to around $1.2 trillion (aboutthe same amount as projected
in August 2012) over the 11-year period from 2013 to 2023. The CBO
and JCTbelieve that more people will obtain health insurance
through the newly established health insurance
-
8/11/2019 Healthcare - Managed Care 2013.12
5/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 3
exchanges and that the reductions in spending from lower
Medicaid enrollment are expected to outweighthe increased costs
from greater participation in the exchanges. It also expects more
people to be uninsured.
US Supreme Court finds healthcare reform law constitutional
On June 28, 2012, the US Supreme Court upheld the
constitutionality of the ACA in a 54 vote. The courtupheld the
individual mandate provision, which will require Americans who can
afford health insurance to
purchase it as of 2014, saying Congress could impose the mandate
under its power to lay and collect taxes(as provided in the US
Constitution). However, the court rejected the part of the law that
made it mandatoryfor the states to expand their Medicaid programs
to include citizens under age 65 with family incomes below138% of
the federal poverty level under the threat of losing their Medicaid
funding. The court ruled that thispart was unconstitutional because
it was coercive. The states now have the option to join the
expanded planand receive enhanced federal funding.
What does healthcare reform do?
The ACA requires most individuals and their families to have
health insurance, and imposes financialpenalties on those who
choose not to purchase it. The law also requires employers to
provide coverage fortheir employees, with tax breaks to help them
provide it and penalties if they do not. It expands
Medicaideligibility and provides funding to states to set up
special health plans to cover those ineligible for Medicaid,but too
poor to pay for their own coverage. It also sets up exchanges where
individuals and employers mayobtain health insurance at competitive
prices. It prevents insurers from limiting, dropping, or refusing
toprovide coverage, and allows dependent children to remain on
their parents plans until they are 26.
The reform legislation includes the following features: an
insurance program from 2010 to 2014 for adultswho have been without
insurance for at least six months and who have a pre-existing
condition; a provisionfor children under 19 having a pre-existing
condition; an early-retiree reinsurance program; and discountson
prescription drugs to Medicare Part D beneficiaries when the
beneficiaries reach the coverage gap. Therules and regulations
regarding coverage will be phased in over a multiyear period.
The legislation originally aimed to cover 94% of all non-elderly
residents (excluding undocumentedimmigrants) by reducing the number
of uninsured by an estimated 32 million by 2019, or 34 million
by2021. We note that an estimated 23 million people would still
have remained uncovered in 2019. However,according to the CBO, the
Supreme Court decision would lead to an increase in the number of
uninsured:29 million in 2019 and 30 million in 2023.
To further its goal of higher enrollment, the ACA includes
provisions for Medicaid coverage, reducedpremium costs, and lower
cost-sharing for families that cannot afford health insurance
coverage (those withincomes ranging from 100% to 400% of the
federal poverty level). According to the June 2012 ruling bythe US
Supreme Court, states have the option of providing Medicaid
coverage to most people with incomelevels below 138% of the poverty
level. According to a study by the KFF published in November 2012,
if allstates agreed to the expansion, Medicaid coverage would
increase by 41%, and an additional 21.3 millionpeople would get
coverage by 2022. Beginning January 1, 2014, the ACA would include
lower premiumcosts through tax credits to people with income levels
up to 400% of the poverty level and insurance planswith reduced
cost-sharing to people with income levels up to 250% of the poverty
level.
As of this writing, each state has its own laws to regulate how
insurance companies set premium rates forthose seeking coverage,
including such factors such as their health condition and
demographic status.
However, starting on January 1, 2014, federal law will govern
the premium rates applied to individuals andsmall businesses. As
per the ACAs minimum premium rating rule, premium rates can vary
based on onlythe following four factors: individual versus family
enrollment, geographic area, age, and tobacco use. Alsoeffective
from January 1, 2014, under the revised ACA guaranteed issue laws,
all individual and small-groupapplicants will be guaranteed the
issuance of policies, irrespective of their health status or any
other factors.
Many will buy their insurance via public state-based) and
private exchanges
Starting October 1, 2013, individuals without employer-covered
health insurance and some small businesseshave been able to shop
for health insurance for the 2014 calendar year (starting January
1) through onlinemarketplaces known as health insurance exchanges.
The health insurance exchange concept was set into law
-
8/11/2019 Healthcare - Managed Care 2013.12
6/64
4 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
by the ACA. Some states (14 states and the District of Columbia)
operate their own exchanges; in otherstates, the federal government
has set up and runs the public exchanges directly (26 states), or
worked inpartnership with some states (10 states) to establish and
run the exchanges.
In addition to the public exchanges, private exchanges offering
health plans conforming to the ACAregulations have been created by
human resource consultancies to offer choices for the employees of
manymid-sized and large companies. The employer mandatethe
requirement that employers with 100 or moreworkers obtain health
insurance for their employeeswas delayed to 2015. Also delayed was
theimplementation of the Small Business Health Options Program, or
SHOP exchange, which would giveemployees of small businesses (less
than 50 employees, but up to 100 in 2016) a choice of health plans
inthe states where the federal government is involved in operating
the exchanges. However, a few statesrunning their own exchanges,
including California and Connecticut, have offered the employee
choicemodel for small businesses for the 2014 plan year, though it
is not required by the federal government.
When one applies for insurance from the exchange, the
application will require such information ashousehold size, income,
location, and citizenship status. Those earning between 100% of the
federal povertylevel, or FPL ($11,490 in 2013 for an individual and
$23,550 for a family of four in the 48 contiguousstates and the
District of Columbia) to 400% ($45,960 and $94,200, respectively)
will be eligible for asubsidy in the form of a tax credit called
the Advance Premium Tax Credit. This tax credit is applied to
themonthly premiums, enabling the applicant to get the lower
insurance price immediately. Hence, for
applicants with incomes within the ranges, the net price they
will have to pay is below the full price listed inthe exchange.
Those with incomes above the ranges pay the full listed price out
of pocket. ParticipatingMCOs receive the full premium price,
whether or not part of it is subsidized.
On the public exchanges, the health plans are grouped by levels
of coverage, including how much the planwill pay for ones
healthcare and what services are covered. All of the health plans
have to offer the sameessential benefits, but each can provide
additional benefits to attract buyers. Each level is named after
ametal (Bronze, Silver, Gold, and Platinum), and they vary by the
percentage of costs one has to pay, onaverage, for the healthcare
received. Bronze plans offer the lowest coverage, and platinum the
most, and theplans vary by the percentage of costs one pays on
average toward the healthcare one receives. At the bronzelevel, one
pays 40% of the costs out-of-pocket whenever one sees a doctor or
purchases a medicine, while atthe platinum level, one pays only
10%. However, bronze has the lowest premium, and platinum the
highest.On the exchanges, the health plans are organized by metal
level, then by brand ( i.e., by insurer), and then by
type of health plan, such as HMO, PPO, POS, or high-deductible
plans with a savings account.
Interestingly, an analysis of the 1,923 plans being sold on 34
federally run exchanges (published in October2013 by KFFs daily
online newsletter, Kaiser Health News) found that the exchange
plans vary withincounties and across the country, even if they are
the same type of plan. This is unsurprising, since the cost
ofliving differs in different parts of the US. In any event, 806 of
these plans are HMOs and 714 are PPOs.
S&P believes there will be plenty of healthier enrollees in
the public exchanges to keep the ratio of healthyand sick
applicants in the risk pool relatively steady. Some businesses that
employ a large percentage ofpart-timers and provide insurance for
those employees are likely to opt to drop that insurance coverage
and,instead, provide a small subsidy to help them purchase
insurance through the public exchanges. One outfitfollowing this
path is Trader Joes, a closely held grocery-store chain, which will
provide these workers witha $500 stipend. In addition, various news
sources report that to save on employee costs, a number of
employers (including some public school systems) have been
reducing their part-time workers hours tounder 30 per week
(regardless of whether they previously provided health insurance to
such workers). Theseworkers are being encouraged to obtain
subsidized health insurance via the public exchanges. (The
ACArequires firms to provide employer coverage to employees working
30 hours per week or more.)
