Embed Size (px)
Citation preview
Vulnerability and the International Health Response in the West Bank and Gaza Strip
An analysis of health and the health sector.
November 2001
Prepared for the Core Group on Health by
Michaela V. Pfeiffer
WHO Consultant & Peacepath Team Leader
for the Palestinian territories
World Health Organization
4 Ibn Batuta Street P.O. Box 54812
Jerusalem
Tel: +972 2 627 6680 Fax: +972 2 627 6690
Email: [email protected]
Via Leonina 38 00184 Rome
ITALY
Tel/fax: +39 06 481 9625 Email: [email protected] Http://wwwpeacepathconsulting.com

Copyright November 2001
by the Department of Emergency and Humanitarian Action (EHA) of the World Health Organization and PEACEPATH CONSULTING.
The views expressed in this report are those of the authors and do not necessarily represent the policies or views of the World Health Organization. The designations employed in this publication and the presentation of the material do not imply on the part of WHO/EHA or PEACEPATH CONSULTING the expression of any opinion whatsoever concerning the legal status of any country or territory, or of its authorities, or the delimitations of its frontiers.
ii

Contents List of figures and tables iv
List of acronyms vi
Acknowledgments vii
Introduction viii
Executive summary ix
Part 1: A snapshot of health and the health sector 1
1.1 Demographics 1
1.2 Health status 3
1.3 Health care system 8
Part 2: Linkages between health and the current context 21
2.1 Who are the vulnerable? 21
2.2 What are the root causes of vulnerability? 25
Part 3: Implications for the international response 39
3.1 Overview of the international health response to date 39
3.2 Determinants of the impact of the international health response 41
3.3 Discussion 52
Appendices 55
A.1 Additional datasets 55
A.2 List of key persons met 57
A.3 Essential Reading List 59
iii
List of figures and tables:
Figures
1.1 Population overview in the West Bank and Gaza (2000) 1 1.2 Fertility rates from 1993 – 2000. 2 1.3 MoH expenditures on health in 2000. 16 1.4 Donor and government health expenditures per capita (1996- 2000) 16 1.5 Organizational structure of the Palestinian MoH. 18 2.1 Unemployment rates in the WBGS (Q1 1999 to Q1 2001). 23 2.2 School enrollment rates by age and sex in 2000. 24 2.3 Deaths and Injuries per month (29 Sep 2001 – 30 Sep 2000). 31 3.1 Donor commitments from 1994 – 2001 by sector. 39 3.2 Factors influencing the impact of the international health response. 42 3.3 General coordination mechanisms in the West Bank and Gaza Strip. 48 3.4 Health coordination structures in the West Bank and Gaza Strip. 49
iv
Tables
1.1 Changes in health status from 1995 to 2000. 3 1.2 Regional comparisons of the status of health in 1999. 4 1.3 Self-reported morbidity in 2000 (% of population). 4 1.4 Incidence of the top 5 infectious diseases in the Gaza Strip (2000) 5 1.5 Leading causes of death among children under 5 (1-4 years) in 2000. 5 1.6 Age standardized mortality rates among children aged 5 –19 in 2000. 5 1.7 Age standardized mortality rates among adults aged 20 – 59 in 2000. 6 1.8 Age standardized mortality rates among adults aged 60+ in 2000. 6 1.9 Rank of the top ten reported infectious diseases in 2000. 6 1.10 EPI vaccination coverage in the WBGS (1995 – 2000) 9 1.11 Percent of the population with access to safe drinking water in 2000. 9 1.12 % of households with access to sewage facilities by locality and region. 10 1.13 Services provided by the 4 main health sector providers. 11 1.14 Distribution of PHC facilities by provider type. 11 1.15 Users of primary care facilities by service provider in 1998 (percent). 12 1.16 Total number of beds by health sector provider in 2000. 13 1.17 Distribution & types of beds available (2000). 13 1.18 Hospital utilization by provider type in 1999. 13 1.19 Human resources in the Palestinian primary health care sector (2000). 15 1.20 Health care providers per population – a regional comparison. 15 1.21 Pharmaceutical sector overview (as of 1997). 19 2.1 Psychological conditions reported among children (5-17 years) during the
period October 2000 – July 2001. 24 2.2 Vulnerability matrix. 25 2.3 Select economic indicators affecting household income in the WBGS. 27 2.4 Change in the average daily wage (NIS) from October to January 2001. 27 2.5 Average price of food items in July 2001. 28 2.6 Average cost of treatment in PHCs by service provider in 1998. 29 2.7 Median fees paid for different items by type of hospital (1998). 29 2.8 Profile of government health insurance in 1998. 30 2.9 Access to primary care facilities by provider type in 1998. 32 3.1 Funds committed in select sectors during the period 2000 – 2001. 40 3.2 Decision making matrix. 53
v

List of acronyms AHLC Ad-hoc Liaison Committee CBR Crude birth rate CDR Crude death rate CG Consultative Group CPI Consumer price index EAP Emergency Assistance Programme EMS Emergency medical services EMT Emergency medical technician EPI Expanded programme on immunization GHI Government health insurance GMP Good manufacturing practice HFTEN Humanitarian task force on emergency needs HIS Health information system HR Human resources ILO International Labor Organization IMR Infant mortality rate INGO International non-governmental organization JLC Joint liaison committee LACC Local aid coordination committee LEB Life expectancy at birth MIS Management information systems MMR Maternal mortality rate MoH Ministry of Health MOPIC Ministry of Planning and International Cooperation NGO Non-governmental organization NHP National Health Plan NIS New Israeli Shekel PA Palestinian Authority PCBS Palestine Central Bureau of Statistics PDP Palestinian Development Plan PHC Primary health care PNGO Palestinian NGOs (an umbrella organization) PRCS Palestinian Red Crescent Society STDs Sexually transmitted diseases SWG Sector Working Group UNDP UN Development Programme UNFPA UN Family and Population Agency UNICEF UN Children’s Fund UNRWA UN Relief and Works Agency for Palestine Refugees in the Near East UNSCO UN Special Coordination for the Occupied Territories USD United States Dollar WBGS West Bank and Gaza Strip WHO World Health Organization
vi
Acknowledgments A number of individuals and organizations were involved in the research and preparation of this report. It has been a collective effort thanks to the enthusiasm, support and generosity of all of those consulted.
Special thanks should be extended to Dr. Giuseppe Masala, Dr. Othman Karameh and Dr. Rafik Zanoun. Thanks also to the WHO Offices in Jerusalem (Mufid, Rania and Lina) and Gaza (Lubna and the field assistants Naema and Dr. Fawaz). Without out their support and enthusiasm, none of this would have come into fruition.
At the WHO headquarters level, thanks should be extended to Dr. Xavier Leus, Dr. Johanna Larusdottir, Dr. Khalid Shibib, Dr. Paolo Piva and Ms. Doreen Brown for their feedback and logistics and administrative support.
Thank you also to Mr. Gregory Hess of Peacepath Consulting for your support and valuable inputs.
Finally, I would like to thank the Core Group, the vulnerability workshop participants and individuals interviewed during this process. Thank you to all of you for listening and sharing your views and experience.
vii
Introduction This Vulnerability Analysis explores the root causes of health vulnerability in the West Bank and Gaza Strip (WBGS). Its primary purpose is to serve as a tool for the Core Group on Health to stimulate dialogue within the health community about potential responses to meet current and future health needs. This analysis aims to generate dialogue and does not contain concrete recommendations or strategies about how the current health sector problems can be addressed. Rather it poses questions and highlights key factors that are influencing the overall impact of the health sector response. The intention is that this document will be used by the Core Group to guide processes for dealing with issues that affect all persons, institutions and organizations working in the health sector.
There are three principal components to the report:
Part 1 contains an overview of the health status of the population and the health care system.
Part 2 looks at vulnerability and examines some of the relationships (explicit and implicit) between changes in the broader socio-economic and political context and the health care needs of the population. As a consequence, who and what are emerging health sector concerns?
Part 3 begins by looking at the nature and extent of the international health response to date and highlights key factors influencing the impact of the international health response. What are the critical challenges facing the international community in this sector?
The information contained in this report was gathered through a detailed literature review (published and unpublished), interviews and workshops held with members of the Core Group. Consequently, many of the issues and ideas included in the analysis are drawn from collective thinking done during the workshops More details about the proceedings of the workshops and the list of participants are provided in Part 3 and the annexes of this report.
viii
Executive summary The Vulnerability Analysis explores the root causes of health vulnerability in the West Bank and Gaza Strip and their implications for the international health sector response. The analysis was prepared through collection and analysis of existing documents, interviews, and workshops held in October 2001 with international and Palestinian representatives. Many of the issues and ideas included in the analysis are drawn from collective thinking done during the workshops.
Part 1: A snapshot of health and the health care system
Health Status The West Bank and Gaza Strip (WBGS) is undergoing a dual faceted epidemiological transition similar to that of middle-income countries. On the one hand disease patterns are characterized by diseases typical of developing countries (respiratory infections, diarrhoea and parasitic diseases) particularly among children under the age of 18 years. On the other hand, diseases of developed countries (hypertension, diabetes, cancer) are most common among adults.
Life expectancy at birth has remained fairly constant in recent years while other indicators of social health, infant mortality (IMR), and crude death rates (CDR) have declined suggesting that positive improvements in health have been achieved.
Determining the precise impacts of recent crisis (which escalated at the end of September 2000) on health was not the purpose of this document. However, data from some sources suggest that there has been a deterioration in certain health conditions notably nutrition, psycho-social health, and maternal and child health.
In relation to neighboring countries, health indicators for the West Bank and Gaza Strip compare favorably. The most striking difference in the WBGS is the high dependency ratio particularly in the Gaza Strip.
Health care system
a) Public health system This section includes information on the collection and use of health information, vaccinations, access to safe drinking water, and sewage and wastewater management.
b) Health care resources There are four major health care providers operating in The Palestinian territories, the Ministry of Health (MoH), UNRWA, NGOs and the private sector. The major providers of primary care services are the MoH and UNRWA. The major providers of secondary services are the MoH and NGOs. The major provider of tertiary care is the private sector.
This section provides a detailed overview of health care facilities, services and expenditures.
c) Pharmaceutical sector Overall availability of drugs in the West Bank and Gaza Strip is satisfactory although fluctuations in stock have been observed during periods of socio-economic and political instability. However, drugs are exceptionally expensive in the Palestinian territories and good pharmaceutical practice is not widespread. Consequently, the proportion of the MoH budget is spent annually on drugs and consumables is considerable.
ix

Part 2: Vulnerability and linkages between health and the current context
From October 2000 to March 2001 nearly half of all Palestinian households received some form of humanitarian assistance. This amounted to 35.1 percent of all families in the West Bank and 71 percent of families in the Gaza Strip.
Included among the vulnerable are the following: social cases (widows, orphans, the elderly, prisoners and students); the physically and mentally disabled; the chronically ill (especially cancer and dialysis patients); refugees and internally displaced families forced to move because of increased insecurity and/or destruction of housing; rural populations most heavily affected by tightened road closures; the growing number of poor and unemployed; and children under the age of 18.
What are the roots of vulnerability? Vulnerability in health is inextricably linked to its broader socio economic and political context. Traditional approaches to vulnerability tend to focus on the identification of the essential needs of the most vulnerable. While this needs-based approach allows for the rapid determination of priority relief interventions, it does not provide insight as to why people are vulnerable.
This section identifies the roots of vulnerability in health on two levels, household and institutional. It then examines the contextual and systemic factors which directly and indirectly influence household and institutional vulnerability.
Contextual factors examined include: a) Closure b) Economics c) Conflict and/or the threat of violence
Systemic factors examined include: a) Distribution of health services b) Multiple service providers c) Separation of the West Bank and Gaza d) Constraints to policy, planning and capacity building
Part 3: Implications for the international health response
From 1994 to June of 2001, over 5.2 billion USD was committed to the West Bank and Gaza Strip by the International Community at an average of 645 million USD per year. Aid per capita during this period (~214 USD) was almost 10 times aid per capita spent in developing counties and second only to the 380 USD spent per capita on post-conflict reconstruction in Bosnia.
The overall shape of the international health response in the West Bank and Gaza Strip is influenced by a number of factors both within and outside the health sector. This section of the analysis groups these factors into four main categories and highlights key issues for the international community:
1. Health sector related issues are factors inherent in the way that the health sector is structured and operates. These include:
a) Multiple health care providers b) Lack of a common vision for the health sector c) Questions about the credibility of health sector counterparts
2. Contextual factors are factors inherent in the overall operating environment which influence the effectiveness of external interventions. These include:
a) Access to health care services and service delivery b) Interim agreements and questions of the jurisdiction of the MoH c) The status of the refugees
x
3. External and/or global factors are factors external to the Palestinian context which may or may not influence external activity/interests in the region. These include:
a) Diversion of aid to other crises b) Media attention c) Global market forces
4. Factors inherent in the international aid system are factors rooted deep within the international aid system which limit the effectiveness and flexibility of interventions. These include:
a) Coordination b) Information for planning, i.e. who is doing what, where and how c) Vision and the lack of an overall strategic development framework
3.3 Discussion
The Vulnerability Analysis aims to stimulate dialogue between actors working within the health sector, not to provide a series of concrete recommendations for a large and diverse set of actors. The report concludes with a discussion of two issues which emerged strongly in the preparation of the analysis:
1. The needs in the West Bank and Gaza Strip are vast and complicated requiring both emergency and longer-term developmental approaches. Given that activities tend to be categorized as “relief” or “development” activities, organizations mandated to work in one track or the other have had difficulties adapting to the Palestinian context.
2. There is a need for a clear plan of action and strategy for the health sector that not only frames short-term relief assistance in the longer-term, but also aligns Palestinian health sector priorities and international interventions. In the absence of this strategic plan, there will continue to be no operating framework within which to measure the performance and effectiveness of external assistance. Mechanisms to measure performance and capitalize on lessons learned would greatly enhance the potential of external assistance to promote a smooth transition in the health sector.
xi
Health Status
Part 1: A snapshot of health and the health sector. This section contains an overview of the health status of the population and the health care system. Where possible, trends will be examined over a 7-year period (since 1994).
1.1 Demographics
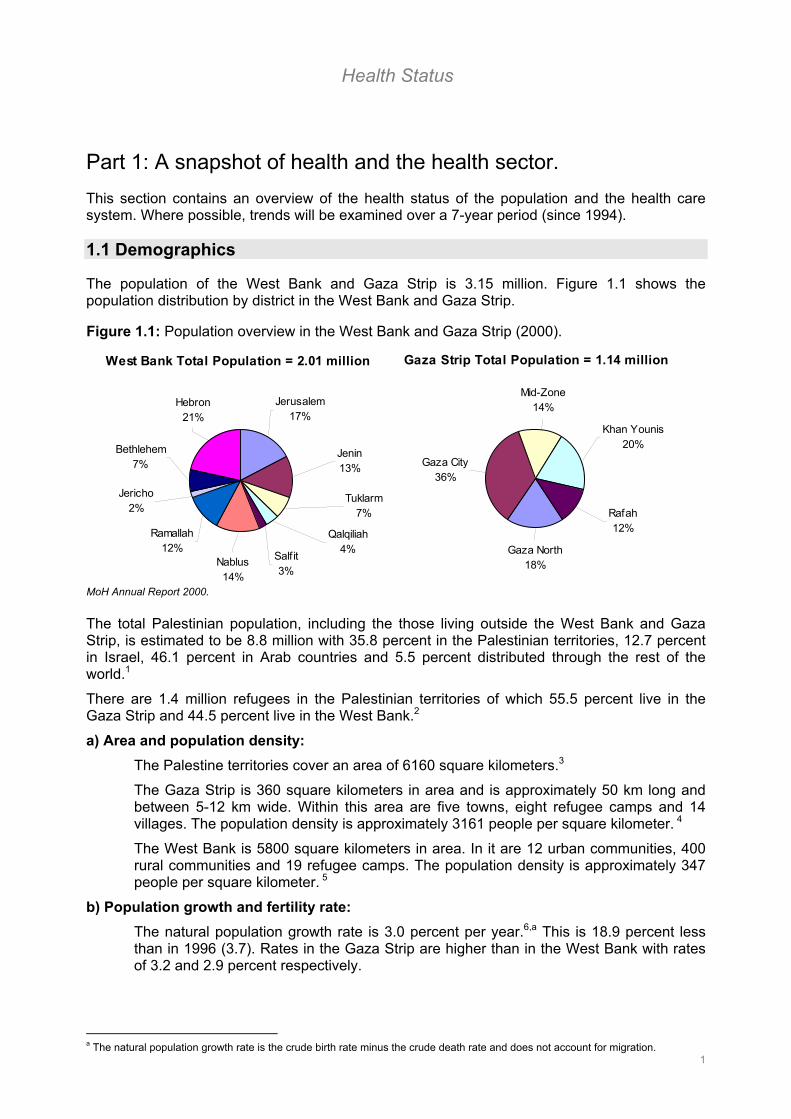
The population of the West Bank and Gaza Strip is 3.15 million. Figure 1.1 shows the population distribution by district in the West Bank and Gaza Strip.
West Bank Total Population = 2.01 million
Ramallah12%
Hebron21%
Jerusalem17%
Jericho2%
Bethlehem7%
Nablus14%
Salfit3%
Qalqiliah4%
Jenin13%
Tuklarm7%
Gaza Strip Total Population = 1.14 million
Gaza City36%
Gaza North18%
Rafah12%
Khan Younis20%
Mid-Zone14%
MoH Annual Report 2000.
Figure 1.1: Population overview in the West Bank and Gaza Strip (2000).
The total Palestinian population, including the those living outside the West Bank and Gaza Strip, is estimated to be 8.8 million with 35.8 percent in the Palestinian territories, 12.7 percent in Israel, 46.1 percent in Arab countries and 5.5 percent distributed through the rest of the world.1
There are 1.4 million refugees in the Palestinian territories of which 55.5 percent live in the Gaza Strip and 44.5 percent live in the West Bank.2
a) Area and population density: The Palestine territories cover an area of 6160 square kilometers.3
The Gaza Strip is 360 square kilometers in area and is approximately 50 km long and between 5-12 km wide. Within this area are five towns, eight refugee camps and 14 villages. The population density is approximately 3161 people per square kilometer. 4
The West Bank is 5800 square kilometers in area. In it are 12 urban communities, 400 rural communities and 19 refugee camps. The population density is approximately 347 people per square kilometer. 5
b) Population growth and fertility rate: The natural population growth rate is 3.0 percent per year.6,a This is 18.9 percent less than in 1996 (3.7). Rates in the Gaza Strip are higher than in the West Bank with rates of 3.2 and 2.9 percent respectively.
1
a The natural population growth rate is the crude birth rate minus the crude death rate and does not account for migration.

