Embed Size (px)
Citation preview
Original articles Oral medicine
Oral hairy leukoplakia:observations in 95 cases andreview of the literatureReichart PA, Langford A, Gelderblom HR, Pohle HD, Becker J, Wolf H; Oralhairy leukoplakia; observations in 95 cases and review of the literature, J OralPathol Med 1989; 18; 410-415.
Oral hairy leukoplakia (HL) was observed in 25.4% of 373 HIV-seropositivepatients (« = 95). 87 were men of an average age of 37.1 yr, 8 were women(30,3 yr). 71.6% of the patients were male homosexuals. At initial diagnosis ofHL the majority of cases was elassified as CDC IVc, (45,3%) and CDC II(22,1%), Average CD4/CD8 ratio {n = 19) was 0,24 with a range of 0,04-1,0,Thirty biopsies of HL revealed some of the histologic features thought to becharacteristic. In only 20 of 30 biopsies EB-virus-specific-capsid antigen wasdetected. The problems of clinical and histological diagnosis of HL arediscussed. Further strict criteria are necessary in order to define HL more 'distinctly.
Peter A. Reichart\Angelika Langford\Hans R. Gelderblom^Hans-Dieter Pohle^Jijrgen Becker\ Hans Wolf^Abteilung fur zahnarztliche Chirurgie/Oralchirurgie - Word - Freie Universitat Bertin,^Robert Koch-lnstitut desBundesgesundheitsamtes, ^11. Innere Abteilung,Universitats-Klinlkum Rudolf Virchow, Berlin and'Max-von-Pettenkofer-institut, Munich, WestGermany
Key words; HIV infection; Epstein-Barr virus;leukoplakia, hairy.
P. A. Reichart, Abteilung fur zahnarztlicheChlrurgie/Oralchirurgie (Nord), Freie UniversitatBerlin, Fohrer Str. 15, D - 1000 Berlin 65, WestGermany
Accepted for publication June 23, 1989.
Three years after the first patients withacquired immunodeficiency syndrome(AIDS) were reported in 1981, oralhairy leukoplakia (HL) was described(1).
Clinical features and epidemiology
Oral hairy leukoplakia is clinicallycharacterized as a white lesion of thelateral border of the tongue, occasion-ally also occurring in the buccal mucosawith slightly raised, poorly demarcatedand corrugated "hairy" surface. Le-sions cannot be rubbed off and are re-ported to be usually symptomless.Hairy leukoplakia has so far not beenobserved in other mucosal areas thanthe oral (2), During recent years anumber of HL cases either as case re-ports or larger series have been re-ported from various areas of the USA,Europe and Africa (3-20),
While HL was initially observed inmale homo- or bisexual men, it has nowbeen shown to occur, though less often,in all HIV risk groups; hemophiliacs (4,8, 21), drug abusers (6, 10, 17), blood
transfusion recipients (21) and femalepartners of HIV-infected men (21). Re-cently, HL has been described in anHIV-negative patient with acute mye-Ioblastic leukemia (22) and an HIV-negative renal transplant patient (23),suggesting that HL is not a specific le-sion associated to the HIV-infection,but may be a sign of immunosuppres-sion in general.
Prevalence rates of HL vary consid-erably. Four out of 23 patients withantibodies against HIV revealed HL(17.5%) (24), Among 115 HIV-sero-positive patients 13% revealed HL(25). Among HIV-seronegative malehomosexuals {n = 492) 1% demon-strated HL (25). Of a total of 375 ho-mosexual men 28% had developed HL;it occurred in 23% of the AIDS cases,in 9% of the ARC cases and 47% inhigh risk persons (9), In a study fromBerlin, 26% of ARC patients had HL(6). In Copenhagen, 32% of 69 sero-positive asymptomatic patients, 36%and 46% of ARC and AIDS patientsrevealed HL (26), Low prevaleneerates were reported from New York(5%) and Frankfurt (4,8%) (28), None
of 30 hemophiliac patients with factorVIII or IX deficiencies revealed HL(29), In contrast, 23 of 120 consecutivepatients belonging to the i.v, drug abus-ing risk group (19%) had developedHL (17), In a study on oral manifes-tations of AIDS in Tanzania 35% of 58patients had developed HL, The male;female ratio in this cohort was 1,6 ; 1,0(20).
The average age of HIV-infected pa-tients with HL showed some variation.The average age of i.v, drug abusingItalian patients was 25 yr (range 20 to50 yr) (17), In contrast, the average ageof male homosexual patients (n = 50)was 38 yr (range from 25 to 53 yr) (13),36,6 yr (range 24 to 51 yr) (8) and 36 yr(range 22 to 65 yr) (9), Duration of HLranged from 1 to 64 months with amean of 13 months in a study of 50cases with HL (13).
