Embed Size (px)
Citation preview
Health Insurance Moral Hazard andManaged Care
Ching-to Albert MaBoston UniversityBoston MA 02215
mabueduand
Hong Kong University of Science and TechnologyClear Water Bay Kowloon Hong Kong
Michael H RiordanGraduate School of Business Columbia University
New York NY 10027mhr21columbiaedu
If an illness is not contractible then even partially insured consumers demandtreatment for it when the benet is less than the cost a condition knownas moral hazard Traditional health insurance which controls moral hazardwith copayments (demand management) can result in either a decient oran excessive provision of treatment relative to ideal insurance In particu-lar treatment for a low-probability illness is decient if illness per se haslittle effect on the consumerrsquos marginal utility of income and if the con-sumerrsquos price elasticity of expected demand for treatment is large relativeto the risk-spreading distortion when these are evaluated at a copaymentthat brings forth the ideal provision of treatment Managed care which con-trols moral hazard with physician incentives can either increase or decreasetreatment delivery relative to traditional insurance depending on whetherdemand management results in decient or excessive treatment
1 Introduction
Before the proliferation of managed care health insurance contractsrelied heavily on deductibles copayments and other coverage limita-tions to control the provision of care These demand management instru-ments cause consumers to limit their demand for health care and
The authors acknowledge helpful comments from the editor two referees DavidBradford David Dranove Thomas McGuire and seminar participants at ColumbiaHarvard and Yale Universities the Federal Reserve Bank of New York MassachusettsInstitute of Technology Universitat Pompeu Fabra (Barcelona) Universitat Autonomade Barcelona and the Universities of New Hampshire North Carolina and Toulouse
copy 2002 Massachusetts Institute of TechnologyJournal of Economics amp Management Strategy Volume 11 Number 1 Spring 2002 81ndash107
82 Journal of Economics amp Management Strategy
thereby reduce premiums by restraining health care costs but mayexpose consumers to large uninsured risks In contrast managed careplans give health care providers explicit nancial incentives such asprospective payments capitations and cost-sharing contracts to limitexpensive treatments Clearly these supply management instrumentshave become more important
Economic theory interprets the emergence of institutions as aresponse to market failures In the health industry market failurestems from the difculty of contracting on illness ex ante1 Due tothis failure ideal insurance which shields consumers from the costsof efciently provided treatment is infeasible Second-best insurancepays only part of treatment expenses or limits coverage in other waysBut patients who do not fully face the cost of medical care maydemand treatment inefciently in the sense that the cost of treatmentsometimes exceeds the benet This problem is known as moral haz-ard Demand and supply management policies in health care attemptto control moral hazard while partly insuring consumers against therisks of illness2
In the 1960s the health economics literature adopted the termmoral hazard to describe the difculty of contracting over health sta-tus (Arrow 1963 1968 Pauly 1968 Zeckhauser 1970) and arguedthat demand management at best only partly cures the moral hazardproblem The very rst lines of Zeckhauserrsquos 1970 article crystallizewhat is now the conventional wisdom
The primary purpose of medical insurance is to spreada risk the risk of incurring substantial medical expensesWithrisk-spreading individualswillnotpaythe full amountsof such expenses Insurance provision will thus introduce aperverse incentive toward overexpenditure if as is usuallythe case (1) the insured has substantial inuence over theamount that is spent on their own behalf in any particularmedical circumstance and (2) the level of reimbursementby the insurance plan is a positively associated function ofthe expenses incurred by its insured
Given that demand management does not solve the moral haz-ard problem it is plausible to interpret supply management (man-
1 See Grossman and Hart (1986) on the difculties of contracting on complex events2 The health economics literature has recognized that demand and supply man-
agement policies are complementary responses to market failure in the health industryEllis and McGuire (1993) emphasize the potential importance of nancial incentivesfor consumers as well as for providers Ma and McGuire (1997) use this basic premiseto investigate the interaction between optimal insurance and provider payment New-house (1996) in a recent survey urges more study of supply-side incentives
Health Insurance Moral Hazard and Managed Care 83
aged care) as an additional attempt to do so On this interpretationZeckhauserrsquos statementof the conventionalwisdom suggests that moralhazard under demand management alone results in excessive pro-vision of treatment and that managed care reduces this excess Wedemonstrate that this is not necessarily so Under some conditionsoptimal demand management results in decient treatment and man-aged care corrects this deciency leading to more treatment
We construct a model of insurance for a particular treatment andcharacterize conditions under which optimal demand managementunder moral hazard results in an excessive or decient provision oftreatment By excessive (decient) we mean that a higher (lower) frac-tion of individuals receive the treatment compared to the ideal bench-mark in the absence of moral hazard We extend the model to allowsupply management (managed care) and prove that this relaxes themoral hazard constraint and under certain conditions achieves idealinsurance In this case the introduction of managed care increases(decreases) the provision of treatment if treatment under optimal dem-and management is decient (excessive) thus alleviating the marketfailure due to moral hazard
The provision of treatment can be decient under optimal dem-and management if the illness per se has little effect on the consumerrsquosmarginal utility of income This possibility depends on the income effectof the copayment the patientrsquos marginal utility of income is higher ifthe copayment is higher3 The intuition is roughly as follows Thereare two important conicting effects on consumer welfare of limit-ing treatment by charging a copayment higher than the one that elic-its the ideal (rst-best) provision First the consumer directly suffersmore income risk as indicated by a higher marginal utility of incomeafter paying for treatment Ceteris paribus the cost to the consumer ofthis departure from optimal risk spreading is greater the greater isthe income effect of the copayment Second the consumer enjoys alower premium because the insurance company has a lower expectedcost This second effect is more pronounced the greater is the incomeeffect of the copayment relative to the marginal utility of income whenan ill consumer declines treatment because the consumerrsquos demandresponse to the increased copayment is greater and translates into a
3 The health economics literature has paid little attention to the importance ofincome effects on the demand for treatment In fact a standard text in health eco-nomics only briey mentions income effects (Phelps 1992 pp 32 301) There are somenotable exceptions de Meza (1983) considers intertemporal income effects of savingsand insurance but assumes that illness severity is contractible so that optimal insur-ance involves an indemnity payment when the consumer is sick Marshall (1976) alsoallows income effects focusing on how the optimal insurance gives the consumer anincentive to exercise care to reduce the likelihood of illness
84 Journal of Economics amp Management Strategy
larger premium reduction Thus the premium-reduction effect is mag-nied if illness per se does not very much increase the marginal utilityof income The optimal provision of treatment under demand man-agement is less than the ideal amount if the price elasticity of demandfor treatment (and hence the premium reductioneffect) is large relativeto the risk-spreading distortion While our main results are developedfor the case of an infrequent illness for which these clearly are themost important effects we also show that the possibility of decienttreatment does not depend crucially on a small illness probability
The rest of the article is organized as follows The next sectionlays out a model of illness treatment and insurance Section 3 stud-ies the rst best when the treatment decision is fully contractible andSection 4 characterizes the second best when the provision of treat-ment is controlled indirectly by demand management Section 5 com-pares the two and establishes conditions under which the second-bestprovision of treatment with optimal demand management is more orless than the rst best with ideal insurance Section 6 employs theseresults as benchmarks to study supply management (managed care)Section 7 concludes by summarizing and describing possible futureresearch An appendix contains the formal proofs of propositions
2 The Basic Model
We focus on optimal health insurance for a particular discrete treat-ment4 Implicitly we hold xed other health and disability insur-ance covering the consumer and study insurance for this particulartreatment in isolation To be concrete and to focus our discussion weinterpret the treatment as being suitable for a specic diagnosis5 Forexample the treatment might be a new class of prescription drugsfor high cholesterol (statins) described in a recent Wall Street Journalarticle6
4 This contrasts with a more familiar reduced-form approach in the health careliterature which assumes that a consumerrsquos health is a function of undifferentiatedhealth care expenditures See for example Baumgardner (1991) Our discrete-choiceapproach perhaps provides a more useful conceptual basis for empirical analyses ofmicro data that indicate whether a patient received a particular treatment or not Seefor example Manning and Phelps (1979) Of course it will be important in futuretheoretical work to study the bundled coverage of the panoply of treatments typical ofhealth insurance policies
5 More generally the treatment in question might be suitable for a variety of diag-noses For example the treatment might be an extra day in the hospital due to compli-cations from a surgical procedure Our model is consistent with this broader interpre-tation
6 See ldquoPrice Prescription Powerful Medications for Cholesterol Pose a Paradox forHMOrsquosrdquo by Ron Winslow Wall Street Journal December 6 1996 p A1
Health Insurance Moral Hazard and Managed Care 85
We assume that a consumer becomes ill with probability 0 ltcedil lt 1 For example cedil is the probability that a consumer is diagnosedas having a high cholesterol condition and is potentially a candidatefor statins Many of our results focus on the case where cedil is smallwhich of course is often realistic For example according to the afore-mentioned Wall Street Journal article 13 million people with seriousheart problems are candidates for statins While this is a lot of peo-ple the probability that one of us will become a candidate for statinsin the next year is hopefully quite small It is easy to think of manyother expensive treatments and tests that may be benecial to an indi-vidual consumer with a small probability (organ transplants neuralsurgeries etc) Our model focuses on health insurance coverage forone of these treatments in isolation
For simplicity we assume that the cost of diagnosing the illnessis zero7 Illness varies by its severity which is described by a randomvariable ` with a cumulative distribution function F(`) and a densityfunction f (`) with support on the positive real line8 As we makeclear below the severity of illness ` indexes the benets of treatmentand F(`) describes the distribution of benets across the population ofpatients The consumer learns the benets of treatment (presumably inconsultation with a physician) only after becoming ill We assume thatillness is not contractible9 and the insurance company can contractneither on the event of illness nor on the realization of `
We adopt an eclectic approach to modeling the consequencesof an untreated illness Specically consumersrsquo preferences are repre-sented by a utility function of the form U(y a`) b` The variabley represents the consumerrsquos expenditure on other goods The func-tion U ( ) is differentiable increasing and strictly concave reectingthe consumerrsquos risk aversion to income uctuations and a and b arenonnegative parameters Nested in this functional form are two spe-cial cases of interest If b 0 and a gt 0 then illness is completelyequivalent to a loss of monetary income we call this the monetaryloss model In this case we sometimes set a 1 as a normalizationmeasuring the loss of health resulting from illness in monetary unitsThe second special case is the utility loss model with a 0 and b gt 0
7 A xed and known diagnostic cost will not change our qualitative results as longas the outcome of the diagnosis is not contractible
8 The random probability of illness effectively puts a mass point at ` 0 It iseasy to extend the model to allow for bounded severity and also for a strictly positivelower bound of the support to be strictly positive as for a Pareto distribution (Ma andRiordan 2000)
9 If the event of illness were contractible the optimal insurance contract couldinvolve a monetary transfer payment to patients who become ill The case is perhapsbetter understood as disability insurance
86 Journal of Economics amp Management Strategy
Here illness affects an additive utility loss and does not directly affectthe consumerrsquos marginal utility of income we sometimes also use thenormalization b 1 interpreting ` as an expected utility loss fromforgoing treatment This broad interpretation implicitly recognizes theuncertainties surrounding illness and alternative treatments The gen-eral formulation allows for mixtures of monetary losses and (additive)utility losses from illness
The utility loss model seems more plausible than the monetaryloss model though both are special cases The monetary loss modelimplies that the demand for treatment does not depend on incomeThis seems unrealistic for many discretionary treatments Manningand Phelps (1979) found signicant income effects for specic den-tal treatments The RAND Health Insurance Study generally foundsmall but positive income elasticities and subsequent studies usingdifferent methods and data found larger elasticities (Phelps 1992) Incontrast the utility loss model implies a positive income elasticity ofthe demand for treatment without restricting its magnitude The util-ity loss model does imply that a consumerrsquos attitude toward incomerisk is independent of illness per se Obviously this is an empiricalquestion but seems extremely difcult to answer We have no a priorireason to think that the effect of illness on risk aversion goes one wayor another Therefore it seems reasonable at least as a rst step toignore this effect For these reasons we are partial to the utility lossmodel