Health Status
Fertility ratesb have been declining over the past few years as shown in Figure 1.2. In 2000, the fertility rate in the Palestinian territories was 4.31; 3.8 in the West Bank and
5.4 in the Gaza Strip. Fertility peaks between the ages of 25 and 29.7 Figure 1.2: Fertility rates from 1993 - 2000.
c) Age and sex characteristics: The male/female split of the population in the West Bank and Gaza Strip is almost even at 51 percent male and 49 percent female. The male/female sex ratio is 102 males to 100 females. 8
The median age of the population in 2000 was 17 years in the West Bank and 15 in the Gaza Strip. Age/sex histograms for the West Bank and Gaza Strip are provided in Annex 1.
50 percent of the population in the Gaza Strip and 45 percent in the West Bank are
under the age of 15. Consequently, the dependency ratioc is high at 101 (94.3 in the West Bank and 112.8 in the Gaza Strip).9 This is considerably higher than in neighboring countries (70.1 percent in Egypt; 83 percent in Jordan; and the 61.9 percent average for the Arab Countries).10
0
1
2
3
4
5
6
7
8
1993 1994 1995 1996 1997 1998 1999 2000
MoH Annual Reports.
d) Household characteristics: The average household size is 6.1 persons. Households in the West Bank are slightly smaller (5.7) than in the Gaza Strip (6.9). Refugee households are even smaller averaging around 4.6 persons.11 The average number of people per room is 1.99. This figure is slightly higher in refugee camp settings (2.11).12
Approximately 8.8 percent of all households are female headed households; 9.7 percent in the West Bank and 7 percent in the Gaza Strip. 13
b The fertility rate is the number of births per 1000 women of child-bearing age (15-44 years).
2
c The dependency ratio is the number of dependents, including children under the age of 15 and elderly over the age of 65 per 100 people of working age.
Health Status
1.2 Health Status
The West Bank and Gaza Strip is undergoing a dual faceted epidemiological transition similar to that of middle-income countries. On the one hand disease patterns are characterized by diseases typical of underdeveloped countries (respiratory infections, diarrhoea and parasitic diseases) particularly among children under the age of 18 years. On the other hand, diseases of developed countries (hypertension, diabetes, cancer) are most common among adults.
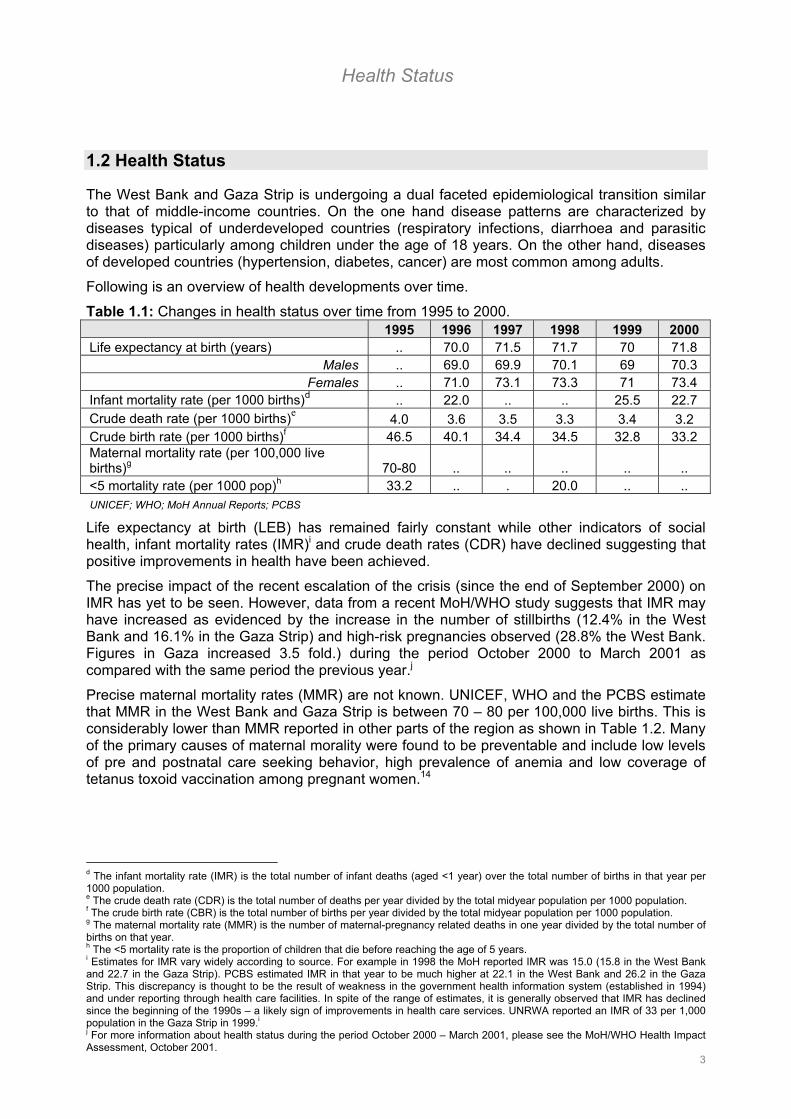
Following is an overview of health developments over time.
Table 1.1: Changes in health status over time from 1995 to 2000. 1995 1996 1997 1998 1999 2000 Life expectancy at birth (years) .. 70.0 71.5 71.7 70 71.8
Males .. 69.0 69.9 70.1 69 70.3 Females .. 71.0 73.1 73.3 71 73.4
Infant mortality rate (per 1000 births)d .. 22.0 .. .. 25.5 22.7 Crude death rate (per 1000 births)e 4.0 3.6 3.5 3.3 3.4 3.2 Crude birth rate (per 1000 births)f 46.5 40.1 34.4 34.5 32.8 33.2 Maternal mortality rate (per 100,000 live births)g 70-80 .. .. .. .. .. <5 mortality rate (per 1000 pop)h 33.2 .. . 20.0 .. .. UNICEF; WHO; MoH Annual Reports; PCBS
Life expectancy at birth (LEB) has remained fairly constant while other indicators of social health, infant mortality rates (IMR)i and crude death rates (CDR) have declined suggesting that positive improvements in health have been achieved.
The precise impact of the recent escalation of the crisis (since the end of September 2000) on IMR has yet to be seen. However, data from a recent MoH/WHO study suggests that IMR may have increased as evidenced by the increase in the number of stillbirths (12.4% in the West Bank and 16.1% in the Gaza Strip) and high-risk pregnancies observed (28.8% the West Bank. Figures in Gaza increased 3.5 fold.) during the period October 2000 to March 2001 as compared with the same period the previous year.j
Precise maternal mortality rates (MMR) are not known. UNICEF, WHO and the PCBS estimate that MMR in the West Bank and Gaza Strip is between 70 – 80 per 100,000 live births. This is considerably lower than MMR reported in other parts of the region as shown in Table 1.2. Many of the primary causes of maternal morality were found to be preventable and include low levels of pre and postnatal care seeking behavior, high prevalence of anemia and low coverage of tetanus toxoid vaccination among pregnant women.14
d The infant mortality rate (IMR) is the total number of infant deaths (aged <1 year) over the total number of births in that year per 1000 population. e The crude death rate (CDR) is the total number of deaths per year divided by the total midyear population per 1000 population. f The crude birth rate (CBR) is the total number of births per year divided by the total midyear population per 1000 population. g The maternal mortality rate (MMR) is the number of maternal-pregnancy related deaths in one year divided by the total number of births on that year. h The <5 mortality rate is the proportion of children that die before reaching the age of 5 years. i Estimates for IMR vary widely according to source. For example in 1998 the MoH reported IMR was 15.0 (15.8 in the West Bank and 22.7 in the Gaza Strip). PCBS estimated IMR in that year to be much higher at 22.1 in the West Bank and 26.2 in the Gaza Strip. This discrepancy is thought to be the result of weakness in the government health information system (established in 1994) and under reporting through health care facilities. In spite of the range of estimates, it is generally observed that IMR has declined since the beginning of the 1990s – a likely sign of improvements in health care services. UNRWA reported an IMR of 33 per 1,000 population in the Gaza Strip in 1999.i
3
j For more information about health status during the period October 2000 – March 2001, please see the MoH/WHO Health Impact Assessment, October 2001.
Health Status
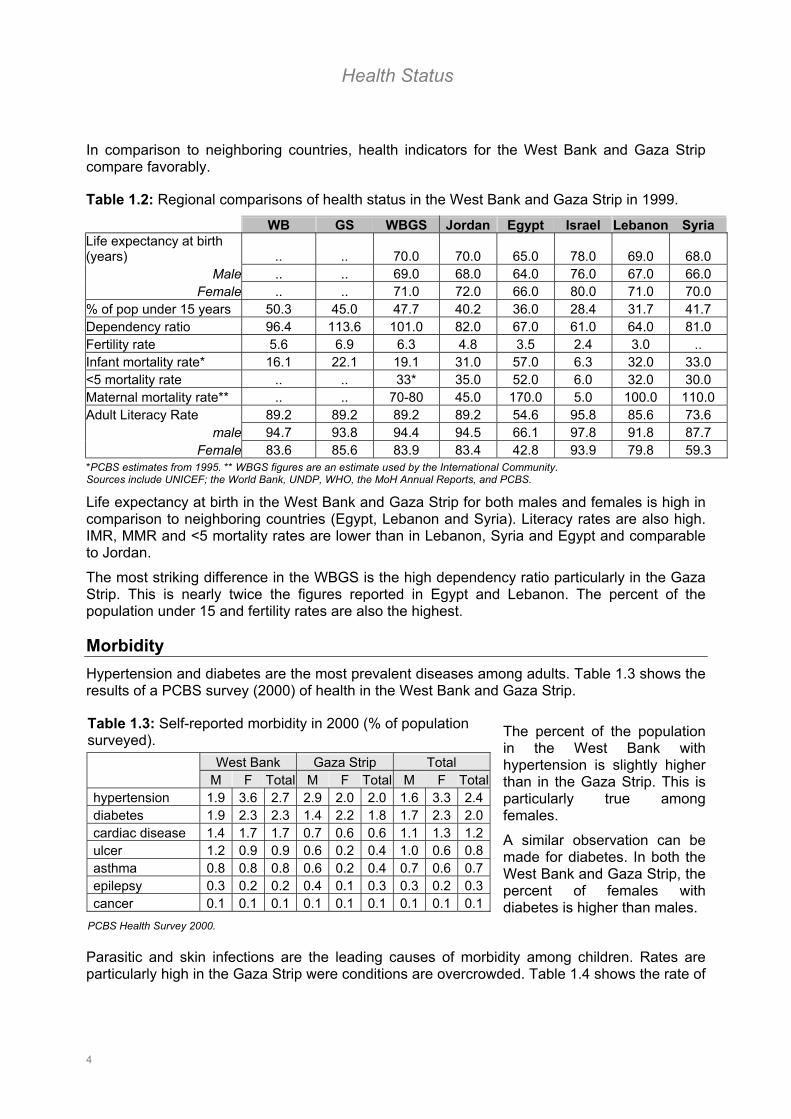
In comparison to neighboring countries, health indicators for the West Bank and Gaza Strip compare favorably.
Table 1.2: Regional comparisons of health status in the West Bank and Gaza Strip in 1999. WB GS WBGS Jordan Egypt Israel Lebanon Syria Life expectancy at birth (years) .. .. 70.0 70.0 65.0 78.0 69.0 68.0
Male .. .. 69.0 68.0 64.0 76.0 67.0 66.0 Female .. .. 71.0 72.0 66.0 80.0 71.0 70.0
% of pop under 15 years 50.3 45.0 47.7 40.2 36.0 28.4 31.7 41.7 Dependency ratio 96.4 113.6 101.0 82.0 67.0 61.0 64.0 81.0 Fertility rate 5.6 6.9 6.3 4.8 3.5 2.4 3.0 .. Infant mortality rate* 16.1 22.1 19.1 31.0 57.0 6.3 32.0 33.0 <5 mortality rate .. .. 33* 35.0 52.0 6.0 32.0 30.0 Maternal mortality rate** .. .. 70-80 45.0 170.0 5.0 100.0 110.0 Adult Literacy Rate 89.2 89.2 89.2 89.2 54.6 95.8 85.6 73.6
male 94.7 93.8 94.4 94.5 66.1 97.8 91.8 87.7 Female 83.6 85.6 83.9 83.4 42.8 93.9 79.8 59.3
*PCBS estimates from 1995. ** WBGS figures are an estimate used by the International Community. Sources include UNICEF; the World Bank, UNDP, WHO, the MoH Annual Reports, and PCBS.
Life expectancy at birth in the West Bank and Gaza Strip for both males and females is high in comparison to neighboring countries (Egypt, Lebanon and Syria). Literacy rates are also high. IMR, MMR and <5 mortality rates are lower than in Lebanon, Syria and Egypt and comparable to Jordan.
The most striking difference in the WBGS is the high dependency ratio particularly in the Gaza Strip. This is nearly twice the figures reported in Egypt and Lebanon. The percent of the population under 15 and fertility rates are also the highest.
Morbidity Hypertension and diabetes are the most prevalent diseases among adults. Table 1.3 shows the results of a PCBS survey (2000) of health in the West Bank and Gaza Strip.
Table 1.3: Self-reported morbidity in 2000 (% of population surveyed). West Bank Gaza Strip Total M F Total M F Total M F Totalhypertension 1.9 3.6 2.7 2.9 2.0 2.0 1.6 3.3 2.4diabetes 1.9 2.3 2.3 1.4 2.2 1.8 1.7 2.3 2.0cardiac disease 1.4 1.7 1.7 0.7 0.6 0.6 1.1 1.3 1.2ulcer 1.2 0.9 0.9 0.6 0.2 0.4 1.0 0.6 0.8asthma 0.8 0.8 0.8 0.6 0.2 0.4 0.7 0.6 0.7epilepsy 0.3 0.2 0.2 0.4 0.1 0.3 0.3 0.2 0.3cancer 0.1 0.1 0.1 0.1 0.1 0.1 0.1 0.1 0.1
PCBS Health Survey 2000.
The percent of the population in the West Bank with hypertension is slightly higher than in the Gaza Strip. This is particularly true among females.
A similar observation can be made for diabetes. In both the West Bank and Gaza Strip, the percent of females with diabetes is higher than males.
Parasitic and skin infections are the leading causes of morbidity among children. Rates are particularly high in the Gaza Strip were conditions are overcrowded. Table 1.4 shows the rate of
4
Health Status
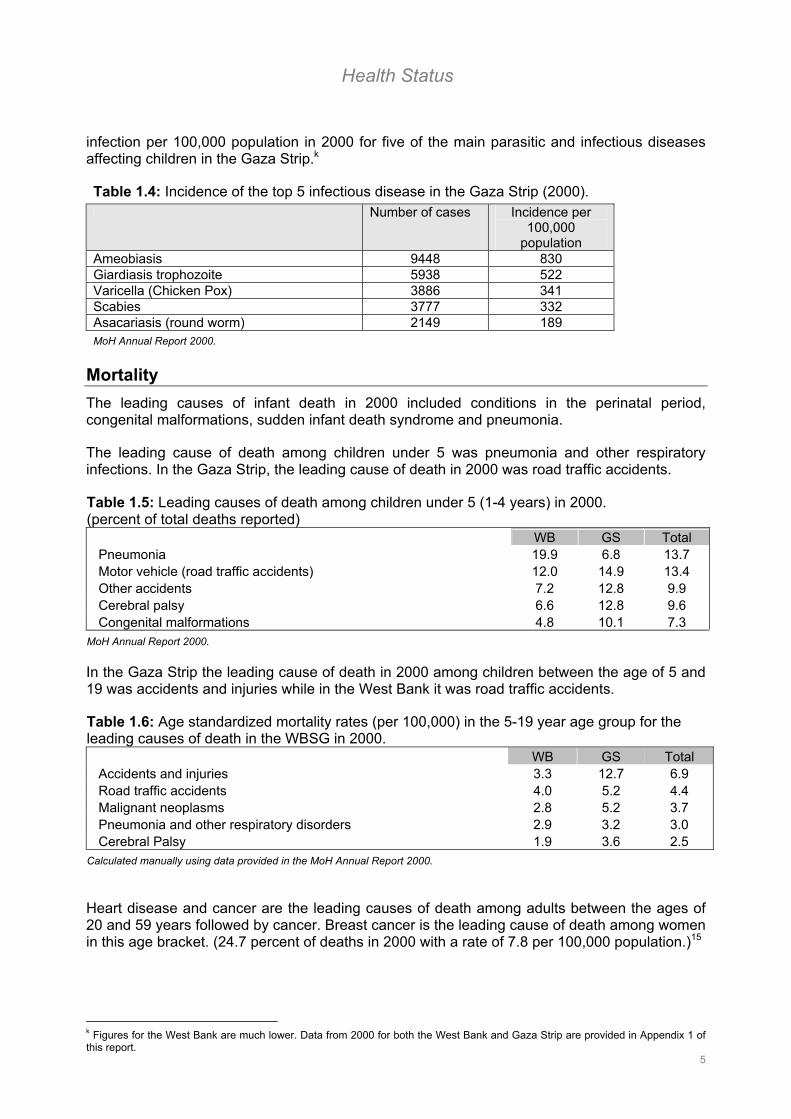
infection per 100,000 population in 2000 for five of the main parasitic and infectious diseases affecting children in the Gaza Strip.k
Table 1.4: Incidence of the top 5 infectious disease in the Gaza Strip (2000). Number of cases Incidence per
100,000 population
Ameobiasis 9448 830 Giardiasis trophozoite 5938 522 Varicella (Chicken Pox) 3886 341 Scabies 3777 332 Asacariasis (round worm) 2149 189 MoH Annual Report 2000.
Mortality The leading causes of infant death in 2000 included conditions in the perinatal period, congenital malformations, sudden infant death syndrome and pneumonia.
The leading cause of death among children under 5 was pneumonia and other respiratory infections. In the Gaza Strip, the leading cause of death in 2000 was road traffic accidents.
Table 1.5: Leading causes of death among children under 5 (1-4 years) in 2000. (percent of total deaths reported) WB GS Total
Pneumonia 19.9 6.8 13.7 Motor vehicle (road traffic accidents) 12.0 14.9 13.4 Other accidents 7.2 12.8 9.9 Cerebral palsy 6.6 12.8 9.6 Congenital malformations 4.8 10.1 7.3
MoH Annual Report 2000.
In the Gaza Strip the leading cause of death in 2000 among children between the age of 5 and 19 was accidents and injuries while in the West Bank it was road traffic accidents.
Table 1.6: Age standardized mortality rates (per 100,000) in the 5-19 year age group for the leading causes of death in the WBSG in 2000. WB GS Total
Accidents and injuries 3.3 12.7 6.9 Road traffic accidents 4.0 5.2 4.4 Malignant neoplasms 2.8 5.2 3.7 Pneumonia and other respiratory disorders 2.9 3.2 3.0 Cerebral Palsy 1.9 3.6 2.5
Calculated manually using data provided in the MoH Annual Report 2000.
Heart disease and cancer are the leading causes of death among adults between the ages of 20 and 59 years followed by cancer. Breast cancer is the leading cause of death among women in this age bracket. (24.7 percent of deaths in 2000 with a rate of 7.8 per 100,000 population.)15
5
k Figures for the West Bank are much lower. Data from 2000 for both the West Bank and Gaza Strip are provided in Appendix 1 of this report.

Health Status
Table 1.7: Age standardized mortality rates (per 100,000) in the 20-59 year age group for the leading causes of death in the WBSG in 2000 WB GS Total
Heart Disease 30.0 35.0 31.7 Malignant neoplasms 23.2 26.7 24.4 Accidents and Injuries 9.4 17.0 11.9 Cerebrovascular diseases 9.3 15.0 11.2 Hypertension disease 5.3 13.0 7.9
Calculated manually using data provided in the MoH Annual Report 2000.
Heart disease and cerebrovascular diseases are the leading causes of death among the elderly (aged 60 years and above). Age-specific mortality rates in this age group for heart diseases are considerably higher in the West Bank than in the Gaza Strip as shown in Table 1.8.
Table 1.8: Age standardized mortality rates (per 100,000) in the 60+ year age group for the leading causes of death in the WBSG in 2000 WB GS Total
Heart diseases 1059 614 922 Cerebrovascular diseases 438 743 532 Senility 467 395 445 Hypertension diseases 296 625 397 Malignant neoplasm 295 376 320
Calculated manually using data provided in the MoH Annual Report 2000.
Infectious disease profile Table 1.9 shows the rank of the top ten infectious diseases reported in the West Bank and Gaza Strip in 2000.
Table 1.9: Rank of top ten reported infectious diseases (2000).
The main infectious diseases reported in the West Bank were sexually transmitted diseases followed by hepatitis.
Chi
West Bank GazaAmeobiasis (trophozoite) 5 1Giardiasis trophozoite 10 2Sexually Transmitted Diseases 1 10
cken Pox (Varicella) 6 3Scabies 8 4Oxyuriasis 2 7Hepatitis B 4 8Asacariasis (round worm) 9 5Meningitis 7 6Hepatitis A 3 9
The main infectious diseases reported in the Gaza Strip in 2000 were intestinal parasites and skin diseases. A full list of the number of cases of each infectious disease reported is provided in Annex 1. MoH Annual Report, 2000.
Sexually Transmitted Diseases and HIV/AIDS: According to the MoH, the incidence of STDs and HIV/AIDS is increasing in the West Bank and Gaza Strip. At the same time, the STD surveillance system is thought to be unreliable. Donated blood is routinely tested for hepatitis B but HIV testing is only done for suspected cases. As a result, the exact number of HIV positive cases is not known.16 The MoH estimates that between 1986 and 2000 there were a total of 48 cases.
One of the main concerns expressed with respect to HIV/AIDs is the need for health education. Preliminary surveys and focus group discussions initiated by the MoH revealed that the majority
6
Health Status
of individuals at risk were at risk of infection because of a lack of understanding about how to protect themselves from infection. 17
Nutritional Status Few data are available on the current overall nutritional status of the population. Data from past surveys suggest that conditions related to chronic malnutrition are more prevalent than conditions resulting from acute malnutrition.
The following figures were obtained during a PCBS Health Survey conducted in 2000.18
• Height-for-age (Stunting, moderate to severe): 7.5% overall; 7.0% in the West Bank and 8.3% in the Gaza Strip
• Weight-for-height (Wasting – moderate to severe): 1.4% overall; 1.5% in the West Bank and 1.4% in the Gaza Strip.
• Weight-for-age: 2.5% overall; 2.6% in the West Bank and 2.4% in the Gaza Strip.
According to UNICEF, the general nutrition situation in the West Bank and Gaza Strip has improved since the mid 1990’s, however, micro-nutrient deficiencies remain a concern. 19 UNICEF and the MoH have plans to undertake a Rapid Nutritional Health Survey in the autumn of 2001.
Anaemia is one of the conditions most commonly observed. According the Nutritional Unit of the MoH, 50% of pregnant women were anaemic in 1999. The predominant form was iron deficiency (80 percent of cases) followed by folic acid and B12 (10 percent of cases).20 The prevalence of anaemia among refugee women of reproductive age in 2000 was 28 percent in the West Bank and 44 percent in the Gaza Strip.21 Anaemia among children under the age of three years was even higher at 49.7 and 74.9 percent respectively.22
WHO recommends that universal implementation of iron be introduced whenever the prevalence of iron deficiency among pregnant women, infants or pre-school children falls below 30 percent. 23 Diet, maternal anemia and a high prevalence of parasitic worm infection are thought to be contributing factors among children. 24
Iodine deficiency is also a concern in the West Bank and Gaza Strip. A UNICEF/MoH Survey conducted in 1999 revealed an overall goiter prevalence of 14.9%. Above average levels were observed in Jericho (68.2%) and the south West Bank (31.9%). 25
Obesity is also a growing problem and risk factor for diabetes and ischemic heart disease.26
Maternal and Child Health Primary health care facilities provide antenatal care which usually consists of testing blood pressure and anemia and the provision of tetanus toxoid vaccinations. These services are normally provided by PHC staff while high-risk cases are referred to hospitals or specialty clinics. According to the World Bank, 80 percent of pregnant women receive antenatal care at least once.27 PCBS estimates are higher at around 96 percent.28
Health seeking behavior for post-natal care is much lower. Although hospitals recommend between 8 and 48 hours of post partum admission, most women tend to discharge a few hours after delivery. Only 20 percent are estimated to receive postnatal check-ups. 29
Roughly 94 percent of all deliveries occur in health institutions and are attended by trained medical professionals in public and private hospitals.30 About 50 percent of home deliveries are attended by traditional birth attendants, relatives or friends. 31The majority of home deliveries occur in the West Bank (8.2%).32
An estimated 96 percent of babies are breastfed and seven percent are weaned within the first three months. 33
7
The Health System
1.3 Health care system
Public health system a) Health information Reliable data in key areas such as morbidity and mortality and other health status measures are lacking in the West Bank and Gaza Strip. According to the National Health Plan (NHP) for 1999-2003:
“The current health information system (HIS) is inadequate and lacks standard operations at both regional and national levels. Health information is not properly processed and health data have not been used for rational planning.”
Birth and death registration is incomplete and there are substantial variations in reporting depending on the source. Heath data is generally broken down by region (West Bank and Gaza Strip) but is not commonly stratified by age and sex.34
These reporting problems are in part due to the under-development of the health information system and a lack of resources; technical, human and financial. The World Bank, the British Council and USAID are working in this area to help develop and strengthen communication links between districts, improve referral systems, and computerize personnel records (human resource management). Efforts are also aimed at computerizing and linking the government health insurance system (GHI).
Some of the main development strategies for the HIS outlined in the NHP include:
- Centralization of data collection (development of a health data warehouse)
- Standardization of health indicators and definitions
- Enhancing communications networks
- Development of an advanced medical information network
- Linking health management information system (MIS) data with planning and policy making processes
There are currently 18 communicable and non-communicable diseases notified on a daily basis, 27 notified on a weekly basis and 27 on a monthly basis. A list of the main diseases notified is provided in Appendix 1.
Health data on morbidity and mortality flows from peripheral clinics to the District Health Directorate and then on to the Central Statistics Department of the MoH. Health data on morbidity and mortality reported at the hospital level is forwarded directly to the Central Statistics Department of the MoH.
In July 2000, the Palestinian Central Bureau for Statistics (PCBS) was designated the official source of government statistics in the General Statistics Law (no5).
8

The Health System
b) Communicable disease control There are three main approaches to communicable disease control in the West Bank and Gaza Strip: vaccination, vector control, and environmental control measures.
Vaccination coverage in the West Bank and Gaza Strip is high. Table 1.10 shows the percent coverage from the Expanded Programme on Immunization (EPI) from 1995 to 2000.
Table 1.10: EPI Vaccination coverage in the West Bank and Gaza Strip. 1995 1996 1997 1998 1999 2000 BCGl 91 95 89 92 91 92 DPT3 100 97 96 98 89 93 OPV3 96 97 96 98 89 93 HepB3 93 91 100 92 91 95 Measles .. .. .. 94 91 93 MMR 73 95 96 92 92 88 MoH of Israel, MoH of the West Bank and Gaza Strip, PCBS.
Vaccination activities are carried out at all PHC clinics and in schools with the support and collaboration of UNRWA, UNICEF, WHO and donor governments.
During the period October 2000 – August 2001 vaccination coverage was maintained in spite of tightened road closure. There was a slight decline in coverage from 98 to 91 percent during this period as compared with the previous year. The greatest decline occured among the refugee population (17%).35 The efficacy of the vaccination activities completed from October 2000 – August 2001 have yet to be determined. Although vaccination coverage was maintained for all antigens, some were not carried out within the time recommended. Delays of as long as two months occurred in some areas. Additional problems occurred with respect to maintenance of the cold chain because of prolonged travel times, electricity shortages and lack of refrigeration maintenance.36
Vector control, in the form of spraying, takes place during the summer months (May-Sept) to control against sand flies (for Leishmaniasis) and mosquitos (for West Nile Fever). Sand flies, the primary vector for Leishmaniasis – cuteaneous and visceral (Kala-Azar), are present mostly in the West Bank (Jenin, Jericho, Nablus and Al Khaleil). In the past years, the incidence of visceral leishmaniasis has remained relatively stable at around 0.72 cases per 100,000 population. The incidence of cutaneous leishmaniasis, the less severe of the two forms, has been higher peaking at 6.7 cases per 100,000 population in 1996 and dropping to 1.9 per 100,000 population in 1999.37
c) Environmental health Environmental control measures range from maintaining and sampling water quality, waste and wastewater management and control and food safety.
Nearly 96 percent of the population has access to safe drinking water. Slightly fewer households in rural areas in the West Bank have access to safe drinking water, but overall the percentage is still high as shown in Table 1.11.
Table 1.11: Percent of the population with access to safe drinking water in 2000. West Bank Gaza Strip Total Camp Rural Urban
Households connected to the public water supply 79.6 89.2 83.1 89.4 63.3 91.9
l According to a PCBS survey carried out in 1996, coverage for BCG in the WBGS was much lower. At that time only UNRWA provided the BCG vaccine and mostly in the Gaza Strip. According to this survey, BCG coverage in 1996 in the Palestinian territories was 43.2 % (21.6% in the West Bank and 90.5% in the Gaza Strip among children aged 11-23 months). The MoH introduced BCG into the regular vaccination programme in 1999. Therefore, figures for other years are MoH estimates from the 2000 Annual Report.
9

The Health System
% with access to safe drinking water 94.9 98.6 96.2 98 91.4 98.3 PCBS Health Survey 2000
The main sources of drinking water in addition to the public water supply system include piped wells (8.5%), tanker trucks (2.7%), outdoor pipes connected to the public water supply system (2.4%), wells (2.2%), springs (0.8%) and other (0.3%).38
Among those households in the West Bank piped wells (11.9%) and tanker trucks (3.8%) are the most common sources of drinking water. m
The municipalities, under the direction of the Ministry of Health and Palestinian Water Authority, are responsible for routine sampling and analysis of the water supply (including the public water supply system, wells, and springs.). One of the main concerns of the current crisis is the disruption of water control programmes. Drinking water sampling for the prevention of water borne diseases reportedly declined by 52% in the West Bank and 36% in the Gaza Strip between October 2000 and March 2001.
Most households in the West Bank particularly those in remote areas do not have access to adequate sewage and wastewater facilities. Many rely upon cesspools which are drained periodically by trucks from the municipalities.
Table 1.12: Percent of households with access to sewage facilities by locality and region in 1999.
West Bank Gaza Strip Total Camp Rural Urban public sewer 36.5 59.3 43.9 71.2 6.8 56.4 cesspool 62.4 40.6 55.4 28.2 92 43
PCBS Health Survey 2000
Eighty-six percent of the population in the West Bank obtains their water from a mountain aquifer. A coastal aquifer provides 96% of the water supply in the Gaza Strip.39 Leakage and inadequate treatment of wastewater are two significant concerns with respect to ground water quality. Untreated industrial waste is another. Currently, less than 5% of solid waste and less than 3% of liquid waste is treated in the West Bank and Gaza Strip. 40
Limited information is available about solid waste. In 1995, researchers estimated that 0.88 kg of solid waste was produced per person per day. Figures for the Gaza Strip are higher, at approximately 1.0 kg per person per day. Local authorities collect 69.5% of solid waste while the remainder is burned or disposed of in a dump.
Management of medical waste is weak. More than 80% of medical waste is disposed in uncontrolled sites. Registration of hazardous materials used in hospitals and pharmacies is incomplete and information about waste generation is unreliable.41
m The issue of water is one of the issues about which a final decision has yet to be taken. In the 1995 Israeli-Palestinian Interim Agreement on the West Bank and Gaza Strip, Israel was made responsible for water control and distribution during the interim period. This agreement provided that 28.6 million cubic meters (m3) be provided annually to the Palestinians for domestic use. Any increase was subject to usage of additional water resources. Future water requirements estimated in the Israeli-Palestinian Interim Agreement on the West Bank and Gaza Strip (Article 40) were between 70 – 80 m3. Currently Palestinians consume 112 cubic meters of water per capita per year in the West Bank and 105 m3 in the Gaza Strip. Non-agricultural consumption amounts to 70 liters per person per day. Source: Passia, 2000.
10