The clinical features of HL vary con-siderably. 70% of patients with HL hadbilateral lesions. The total area of HLlesions ranged from 14 to 4200 mm-with a mean of 814 mm*. The degree ofintensity of HL was mild in 40% of thecases, moderate in 52 and severe in 8%
(13). While flat lesions were usually lo-cated on the inferior surface of thetongue, the more corrugated hairy le-sions were observed on its lateral bor-der (13), There is no apparent associ-ation between the size and intensity ofHL and the relative risk for subsequentdevelopment of AIDS (30), While moststudies have stated that HL is rathersymptomless, burning sensation oftongues with HL even after antimycotictherapy has been described (28), Therelation of HL to infection with HIVand the risk of developing AIDS hasbeen studied. Of 155 patients examined12 had AIDS at the time of diagnosisthe syndrome developing in an addi-tional 43 patients in 1 to 31 months.Survival analysis showed that the prob-ability of AIDS developing in patientswith HL was 48% by 16 months and83% by 31 months. As such HL wascotisidered to be a predictor of the de-velopment of AIDS (31), In this con-text it is noteworthy that HL has beenincluded in the group of secondary in-fectious diseases (group IV, subgroupC, category C-2) of the CDC surveil-lance case definition (32),
Histopathoiogy
In their original description of HLGREENSPAN et al. (1) stated that thehistopathology of HL was similar tothat of the flat wart of the skin. Thefollowing criteria were proposed; 1;keratin projections 2; some degree ofparakeratosis and acanthosis. 3; char-acteristic ballooning of cells in theprickle cell layer (pyknotic nuclei andperinuclear halos); these changes werecompared to koilocytosis as describedin dermal warts and uterine condylo-mata, 4: little or no inflammation, 5;mild epithelial atypia in some cases.
Most researchers describing histo-pathologic features of HL followed theproposed criteria. Koilocytosis, how-ever, has been used when describingcells with pyknotic or crenated nucleiwith voluminous cytoplasm with fainteosinophilia (8), as koilocytoid cells(12), as large, pale staining cells similarto koilocytes as described in uterinecondylomata (15), as cells which hadundergone cytopathic changes reveal-ing a ground glass nucleus with baso-philic nuclear inclusions, ballooning ofcytoplasm and intracellular edema(33), as well as vacuolated cells resem-bling koilocytes (13). It has been statedthat parakeratosis and subcorneal koi-locytosis are not specific for HL since
these findings have also been observedin candidiasis and leukoplakias (8), In areeent study of histologic features of 40HL cases hyperparakeratosis was ob-served in 100%, hyperplasia/acanthosisin 80%, hair-like projections in 80%,koilocytosis in 98% and lack of inflam-matory infiltrate in 78%. The absenceof Langerhans cells in HL has beenconsidered to be an important factor inthe pathogenesis of HL (38), Not alllesions exhibit all mieroscopic charac-teristics as described in the first report(13),
The role of Candida infection in HLwas of considerable interest beeauseinitially Candida infection was sup-posed to be an underlying cause of HL(1), Larger series of HL cases in whichoral smears for Candida were takenshowed varying percentage of positivesmears; 70,3% (3), 58.8% (2), 50,7%(31), 26,1% (17), Demonstration of hy-phae in PAS sections revealed presenceof Candida in; 100% (12), 66,7% (13),50% (18), 49,3% (3), 46.7% (1),46,2% (19), 43% (13),
Immunohistochemistry
DNA hybridization studies with Ep-stein-Barr virus (EBV) probes inSouthern blots demonstrated EBVDNA in epithelial cells of HL (3),Other immunohistochemical studies us-ing in situ hybridization to detect EBVDNA confirmed the presence of thisvirus in HL (16, 33, 34). However, itmust be stated that EBV DNA was alsofound in an HIV-1-seronegative patient(16). Using semithin cryosections inconjunction with the APAAP stainingteehnique, EBV capsid as well as nucle-ar antigen of EBV was demonstrated incases of HL (35), While the presence ofHPV was stated using immunohisto-chemical methods and electron-micros-copy in the first reports on HL (1, 3) itwas not revealed in subsequent studies,HIV structural proteins were detectedusing immunohistochemistry (36),
Electron microscopy
Electron microscopic studies have re-vealed the presence of herpes type vi-rus with clusters of nucleocapsids lo-cated in nuclei and enveloped completeparticles occurring in the cytoplasm andextracellular spaces (1, 11, 12, 15, 17,18, 35), In addition, tubuloreticularstructures as well as membrane differ-entiations were revealed in HL (12,35), Cristalline inelusions in epithelial
Oral hairy leukoplakia 411
cells of HL have recently been de-scribed (37),
Treatment
While most investigators do not con-sider HL to be a clinical conditionwhich requires therapy, some reportson the effect of treatment have beenpublished. Thus, HL has been shown todisappear during acyciovir therapy (7,19) and resolution has occurred follow-ing therapy with DHPG (39), anothernucleoside analogue, topical vitamin Aacid (28) and following azidothymidinetherapy (AZT) (4, 21)". After discontin-uation of therapy recurrence was ob-served in all responders.
Material and methods
During a period of 5 yr 373 HIV-sero-positive patients (326 men, 47 women)of an average of 36,2 years were exam-ined for the presence of HL (CDC II;25%, CDC III; 9%, CDC IVa; 12%,CDC IVb-e; 54%), Clinical diagnosiswas based on the presence of white,non-removable patches on the lateralborder of the tongue in accordancewith the original description of HL (1),In eases of oral candidiasis involvingthe HL lesion, either a topical (micona-zote) or systemic antimycotic treatment(ketokonazole) was administered. Thediagnosis of HL was made in thosecases where a whitish lesion at the lat-eral border of the tongue persisted af-ter a minimum of 10 days in spite of thisantimycotic regimen, A number of pa-rameters were recorded; 1; sex. 2; age,3; risk group, 4; period of observation,5; CDC-classification, 6; CD4/CD8-cellratio, 7; regression in relation to ther-apy, 8: deaths occurring during obser-vation. 9; smears for oral Candida in-fection.