As noted earlier, in addition to the public exchanges,
multi-insurer private (or corporate) exchanges havebeen created by
human resource consultancies Aon Hewitt, Towers Watson, and Mercer,
a division ofMarsh & McLennan Companies Inc. The insurance
offered via the private exchanges must comply with theACA and state
regulations. One major difference between the two types is that the
government does notsubsidize the purchase of policies in private
exchanges. Instead, employers will give eligible employees a
-
8/11/2019 Healthcare - Managed Care 2013.12
7/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 5
fixed amount for individual or family coverage, regardless of
the plan, and the employee chooses among thedifferently priced
plans offered by the various insurers participating in the private
exchange. The employeecontributes from his or her salary, on a
pre-tax basis, the difference between the price of
insurancepremiums and the subsidy from the employer. This model has
been referred to as defined contributionhealth care, given its
similarity to a 401(k) retirement plan, wherein employers monetize
their commitmentin the form of a defined contribution rather than a
defined benefit, as defined in a report by the Society for
Human Resource Management, a trade group. We believe the use of
private exchanges will have a neutralimpact on MCOs
profitability.
According to CBO estimates as of May 2013, seven million people
would buy health insurance through thepublic exchanges for the 2014
health plan year, while employment-based coverage would total 157
million.The CBO estimated, as of May 2013, that public exchange
enrollment by individuals and their familieswould reach 24 million
by 2023, while employment-based coverage would increase by 12
million, to 169million.
but the selection in the public exchanges might be somewhat
limited at first
For the 2014 health plan year, some large publicly traded MCOs,
including Aetna Inc., Cigna Inc., andUnitedHealth Group Inc.,
severely limited their participation in the public exchanges.
S&P believes theywanted to test the waters first to see the
profitability of exchange participation. Indeed, UnitedHealth
pulledout of Californias individual market in early July 2013,
while Aetna has exited seven of the 14 publichealth insurance
exchanges in which it originally intended to participate. However,
Coventry Health Care,which was acquired by Aetna in 2012, also
filed plans under its own name for some exchanges. Aetnadecided to
drop out of some states where Coventry filed plans and dropped
Coventry plans in some stateswhere it decided to file plans under
its own name. All told, Aetna and Coventry combined have
plansavailable statewide in 10 states and with limited geographies
in seven others. Cigna Corp. is selling plans inonly five states,
half of the states in which it had been selling individual plans.
In any event, these MCOshave a relatively small presence in the
individual market. Humana Inc. and WellPoint Inc., which have
largeindividual businesses, appear to be more committed to the
public exchanges. All large MCOs will beactively participating in
the private exchanges, however.
The large, publicly traded MCOs were not alone in pulling out of
exchanges in which they initially plannedto participate.
Interestingly, FirstCarolinaCare Insurance Co., a subsidiary of the
private, not-for-profithealthcare services network FirstHealth of
the Carolinas, exited the public exchange of its home state,
North Carolina. However, Coventry Health Care of the Carolinas,
a part of Aetna, remained in theexchange. FirstHealthcares exit
appears to us to parallel Aetnas exit from the public exchange of
its homestate, Connecticut.
Some smaller, publicly traded MCOs with a significant percentage
of Medicaid enrollment (such as MolinaHealthcare Inc., Health Net
Inc., and Centene Corp.) are participating in the public exchanges
for the 2014plan year, while WellCare Health Plans Inc. is not.
However, Health Net has been a long-term player in theindividual,
non-Medicaid market. At its September 19, 2013, investor meeting,
Molina indicated that it isnot participating in the exchanges to
get new Medicaid beneficiaries (which are assigned by the states),
butmainly to retain members they are poised to lose due to a change
in status (e.g., new employment that givesthe member an income too
high to qualify for Medicaid). Those members may wish to remain
with theirinsurers to keep their providers (doctors and hospitals),
and we do not see pent-up demand from them.However, given these
MCOs Medicaid market experience, we believe they are reasonably
well equipped to
handle the initial pent-up demand from the previously uninsured
who sign up with them through the publicexchanges.
The transition begins
A number of companies have already begun to transition employees
and/or retirees (both those under 65years of age and those
Medicare-eligible) to private exchanges. The public exchanges are
not available forMedicare beneficiaries. Those without access to
private exchanges could continue to go to Medicare.govduring its
open enrollment period, which began October 15. Early users of Aon
Hewitts exchange for the2013 plan year include employees of Sears
Holding Corp. and Darden Restaurants. International Business
-
8/11/2019 Healthcare - Managed Care 2013.12
8/64
6 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
Machines Corp., Time Warner Inc., Caterpillar Inc., and E.I. du
Pont de Nemours and Co. are among thoselarge companies reported to
be moving their retirees to private exchanges run by Aon Hewitt and
the otherconsultancies for the 2014 plan year. Walgreen Co. has
announced that it will give employees acontribution toward coverage
in a private exchange. Employers are also raising deductibles,
giving workershealth savings accounts that look like 401(k)
retirement plans, setting up private in-house exchanges thatmimic
the online insurance exchanges, and encouraging workers to compare
prices and shop around for
treatments, according to a September 17, 2013 article in Kaiser
Health News.
Note, though, that the ACA does not require companies with fewer
than 50 workers to offer coverage fortheir workers. It created
online exchanges for the small employers to purchase insurance
similar to policiesoffered through the online exchanges for
individuals. However, employees of small businesses will be
unableto choose from multiple plans in most states until 2015.
but there will still be millions who remain uninsured
Adults living with dependent children and single adults with
disabilities whose income falls below 100% ofthe FPL, or all adults
with incomes below 138% in states that accepted the ACAs Medicaid
eligibilityexpansion, can qualify for his or her states Medicaid
program. This can be determined when one appliesfor insurance via a
public exchange. S&P believes only a very small percentage of
those applying throughthe exchanges will fall into the below-100%
category. In any event, once a person is deemed eligible
forMedicaid, that person does not choose his or her health plan.
The state assigns the Medicaid coverage eitherthrough direct
coverage or to an insurer operating in the new Medicaid
beneficiarys home county. Thatsaid, S&P believes MCOs will
continue to see enrollment expansion from states still
transitioning theirMedicaid populations to private insurers.
However, in many states, impoverished adults under 65 years of
age, without disabilities and withoutdependent children, are
currently ineligible for Medicaid. Under the ACA, their coverage
would besubsidized if their incomes are at least 100% of the FPL.
However, the Commonwealth Fund, a privatefoundation supporting
research on healthcare issues, estimates that some two in five
uninsured adults whoare living in the 26 states that have decided
not to expand their Medicaid programs (or are undecided) willnot
have access to Medicaid or to subsidized health insurance plans on
the public exchanges. The CBOprojected in May 2013 that the number
of uninsured non-elderly people (including unauthorizedimmigrants,
as well as people who are eligible for but not enrolled in
Medicaid) will decline from 55 millionin 2013 to 30 million by
2017, and will remain in the 30 million31 million range through
2023.
RESISTANCE TO THE ACA BECOMES SHARPER
The implementation of the healthcare reforms contained in the
ACA became more certain with the SupremeCourt decision on the ACAs
constitutionality in June 2012 and President Obamas re-election in
November2012. Nevertheless, resistance to the ACA has continued. At
the federal level, in March 2013, the US Senaterejected Republican
Paul D. Ryans attempt to repeal the ACA.
The fight later became more extreme. From September 20 to
October 1, 2013, the Republican-controlled USHouse of
Representatives sent a bill to raise the federal debt ceiling four
times to the Democratic-led Senate.However, it also included
provisions to strip financing for the ACA in the first attempt, to
delay the healthcarelaw by one year and repeal the tax on medical
devices in the second attempt, to delay the individual mandatein
the third attempt, and to cancel subsidies for lawmakers in the
fourth attempt. In each of the first three
times, the Senate stripped the healthcare provisions and sent
the bill back to the House.