We make several simplifying assumptions about treatment Firstthe cost of treatment is xed at C gt 0 It will be useful to think of C asa large number creating a signicant demand for insurance but notprohibitively large10 For example the Wall Street Journal article saysthat statin therapy costs $700 a year for life While this is an expen-sive therapy some consumersrsquo benets obviously are much higherthan $700 a year Second if the patient receives treatment then thelosses from illness are eliminated completely11 Thus ` indexes thebenets from receiving treatment These benets vary across patientsimplying that some patients are better candidates for treatment than
10 Obviously this treatment cost cannot be too large Otherwise there would be lit-tle demand for insurance in our model If C is sufciently small then there is a demandfor insurance to smooth the income uctuation resulting from illness and treatmentInterestingly in the monetary loss model the uctuation to be smoothed is the mone-tary equivalent of illness itself In the utility loss model the uctuation to be smoothedis the cost of treatment
11 As mentioned above we do not need to assume this in the utility loss model Inthis special case ` is the benet of possibly imperfect treatment
Health Insurance Moral Hazard and Managed Care 87
others12 Third we model the treatment decision as a binary choiceEither the patient receives treatment or not13 Consequently for a xedcopayment there is a critical value of ` such that more severely illpatients demand treatment while less severely ill patients do not aswe show later Finally the delivery of treatment is contractible mean-ing that the insurance company can prevent fraudulent claims for thereimbursement of nonexistent treatment costs
3 Ideal insurance
We begin by studying the ideal insurance contract in the absence ofmoral hazard In this regime illness and loss are assumed to be com-pletely contractible payments and treatment decisions can be contin-gent on the severity of illness Under an ideal contract the consumerpays a xed premium P and receives treatment whenever the benetof treatment ` is above a xed threshold L Moreover when treat-ment is withheld the consumer can be compensated by an indemnitypayment t(`) that depends on the severity of the illness In principlethe consumer receiving treatment can also receive a transfer paymentThis possibility however plays no role in our model because treat-ment eliminates all illness losses Therefore under an ideal contracta consumer with income Y enjoys an expected utility given by theformula
(1 )U (Y P)
cedil HL
0[U (Y P a` t(`)) b`]f (`)d` [1 F(L)]U(Y P) (1)
This expected-utility formula is a weighted sum of two componentsThe rst component is the utility of a healthy consumer who has paidthe insurance premium14 The second component (in curly braces) isthe conditional expected utility of an ill consumer who receives treat-ment when the benet is sufciently great but otherwise is compen-sated only by the indemnity payment The weights are the respectiveprobabilities of illness and health
12 We emphasize that our interpretation of ` is the treatmentrsquos potential benet topatients One could interpret alternatively that ` refers to patientsrsquo losses although wedo not think that this is always true For some illnesses it may be more natural to allowfor multiple treatments when severity varies See Chernew et al (2000)
13 A more general mechanism design approach to optimal insurance would allowthe insurance company to randomize the provision of treatment We ignore this possi-bility because it is unrealistic
14 The variable Y can be interpreted as income net of premiums paid for otherhealth insurance Thus Y P is net income after the premium insuring for this particulartreatment
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
82 Journal of Economics amp Management Strategy
thereby reduce premiums by restraining health care costs but mayexpose consumers to large uninsured risks In contrast managed careplans give health care providers explicit nancial incentives such asprospective payments capitations and cost-sharing contracts to limitexpensive treatments Clearly these supply management instrumentshave become more important
Economic theory interprets the emergence of institutions as aresponse to market failures In the health industry market failurestems from the difculty of contracting on illness ex ante1 Due tothis failure ideal insurance which shields consumers from the costsof efciently provided treatment is infeasible Second-best insurancepays only part of treatment expenses or limits coverage in other waysBut patients who do not fully face the cost of medical care maydemand treatment inefciently in the sense that the cost of treatmentsometimes exceeds the benet This problem is known as moral haz-ard Demand and supply management policies in health care attemptto control moral hazard while partly insuring consumers against therisks of illness2
In the 1960s the health economics literature adopted the termmoral hazard to describe the difculty of contracting over health sta-tus (Arrow 1963 1968 Pauly 1968 Zeckhauser 1970) and arguedthat demand management at best only partly cures the moral hazardproblem The very rst lines of Zeckhauserrsquos 1970 article crystallizewhat is now the conventional wisdom
The primary purpose of medical insurance is to spreada risk the risk of incurring substantial medical expensesWithrisk-spreading individualswillnotpaythe full amountsof such expenses Insurance provision will thus introduce aperverse incentive toward overexpenditure if as is usuallythe case (1) the insured has substantial inuence over theamount that is spent on their own behalf in any particularmedical circumstance and (2) the level of reimbursementby the insurance plan is a positively associated function ofthe expenses incurred by its insured
Given that demand management does not solve the moral haz-ard problem it is plausible to interpret supply management (man-
1 See Grossman and Hart (1986) on the difculties of contracting on complex events2 The health economics literature has recognized that demand and supply man-
agement policies are complementary responses to market failure in the health industryEllis and McGuire (1993) emphasize the potential importance of nancial incentivesfor consumers as well as for providers Ma and McGuire (1997) use this basic premiseto investigate the interaction between optimal insurance and provider payment New-house (1996) in a recent survey urges more study of supply-side incentives
Health Insurance Moral Hazard and Managed Care 83
aged care) as an additional attempt to do so On this interpretationZeckhauserrsquos statementof the conventionalwisdom suggests that moralhazard under demand management alone results in excessive pro-vision of treatment and that managed care reduces this excess Wedemonstrate that this is not necessarily so Under some conditionsoptimal demand management results in decient treatment and man-aged care corrects this deciency leading to more treatment
We construct a model of insurance for a particular treatment andcharacterize conditions under which optimal demand managementunder moral hazard results in an excessive or decient provision oftreatment By excessive (decient) we mean that a higher (lower) frac-tion of individuals receive the treatment compared to the ideal bench-mark in the absence of moral hazard We extend the model to allowsupply management (managed care) and prove that this relaxes themoral hazard constraint and under certain conditions achieves idealinsurance In this case the introduction of managed care increases(decreases) the provision of treatment if treatment under optimal dem-and management is decient (excessive) thus alleviating the marketfailure due to moral hazard
The provision of treatment can be decient under optimal dem-and management if the illness per se has little effect on the consumerrsquosmarginal utility of income This possibility depends on the income effectof the copayment the patientrsquos marginal utility of income is higher ifthe copayment is higher3 The intuition is roughly as follows Thereare two important conicting effects on consumer welfare of limit-ing treatment by charging a copayment higher than the one that elic-its the ideal (rst-best) provision First the consumer directly suffersmore income risk as indicated by a higher marginal utility of incomeafter paying for treatment Ceteris paribus the cost to the consumer ofthis departure from optimal risk spreading is greater the greater isthe income effect of the copayment Second the consumer enjoys alower premium because the insurance company has a lower expectedcost This second effect is more pronounced the greater is the incomeeffect of the copayment relative to the marginal utility of income whenan ill consumer declines treatment because the consumerrsquos demandresponse to the increased copayment is greater and translates into a
3 The health economics literature has paid little attention to the importance ofincome effects on the demand for treatment In fact a standard text in health eco-nomics only briey mentions income effects (Phelps 1992 pp 32 301) There are somenotable exceptions de Meza (1983) considers intertemporal income effects of savingsand insurance but assumes that illness severity is contractible so that optimal insur-ance involves an indemnity payment when the consumer is sick Marshall (1976) alsoallows income effects focusing on how the optimal insurance gives the consumer anincentive to exercise care to reduce the likelihood of illness
84 Journal of Economics amp Management Strategy
larger premium reduction Thus the premium-reduction effect is mag-nied if illness per se does not very much increase the marginal utilityof income The optimal provision of treatment under demand man-agement is less than the ideal amount if the price elasticity of demandfor treatment (and hence the premium reductioneffect) is large relativeto the risk-spreading distortion While our main results are developedfor the case of an infrequent illness for which these clearly are themost important effects we also show that the possibility of decienttreatment does not depend crucially on a small illness probability
The rest of the article is organized as follows The next sectionlays out a model of illness treatment and insurance Section 3 stud-ies the rst best when the treatment decision is fully contractible andSection 4 characterizes the second best when the provision of treat-ment is controlled indirectly by demand management Section 5 com-pares the two and establishes conditions under which the second-bestprovision of treatment with optimal demand management is more orless than the rst best with ideal insurance Section 6 employs theseresults as benchmarks to study supply management (managed care)Section 7 concludes by summarizing and describing possible futureresearch An appendix contains the formal proofs of propositions
2 The Basic Model
We focus on optimal health insurance for a particular discrete treat-ment4 Implicitly we hold xed other health and disability insur-ance covering the consumer and study insurance for this particulartreatment in isolation To be concrete and to focus our discussion weinterpret the treatment as being suitable for a specic diagnosis5 Forexample the treatment might be a new class of prescription drugsfor high cholesterol (statins) described in a recent Wall Street Journalarticle6
4 This contrasts with a more familiar reduced-form approach in the health careliterature which assumes that a consumerrsquos health is a function of undifferentiatedhealth care expenditures See for example Baumgardner (1991) Our discrete-choiceapproach perhaps provides a more useful conceptual basis for empirical analyses ofmicro data that indicate whether a patient received a particular treatment or not Seefor example Manning and Phelps (1979) Of course it will be important in futuretheoretical work to study the bundled coverage of the panoply of treatments typical ofhealth insurance policies
5 More generally the treatment in question might be suitable for a variety of diag-noses For example the treatment might be an extra day in the hospital due to compli-cations from a surgical procedure Our model is consistent with this broader interpre-tation
6 See ldquoPrice Prescription Powerful Medications for Cholesterol Pose a Paradox forHMOrsquosrdquo by Ron Winslow Wall Street Journal December 6 1996 p A1
Health Insurance Moral Hazard and Managed Care 85
We assume that a consumer becomes ill with probability 0 ltcedil lt 1 For example cedil is the probability that a consumer is diagnosedas having a high cholesterol condition and is potentially a candidatefor statins Many of our results focus on the case where cedil is smallwhich of course is often realistic For example according to the afore-mentioned Wall Street Journal article 13 million people with seriousheart problems are candidates for statins While this is a lot of peo-ple the probability that one of us will become a candidate for statinsin the next year is hopefully quite small It is easy to think of manyother expensive treatments and tests that may be benecial to an indi-vidual consumer with a small probability (organ transplants neuralsurgeries etc) Our model focuses on health insurance coverage forone of these treatments in isolation
For simplicity we assume that the cost of diagnosing the illnessis zero7 Illness varies by its severity which is described by a randomvariable ` with a cumulative distribution function F(`) and a densityfunction f (`) with support on the positive real line8 As we makeclear below the severity of illness ` indexes the benets of treatmentand F(`) describes the distribution of benets across the population ofpatients The consumer learns the benets of treatment (presumably inconsultation with a physician) only after becoming ill We assume thatillness is not contractible9 and the insurance company can contractneither on the event of illness nor on the realization of `
We adopt an eclectic approach to modeling the consequencesof an untreated illness Specically consumersrsquo preferences are repre-sented by a utility function of the form U(y a`) b` The variabley represents the consumerrsquos expenditure on other goods The func-tion U ( ) is differentiable increasing and strictly concave reectingthe consumerrsquos risk aversion to income uctuations and a and b arenonnegative parameters Nested in this functional form are two spe-cial cases of interest If b 0 and a gt 0 then illness is completelyequivalent to a loss of monetary income we call this the monetaryloss model In this case we sometimes set a 1 as a normalizationmeasuring the loss of health resulting from illness in monetary unitsThe second special case is the utility loss model with a 0 and b gt 0