In addition, biopsies of HL were tak-en from 30 patients. Specimens weredivided and one part was fixed in for-malin for routine histology (H & E,PAS), The other part was deep frozenin liquid nitrogen. For the immunohis-tochemical detection of EBV-capsidantigen (EBV-VCA, BcLFl pl50)cryostat sections of 3-4 ^m were air-dried for 2 h and fixed in acetone for 15min at room temperature. Sectionswere first incubated with primarymonoclonal antibody against EBV-VCA (dilution 1 ; 2000), followed bythe unlabelled goat-anti-mouse bridg-ing antibody (dilution 1 ; 60; Jackson,Avondale, USA) and finally with the
-^ Oral IS:7.
412 REICHART ET AL, et al.
Table I. Risk groups for 95 patients withHL,
Risk factors Men: « = 87 Women: n = 8
Homosexuali, v,/homosex.i. V. drug userHemophiliacTransplant pat.Unknown
71392
2
1
7
1
alkaline phosphatase-mouse-anti alka-line phosphatase (APAAP) immunecomplexes (dilution 1 : 50; Dianova,Hamburg, FRG) (35),
Results
Of a total of 373 HIV-seropositive indi-viduals 95 patients revealed HL clin-ically (25,4%), In 75% HL was bilat-eral, HL in extralingual sites was notseen. Clinically, HL varied in appear-ance, A corrugated pattern {n = 80) aswell as whitish plaque-like lesions (n =15) (16%) extending on to the sublin-gual surface was observed. Hair-likeprojections were rarely seen. In 17% ofpatients HL covered an area of up to 15mm in diameter. None of the patientsreally complained about the lesion.More than 75% of patients, especiallyhomosexual men, were aware of theirlesion, had heard about its significanceand usually were those who refused tohave biopsy taken. Average age of themale patients was 37,1 yr (range 19 to82 yr), of the female patients 30,3 yr(range 26 to 46 yr), 87 patients weremen, 8 were women. The majority ofthe male patients were homosexualmen (n = 68) (71,6%), Risk factors for95 patients with HL are shown in Table1, 9 men and 7 women were i,v, drugabusers (16,8%), 14 homosexual men(average age 49,9 yr, range 39-82 yr)with HL had died after an average pe-riod of observation of 7,2 months(range 1 to 27 months), 13 patients withHL have been observed more than 4wk with an average of 5,2 months(range 1 to 13 months). In 68 patientsthe period of observation was less than4 wk. Out of 95 patients with HL 18had no general symptoms, 17 presentedwith ARC and 60 had developedAIDS, The CDC classification at theinitial diagnosis of HL in 95 patients isshown in Table 2,
CD4/CD8 ratios at the time of initialdiagnosis of HL could be stated in 19
patients revealing an average of CD4/CD8: 0,24 with a range from 0,04-1,0,The absolute number of CD4 cells was :149 mm^ (range 10-470) (average IgA :270 (134-380); average IgG : 1690(1100-2400), average IgM : 243 (149-374), A total of 13 patients with HLreceived AZT, In seven patients HLregressed clinically; two of these pa-tients developed resolution of HL dur-ing acyclovir therapy, one patientshowed regression under HOE/Bay 946therapy and in one case the regressiondid not coincide with a particular treat-ment.