The Health System
Health care facilities There are four major health care providers operating in the West Bank and Gaza Strip, the Ministry of Health (MoH), UNRWA, NGOs and the private sector. Table 1.13 shows the areas and levels of services covered by each.
Table 1.13: Overview of services provided by the four main health sector providers in the West Bank and Gaza Strip.*
MoH UNRWA NGOs Private
PHC XXXX XXX X X
Secondary and general hospital care X -- X X
Tertiary and specialty care -- -- X XXX *The X’s correspond to main areas of service provision. West Bank and Gaza: Medium Term Development Strategies for the Health Sector, World Bank, 1998 a) Primary health care services The major providers of primary care services are the MoH and UNRWA. Table 1.14 shows the distribution of primary health care centers (PHCs) per region by health care provider.
Table 1.14: Distribution of PHC facilities by provider type (2000). Government UNRWA NGOs and private TOTAL
West Bank 316 34* 145 495 Gaza Strip 43 17* 40 100 Total 359 51 185 595
*From UNRWA as of June 2001. MoH Annual Report, 2000.
1) Government Clinics:
Primary care services are provided free of charge by Government clinics to individuals enrolled in the Government Health Insurance (GHI) scheme. Prior to October 2000, more than 52% of the population or approximately 1.6 million people were covered through GHI.42,n
Prenatal care, vaccinations and treatment for children under the age of 3 are provided free of charge to all people regardless of insurance status.43
There are four types/levels of Government PHCs:44
Level I: Health Posts serve a population of less than 1,000 and are typically staffed by a community health worker. Only preventative care services are provided at health posts (hygiene, sanitation, registration and reporting, Maternal and Child Health).
Level II: Health Clinics serve a population between 1,000 and 3,000. They are typically staffed by a nurse and are visited by a general physician (GP) once or twice weekly. The services provided include vaccination, environmental health management functions (water quality and waste monitoring, food safety), maternal and child health, and general medicine.
Level III: Health Centers serve a population between 3,000 and 10,000. There are usually 13 medical staff at this level, including a GP and nurse. Services provided in a Level III health center include those provided at Level II clinics as well as occasional specialty services and preventative dental care.
Level IV: At this level, facilities are considered Comprehensive Health Centers and serve a population of greater than 10,000. They are typically staffed by up to 30 people. In addition to the staff posted to Level III Health Centers, there are physiotherapists and
n For more information about the Government Health Insurance Scheme, please refer to Part 2.
11

The Health System
x-ray technicians. At this level, additional services provided include specialized consultations and emergency care.
In 1998, 64.5 percent of all government PHC facilities were Level II health clinics. The majority of Level I and Level II facilities were in the West Bank.45 This is consistent with the larger area of this region and with the lower population density in comparison to the Gaza Strip.
Outlined in the National Health Plan (1999-2003) were plans to build 14 more Level III facilities and 5 Level IV facilities in the West Bank by the year 2000. An additional 60 Level I & Level II clinics were also planned to be rehabilitated/renovated.
In addition to the PHCs, the MoH also operates 13 Mental Health and 31 Rehabilitation clinics.
2) UNRWA Clinics:
UNRWA provides primary care services free of charge to the refugee populations in the West Bank and Gaza Strip through primary clinics and health points at which a full range of preventative, curative and community health services is available. The same services are provided at health points but only on one day per week. Services for diabetes, hypertension, pediatric care, obstetrics, gynecology and cardiology, and laboratory and diagnostic services are available at all UNRWA health facilities. Dental services are available in 83% of the facilities in the Gaza Strip and 62% of those in the West Bank.46
3) NGO Clinics:
A number of NGOs operate primary health clinics in the West Bank and Gaza Strip. Services are provided to anyone upon payment of a nominal fee. The number of NGO clinics has increased and decreased over the past decade peaking during the first Intifada (210 in 1992) and declining in the mid 1990’s (128 in 1996).o
Both curative and preventative services are available depending on the operating organization. As of 1996, treatment for diabetes, gynecology, oncology and dermatology were available in 25 percent of NGO primary care facilities.47
4) Private Clinics:
A range of primary care services are available in the private sector. Reliable data on the current number of clinics operating in the West Bank and the Gaza Strip are not known. However, estimates in 1994 suggest that there were 164 private clinics operating in rural areas of the West Bank. In more heavily populated areas, private doctors tended to work from large health facilities providing more comprehensive services.48
Many physicians work part time in private practice while maintaining other positions in government, UNRWA and NGO facilities. The exact number of physicians working in both the public and private sector and the amount of time spent in each is not known.
A survey conducted in 1998 revealed that where possible, the majority of the population in the West Bank has sought primary health care treatment in private clinics. In the Gaza Strip, the majority of individuals tended to visit government and UNRWA facilities.
Table 1.15: Distribution of users of primary care clinics by service provider in 1998 (percent). Type of clinic West Bank Gaza Strip Government 19 33 NGO 14 7 UNRWA 8 31 Private 60 29
Health Insurance and Health Service Utilization in the West Bank and Gaza Strip, Lennock J and A Shubita, HDIP Policy Paper, February 1998.
o For more information about trends in the NGOs sector, please refer to Part 3 of this report.
12

The Health System
b) Secondary and general hospital services The MoH operates 17 hospitals in the West Bank and Gaza Strip with a total of 2622 beds. There is one psychiatric hospital in Bethlehem which has 320 beds.
NGOs are the second largest provider of secondary care services in the West Bank and Gaza Strip after the MoH. There are 25 non-governmental hospitals with a total of 1442 beds. This is nearly a third of the total beds available.49
Table 1.16: Total number of beds by health sector provider in 2000. West Bank Gaza Strip Total % of total beds
Government 1110 1512 2622 57.6 NGO 1098 344 1442 31.7 UNRWA 38 0 38 0.8 Private 413 40 453 9.9
MoH Annual Report 2000.
UNRWA operates one 38 general-bed hospital in Qalquiliya. Additional hospital care is provided either through contracting beds at NGO and private hospitals or through partial reimbursement of costs incurred by refugees.
There are 1.01 general and 0.30 specialty beds per 1,000 population. The total number of beds per 1,000 pop is 1.45 and varies slightly between the West Bank (1.32) and Gaza Strip (1.67). Table 1.17 provides an overview of the distribution and types of beds available.
Table 1.17: Distribution and types of beds available in the West Bank and Gaza Strip in 2000. General Specialty Maternity Rehabilitation Total West Bank 1695 584 291 89 2659
Beds per 1,000 pop 0.84 0.29 0.14 0.04 1.32 Gaza Strip 1487 363 15 31 1896
Beds per 1,000 pop 1.31 0.32 0.01 0.03 1.67 Total 3182 947 306 120 4555
Beds per 1,000 pop 1.01 0.30 0.10 0.04 1.45 MoH Annual Report 2000.
Regionally, there are some disparities in the availability of beds per population particularly in the West Bank. Hospital services are concentrated in urban settings in the central areas of the West Bank. In these parts the ratio of beds per pop reaches 1.4 beds per population while in the north and south this ratio falls to 0.8 and 1.2 beds per population respectively.50
Table 1.18 shows the utilization of hospitals in the West Bank and Gaza Strip by health sector provider in 1999. The largest providers of hospital care (all levels) are the MoH and NGOs. The average length of stay (LOS) in NGO hospitals is considerably longer than in all other hospitals. The low levels of utilization of the private sector hospitals might suggest that costs are prohibitive. Many facilities are unlikely to be able to sustain running costs at less than 50% percent occupancy rates which in turn might drive up individual user charges.
Table 1.18: Hospital utilization by provider type in 1999.
MoH NGO Private UNRWA Total
Total # of inpatient days 479,215 288,885 65,797 9,765 860,460
Average length of stay (days) 2.7 16.6 1.9 3.5 6.2
Percent occupancy rate 80% 68% 46% 84% 68% *Figures for MoH from the Annual Report, 1999. The Palestinian Health System: An Updated Overview. HDIP, March 2000.
13

The Health System
c) Tertiary and specialty care: One of the only tertiary level care hospitals for Palestinians is the NGO Al Makassed Hospital in Jerusalem. It is the main referral hospital in the West Bank and serves over 60% of population.51 Some specialty care services, e.g. cardiovascular surgery, open heart surgery and neurosurgery, are provided in MoH hospitals in Ramallah and the Shifa Hospital in Gaza City
However, the private sector is the primary provider of tertiary care services, especially advanced diagnostics. Typically the MoH and UNRWA contract out tertiary care services not available in their own facilities, e.g. cancer treatment and complicated cardiac surgical needs. In some cases patients are referred outside of the Palestinian territories for treatment.
Referrals abroad are a considerable financial burden to the MoH. In 2000, more than 6 million USD (6.5% of the total MoH budget) was spent on referrals to Jordan, Egypt, Israel or the private sector. The MoH has subsequently encouraged the development of the private sector in the West Bank and Gaza Strip. Overall, financial and opportunity costs should be lower than those involved in transfer of patients abroad.52
Two of the largest private sector medical companies are Arabcare Medical Services and Medlab Palestine. Each invests (1996) roughly 14 million USD in the provision of advanced diagnostics and specialty care services.53
The main provider of EMS and ambulatory services is the Palestinian Red Crescent Society (PRCS). The PRCS has 20 emergency centers – 14 in the West Bank and 6 in the Gaza Strip. There are a total of 78 ambulances in the fleet manned by 270 staff.
Twenty-four hospitals in the West Bank and Gaza Strip also have ambulatory services.
14
The Health System
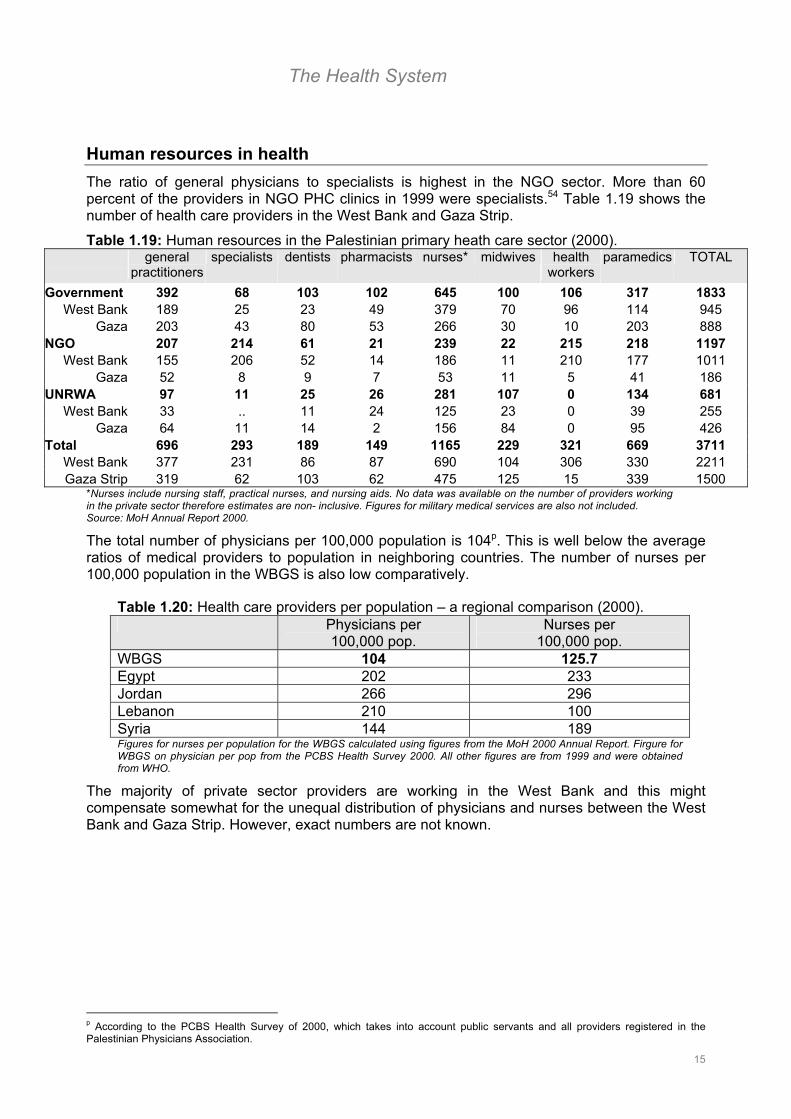
Human resources in health The ratio of general physicians to specialists is highest in the NGO sector. More than 60 percent of the providers in NGO PHC clinics in 1999 were specialists.54 Table 1.19 shows the number of health care providers in the West Bank and Gaza Strip.
Table 1.19: Human resources in the Palestinian primary heath care sector (2000).
general
practitioners specialists dentists pharmacists nurses* midwives health
workers paramedics TOTAL
Government 392 68 103 102 645 100 106 317 1833 West Bank 189 25 23 49 379 70 96 114 945
Gaza 203 43 80 53 266 30 10 203 888 NGO 207 214 61 21 239 22 215 218 1197
West Bank 155 206 52 14 186 11 210 177 1011 Gaza 52 8 9 7 53 11 5 41 186
UNRWA 97 11 25 26 281 107 0 134 681 West Bank 33 .. 11 24 125 23 0 39 255
Gaza 64 11 14 2 156 84 0 95 426 Total 696 293 189 149 1165 229 321 669 3711
West Bank 377 231 86 87 690 104 306 330 2211 Gaza Strip 319 62 103 62 475 125 15 339 1500
*Nurses include nursing staff, practical nurses, and nursing aids. No data was available on the number of providers working in the private sector therefore estimates are non- inclusive. Figures for military medical services are also not included. Source: MoH Annual Report 2000. The total number of physicians per 100,000 population is 104p. This is well below the average ratios of medical providers to population in neighboring countries. The number of nurses per 100,000 population in the WBGS is also low comparatively.
Table 1.20: Health care providers per population – a regional comparison (2000). Physicians per
100,000 pop. Nurses per
100,000 pop. WBGS 104 125.7 Egypt 202 233 Jordan 266 296 Lebanon 210 100 Syria 144 189 Figures for nurses per population for the WBGS calculated using figures from the MoH 2000 Annual Report. Firgure for WBGS on physician per pop from the PCBS Health Survey 2000. All other figures are from 1999 and were obtained from WHO.
The majority of private sector providers are working in the West Bank and this might compensate somewhat for the unequal distribution of physicians and nurses between the West Bank and Gaza Strip. However, exact numbers are not known.
p According to the PCBS Health Survey of 2000, which takes into account public servants and all providers registered in the Palestinian Physicians Association.
15

The Health System
Health finances Total Government expenditures in health in 2000 amounted to 95.7 million USD. Per capita government expenditure on health was 30 USD.q This is lower than per capita expenditures in Egypt (48 USD), Syria (90 USD) and Jordan (123 USD). Per capita expenditure in health in Israel was 1609 USD.r
Figure 1.3: MoH expenditures on health in 2000.
The largest proportion of MoH spending in 2000 went to cover salaries followed by operating costs and pharmaceuticals.
There are three primary sources of revenue for the MoH: 1) Regular budget allocated by the PA through the Ministry of Finance (MoF) (60%); 2) revenues from government health insurance (GHI) premiums (25-30%); and 3) co-payments (10-30%). All GHI revenues are collected by the MoH and transferred to the MoF who then allocate an annual budget.55
Total MoH expenditures = 95.7 million USD
Salaries48%
Drugs and consumables
21%
Operating costs25%
Referral Abroad
6%
MoH Annual Report, 2000.
UNRWA’s activities are funded entirely through voluntary donations. In 1999, UNRWA health expenditures amounted to roughly 20 million USD. Per capita spending was 21.6 USD in the West Bank and 20.7 USD in the Gaza Strip.56
Funding for NGO activities is provided largely by foreign NGOs and donors. NGO expenditures on health in 1997 were between 20-30 million USD. Expenditures in the private sector amounted to around 105 million USD. 57
Donor disbursements in the health sector between 1994 and December 2000 amounted to 266 million USD.s Per year, this amounted to an average of nearly 44.3 million USD. Figure 1.4 compares MoH expenditures per capita with the overall health assistance per capita (disbursed). Aid to the health sector has fluctuated while overall government spending per capita has remained relatively stable in the past four years.
Figure 1.4: Donor and government expenditures per capita (1996 – 2000).
12.8
8.7
11.5
8.7
33.8
30.2
29.0
30.4
1997
1998
1999
2000
health aid per capita (USD) govt expenditures per capita (USD)
19.1 42.7
0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0
1996
MoH Annual Reports, MOPIC Quarterly Monitoring Report, December 31, 2000.
q Calculated based on the total MoH expenditure for that year divided by the total population for that year. r These figures obtained from the World Health Organization and are for 1999. Figures from 2000 were not available. Per capita health spending in the West Bank and Gaza Strip in 1999 was 29 USD. s For more information about international aid coming into the health sector, please refer to Part 3.
16