7 A xed and known diagnostic cost will not change our qualitative results as longas the outcome of the diagnosis is not contractible
8 The random probability of illness effectively puts a mass point at ` 0 It iseasy to extend the model to allow for bounded severity and also for a strictly positivelower bound of the support to be strictly positive as for a Pareto distribution (Ma andRiordan 2000)
9 If the event of illness were contractible the optimal insurance contract couldinvolve a monetary transfer payment to patients who become ill The case is perhapsbetter understood as disability insurance
86 Journal of Economics amp Management Strategy
Here illness affects an additive utility loss and does not directly affectthe consumerrsquos marginal utility of income we sometimes also use thenormalization b 1 interpreting ` as an expected utility loss fromforgoing treatment This broad interpretation implicitly recognizes theuncertainties surrounding illness and alternative treatments The gen-eral formulation allows for mixtures of monetary losses and (additive)utility losses from illness
The utility loss model seems more plausible than the monetaryloss model though both are special cases The monetary loss modelimplies that the demand for treatment does not depend on incomeThis seems unrealistic for many discretionary treatments Manningand Phelps (1979) found signicant income effects for specic den-tal treatments The RAND Health Insurance Study generally foundsmall but positive income elasticities and subsequent studies usingdifferent methods and data found larger elasticities (Phelps 1992) Incontrast the utility loss model implies a positive income elasticity ofthe demand for treatment without restricting its magnitude The util-ity loss model does imply that a consumerrsquos attitude toward incomerisk is independent of illness per se Obviously this is an empiricalquestion but seems extremely difcult to answer We have no a priorireason to think that the effect of illness on risk aversion goes one wayor another Therefore it seems reasonable at least as a rst step toignore this effect For these reasons we are partial to the utility lossmodel
We make several simplifying assumptions about treatment Firstthe cost of treatment is xed at C gt 0 It will be useful to think of C asa large number creating a signicant demand for insurance but notprohibitively large10 For example the Wall Street Journal article saysthat statin therapy costs $700 a year for life While this is an expen-sive therapy some consumersrsquo benets obviously are much higherthan $700 a year Second if the patient receives treatment then thelosses from illness are eliminated completely11 Thus ` indexes thebenets from receiving treatment These benets vary across patientsimplying that some patients are better candidates for treatment than
10 Obviously this treatment cost cannot be too large Otherwise there would be lit-tle demand for insurance in our model If C is sufciently small then there is a demandfor insurance to smooth the income uctuation resulting from illness and treatmentInterestingly in the monetary loss model the uctuation to be smoothed is the mone-tary equivalent of illness itself In the utility loss model the uctuation to be smoothedis the cost of treatment
11 As mentioned above we do not need to assume this in the utility loss model Inthis special case ` is the benet of possibly imperfect treatment
Health Insurance Moral Hazard and Managed Care 87
others12 Third we model the treatment decision as a binary choiceEither the patient receives treatment or not13 Consequently for a xedcopayment there is a critical value of ` such that more severely illpatients demand treatment while less severely ill patients do not aswe show later Finally the delivery of treatment is contractible mean-ing that the insurance company can prevent fraudulent claims for thereimbursement of nonexistent treatment costs
3 Ideal insurance
We begin by studying the ideal insurance contract in the absence ofmoral hazard In this regime illness and loss are assumed to be com-pletely contractible payments and treatment decisions can be contin-gent on the severity of illness Under an ideal contract the consumerpays a xed premium P and receives treatment whenever the benetof treatment ` is above a xed threshold L Moreover when treat-ment is withheld the consumer can be compensated by an indemnitypayment t(`) that depends on the severity of the illness In principlethe consumer receiving treatment can also receive a transfer paymentThis possibility however plays no role in our model because treat-ment eliminates all illness losses Therefore under an ideal contracta consumer with income Y enjoys an expected utility given by theformula
(1 )U (Y P)
cedil HL
0[U (Y P a` t(`)) b`]f (`)d` [1 F(L)]U(Y P) (1)
This expected-utility formula is a weighted sum of two componentsThe rst component is the utility of a healthy consumer who has paidthe insurance premium14 The second component (in curly braces) isthe conditional expected utility of an ill consumer who receives treat-ment when the benet is sufciently great but otherwise is compen-sated only by the indemnity payment The weights are the respectiveprobabilities of illness and health
12 We emphasize that our interpretation of ` is the treatmentrsquos potential benet topatients One could interpret alternatively that ` refers to patientsrsquo losses although wedo not think that this is always true For some illnesses it may be more natural to allowfor multiple treatments when severity varies See Chernew et al (2000)
13 A more general mechanism design approach to optimal insurance would allowthe insurance company to randomize the provision of treatment We ignore this possi-bility because it is unrealistic
14 The variable Y can be interpreted as income net of premiums paid for otherhealth insurance Thus Y P is net income after the premium insuring for this particulartreatment
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 83
aged care) as an additional attempt to do so On this interpretationZeckhauserrsquos statementof the conventionalwisdom suggests that moralhazard under demand management alone results in excessive pro-vision of treatment and that managed care reduces this excess Wedemonstrate that this is not necessarily so Under some conditionsoptimal demand management results in decient treatment and man-aged care corrects this deciency leading to more treatment
We construct a model of insurance for a particular treatment andcharacterize conditions under which optimal demand managementunder moral hazard results in an excessive or decient provision oftreatment By excessive (decient) we mean that a higher (lower) frac-tion of individuals receive the treatment compared to the ideal bench-mark in the absence of moral hazard We extend the model to allowsupply management (managed care) and prove that this relaxes themoral hazard constraint and under certain conditions achieves idealinsurance In this case the introduction of managed care increases(decreases) the provision of treatment if treatment under optimal dem-and management is decient (excessive) thus alleviating the marketfailure due to moral hazard
The provision of treatment can be decient under optimal dem-and management if the illness per se has little effect on the consumerrsquosmarginal utility of income This possibility depends on the income effectof the copayment the patientrsquos marginal utility of income is higher ifthe copayment is higher3 The intuition is roughly as follows Thereare two important conicting effects on consumer welfare of limit-ing treatment by charging a copayment higher than the one that elic-its the ideal (rst-best) provision First the consumer directly suffersmore income risk as indicated by a higher marginal utility of incomeafter paying for treatment Ceteris paribus the cost to the consumer ofthis departure from optimal risk spreading is greater the greater isthe income effect of the copayment Second the consumer enjoys alower premium because the insurance company has a lower expectedcost This second effect is more pronounced the greater is the incomeeffect of the copayment relative to the marginal utility of income whenan ill consumer declines treatment because the consumerrsquos demandresponse to the increased copayment is greater and translates into a
3 The health economics literature has paid little attention to the importance ofincome effects on the demand for treatment In fact a standard text in health eco-nomics only briey mentions income effects (Phelps 1992 pp 32 301) There are somenotable exceptions de Meza (1983) considers intertemporal income effects of savingsand insurance but assumes that illness severity is contractible so that optimal insur-ance involves an indemnity payment when the consumer is sick Marshall (1976) alsoallows income effects focusing on how the optimal insurance gives the consumer anincentive to exercise care to reduce the likelihood of illness
84 Journal of Economics amp Management Strategy
larger premium reduction Thus the premium-reduction effect is mag-nied if illness per se does not very much increase the marginal utilityof income The optimal provision of treatment under demand man-agement is less than the ideal amount if the price elasticity of demandfor treatment (and hence the premium reductioneffect) is large relativeto the risk-spreading distortion While our main results are developedfor the case of an infrequent illness for which these clearly are themost important effects we also show that the possibility of decienttreatment does not depend crucially on a small illness probability
The rest of the article is organized as follows The next sectionlays out a model of illness treatment and insurance Section 3 stud-ies the rst best when the treatment decision is fully contractible andSection 4 characterizes the second best when the provision of treat-ment is controlled indirectly by demand management Section 5 com-pares the two and establishes conditions under which the second-bestprovision of treatment with optimal demand management is more orless than the rst best with ideal insurance Section 6 employs theseresults as benchmarks to study supply management (managed care)Section 7 concludes by summarizing and describing possible futureresearch An appendix contains the formal proofs of propositions
2 The Basic Model
We focus on optimal health insurance for a particular discrete treat-ment4 Implicitly we hold xed other health and disability insur-ance covering the consumer and study insurance for this particulartreatment in isolation To be concrete and to focus our discussion weinterpret the treatment as being suitable for a specic diagnosis5 Forexample the treatment might be a new class of prescription drugsfor high cholesterol (statins) described in a recent Wall Street Journalarticle6
4 This contrasts with a more familiar reduced-form approach in the health careliterature which assumes that a consumerrsquos health is a function of undifferentiatedhealth care expenditures See for example Baumgardner (1991) Our discrete-choiceapproach perhaps provides a more useful conceptual basis for empirical analyses ofmicro data that indicate whether a patient received a particular treatment or not Seefor example Manning and Phelps (1979) Of course it will be important in futuretheoretical work to study the bundled coverage of the panoply of treatments typical ofhealth insurance policies
5 More generally the treatment in question might be suitable for a variety of diag-noses For example the treatment might be an extra day in the hospital due to compli-cations from a surgical procedure Our model is consistent with this broader interpre-tation
6 See ldquoPrice Prescription Powerful Medications for Cholesterol Pose a Paradox forHMOrsquosrdquo by Ron Winslow Wall Street Journal December 6 1996 p A1
Health Insurance Moral Hazard and Managed Care 85
We assume that a consumer becomes ill with probability 0 ltcedil lt 1 For example cedil is the probability that a consumer is diagnosedas having a high cholesterol condition and is potentially a candidatefor statins Many of our results focus on the case where cedil is smallwhich of course is often realistic For example according to the afore-mentioned Wall Street Journal article 13 million people with seriousheart problems are candidates for statins While this is a lot of peo-ple the probability that one of us will become a candidate for statinsin the next year is hopefully quite small It is easy to think of manyother expensive treatments and tests that may be benecial to an indi-vidual consumer with a small probability (organ transplants neuralsurgeries etc) Our model focuses on health insurance coverage forone of these treatments in isolation
For simplicity we assume that the cost of diagnosing the illnessis zero7 Illness varies by its severity which is described by a randomvariable ` with a cumulative distribution function F(`) and a densityfunction f (`) with support on the positive real line8 As we makeclear below the severity of illness ` indexes the benets of treatmentand F(`) describes the distribution of benets across the population ofpatients The consumer learns the benets of treatment (presumably inconsultation with a physician) only after becoming ill We assume thatillness is not contractible9 and the insurance company can contractneither on the event of illness nor on the realization of `
We adopt an eclectic approach to modeling the consequencesof an untreated illness Specically consumersrsquo preferences are repre-sented by a utility function of the form U(y a`) b` The variabley represents the consumerrsquos expenditure on other goods The func-tion U ( ) is differentiable increasing and strictly concave reectingthe consumerrsquos risk aversion to income uctuations and a and b arenonnegative parameters Nested in this functional form are two spe-cial cases of interest If b 0 and a gt 0 then illness is completelyequivalent to a loss of monetary income we call this the monetaryloss model In this case we sometimes set a 1 as a normalizationmeasuring the loss of health resulting from illness in monetary unitsThe second special case is the utility loss model with a 0 and b gt 0
7 A xed and known diagnostic cost will not change our qualitative results as longas the outcome of the diagnosis is not contractible
8 The random probability of illness effectively puts a mass point at ` 0 It iseasy to extend the model to allow for bounded severity and also for a strictly positivelower bound of the support to be strictly positive as for a Pareto distribution (Ma andRiordan 2000)
9 If the event of illness were contractible the optimal insurance contract couldinvolve a monetary transfer payment to patients who become ill The case is perhapsbetter understood as disability insurance