In 31 patients with HL without previ-ous antimycotic treatment smears forCandida albieans were taken. Of these,14 smears were positive for C, albieans.When diagnosis of HL was stated 79%of patients showed clinical symptoms oforal C, albieans infection, 22% sufferedfrom periodontal lesions of RPP and/orNUG, and 8% of oral Kaposi's sar-coma. In 18% of patients HL was theonly oral manifestation of HIV infec-tion,
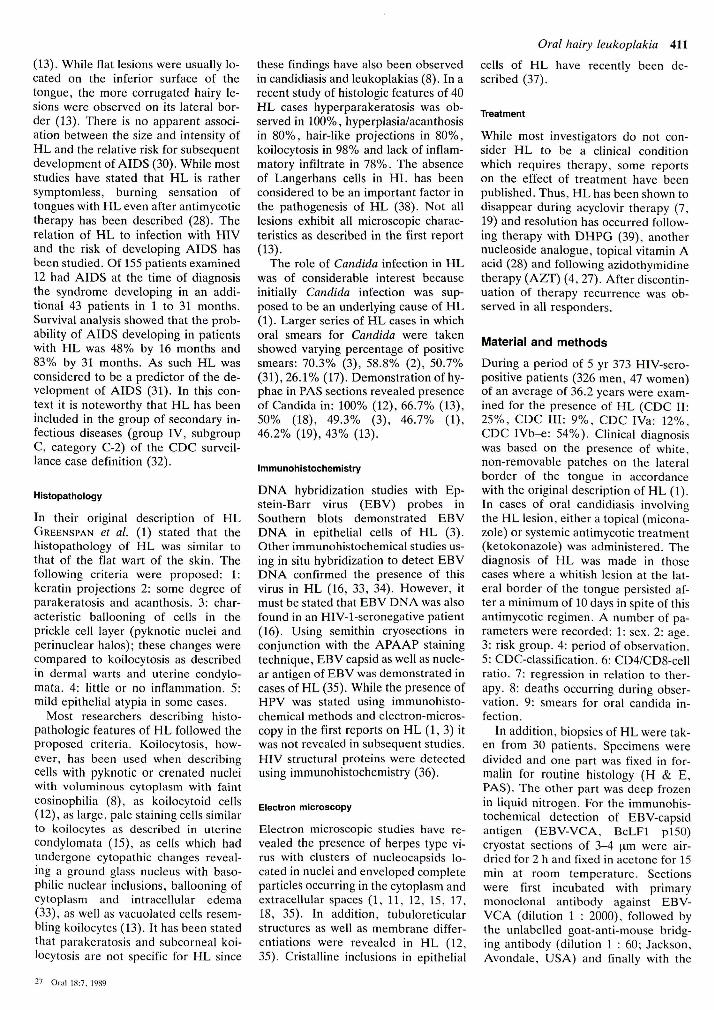
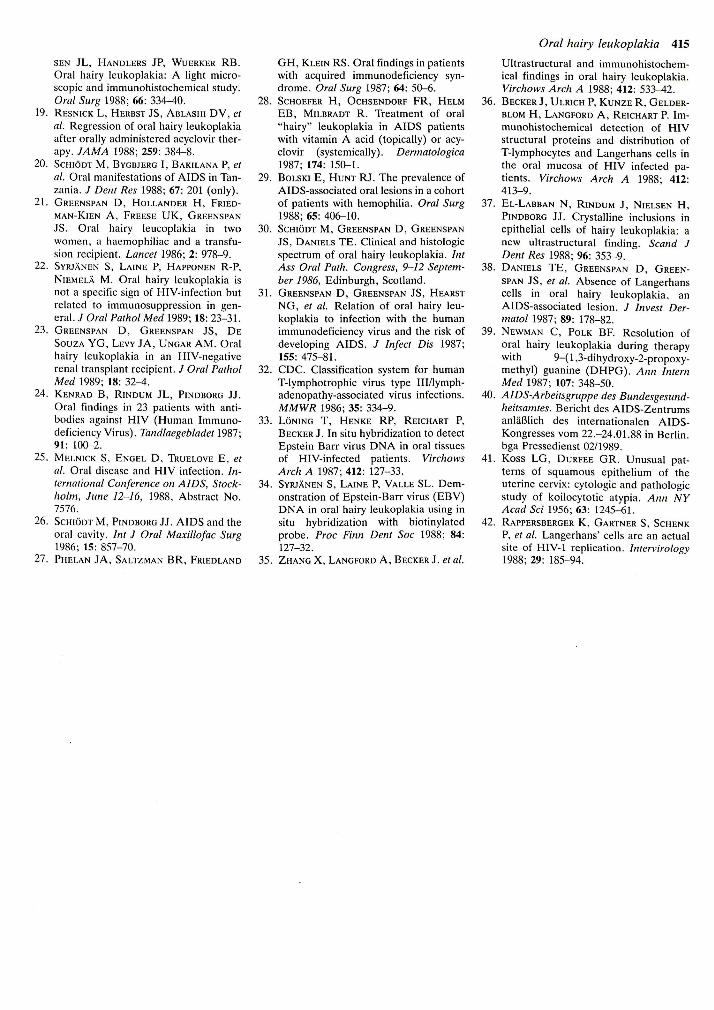
Histologic and immunohistochemicalfindings are summarized in Table 3,Hyperparakeratosis (100%), acantho-sis/hyperplasia (100%), relatively fewhair-like projections (33%) and koilo-cyte-like cells (90%) were found. Ab-sence of inflammatory changes was alsoobserved (53%), In PAS-stained sec-tions candidal hyphae in epitheliumwere found in 47%, Immunohisto-chemically, EBV-capsid antigen(VCA) was only detected in 20 out of30 biopsies, A strong nuclear immuno-labelling was found in cells of the upperstratum spinosum and in the ballooned,koilocyte-like epithelial cells (Fig, 1),Staining was often not continuous overthe whole section and large areas,whieh showed the same histologic char-acteristics as areas with an intense im-munolabelling did, were essentiallynegative for VCA (Fig, 2),
DiscussionThe largest group of individuals suf-fering from AIDS in the Federal Re-public of Germany including West Ber-lin are homosexual men (40), This isthe risk group with a high prevalencerate of HL, as has been found in thepresent study. Although the prevalencerate showed significant differencessome centers (San Francisco, Copenh-agen) have recorded comparable prev-alence rates (25,4%), Also the data foraverage age and range were very simi-
Table 2, Initial CDC classification of 9,5 pa-tients with HL,
CDC group
CDC IICDC IVCDC IVaCDC IVbCDC IVc,CDC IVcjCDC IVdCDC IVe
n
211221
432
131
%
22,112,62,11,1
45.32.1
13.51,1
lar. In contrast, i,v, drug abusing HLpatients (16) appear to be eonsiderablyyounger (27 years). Larger studies ofcohorts of i,v, drug abusers with HLcompared to homosexual/bisexualmales are necessary in order to revealdifferences in the development andcourse of HL, The short period of ob-servation of HL (68 patients less than 4wk) does not allow to draw any conclu-sions on the development of HIV-in-fection in patients with HL, It must alsobe stated that in this cohort the major-ity of patients were classified as CDCIVb, IVc, IVd or IVe (AIDS eases54%), Of considerable interest is theCD4/CD8 ratio and the development ofHL, In HIV periodontitis a elear-eutrelation between the decrease of thenumber of CD4 cells as well as in CD4/CD8 ratio has been found (J, Winkler,personal communication). It would beof interest to see when and at whichCD4/CD8 ratio HL is first observed.