The government shutdown began at 12 a.m. October 1, and later
that morning, the Senate rejected theHouse measure. Senate Majority
Leader Harry Reid (D., Nevada) and President Obama refused to
negotiateon the ACA and sought a clean spending bill. Neither side
was giving in and many federal governmentdepartments and services
shut down. On October 17, after the Democratic-led Senate passed an
agreementbetween Senate Majority Leader Harry Reid and Minority
Leader Mitch McConnell (R., Kentucky) to endthe tense political
standoff by an 8118 vote, the House voted 285144 to pass the deal,
and PresidentObama quickly signed it.
-
8/11/2019 Healthcare - Managed Care 2013.12
9/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 7
Interestingly, a conservative group of House Republicans, known
as the Republican Study Committee,unveiled a healthcare reform
alternative on September 18, 2013, called American Health Care
ReformAct. This calls for the full repeal of the ACA and, instead,
would provide $20,000 in tax deductions tofamilies and a $7,500
deduction to individuals, so they can purchase insurance from
vendors in any state. Italso creates a 10-year, $25 billion fund to
lower costs for those with pre-existing conditions such as
cancer,and allows consumers to carry their insurance from job to
job. On October 15, this proposed bill was
referred to the Subcommittee on Regulatory Reform, Commercial
and Antitrust Law. As this Surveywentto press in mid-November 2013,
the bill had not yet been reviewed on the floor of the House
ofRepresentatives.
Meanwhile, at the state level, the setting up of insurance
exchanges had generated opposition, with 26 statesdefaulting to
fully federally built and operated exchanges for individuals and
families without employment-based insurance. Another example of
state resistance, according to an article published September 17,
2013, inthe New York Times, is Florida, which is not participating
in the exchange program (thus leaving the federalgovernment fully
responsible for setting one up in the state and running it). In
addition, however, the state hasrequired that health navigators
(i.e., individuals assigned to help people enroll in the exchanges)
undergofingerprinting and criminal background checks, and bars them
from conducting any business on propertycontrolled by the state or
county health agencies. In an article posted on the website of The
Hill, aWashington, D.C.based newspaper that specializes in coverage
of the US Congress, at least 18 states havetaken steps to restrict
the counselors activities or have imposed additional training. And,
among these states,several that are Republican-led have imposed
criminal background checks and examination requirementsthat exceed
whats mandated by federal law. The Republicans have argued that
they are trying to protectpeople from fraud and that without this
additional scrutiny, the program could admit felons as
counselors.Indeed, in October 2013, the websites of several
conservative media outlets (Fox News and the NationalReview)
provided examples of some people they felt should not have been
hired as navigators.
Republican-led states, for the most part, have continued to
oppose Medicaid expansion to cover people withincomes up to 138% of
the FPL. For example, the Republican governor of Texas, Rick Perry,
rejectedMedicaid expansion in his state. Even Republicans who
support Medicaid expansion, such as FloridaGovernor Rick Scott,
faced opposition from the Republican-controlled Florida House and
Senate.
As of September 23, 2013, the governors of 22 states and the
District of Columbia supported Medicaidexpansion, 12 opposed, and
16 were weighing options. Many governors opposing expansion said
they could
not support expansion without program reforms, legislative
approval, or permission to use the Medicaid fundsto purchase
private health insurance, according to KFFs statehealthfacts.org
website. Interestingly, despite thelaws unpopularity in Southern
states, the expansion of Medicaid is supported by about two-thirds
of adults inAlabama, Georgia, Louisiana, Mississippi, and South
Carolina, according to the Joint Center for Political andEconomic
Studies, a think tank. Separately, according to the a May 23, 2013,
Politico article, many statesmired in the fight over Medicaid
expansion are starting to give up on their first year of full
funding, and itsunclear whether they would be able to tap into the
funds before 2015. This could mean the loss of hundreds ofmillions,
and in some cases, billions, of dollars to cover low-income
residents. The challenge many face is theset-up of the
infrastructure to accommodate the influx of enrollees.
and some once in favor are having second thoughts
Having once supported the ACA, some unions are now concerned
that it will jeopardize benefits for millionsof their members,
according to a May 24, 2013, Associated Press article. The problem
is that multi-employer
plans, which cover over 20 million unionized workers in retail,
construction, transportation, and otherindustries with seasonal or
temporary employment, are more costly to run than single-employer
plans. Theyhave been facing higher costs as a result of certain ACA
mandates: that health plans cover dependents up toage 26, extend
coverage to people with pre-existing conditions, and eliminate
annual and lifetime coveragelimits. The unions fear that employers
will be tempted to drop coverage and have members fend for
themselvesin the health insurance exchanges. Interestingly, while
workers seeking coverage through the exchanges canqualify for
subsidies, the ACA does not allow union members to receive similar
subsidies. S&P believes theseunion plans will not disappear
quickly, as workers are covered under collective bargaining
agreements. The
-
8/11/2019 Healthcare - Managed Care 2013.12
10/64
8 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
New York Timesreported that on September 13, 2013, the US
Treasury Department denied federal tax creditsto workers who
receive health coverage under employee benefit plans sponsored by
more than one employer.
While not exactly resisting the ACA, some large employers may be
now considering offering bare-bones plans,according to a May 20,
2013, article in the Wall Street Journal. Some such plans may offer
only preventativeservices, and not cover surgery, X-rays, or
prenatal care. The ACA requires only plans sold to small
employersand individuals to be comprehensive. Apparently, a close
reading of the law reveals that companies with 50 ormore workers,
which would have to provide coverage or pay a penalty, are not
affected by the mandates ofessential benefits. Indeed, employers in
low-wage industries have been concerned how they can afford
thesebenefits, and some of the policies being offered cost less
than the penalty. Interestingly, such plans look to uslike the
so-called mini-med plans currently provided by low-wage
industries.
THE PUBLIC EXCHANGES OPEN WITH A BANG
The partial government shutdown did not delay the October 1
launch of the public healthcare exchanges,whereby individuals will
be able to purchase health insurance for themselves and their
families. The Presidentand the US Senate did not budge and the
exchange process is moving ahead, despite resistance to
thehealthcare reform law, including attempts to delay its
implementation by the Republican-controlled House.Indeed, the US
Department of Health & Human Services (HHS) has announced the
opening of the exchangeswith fanfare.
However, there have been problems, as S&P and others
expected, given the glitches in the federally run systemthat were
discovered while the system was being tested. One software glitch
was the problem in determiningthe level of subsidy one could
receive if he or she had income in the 100%400% of the federal
poverty level.Many problems have likely been fixed, but various
news sources have been reporting heavy on-line exchangetraffic on
the first couple of days, suggesting better-then-expected demand,
and system problems the first daysthe exchanges were open. S&P
believes many of the system problems relate to possible initial
system overload.S&P views this, plus the long wait times at
call centers, making the individual attempts to purchase
insuranceduring that time difficult.
On October 15, the HHS set the deadline of November 30 to fix
the system and appointed one of thecompanies behind HealthCare.gov
(the name of the federally run exchange website) as the
generalcontractor for the repairs. That company is Quality Software
Services Inc. (also known as QSSI Inc.),
which was acquired by giant MCO UnitedHealth Group Inc. in
September 2012, after the MCO wasselected to help set up
HealthCare.gov. (The acquisition was not announced by UnitedHealth,
S&P believes,because it was small. Jenner & Block, the law
firm representing QSSI in the takeover, announced it onOctober 9.)