86 Journal of Economics amp Management Strategy
Here illness affects an additive utility loss and does not directly affectthe consumerrsquos marginal utility of income we sometimes also use thenormalization b 1 interpreting ` as an expected utility loss fromforgoing treatment This broad interpretation implicitly recognizes theuncertainties surrounding illness and alternative treatments The gen-eral formulation allows for mixtures of monetary losses and (additive)utility losses from illness
The utility loss model seems more plausible than the monetaryloss model though both are special cases The monetary loss modelimplies that the demand for treatment does not depend on incomeThis seems unrealistic for many discretionary treatments Manningand Phelps (1979) found signicant income effects for specic den-tal treatments The RAND Health Insurance Study generally foundsmall but positive income elasticities and subsequent studies usingdifferent methods and data found larger elasticities (Phelps 1992) Incontrast the utility loss model implies a positive income elasticity ofthe demand for treatment without restricting its magnitude The util-ity loss model does imply that a consumerrsquos attitude toward incomerisk is independent of illness per se Obviously this is an empiricalquestion but seems extremely difcult to answer We have no a priorireason to think that the effect of illness on risk aversion goes one wayor another Therefore it seems reasonable at least as a rst step toignore this effect For these reasons we are partial to the utility lossmodel
We make several simplifying assumptions about treatment Firstthe cost of treatment is xed at C gt 0 It will be useful to think of C asa large number creating a signicant demand for insurance but notprohibitively large10 For example the Wall Street Journal article saysthat statin therapy costs $700 a year for life While this is an expen-sive therapy some consumersrsquo benets obviously are much higherthan $700 a year Second if the patient receives treatment then thelosses from illness are eliminated completely11 Thus ` indexes thebenets from receiving treatment These benets vary across patientsimplying that some patients are better candidates for treatment than
10 Obviously this treatment cost cannot be too large Otherwise there would be lit-tle demand for insurance in our model If C is sufciently small then there is a demandfor insurance to smooth the income uctuation resulting from illness and treatmentInterestingly in the monetary loss model the uctuation to be smoothed is the mone-tary equivalent of illness itself In the utility loss model the uctuation to be smoothedis the cost of treatment
11 As mentioned above we do not need to assume this in the utility loss model Inthis special case ` is the benet of possibly imperfect treatment
Health Insurance Moral Hazard and Managed Care 87
others12 Third we model the treatment decision as a binary choiceEither the patient receives treatment or not13 Consequently for a xedcopayment there is a critical value of ` such that more severely illpatients demand treatment while less severely ill patients do not aswe show later Finally the delivery of treatment is contractible mean-ing that the insurance company can prevent fraudulent claims for thereimbursement of nonexistent treatment costs
3 Ideal insurance
We begin by studying the ideal insurance contract in the absence ofmoral hazard In this regime illness and loss are assumed to be com-pletely contractible payments and treatment decisions can be contin-gent on the severity of illness Under an ideal contract the consumerpays a xed premium P and receives treatment whenever the benetof treatment ` is above a xed threshold L Moreover when treat-ment is withheld the consumer can be compensated by an indemnitypayment t(`) that depends on the severity of the illness In principlethe consumer receiving treatment can also receive a transfer paymentThis possibility however plays no role in our model because treat-ment eliminates all illness losses Therefore under an ideal contracta consumer with income Y enjoys an expected utility given by theformula
(1 )U (Y P)
cedil HL
0[U (Y P a` t(`)) b`]f (`)d` [1 F(L)]U(Y P) (1)
This expected-utility formula is a weighted sum of two componentsThe rst component is the utility of a healthy consumer who has paidthe insurance premium14 The second component (in curly braces) isthe conditional expected utility of an ill consumer who receives treat-ment when the benet is sufciently great but otherwise is compen-sated only by the indemnity payment The weights are the respectiveprobabilities of illness and health
12 We emphasize that our interpretation of ` is the treatmentrsquos potential benet topatients One could interpret alternatively that ` refers to patientsrsquo losses although wedo not think that this is always true For some illnesses it may be more natural to allowfor multiple treatments when severity varies See Chernew et al (2000)
13 A more general mechanism design approach to optimal insurance would allowthe insurance company to randomize the provision of treatment We ignore this possi-bility because it is unrealistic
14 The variable Y can be interpreted as income net of premiums paid for otherhealth insurance Thus Y P is net income after the premium insuring for this particulartreatment
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
84 Journal of Economics amp Management Strategy
larger premium reduction Thus the premium-reduction effect is mag-nied if illness per se does not very much increase the marginal utilityof income The optimal provision of treatment under demand man-agement is less than the ideal amount if the price elasticity of demandfor treatment (and hence the premium reductioneffect) is large relativeto the risk-spreading distortion While our main results are developedfor the case of an infrequent illness for which these clearly are themost important effects we also show that the possibility of decienttreatment does not depend crucially on a small illness probability
The rest of the article is organized as follows The next sectionlays out a model of illness treatment and insurance Section 3 stud-ies the rst best when the treatment decision is fully contractible andSection 4 characterizes the second best when the provision of treat-ment is controlled indirectly by demand management Section 5 com-pares the two and establishes conditions under which the second-bestprovision of treatment with optimal demand management is more orless than the rst best with ideal insurance Section 6 employs theseresults as benchmarks to study supply management (managed care)Section 7 concludes by summarizing and describing possible futureresearch An appendix contains the formal proofs of propositions
2 The Basic Model
We focus on optimal health insurance for a particular discrete treat-ment4 Implicitly we hold xed other health and disability insur-ance covering the consumer and study insurance for this particulartreatment in isolation To be concrete and to focus our discussion weinterpret the treatment as being suitable for a specic diagnosis5 Forexample the treatment might be a new class of prescription drugsfor high cholesterol (statins) described in a recent Wall Street Journalarticle6
4 This contrasts with a more familiar reduced-form approach in the health careliterature which assumes that a consumerrsquos health is a function of undifferentiatedhealth care expenditures See for example Baumgardner (1991) Our discrete-choiceapproach perhaps provides a more useful conceptual basis for empirical analyses ofmicro data that indicate whether a patient received a particular treatment or not Seefor example Manning and Phelps (1979) Of course it will be important in futuretheoretical work to study the bundled coverage of the panoply of treatments typical ofhealth insurance policies
5 More generally the treatment in question might be suitable for a variety of diag-noses For example the treatment might be an extra day in the hospital due to compli-cations from a surgical procedure Our model is consistent with this broader interpre-tation
6 See ldquoPrice Prescription Powerful Medications for Cholesterol Pose a Paradox forHMOrsquosrdquo by Ron Winslow Wall Street Journal December 6 1996 p A1
Health Insurance Moral Hazard and Managed Care 85
We assume that a consumer becomes ill with probability 0 ltcedil lt 1 For example cedil is the probability that a consumer is diagnosedas having a high cholesterol condition and is potentially a candidatefor statins Many of our results focus on the case where cedil is smallwhich of course is often realistic For example according to the afore-mentioned Wall Street Journal article 13 million people with seriousheart problems are candidates for statins While this is a lot of peo-ple the probability that one of us will become a candidate for statinsin the next year is hopefully quite small It is easy to think of manyother expensive treatments and tests that may be benecial to an indi-vidual consumer with a small probability (organ transplants neuralsurgeries etc) Our model focuses on health insurance coverage forone of these treatments in isolation
For simplicity we assume that the cost of diagnosing the illnessis zero7 Illness varies by its severity which is described by a randomvariable ` with a cumulative distribution function F(`) and a densityfunction f (`) with support on the positive real line8 As we makeclear below the severity of illness ` indexes the benets of treatmentand F(`) describes the distribution of benets across the population ofpatients The consumer learns the benets of treatment (presumably inconsultation with a physician) only after becoming ill We assume thatillness is not contractible9 and the insurance company can contractneither on the event of illness nor on the realization of `
We adopt an eclectic approach to modeling the consequencesof an untreated illness Specically consumersrsquo preferences are repre-sented by a utility function of the form U(y a`) b` The variabley represents the consumerrsquos expenditure on other goods The func-tion U ( ) is differentiable increasing and strictly concave reectingthe consumerrsquos risk aversion to income uctuations and a and b arenonnegative parameters Nested in this functional form are two spe-cial cases of interest If b 0 and a gt 0 then illness is completelyequivalent to a loss of monetary income we call this the monetaryloss model In this case we sometimes set a 1 as a normalizationmeasuring the loss of health resulting from illness in monetary unitsThe second special case is the utility loss model with a 0 and b gt 0
7 A xed and known diagnostic cost will not change our qualitative results as longas the outcome of the diagnosis is not contractible
8 The random probability of illness effectively puts a mass point at ` 0 It iseasy to extend the model to allow for bounded severity and also for a strictly positivelower bound of the support to be strictly positive as for a Pareto distribution (Ma andRiordan 2000)
9 If the event of illness were contractible the optimal insurance contract couldinvolve a monetary transfer payment to patients who become ill The case is perhapsbetter understood as disability insurance
86 Journal of Economics amp Management Strategy
Here illness affects an additive utility loss and does not directly affectthe consumerrsquos marginal utility of income we sometimes also use thenormalization b 1 interpreting ` as an expected utility loss fromforgoing treatment This broad interpretation implicitly recognizes theuncertainties surrounding illness and alternative treatments The gen-eral formulation allows for mixtures of monetary losses and (additive)utility losses from illness
The utility loss model seems more plausible than the monetaryloss model though both are special cases The monetary loss modelimplies that the demand for treatment does not depend on incomeThis seems unrealistic for many discretionary treatments Manningand Phelps (1979) found signicant income effects for specic den-tal treatments The RAND Health Insurance Study generally foundsmall but positive income elasticities and subsequent studies usingdifferent methods and data found larger elasticities (Phelps 1992) Incontrast the utility loss model implies a positive income elasticity ofthe demand for treatment without restricting its magnitude The util-ity loss model does imply that a consumerrsquos attitude toward incomerisk is independent of illness per se Obviously this is an empiricalquestion but seems extremely difcult to answer We have no a priorireason to think that the effect of illness on risk aversion goes one wayor another Therefore it seems reasonable at least as a rst step toignore this effect For these reasons we are partial to the utility lossmodel
We make several simplifying assumptions about treatment Firstthe cost of treatment is xed at C gt 0 It will be useful to think of C asa large number creating a signicant demand for insurance but notprohibitively large10 For example the Wall Street Journal article saysthat statin therapy costs $700 a year for life While this is an expen-sive therapy some consumersrsquo benets obviously are much higherthan $700 a year Second if the patient receives treatment then thelosses from illness are eliminated completely11 Thus ` indexes thebenets from receiving treatment These benets vary across patientsimplying that some patients are better candidates for treatment than
10 Obviously this treatment cost cannot be too large Otherwise there would be lit-tle demand for insurance in our model If C is sufciently small then there is a demandfor insurance to smooth the income uctuation resulting from illness and treatmentInterestingly in the monetary loss model the uctuation to be smoothed is the mone-tary equivalent of illness itself In the utility loss model the uctuation to be smoothedis the cost of treatment
11 As mentioned above we do not need to assume this in the utility loss model Inthis special case ` is the benet of possibly imperfect treatment
Health Insurance Moral Hazard and Managed Care 87
others12 Third we model the treatment decision as a binary choiceEither the patient receives treatment or not13 Consequently for a xedcopayment there is a critical value of ` such that more severely illpatients demand treatment while less severely ill patients do not aswe show later Finally the delivery of treatment is contractible mean-ing that the insurance company can prevent fraudulent claims for thereimbursement of nonexistent treatment costs
3 Ideal insurance
We begin by studying the ideal insurance contract in the absence ofmoral hazard In this regime illness and loss are assumed to be com-pletely contractible payments and treatment decisions can be contin-gent on the severity of illness Under an ideal contract the consumerpays a xed premium P and receives treatment whenever the benetof treatment ` is above a xed threshold L Moreover when treat-ment is withheld the consumer can be compensated by an indemnitypayment t(`) that depends on the severity of the illness In principlethe consumer receiving treatment can also receive a transfer paymentThis possibility however plays no role in our model because treat-ment eliminates all illness losses Therefore under an ideal contracta consumer with income Y enjoys an expected utility given by theformula