Therapy of HL does not seem to beof major priority. In most cases HL wassymptomless and exclusive treatmentof HL lesions was never necessary,Acyclovir as well as AZT therapy re-sulted in clinical disappearance of HLlesions, as has been observed in otherstudies (6, 28, 39), As could be sus-pected in cases of immunodeficiency,recurrences occurred.
Table 3. Histologic findings in 30 biopsies ofHL,
EBV-VCA+ 20Hyperparakeratosis 30Hyperplasia/acanthosis 30Hairlike projections 10Koilocyte-like cells 27Bacteria on surface 11PAS + ; (Candida) 14Leukocytes in rel, to Catidida 0Leukocytes in epithelium 10Inflammation absent 16Superf, slight diffuse infl, 9Superf, small clusters 5
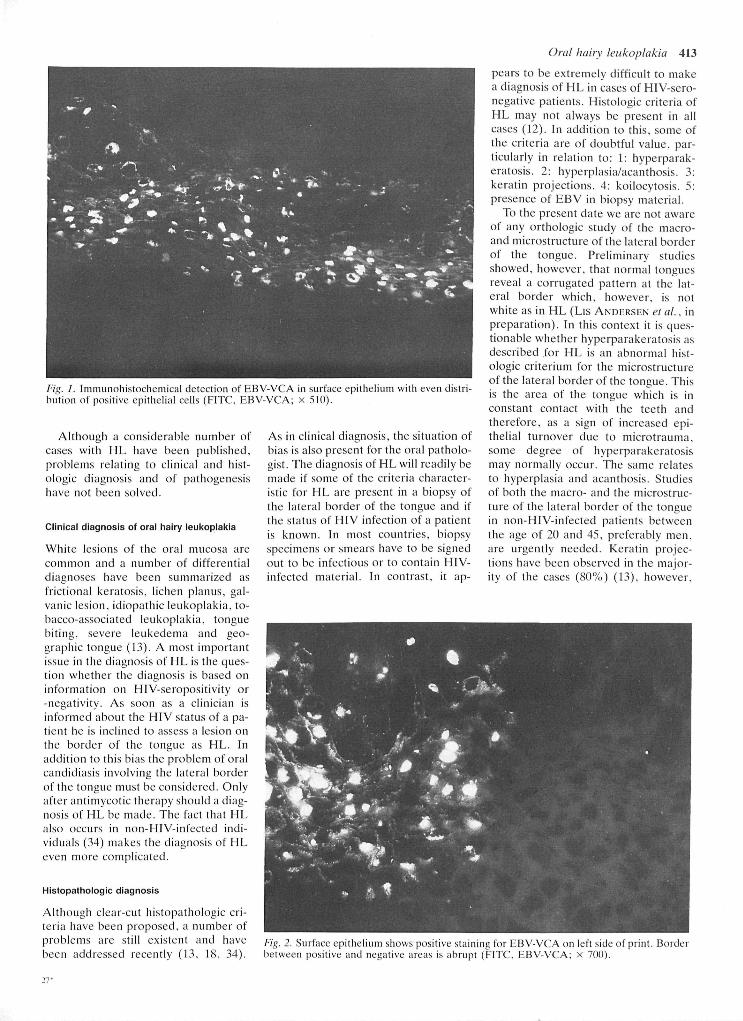
Fig. 1. Immunohistochemical detection of EBV-VCA in surface epithelium with even distri-bution of positive epithelial cells (FITC, EBV-VCA; x 510),
Although a considerable number ofcases with HL have been published,problems relating to clinical and hist-ologic diagnosis and of pathogenesishave not been solved.
Clinical diagnosis of orai hairy ieukoplakia
White lesions of the oral mucosa arecommon and a number of differentialdiagnoses have been summarized asfrictional keratosis, lichen planus, gal-vanic lesion, idiopathic leukoplakia, to-bacco-associated leukoplakia, tonguebiting, severe leukedema and geo-graphic tongue (13), A most importantissue in the diagnosis of HL is the ques-tion whether the diagnosis is based oninformation on HIV-seropositivity or-negativity. As soon as a clinician isinformed about the HIV status of a pa-tient he is inclined to assess a lesion onthe border of the tongue as HL, Inaddition to this bias the problem of oralcandidiasis involving the lateral borderof the tongue must be considered. Onlyalter antimycotic therapy should a diag-nosis of HL be made. The fact that HLalso occurs in non-HIV-inlected indi-viduals (34) makes the diagnosis of HLeven more complicated,
HIstopathoiogic diagnosis
Although clear-cut histopathologic cri-teria have been proposed, a number ofproblems are still existent and havebeen addressed recently (13, 18, 34),
As in clinical diagnosis, the situation ofbias is also present for the oral patholo-gist. The diagnosis of HL will readily bemade if some of the criteria character-istic for HL are present in a biopsy ofthe lateral border of the tongue and ifthe status of HIV infection of a patientis known. In most countries, biopsyspecimens or smears have to be signedout to be infectious or to contain HIV-infected material. In contrast, it ap-
Orat hairv tettkoptakia 413
pears to be extremely difficult to makea diagnosis of HL in cases of HIV-sero-negative patients. Histologic criteria ofHL may not always be present in allcases (12), In addition to this, some ofthe criteria are of doubtful value, par-ticularly in relation to: 1: hyperparak-eratosis, 2: hyperplasia/acanthosis, 3:keratin projections, 4: koilocytosis, 5:presence of EBV in biopsy material.