The Health System
Health policy and planning The first Palestinian body responsible for health decision-making, the Palestine Council on Health, was established in 1992. In 1994, this council in collaboration with the Planning and Research Center developed the first National Health Plan (NHP) for the West Bank and Gaza Strip.
In 1994, the nascent Ministry of Health assumed responsibility of the health sector (the Gaza Strip in May and the West Bank in November). Five years later, the second NHP for the West Bank and Gaza Strip for the period 1999-2003 was published. The second plan has been considered an ambitious attempt to set an agenda for change, although there is concern about the amount of resources required to implement the proposed activities and to coordinate and manage implementation.58 This is particularly true with respect to ensuring that priorities and activities planned match operational capacities.
a) Management structure The MoH is the primary provider and regulator of the health sector. Due to the geographical layout of the Palestinian territories, a number of functions have been duplicated largely because of the need to set up parallel structures in the WB and GS.
Figure 1.5: Organizational structure of the Palestinian MoH.
Ministry Director General
Deputy Minister
Minister of Health
Director General’s Office
EmergencyHospitals Primary Health Care
PharmaceuticalsRes., Planning & Development
Financial & Administrative Affairs
Ministry DG/West Bank Ministry DG/Gaza
Purchase Department Dental Department Treatment Abroad Department Nursing Department Physiotherapy Department Lab & Blood Bank
Health Insurance Department General Inspection Department Private Medicine Department Quality Improvement Department Health Education Department Coordination with Rehab Centers Dept Coordination with NGOs Department
Deputy Minister’s Office
Public Relations Department International Cooperation Dept. Legal Advisor Abroad Palestinian’s Health Dept.Women’s Health Department Child Health Department
Minister’s Office
Planning and Policy Making Council
Deputy Minister Director General
17
The Health System
Overall policy decisions are made by the Minister and his Deputy. District managers input and influence health policy at the regional level.
b) Regulation & legislation The legacy of health care provision in the West Bank and Gaza Strip has left the current legislation with a mixture of policies. Prior to 1967, the Gaza Strip was administered by Egypt, the West Bank formed part of Jordan, and parts of the West Bank and Gaza Strip were administered by the Israeli Civil Administration. Current legislation is not unified between the West Bank and Gaza Strip.
A comprehensive law on health insurance has yet to be developed.
c) Licensing and Quality Assurance Physicians in the West Bank are licensed through a joint agreement between the Jordanian Medical Association and the MoH. In the Gaza Strip physicians are licensed through a similar agreement between the MoH and the Arab Medical Association. Some progress was made in terms of establishing licensing legislation, however implementation has been slow due to a lack of capacity for quality control and inspection. 59 Little has been done in terms of monitoring and quality control because of a lack of resources and provider utilization data.
Pharmaceutical sector Overall availability of drugs in the West Bank and Gaza Strip is satisfactory although fluctuations in stock have been observed during periods of socio-economic and political instability.
According to a WHO survey published in 2000, too many drugs (more than 4,000) are available in the domestic market. Local institutions use only 720 of available drugs. 725 are produced locally and the rest are from neighboring countries and the Israeli market.
Drugs are exceptionally expensive. Israeli restrictions on the pharmaceutical market have limited potential for competition to reduce prices. Additional factors pushing up the price of medicines include high level of patient demand for drugs, especially antibiotics, irrational drug use and over prescription, and high use of brand name drugs. Public sector providers are largely unaware of the costs of the drugs they prescribe and there is little to no generic drug substitution.
As a consequence of the high cost, the proportion of the MoH budget spent annually on drugs and consumables is considerable. In 2000, 21% of the MoH budget (20 million USD) was spent on drugs and consumables. This is less than in previous years. In 1999 the proportion spent was 30.2% or 26.4 million USD and in 1998 it was 29% or 25.4 million USD.60
There is a need for a drug monitoring system because there is little sense of costs and utilization patterns. The MoH budget on Pharmaceuticals is derived from the previous year’s expenditures plus a 10% increase.
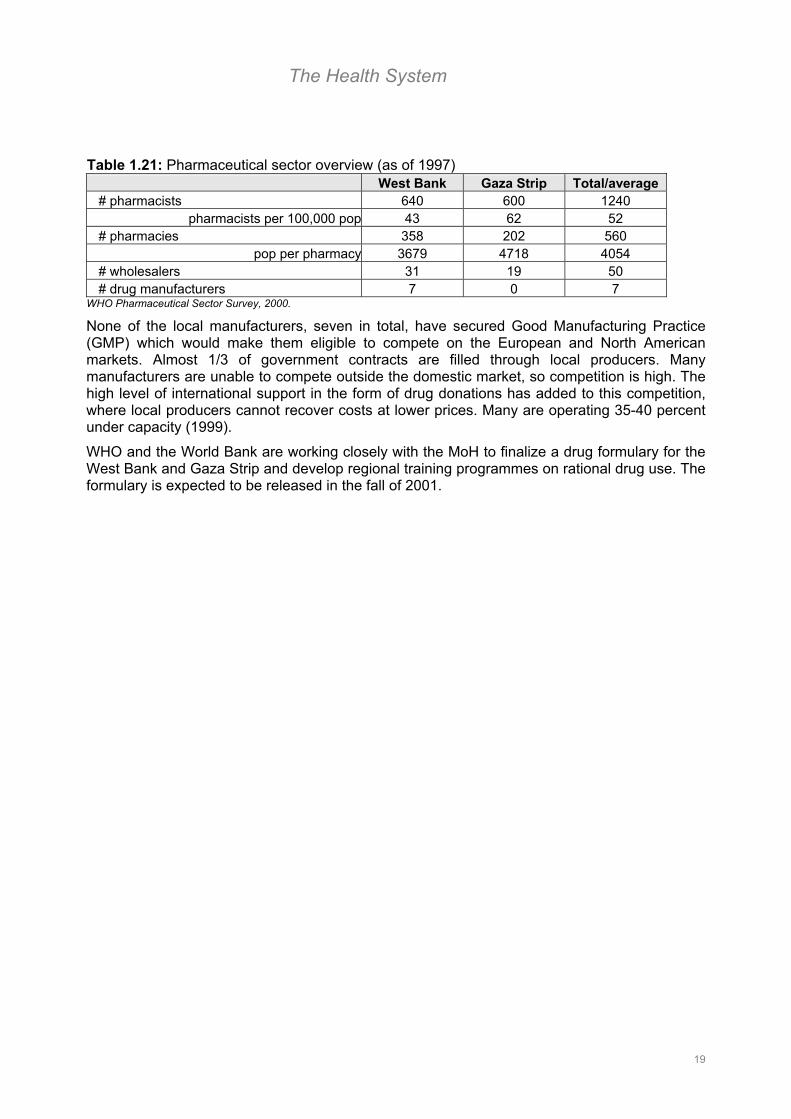
Pharmaceutical policies are inadequate and do not cover different aspects of pharmacy. There are no policies which match the number of pharmacists to the population they serve.61 The population to pharmacist ratio is also high as shown in Table 1.21.
18
The Health System
Table 1.21: Pharmaceutical sector overview (as of 1997) West Bank Gaza Strip Total/average
# pharmacists 640 600 1240 pharmacists per 100,000 pop 43 62 52
# pharmacies 358 202 560 pop per pharmacy 3679 4718 4054
# wholesalers 31 19 50 # drug manufacturers 7 0 7
WHO Pharmaceutical Sector Survey, 2000.
None of the local manufacturers, seven in total, have secured Good Manufacturing Practice (GMP) which would make them eligible to compete on the European and North American markets. Almost 1/3 of government contracts are filled through local producers. Many manufacturers are unable to compete outside the domestic market, so competition is high. The high level of international support in the form of drug donations has added to this competition, where local producers cannot recover costs at lower prices. Many are operating 35-40 percent under capacity (1999).
WHO and the World Bank are working closely with the MoH to finalize a drug formulary for the West Bank and Gaza Strip and develop regional training programmes on rational drug use. The formulary is expected to be released in the fall of 2001.
19
The Health System
1 MoH Annual Report, 2000. 2 UNRWA. As of March 2001. 3 MoH Annual Report 2000. 4 IBID, 2000. 5 IBID, 2000; The Palestinian Health System: An updated Overview, HDIP, March 2000. 6 Manually calculated using population data from the PCBS Health Survey, 2000. 7 MoH Annual Report 2000. 8 IBID, 2000. 9 PCBS Census 1997; MoH Annual Report 1999. 10 MAS Social Monitor Issue No. 3, 1999. 11 Verbal estimates from UNRWA, August 2001. 12 PCBS Health Survey 2000. 13 IBID, 2000. 14 The Situation Analysis of Palestinian Children, Young People and Women in the West Bank and Gaza Strip, UNICEF, August 2000. 15 MoH Annual Report 2000. 16 West Bank and Gaza: Medium-term development strategy for the health sector, World Bank, 1998 17 MOH National Health Plan, 1999-2003. 18 PCBS Health Survey 2000; The Situation Analysis of Palestinian Children, Young People and Women in the West Bank and Gaza Strip, UNICEF, August 2000. 19 The Situation Analysis of Palestinian Children, Young People and Women in the West Bank and Gaza Strip, UNICEF, August 2000. 20 WHO and MoH Estimates. 21 MoH Annual Report 2000. 22 UNRWA Annual Report of the Department of Health, 1999. 23 The Situation Analysis of Palestinian Children, Young People and Women in the West Bank and Gaza Strip, UNICEF, August 2000. 24 WHO and MoH Estimates. 25 The Situation Analysis of Palestinian Children, Young People and Women in the West Bank and Gaza Strip, UNICEF, August 2000. 26 WHO and MoH Estimates. 27 West Bank and Gaza: Medium-term development strategy for the health sector, World Bank, 1998 28 MoH Annual Report 2000. 29 West Bank and Gaza: Medium-term development strategy for the health sector, World Bank, 1998 30 IBID, 1998. 31 IBID, 1998. 32 IBID, 1998. 33 IBID, 1998. 34 The Situation Analysis of Palestinian Children, Young People and Women in the West Bank & Gaza Strip, UNICEF, August 2000. 35 Verbal estimates from UNRWA, August 2001. 36 Unpublished MoH/WHO Health Impact Assessment, October 2001. 37 MoH Annual Report, 1999. 38 PCBS Health Survey 2000. 39 Thirsty for a Solution, B’Tselem, July 2000. 40 IBID, July 2000. 41 MoH Annual Report, 1999. 42 Personal communication from the MoH Office for Health Insurance in the West Bank. 43 MoH Annual Report, 1999. 44 The Planning and Research Center 1994. The National Health Plan for the Palestinian People. 45 National Strategic Health Plan 1999-2003. 46 Health in Palestine: Potential and Challenges, MAS/HDIP, March 1997. 47 IBID, 1997. 48 Health Insurance and Health Service Utilization in the West Bank and Gaza Strip, Lennock J and A Shubita, HDIP Poliy Paper, February 1998. 49 MoH Annual Report 1999. 50 The Palestinian Health System: An Updated Overview, HDIP, March 2000 51 Health in Palestine: Potential and Challenges, MAS/HDIP, March 1997. 52 IBID, March 1997. 53 IBID, March 1997. 54 MOH Annual Report 2000. 55 “Health Sector Strategy Paper for the West Bank and Gaza”, DfiD Health Mission, May 1999. 56 UNRWA Annual Report from the Department of Health, 1999. 57 The Palestinian Health System: An Updated Overview, HDIP, March 2000. 58 Health Sector Strategy Paper for the West Bank and Gaza, DfiD Health Mission, May 1999. 59 IBID, May 1999. 60 MoH Annual Report, 2000. 61 WHO Pharmaceutical Sector Survey, 2000.
20
Vulnerability
Part 2: Vulnerability and linkages between health and the current context Part 2 examines some of the relationships (explicit and implicit) between changes in the broader socio-economic and political context and the health care needs of the population. As a consequence, who and what are emerging health sector concerns?
2.1 Who are the vulnerable?
Social cases: As of October 2001, the Ministry of Social Welfare reported that there were approximately 61,000 social cases in the West Bank and 64,000 in the Gaza Strip.
There are two types of social cases, hardship cases and special hardship cases. Hardship cases include widows, orphans, the elderly, mentally and physically disabled, prisoners, students and the poor. Special hardship cases include individuals who are in need to assistance since October 2000. Typically special hardship cases are individuals that have suffered loss of job, income and/or shelter.
UNRWA reported that the number of special hardship cases among refugees in March 2001 was 103,050.
Disabled: Prior to October 2000, almost two percent of the population (roughly 63,000 individuals) had a permanent disability. An estimated 3000 Palestinians injured between October 2000 and April 2001 will suffer some form of permanent disability. The Ministry of Health estimated that 437 of those injured were children. Disabilities range from the loss of an eye or a limb to complete paralysis.1
The disabled are not able to access 98% of public facilities.2
Chronically ill: Drug shortages due to the high costs and the inability of the MoH to maintain current high levels of spendinga and the limited availability of specialized health care the WBGS has meant that care for the chronically ill has become increasingly inaccessible. Two particular areas of concern include cancer patients and heomodialysis patients.
a) Cancer patients: Cancer is the second leading cause of death in the West Bank and Gaza Strip. An estimated 600 individuals are diagnosed with cancer each year. Roughly 2/3 of these individuals die within the first year of diagnosis. Fifty percent of the remaining cancer patients are treated with chemotherapy, 20% with radiotherapy, and 30% with both chemotherapy and radiotherapy. There are currently 3474 registered cancer patients in the West Bank and Gaza Stripb The incidence of cancer is higher in the WB than in the GS at 71 per 100,000 and 61 per 100,000 population respectively.
There are no radiotherapy facilities in the West Bank and Gaza Strip and most cancer patients are referred to Israeli or neighboring country hospitals for treatment. As of August 2001, 150 cancer patients from the West Bank were referred for treatment abroad at a rate of 25 patients per month.
During the period October 2000 to August 2001, emergency supplies of essential drugs used for chemotherapy were been depleted by 15%.
a See Part 1 for an overview of the pharmaceutical situation. b According to MoH estimates.
21
Vulnerability
b) Dialysis Patients: Dialysis services in the Gaza Strip are provided in three hospitals - one in Gaza City (Shifa), the Middle Zone and Khan Younis. There is only one pediatric dialysis unit located in Gaza City. There are currently 148 dialysis patients in the Gaza Strip and 184 in the West Bank who require treatment at least twice weekly. More than half of these individuals live outside the locality in which their center is located. Therefore, accessing these facilities during periods of tightened road closure has become increasingly problematic.
Mentally ill: According to the Ministry of Health, there were 40,000 mentally ill individuals in the West Bank and Gaza Strip in 2000.
The precise impact of the recent crisis on the mental health of the population is not known. However, the MoH and WHO have reported an increase in attendance at mental health clinics and increased contacts with community health workers when comparing patterns observed from October 2000 – March 2001 with the same period of the previous year. The Community Mental Health Department of the MoH also reported a 105% increase in the number of new cases registered at mental health clinics in the West Bank and Gaza Strip. Counseling activities increased by an average of 72.2% in the West Bank.
The majority of cases reported in both the West Bank and Gaza Strip were children under the age of 18. Most of the cases reported were preschool aged children. Psychotic syndromes, neurosis, and mental distress were among the list of conditions cited.
Refugees: As of March 2001, there were approximately 1.4 million registered refugees in the West Bank and Gaza Strip. Forty-five percent live in the West Bank and 55.5% in the Gaza Strip.
Forty six percent of the refugees live in camps. Out of those living in camps, 26.0 percent live in the 19 camps in the West Bank and 74.0 percent live in the eight camps in the Gaza Strip.3
The average refugee family size in the West Bank is 4.53 persons and 4.76 persons in the Gaza Strip. 4 In 1999, 32.3% of the population in the West Bank and 43.6% in the Gaza Strip were under the age of 15.5 In March 2001, 12% of the refugee population in the Gaza Strip and 6% in the West Bank was under the age of three.6
Internally displaced: A number of families have been forced to move because of the conflict. Either their homes have been destroyed or they have been forced to move for economic and/or security reasons.
According to the Al-Mezan Center for Human rights, approximately 370 houses in the Gaza Strip and 202 houses in the West Bank were destroyed or partially destroyed from September to December 2000.7
Urban/ rural: As of the 1997 census, 54% of the population in the West Bank and Gaza Strip live in rural areas. A higher proportion of West Bankers live in rural areas, and are, therefore, more likely to be affected by road closures.
Road closures have resulted in the virtual isolation of some remote areas of the Gaza Strip and the West Bank. This has created pockets of vulnerability in areas such as Shoka, Mawasy, Mograga, Joher Al Deek, Rashayadeh, and Ramadeen where movement of supplies and health professionals is extremely limited. According to the MoH, roughly 40,000 people live in these pockets of vulnerability, many of which are Bedouin villages and camps.
22

Vulnerability
Poor: The World Bank estimated that nearly 23.2% of the population in the WBGS lived below the poverty line in 1998.c The percent of the population living below the poverty line in the Gaza Strip (37.2) was more than twice as high as the percent in the West Bank (15.4).8
As of March 2001, the World Bank estimated that 64.2% of the population (more than 2 million people) was living below the poverty line. Again the percent in the Gaza Strip (81.4) was considerably higher than in the West Bank (55.7). This increase is almost 40% higher than poverty levels observed in 1998.9
A key determinant of poverty among the Palestinians is the employment status of the head of household.10
Unemployed: From 1998 until the beginning of the recent crisis (October 2000) unemployment levels were declining and averaged around 13%. Between the third and fourth quarter of 2000, unemployment rates doubled as shown in Figure 2.1.
This dramatic increase in unemployment is attributed to the loss of jobs in Israel which is estimated to have affected some 130,000 individuals.
0
5
10
15
20
25
30
Q11999
Q21999
Q31999
Q41999
Q12000
Q22000
Q32000
Q42000
Q12001
unem
ploy
men
t rat
e
Source: Palestinian Central Bureau for Statistics (PCBS)
Figure 2.1: Unemployment rates from the first quarter of 1999 until the first quarter of 2001.
By the first quarter of 2001, unemployment rates were estimated at around 26.9%. This figure exceeded the highest unemployment rates observed during the first Intifada, which peaked at 23.8% in 1996.11 Due to the high dependency ratiod in the West Bank and Gaza Strip (101.9 in 2000), unemployment directly affects almost 29% of the entire population or almost 1 million individuals. 12
Children (under 18 years old): Almost 55 percent of the population in the West Bank and Gaza Strip is under the age of 18.e
Research carried out on the psychological effects of violence on children in the WBGS, particularly those suffering permanent disabilities, has not yet been conclusive. 13 However, it is assumed that long-term exposure to low intensity violence will impact their well-being.
Findings from a recent PCBS survey (July 2001) illustrated some of the current psychological conditions reported among children aged 5 -17 years as shown in Table 2.1.
23
c The poverty line in 1998 was estimated at NIS 1,460 per month for a household of 2 adults and 4 children. d Please see Part 1 of this report for a definition of the dependency ratio. e Please see annex 1 for age/sex histogrames for 1999.

Vulnerability
Table 2.1: Psychological conditions reported among children (5-17 years) during the period October 2000 – July 2001.
Condition cited % of children surveyed
Crying attacks 43.6 Fear of loneliness 53.1 Fear of darkness 55.4 Fear of blood color 41.3 Feelings of hopelessness & frustration 33.6 Anger and nervous breakdown 22.4 Pre-occupation with death 27.6
Source: PCBS Survey: Impact of the Israeli Measures on the Well-being of Palestinian Children, Women and Households, 2001.
Figure 2.2: School enrollment rates by sex and age in the West Bank and Gaza Strip in 2000.
Factors likely to enhance the preoccupation of children with violence and the uncertainty of the socio-economic and political context include a lack of activity for leisure and entertainment and a lack of school.
In the past 12 months, many children were unable to attend school due to the crisis. An estimated 60% of students surveyed were absent from school during period October 2001 to June 2000 for at least 1 day with a median of ten days.14
In general, school enrollment by age declines rapidly from the age of 12 onwards as shown in Figure
2.2. Many of these children are thought to enter the labor force. In 2000, approximately 19.6% of children between the ages of 5 and 17 reportedly worked 4 hours or more per day. Most of these children worked in the agricultural sector and in family enterprises.15
0
20
40
60
80
100
120
6-11 12-14 15-17 18+
age
perc
ent
Male
Female
Source: PCBS Health Survey, 2000.
According to the ILO, a coping strategy of the recent economic crisis has been to send children under the age of 18 into Israel for “causal work” to help contribute to family income. Children cannot be punished for crossing the “Green Line” between Israel and the West Bank and are therefore able to move more freely.16
Criminal activity by minors may also be a sign of the strain of the instability of the current socio-economic and political environment. There were 1404 juvenile offenders in 1999. More than 55 percent were between the age of 16-18 years, and 34.7 percent between 13-15. Only 2.5 percent of all juvenile offenders were female. The main offences reported were assault and property damage. 17
24