QSSI had been behind the sites problematic account registration
tool and its data hub, whichallows information to be transferred
between different groups, but which officials said is functioning
well,according to an article posted October 25 on the website of
The Hill. In this regard S&P is not surprisedthat some
Republican senators became concerned that QSSI might have access to
information or wouldbuild the technology in a way that would give
UnitedHealths insurance business an advantage, according toan
article posted October 25 on the Washington Postwebsite. In
addition, computer engineers from techcompanies Google, Oracle, and
Red Hat have been enlisted to help with the tech surge to fix the
system.S&P has viewed the technical glitches as fixable.
People who wish to be covered as of January 1 have until
December 15 to sign up and pay for their first
month of the 2014 health plan year. As this Surveywent to press
in mid-November, the HHS had released theenrollment data on the
public exchanges covering the period of October 1 to November 2,
approximately thefirst month of open enrollment. According to the
HHSs November 13 press release, only 106,185 Americanshad selected
plans from the state and federal Health Insurance Marketplaces (the
HHSs term for the publichealth insurance exchanges) during that
period: 79,391 enrolled through exchanges run solely by 14 states
and26,794 enrolled in federally run exchanges in the other 36
states and the District of Columbia. According to aWall Street
Journalreport on November 13, one HHS memo had projected that some
500,000 people wouldobtain private health insurance coverage.
However, HHS notes another 975,407 made it through the processof
applying and receiving an eligibility determination, but have not
yet selected a plan. (Note that the healthinsurers will not count
any of those that enrolled as members until they pay their first
months premium.)
-
8/11/2019 Healthcare - Managed Care 2013.12
11/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 9
S&P Capital IQ believes the much smaller federal figure
relates to the technical issues plaguing the federalmarketplaces
(the state marketplaces, in contrast, had very few problems). We
also think that those who didnot yet select a plan are still
determining which one would be the most suitable. This is likely to
be time-consuming process: the associated provider networks may
differ, and consumers may be trying to determinewhich set of
doctors and hospitals would cover most, if not all, of their needs.
While we view the sign-upfigures to date as a bit disappointing,
people are looking. HHS reported that there were 26,876,727
visitors to
the state- and federally run exchange websites, and an estimated
3,158,436 calls to state and federal exchangecall centers. We also
think the low initial enrollment numbers may reflect the pattern
seen in Massachusetts,when that state initiated healthcare reform.
According to a New York Timesarticle published November 14,2013,
when that state expanded health coverage in 2007, only 127 people
(of the 36,167 who ultimatelyenrolled) signed up in the first
month, while 7,000 signed up in the last month. The federally run
exchangestechnical issues might also explain some of the difference
between what was expected and what occurred.
Meanwhile, another problem cropped up. Millions of currently
covered Americans were informed by theirinsurers that their plans
would be dropped as of January 1, primarily because the plans did
not meet all ofthe ACAs essential benefits requirements. This move
by the insurers ran counter to President Obamaspromise that those
who liked their insurance can keep it, and he expressed regret on
an NBC News interviewon November 7. Congress wanted to legislate a
change. On November 4, US Senator Mary L. Landrieu (D-Louisiana)
introduced the Keeping the Affordable Care Act Promise Act to keep
the promise that if apolicyholder liked his or her health
insurance, he or she could keep it as long as payments were
up-to-date.On November 7, US Senators Joe Manchin (D-West Virginia)
and Mark Kirk (R-Illinois) introducedlegislation to delay the
implementation of the individual mandate from January 1, 2014, to
January 1,2015. On November 8, Representative Fred Upton
(R-Michigan) introduced his Keep Your Health PlanAct, which would
enable people to keep their old insurance as long as they want; it
passed the House onNovember 14. President Obama promised to veto it
if it came across his desk.
On November 14, President Obama announced changes to the ACA to
give insurers the option to keepoffering consumers plans that would
otherwise be cancelled, even if they do not include all of the
essentialbenefits. This administrative change is only good for a
one-year extension. The term optional suggests tous that the
insurers have a choice to offer it to some plans and not others.
However, as this Surveywent topress, some state insurance
commissioners were for the policy change and some were against. The
healthinsurance industry, though not unanimous, was expressing
concern that the younger, healthier people willbe interested in
keeping old policies, which could overburden the new plans with a
greater-than-expected
proportion of high-cost members. We note that the Wall Street
Journalreported on November 18 that so-called high risk pools for
people rejected by health insurance companies that were supposedly
being phasedout as ACA rules kicked in are being given brief second
lives in some states due to problems with the federalexchanges.
S&P believes this should help temporarily reduce the costliest
members as a percentage of thetotal population enrolling through
the federal exchanges until the system is fully fixed. In addition,
the ACAprovides for a $20 billion fund, paid for by a reinsurance
tax imposed on health insurers and employerswho self-insure from
2014 to 2016, that would provide money to insurers that incur high
claims forconsumers in the individual insurance market, both inside
and outside the public exchanges.
However, open enrollment continues through March 31, 2014, and
people have been encouraged to try toaccess the system again if
they encounter problems the first time. In any event, the CBO
expects seven millionpeople to obtain coverage for the 2014 health
plan year through the public exchanges, and has not yet revisedthe
figure.
PAYING FOR IT ALL
The federal government plans to provide significant financial
help directly to eligible individuals (in the formof premium and
cost-sharing tax credits), employers (tax credits), and states
(assumption of a greaterpercentage of Medicaid and Childrens Health
Insurance Program costs). In addition, the ACA finesindividuals who
do not opt for purchasing coverage and employers who offer no
coverage to theiremployees. Since these fines will constitute only
a small percentage of the total cost of healthcare reform, themoney
has to come from elsewhere.
-
8/11/2019 Healthcare - Managed Care 2013.12
12/64
10 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
To compensate for the overall cost, the law has imposed certain
rules in the form of cuts and deductionsthat will affect different
groups across the industry. For instance, the ACA calls for closing
the coverage gapin the Medicare Part D prescription drug benefit
(the so-called donut holethe difference between theinitial coverage
limit and the catastrophic coverage threshold) by 2020. To help
accomplish this, the drugindustry will reduce prices by 50% on
brand-name drugs purchased in the donut hole, saving $20
billionover the next 10 years.
The pharmaceuticals industry agreed to increase the Medicaid
rebate (which drugmakers pay to stateMedicaid funds for the drugs
purchased), plus other concessions and fees on sales to other
governmenthealth programs, bringing Big Pharmas fees to about $85
billion over the next 10 years. Medical devicemanufacturers will
also contribute to the funding via the laws imposition of a 2.3%
excise tax on the sale oftaxable products in the US starting in
2013, which is expected to raise $20 billion over 10 years. (Unlike
fees,excise taxes are tax-deductible, thereby lowering the
after-tax impact and cushioning the overall effect.)
Meanwhile, in July 2009, the hospital industry agreed to a
reimbursement cut of about $155 billion over 10years, in part by
reducing the size of Medicares annual market basket updates (the
inflation rate adjustment).The ACA also calls for Medicare and
Medicaid disproportionate share hospital (DSH) payments to
bereduced (effective in fiscal 2014), and that payments made to
hospitals will be reduced to account forpreventable hospital
readmissions (effective fiscal 2013) and for hospital-acquired
conditions (effective fiscal2015), yielding a total $40 billion in
savings between 2014 and 2019.
Health insurers face additional fees, minimum medical cost
spending limits
The managed care group faces a fee that increases from $8.0
billion in 2014 to $14.3 billion in 2018; insubsequent years, fees
will rise by the rate of premium growth. (For not-for-profit
insurers, only 50% of netpremiums are counted.) Effective in
calendar 2009, the tax-deductibility of health insurer executive
andemployee compensation is limited to $500,000 per applicable
individual. A 40% excise tax imposed on thevalue of
employer-sponsored plans exceeding a certain threshold starts in
2018 and will raise an estimated$32 billion over 10 years.