To the present date we are not awareof any orthologic study of the macro-and microstructure of the lateral borderof the tongue. Preliminary studiesshowed, however, that normal tonguesreveal a eorrugated pattern at the lat-eral border which, however, is notwhite as in HL (Lis ANDERSEN et at., inpreparation). In this context it is ques-tionable whether hyperparakeratosis asdescribed for HL is an abnormal hist-ologic criterium for the microstructureof the lateral border of the tongue. Thisis the area of the tongue which is inconstant contact with the teeth andtherefore, as a sign of increased epi-thelial turnover due to microtrauma,some degree of hyperparakeratosismay normally occur. The same relatesto hyperplasia and acanthosis. Studiesof both the macro- and the microstruc-ture of the lateral border of the tonguein non-HlV-infected patients betweenthe age of 20 and 45, preferably men,are utgently needed. Keratin projec-tions have been observed in the major-ity of the cases (80%) (13), however.
Fig. 2. Surface epithelium shows positive staining for EBV-VCA on left side of print. Boidcrbetween positive and negative areas is abrupt (FITC, EBV-VCA; x 700).

414 REICHART ET AL, et al.
they are missing in about 20% of diag-nosed HL cases. Clinically, as well ashistologically, these keratin projectionsor hair-like formations have not beenobserved in our material (33,3%) asfrequently as it has been reported inother studies.
The concept of koilocytosis in HLhas also been questioned recently (18,34). Originally, this particular changehas been described in uterine cervicalmucosa (41), Human papillomavirus(HPV) has been considered to be theunderlying eause of koilocytosis in cer-vical mucosa. In HL HPV, however,has to date not convincingly been dem-onstrated. The fact that some research-ers have used the term 'koilocyte-likechanges' is a hint towards a differen-tiated understanding of the eoncept ofthese changes. EBV has undoubtedlybeen demonstrated in HL and has beendiscussed in the etiology of this lesion.According to SYRJANEN et al. (34) thevacuolized or ballooning epithelial cellsfound in HL are not identical with thetrue "koilocytes". The characterizationof these large pale staining cells in theprickle cell layer of HL is even morecomplicated by the fact that such cellsmay also be observed in oral mucosaaffected by candidiasis and in oral pa-rakeratotie leukoplakias (8), Enlargedepithelial cells of the surface layers mayalso occur in lesions such as tongue bit-ing. It is unknown whether koilocyte-like cells also occur in the normal oralmucosa of the lateral border of thetongue.
Due to the insecurities which mayoccur in the histopathological diagnosisof HL SYRJANEN et al. (34) have sug-gested that in patients whose HIV anti-body status is unknown the presence ofEBV in lesions should be demonstratedimmunohistochemically or using DNAtechniques. Although this proceduremay help in clarifying the diagnosis ofHL, it must be considered that EBVhas now also been demonstrated in oralmucosa other than that of the lateralborder of the tongue (33), In particularthe demonstration of structural pro-teins of EBV (capsid antigen) in super-ficial layers of oral epithelium would behelpful in the histopathological diag-nosis of HL. However, due to thespotty distribution of EBV expressionin oral epithelium, VCA may not bedemonstrated if biopsies are too smallor non-representative as was found inthe present study where EBV could on-ly be found in 20 out of 30 biopsies. Itappears from the present knowledge
that comparative studies of the normallateral border of the tongue are neees-sary in order to reassess the varioushistological criteria used for the diag-nosis of HL,
Etioiogy, pathogenesis
The detailed etiology of HL is un-solved. Several factors have been sug-gested to play a role in pathogenesis.Initially, Candida infection had beenconsidered to be the eause of HL (1),In fact it must be stated that even afterantimycotic therapy a high number ofbiopsy specimens (14 of 30) revealedhyphae in PAS-stained sections. In EMstudies the presence of both Candidaand EBV particles in oral epitheliumhas been demonstrated (35), The roleof both Candida and EBV in producinga whitish lesion at the lateral border ofthe tongue has not been solved. In fact,our observation of HL-biopsies nega-tive for EBV antigen may hint to HL asa condition for EBV expression ratherthan EBV as a cause of these lesions.
Although the absence of Langerhanscells at the lateral border of the tonguehas been discussed in the pathogenesisof HL (38) it is not clear why HL pre-dominantly involves the lateral borderof the tongue. It has recently beenshown that Langerhans cells representa susceptible substratum for HIV-1 rep-lication also serving as reservoir forHIV (42),
While HL appears to be a newly rec-ognized oral disease entity a number ofproblems are still unsolved. These re-late to global epidemiology, clinicaland histologic diagnosis, to etiology aswell as pathogenesis. In all these fields,further studies are needed.