Vulnerability
2.2 What are the root causes of vulnerability?
Vulnerability in health is inextricably linked to its broader socio-economic and political context. Traditional approaches to vulnerability tend to focus on the identification of the essential needs of the most vulnerable. While this needs-based approach allows for the rapid determination of priority relief interventions, it does not provide insight as to why people are vulnerable. In order to understand how and why people are vulnerable, it is necessary to look at the “root-causes” of vulnerability.
The roots of vulnerability in health in the West Bank and Gaza Strip can be identified on two levels, household and institutional. Household vulnerability is reflected in the ability of households to maintain their own health and is determined by access and availability of health care services. Institutional vulnerability is reflected in the ability of the health care system to meet the health care needs of its constituents. Key determinants in this regard include capacity and systemic factors.
Following is a matrix that outlines some of the key factors influencing vulnerability. The factors are grouped into two main categories: contextual and systemic.
Table 2.2: The vulnerability matrix. Factor Impacts on institutional vulnerability Impacts on household vulnerability Direct Indirect Direct Indirect Contextual: a) Closure ↓ service delivery ↑ operating costs ↓ access to
services ↓ access to income and subsequent ↓ in purchasing power
b) Economic decline
↓ Health care finances
↑ budget deficit; potential shift of burden of costs to patients
↓ income and savings and purchasing power
↓ access to health care because of cost
↑ risk to health professionals;
↓ service delivery
↑ and change in nature of demand for services (e.g. more EMS)
↑ operating costs
Risk of ↑ morbidity and mortality
↓ access to income and subsequent ↓ in purchasing power
c) Conflict and threat of violence
Potential for damage to infrastructure
↑ reconstruction costs, ↓ service delivery
Risk of damage of homes and infrastructure
Population displacement, loss of essential services (e.g. water); ↑ morbidity & mortality
Systemic: a) Weakness in capacity
↑ strain on resources (human, material, financial, technological)
↓ Access, availability and quality of services
b) Parallel systems in the WB and Gaza Strip
↓ operational efficiency and ↑ running costs
↓ Access and availability of health care
c) Multiple service providers
↑ Risk of poor coverage; ↓ efficiency, and ↑ challenge of coordination and regulation
↓ Quality and equity of services
25
Vulnerability
Contextual factors are factors inherent in the overall socio-economic and political environment, which directly and indirectly influence health status and health care delivery. Systemic factors are factors inherent in the health care system that influence its operational capacity and subsequently the quality and accessibility of medical care. International aid is an additional component affecting vulnerability and will be addressed separately in Part 3.
Contextual Factors
a) Closure The most significant aspect of the current socio-economic and political context impacting household and institutional vulnerability is border and road closure. The main issue connected with closure has been the issue of access both in terms of the population being able to obtain health care and in terms of the ability of health sector providers to maintain coverage.
During the last quarter of 2000, UNSCO estimated that the Palestinian border with Israel was closed for 72 out of 92 days. “Severe” internal closures were in effect for 52 days in the West Bank and 14 days in the Gaza Strip. “Partial” internal closure was in effect for 40 days in the West Bank and 75 days in the Gaza Strip.18
As of August 2001, there were approximately 174 checkpoints through out the West Bank and Gaza Strip. Many were introduced over time (1993 and onwards). However, given the escalation of fighting in October 2000, these checkpoints were been tightened.
Primary impacts of closure on household vulnerability have been a reduced access to health care and reduction in purchasing power due to reduced access to income. (Purchasing power and factors influencing household income are discussed in the next section.)
A large portion of the population, especially those living in remote areas, experienced moderate to serious difficulty accessing health care facilities. A recent PCBS survey (July 2001) found that 23% of households reported that the main barrier to accessing health care was the inability to reach points of service.
Closure is also limiting the ability of health care providers to reach patients. In the West Bank, many health professionals were not able to reach their place of work during periods of road closure from October 2000 – March 2001. 19 This was particularly true for physicians traveling to primary health care centers many of whom do not reside in the communities in which they work.
An operational consequence of closure has been a decline in utilization rates for some specialty care facilities (e.g. Jerusalem). This in turn as resulted in a significant decline in revenue for health care facilities struggling to cover their operating costs.20
External border closures have resulted in problems with patient referrals to tertiary care facilities outside of the West Bank and Gaza Strip.
b) Economic factors
• Factors influencing household income and relative purchasing power:
Economic factors are directly linked to and influenced by the overall context and determine the significance of cost as a barrier to health care. In order to fully gauge the significance of this barrier, it is necessary to look at the purchasing power and factors influencing average household income. The following discussion will focus on factors influencing household income during period after the conflict escalated in October 2000. Although the economic situation is becoming acute, it is important to bear in mind that the economic crisis has been exacerbated, not caused by, the result of the recent escalation of the Israeli/Palestinian conflict.
Table 2.3 provides an overview of the economic indicators influencing household income.
26
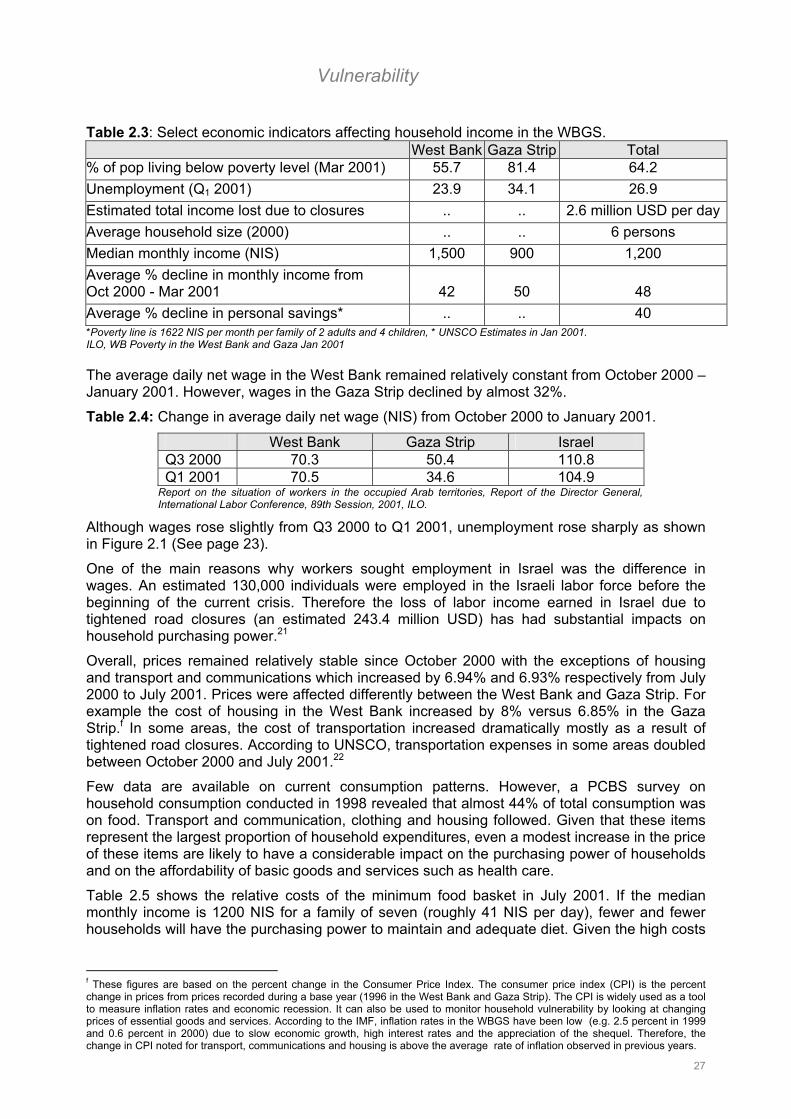
Vulnerability
Table 2.3: Select economic indicators affecting household income in the WBGS. West Bank Gaza Strip Total % of pop living below poverty level (Mar 2001) 55.7 81.4 64.2 Unemployment (Q1 2001) 23.9 34.1 26.9 Estimated total income lost due to closures .. .. 2.6 million USD per dayAverage household size (2000) .. .. 6 persons Median monthly income (NIS) 1,500 900 1,200 Average % decline in monthly income from Oct 2000 - Mar 2001 42 50 48 Average % decline in personal savings* .. .. 40 *Poverty line is 1622 NIS per month per family of 2 adults and 4 children, * UNSCO Estimates in Jan 2001. ILO, WB Poverty in the West Bank and Gaza Jan 2001
The average daily net wage in the West Bank remained relatively constant from October 2000 – January 2001. However, wages in the Gaza Strip declined by almost 32%.
Table 2.4: Change in average daily net wage (NIS) from October 2000 to January 2001.
West Bank Gaza Strip Israel Q3 2000 70.3 50.4 110.8 Q1 2001 70.5 34.6 104.9
Report on the situation of workers in the occupied Arab territories, Report of the Director General, International Labor Conference, 89th Session, 2001, ILO.
Although wages rose slightly from Q3 2000 to Q1 2001, unemployment rose sharply as shown in Figure 2.1 (See page 23).
One of the main reasons why workers sought employment in Israel was the difference in wages. An estimated 130,000 individuals were employed in the Israeli labor force before the beginning of the current crisis. Therefore the loss of labor income earned in Israel due to tightened road closures (an estimated 243.4 million USD) has had substantial impacts on household purchasing power.21
Overall, prices remained relatively stable since October 2000 with the exceptions of housing and transport and communications which increased by 6.94% and 6.93% respectively from July 2000 to July 2001. Prices were affected differently between the West Bank and Gaza Strip. For example the cost of housing in the West Bank increased by 8% versus 6.85% in the Gaza Strip.f In some areas, the cost of transportation increased dramatically mostly as a result of tightened road closures. According to UNSCO, transportation expenses in some areas doubled between October 2000 and July 2001.22
Few data are available on current consumption patterns. However, a PCBS survey on household consumption conducted in 1998 revealed that almost 44% of total consumption was on food. Transport and communication, clothing and housing followed. Given that these items represent the largest proportion of household expenditures, even a modest increase in the price of these items are likely to have a considerable impact on the purchasing power of households and on the affordability of basic goods and services such as health care.
Table 2.5 shows the relative costs of the minimum food basket in July 2001. If the median monthly income is 1200 NIS for a family of seven (roughly 41 NIS per day), fewer and fewer households will have the purchasing power to maintain and adequate diet. Given the high costs
f These figures are based on the percent change in the Consumer Price Index. The consumer price index (CPI) is the percent change in prices from prices recorded during a base year (1996 in the West Bank and Gaza Strip). The CPI is widely used as a tool to measure inflation rates and economic recession. It can also be used to monitor household vulnerability by looking at changing prices of essential goods and services. According to the IMF, inflation rates in the WBGS have been low (e.g. 2.5 percent in 1999 and 0.6 percent in 2000) due to slow economic growth, high interest rates and the appreciation of the shequel. Therefore, the change in CPI noted for transport, communications and housing is above the average rate of inflation observed in previous years.
27
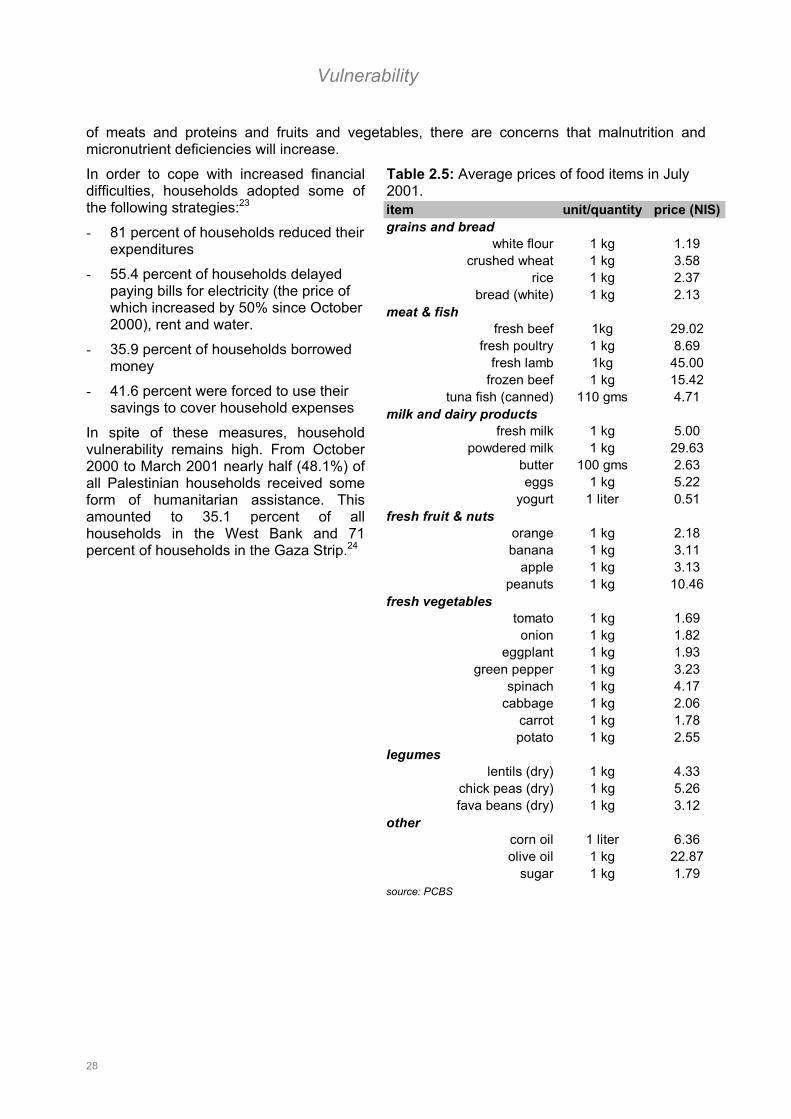
Vulnerability
of meats and proteins and fruits and vegetables, there are concerns that malnutrition and micronutrient deficiencies will increase.
Table 2.5: Average prices of food items in July 2001.
In order to cope with increased financial difficulties, households adopted some of the following strategies:23
- 81 percent of households reduced their expenditures
- 55.4 percent of households delayed paying bills for electricity (the price of which increased by 50% since October 2000), rent and water.
- 35.9 percent of households borrowed money
- 41.6 percent were forced to use their savings to cover household expenses
In spite of these measures, household vulnerability remains high. From October 2000 to March 2001 nearly half (48.1%) of all Palestinian households received some form of humanitarian assistance. This amounted to 35.1 percent of all households in the West Bank and 71 percent of households in the Gaza Strip.24
fr
item unit/quantity price (NIS)grains and bread
white flour 1 kg 1.19crushed wheat 1 kg 3.58
rice 1 kg 2.37bread (white) 1 kg 2.13
meat & fishfresh beef 1kg 29.02
fresh poultry 1 kg 8.69fresh lamb 1kg 45.00
frozen beef 1 kg 15.42tuna fish (canned) 110 gms 4.71
milk and dairy productsfresh milk 1 kg 5.00
powdered milk 1 kg 29.63butter 100 gms 2.63eggs 1 kg 5.22
yogurt 1 liter 0.51esh fruit & nuts
orange 1 kg 2.18banana 1 kg 3.11
apple 1 kg 3.13peanuts 1 kg 10.46
fresh vegetablestomato 1 kg 1.69
onion 1 kg 1.82eggplant 1 kg 1.93
green pepper 1 kg 3.23spinach 1 kg 4.17
cabbage 1 kg 2.06carrot 1 kg 1.78potato 1 kg 2.55
legumeslentils (dry) 1 kg 4.33
chick peas (dry) 1 kg 5.26fava beans (dry) 1 kg 3.12
othercorn oil 1 liter 6.36olive oil 1 kg 22.87
sugar 1 kg 1.79source: PCBS
28
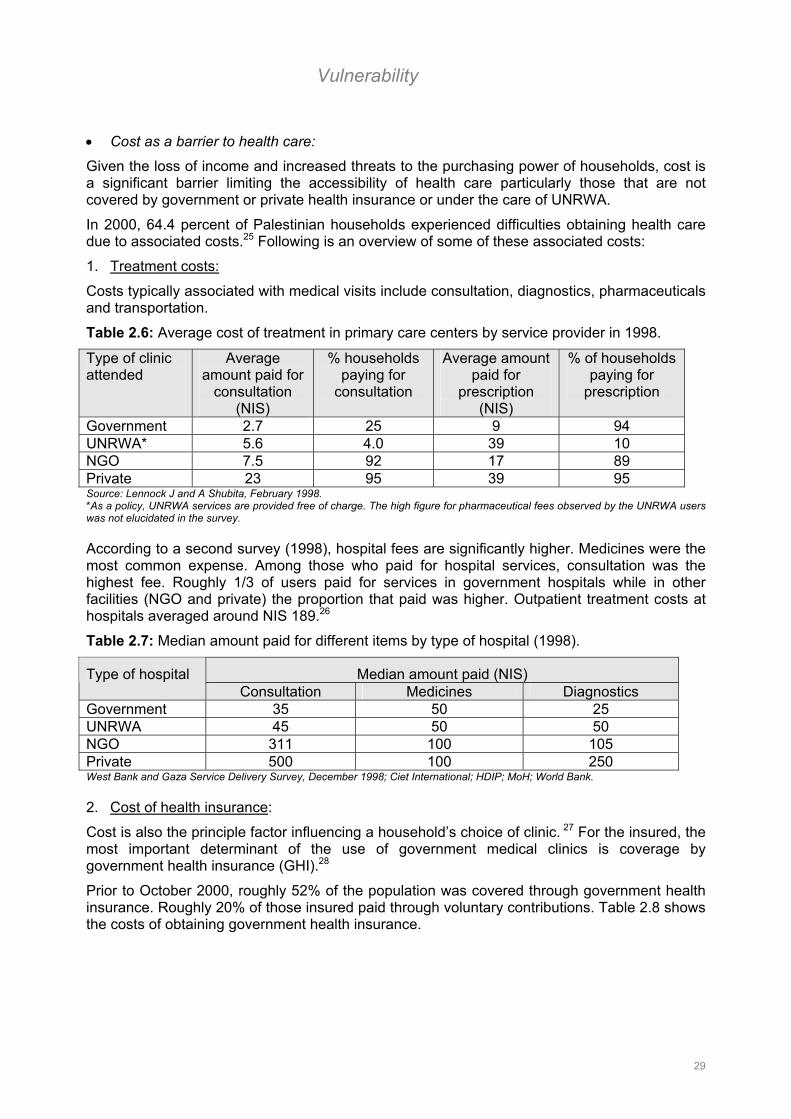
Vulnerability
• Cost as a barrier to health care:
Given the loss of income and increased threats to the purchasing power of households, cost is a significant barrier limiting the accessibility of health care particularly those that are not covered by government or private health insurance or under the care of UNRWA.
In 2000, 64.4 percent of Palestinian households experienced difficulties obtaining health care due to associated costs.25 Following is an overview of some of these associated costs:
1. Treatment costs:
Costs typically associated with medical visits include consultation, diagnostics, pharmaceuticals and transportation.
Table 2.6: Average cost of treatment in primary care centers by service provider in 1998.
Type of clinic attended
Average amount paid for
consultation (NIS)
% households paying for
consultation
Average amount paid for
prescription (NIS)
% of households paying for
prescription
Government 2.7 25 9 94 UNRWA* 5.6 4.0 39 10 NGO 7.5 92 17 89 Private 23 95 39 95 Source: Lennock J and A Shubita, February 1998. *As a policy, UNRWA services are provided free of charge. The high figure for pharmaceutical fees observed by the UNRWA users was not elucidated in the survey.
According to a second survey (1998), hospital fees are significantly higher. Medicines were the most common expense. Among those who paid for hospital services, consultation was the highest fee. Roughly 1/3 of users paid for services in government hospitals while in other facilities (NGO and private) the proportion that paid was higher. Outpatient treatment costs at hospitals averaged around NIS 189.26
Table 2.7: Median amount paid for different items by type of hospital (1998).
Median amount paid (NIS) Type of hospital Consultation Medicines Diagnostics
Government 35 50 25 UNRWA 45 50 50 NGO 311 100 105 Private 500 100 250 West Bank and Gaza Service Delivery Survey, December 1998; Ciet International; HDIP; MoH; World Bank.
2. Cost of health insurance:
Cost is also the principle factor influencing a household’s choice of clinic. 27 For the insured, the most important determinant of the use of government medical clinics is coverage by government health insurance (GHI).28
Prior to October 2000, roughly 52% of the population was covered through government health insurance. Roughly 20% of those insured paid through voluntary contributions. Table 2.8 shows the costs of obtaining government health insurance.
29
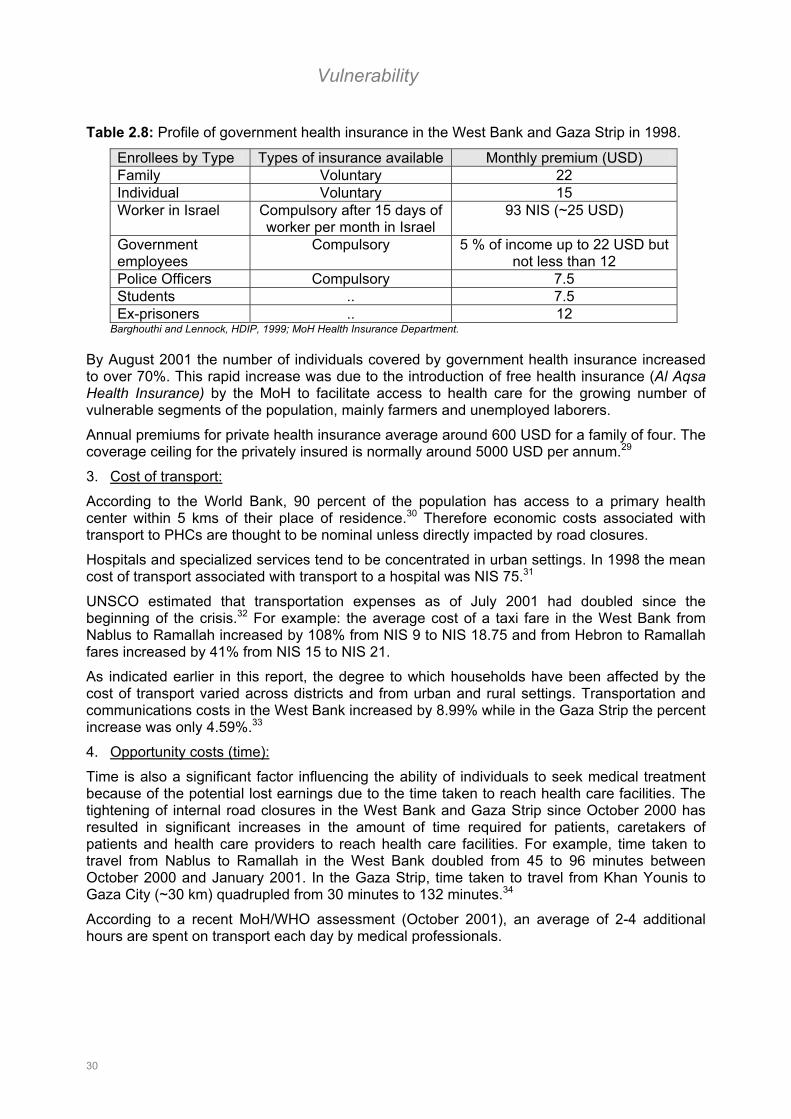
Vulnerability
Table 2.8: Profile of government health insurance in the West Bank and Gaza Strip in 1998.
Enrollees by Type Types of insurance available Monthly premium (USD) Family Voluntary 22 Individual Voluntary 15 Worker in Israel Compulsory after 15 days of
worker per month in Israel 93 NIS (~25 USD)
Government employees
Compulsory 5 % of income up to 22 USD but not less than 12
Police Officers Compulsory 7.5 Students .. 7.5 Ex-prisoners .. 12
Barghouthi and Lennock, HDIP, 1999; MoH Health Insurance Department.
By August 2001 the number of individuals covered by government health insurance increased to over 70%. This rapid increase was due to the introduction of free health insurance (Al Aqsa Health Insurance) by the MoH to facilitate access to health care for the growing number of vulnerable segments of the population, mainly farmers and unemployed laborers.
Annual premiums for private health insurance average around 600 USD for a family of four. The coverage ceiling for the privately insured is normally around 5000 USD per annum.29
3. Cost of transport:
According to the World Bank, 90 percent of the population has access to a primary health center within 5 kms of their place of residence.30 Therefore economic costs associated with transport to PHCs are thought to be nominal unless directly impacted by road closures.
Hospitals and specialized services tend to be concentrated in urban settings. In 1998 the mean cost of transport associated with transport to a hospital was NIS 75.31
UNSCO estimated that transportation expenses as of July 2001 had doubled since the beginning of the crisis.32 For example: the average cost of a taxi fare in the West Bank from Nablus to Ramallah increased by 108% from NIS 9 to NIS 18.75 and from Hebron to Ramallah fares increased by 41% from NIS 15 to NIS 21.
As indicated earlier in this report, the degree to which households have been affected by the cost of transport varied across districts and from urban and rural settings. Transportation and communications costs in the West Bank increased by 8.99% while in the Gaza Strip the percent increase was only 4.59%.33
4. Opportunity costs (time):
Time is also a significant factor influencing the ability of individuals to seek medical treatment because of the potential lost earnings due to the time taken to reach health care facilities. The tightening of internal road closures in the West Bank and Gaza Strip since October 2000 has resulted in significant increases in the amount of time required for patients, caretakers of patients and health care providers to reach health care facilities. For example, time taken to travel from Nablus to Ramallah in the West Bank doubled from 45 to 96 minutes between October 2000 and January 2001. In the Gaza Strip, time taken to travel from Khan Younis to Gaza City (~30 km) quadrupled from 30 minutes to 132 minutes.34
According to a recent MoH/WHO assessment (October 2001), an average of 2-4 additional hours are spent on transport each day by medical professionals.
30
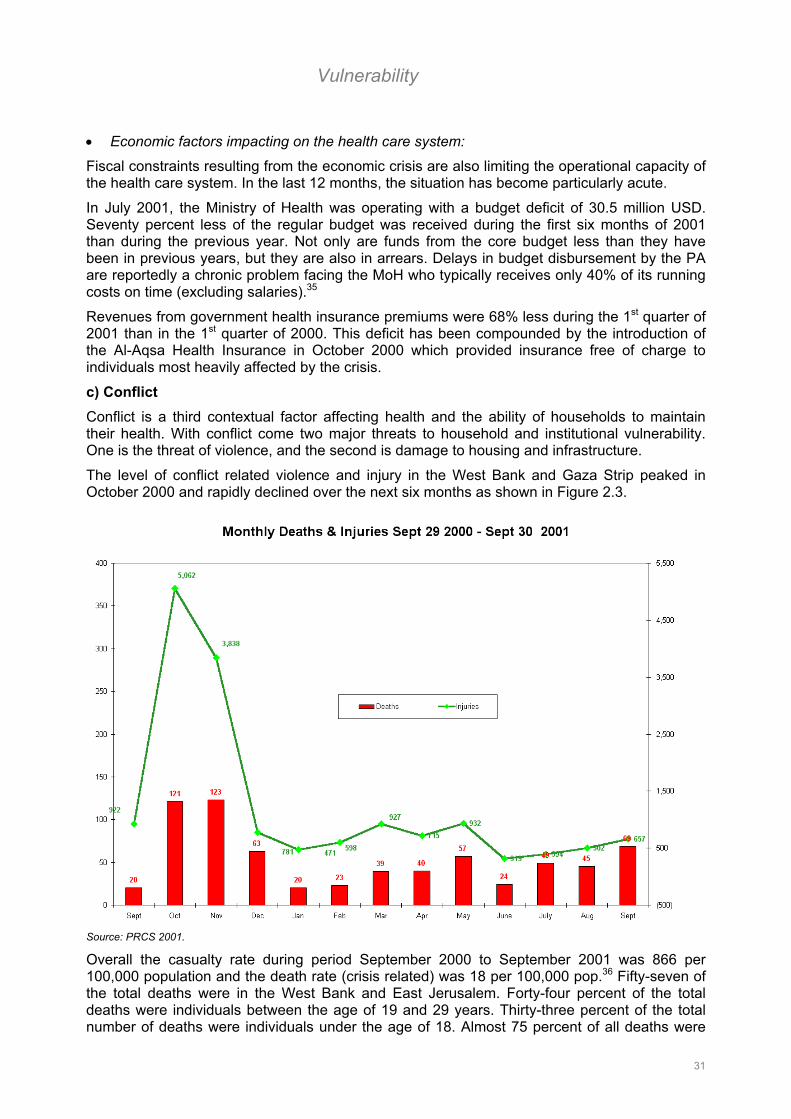
Vulnerability
• Economic factors impacting on the health care system:
Fiscal constraints resulting from the economic crisis are also limiting the operational capacity of the health care system. In the last 12 months, the situation has become particularly acute.
In July 2001, the Ministry of Health was operating with a budget deficit of 30.5 million USD. Seventy percent less of the regular budget was received during the first six months of 2001 than during the previous year. Not only are funds from the core budget less than they have been in previous years, but they are also in arrears. Delays in budget disbursement by the PA are reportedly a chronic problem facing the MoH who typically receives only 40% of its running costs on time (excluding salaries).35
Revenues from government health insurance premiums were 68% less during the 1st quarter of 2001 than in the 1st quarter of 2000. This deficit has been compounded by the introduction of the Al-Aqsa Health Insurance in October 2000 which provided insurance free of charge to individuals most heavily affected by the crisis.
c) Conflict Conflict is a third contextual factor affecting health and the ability of households to maintain their health. With conflict come two major threats to household and institutional vulnerability. One is the threat of violence, and the second is damage to housing and infrastructure.
The level of conflict related violence and injury in the West Bank and Gaza Strip peaked in October 2000 and rapidly declined over the next six months as shown in Figure 2.3.
Source: PRCS 2001.
Overall the casualty rate during period September 2000 to September 2001 was 866 per 100,000 population and the death rate (crisis related) was 18 per 100,000 pop.36 Fifty-seven of the total deaths were in the West Bank and East Jerusalem. Forty-four percent of the total deaths were individuals between the age of 19 and 29 years. Thirty-three percent of the total number of deaths were individuals under the age of 18. Almost 75 percent of all deaths were
31
Vulnerability
caused by live bullets and the majority of injuries sustained (40 percent) were to the head and neck.37
Physical damage sustained as a result of the conflict ranges from the destruction of homes to the destruction of basic infrastructure. According to the Al-Mezan Center for Human rights, approximately 370 houses in the Gaza Strip and 202 houses in the West Bank were destroyed or partially destroyed from September to December 2000.38
Damage was also sustained to essential infrastructure. Approximately seven drinking water wells and 44 agricultural wells were damaged and/or destroyed between October 2000 and March 2001 in the Gaza Strip. Many of these agricultural wells are used as a source of drinking water.39 Municipal buildings, mostly police and law enforcement offices were also damaged during this period.
UNSCO estimated that the value of damage sustained during the last quarter of 2000 to residences, shops, offices, workshops and private vehicles was in the tens of millions of USD.40
Violence stemming from the conflict has affected the health care delivery in two ways. The first has been an increase in the need for emergency medical services to cope with number and types of injuries sustained. The second has been a decrease in security for health care providers, which in turn has implications for freedom of movement and access. A reported 56 government health professionals were injured from October 2000 to April 2001. Ninety-one Palestinian Red Crescent Society (PRCS) emergency medical technicians were injured and 57 ambulances (76% of their fleet) were damaged and/or assaulted.41 The result has been a decline in service provision and an increase in costs due to the need for repair and/or replacement of equipment and staff.
Systemic Factors Systemic factors that influence vulnerability are factors rooted in the structure and distribution of services.
a) Distribution of services The geographic distribution of health care services determines the proximity of medical care and is one of the factors most affected by closure.
Primary care: Primary care services are largely available to the Palestinian population. In 1997, 90% of the population had access to public and private primary care clinics within 5 kilometers of their residence.42 Table 2.9 shows access by type of service provider from a survey conducted in 1998.43
Table 2.9: Percent of population with access to primary care facilities by provider type in the West Bank and Gaza Strip in 1998. (% surveyed).
Government clinic UNRWA NGO Private Clinic West Bank 70% .. 81% 52% Gaza Strip 75% 73% .. 32% Source: Lennock J and A Shubita, February 1998.
For many, internal road closures resulted in reduced access to PHC facilities as described earlier in this report.44
Hospital and specialty care: In 1996, 25% of households in the West Bank and 74% in the Gaza Strip had access to hospitals within 5 kilometers of their place of residence.g45 However, regionally there were significant variations in accessibility. For example, while the overall hospital bed to population ratio in 1993 was 1.2 per 1000 population, the ratio in the north of the West Bank was 0.5 per 1000 population and 0.4 per 1000 population in the south. 46
g According to the 1996 PCBS Health Survey, these figures are higher in the West Bank and lower in the Gaza Strip at 74.5% and 65.4% respectively.
32
Vulnerability
A similar imbalance exists in relation to infrastructure. Many specialty services are not provided in primary care centers particularly in remote areas and most of the existing facilities are concentrated in metropolitan areas in central West Bank and Gaza City.
The physical separation of parts of Jerusalem from the West Bank and Gaza Strip has affected the accessibility of certain key hospitals. Prior to 1996, four major hospitals in Jerusalem provided essential services to Palestinians from the West Bank and Gaza Strip (e.g. oncology, burn treatment, cardiovascular surgery, complex neonatal and pediatric surgery). After 1996, in order to obtain access to these facilities, individuals needed to obtain a permit form the Israeli authorities. This permit was reportedly very difficult to obtain unless the patient required urgent care and/or surgery.47
The Ministry of Health currently purchases specialty care services and advance diagnostic services from health facilities abroad (Egypt and Jordan), from Israel and from the private sector. The implications of international border closures on the health of these patients are evident. According to a recent MoH/WHO Health Impact Assessment, international road closures have increased the risks of complication among patients referred abroad for treatment. For example, medical complications were reported for 20% of the cancer patients referred from the Gaza Strip for treatment abroad during the period of study.
b) Multiple service providers As outlined in Part 1, there are four main health service providers – the MoH, UNRWA, NGOs and the Private Sector. These divisions of service delivery and of catchment populations (e.g. MoH services to holders of GHI and UNRWA to refugees) have serious implications for policy making, regulation and on ensuring quality and equity in coverage.
c) Separation of the West Bank and Gaza Strip The physical separation of the West Bank and Gaza Strip has necessitated the establishment of parallel health structures. This in turn has resulted in increased operational inefficiency, a weakening in management capacities and fragmentation of systems and functions. Some specific examples include:48
- Key decision makers are largely unable to travel between the West Bank and Gaza Strip. This separation has presented serious obstacles to effective coordination and planning and legislation policy
- Inconsistent and un-harmonized regulatory mechanisms including licensing, certification and inspection
- Differences between reporting and hospital registration systems
- Separate collection of premiums and management of government health insurance mechanisms
- Duplicate support functions such as human resource management and development, financial management, facilities management, information systems, etc.
- Effectiveness of training and education undermined by the inability to conduct joint sessions.
d) Constraints to policy, planning and capacity building The uncertainty of the current socio-economic and political environment in the West Bank and Gaza Strip presents considerable challenges for policy makers and makes planning for the health sector complicated and unpredictable. Consequently, the potential for strategic planning has been weakened.
The Department of Health Planning developed a National Health Plan (NHP) for the West Bank and Gaza Strip to be implemented during the period 1999-2003. In this plan, a vision for the health care system and target aims and objectives are outlined. The plan was considered an
33
Vulnerability
important step for the MoH in outlining and affirming its role as regulator and coordinator of health care services.49 However, several key concerns were identified with respect to the operationalizability of the NHP and are summarized below: 50
- The NHP appears to present objectives for the management and running capacity of the health care system in isolation of objectives for its operational targets for primary, secondary and tertiary care. As a consequence, there is no clear link between operational targets and resources needed to reach that target.
- The NHP does not distinguish between strategic objectives and priorities. This lack of clearly stated priorities may result in a lack of focus for development activities. It might also allow for increased mismatches between donor and MoH priorities where because of the lack of a clear “road-map” for health sector development.
- The NHP did not outline a holistic vision that incorporates the four main service providers in this sector (UNRWA, the MoH, NGOs and the private sector). No formal structure exists to allow for discussions and interaction between the four major health care providers on policy issues and to plot the range of services provided and required.
- Also, it is not clear to which degree the activities and objectives outlined NHP complement and support goals and objectives outlined in the Palestinian Development Plan.
At the same time, it is important to acknowledge that there are a number of factors related to the overall context and to the set-up of the institution that affected its capacities for policy, planning and ultimately development. Some of these factors are summarized below:
- Legacies of the Israeli Civil Administration: One of the greatest challenges to policy making and the development of the health sector in the WBGS has been the task of building a health administration. In 1994 after the transfer of responsibility from the Israeli Civil Administration, the PA was faced with the task of “staffing ministries; acquiring the necessary office space, equipment and other supports; delineating bureaucratic responsibilities; establishing coordination and communication mechanisms; reforming legal and regulatory mechanisms; and setting national priorities – all essentially from scratch.”51 Although the progress that has been made is commendable, there has been an underestimation (on all sides) of the level of “institutional growing pains” that would be experienced.
- Interim agreements and the subsequent uncertainty over jurisdiction and control over the West Bank and Gaza Strip: The challenge of policy making is exacerbated by the uncertainty of the extent of Palestinian Authority and MoH control and jurisdiction over the Palestinian territories. With each interim agreement, there was a resulting change in the geographic area under the jurisdiction of the PA and a change in its revenue base. For example, the Israeli-Palestinian Interim Agreement on the West Bank and Gaza Strip (September 1995) allowed for PA control over health, education, and the tax system. However, it did not allow for choice over instruments and strategies used particularly with respect to fiscal instruments and the choice of external economic relations. 52 According to these agreements, Israel remains in control of 40% of the Gaza Strip and 70% of the West Bank. As such, the PA is limited in its ability to supervise and set policy with respect to management of basic infrastructure and health care legislation. Key areas affected include water supply management, sanitation services, environmental health management, communication systems and transportation.
- Dominance of a bio-medical model: A biomedical curative model of health care is the driving focus of health care development in the West Bank and Gaza Strip. 53 Growth of the private sector (mostly in the area of advanced diagnostics) is thought to be reinforcing this trend.
34
Vulnerability
Existing disease management strategies for chronic diseases – hypertension, diabetes, and coronary heath disease – are almost entirely curative. Similarly, while road traffic accidents and injuries are the leading cause of mortality among children, little attention has been given to prevention.
As of 1997, only 15% of recurrent health expenditure was spent on primary and preventative care while curative secondary and tertiary services accounted for more than 80% of spending. The emphasis on hospital development evident in most development initiatives is likely to worsen this focus on curative rather than preventative care. 54
- Lack of a rational fiscal policy: Control over decision-making in the health sector is highly centralized within the PA and Ministry of Finance. No decision-making powers have been granted at the district level and decisions are limited to resource allocation and consumption. As a consequence, incentives to maximize savings are weak since all excess funds are returned to the Central Treasury. 55
There is no access to information about performance and spending patterns outside the central level. There is also a shortage of technical expertise on financial management tools and techniques. Consequently, little consideration is given to the connection between development plans and their financial consequences.
- Top heavy administration: During the period 1994-1998 there was a massive expansion in public sector employment introduced as a means of job creation. The MoH’s personnel increased from 3,984 to 6,554 during that period.
Salaries of public servants in the MoH are low averaging about 1/3 salaries earned in the private sector.h One of the consequences of low pay has been a high amount of “grade-creep” leaving the MoH with some 60 general directors. The top heavy structure not only complicates decision making, but also salaries consume over 48 percent of the annual MoH budget. 56
Complicating this human resource (HR) problem is the fact that the General Personnel Council of the Palestinian Authority manages all civil service HR matters. All appointments of General Directors and their cabinet members have to be approved by the Council. This in turn raises questions about the impartiality and credibility of appointments of some high level MoH officials.57 According to the ILO, 52% of all PA posts were filled in a non-competitive manner.58
A Civil Service Law was drafted in 1998 that outlined merit-based processes for recruitment and promotion, conditions of service, performance review mechanisms, and discipline and grievance procedures. This law is still awaiting implementation. 59
- Unregulated growth and activity of the private sector: Private sector growth was viewed by the international community as one of the main mechanisms for growth following the establishment of the PA in 1993. Domestic private sector development in health was encouraged by the MoH as a means of reducing cost and dependency on Israeli, Jordanian and Egyptian hospitals for specialty care and advanced diagnostic testing. What followed was a growth in the number of facilities providing services ranging from clinical services to specialized diagnostic testing.
Few regulatory mechanisms exist that can influence prices, quantity and quality of services provided in the private sector. Service providers generally set fees with little reference to the associated treatment and operating costs. There are concerns that unless policies are established that ensure that the growth of the private sector is in-line with plans for the overall development of the health sector, rationalizing costs associated with health care will become increasingly difficult.
h This has contributed to the problem of conflict of interest where public servants take up secondary employment in the private sector.
35