(1 )U (Y P)
cedil HL
0[U (Y P a` t(`)) b`]f (`)d` [1 F(L)]U(Y P) (1)
This expected-utility formula is a weighted sum of two componentsThe rst component is the utility of a healthy consumer who has paidthe insurance premium14 The second component (in curly braces) isthe conditional expected utility of an ill consumer who receives treat-ment when the benet is sufciently great but otherwise is compen-sated only by the indemnity payment The weights are the respectiveprobabilities of illness and health
12 We emphasize that our interpretation of ` is the treatmentrsquos potential benet topatients One could interpret alternatively that ` refers to patientsrsquo losses although wedo not think that this is always true For some illnesses it may be more natural to allowfor multiple treatments when severity varies See Chernew et al (2000)
13 A more general mechanism design approach to optimal insurance would allowthe insurance company to randomize the provision of treatment We ignore this possi-bility because it is unrealistic
14 The variable Y can be interpreted as income net of premiums paid for otherhealth insurance Thus Y P is net income after the premium insuring for this particulartreatment
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 85
We assume that a consumer becomes ill with probability 0 ltcedil lt 1 For example cedil is the probability that a consumer is diagnosedas having a high cholesterol condition and is potentially a candidatefor statins Many of our results focus on the case where cedil is smallwhich of course is often realistic For example according to the afore-mentioned Wall Street Journal article 13 million people with seriousheart problems are candidates for statins While this is a lot of peo-ple the probability that one of us will become a candidate for statinsin the next year is hopefully quite small It is easy to think of manyother expensive treatments and tests that may be benecial to an indi-vidual consumer with a small probability (organ transplants neuralsurgeries etc) Our model focuses on health insurance coverage forone of these treatments in isolation
For simplicity we assume that the cost of diagnosing the illnessis zero7 Illness varies by its severity which is described by a randomvariable ` with a cumulative distribution function F(`) and a densityfunction f (`) with support on the positive real line8 As we makeclear below the severity of illness ` indexes the benets of treatmentand F(`) describes the distribution of benets across the population ofpatients The consumer learns the benets of treatment (presumably inconsultation with a physician) only after becoming ill We assume thatillness is not contractible9 and the insurance company can contractneither on the event of illness nor on the realization of `
We adopt an eclectic approach to modeling the consequencesof an untreated illness Specically consumersrsquo preferences are repre-sented by a utility function of the form U(y a`) b` The variabley represents the consumerrsquos expenditure on other goods The func-tion U ( ) is differentiable increasing and strictly concave reectingthe consumerrsquos risk aversion to income uctuations and a and b arenonnegative parameters Nested in this functional form are two spe-cial cases of interest If b 0 and a gt 0 then illness is completelyequivalent to a loss of monetary income we call this the monetaryloss model In this case we sometimes set a 1 as a normalizationmeasuring the loss of health resulting from illness in monetary unitsThe second special case is the utility loss model with a 0 and b gt 0
7 A xed and known diagnostic cost will not change our qualitative results as longas the outcome of the diagnosis is not contractible
8 The random probability of illness effectively puts a mass point at ` 0 It iseasy to extend the model to allow for bounded severity and also for a strictly positivelower bound of the support to be strictly positive as for a Pareto distribution (Ma andRiordan 2000)
9 If the event of illness were contractible the optimal insurance contract couldinvolve a monetary transfer payment to patients who become ill The case is perhapsbetter understood as disability insurance
86 Journal of Economics amp Management Strategy
Here illness affects an additive utility loss and does not directly affectthe consumerrsquos marginal utility of income we sometimes also use thenormalization b 1 interpreting ` as an expected utility loss fromforgoing treatment This broad interpretation implicitly recognizes theuncertainties surrounding illness and alternative treatments The gen-eral formulation allows for mixtures of monetary losses and (additive)utility losses from illness
The utility loss model seems more plausible than the monetaryloss model though both are special cases The monetary loss modelimplies that the demand for treatment does not depend on incomeThis seems unrealistic for many discretionary treatments Manningand Phelps (1979) found signicant income effects for specic den-tal treatments The RAND Health Insurance Study generally foundsmall but positive income elasticities and subsequent studies usingdifferent methods and data found larger elasticities (Phelps 1992) Incontrast the utility loss model implies a positive income elasticity ofthe demand for treatment without restricting its magnitude The util-ity loss model does imply that a consumerrsquos attitude toward incomerisk is independent of illness per se Obviously this is an empiricalquestion but seems extremely difcult to answer We have no a priorireason to think that the effect of illness on risk aversion goes one wayor another Therefore it seems reasonable at least as a rst step toignore this effect For these reasons we are partial to the utility lossmodel
We make several simplifying assumptions about treatment Firstthe cost of treatment is xed at C gt 0 It will be useful to think of C asa large number creating a signicant demand for insurance but notprohibitively large10 For example the Wall Street Journal article saysthat statin therapy costs $700 a year for life While this is an expen-sive therapy some consumersrsquo benets obviously are much higherthan $700 a year Second if the patient receives treatment then thelosses from illness are eliminated completely11 Thus ` indexes thebenets from receiving treatment These benets vary across patientsimplying that some patients are better candidates for treatment than
10 Obviously this treatment cost cannot be too large Otherwise there would be lit-tle demand for insurance in our model If C is sufciently small then there is a demandfor insurance to smooth the income uctuation resulting from illness and treatmentInterestingly in the monetary loss model the uctuation to be smoothed is the mone-tary equivalent of illness itself In the utility loss model the uctuation to be smoothedis the cost of treatment
11 As mentioned above we do not need to assume this in the utility loss model Inthis special case ` is the benet of possibly imperfect treatment
Health Insurance Moral Hazard and Managed Care 87
others12 Third we model the treatment decision as a binary choiceEither the patient receives treatment or not13 Consequently for a xedcopayment there is a critical value of ` such that more severely illpatients demand treatment while less severely ill patients do not aswe show later Finally the delivery of treatment is contractible mean-ing that the insurance company can prevent fraudulent claims for thereimbursement of nonexistent treatment costs
3 Ideal insurance
We begin by studying the ideal insurance contract in the absence ofmoral hazard In this regime illness and loss are assumed to be com-pletely contractible payments and treatment decisions can be contin-gent on the severity of illness Under an ideal contract the consumerpays a xed premium P and receives treatment whenever the benetof treatment ` is above a xed threshold L Moreover when treat-ment is withheld the consumer can be compensated by an indemnitypayment t(`) that depends on the severity of the illness In principlethe consumer receiving treatment can also receive a transfer paymentThis possibility however plays no role in our model because treat-ment eliminates all illness losses Therefore under an ideal contracta consumer with income Y enjoys an expected utility given by theformula
(1 )U (Y P)
cedil HL
0[U (Y P a` t(`)) b`]f (`)d` [1 F(L)]U(Y P) (1)
This expected-utility formula is a weighted sum of two componentsThe rst component is the utility of a healthy consumer who has paidthe insurance premium14 The second component (in curly braces) isthe conditional expected utility of an ill consumer who receives treat-ment when the benet is sufciently great but otherwise is compen-sated only by the indemnity payment The weights are the respectiveprobabilities of illness and health
12 We emphasize that our interpretation of ` is the treatmentrsquos potential benet topatients One could interpret alternatively that ` refers to patientsrsquo losses although wedo not think that this is always true For some illnesses it may be more natural to allowfor multiple treatments when severity varies See Chernew et al (2000)
13 A more general mechanism design approach to optimal insurance would allowthe insurance company to randomize the provision of treatment We ignore this possi-bility because it is unrealistic
14 The variable Y can be interpreted as income net of premiums paid for otherhealth insurance Thus Y P is net income after the premium insuring for this particulartreatment
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
86 Journal of Economics amp Management Strategy
Here illness affects an additive utility loss and does not directly affectthe consumerrsquos marginal utility of income we sometimes also use thenormalization b 1 interpreting ` as an expected utility loss fromforgoing treatment This broad interpretation implicitly recognizes theuncertainties surrounding illness and alternative treatments The gen-eral formulation allows for mixtures of monetary losses and (additive)utility losses from illness
The utility loss model seems more plausible than the monetaryloss model though both are special cases The monetary loss modelimplies that the demand for treatment does not depend on incomeThis seems unrealistic for many discretionary treatments Manningand Phelps (1979) found signicant income effects for specic den-tal treatments The RAND Health Insurance Study generally foundsmall but positive income elasticities and subsequent studies usingdifferent methods and data found larger elasticities (Phelps 1992) Incontrast the utility loss model implies a positive income elasticity ofthe demand for treatment without restricting its magnitude The util-ity loss model does imply that a consumerrsquos attitude toward incomerisk is independent of illness per se Obviously this is an empiricalquestion but seems extremely difcult to answer We have no a priorireason to think that the effect of illness on risk aversion goes one wayor another Therefore it seems reasonable at least as a rst step toignore this effect For these reasons we are partial to the utility lossmodel
We make several simplifying assumptions about treatment Firstthe cost of treatment is xed at C gt 0 It will be useful to think of C asa large number creating a signicant demand for insurance but notprohibitively large10 For example the Wall Street Journal article saysthat statin therapy costs $700 a year for life While this is an expen-sive therapy some consumersrsquo benets obviously are much higherthan $700 a year Second if the patient receives treatment then thelosses from illness are eliminated completely11 Thus ` indexes thebenets from receiving treatment These benets vary across patientsimplying that some patients are better candidates for treatment than
10 Obviously this treatment cost cannot be too large Otherwise there would be lit-tle demand for insurance in our model If C is sufciently small then there is a demandfor insurance to smooth the income uctuation resulting from illness and treatmentInterestingly in the monetary loss model the uctuation to be smoothed is the mone-tary equivalent of illness itself In the utility loss model the uctuation to be smoothedis the cost of treatment
11 As mentioned above we do not need to assume this in the utility loss model Inthis special case ` is the benet of possibly imperfect treatment
Health Insurance Moral Hazard and Managed Care 87
others12 Third we model the treatment decision as a binary choiceEither the patient receives treatment or not13 Consequently for a xedcopayment there is a critical value of ` such that more severely illpatients demand treatment while less severely ill patients do not aswe show later Finally the delivery of treatment is contractible mean-ing that the insurance company can prevent fraudulent claims for thereimbursement of nonexistent treatment costs
3 Ideal insurance
We begin by studying the ideal insurance contract in the absence ofmoral hazard In this regime illness and loss are assumed to be com-pletely contractible payments and treatment decisions can be contin-gent on the severity of illness Under an ideal contract the consumerpays a xed premium P and receives treatment whenever the benetof treatment ` is above a xed threshold L Moreover when treat-ment is withheld the consumer can be compensated by an indemnitypayment t(`) that depends on the severity of the illness In principlethe consumer receiving treatment can also receive a transfer paymentThis possibility however plays no role in our model because treat-ment eliminates all illness losses Therefore under an ideal contracta consumer with income Y enjoys an expected utility given by theformula
(1 )U (Y P)
cedil HL
0[U (Y P a` t(`)) b`]f (`)d` [1 F(L)]U(Y P) (1)
This expected-utility formula is a weighted sum of two componentsThe rst component is the utility of a healthy consumer who has paidthe insurance premium14 The second component (in curly braces) isthe conditional expected utility of an ill consumer who receives treat-ment when the benet is sufciently great but otherwise is compen-sated only by the indemnity payment The weights are the respectiveprobabilities of illness and health
12 We emphasize that our interpretation of ` is the treatmentrsquos potential benet topatients One could interpret alternatively that ` refers to patientsrsquo losses although wedo not think that this is always true For some illnesses it may be more natural to allowfor multiple treatments when severity varies See Chernew et al (2000)