Acknowledgment - Supported by a grantfrom Bundesministerium fur Forschung undTechnologie, No, 11-071-88,
References
1, GREENSPAN D , GREENSPAN JS, CONANT
M, PETERSEN V, SILVERMAN S JR, DH
SouzA Y, Oral "bairy" leukoplakia inmale homosexuals: evidence of associ-ation with both papillomavirus and aherpes-group virus. Lancet 1984; 2:
2. HOLLANDER H , GREENSPAN D , STRIN-
GARi S, GREENSPAN J, SCHIODT M . Hairyleukoplakia and the acquired immuno-deficiency syndrome, Atin Interti Med1986: 104: 892 (only),
3, GREENSPAN JS, GREENSPAN D , LEN-
NEiTE ET, et al. Replication of Epstein-Barr virus within the epithelial cells of
oral "hairy" leukoplakia, an AIDS-as-sociated lesion, N Engt J Med 1985; 313:1564-71,
4, PINDBORG JJ, SCHIODT M , REIBEL J,
PRAETORIUS F, HANSEN HJ, GAUB J, Re-
gression of oral "haret" leukoplaki hospatient med AIDS, Tandtaegebtadet1986; 90: 356-60,
5, REICHART P, POHLE HD, GELDERBLOM
H, STRUNZ V, AIDS - Orale Manifes-tationen, Dtsch Zatinaerztt Z 1986; 4:374-6,
6, REICHART P, GELDERBLOM H , POHLE
HD, PHILIPSEN HP, "Hairy leukopla-kia" (AIDS) - Klinik und Morphologie,Dtscti Z Mund Kiefer Gesichtsdiir 1986;10: 161-5,
7, FRIEDMAN-KIEN AE, Viral origin ofhairy leukoplakia. Lancet 1986; 2:694-5,
8, EvERSOLE LR, JACOBSEN P, STONE CE,
FRECKLETON V, Oral condyloma planus(hairy leukoplakia) among homosexualmen: a clinicopathologic study of thirty-six cases, Orat Surg 1986; 61: 249-55,
9, SILVERMAN S JR, MIGLIORATI CA, Lo-
ZADA-NuR F, GREENSPAN D , CONANT
MA, Oral findings in people with or athigh risk for AIDS: a study of 375 ho-mosexual males. JADA 1986; 112:187-92.
10, WRAY D , MOODY GH, MCMILLAN A,
Oral "hairy" leukoplakia associatedwith human immtmodeficiency virus in-fection: report of two cases, Br Dent J1986; 161: 338-9,
11, KiMMiG W, MENSING H , SEYFARTH K ,
ScHAEG G, JAENNER M , NASEMANN T ,
Orale "hairy" Leukoplakie - Frubsymp-tom bei HTLV-III/LAV-Infektion,Dtsch Med Wsehr 1986; 111: 1394-7,
12, BELTON C M , EVERSOLE LR, Oral hairyleukoplakia: ultrastructural features, JOrat Pattiot 1986; 15: 493-9,
13, SCHIODT M , GREENSPAN D , DANIELS
TE, GREENSPAN JS, Clinical and hist-ologic spectrutn of oral hairy leukopla-kia, Orat Surg 1987; 64: 7K>-20.
14, RiNDUM JL, SCHIODT M , PINDBORG JJ,
ScHEiBEL E, Oral hairy leukoplakia inthree hemophiliacs with human immu-nodeficiency virus infection, Orat Surg1987; 63: 437-40,
15, LuPTON GP, JAMES WD, REDFIELD RR,
BROWN C , RODMAN OG, Oral hairy leu-koplakia, A distictivc marker of humanT-cell lymphotropic virus type III(HTLV-III) infection. Arch Dertnatot1987; 123: 624-8,
16, GROSS G , WIEGAND H , ZENTGRAF H ,
Epstein Barr-Virus-Nachweis in oralerhaariger Leukoplakie bei AIDS-Patien-ten, in Leukoplakien und unauffiilligenZungenepithelien HIV-1-negativer Pa-tienten. Z Hatttkr 1988; 63: 44-8.
17, FiCARRA G, BARONE R , GAGLIOTI D , et
at. Oral hairy leukoplakia among HIV-positive intravenous drug abusers: aclinicopathologic and ultrastructuralstudy. Orat Surg 1988; 65: 421-6.
18, KANAS R J , ABRAMS AM, RECHER L ,
JEN-
SEN JL, HANDLERS JP, WUERKER RB,
Oral hairy leukoplakia: A light micro-scopic and immunohistochemical study,Orat Surg 1988; 66: 334-40,
19, RESNICK L , HERBST JS, ABLASHI DV, et
al. Regression of oral hairy leukoplakiaafter orally administered acyelovir ther-apy, JAMA 1988; 259: 384-8.
20, SCHIODT M , BYGBJERG I, BAKILANA P, et
at. Oral manifestations of AIDS in Tan-zania. J Dent Res 1988; 67: 201 (only).