Vulnerability
There is also concern about the number of physicians that work in both the private and public sectors. A clear and fair regulatory framework is lacking that prevents conflict of interest, ensures that value for money is assured and ethical standards are maintained.60
- Weakness in technical capacities: Given the challenges of building a MoH in the current context in the Palestinian territories, it is to be expected that certain technical capacities would be weak. At the same time, the PA does have the advantage of having a highly education population and access to considerable skills among Palestinians living outside of the West Bank and Gaza Strip. Donor assistance is also a considerable resource.
One key technical area identified that is in need of strengthening is the area of emergency and disaster management. This weakness became particularly evident after the escalation of the recent crisis in October 2000. This includes the promotion of disaster preparedness and response activities including early warning systems and rapid damage assessments. The development of an integrated national disaster preparedness and response plan is critical to ensuring that emergency interventions are in line with medium and long-term development plans for the health sector.61
In October 2000, the Ministry of Health developed a strategy for coping with the escalation of the conflict and subsequent increases in demand.62 These strategies are summarized below:
1) Decentralization of services 2) Strengthening the idea of community participation in health services 3) Strengthening telecommunication 4) Consolidating cooperation 5) Upgrading Emergency Medical Services 6) Improving community mental health services 7) Improving rehabilitation services for the disabled 8) Expanding the scope of cooperation 9) MoH to continue with ongoing activities
Approximately 540 new hospital beds were added to accommodate the crisis. 50 PHCs in the West Bank and 14 in the Gaza Strip were also upgraded and expanded to include emergency services. In some remote areas, hours of operation were extended to 12 and 24 hours.63
Although these measures were introduced quickly, it is not clear to what extent they are in-line with the NHP for health sector development. It is also not clear whether the increases in health system capacity were balanced with operational and financial capacities. According to the MoH the expansion of services and the extension of service hours were not coupled with an increase in financial and human resources.64
After the introduction of the Al Aqsa Health Insurance, the number of individuals covered by government health insurance increased to over 70% (by August 2001). If GHI coverage is still the predominant factor influencing choice of medical facility (as outlined on page 29), then a 20% increase in coverage in less than one year has serious implications on the operational capacity of government facilities particularly where not matched with and increase in resources.
36
Vulnerability
1 Health Care Under Siege II, HDIP, May 2001 2 Palestine Human Development Report 1998-1999, Bir Zeit Univeristy, UNDP. 3 According to UNRWA as of 31 March 2001. 4 UNRWA Refugee Update June 2001. 5 Annual Report of the Department of Health, 1999 UNRWA. 6 UNRWA Refugee Update June 2001. 7 Al-Mezan Center for Human Rights. Reports covering the period September 29th – December 9th, 2000. 8 Poverty in the West Bank and Gaza – Summary Report, World Bank, May 2001. 9 IBID, May 2001. 10 IBID, May 2001. 11 PCBS Labor Force Current Main Indicators, August 2001. 12 Impact on the Palestinian economy of confrontation, border closures and mobility restrictions from 1 October 2000 – 30 June 2001. UNSCO, August 2001; PCBS Census 1997. 13 IBID, August 2000. 14 PCBS Survey: Impact of the Israeli Measures on the Well-being of Palestinian Children, Women and Households, 2001. 15 The Situation Analysis of Palestinian Children, Young People and Women in the West Bank and Gaza Strip, UNICEF/PA, August 2000. 16 Report on the situation of workers in the occupied Arab territories, Report of the Director General of the ILO, International Labour Conference, 89th Session, 2001. 17 MAS Social Monitor Issue No. 3, 1999; These figures are from the PCBS Crime and Victimization Statistics carried out in 1998. 18 Impact on the Palestinian economy of confrontation, border closures and mobility restrictions from 1 October 2000 – 30 June 2001. UNSCO, August 2001. 19Health Impact Assessment –A comparative assessment of the impacts of the current crisis on health and health system delivery in the West Bank & Gaza. WHO and the MoH, UNPUBLISHED - October 2001. 20 Health in Palestine: Potential and Challenges, MAS Discussion Paper, Barghouthi M, Lennock J, March 1997. 21 Report on the situation of workers in the occupied Arab territories, Report of the Director General of the ILO, International Labour Conference, 89th Session, 2001. 22 The impact on the Palestinian Economy of Confrontations, Mobility Restrictions and Border Closures – 1 October 2000 – 31 January 2001, UNSCO. 23 PCBS Survey: Impact of the Israeli Measures on the Well-being of Palestinian Children, Women and Households, 2001. 24 Report on the situation of workers in the occupied Arab territories, Report of the Director General of the ILO, International Labour Conference, 89th Session, 2001. 25 IBID, 2001. 26 Health Insurance and Health Service Utilization in the West Bank and Gaza Strip, HDIP, February 1998 27 IBID, February 1998 28 IBID, February 1998 29 The Palestinian Health System: An Updated Overview, Barghouthi M, Shubita A, and L Fragiacomo, HDIP, March 2000. 30 West Bank and Gaza: Medium-term development strategy for the health sector, World Bank, 1998. 31 West Bank and Gaza Service Delivery Survey, Ciet International, HDIP, PA and World Bank, December 1998. 32 The impact on the Palestinian Economy of Confrontations, Mobility Restrictions and Border Closures – 1 October 2000 – 31 January 2001, UNSCO. 33 PCBS 2001. 34 The impact on the Palestinian Economy of Confrontations, Mobility Restrictions and Border Closures – 1 October 2000 – 31 January 2001, UNSCO. 35 Health in Palestine: Potential and Challenges, MAS Discussion Paper, Barghouthi M, Lennock J, March 1997. 36 Impact of Current Crisis in the West Bank and Gaza on Health Care and Education, Rapid Donor Assessment, World Bank, July 2001 – UNPUBLISHED DRAFT. 37 Health Care Under Siege II, HDIP, May 2001 38 Al-Mezan Center for Human Rights. Reports Covering the period September 29th – Dcember 9th, 2000. 39 UNPUBLISHED WHO/MoH Health Impact Assessment. October 2001; Personal communication from Oxfam Public Health Engineer, August 2001. 40 The impact on the Palestinian Economy of Confrontations, Mobility Restrictions and Border Closures – 1 October 2000 – 31 January 2001, UNSCO. 41 Health Impact Assessment –A comparative assessment of the impacts of the current crisis on health and health system delivery in the West Bank & Gaza. WHO and the MoH, October 2001. UNPUBLISHED DRAFT. 42 West Bank and Gaza: Medium-term development strategy for the health sector, World Bank, 1998 43 Health Insurance and Health Service Utilization in the West Bank and Gaza Strip, HDIP, February 1998. 44Health Impact Assessment –A comparative assessment of the impacts of the current crisis on health and health system delivery in the West Bank & Gaza. WHO and the MoH, October 2001. UNPUBLISHED DRAFT. 45 Palestinian Household Survey, Palestinian Central Bureau for Statistics, 1996. 46 The Palestinian Health System: An Updated Overview, HDIP, March 2000 47 Health in Palestine: Potential and Challenges, MAS Discussion Paper, Barghouthi M, Lennock J, March 1997. 48 IBID, March 1997. 49 ”Health Sector Strategy Paper for the West Bank and Gaza”, DfiD Health Mission, May 1999. 50 IBID, May 1999. 51 “The Palestinian Territories” from Good Intentions, Pledges of Aid for Post-Conflict Recovery, edited by Shepard Forman and Stewart Patrick, Center on International Cooperation, 2000. 52 IBID, 2000. 53 Health in Palestine: Potential and Challenges, MAS Discussion Paper, Barghouthi M, Lennock J, March 1997. 54 IBID, March 1997. 55 “Health Sector Strategy Paper for the West Bank and Gaza”, DfiD Health Mission, May 1999. 56 IBID, May 1999.
37

Vulnerability
57 IBID, May 1999. 58 Report on the situation of workers in the occupied Arab territories, Report of the Director General of the ILO, International Labour Conference, 89th Session, 2001. 59 “Health Sector Strategy Paper for the West Bank and Gaza”, DfiD Health Mission, May 1999. 60 IBID, May 1999. 61 Impact of Current Crisis in the West Bank and Gaza on Health Care and Education, Rapid Donor Assessment, World Bank, July 2001 – UNPUBLISHED DRAFT. 62 As presented by the MoH at the Health Sector Working Group Meeting on 12 July 2001. 63 IBID, July 2001. 64 Health Impact Assessment –A comparative assessment of the impacts of the current crisis on health and health system delivery in the West Bank & Gaza. WHO and the MoH, October 2001. UNPUBLISHED DRAFT.
38