Under the medical loss ratio (MLR; also known as the medical
cost ratio, or MCR) provision of the ACA,effective January 1, 2011,
health insurance plans have been required to reserve at least 80%
of thepremiums towards healthcare expenditure and quality
improvement initiatives, leaving only 20% for SG&Acosts. This
provision required the larger group plans to set aside a higher 85%
for healthcare and other such
expenses. If a plans MLR falls below the required minimum, MCOs
are required to rebate the difference tocustomers. In June 2012,
the US Department of Health & Human Services (HHS) announced
that insurancecompanies that failed to comply with the MLR
provision of the ACA were required to pay $1.1 billion in theform
of rebates to around 12.8 million Americans. The rebates received
covered premiums collected for the2011 plan year.
and, over time, reduced Medicare Advantage payments
Payments to Medicare Advantage (MA) plans will be restructured
going forward. For 2011, MA paymentswere frozen at 2010 levels.
Beginning in 2012, the payments had to begin to transition to a
percentage ofthe fee-for-service (FFS) cost in each state,
estimated by the Centers for Medicare & Medicaid Services(CMS),
a division of the US Department of Health & Human Services
(HHS). These payments wouldeventually range from 95% of traditional
Medicare FFS payment levels in high-spending states to 115%
inlow-spending states. The transition will be phased in over three
years for most areas, and over four to six
years in other areas, depending on the initial difference
between the current MA payments and thebenchmarks.
According to the CMS, MA premiums declined by 10% from 2010
through 2013, while enrollment in MAprograms increased by an
estimated 28%. However, on February 15, 2013, the CMS proposed a
2.3%reduction in MA payments for 2014. This outlook changed on
April 1, when the CMS issued its final 2014MA payment rate,
reflecting a positive 3.3% growth percentage. The new rate assumes
Congress will againprevent physician payment rates from
dropping.
-
8/11/2019 Healthcare - Managed Care 2013.12
13/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 11
The CBO projected the government will save $136 billion over 10
years to 2019. However, starting in2012, bonuses were given to MA
plans with quality rankings of at least three stars out of five or
those thatare unrated (i.e., plans that are too new or that have
too few enrollees).
On November 15, the Wall Street Journalreported that
UnitedHealth Group had dropped thousands ofdoctors from its
networks in recent weeks, leaving many Medicare patients unsure
whether they need toswitch plans to continue seeing their doctors.
In its third-quarter 2013 earnings conference call on October17,
the company said it expects its 2014 earnings outlook to be
impacted by overall Medicare Advantagefunding levels. It also
reported spending more healthcare premiums on medical claims in the
third quarter,due mainly to government cuts in payments for
Medicare Advantage services. According to the notices sentto the
doctors, the terminations can be appealed within 30 days.
UnitedHealth informed the Wall Street
Journal that the company expects its Medicare Advantage network
to be 85%90% of its present size by theend of 2014. Looking ahead,
we would not be surprised if other health insurers follow
UnitedHealths path.
IMPACT OF HEALTHCARE REFORM ON MANAGED CARE PROFITABILITY
We believe that managed care organizations will face more
restrictions as more provisions of the law comeinto effect. (See
the accompanying table entitled Healthcare Reform Legislation
Implementation Timeline.)Because healthcare reform extends health
insurance coverage to the uninsured, the law prohibits
certainactions: denying coverage to individuals with pre-existing
health conditions; rescission (rescinding enrollees
coverage); applying annual and lifetime limits on required
health benefits; and requiring prior authorizationfor emergency and
obstetric/ gynecological services. In addition, premiums can vary
by no more than 3:1 forage and 1.5:1 for tobacco use, though these
premium variations do not apply to self-insured plans (thosewhere
employers absorb the insurance risk and pay MCOs fees to administer
the plans). Of course, the marginpressure from the new MLR rules
and the industry fee also affects profitability.
What qualifies as a medical or benefit cost?
Requirements for minimum MLRs raised concerns among the insurers
regarding the cost components thatwill qualify as a medical or
benefit cost. MCOs have sought to transfer medical-related
administrationcostswhich have been accounted for as selling,
general and administrative (SG&A) costs on the
incomestatementto medical or benefit costs. On December 1, 2010,
the US Department of Health & HumanServices (HHS) published its
interim final rule on the MLR requirements for 2011, 2012, and
2013, afterreceiving guidance from the National Association of
Insurance Commissioners (NAIC), as required by the
ACA, and one year later issued its final rule.
Following the NAIC, the HHS defines medical costs (the numerator
in the MLR ratio) as health careclaims, plus any expenses to
improve health care quality. Expenses in the quality improvement
categorycould include activities that result in measurable
improvements in patient safety or patient outcomes, preventhospital
readmissions, promote wellness, or enhance health information
technology (IT) to improve quality,transparency, or outcomes. Under
the ACA, the provider credentialing is a part of the quality
improvementexpenses; however, insurance broker and agent
compensation are viewed as administrative expenses andfunds used to
fight medical fraud are viewed as cost-containment expenses. The
denominator of the MLRcalculation comprises earned premium revenue,
minus federal and state taxes (including regulatory licensesand
fees). The taxes, however, do not include taxes on investment
income and capital gains.
In any event, some rules do not apply until 2014 and later. This
is due to changes to the marketplace in
2014 related to the offering of individual and small group plans
through the exchanges, and to adjustmentsrequired by statute to the
MLR formula to account for payments or receipts for risk
adjustment, riskcorridors (which pertain to the potential for
changes in risk), and reinsurance. In the absence of waivers,many
insurers paid rebates in 2012 for below-floor medical loss ratios
they realized in 2011.
Competition from CO-OPs?
The ACA created the Consumer Operated and Oriented Plan (CO-OP),
a new kind of nonprofit health insurerrun by its customers. CO-OPs
are designed to offer affordable and consumer-friendly health
insurance optionsto individuals and small businesses, who may come
together to create a CO-OP and apply for a federal loan.The federal
government has committed to offer loans to non-profit organizations
to help establish CO-OPs.
-
8/11/2019 Healthcare - Managed Care 2013.12
14/64
12 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
They are still required, however, to meet the same state and
federal quality and financial standards as otherhealth insurance
plans and, like insurers, offer a variety of health plans. The aim
of the CO-OP is to increasecompetition, leading to a reduction of
premiums, and improving healthcare quality and customer
service.Consumer-governed health insurers have a 40-year history,
but they cover only two million Americans and,therefore, experts
are skeptical about CO-OPs.
Nevertheless, CO-OPs have generated much interest. The
government had set an October 17, 2012, deadlinefor nonprofit
groups to apply for the first round of $3.8 billion in funding to
start CO-OPs. Eventually, 24CO-OPs that had signed loan agreements
with HHS as of December 2012 received funding under the plan.This
accounted for just $2 billion, and the remaining part of the
funding was eliminated by the legislationpassed by the US Congress
on January 1, 2013, as a part of the fiscal cliff deal.
HEALTHCARE REFORM LEGISLATION ORIGINAL IMPLEMENTATION
TIMELINE*MANAGED CARE ITEMS
2 1
Bans lifetime limits on health insurance policies and permits
only annual coverage limits, as determined by the Secretary of
Health and Human Services(HHS); bans rescissions (revocation of a
policy due to illness).
Eliminates pre-existing condition clauses for children up to age
19.
Establishes a tax credit for small business with up to 25
employees and annual wages of below $50K to help subsidize
employees insurance costs.
Requires insurers to adopt specified internal claims and appeals
procedures.
Creates a temporary high-risk health insurance pool program to
provide coverage for uninsured individuals with pre-existing
conditions.
Provides a one-time rebate of $250 to Medicare Part D
participants to begin process of reducing the so-called donut hole
gap in coverage. Between 2010
and 2011, gradually reduces coverage gap for both branded and
generic drugs.
2 11
Tax on pharmaceutical industry begins: a fee of $2.5B in 2011
increases to $4.1B by 2018, then declines to $2.8B in 2019 and
thereafter.
Establishes minimum medical loss ratio (85% of premium revenue
for large groups and 80% for small groups) by requiring payment of
a rebate to eachenrollee below that amount.