13 A more general mechanism design approach to optimal insurance would allowthe insurance company to randomize the provision of treatment We ignore this possi-bility because it is unrealistic
14 The variable Y can be interpreted as income net of premiums paid for otherhealth insurance Thus Y P is net income after the premium insuring for this particulartreatment
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 87
others12 Third we model the treatment decision as a binary choiceEither the patient receives treatment or not13 Consequently for a xedcopayment there is a critical value of ` such that more severely illpatients demand treatment while less severely ill patients do not aswe show later Finally the delivery of treatment is contractible mean-ing that the insurance company can prevent fraudulent claims for thereimbursement of nonexistent treatment costs
3 Ideal insurance
We begin by studying the ideal insurance contract in the absence ofmoral hazard In this regime illness and loss are assumed to be com-pletely contractible payments and treatment decisions can be contin-gent on the severity of illness Under an ideal contract the consumerpays a xed premium P and receives treatment whenever the benetof treatment ` is above a xed threshold L Moreover when treat-ment is withheld the consumer can be compensated by an indemnitypayment t(`) that depends on the severity of the illness In principlethe consumer receiving treatment can also receive a transfer paymentThis possibility however plays no role in our model because treat-ment eliminates all illness losses Therefore under an ideal contracta consumer with income Y enjoys an expected utility given by theformula
(1 )U (Y P)
cedil HL
0[U (Y P a` t(`)) b`]f (`)d` [1 F(L)]U(Y P) (1)
This expected-utility formula is a weighted sum of two componentsThe rst component is the utility of a healthy consumer who has paidthe insurance premium14 The second component (in curly braces) isthe conditional expected utility of an ill consumer who receives treat-ment when the benet is sufciently great but otherwise is compen-sated only by the indemnity payment The weights are the respectiveprobabilities of illness and health
12 We emphasize that our interpretation of ` is the treatmentrsquos potential benet topatients One could interpret alternatively that ` refers to patientsrsquo losses although wedo not think that this is always true For some illnesses it may be more natural to allowfor multiple treatments when severity varies See Chernew et al (2000)
13 A more general mechanism design approach to optimal insurance would allowthe insurance company to randomize the provision of treatment We ignore this possi-bility because it is unrealistic
14 The variable Y can be interpreted as income net of premiums paid for otherhealth insurance Thus Y P is net income after the premium insuring for this particulartreatment
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
88 Journal of Economics amp Management Strategy
The insurance premium must cover the expected costs of treat-ment and indemnity payments Thus the premium constraint for theideal contract is given by the inequality
P cedil HL
0t(`)f (`) d` [1 F(L)]C (2)
The ideal contract maximizes expected utility subject to the premiumconstraint it is the solution (P t (`) L ) to the problem of maximiz-ing (1) subject to (2) The premium constraint is necessarily bindingat an optimum
Proposition 1 The ideal insurance contract species (a) a treatmentthreshold that equates the marginal benets of treatment to the marginalcost ie
U (Y P )aL bL U (Y P )C (3)
(b) indemnity payments that exactly compensate for the monetary losses froman untreated illness ie t (`) a` and (c) a premium that exactly coversthe expected costs Finally fewer patients receive treatment if the cost oftreatment is higher ie L is strictly increasing in C
The characterization of the optimal treatment threshold needs abit more interpretation The marginal cost of treatment C is in mon-etary units To measure the value of C in utility units it is multi-plied by the marginal utility of income U (Y P ) Equation (3) saysthat the utility of treatment evaluated at the threshold level of illness[U (Y P )a b]L equals the cost of treatment measured in utilityU (Y P )C In the monetary loss model (a 1 b 0) equation(3) states that treatment will be provided whenever the monetaryloss from an untreated illness exceeds the monetary cost of treatment(` C) In the utility loss model (a 0 b 1) the treatment thresh-old is set equal to the cost of an untreated illness [L U (Y P)C]and there is no indemnity payment for an untreated illness [t (`) 0]
4 Demand Management
We now turn to optimal insurance when illness and loss are not con-tractible The insurance company contracts with the consumer to reim-burse part or all of the cost of treatment but does not directly observeillness The treatment decision itself is delegated to the patient pre-sumably in consultation with a physician15 We refer to this schemeof insurance as demand management
15 Implicitly we assume that the physician is a perfect agent for consumers At theend of this section we briey discuss competition between self-interested physiciansIn Section 5 we examine physician incentives under managed care
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 89
Under a demand-managed insurance contract the patient paysa xed premium P up front and copays D for treatment Given thiscontract the patient demands treatment when the benets exceed theutility cost of the copayment Thus treatment is provided when theseverity of illness exeeds a threshold value L satisfying the treatmentconstraint
U (Y P aL) bL U(Y P D) (4)
This constraint states that a patient with illness severity L is indifferentabout receiving treatment and implicitly denes L as a function of Dand P This function determines the expected demand for treatmentby consumers who fall ill which is equal to 1 F(L)
As with ideal insurance the premium must cover the expectedcost of the insurance company Since treatment is provided only whenillness severity exceeds L the ex ante probability of treatment is [1F(L)] and the insurance company breaks even if the premium coversits expected liability16
P [1 F(L)](C D) (5)
The breakeven constraint denes a trade-off between the premiumand the copayment17
dPdD
[1 F(L)] f (L)(C D)LD
LP
dPdD
The rst term in this expression is the direct effect of shifting morecost to the patient while the second is the marginal demand reductionfrom a higher copayment Solving for the total effect reveals that ahigher copayment translates into a lower premium18
dPdD
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[aU (Y P aL) b] f (L)(C D)[U (Y P D) U (Y P aL)]
lt 0 (6)
16 The premium constraint P [1 F(L)](C D) must be binding for an optimalinsurance contract because expected utility given by (7) below is decreasing in thepremium
17 From the treatment constraint L D [U (Y P D)] [aU (Y P aL)b] gt 0 and L P [U (Y P D) U (Y P aL)] [aU (Y P aL) b] gt
0 For a small illness probability the effect of (L P) dP dD is of second-orderimportance
18 dP dD lt 0 follows from the fact that the treatment constraint implies D aL
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
90 Journal of Economics amp Management Strategy
Consumer expected utility is a probability-weighted average ofutility when healthy and when ill
(1 )U (Y P)
cedil HL
0[U (Y P a`) b`]f (`)d` [1 F(L)]U(Y P D) (7)
The event of illness occasions two possible losses First a consumersuffers monetary (a gt 0) and additive utility (b gt 0) losses from anuntreated illness (when ` L) Second the copayment reduces thedisposable income of a patient receiving treatment (when ` L)
Optimal demand management sets a premium and copaymentto maximize expected utility given that consumers determine treat-ment and the insurance company breaks even Thus the optimal con-tract (Pd Dd Ld) maximizes (7) subject to (4) and (5) We call this thedemand management problem A rst result traced to Zeckhauser (1970)is that consumers are only partially insured for the cost of treatmentThe consumer faces some risk of untreated illness and copays lessthan the full cost of treatment The solution balances the negativeconsumer welfare effect of a higher copayment against the positiveeffect of a lower premium
Proposition 2 Optimaldemandmanagementpartiallyinsures consumersagainst the cost of treatment (0 lt Dd lt C) and less severely ill patientsdecline treatment (Ld gt 0) The optimal copayment balances the expectedutility cost of a marginally higher copayment against the corresponding ben-ets of a lower premium ie
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L)]U (Y P D) (8)
where dP dD is given by (6)
The proposition reveals two marginal effects on consumer wel-fare of raising the copayment a direct effect of more income risk anda premium-reduction effect At an optimum there is no need to weighthe marginal effects on the demand for treatment because these areof second-order importance19
19 Taking the total derivative of (7) with respect to (D P L) yields
(1 cedil)U (Y P) cedilHL
0U (Y P a`) f (`) d` [1 F(L)]U (Y P D) dP
[1 F(L)]U (Y P D) dD [U(Y P aL) bL U(Y P D)]f (L) dL
The treatment constraint (4) implies that the last term vanishes leaving the two effectsidentied in the proposition
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 91
The optimal copayment depends on the consumerrsquos risk aver-sion and on the price elasticity of the expected demand for treat-ment both of which depend on the curvature of the utility functionThe well-known Arrow-Borch condition for optimal risk-spreadingrequires that marginal utilities of income be equal in all states ofillness and health However a copayment will create a distortionfrom optimal risk-spreading across the states in which the consumeris healthy and the states in which the consumer is treated for ill-ness The magnitude of the Arrow-Borch distortion for a given copay-ment U (Y P D) U (Y P) 1 depends only on the curvatureof the utility function on the domain between Y D and Y The con-sumerrsquos elasticity of expected demand for treatment with respect tothe copayment (holding the premium constant)20 f (L) [1 F(L)]DU (Y D) [aU (Y aL) b] also depends on the curvature of theutility function as well as on the losses from untreated illness andon the severity distribution These two magnitudes the Arrow-Borchdistortion and the price elasticity of demand are prominent in deter-mining the optimal cost-sharing ratio (C D) D when the probabilityof illness is small
Corollary 1 If the probability of illness is small then the optimal ratioof cost shares for the insurance company and the patient is approximatelyequal to the ratio of the Arrow-Borch distortion to the price elasticity ofdemand for treatment ie
f (Ld)
1 F(Ld)DdU (Y Dd)
aU (Y aLd) bC Dd
Dd
U (Y Dd)U (Y )
1 (9)
in the limit as cedil 021
20 To derive this elasticity differentiate [1 F(L)] with respect to D using (4) andthe chain rule and apply the denition of elasticity
21 The corollary is proved by substituting (6) into the rst-order condition inProposition 2 dividing through by and taking the limit as cedil 0 In the limitthe premium is zero because the consumer never becomes ill (Pd 0) However thepremium is positive in the neighborhood of the limit In general the consequencesof a change in the premium on expected consumer welfare are multifaceted partlybecause the marginal utility of income varies across the different states of illness andhealth However some of the premium effects of a small variation of the insurancecontract are more important than others viz some are proportional to cedil (rst-orderimportance) while others are proportional to 2 (second-order importance) The small-cedil approximation focuses on the rst-order effects The second-order effects that theapproximation ignores can be described as follows any change in the premium (P)affects consumer welfare differently across the different states of illness and healthbecause of the income effects of the copayment (D) and untreated illness (aL) Becausethe rst-order effects are roughly proportional to cedil and the second-order effects areroughly proportional to 2 there is no particular reason to think that the second-ordereffects dominate for plausible values of
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
92 Journal of Economics amp Management Strategy
The corollary illustrates neatly the conict between providinginsurance and controlling moral hazard On the one hand if the con-sumer is highly averse to income risk (a large Arrow-Borch distortion)then the insurance company should bear a high fraction of the treat-ment cost in order to better insure the patient On the other handif the demand for treatment is sensitive to price (a high price elastic-ity of demand) then the consumer should face a substantial treatmentexpense in order to curtail an excessive demand Optimal cost-sharingbalances these two concerns
We close this section on a technical note The demand man-agement problem is not in general a concave programming prob-lem Therefore the rst-order condition for an optimal contract inProposition 2 is not necessarily sufcient nor is the solution neces-sarily well behaved The following corollary provides an assumptionunder which this is not an issue22
Corollary 2 Assume that the following function is strictly increasingin D
D1
U (Y )1
U (Y D)[aU (Y aL) b]
1 F(L)
f (L)
with L determined by the treatment constraint and P 0 (the hazard-rateassumption) For cedil sufciently small the optimal threshold Ld and copay-ment Dd are unique differentiable and increasing in the treatment cost C
The hazard-rate assumption requires that the inverse hazard rateH (L) [1 F(L)] f (L) not decline too quickly It is satised forexample if H (L) is constant (exponential distribution) or increasing(eg Pareto distribution)
5 Does Moral Hazard Increase Treatment
We now turn to our main question How does moral hazard inuencetreatment Is the delivery of treatment under demand managementmore or less than that under the ideal contract We make two pointsin this section First the provision of treatment can be either decient(Ld gt L ) or excessive Second decient treatment is a robust possi-bility and occurs under various plausible conditions We focus on thecase of a small probability of illness
22 See Proposition 4 in Ma and Riordan (2000) for a formal proof The assumption isnot necessary for the result of the corollary It is sufcient that the demand managementproblem have a unique continuous global maximum
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 93
It is convenient to reformulate the demand management prob-lem slightly The treatment constraint (4) and the binding premiumconstraint (5) implicitly dene the premium P and copayment D asfunctions of treatment threshold L Solving for P and D as functionsof L and substituting these into the expression for consumer welfare(7) we obtain an expression for consumer welfare as a function of Lalone which we denote by Z(L) Optimal demand management deter-mines a treatment threshold that maximizes Z(L) Under the hazard-rate assumption (of Corollary 2) Z(L) is a quasiconcave function andtherefore achieves a unique local maximum at Ld We ask whetherthe derivative Z (L ) is positive or negative If Z(L) is quasiconcaveand Z (L ) gt 0 then treatment is provided deciently under demandmanagement (Ld gt L ) and conversely