The International Health Response
Part 3: Implications for the international health response Part 3 looks first at the nature and extent of the humanitarian health response to date: what has been done in which areas? The discussion then moves into key challenges/obstacles constraining the effectiveness and impact of the international response.
3.1 Overview of the international response to date:
From 1994 to June of 2001, over 5.2 billion USD were committed to the West Bank and Gaza Strip by the International Community at an average of 645 million USD per year.1 Aid per capita during this period (~214 USD) was almost 10 times aid per capita spent in developing countries and second only to the 380 USD spent per capita on post-conflict reconstruction in Bosnia.2
The first agenda for development assistance was the Emergency Assistance Programme (EAP) developed by the World Bank for the period 1994 – 1996. In it some 1.2 billion USD was to be disbursed for public investments (600 million USD); private sector support (300 million USD); start-up expenditures (225 million USD); and technical assistance (75 million USD). In practice the sectoral needs proved greater than anticipated and the PA’s need for budgetary support exceeded projects (2 fold).
In practice, some sectors prioritized in the EAP were grossly overfunded (education 343% and health 161%) while others were grossly under funded (power received only 10% of planned funds while agriculture and support to the private sector and industry received only 6% and 0% respectively.) At the same time, assistance in different geographical areas varied depending on the inherent scale, technical complexity and political complications of projects in particular sectors. For example, although agriculture accounts for 1/5 of Palestinian employment, trade and GDP, it received only 1.5% of donor commitments and 1% of donor disbursements by the end of 1997. This low level of support may have been due in part to the political sensitivities linked to land and water consumption as well as the priority given to emergency job creation. 3
Funding for NGOs, formerly a major health and social service, also declined significantly. After the establishment and growth of the PA in 1993, support for NGOs declined sharply. In the early 1990s this sector received 170-240 million USD per year while after 1994, financial support dropped to 60 – 90 million USD. Several reasons were cited for this decline in funding: NGOs lacked the capacity to implement large development projects; a large amount of staff would have been required to oversee and steer NGO funded activities; coordination between NGOs was considered weak; and NGOs lacked a formal channel of representation within donor coordination frameworks.4
Figure 3.1: Donor commitments from 1994 to 2001 by sector outlined in the Palestinian Development Plan.
5
35
35
25
15
30
25
30
20
25
20
35
20
20
15
45
0%10%20%30%40%50%60%70%80%90%
100%
1994-1995 1996-1997 1998-1999 2000-2001(Q1)
productive sector social sectorinstitution building infrastructure development
Source: MOPIC Quarterly Report, June 2001.
39
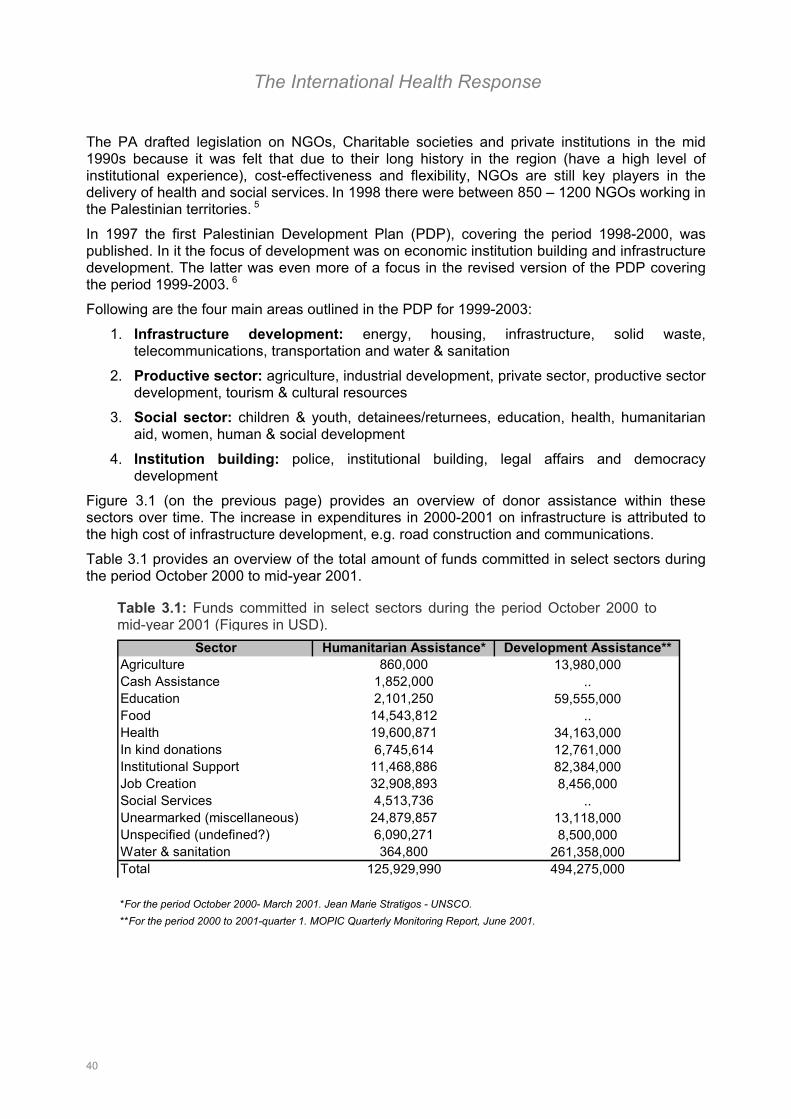
The International Health Response
The PA drafted legislation on NGOs, Charitable societies and private institutions in the mid 1990s because it was felt that due to their long history in the region (have a high level of institutional experience), cost-effectiveness and flexibility, NGOs are still key players in the delivery of health and social services. In 1998 there were between 850 – 1200 NGOs working in the Palestinian territories. 5
In 1997 the first Palestinian Development Plan (PDP), covering the period 1998-2000, was published. In it the focus of development was on economic institution building and infrastructure development. The latter was even more of a focus in the revised version of the PDP covering the period 1999-2003. 6
Following are the four main areas outlined in the PDP for 1999-2003:
1. Infrastructure development: energy, housing, infrastructure, solid waste, telecommunications, transportation and water & sanitation
2. Productive sector: agriculture, industrial development, private sector, productive sector development, tourism & cultural resources
3. Social sector: children & youth, detainees/returnees, education, health, humanitarian aid, women, human & social development
4. Institution building: police, institutional building, legal affairs and democracy development
Figure 3.1 (on the previous page) provides an overview of donor assistance within these sectors over time. The increase in expenditures in 2000-2001 on infrastructure is attributed to the high cost of infrastructure development, e.g. road construction and communications.
Table 3.1 provides an overview of the total amount of funds committed in select sectors during the period October 2000 to mid-year 2001.
Table 3.1: Funds committed in select sectors during the period October 2000 tomid-year 2001 (Figures in USD).
Sector Humanitarian Assistance* Development Assistance**Agriculture 860,000 13,980,000Cash Assistance 1,852,000 ..Education 2,101,250 59,555,000Food 14,543,812 ..Health 19,600,871 34,163,000In kind donations 6,745,614 12,761,000Institutional Support 11,468,886 82,384,000Job Creation 32,908,893 8,456,000Social Services 4,513,736 ..Unearmarked (miscellaneous) 24,879,857 13,118,000Unspecified (undefined?) 6,090,271 8,500,000Water & sanitation 364,800 261,358,000Total 125,929,990 494,275,000
*For the period October 2000- March 2001. Jean Marie Stratigos - UNSCO.**For the period 2000 to 2001-quarter 1. MOPIC Quarterly Monitoring Report, June 2001.
40
The International Health Response
3.2 Determinants of the impact of the international health response
The overall shape of the international health response in the West Bank and Gaza Strip is influenced by a number of factors both within and outside the health sector. Given that the main purpose of the vulnerability analysis is to inform planning and development of the health sector agenda, the analysis provided in the final section of the report was completed through a participatory approach drawing on the knowledge and experience of key health sector actors.
The following sector-wide issues and questions related to the international health response were collectively identified by the Core Group, representatives of the MoH, MOPIC, the donor community, international agencies and Palestinian organizations working in the health sector. Two informal working group sessions were held in October 2001 in Jerusalem and Ramallah. The following three questions were explored:
1. What are the key issues influencing the impact and/or effectiveness of the international health response?
2. How should these issues be prioritized?
3. How should the Core Group advise the SWG on health to address these issues? What processes could the SWG put in place to address these issues?
After an initial “brainstorming” session, the participants grouped the main factors identified into the following four categories:
1. Health sector related issues are factors inherent in the way that the health sector is structured and operates. Who are the main service providers? What resources are currently available? What is the overall direction of health sector development? For example one health sector related factor that is influencing the nature of the international health response is the fact that there are four major service providers. This has implications for the international health response vis-à-vis partners, policy-making and coverage.
2. Contextual factors are factors inherent in the overall operating environment which influence the effectiveness of external interventions. For example, the geographic separation between the West Bank and Gaza has implications for coordination and programme implementation especially where national staff are unable to travel between the two areas.
3. External and/or global factors are factors external to the Palestinian context which may or may not influence external activity/interests in the region. For example, the development of an acute crisis in other parts of the world (e.g. Afghanistan) may result in a diversion of resources away from the West Bank and Gaza Strip.
4. Factors inherent in the international aid system are factors rooted deep within the international aid system which limit the effectiveness and flexibility of interventions. Examples include extensive bureaucratic procedures for fund disbursement, coordination issues, and operational restrictions due to donor inflexibility and/or mandates.
Figure 3.2 contains a diagramme outlining some of these factors and highlights ways in which they are related.
41
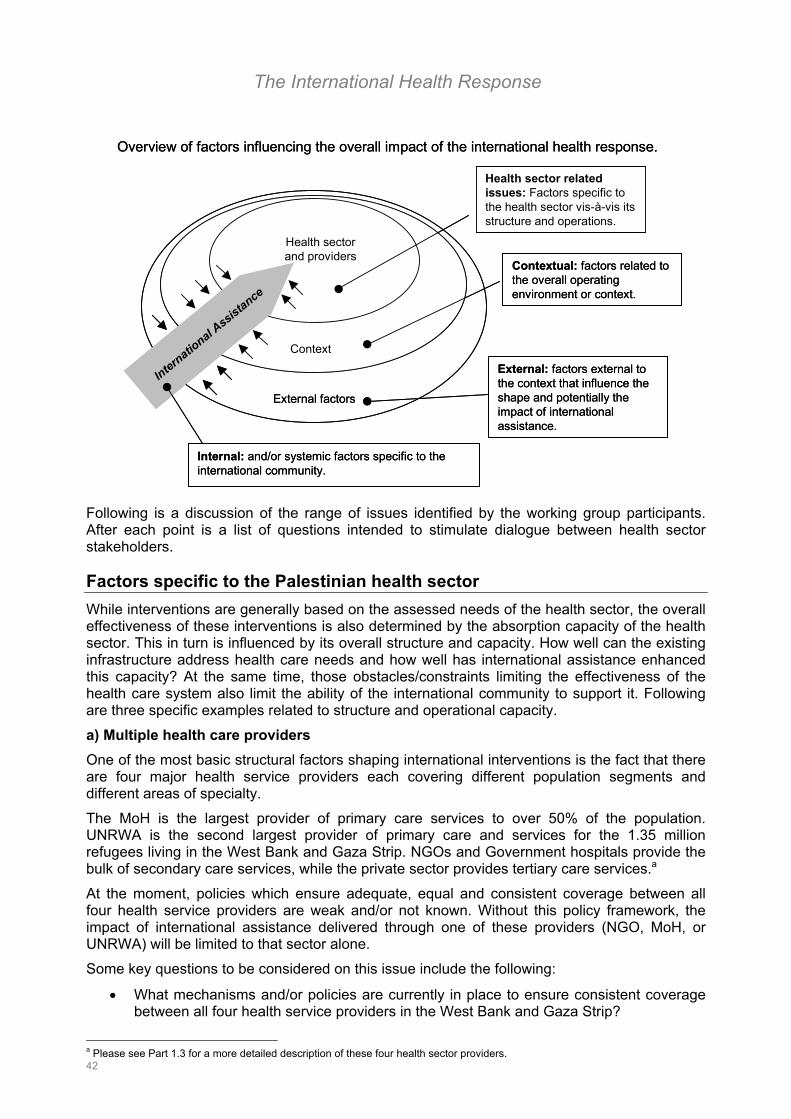
The International Health Response
Contextual: factors related to the overall operating environment or context.
Internal: and/or systemic factors specific to the international community.
Health sector related issues: Factors specific to the health sector vis-à-vis its structure and operations.
Context
External factors
External: factors external to the context that influence the shape and potentially the impact of international assistance.
Health sector and providers
International A
ssistance
Overview of factors influencing the overall impact of the international health response.
Contextual: factors related to the overall operating environment or context.
Internal: and/or systemic factors specific to the international community.
Health sector related issues: Factors specific to the health sector vis-à-vis its structure and operations.
Context
External factors
External: factors external to the context that influence the shape and potentially the impact of international assistance.
Health sector and providers
International A
ssistance
Overview of factors influencing the overall impact of the international health response.
Following is a discussion of the range of issues identified by the working group participants. After each point is a list of questions intended to stimulate dialogue between health sector stakeholders.
Factors specific to the Palestinian health sector While interventions are generally based on the assessed needs of the health sector, the overall effectiveness of these interventions is also determined by the absorption capacity of the health sector. This in turn is influenced by its overall structure and capacity. How well can the existing infrastructure address health care needs and how well has international assistance enhanced this capacity? At the same time, those obstacles/constraints limiting the effectiveness of the health care system also limit the ability of the international community to support it. Following are three specific examples related to structure and operational capacity.
a) Multiple health care providers One of the most basic structural factors shaping international interventions is the fact that there are four major health service providers each covering different population segments and different areas of specialty.
The MoH is the largest provider of primary care services to over 50% of the population. UNRWA is the second largest provider of primary care and services for the 1.35 million refugees living in the West Bank and Gaza Strip. NGOs and Government hospitals provide the bulk of secondary care services, while the private sector provides tertiary care services.a
At the moment, policies which ensure adequate, equal and consistent coverage between all four health service providers are weak and/or not known. Without this policy framework, the impact of international assistance delivered through one of these providers (NGO, MoH, or UNRWA) will be limited to that sector alone.
Some key questions to be considered on this issue include the following:
• What mechanisms and/or policies are currently in place to ensure consistent coverage between all four health service providers in the West Bank and Gaza Strip?
42
a Please see Part 1.3 for a more detailed description of these four health sector providers.
The International Health Response
• What additional mechanisms and/or policies are needed? Licensing? Clear and efficient contracting mechanisms? Quality control?
• Whose role/responsibility is it to develop and put these mechanisms and/or policies in place?
• And how can the international community best support this?
b) Lack of a common vision for the health sector A vision for health in the Palestinian territories was outlined in the National health Plan in 1998.b However, because there are questions about the aims, priorities and “operationalizability” of this plan, although considered ambitious it has not been seen as credible. This vision is also not widely known or shared across the four health sector providers (MoH, NGO, UNRWA and the private sector).
Without a clear framework for health sector development, external assistance appears fragmented and inconsistent. This in turn has resulted in frustration for Palestinian health sector providers who feel that health interventions are largely “donor driven”; that Palestinians have little say in influencing the international development agenda; and that there is constant pressure to change the focus of activities in order to obtain funding. This then has left the impression that the international health agenda is unclear and “ever-changing”.
Some key questions to be considered on this issue include the following:
• Perceptions about responsibility for bridging the gap between the international health agenda and the Palestinian health development plan are varied. Where does the responsibility for this alignment lie?
• Can and should the Palestinian MoH facilitate this process given their current operational and contextual constraints? If no, what inputs and support do they need?
• Would the development and re-articulation of a clear and operational strategy for health sector be one way to begin to empower the MoH in this regard?
c) Questions about the credibility of health sector counterparts One of the most commonly articulated concerns with respect to international assistance in the health sector has been the need to build capacity for policy and decision making within the MoH. Some of the problems encountered by the MoH in handling external assistance seems to have stemmed from shortages in human resources. In many cases, the line ministries lacked both trained senior management and technical experts in many policy areas, which include policy and planning, financial and human resource management and health sector regulation.
At the same time it is important to consider that the MoH is still a young administration and many of the problems affecting its institutional credibility might have been predicted given the complexity of the operating environment and short period of development (7 years).
The task to establish a functional MoH in the West Bank and Gaza Strip in 1994 was far from straightforward and it is clear that the international community may have underestimated its “institutional growing pains”.c This in turn may have led to unrealistic expectations about absorption capacities. Key questions to consider in this regard include:
• What aspects of the health administration were shaped by the overall operating context and cannot be changed unless broader economic and political solutions are reached
b Please see in Part 2 for more information.
43
c Please see Part 2 for a detailed discussion of systemic and contextual factors that influenced the development of the health care system.
The International Health Response
(.e.g. physical separation of the West Bank and Gaza which has necessitated the establishment of two parallel health systems)?
• Which factors and policies can be changed within the current context?
• What steps need to take place in order to identify how best to support capacity building within the MoH? What inputs and support are needed?
• PA officials have complained about the high number and low quality of technical experts provided by donors. Many lack experience in the region and cannot speak Arabic. Fees and salaries paid to consultants are an additional source of tension. The differences in perceived and actual utility of technical assistance are thought to be a reflection of the “bureaucratic position of the observer, the technical expertise of the specialist, and the ideological orientation of the analyst.” 7 Given that technical assistance is needed for the future development of the Palestinian health sector, what type of technical assistance, budgetary assistance and/or combination would be most affective? How would it be determined? Through what channels could it be delivered to minimize some of the negative tensions outlined above?
Contextual factors Many of the contextual constraints influencing the overall impact of humanitarian and development health assistance are the same as those influencing household and institutional vulnerability and include uncertainties and risks stemming from the overall conflict context, closure and restrictions in access and movement.
Following is a summary of some of the key obstacles/issues for the international community that emerged as a consequence of these contextual factors.
a) Access to health care services and service delivery The most significant contextual factor affecting the impact of international health assistance is the problem of access. The principal concern with respect to this issue is how to ensure consistent and equal coverage of the population.
There are two sides to the problem of access. The first is access of patients to health care facilities and the second is access of health care providers and supplies/equipment to points of service. Part 2.2 of this report contains an overview of the practical implications of closure and economics on health utilization and health care delivery.
Some of the implications of a lack of access on the ability of the local and international health interventions to ensure coverage are summarized below. Following each point is a list of key questions for health decision makers and planners of international health interventions.
The impact of closure on access varies considerably between the West Bank and Gaza Strip. Distances required to travel to points of service in the West Bank are much greater than in the Gaza Strip.
• What are the implications of this for international health interventions?
• What are the implications for planning and possibly operational efficiency, especially where each zone requires different strategies and inputs?
In many cases the separation of the West Bank and Gaza Strip has necessitated the establishment of duplicate structures and programmes.
• What are the implications of this on planning, coordination and management, resource allocation and operational efficiency?
• What current structures are in place given this constraint? Are there alternatives?
44
The International Health Response
Utilization patterns have shifted as a result of a lack of access to health facilities. This shift has been a shift in both the type of service provider and in the geographic location of the health care facility. Households experiencing financial difficulties have begun to shift from private and NGO facilities to Government health facilities where the barrier of cost is the lowest. This was especially true after the introduction of the Al Aqsa Health Insurance Decree in October 2000.d
At the same time, utilization patterns have changed geographically. In areas most heavily affected by closure, utilization of services has increased or decreased according to points of closure. This in turn has resulted in an overload in some health care facilities and an under use of others.
• What are the implications of this change in utilization patterns on health intelligence?
• What are the implications of this change in utilization patterns on service delivery?
• How much support should be given to those facilities burdened by the increase in demand?
• How much support should be given to sustain those facilities struggling to recoup their running costs because of underutilization?
• What other means are available to the international community to improve access under these conditions and what are their implications on health planning?
Theoretically, the state of closure is a “temporary” condition. One of the main strategies put in place by the MoH (and supported by the international community) is the upgrading of primary health clinics from level I to levels II and III. This has involved rehabilitation of facilities and the introduction of new services and equipment.
• Given that “upgrading of facilities” involves significant structural changes, is this actually a “permanent” solution for a problem that is “temporary”?
• How flexible is “the upgrading of resources” for reallocation and/or rationalization in the future?
• Although it is true that changes at the PHC level are less costly than at the secondary and tertiary level, the overall questions vis-à-vis sustainability and running costs are the same. That said, what measures can be put in place by health service providers and the international community to balance both immediate needs and long-term development plans?
b) Interim agreements Many issues related to the overall question of the West Bank and Gaza Strip (e.g. sovereignty and the refugee question) have yet to be resolved. Therefore, almost all development and relief activities are taking place in a context of uncertain transition, which in and of itself has serious implications for long-term planning and sustainability.
Some of the main factors limiting the effectiveness of donor assistance include changes in the geographic area under the PA jurisdiction; division of PA authority into zones with varying authority in each; changes in the PA’s revenue base; and sustained structural and economic dependency on Israel.
The fact that there are a number of security zones & delineations across the Palestinian territories (A, B and C zones) has a number of implications for progamming. These include delays and implementation due to the need to obtain permits and approval for work. Some organizations are also bound by more stringent donor policies which forbid them to travel to and work in certain geographic zones.
d Please see Part 2 of this report for a more detailed discussion of vulnerability.
45
The International Health Response
At the same time, structural and economic dependency on Israel continues. Most utilities, water, gas and electricity are still under Israeli control, which means that the PA is limited in its influence to regulate and or influence policies and prices. Operationally, this means organizations working on infrastructure development programmes are required to obtain approval and permits through long and bureaucratic processes involving joint committees set up in each sub-sector (e.g. water).
One of the main sources of revenue for the PA and therefore the MoH is taxes collected and transferred annually from the Israeli administration. Therefore any delays and/or shortfall in this revenue will have the power to cripple the PA and subsequently the MoH. At the household level, the extent of economic dependency on Israel has become evident especially since the period beginning October 2000. The implications of a decline in household purchasing power on the ability to sustain and obtain health care are summarized in Part 2.
Key questions to consider by organizations working in this context include:
• What means are available to local and international health sector providers to ensure continuity in this operating context?
• How can the international health community ensure that interventions introduced in a time of transition will be sustainable in the longer-term? What mechanisms are needed? With what inputs and levels of support?
• Given this sustained dependency on the international community what are the implications of donor fatigue on the ability of the health sector to protect the health and well being of the population?
c) The refugee question The status of the refugees living in the West Bank and Gaza Strip (some 1.4 million people) has still to be determined. This in turn means that the future of UNRWA, the primary service provider for the refugees is also to be determined.
There are a number of key questions about the presence of so large a refugee population for international health assistance.
One of the first questions is about absorption capacities. If a definitive agreement on Palestinian statehood is reached, does the West Bank and Gaza Strip have the capacity to absorb more than 3 million refugees currently dispersed throughout the region? If no, what are the implications of this vis-à-vis continued dependency on external assistance?
The refugee community as a proportion of the total population is considerable (30% on the West Bank and >75% in the Gaza Strip). What are the implications of humanitarian assistance on social stability given that a majority of the refugees are integrated within local communities? Key questions in this regard include:
• Given that the refugees have their own primary service provider, what are the implications for equity and accessibility of services between refugees and non-refugees?
• Almost half of the refugees (46%) live outside of the camps and are integrated within larger Palestinian communities. What are the implications of targeted assistance on social stability in this context especially where the needs of both refugees and non-refugees are acute?
• Is there a risk for the potential “ghettoization” of the refugee communities especially for those living inside the camps?
• How can the international community ensure that targeted assistance to this population segment is fair, equal and does not undermine social stability?
46
The International Health Response
External factors External factors are global factors that have the power to influence external assistance in the West Bank and Gaza Strip. The redirection of external assistance to another humanitarian crisis (e.g. Afghanistan) is one example. Although this may not be an area that international health interventions can typically address, it does have implications on the continuity and potentially sustainability of interventions.
One element that has the power to potential steer external assistance to and from the West Bank and Gaza Strip is the media. This is seemingly less of a concern than expressed, for example, in Kosovo where there was a feeling that “everyone was trying to get on the humanitarian bandwagon” as a result of the high media coverage given the crisis. Although the media does have the power to influence donor and international interests in the health sector through the interests of its broader constituencies, it seems that there has been no sudden influx in the number of organizations working in the Palestinian territories. It seems that many organizations recognize the protracted nature of this crisis and are ware of the socio-economic and political complexities inherent in it.
As the same time, the high profile media status of the Israeli/Palestinian conflict does have implications for the international health response:
• If the crisis continues in its current protracted form, what are the implications of a shift in focus to a more “acute” emergency especially given the current level of dependency on external assistance?
• What will this do for service provision, especially for UNRWA who is entirely funded by voluntary donor contributions?
• If the crisis escalates, what are the risks of over-humanitarianization to future growth?
• What mechanisms can local and international health providers put in place to ensure coverage and continuity and sustainability of interventions?
Factors inherent in the international aid system These factors are systemic factors that limit and/or constrain the effectiveness of international assistance in the health sector. They are rooted in the way in which the aid system is structured and operates and are external to the Palestinian context.
a) Coordination One of the main factors that has the potential to enhance and or undermine the effectiveness of external assistance in the health sector is weak coordination.
The overall coordination mechanism in the West Bank and Gaza Strip is both extensive and complex as shown in Figure 3.3.
Established in 1993, this structure was intended to be a vehicle for the PA and donors to facilitate coordination between the PA and international community as well as within the international community itself. The tasks were numerous and included addressing the short and medium term needs in a complex and unpredictable an environment; laying the foundations for PA management of development assistance; and linking practical operational issues with policy and decision making.
The Ad-Hoc Liason Committee was established in October 1993 and was charged with the responsibility of mobilizing international support for the West Bank and Gaza Strip; ensuring linkages with the Middle East Peace Process; and promotion of policy dialogue. It is a 12 member committee and is the principle policy-level coordination mechanism for the Palestinian reconstruction and development programme.8
47

The International Health Response
Figure 3.3: General coordination mechanisms in the Palestinian territories.
Steering committeeMultilateral Track, Middle East Peace Process
Multilateral Working Groups•Arms Control and Regional Security (ACRS)•Environment•Refugees (RWG)•Regional Economic Development•Water
Ad-hoc Liaison Committee (AHLC)World Bank
Consultative Group (CG)
UN Special Coordinator’s Office (UNSCO)
Join Liaison Committee (JLC)
Task Force on Project Implementation
Local Aid Coordination Committee (LACC)
Sector Working Groups (SWGs)
•Police•Private Sector•Public Finance•Tourism•Transportation & Communications
•Agricullture•Education•Employment Generation•Environment•Health•Institution Building
•Holst Fund•Technical Assistance Trust Fund (TATF)•Investment Programme
Senior representatives of major donors.
(Secretariat)(Chair)
PA and local representatives.
Israel, PA and local representatives of major donors.
PA and local donor representatives and UN agencies.
Adapted from The (very) political economy of the West Bank and Gaza, Rex Bryan; and Donor Investment in Palestinian Development 1994 – 1998, World Bank and UNSCO, 2000.
Steering committeeMultilateral Track, Middle East Peace Process
Multilateral Working Groups•Arms Control and Regional Security (ACRS)•Environment•Refugees (RWG)•Regional Economic Development•Water
Ad-hoc Liaison Committee (AHLC)World Bank
Consultative Group (CG)
UN Special Coordinator’s Office (UNSCO)
Join Liaison Committee (JLC)
Task Force on Project Implementation
Local Aid Coordination Committee (LACC)
Sector Working Groups (SWGs)
•Police•Private Sector•Public Finance•Tourism•Transportation & Communications
•Agricullture•Education•Employment Generation•Environment•Health•Institution Building
•Holst Fund•Technical Assistance Trust Fund (TATF)•Investment Programme
Senior representatives of major donors.
(Secretariat)(Chair)
PA and local representatives.
Israel, PA and local representatives of major donors.
PA and local donor representatives and UN agencies.
Adapted from The (very) political economy of the West Bank and Gaza, Rex Bryan; and Donor Investment in Palestinian Development 1994 – 1998, World Bank and UNSCO, 2000.
The Consultative Group (CG) consists of the PA and nearly 50 bilateral and multilateral donors. The CG meets annually to discuss development investment priorities, programming, and donor support.
The Local Aid Coordination Committee (LACC) is co-chaired by the Norwegian Government, the World Bank and UNSCO. The LACC addresses planning and aid coordination issues on the ground.
Sector Working Groups (SWG) were established in each sector. The SWGs are managed by a Gavel Holder, usually the line ministry; a Shepherd, usually the major donor in that sector; and a Secretariat, usually the leading agency working in that sector. In the case of health, the Gavel Holder is the MoH; the Shepherd is the Italian Government and the Secretariat is the World Health Organization.
UNSCO is coordinator of the UN agencies working in the West Bank and Gaza Strip. UNRWA, as the main provider of relief and community services, is one of the leading humanitarian agencies.
48
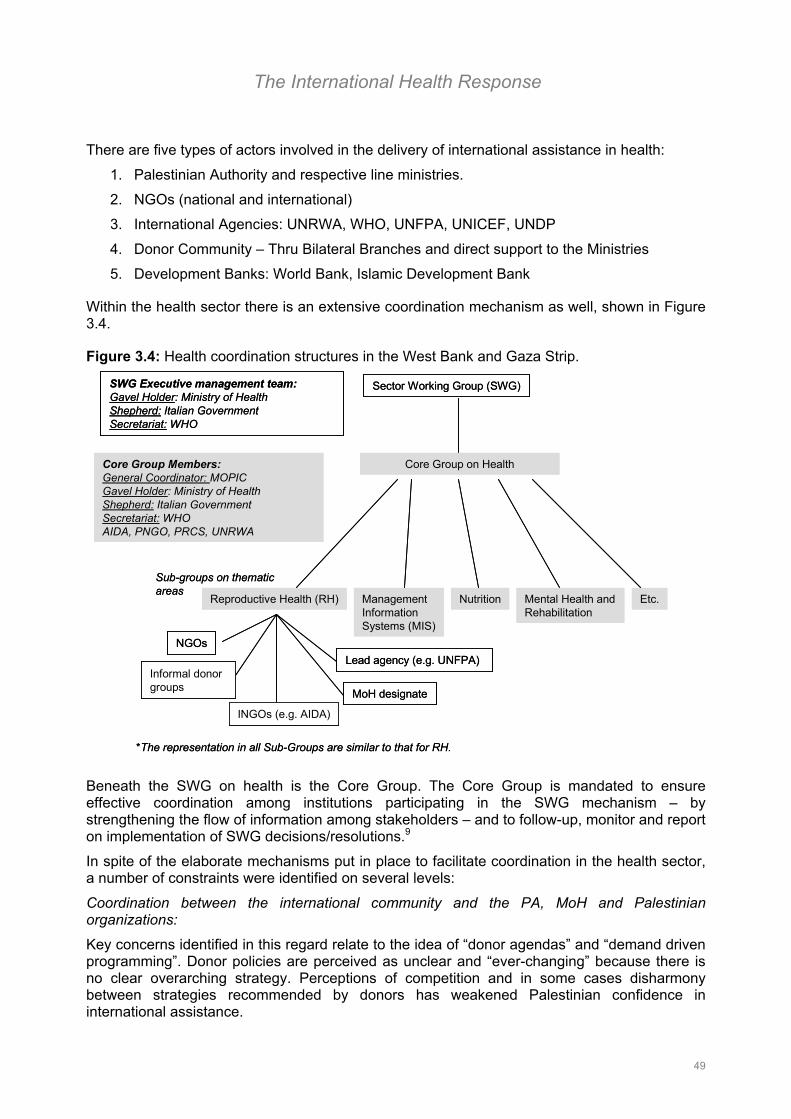
The International Health Response
There are five types of actors involved in the delivery of international assistance in health:
1. Palestinian Authority and respective line ministries.
2. NGOs (national and international)
3. International Agencies: UNRWA, WHO, UNFPA, UNICEF, UNDP
4. Donor Community – Thru Bilateral Branches and direct support to the Ministries
5. Development Banks: World Bank, Islamic Development Bank
Within the health sector there is an extensive coordination mechanism as well, shown in Figure 3.4.
Figure 3.4: Health coordination structures in the West Bank and Gaza Strip.
Sector Working Group (SWG)
Core Group on Health
Sub-groups on thematic areas
Reproductive Health (RH) ManagementInformationSystems (MIS)
Nutrition Etc.
NGOsLead agency (e.g. UNFPA)
MoH designate
SWG Executive management team:Gavel Holder: Ministry of HealthShepherd: Italian GovernmentSecretariat: WHO
Core Group Members:General Coordinator: MOPICGavel Holder: Ministry of HealthShepherd: Italian GovernmentSecretariat: WHOAIDA, PNGO, PRCS, UNRWA
*The representation in all Sub-Groups are similar to that for RH.
INGOs (e.g. AIDA)
Informal donor groups
Mental Health and Rehabilitation
Sector Working Group (SWG)
Core Group on Health
Sub-groups on thematic areas
Reproductive Health (RH) ManagementInformationSystems (MIS)
Nutrition Etc.
NGOsLead agency (e.g. UNFPA)
MoH designate
SWG Executive management team:Gavel Holder: Ministry of HealthShepherd: Italian GovernmentSecretariat: WHO
Core Group Members:General Coordinator: MOPICGavel Holder: Ministry of HealthShepherd: Italian GovernmentSecretariat: WHOAIDA, PNGO, PRCS, UNRWA
*The representation in all Sub-Groups are similar to that for RH.
INGOs (e.g. AIDA)
Informal donor groups
Mental Health and Rehabilitation
Beneath the SWG on health is the Core Group. The Core Group is mandated to ensure effective coordination among institutions participating in the SWG mechanism – by strengthening the flow of information among stakeholders – and to follow-up, monitor and report on implementation of SWG decisions/resolutions.9
In spite of the elaborate mechanisms put in place to facilitate coordination in the health sector, a number of constraints were identified on several levels:
Coordination between the international community and the PA, MoH and Palestinian organizations:
Key concerns identified in this regard relate to the idea of “donor agendas” and “demand driven programming”. Donor policies are perceived as unclear and “ever-changing” because there is no clear overarching strategy. Perceptions of competition and in some cases disharmony between strategies recommended by donors has weakened Palestinian confidence in international assistance.
49