Payments to Medicare Advantage (MA) plans set to different
percentages of Medicare fee-for-service (FFS) rates (ranging from
95% to 115%). Cost sharingfor Medicare-covered preventative
services eliminated.
Five-year demonstration grants awarded to states to develop,
implement, and evaluate alternatives to current tort
litigation.
Develop national strategy for quality improvement, with
healthcare services delivery, patient outcomes, and population
health given priority.
2 12
Insurers required to use uniform explanation of benefits (EOB)
forms developed by the US Secretary of Health and Human
Services.
Bonus payments to high-quality MA plans begin; rebates for MA
plans reduced.
Fee-for-service and managed care payments for Medicaid increased
to at least 100% of Medicare Part B FFS rates for primary care
services fromphysicians in family medicine, general internal
medicine, and internal medicine specialties.
2 13
Establishes of Consumer Operated and Oriented Plan (CO-OP)
program to foster creation of nonprofit, member-run health
insurance companies to be
offered through exchanges to spur industry competition.
Medical device excise tax (equal to 2.3% of providers device
revenues) begins; excludes devices sold to the general public
(e.g., eyeglasses, contactlenses, hearing aids, etc.).
2 14
Increased Medicaid and SCHIP eligibility will extend health
insurance coverage to some 10 million individuals (rising to
approximately 16 million in 2017).
Penalties implemented for hospitals that do not meet ARRA
requirements for use of electronic health records under
Medicare.
Imposes fee on health insurance providers, starting at $8B for
2014, rising to $14.3B in 2018 and thereafter.
The establishment of health insurance exchanges will extend
health insurance coverage to some 8 million individuals (rising to
some 23 million in 2017).
Requires states to establish American Health Benefit Exchanges,
to facilitate the purchase of insurance. Insurers will compete for
the business ofindividuals and predominantly small employers that
have not been able to obtain coverage at the same favorable rates
as large employers. In addition,states may form regional exchanges.
Each plan participating in an exchange must meet standardized
affordability, basic benefit, and consumer protectionrequirements,
as well as state requirements. Initially, only individuals and
small employers (up to 100 employees) will be eligible to
participate. Multistateplans may be offered in the exchanges
beginning in 2016. States may permit businesses with more than 100
employees to purchase coverage in theexchanges starting in
2017.
Establishes a so-called individual mandate: all US citizens and
legal residents will be required to obtain qualifying health
coverage. When fully phasedin, it imposes a tax penalty of $695 (or
2.5% of income) for individuals who do not purchase coverage or do
not meet the hardship exemption.
Establishes an employer mandate under which employers must
provide insurance, pay penalties, or, in certain situations, do
both.
Extends prohibition on rescissions to all individuals in group
health plans; limits ability of insurance companies to discriminate
in terms of premium ratingsbased on family rating, age, or tobacco
use, and implements guaranteed issue requirement.
Establishes an independent Payment Advisory Board to submit
legislative proposals with recommendations to reduce the rate of
growth in Medicarespending if it exceeds a target rate.
MA rebate system based on plan quality phased in; MA plans
required to have medical loss ratios no lower than 85%.
Annual fee on health insurance plans begins.
After 2 14
Effective January 1, 2018, the Cadillac tax beginsan excise tax
levied on health insurers of employer-sponsored health plans whose
aggregate valueexceeds a certain threshold. For 2018, the threshold
is $10,200 for individual plans and $27,500 for family plans; the
tax is to be indexed to inflation.
*Any changes or temporary adjustments to this original timeline
are discussed in the text of this Survey.
Sources: Standard & Poors; Congressional Budget Office;
Ropes & Gray; Foley Hoag; US Chamber of Commerce.
-
8/11/2019 Healthcare - Managed Care 2013.12
15/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 13
Each state has seen different combinations of people and
organizations coming together to form a CO-OP. Forinstance, in
Montana, the states former insurance commissioner has joined some
prominent physicians andleaders in labor and business to found a
CO-OP. In contrast, in New York, the Freelancers Union, a
nonprofitorganization for independent workers, has formed a CO-OP
and plans to bring in some of its 150,000members, among others.
Some positive aspects to reform for MCOs
Under the healthcare reform law, the CBO in May 2013 estimated
that there will be 25 million fewer peopleuninsured by 2016, a
number that will remain unchanged through 2023. MCOs have started
benefitingfrom some positive effects of the healthcare reform. One
example has been the rise in enrollment amongyoung adults between
18 and 25 years of age (who may be covered by their parents
policies) amid declinesin other age groups within the under-65
cohort. Looking ahead, S&P believes the increasing
enrollmentexpected to start in 2014 through expanded Medicaid
eligibility will not only help increase MCOspremium revenue, but
also help them leverage SG&A costs. Note, though, that the size
of the premium ratehikes that the MCOs may be able to charge will
likely be limited by several factors: competition from
theexchanges, an actuarial-based formula designed to achieve the
requisite MLRs, and state and federalmonitoring of premium
increases. In addition, higher enrollment may provide MCOs more
clout in pricenegotiations with hospitals and doctors.
Further, according to a study published in September 2011 in
Health Affairs, a monthly health-policyjournal published under the
aegis of Project HOPE, a nonprofit international health education
organization,the number of uninsured and underinsured adults in the
19-to-64 age group increased from 61 million(36% of that age group)
in 2003 to 81 million (44%) in 2010. In this context, underinsured
refers to thoseadults who report at least one of the following
three indicators: family out-of pocket medical care expensesare
equal to or more than 10% of income; medical expenses are at least
5% of income; or the per-persondeductible is equal to or more than
5% of income. Rising health costs and recessionary pressures
haveaccounted for the increase in the underinsured population.
According to the study, the ACAs reforms, ifsuccessful, could
result in a 70% drop in the number of uninsured people and a huge
decline in the numberof underinsured people. Also, based on the
latest census figures (see The Pressing Need for HealthcareReform
below), the number of uninsured declined in 2011, which was the
first full year the ACA was ineffect. Meantime, millions of
Americans are expected to have their existing individual health
policiesterminated by the MCOs at the end of 2013 because the plans
do not comply with all of the ACArequirements, which state that the
new policies have to cover all 10 essential health benefits.
S&P expectsthis group to be among the first to utilize the
exchanges.
S&P believes the MCOs that are better able to manage under
healthcare reform may well benefit byacquiring the less successful
ones, thus improving economies of scale and negotiating clout.
THE PRESSING NEED FOR HEALTHCARE REFORM
The problems facing the US healthcare system, while not new,
have been intensifying, partly due to an agingpopulation, but
recently exacerbated by the overall weak economic environment. US
spending on healthcarerose at more than twice the rate of general
inflation from 2004 to 2009, according to the Centers forMedicare
& Medicaid Services (CMS), a division of the US Department of
Health & Human Services(HHS). In 2011, healthcare spending is
estimated to have grown 3.9%, to around $2.7 trillion, while
overallinflation, as measured by the consumer price index, rose
1.2%.
Based on CMSs latest projections (published in September 2012),
healthcare spending was estimated to havegrown by 3.9% in 2012
(over the estimated spending in 2011) to around $2.8 trillion and
is projected to growby slightly under 3.9% in 2013. According to
the CMS, these projections assume that the scheduledMedicare
physician payment rate updates under the Sustainable Growth Rate
formula do not occur,including a 24.7% cut scheduled for January 1,
2014. S&P is not surprised, since the US Congress hascontinued
to override this physician payment reduction provision. Instead, it
employs an alternativescenario, one in which physician fee schedule
rates are assumed to grow 0.7% annually from 2014, amethod and rate
consistent with the 2013 Medicare Trustees Report.
-
8/11/2019 Healthcare - Managed Care 2013.12
16/64
14 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
The US healthcare budget is expanding and growing more
burdensome. In 2012, the federal government isestimated to have
paid around 26% of healthcare expenses in the US, a proportion that
would graduallygrow to 31% by 2022, according to CMS estimates
based on current law as of September 2013.