Proposition 3 Under the hazard-rate assumption if the probability ofillness is small then treatment under optimal demand management is de-cient if the cost-share ratio exceeds the ratio of the Arrow-Borch distortionto the price elasticity of demand evaluated at the copayment for which theconsumer demands treatment if and only if the illness severity (`) exceedsthe ideal treatment threshold (L ) ie as cedil 0 L lt Ld if and only if
f (L )1 F(L )
D U (Y D )
aU (Y aL ) bC D
Dgt
U (Y D )
U (Y )1 (10)
where D satises the treatment constraint (4) evaluated at P 0 andL L The converse also holds
In the monetary loss model (b 0) the demand price for L isequal to the cost of treatment ie D C In this case inequality(10) obviously fails and we conclude that more treatment is providedunder demand management than under the ideal contract In this spe-cial case an uninsured consumer seeks treatment efciently (ie onlywhen the monetary benet exceeds the cost a` gt C) but this cannotbe optimal A risk-averse consumer will always demand some insur-ance resulting in an excessive provision of treatment starting fromD C the consumer is willing to pay a higher premium to achieve alower copayment which increases the demand for treatment23
Corollary 3 In the monetary loss model (b 0) treatment is excessiveunder demand management (Ld lt L )
23 The higher premium has a much smaller effect on the demand for treatmentbecause of the low probability of illness Actually though the following corollary doesnot require a small illness probability For the monetary loss model treatment is alwaysexcessive relative to the rst best That is the conditions in Proposition 3 are unneces-sary See Ma and Riordan (2000)
94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26

94 Journal of Economics amp Management Strategy
For the utility loss model (a 0) (3) implies that b U (Y )C Las cedil tends to 0 because the premium is proportional to In thislimiting case inequality (10) is equivalent to
C DC
U (Y D )U (Y D ) U (Y )
gt1 F(L )L f (L )
(11)
with D satisfying U(Y ) U (Y D ) CU (Y ) Substituting for Cusing the denition of D we can simplify (11) to
1 U (Y )[U (Y ) U (Y D )] D
1 U (Y )U (Y D )
gt1 F(L )
L f (L )
whose left-hand side lies between 0 and 1 because U (Y D )D gtU (Y ) U (Y D ) The elasticity of demand with respect to the disutil-ity ` is `f (`) [1 F(`)] we refer to this as the loss elasticity of demandIf demand is inelastic with respect to the utility loss then the right-hand side of (11) is greater than 1 in which case (10) is violated andtreatment is excessive The other side of the coin is that moral hazardcauses decient treatment if the loss elasticity is sufciently large
Corollary 4 In the utility loss model (a 0 and b 1) under thehazard-rate assumption if the illness probability is small and demand isinelastic with respect to the additive utility loss evaluated at the ideal thresh-old (L f (L ) [1 F(L )] lt 1) then treatment is excessive under demandmanagement (Ld lt L ) if the loss elasticity is sufciently large then treat-ment is decient
The corollary can also be interpreted as saying that treatment isdecient in the additive loss model if and only if the price elasticity ofdemand is sufciently high The ordinary price elasticity of demandin the utility loss model L f (L ) [1 F(L ) ] D U (Y D ) CU (Y ) isproportional to the loss elasticity Therefore holding the utility func-tion constant an increase in the loss elasticity (which depends only onF) translates directly into an increase in the price elasticity of demand
An interesting special case of the utility loss model occurs whenthe utility-of-income function exhibits constant absolute risk aversionie U (y) exp( ry) where r gt 0 is the coefcient of absolute riskaversion In this case D ln(1 rC) and (11) is equivalent to
rC ln(1 rC)
rC1 rC
rCgt
1 F(L )
L f ( ) (12)
The right-hand side of (12) is the elasticity of demand with respectto the disutility of illness evaluated at L The left-hand side is an
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 95
increasing concave function of rC ranging from 05 as r 0 to 10as r Thus holding the right-hand side constant24 we concludefrom this special case that treatment is decient if the consumer issufciently risk-averse and the loss elasticity is sufciently small Theintuitive explanation for this result is subtle A higher degree of riskaversion clearly increases the magnitude of the Arrow-Borch distor-tion when D is raised above D to curtail treatment However a higherdegree of risk aversion also corresponds to a greater income effect ofD on the demand for treatment Thus if r is higher then a givenincrease in D curtails treatment more resulting in a greater reductionin the premium The latter effect dominates making the increase in Dattractive to the consumer from an ex ante perspective
The above example and corollaries clearly demonstrate that de-cient treatment is a robust possibility This robustness argument canalso be made in a more general way Toward this end for a given L normalize the parameters a and b so that
b U (Y )CL
a (13)
Thus the treatment threshold under the ideal contract is held con-stant as the parameters a and b vary according to this constraint Theinequality (10) can be expressed alternatively as
C D1
U (Y )1
U (Y D )
gt1 F(L )
f (L )aU (Y aL ) U (Y )
CL
a (14)
The normalization (13) keeps L constant at the limit as cedil tends tozero An increase in a increases the right-hand side of (14) becauseU (Y aL ) gt U (Y ) Moreover since P tends to zero with thetreatment constraint implies that D increases with a for the samereason Therefore the left-hand side of (10) decreases as the value ofa increases and (14) is more likely to hold when a is smaller Nowxing values for C U(Y ) U (Y ) and D we can make the left-handside of (11) arbitrarily large by choosing a utility function with enoughcurvature on the interval [Y Y D ]25 This curvature is greater themore risk-averse is the consumer on this interval Putting togetherthese implications of Proposition 3 we conclude that decient treat-ment is a robust possibility over a range of values of a and b
24 Note that L can be held constant as rC varies by adjusting Y suitably25 Meanwhile the right-hand side can be held constant by adjusting a appropri-
ately and is constant if a 0
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
96 Journal of Economics amp Management Strategy
Corollary 5 Under the hazard-rate assumption and for a small illnessprobability less treatment is delivered under demand management thanunder the ideal contract (Ld gt L ) if and only if the parameter a is suf-ciently small and the consumer is sufciently risk-averse
The robust possibility of decient treatment does not hinge ona small illness probability as mentioned earlier Let the utility func-tion be logarithmic U(Y ) ln y and assume a standard uniformdistribution for losses f (`) 1 F(`) ` with 0 ` 1 (thusdispensing with the hazard-rate assumption as well) Let the cost oftreatment be expressed as a fraction of income C c Y Numeri-cal results are displayed in Figure 1 The graphs describe the treat-ment thresholds L as functions of the lower one corresponds to thetreatment threshold under the ideal contract the higher one demandmanagement Figure 1 shows that the threshold under demand man-agement is higher for all values of The graphs correspond to anexpensive treatment the value of c was set at 065 Further numeri-cal comparisons show that the difference between the two thresholds(the second-best threshold minus the rst-best threshold) increaseswith c For small values of c this difference is uniformly negativewhile for high values of c it is uniformly positive We have foundthat there are two local maxima for the numerical example and thatthe discontinuity in the second-best L represents a jump betweenthem Thus the numerical example also illustrates that our decient-treatment possibility is robust even when the objective function is notquasiconcave26
In the introduction we discussed the conventional wisdom thatmoral hazard causes an excessive provision of treatment Of coursethe conventional wisdom is imprecise as are most conventional wis-doms What is the relevant benchmark for determining if treatmentis excessive under demand management We have shown that theconventional wisdom is incorrect if the relevant benchmark is thedelivery of treatment under an ideal contract when moral hazard isabsent27
We have assumed implicitly that physicians act as perfect agentsfor the patients In Ma and Riordan (2000) we extend the utility
26 It also illustrates how moral hazard can result in a rather extreme marketfailuremdashno treatment or insurance
27 Other benchmarks for the conventional wisdom are possible (I) the amount oftreatment that would be provided if consumers lacked insurance or (II) the amountof treatment that is efcient ex post ie after consumers have paid the premiumThe conventional wisdom according to interpretation (I) is obvious The conventionalwisdom according to interpretation (II) is not necessarily correct Once consumershave paid the insurance premium Pd it is socially efcient to provide treatment to
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
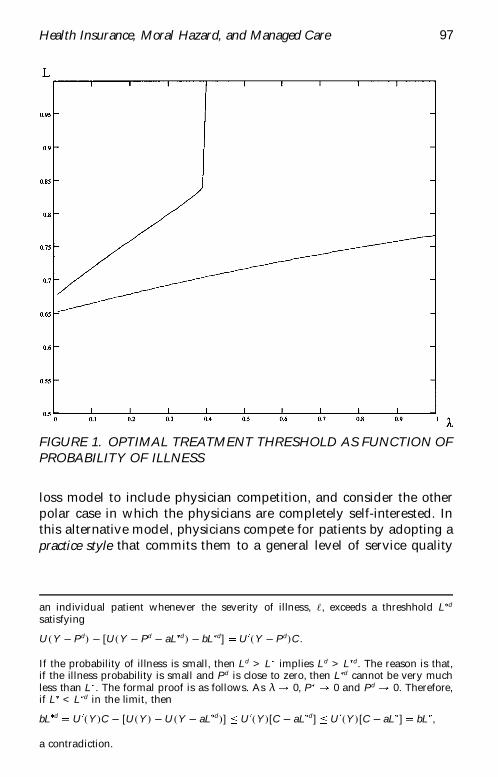
Health Insurance Moral Hazard and Managed Care 97
FIGURE 1 OPTIMAL TREATMENT THRESHOLD AS FUNCTION OFPROBABILITY OF ILLNESS
loss model to include physician competition and consider the otherpolar case in which the physicians are completely self-interested Inthis alternative model physicians compete for patients by adopting apractice style that commits them to a general level of service quality
an individual patient whenever the severity of illness ` exceeds a threshhold L d
satisfying
U (Y Pd) [U(Y Pd aL d ) bL d] U (Y Pd)C
If the probability of illness is small then Ld gt L implies Ld gt L d The reason is thatif the illness probability is small and Pd is close to zero then L d cannot be very muchless than L The formal proof is as follows As cedil 0 P 0 and Pd 0 Thereforeif L lt L d in the limit then
bL d U (Y )C [U(Y ) U (Y aL d )] U (Y )[C aL d ] U (Y )[C aL ] bL
a contradiction
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
98 Journal of Economics amp Management Strategy
and a treatment threshold Surprisingly optimal demand managementwhen prot-maximizing physicians compete on practice style yieldsresults almost identical to the case when physicians are perfect agentsfor consumers Competition forces physicians to act in the interestsof their patients and in equilibrium physicians adopt a treatmentthreshold that maximizes a consumerrsquos ex post utility
6 Supply Management and Managed Care
A distinguishing feature of managed care is that health-care providersare given explicit incentives to limit treatments Contracts with physi-cian groups often feature a ldquocapitated paymentrdquo for each patient butleave the physicians responsible for some or all of the treatment costsThis gives physicians an incentive to ration care in order to econo-mize on treatment costs Such supply management potentially com-plements and may even replace demand management as a method tocontrol moral hazard In this section we introduce a prot-consciousphysician into the model and allow a role for managed care For sim-plicity we rely on the utility loss model We argue that managed carebenets consumers and may expand treatment Indeed managed careachieves ideal insurance in some cases
The technology of illness and treatment is the same as in ourbasic model Consumer preferences have a utility loss representationU (y) ` The insurance company contracts with the risk-averse con-sumer and also with a risk-neutral physician (or physician group) todiagnose the patient and determine treatment The physician learnsthe realization of ` from the diagnosis and subsequently decides ontreatment
We interpret managed care as a capitated payment arrangementin which the physician is credited a total payment of S B for eachdiagnosed patient but is liable for an amount B of the treatment costEquivalently the physician is paid a xed fee S for a diagnosis andan additional bonus B if the diagnosed patient does not receive treat-ment28 If the physician treats a patient with ` gt L then his expectedpayment is [S F(L)B] Without loss of generality we assume that thetreatment cost C is paid directly by the insurance company ie thephysician receives a net payment that deducts treatment-cost liabilityfrom the capitation payments
The treatment decision is jointly determined by the physicianand patient To quote Arrow (1963 p 960)
28 In principle the contract could specify a payment to the physician even if theconsumer does not become ill However under the limited liability assumption intro-duced below this payment must be zero
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 99
By certifying to the necessity of given treatment or the lackthereof the physician acts as a controlling agent on behalfof the insurance companies Needless to say it is a far fromperfect check the physicians themselves are not under anycontrol and it may be convenient for them or pleasing totheir patients to prescribe more expensive medication pri-vate nurses more frequent treatments and other marginalvariations of care
In this spirit we interpret the treatment decision as a collectivedecision that maximizes a weighted sum of the benets to the physi-cian and the patient29 This might be interpreted as a ldquoreduced formrdquoof a bargaining model with the weights representing the bargain-ing strengths of the physician and the patient Implicitly we assumethat bargaining occurs after the consumer becomes ill but beforethe patient learns the severity of illness Thus the collective treat-ment decision in the utility loss model establishes a threshold thatmaximizes the physicianrsquos expected treatment payment minus theweighted patientrsquos expected loss from illness ie a value of L thatmaximizes
S F(L)B h HL
0`f (`) d` [1 F(L)][U (Y P) U(Y P D)]
The magnitude of the weight h captures the bargaining strength of thepatient ie the higher the value of h the greater the weight given tothe patientrsquos expected loss
The solution to the collective decision problem balances thephysicianrsquos bonus payment against the treatment benets of the mar-ginal patient
B h [L U(Y P) U (Y P D)] 0 (15)
This optimality condition is analogous to a treatment constraint in thedemand management problem If B 0 then it is identical If B gt 0so that the physician is at least partially liable for the treatment costthen it is weaker [L gt U (Y P) U (Y P D)] and some patientsare rationed ie a patient who wants treatment does not get it30