The International Health Response
At the same time, questions of absorption capacity vis-à-vis the ability of the Palestinian authorities to operationalize health interventions has undermined confidence in the PA/MoH.e
Some key questions identified with respect to coordination between the international community and the Palestinians include:
• To what extent are national and international policies understood? Are they widely known and communicated?
• How are perceptions of “donor driven agendas” influencing ownership, endorsement, commitment to and sustainability of programmes and strategies? What can be done to mitigate potential negative consequences of this perception?
• To what extent is competition impacting coordination especially where there is the perception that there are too many players in the health sector?
• What are the consequences of “non-coordination” in the health sector? And how might this reverse perspective influence decision making?
• Coordination is one thing; implementation is another. How much attention has been given to evaluating the effectiveness of cooperation and implementation?
• To what extent can the Palestinians influence coordination (as the beneficiaries)? How participatory are coordination processes?
• Who’s responsibility is it to ensure effective coordination in the health sector?
Coordination within the international community:
Coordination within the international community itself has been characterized as adequate and duplication has been kept to a minimum, but there is some uncertainty as to the effectiveness of the coordination. Is this communication or cooperation?
Coordination within the health sector (i.e. through the SWG, the Core Group and Thematic Groups) appears to be the most proactive, however, even in this sector there are concerns about divergent and varying agendas/approaches to the crisis. The consequences of this may result in programmatic discord.
Key questions to consider with respect to coordination within the international community include:
• What are the consequences of donor “disharmony” for health sector development? What mechanisms could be put in place and/or strengthened that would ensure harmony between international health interventions?
• Given all the international actors working in the health sector, is there a need for a clear lead agency? If yes, what criteria would be used to determine who to take that lead? What would their role be?
• Information was cited as one of the key factors that might enhance coordination. This would include sharing of information about the overall health situation as well as information about operations and activities, i.e. who is doing what, where and how. To what extent is competition influencing sharing of this type of information? Are there mechanisms that could be put in place and/or strengthened to reduce/eliminate this threat?
• To what extent do internal organizational constraints (such as lengthy procurement procedures, reporting requirements, bureaucratic disbursement mechanisms and operational interests/policies) affect coordination? In the absence of transparency about these organizational constraints, assumptions have been made about the flexibility,
50
e (See page 43 for a more detailed discussion about this point.)
The International Health Response
capacity and interests of donors working in the health sector. Failure to live up to these expectations has undermined confidence between partners. How could these operational limitations be more openly communicated? What mechanisms could be put in place that would ensure coverage in spite of these organizational limitations?
• Do ground rules need to be set for more effective coordination?
Tensions seem to exist between the International NGO (INGO) community and the Palestinian NGO community. Coordination structures between them appear to be weak. There is also a feeling that the NGO community is isolated from the donor and international agency deliberations.
• To what extent should INGO and NGO participation be involved in health policy making?
• To what extent should INGO and NGO participation be involved in decision making about international interventions in the health sector, especially since NGOs are one of the four primary service providers in health?
• What mechanisms exist to incorporate INGO/NGO perspectives in overall coordination of the health sector? Are they adequate? If no, how might they be strengthened?
b) Information Information is the second key factor affecting the overall impact of the international response first because of its implications for strategic planning and second because of its implications for coordination.
There is an abundance of health data in the Palestinian territories. At the same time, the West Bank and Gaza Strip is said to be data rich and information poor. There is no clear policy on data collection, analysis and dissemination in the health sector. Consequently there is no centralized source for health data. Tools are not harmonized between health sector providers (MoH, NGO and UNRWA) as well as between international organizations. In some cases, such as IMR, there are broad discrepancies between figures reported.
• What are the implications of a lack of reliable health indicators on the design and planning of health interventions?
• How might this affect evaluation efforts to gauge the effectiveness of interventions?
• If efforts were introduced to centralized and harmonize health data (already under way by the MoH through the establishment of a health data warehouse), what obstacles might be encountered? How might they be overcome?
• What mechanisms, tools and processes currently exist for health intelligence? Are they adequate? If no, what mechanisms, tools and processes could the international community support in the Palestinian territories to enhance this?
• How do differences between tools, methodologies and strategies used by the international community to gather and analyze health intelligence influence the overall impact of the health sector response?
• How is health information used for planning and decision making? I.e. how are priorities determined? By whom?
• What information and tools are currently available for health planning? Are they adequate?
Information related to activities in the health sector is also an issue of concern. Numerous tools exist (maps, databases, assessments and surveys), however little seems to be centralized in any one source be it the MoH, MOPIC or implementing agency. Key questions in this regard include:
51
The International Health Response
• How can information related to activities going on in the health sector be better disseminated between health actors? Through what forums and/or mechanisms?
• Is the current level of information sufficient or are additional tools and analysis needed?
• Who should be responsible for managing this information/intelligence?
3.3 Discussion
Rather than go into specific recommendations for the international and local health community on how to address these issues and meet the needs of the most vulnerable, this report aims to stimulate dialogue between actors working within the health sector. Therefore an attempt tp provide concrete recommendations and alternatives solutions is not made.
It is clear that some of the constraints identified in the report cannot necessarily be directly influenced by the health sector. For example, some of the contextual factors (closure) will remain until a broader political settlement is reached. At the same time, there are other areas related to the systemic and structural factors outlined in this report that can be influenced.
Are the needs emergency, development or somewhere in between? One of the main themes to have emerged in this report is that of the dual nature of the current health and health sector needs in the West Bank and Gaza Strip. On the one hand, there are pockets of acute vulnerability which require urgent and immediate relief interventions. At the same time, there are a number of problems rooted deep within the development and therefore functioning of the health sector that also need addressing. Many of these deep rooted problems (related to structure, policy and operational capacity) require much longer developmental approaches (e.g. health policy reform, rationalization of health care resources, etc.). Balancing these two needs in so uncertain and complicated an environment has proved to be one of the most difficult challenges for local and international health care providers.
Tools for decision making: An exercise
Following is an example of a decision making grid developed by the working group participants which considers solutions to the problem of access – of the population to health care facilities. The aim of this exercise was to identify a solution that would solve the immediate problem (of ensuring coverage) and would meet (and/or not undermine) medium and long-term needs.
Four suggested solutions include:
1. Humanitarian convoys
2. Mobile clinics
3. Upgrading of remote clinics, equipment and skills
4. Enhanced transfer of patients between existing facilities
For each solution questions were raised as to the short, medium and long-term potential impacts. What are the negative potential consequences of implementing the suggested solution? What risks and/or obstacles might be encountered that could undermine the effectiveness of the suggested solution?
52
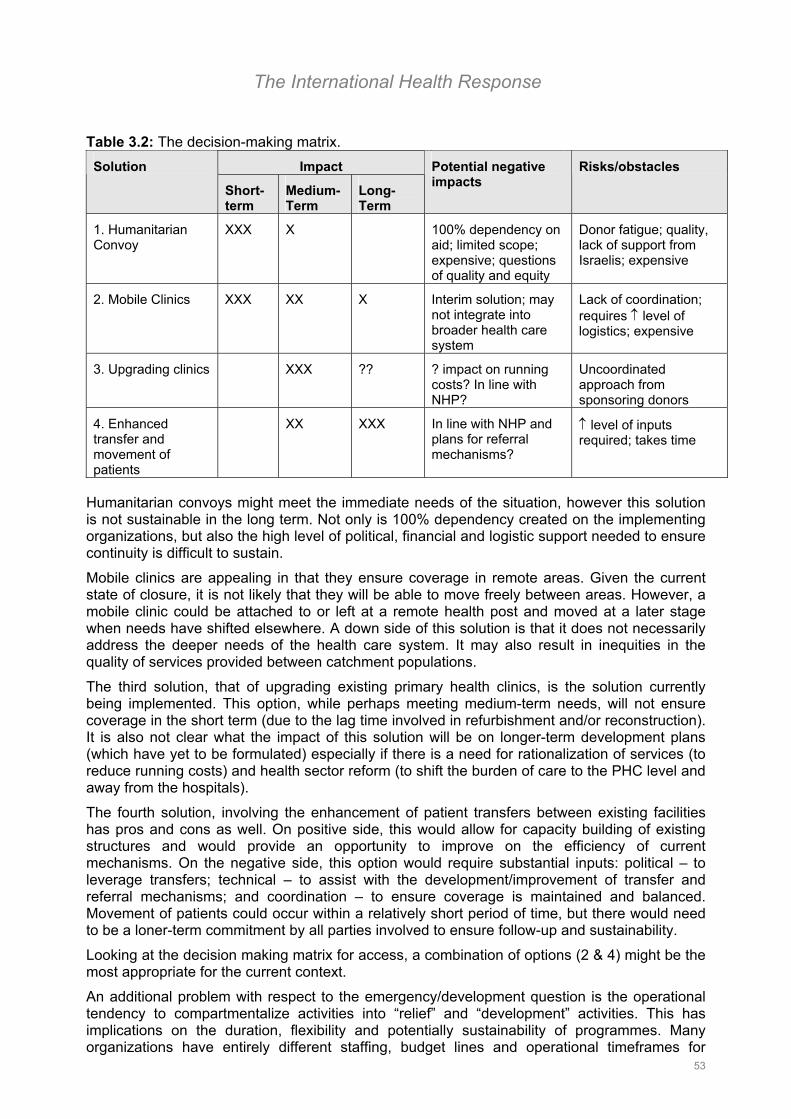
The International Health Response
Table 3.2: The decision-making matrix. Impact Solution
Short-term
Medium-Term
Long-Term
Potential negative impacts
Risks/obstacles
1. Humanitarian Convoy
XXX X 100% dependency on aid; limited scope; expensive; questions of quality and equity
Donor fatigue; quality, lack of support from Israelis; expensive
2. Mobile Clinics XXX XX X Interim solution; may not integrate into broader health care system
Lack of coordination; requires ↑ level of logistics; expensive
3. Upgrading clinics XXX ?? ? impact on running costs? In line with NHP?
Uncoordinated approach from sponsoring donors
4. Enhanced transfer and movement of patients
XX XXX In line with NHP and plans for referral mechanisms?
↑ level of inputs required; takes time
Humanitarian convoys might meet the immediate needs of the situation, however this solution is not sustainable in the long term. Not only is 100% dependency created on the implementing organizations, but also the high level of political, financial and logistic support needed to ensure continuity is difficult to sustain.
Mobile clinics are appealing in that they ensure coverage in remote areas. Given the current state of closure, it is not likely that they will be able to move freely between areas. However, a mobile clinic could be attached to or left at a remote health post and moved at a later stage when needs have shifted elsewhere. A down side of this solution is that it does not necessarily address the deeper needs of the health care system. It may also result in inequities in the quality of services provided between catchment populations.
The third solution, that of upgrading existing primary health clinics, is the solution currently being implemented. This option, while perhaps meeting medium-term needs, will not ensure coverage in the short term (due to the lag time involved in refurbishment and/or reconstruction). It is also not clear what the impact of this solution will be on longer-term development plans (which have yet to be formulated) especially if there is a need for rationalization of services (to reduce running costs) and health sector reform (to shift the burden of care to the PHC level and away from the hospitals).
The fourth solution, involving the enhancement of patient transfers between existing facilities has pros and cons as well. On positive side, this would allow for capacity building of existing structures and would provide an opportunity to improve on the efficiency of current mechanisms. On the negative side, this option would require substantial inputs: political – to leverage transfers; technical – to assist with the development/improvement of transfer and referral mechanisms; and coordination – to ensure coverage is maintained and balanced. Movement of patients could occur within a relatively short period of time, but there would need to be a loner-term commitment by all parties involved to ensure follow-up and sustainability.
Looking at the decision making matrix for access, a combination of options (2 & 4) might be the most appropriate for the current context.
An additional problem with respect to the emergency/development question is the operational tendency to compartmentalize activities into “relief” and “development” activities. This has implications on the duration, flexibility and potentially sustainability of programmes. Many organizations have entirely different staffing, budget lines and operational timeframes for
53
The International Health Response
emergency and development programmes. The fact that the situation in the West Bank and Gaza Strip falls somewhere in between has posed unexpected challenges for those organizations mandated to work in one context or the other.
As the potential for a “true” humanitarian emergency grows, there has been more and more discussion about the need for a humanitarian contingency plan. At the beginning of the crisis (October 2000) the MoH and PA requested that a Humanitarian Task force be established to help plan for and cope with predicted emergency needs. This task force would consist of a primary unit (the Humanitarian Task Force on Emergency Needs (HTFEN)) and field coordination subgroups – one in Gaza and one in the West Bank. This structure failed due to a lack of overall support, and UNOCHA is actively seeking an alterative structure to take its place.
Evaluating the effectiveness of the response The need for a clear plan of action and strategy for the health sector has been a second major theme of this report. This plan is needed to align national and international health initiatives as well as outline ways in which to address immediate and long-term development needs.
Another key element inherent in the development of a sector wide plan is the development of targets and measures by which to measure progress in its implementation. Key questions that this might address include:
• How well are interventions meeting their targets?
• Are they delivered in a timely fashion?
• Are they having the desired affect?
• Are they being implemented in the most effective and efficient manor?
• What are the impressions of the beneficiaries (the ultimate client) and authorities about the effectiveness of interventions? Efforts have been made to consider this for specific projects and within organizations, however no such effort has been made to gauge the overall effectiveness of the health sector response?
In the absence of a clear sector wide strategy, there will continue to be no operating framework in which to measure the performance of external assistance in the health sector in the West Bank and Gaza Strip. Mechanisms to measure performance and capitalize on lessons learned, would greatly enhance the potential of external assistance to promote a smooth transition in the health sector.
1 MOPIC Quarterly Report, June 2001. 2 “The Palestinian Territories” in Good Intentions: Pledges of Aid fro Post-Conflict Recovery, edited by S Forman and S Patrick, Center on International Cooperation, NYU, 2000. 3 IBID, 2000. 4 IBID, 2000. 5 IBID, 2000. 6 IBID, 2000. 7 IBID, 2000. 8 Donor Investment in Palestinian Development: 1994- 1998, Prepared by the World Bank and UNSCO, 2000. 9 Terms of Reference for the Core Group for Health, presented to the SWG on Health on the 12 of July 2001 in Gaza.
54
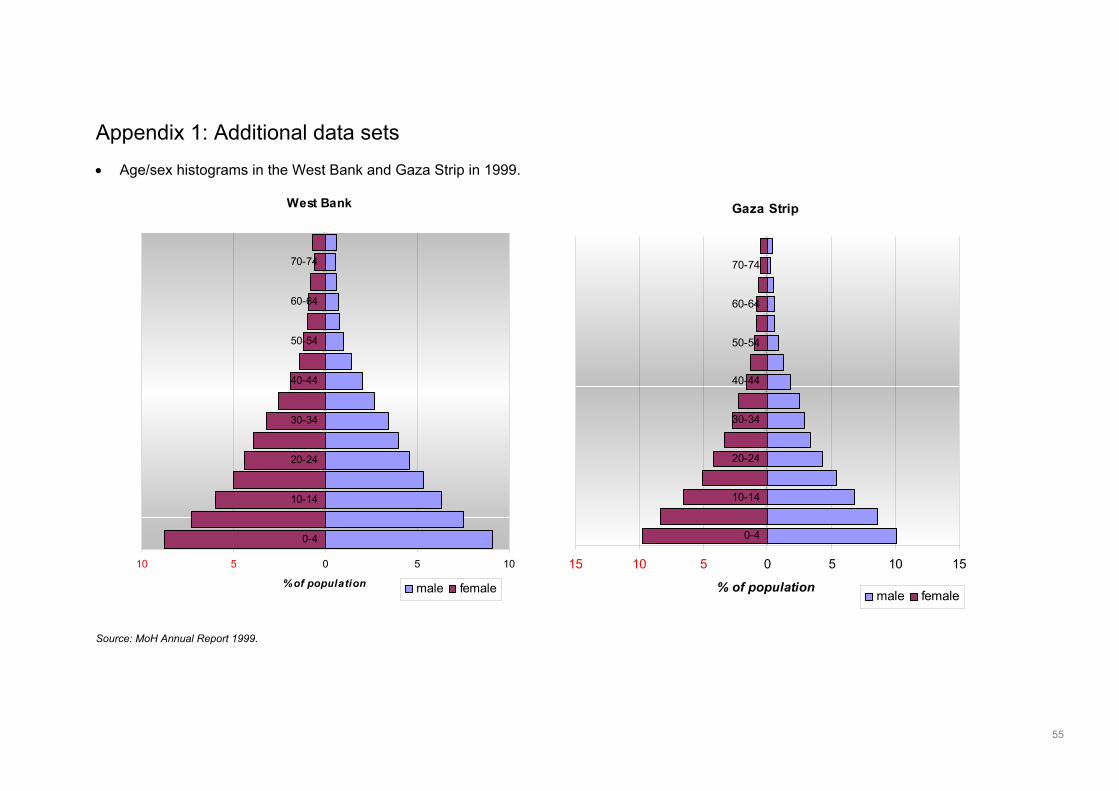
Appendix 1: Additional data sets • Age/sex histograms in the West Bank and Gaza Strip in 1999. Source: MoH Annual Report 1999.
West Bank
0 5 10
0-4
10-14
20-24
30-34
40-44
50-54
60-64
70-74
% of population male female
Gaza Strip
0 5 10 15
0-4
10-14
20-24
30-34
40-44
50-54
60-64
70-74
% of population male female
10 5 15 10 5
55

• Reported infectious diseases in 2000 (as listed in the MoH Annual Report for 1999). Diseases notified on a daily basis
West Bank Gaza TotalMeningitis 297 1827 2124Food Poisoning 729 177 906Accute Flaccid Paralysis 9 1 10Tetanus 3 6 9Measles 4 1 5AIDS 3 1 4Cholera 0 0 0Diptheria 0 0 0Plague 0 0 0H. Fever 0 0 0Poliomyelitis 0 0 0Rabies 0 0 0
Diseases notified on a weekly basisWest Bank Gaza Total
Gonorrhea 0 0 0Syphilis 0 0 0
Other 4535 194 4729
Hep A 1303 566 1869Hep B 1247 970 2217Hep C 173 73 246
Rickettsial Diseases (Typhus) 0 927 927Chemical posioning 329 229 558Brucellosis 272 31 303Typhoid and Paratyphoid 35 203 238
Cutaneous 115 1 116Visceral 11 0 11
Rubella 55 44 99Tuberculosis 29 18 47Pertussis (Whooping Cough) 8 18 26Encephalitis 4 0 4Malaria 1 2 3Lasa fever 0 0 0Leprosy 0 0 0Yellow Fever 0 0 0
Hepatitis
Sexually Transmitted Diseases
Leishmaniasis
Diseases notified on a monthly basisWest Bank Gaza Total
Ameobiasis (trophozoite) 837 9448 10285Giardiasis trophozoite 32 5938 5970Chicken Pox 534 3886 4420Scabies 152 3777 3929
Oxyuriasis 1507 1337 2844Asacariasis (round Worm) 62 2140 2202
Strongyloidiasis 0 216 216Bites - snakes & Scorpions 982 16 998Shigellosis 558 22 580Mumps 358 168 526Septicemia 200 187 387Rheumatic Fever 1 313 314Toxoplasmosis 1 96 97Herpes - zoster & simplex 81 0 81Scarlet Fever 2 5 7Hydated Cyst 6 0 6Taeniasis (beef & pork worm) 1 0 1Bilharzia 0 0 0
Intestinal Parasitic diseases
56
Appendix 2: List of key persons consulted Individual Title, Organization Abdul Munem Salem Programme Management Officer, Environment and Infrastructure
Unit, UNDP Annie Ervard French Cooperation Aqil Abu Shammala Chief, Field Relief and Social Services Programme, UNRWA -
Gaza Asad Ramlawi Director Preventative Medicine Ayyoub El-Alem Chief Field Health Programme, UNRWA – Gaza Bertrand Bainvel Programme Officer, UNICEF Claudio Giubbo Italian Cooperation, Emergency Programmes Coordinator Munther Sharief Deputy Minister of Health Elizabeth Cousens Chief, Donors Affairs Unit, UNSCO Emad Shaat Director General, International Aid Coordination, MOPIC Fathi Arafat Honorary President, PRCS Fathi Abumoghli Health System Development Project Coordinator, MoH Fawaz Abu Ziyada Field Health Assistant, WHO– Gaza Florence Baingana Mental Health Specialist, World Bank Giuseppe Masala WHO Health Coordinator, West Bank and Gaza Grigor Hovhannisyan Team Leader Palestine Mission, UNOCHA Hassan Basharat Coordinator, Disaster Management and Coordination Unit, PRCS Irene Anne Jillson President, PRI Incorporated Jean Breteche Delegate, European Commission Jean Marie Stratigos UNSCO Jean McCluskey Public Health Engineer, Technical Programme Coordinator,
OXFAM Jean-Bernard De Milito Food Security Officer, ECHO Jens Mjaūgedal Norwegian Development Agency Jihad Mishal Director General, UPMRC Kamal Zaineh Union of Health Care Workers Khaled M. Doudine Senior Programme Advisor & General Coordiantor West Bank &
Gaza, ILO Khalid Jondeh General Director, PRCS; Deputy Al Quds Hospital Laila Baker Programme Officer, UNFPA Lama Jamjoun Director of Research, HDIP Luay Shabaneh Deputy Assistant of President for Technical Affairs, PCBS Mahdi F. Abdul – Hadi Head, PASSIA Marc Jessel Project Manager, Health Sector, British Council Marco Barone Italian Cooperation Marieke Feitsma Programme Management Officer, Environment and Infrastructure
Unit, UNDP Mirca Barbolini Health Expert, MEDA Team, European Commission Mustafa Barghouthi Director, HDIP Mustaq Quereshi Country Director, WFP Nader Atta Programme Management Officer, Environment and Infrastructure
Unit, UNDP Nadim Al-Adili Health Officer, UNICEF Naema Mabed Field Health Assistant, WHO – Gaza Ola Farah Awad Director, Projects Coordination Department, PCBS Omar Abu Argoub Director of MIS, MoH Othman Karameh Medical Officer, WHO Paola Cirillo Humanitarian Affairs Officer, UNOCHA
57

Pierre Poupard Country Representative, UNICEF Rafik Zanoun National Programme Officer, WHO – Gaza Ray Dolphin Humanitarian Affairs Officer, UNOCHA Salam Kanaan Education & Health Operations Analyst, World Bank Sally Aires AIDA, Oxfam Samia Bamieh Director of the UN Department, MOPIC Sherry Carlin Health Officer, General Development Office, USAID Stefano Mocci Information Officer, World Bank Stuart Shepard MAP-UK Timothy Rothermel Resident Representative, UNDP Zeina Mogarbel European Commission
58
Appendix 3: Essential reading list Title/Document Year
Published Period
covered Published BY Authors key words
Strengthening Palestinian Public Institutions - executive summary.
1999 Council on Foreign Relations
Rochard M, Siegman H, Sayigh Y, Shikaki K
assessment, public institutions, governance, transparency, accountability
Palestinian Children - Five years under Palestinian National Authority
Apr-00 annual report PCBS Child Statistics Programme
child health
The situation of Palestinian Children in the West Bank and Gaza Strip; Jordan, Syria and Lebanon - An assessment based on the UN Convention of the Rights of the Child
2000 UNICEF - Regional Office for the Middle East and North Africa
children and the convention on the rights of the child
The situation analysis of Palestinian Children, young people and women in the West Bank and Gaza Strip
Aug-00 UNICEF - Regional Office for the Middle East and North Africa; MOPIC
children and the convention on the rights of the child
West Bank and Gaza Service Delivery Survey - Health and Basic Education Services
Dec-98 PA, CIET International, World Bank, HDIP, PCBS
Cockcroft, Anne consumer perceptions of health services, utilisation of health care services
Impact of the Israeli Measures: Survey on the well-being of the Palestinian Children, Women and the Palestinian Household (Press conference on the survey results)
Jul-01 November 2000- May 2001
Palestinian Central Bureau of Statistics (PCBS)
dislocation, maternal health, mental health, health care services, education services, mass media, deaths and injuries
Quarterly Monitoring Report of Donor assistance annual Ministry of Planning and International Cooperation (MOPIC) Aid coordination department
donor assistance
59
Title/Document Year Published
Period covered
Published BY Authors key words
Development Under Adversity - The Palestinian Economy in Transition (SUMMARY)
1993-1997 Palestinian Economic Policy Research Institute (MAS) and the World Bank
Editors: Diwan, I and Shaban, R.A.
economic prospects, strategic development choices, risks and roles of donors/aid
Donor Investment in Palestinian Development 1994 - 1998
1999 1994-1998 World Bank and UNSCO
evaluation of donor assistance
“The Palestinian Territories” in Good Intentions: Pledges of Aid fro Post-Conflict Recovery
2000 1994 - 1998 Center on International Cooperation, New York Univeristy
edited by S Forman and S Partick
evaluation of donor assistance
Strengthening Public Sector Management - West Bank and Gaza
1999 World Bank - Social and Economic Development Group, Middle East and North Africa Region (MENA)
fiscal outlook, PA civil service, public service delivery (role of NGOs and private organizations), local government and utility reform
The Palestinian Health System: An Updated Overview Mar-00 Health, Development, Information and Policy Unit (HDIP)
Barghouthi M, Shubita A, Fragiacomo L
health care system, health policy, health specific data
Health Insurance and health service utilization in the West Bank and Gaza Strip
Feb-98 Health,Development, Information and Policy Unit (HDIP)
Lennock J and A Shubita
health insurance; health services utilization
Health Insurance and utlization of health care institutions - Part of The Health Survey in the West Bank and Gaza Strip 1996
Sep-99 Palestinian Central Bureau of Statistics (PCBS)
health insurance; health status
National Strategic Health Plan 1998 Ministry of Health - Palestinian National Authority
health policy in Palestine
60
Title/Document Year Published
Period covered
Published BY Authors key words
West Bank and Gaza: Medium-term development strategy for the health sector
1998 MoH, Worldbank, WHO
health sector reform, demographic & health status, health services overview, health financing
The Status of Health in Palestine – Annual Report 1999
Sep-00 1999 Palestine NationalAuthority – Minsitry of Health
health status
Health Survey 2000 – Main Findings Nov-00 Palestinian Central Bureau of Statistics (PCBS)
health status
Health Sector Strategy Paper for the West Bank and Gaza Strip
Aug-99 DfID Health Mission health status, health sector reform, DfID programme overview and proposed areas of activity
Health and Palestine: Potential and Challenges Mar-97 Palestine Economic Policy Research Institute (MAS) Discussion Paper; HDIP
Barghouthi M, Lennock J
health status, health services, health insurance, financial policy, obstacles to the establishment of an effective health care system
Palestine Human Development Profile 1996-1997 1997 Bir Zeit University and MOPIC
human development
Report of the Director-General – International Labour Conference 89th Session 2001 (Appendix: Report on the Situation of workers of the occupied Arab territories)
May-01 ILO labour legislation, insdustrial relations, social security, economy and the labour market, technical cooperation
Drug Situation Analysis for the West Bank and Gaza Strip
2000 WHO – Department of Essnetial Drugs and Medicines Policy
pharmaceutical profile, availability, drug use, economics and financing, overview of local industry
West Bank and Gaza Update: Quarterly Publication of the World Bank Group
Jun-01 Worldbank poverty maps, economic trends, World Bank operations
61
Title/Document Year Published
Period covered
Published BY Authors key words
International and Local Aid during the second Intifada Jul-01 Feb - June 2001
Graduate Institute of Development Studies, University of Geneva
Bocco, R; Brunner M; Rabah J
public opinion; effectiveness of international assistance; intifada
Annual Report of the Department of Health of UNRWA annual UN Relief and Works Agency for Palestine Refugees in the Near East
refugee health
Settlements and the Final Status Talks Mar-01 Palestinian Academic Society for the Study of International Affairs (PASSIA)
settlements
62





