Despite continued efforts to improve the level of coverage in
the US via the expansion of Medicare, theChildrens Program (CHIP),
and other private and government programs, the number of those
lackingaccess to health insurance coverage has remained stubbornly
high as a percentage of population since 2002.While the latest
available data from the US Census Bureau indicates that the number
of uninsured peopledeclined to 48.0 million in 2012, or 15.4% of
the US population (from 48.6 million in 2011, or 15.7%), itremains
one of the highest percentages in the industrialized world.
The Census Bureau also noted that the percentage of people
covered by private health insurance hasessentially leveled off; it
was 63.9% in both 2011 and 2012. However, this figure is below
2009s 64.5%and 2008s 67.2%. Meanwhile the percentage covered by
government health insurance programs, includingMedicare and
Medicaid, increased to 32.6% in 2012, from 32.2% in 2011, 31.2% in
2010, 30.6% in
2009, and 29.1% in 2008.
S&P believes that the number andpercentage of uninsured
increasedthrough 2010, given the loss of jobs
amid the weak economy, while thedecline in 2011 was attributed
mainly tothe ACA rule that children may becovered by their parents
healthinsurance policies until the age of 26.Although the
unemployment rate hasdeclined from its peak of 10.1% inOctober 2009
to 7.3% in August 2013,S&P believes that many of the new
jobopenings, particularly in small firms, stilldo not provide
insurance coverage.However, by 2015, according to theACA, they will
be required to enroll the
new hires in a health plan. (The targetdate was 2014 for large
firms, but thiswas delayed by one year.) Indeed, the
KFF noted that 57% of small firms (those with three to 199
workers) offered health benefits in 2013, downfrom 61% in 2012. In
contrast, 99% of employers with 200 or more workers offered health
benefits in2013, up from 98% in 2012.
State budget deficits appear to be abating
According to the June 2012 report by The Center on Budget and
Policy Priorities (CBPP), which conductsresearch on public policy,
budget shortfalls in the fiscal year (FY) 2012 collectively totaled
$107 billion. ForFY 2013, the report said that 31 states are
projecting budget shortfalls totaling $55 billion. (Forty-six
stateshave fiscal years ending on June 30. Unlike the federal
government, all states but Vermont are legally requiredto balance
their budgets.) Without the necessary revenues, states will have
difficulty providing services such as
healthcare and education. Nonetheless, according to a September
2013 report by the CBPP (an update from areport first released in
June), in the 31 states for which data were available in June 2013,
state income taxcollections in the first ten months of FY 13 were,
on average, 5.7% higher than in the year-earlier period.
According to the CBPP, state revenue systems still face major
challenges. States are still recovering from theimpact of the
recession as their revenues likely still remain 3% below
pre-recession (200709) levels, afteradjusting for inflation. It
also noted that states without income taxes are missing out on the
opportunity forincreased revenues, noting that part of the recent
boost reflects the fact that income taxes are better growingwith
the economy than sales or other taxes. In earlier reports, the CBPP
noted that the states obsolete tax
Chart H01: THEUNINSUREDPOPULATION INTHE US
12
13
14
15
16
17
30
35
40
45
50
55
2002 03 04 05 06 07 08 09 10 11 2012
THE UNINSURED POPULATION IN THE US
Number of uninsured (millions, left scale)
Percent of total population (right scale)
Source: US Census Bureau.
-
8/11/2019 Healthcare - Managed Care 2013.12
17/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 15
systems are unable to keep track of the e-commerce sales and
service sector, and that the federal government iscutting federal
spending, which accounts for around 25% of the states revenues. It
also warned that manystate policymakers, such as governors and
leading legislators, have been planning large tax cuts, which
wouldfurther deteriorate state revenues.
In FY 2012, states were compelled to increase their Medicaid
spending by an average of 28.7%, primarily tosubstitute temporary
Medicaid federal stimulus funds that expired in June 2011. The vast
majority of theseshortfalls in FY 2013 have been closed through
spending cuts.
To help find cost savings, states have been re-engineering
healthcare payment and delivery systems byupgrading their health
information technology (IT) systems and developing integrated
healthcare models.States have been increasingly relying on MCOs
over the years to care for their Medicaid beneficiaries.Indeed, in
FY 2010, 13 states expanded their use of managed care. By FY 2013,
35 states reported theywere expanding managed care, including 10
states that indicated plans to implement managed long-termcare,
according to the KFF in a report dated October 2012.
According to a study published October 2013 by the Brookings
Institution, a private nonprofit organizationdevoted to independent
research and innovative policy solutions, by mid-2013, at least
nine states hadapproved utilization of Accountable Care
Organizations (ACOs) for providing care to their
Medicaidbeneficiaries. An ACO is an organization run by the
healthcare service provider, in which the participating
providers are collectively responsible for the care of an
enrolled population. They also share in any savingsassociated with
improvements in the quality and efficiency of care by aligning
Medicare with Medicaid.Nonetheless, S&P believes the MCOs would
be directly affected by state rate cuts.
Approximately 11 million more individuals will get health
insurance through Medicaid under the ACA,according to the CBO.
Given this, we believe state budget pressures would worsen
dramatically, if not forthe ACA calling for the federal government
to cover 100% of the costs related to newly eligible individualsfor
the years 201416. While the new number of individual getting
insurance under the ACA is expected todecline due to the Supreme
Court decision, the number varies for different years. For 2022,
four millionfewer people are expected to be insured under Medicaid.
However, states would be on the hook forpotential Medicaid budget
shortfalls that could occur as the federal support gradually
declines to 90% foryears 2020 and later.
Uninsured struggle with healthcare access, costs
According to a KFF report published in October 2012, uninsured
patients are experiencing significantdifficulties in accessing and
affording health care. About 26% of uninsured adults surveyed say
they haveforgone care in the past year because of its cost,
compared with 4% of adults with private coverage. Thereport also
noted that people without Medicaid or some other insurance were
less likely to visit a doctor, andmore likely to have unmet needs
for prescription drugs, eye care, or mental healthcare. Further,
these peopleare less likely to receive timely preventive care, such
as check-ups and screenings.
According to an article published online by Health Affairsin
October 2012, the proportion of people under 65years of age, with a
high medical cost burden (defined as spending greater than 10% of
family income onhealthcare) grew to 19.2% in 2006 from 14.4% in
2001. However, this figure did not change much during the200709
recession and stood at 18.8% in 2009, despite decreasing income and
rising unemployment. Thedrop in average annual family income to
$61,000 in 2009 (from $65,000 in 2006) was offset by lower
out-of-
pocket health spending, which declined to $1,231 in 2009 (from
$1,454 in 2006) due to the shift fromprescription drugs to cheaper
generics.
To show that insurance garnered under the ACA will be
affordable, the HHS released a report in September2013, stating
that about 10.7 million of the estimated 21.9 million uninsured
Americans eligible to buyinsurance through the healthcare exchanges
may be able to pay $100 or less per person per month, aftertaking
into account their available premium tax credits. In a report
published in October, the HHS claimedthat based on data from the
federally-facilitated and state partnership exchanges, 1.3 million
(46%) of the 2.9million uninsured single, young adults (ages 18-34)
eligible for the health insurance exchanges could getcoverage for
$50 per month or less after tax credits. Finally, a study published
November 2013 by the
-
8/11/2019 Healthcare - Managed Care 2013.12
18/64
16 HEALTHCARE: MANAGED CARE/ NOVEMBER 2013 INDUSTRY SURVEYS
McKinsey Center for U.S. Health System Reform, a unit of
management consulting firm McKinsey & Co.,found
zero-net-premium products widely available on the exchanges. The
study estimated that seven to eightmillion people (85% of which
were currently uninsured) might be eligible for such plans, though
many maystill face co-payments for services delivered.