21, GREENSPAN D , HOLLANDER H , FRIED-
MAN-KIEN A, FREESE UK, GREENSPAN
JS, Oral hairy leucoplakia in twowomen, a baemophiliae and a transfu-sion recipient, Laticet 1986; 2: 978-9,
22, SYRJANEN S, LAINE P, HAPPONEN R - P ,
NiEMELA M, Oral hairy leukoplakia isnot a specific sign of HIV-infection butrelated to immunosuppression in gen-eral, J Orat Pattiol Med 1989; 18: 23-31,
23, GREENSPAN D , GREENSPAN JS, D E
SouzA YG, LEVY JA, UNGAR AM, Oralhairy leukoplakia in an HIV-negativerenal transplant recipient, / Oral PatholMed 1989; 18: 32-4,
24, KENRAD B , RINDUM JL, PINDBORG JJ,
Oral findings in 23 patients with anti-bodies against HIV (Human Immuno-deficiency Virus), Tatidtaegebtadet 1987;91: 100-2,
25, MELNICK S, ENGEL D , TkuELOVE E, et
at. Oral disease and HIV infection, Iti-ternatiotiat Cotiference oti AIDS, Stock-holtn, June 12-16, 1988, Abstract No,7576.
26, SCHIODT M , PINDBORG JJ. AIDS and the
oral eavity. hit J Orat Maxittofac Surg1986; 15: 857-70.
27, PHELAN JA, SALTZMAN BR, FRIEDLAND
GH, KLEIN RS. Oral findings in patientswith aequired immunodeficiency syn-drome, Orat Surg 1987; 64: 50-6,
28, SCHOEFER H, OCHSENDORF FR, HELMEB, MiLBRADT R, Treatment of oral"hairy" leukoplakia in AIDS patientswith vitamin A aeid (topically) or acy-clovir (systemically), Dermatotogica1987; 174: 150-1,
29, BoLSKi E, HUNT RJ, The prevalence ofAIDS-associated oral lesions in a cohortof patients with hemophilia, Orat Surg1988; 65: 406-10,
30, SCHIODT M , GREENSPAN D , GREENSPAN
JS, DANIELS TE. Clinical and histologicspectrum of oral hairy leukoplakia, bitAss Orat Path. Congress, 9-12 Septem-ber 1986, Edinburgh, Scotland,
31, GREENSPAN D , GREENSPAN JS, HEARST
NG, et at. Relation of oral hairy leu-koplakia to infection with the humanimmunodeficiency virus and the risk ofdeveloping AIDS, J Itifect Dis 1987;155: 475-81,
32, CDC, Classification system for humanT-lymphotrophic virus type Ill/lymph-adenopathy-associated virus infections,MMWR 1986; 35: 334-9,
33, LONING T , HENKE RP, REICHART P,
BECKER J, In situ hybridization to detectEpstein Barr virus DNA in oral tissuesof HIV-infected patients, VirchowsArch A 1987; 412: 127-33,
34, SYRJANEN S, LAINE P, VALLE SL, Dem-
onstration of Epstein-Barr virus (EBV)DNA in oral hairy leukoplakia using insitu hybridization with biotinylatedprobe, Proc Fitin Dent Soc 1988; 84:127-32,
35, ZHANG X, LANGFORD A, BECKER J, et al.
Oral hairy leukoplakia 415
Ultrastruetural and immunohistoehem-ical findings in oral hairy leukoplakia,Virchows Arch A 1988; 412: 533-42,
36, BECKER J, ULRICH P , KUNZE R , GELDER-
BLOM H, LANGFORD A, REICHART P, Im-
munohistochemical detection of HIVstructural proteins and distribution ofT-lymphocytes and Langerhans cells inthe oral mucosa of HIV infected pa-tients, Virchows Arch A 1988; 412:413-9,
37, EL-LABBAN N , RINDUM J, NIELSEN H ,
PINDBORG JJ, Crystalline inclusions inepithelial cells of hairy leukoplakia: anew ultrastructural finding, Scand JDetit Res 1988; 96: 353-9,
38, DANIELS TE, GREENSPAN D , GREEN-
SPAN JS, et al. Absence of Langerhanscells in oral hairy leukoplakia, anAIDS-associated lesion, J Itivest Der-matot 1987; 89: 178-82,
39, NEWMAN C , POLK BF, Resolution of
oral hairy leukoplakia during therapywith 9-( 1,3-dihydroxy-2-propoxy-methyl) guanine (DHPG), Atin ltitertiMed 1987; 107: 348-50,
40, AIDS-Arbeitsgrtippe des Butidesgesund-heitsatntes. Bericht des AIDS-ZentrumsanlaBlich des internationalen AIDS-Kongresses vom 22,-24,01,88 in Berlin,bga Pressedienst 02/1989,
41, Koss LG, DuRFEE GR. Unusual pat-terns of squamous epithelium of theuterine cervix: cytologic and pathologicstudy of koilocytotie atypia, Atiti NYAcad Sci 1956; 63: 1245-61,
42, RAPPERSBERGER K , GARTNER S, SCHENK
P, et al. Langerhans' cells are an actualsite of HIV-1 replication, Ititervirology1988; 29: 185-94,




















![ESGCT Berlin2017 Programme · Hans Dieter Volk [CHARITÉ MEDICAL UNIVERSITY BERLIN] INV56 Ageing and myelin regeneration in the CNS Robin Franklin [UNIVERSITY OF CAMBRIDGE]](https://img.pdfslide.us/doc/110x75/5b9f445709d3f2083f8cd69f/esgct-berlin2017-programme-hans-dieter-volk-charite-medical-university-berlin.jpg)