29 Ellis and McGuire (1990) use a similar assumption30 The physician has no incentive to treat the patient and then not report the treat-
ment to the insurer in order to collect the bonus This is because the physician wouldhave to be responsible for the treatment cost
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
100 Journal of Economics amp Management Strategy
The other constraints on contractual relationships of the insur-ance company are as follows First the premium and expected copay-ment must cover the expected costs to the insurance company
P cedil S F(L)B [1 F(L)](C D) (16)
Second the physician must nd the relationship protable
[S F(L)B] U (17)
The parameter U in this individual rationality constraint is the oppor-tunity value of the physicianrsquos time and effort in diagnosing and treat-ing the patient Finally nancial constraints put lower bounds on pay-ments to the physician ie
S S S B S (18)
The second of these limited-liability constraints is generally slack andwill be ignored The rst may or may not be slack The assumptionthat S is bounded from below by S allows the interpretation thatthe physician must be guaranteed a minimum compensation for theopportunity cost of diagnosis31
The optimal insurance contract maximizes the ex ante expectedutility of the patient given by (7) after setting a 0 and b 1 toconform with the utility loss model subject to the treatment individ-ual rationality and limited-liability constraints given by (15) to (18)The problem can be simplied further At an optimum the premiumconstraint (16) must bind Using this and the treatment constraint toeliminate S and B from (17) and (18) leaves a modied individualrationality constraint
P U [1 F(L)](C D) (19)
and a modied limited-liability constraint
P cedil S h F(L)[L U (Y P) U(Y P D)] [1 F(L)](C D) (20)
This reduces the managed care problem to choosing P D and L tomaximize (7) subject to the modied individual rationality constraint(19) and the modied limited-liability constraint (20)
31 Alternatively the limited-liability constraint can be interpreted as capturing riskaversion in a crude way that is the physician is risk-neutral with respect to incomevariation above some critical level and extremely risk-averse for income variationbelow this level (Sappington 1983) What is crucial for our analysis of managed careis that the physician is less risk-averse than the patient with respect to the uncertaincost of treatment and therefore better able to absorb this risk This is natural becausethe physician can diversify the treatment-cost risks across a population of patients andphysicians can further pool this risk within a group practice
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 101
The managed care problem has the same structure as the demandmanagement problem analyzed in Sections 3 and 4 (with S and U nor-malized to 0) except that the modied limited-liability constraint (20)relaxes the treatment constraint (4) Therefore since (4) was bindingin the demand management problem managed care must improve exante consumer welfare We expect this relaxation of the treatment con-straint to move the optimal treatment cutoff in the direction of idealinsurance Therefore if optimal demand management results in de-cient treatment relative to the ideal contract (eg as in Corollary 4)managed care should cause an expansion of treatment Our next resultshows that ideal insurance sometimes can be achieved when supplymanagement is possible
Consider a relaxed managed care insurance problem in whichthe modied limited-liability constraint (20) is ignored That is con-sider the maximization of (7) subject only to (19) The only differ-ence between this problem and the maximization problem for theideal contract in Section 3 is that the premium must also compen-sate for the physicianrsquos opportunity cost of diagnosis Proposition 1applies directly and the solution to the relaxed program species theideal treatment threshold L and a premium P that solve LU (Y P )C and P U [1 F(L )]C The ideal copayment iszero32
Proposition 4 The optimal treatment decision premium and copay-ment under managed care are the same as for the ideal contract if and onlyif the minimum payment for diagnosis is low enough so that the limited-liability constraint does not bind ie [S h F(L )L ] U
Under what conditions is the limited-liability constraint slackand ideal insurance possible If copayment is set at zero then thevalue of B must be set at h L to satisfy the treatment constraint (15)for the implementation of L For the physicianrsquos reservation wageconstraint to hold the value of S must be set to U F(L )BU h L F(L ) If this value of S is at least S then the limited lia-bility is slack When this is the case ideal insurance can be achievedwhile leaving the physician willing to participate The condition in theproposition is more easily satised when the interests of the patientare given little weight in the collective decision ie when h is smallindicating that the selsh physician has most of the bargaining poweror when C is sufciently small indicating that the treatment thresholdL is low The former situation suggests ironically that the consumer
32 The formal proof is straightforward and omitted
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
102 Journal of Economics amp Management Strategy
may be better off ex ante by having less control over the treatmentdecision ex post
Under the condition in Proposition 4 supply management is suf-cient to eliminate the loss due to moral hazard When the value ofh is high (relative to U and L ) then the condition will not be satis-ed and ideal insurance is infeasible In this case both demand andsupply management are combined in an optimal insurance contractthe physician will be strictly liable for a portion of treatment costsand the patient will have a strictly positive copayment This is statedformally in our nal result
Proposition 5 The physician bonus for withholding treatment and pa-tient copayment are both strictly positive (ie B gt 0 and D gt 0) if and onlyif [S h F(L )L ] gt U In this case S S
7 Concluding Remarks
Conventional wisdom presumes an overutilization of health care fromthe availability of insurance that insulates consumers from the full costof treatment We introduce a simple but realistic model of insuranceand treatment in order to evaluate this presumption We show that theconventional wisdom is not generally true An insurance plan basedoptimally on demand management (via copayments) can result indecient treatment relative to ideal insurance In particular treatmentfor a low-probability illness is decient if illness per se has little effecton the consumerrsquos marginal utility of income and if the consumerrsquosprice elasticity of demand for treatment is sufciently large relative tothe Arrow-Borch risk-spreading distortion when these are evaluatedat a copayment that brings forth the ideal provision of treatment
We also consider managed care based on a combination of dem-and and supply management instruments Our model of managedcare allows an insurer to reward a physician for withholding treat-ment This simple form of managed care may be sufcient to achieveideal insurance In this situation the patient makes no copaymentbecause physician incentives are sufcient for an efcient provisionof treatment Thus managed care corrects the treatment and risk-spreading distortions that arise under pure demand management andexpands or contracts the delivery of treatment accordingly When idealinsurance is infeasible under managed care then patient copaymentsare employed in combination with physician incentives In this casemanaged care alleviates the distortions that arise under pure demandmanagement but does so incompletely
For realism and simplicity we have avoided more general mech-anisms for the provision of health insurance Given the information
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 103
structure of our model a simple demand-managed health insurancecontract (premium plus copayment) is not necessarily optimal Therevelation principle states that any feasible insurance contract is equiv-alent to a direct revelation mechanism specifying a transfer paymentand a probability of treatment based on the patientrsquos (or physicianrsquos)disclosure of private knowldege about the benet of treatment Wedo not think that contracts providing treatment randomly are real-istic (although a cynic might argue that the purpose of utilizationreview is indeed to randomize the provision of treatment) Thus wedo think that the contracts we have studied are an appropriate norma-tive benchmark given the information structure of our model Still aformal treatment of a more general class of insurance contracts underprivate information may illuminate additional aspects of how moralhazard affects health care treatment decisions It would also be inter-esting to consider variable levels of treatment in this more generalframework
Appendix Proofs of Propositions
Proof of Proposition 1 The rst-order conditions for a solution P t( ) and L are respectively
(1 )U (Y P) cedilHL
0U (Y P a` t(`))f (`) d`
[1 F(L)]U (Y P) a 0
cedilU (Y P a` t(`))f (`) a f (`) 0
[U (Y P aL t(L)) bL]f (L)
f (L)U (Y P) a f (L)[t(L) C] 0
where a 0 is the multiplier The characterization of the rst bestfollows from solving the rst-order conditions
For the comparative statics of L with respect to C we totallydifferentiate (3) and the expression for P to obtain
dLdC
U (Y P)2 [1 F(L)]bLU (Y P)[aU (Y P) b]U (Y P) f (L)(aL C)bLU (Y P)
gt 0
where the inequality follows from aL C lt 0 which in turn followsfrom (3) and the concavity of U u
104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26

104 Journal of Economics amp Management Strategy
Proof of Proposition 2 Use the constraints (4) and (5) to dene P and Las functions of D Apply the implicit-function theorem and we obtainthe derivative in (6) Now regard the objective function
(1 )U(Y P) cedil HL
0[U (Y P a`) b`]f (`) d`
[1 F(L)]U (Y P D)
as a function in D where L and P in the expression are now functionsof D Differentiating with respect to D applying the chain rule andusing constraint (4) we obtain the derivative of the objective function
(1 )U (Y P) cedilHL
0U (Y P a`)f (`) d`
[1 F(L)]U (Y P D)dPdD
[1 F(L) ]U (Y P D) (21)
Equation (8) is obtained by setting (21) equal to zeroIt remains to show that 0 lt Dd lt C and Ld gt 0 But of course
from (4) 0 lt Dd lt C implies Ld gt 0 So we only need to show that Dd
is interior To show that D gt 0 we rst evaluate (6) at D 0 we get
dPdD
cedil cedilf (0)CU (Y P)
aU (Y P) b (22)
which makes use of the fact that D 0 implies that L 0 Next aftersimplication we obtain the value of (21) at D 0
U (Y P)dPdD
cedil
which is positive by (22) So D gt 0To show that D lt C we use the same method At D C P 0
and (6) becomes
dPdD
[1 F(L)]
The value of (21) at D C is
(1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D) [1 F(L)] [1 F(L)]U (Y D)
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
Health Insurance Moral Hazard and Managed Care 105
which becomes
U (Y D) (1 )U (Y ) cedilHL
0U (Y a`)f (`) d`
[1 F(L)]U (Y D)
after the common factor [1 F(L)] has been taken out Because U (Ya`) b` gt U(Y D) for ` lt L we have U (Y a`) lt U (Y D) So theabove expression must be negative and we conclude that D lt C u
Proof of Proposition 3 By the discussion preceding it the proposition isproved if (10) is necessary and sufcient for Z (L ) gt 0 as cedil 0Total differentiation gives
Z (L) [1 F(L)][aU (Y P(L) aL) b]
dPdL
(1 cedil)U (Y P(L))
cedil HL
0U (Y P(L) a`)f (`) d`
[1 F(L)]U (Y P(L) aL)
The derivative P (L) is
dPdL
[1 F(L)][aU (Y P aL) b] f (L)(C D)U (Y P D)[1 F(L)][U (Y P D) U (Y P aL)] U (Y P D)
(23)
which is obtained from applying the implicit-function theorem to theconstraints (4) and (5) to dene P and D as functions of L Using theabove we can show that P 0 as cedil 0 and with (23) Z (L) hasthe same sign as
(C D)1 F(L)
f (L)1
U (Y )1
U (Y D)[aU (Y aL) b] (24)
where
bL U(Y aL) U (Y D) (25)
Therefore we have Z (L ) gt 0 if and only if (10) and conversely u
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26
106 Journal of Economics amp Management Strategy
Proof of Proposition 5 The rst-order conditions for the maximizationof (7) with respect to (19) and (20) after simplication yield
U (Y P) ( a b )1 cedil F(L)
1 cedil F(L) b h F(L)
U (Y P D) ( a b )1 F(L)
1 F(L) b h F(L)
where a and b are respectively the multipliers of (19) and (20) Thesefurther simplify to
U (Y P) ( a b ) 1b h F(L)
1 cedil F(L)
1
U (Y P D) ( a b ) 1b h F(L)1 F(L)
1
Because the rst best is infeasible under the condition of the pro-position we have b gt 0 Therefore U (Y P D) gt U (Y P) orD gt 0
Also because the rst best is infeasible S 0 Since U gt 0 wehave B gt 0 from (17) u
References
Arrow KJ 1963 ldquoThe Welfare Economics of Medical Carerdquo American Economic Review53 941ndash973
1968 ldquoThe Economics of Moral Hazard Further Commentrdquo American EconomicReview 58 537ndash539
Baumgardner JR 1991 ldquoThe Interaction between Forms of Insurance and Types ofTechnical Change in Medical Carerdquo RAND Journal of Economics 22 36ndash53
Chernew ME WE Encinosa and RA Hirth 2000 ldquoOptimal Health Insurance TheCase of Observable Severe Illnessrdquo Unpublished Manuscript
de Meza David 1983 ldquoHealth Insurance and the Demand for Medical Carerdquo Journalof Health Economics 2 47ndash54
Ellis RP and TG McGuire 1990 ldquoOptimal Payment Systems for Health ServicesrdquoJournal of Health Economics 9 (4) 375ndash396
and 1993 ldquoSupply-Side and Demand-Side Cost Sharing in Health CarerdquoJournal of Economic Perspectives 7 135ndash152
Grossman SJ and OD Hart 1986 ldquoThe Costs and Benets of Ownership A Theoryof Vertical and Lateral Integrationrdquo Journal of Political Economy 94 691ndash719
Ma CA and TG McGuire 1997 ldquoOptimal Health Insurance and Provider PaymentrdquoAmerican Economic Review 87 685ndash704
and MH Riordan 2000 ldquoHealth Insurance Moral Hazard and Managed CarerdquoBoston University Discussion Paper
Manning WG Jr and CE Phelps 1979 ldquoThe Demand for Dental Carerdquo The BellJournal of Economics 10(2) 503ndash525
Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26

Health Insurance Moral Hazard and Managed Care 107
Marshall JM 1976 ldquoMoral Hazardrdquo American Economic Review 66(5) 880ndash890Newhouse JP 1996 ldquoReimbursing Health Plans and Health Providers Selection versus
Efciency in Productionrdquo Journal of Economic Literature 34 1236ndash1263Pauly M 1968 ldquoThe Economics of Moral HazardCommentrdquo American Economic Review
58 531ndash537Phelps CE 1992 Health Economics Harper Collins New YorkSappington DEM 1983 ldquoLimited Liability Contracts between Principal and Agentrdquo
Journal of Economic Theory 29 1ndash21Zeckhauser R 1970 ldquoMedical Insurance A Case Study of the Tradeoff between Risk
Spreading and Appropriate Incentivesrdquo Journal of Economic Theory 2 10ndash26





