MEDICARE MANAGED CARE UNDER INCREASING PRESSURE
Medicare Advantage (MA), which uses private payers to manage the
care and cost of Medicare participants,is not new, but the program
became more popular because of provisions in the Medicare
Prescription Drug,Improvement, and Modernization Act of 2003 (MMA)
that significantly raised MMA plans reimbursementrates and expanded
their availability and flexibility. The program aimed to attract
more Medicare recipientsand private payers to Medicare managed
care. While most Medicare recipients (approximately 49.4
million,according to the KFF) are still enrolled in traditional
fee-for-service plans, a growing number participate inMedicare
private health plans: around 15.0 million (including 14.4 million
in MA) as of September 2013,according to the CMSroughly 28% of all
beneficiaries, according to our estimates. MA has providedMCOs an
opportunity for additional profits and revenue growth.
The MMA is best known for creating the Medicare Part D program,
the first government-sponsoredprescription drug benefit for
seniors. Part D members who do not participate in MA plans (most of
whichinclude Part D benefits) numbered 20.1 million as of December
2012. For MCOs, one of the attractions of
participating in Medicare Part D has been the opportunity to
transfer some Part D enrollees to the broaderand higher-margin MA
contracts.
Nonetheless, the Medicare Advantageprogram has become
increasinglycontroversial, mainly becausegovernment payouts per
Medicarebeneficiary are higher in MA than intraditional Medicare
fee-for-service.In its March 2011, March 2012, andMarch 2013
reports to Congress,MedPAC estimated the MA paymentper person to be
110%, 107%, and
104%, respectively, of traditionalMedicare fee-for-service
payments.
According to an article publishedDecember 2012 in Health
Affairs,
utilization rates for a majority of services in Medicare
Advantage HMO plans were lower during the periodfrom 2003 through
2009 than in traditional Medicare. For instance, compared with
traditional Medicare,emergency department visits were 25%35% lower;
inpatient medical days were 20%25% lower; andambulatory surgery or
procedures, which were 25% lower in 2003, narrowed to a 7%
difference in 2008.Proponents of managed care say that integrated
managed care plans deliver services more rationally bytailoring
their provider networks to the needs of users, imposing
pre-approval requirements, and reviewingutilization rates, because
they have financial incentives to reduce the use of services.
According to a report released by the KFF in December 2012,
beneficiaries will have around 20 MedicareAdvantage plans to choose
from in 2013 (about the same number as in 2012), well below the
high of 48 in2009. Further, the report states that most of the
enrollees in Medicare Advantage plans in 2012 will be ableto stay
in the same plans, with higher premiums in 2013. An article dated
March 28, 2012, in the NewEngland Journal of Medicinestates that
over the last four decades, Medicare spending per enrollee hasgrown
by a rate 2.6% higher than the rate of growth of per capita GDP. If
the trend goes on, by 2060, allfederal revenues will be spent on
Medicare. However, according to the article, there have been signs
ofslowing growth in Medicaid expenditures, with Medicare spending
per enrollee falling in line with thegrowth in per capita GDP.
Further, in November 2011, the actual Part B premium for 2012 was
fixed at$99.90, as against the actuary-projected premium of
$106.60. In addition, in February 2013, the CBO
Chart H03: MedicarePrivate PlanEnrollment
5.3 5.56.1
7.6
9.0
10.411.3
11.912.6
13.9
15.0
0
2
4
6
8
10
12
14
16
2003 04 05 06 07 08 09 10 11 12 *2013
MEDICARE PRIVATE HEALTH PLAN ENROLLMENT
(Millions of enrollees)
*As of September.Source: Centers for Medicare & Medicaid
Services.
-
8/11/2019 Healthcare - Managed Care 2013.12
19/64
INDUSTRY SURVEYS HEALTHCARE: MANAGED CARE / NOVEMBER 2013 17
brought its Medicare spending projection down by $143 billion
for the 10-year period from 2014 to 2023(partly offset by
reductions of $48 billion in collections of offsetting receipts and
$10 billion in Medicaresavings as a result of sequestration) from
its August 2012 projection, which implies slower growth inMedicare
spending.
Insurers say that their plans provide more benefits and save
money for recipients vis--vistraditionalMedicare. Nevertheless,
national MA reimbursement rates, which edged up in 2009, grew more
slowly in2010, despite the deferral of the drop in the physician
payment rate required by a legal formula. (Congressonce again
postponed the latest rate cut until December 2013, and we think it
will be above the 27.4% cutexpected in 2012 unless it is delayed
again or a permanent fix is found. As we noted earlier, the
CMSassumed that this cut would be postponed again when it set its
final MA reimbursement rate for 2014.)Looking ahead, while MA
payment rates will transition over a three-year period to 2014 to a
benchmarkthat varies from 95% to 115% of fee-for-service payment
levels, depending on the geography, the MCOswould also be eligible
for bonus payments, based on quality rankings.
Consequently, MCOs that have banked heavily on Medicare growth,
such as Humana Inc., WellCareHealth Plans Inc., and Universal
American Inc., have said they might curtail benefits to maintain
margins orat least temper the pressure on margins. Indeed, Avalere
Health, a healthcare advisory, published in March2012 an analysis
of the Medicare private plan payment data released by the CMS, and
noted that MedicareAdvantage plan enrollees received on average
over $70 in additional benefits and reduced cost-sharing in
2010 at no charge to them.
A phased payment rate cut may notkeep MA packages as attractive
asthey were in 201012, but S&Pbelieves that they will still
offermore benefits than the traditionalfee-for-service program in
order toretain members. As long as they do,MCOs are likely to see
MAenrollment expand, aided by thecoming influx of the
baby-boomergeneration, many of whom work for
companies that provide managedcare health insurance
coverageunder the aegis of the MCOs.Companies may also
findopportunities for consolidation and,
hence, improving economies of scale, as smaller, weaker players
(including not-for-profit MA plans) findthemselves unable to
operate profitably under the ACA rules. We think the probability of
an eventualshakeout in the industry is high. Starting in 2014, MA
plans will be faced with reduced reimbursement ratesthat are
designed to bring MA payments in line with traditional Medicare
payments and a mandated MLRfloor of 85%. Separately, the standalone
Medicare Part D programs, now mature, will also continue togrow,
but remain only modest earnings-per-share (EPS) contributors due to
their very slim margins.
DUAL ELIGIBLES
According to MedPAC, in 2011, there were about 10 million dual
eligibles: low-income seniors andyounger persons with disabilities
who are enrolled in both Medicare and Medicaid programs. They are
themost costly group of beneficiaries for both Medicaid and
Medicare, accounting for a disproportionateamount of spending. In
the Medicare program, dual eligibles account for about 19% of the
population, but31% of spending; in the Medicaid program, they
account for 15% of enrollees, but 40% of spending. GiantMCO
UnitedHealth Group estimated that for 2013, combined Medicare and
Medicaid spending on dualeligibles will reach $330 billion, with
Medicare covering $180 billion (including costs for
prescription
Table B04: MCOmembershipenrollment
MANAGED CARE ORGANIZATION MEMBERSHIP ENROLLM ENT
(Ranked by Medicare Advantage enrollees, as of June 2013)
TOTAL MEDICAL % CHANGE MEDICARE ADVANTAGE
ENROLLMENT FROM DEC. ENROLLMENT (THOUS.)
COMPANY (THOUS.) 2012 DEC. 2012 JUN. 2013
UnitedHealth Group 45,000 10.0 2,565 2,920
Humana 12,371 2.3 2,326 2,446
WellPoint* 35,666 (1.3) 1,545 1,467
Aetna Inc. 21,968 20.4 448 948
CIGNA 14,286 1.7 426 458
WellCare Health Plans 2,842 57.9 213 272
Health Net 5,352 (1.5) 234 236Universal American 134 0.0 134
134
Molina Healthcare 1,847 2.8 36 36
*Senior membership; Medicare Advantage membership not reported
separately.
Source: Company reports.