Embed Size (px)
Citation preview

TECHNICAL MONOGRAPH SERIES 5Handbook on Vitamin ATracer Dilution Methods toAssess Status and EvaluateIntervention Programs
Marjorie J. Haskell, Judy D. Ribaya-Mercado,and the Vitamin A Tracer Task Force

HarvestPlus Technical Monographs are designed to provide a forum for HarvestPlus research outputs.
Technical Monographs can be of two kinds:• state-of-the-art reviews that help to establish and define HarvestPlus research questions or• “gold standard” procedures to be followed in HarvestPlus research.
HarvestPlus technical monographs are written by recognized experts in the field and are externally peer reviewed prior to publication.
Marjorie J. Haskell, Judy D. Ribaya-Mercado, and the Vitamin A Tracer Task Force, 2005.Handbook on Vitamin A Tracer Dilution Methods to Assess Status and Evaluate Intervention ProgramsHarvestPlus Technical Monograph 5.
Washington, DC and Cali: International Food Policy Research Institute (IFPRI) andInternational Center for Tropical Agriculture (CIAT).
Copyright HarvestPlus, 2005
The vitamin A Tracer Task Force was initiated by IAEA, USAID, and HarvestPlus to prepare a series of three documents. The first on the appropriate use of vitamin A tracer (stable isotope) methods was published in 2004 by USAID/ILSI through the Micronutrient Global Leadership(MGL) project: http://www-naweb.iaea.org/nahu/nahres/pdf_files/vitatracer.pdf. This handbook us the second TracerForce Handbook and is being published as a HarvestPlus Technical Monograph. The third handbookwill be on model-based estimates of absorption efficiency and will be published by the IAEA in 2005.

1 Department of Nutrition, University of California, Davis, USA; 2 Jean Mayer US Department of AgricultureHuman Nutrition Research Center on Aging at Tufts University, USA; 3 Harold C. Furr, Craft Technologies, USA;Michael H. Green, Nutrition Department, Pennsylvania State University, USA; Najat Mokhtar, InternationalAtomic Energy Agency, Austria; Penelope Nestel, HarvestPlus, Washington DC, USA; Sherry Tanumihardjo,Department of Nutritional Sciences, University of Wisconsin, USA; Emorn Wasantwisut, The Institute ofNutrition, Mahidol University, Thailand.
Handbook on Vitamin ATracer Dilution Methods toAssess Status and EvaluateIntervention Programs
Marjorie J. Haskell,1 Judy D. Ribaya-Mercado,2
and the Vitamin A Tracer Task Force3
1

2HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
Table of contents
Introduction 4
1|Description of the stable isotope dilution technique 51.1 Requirements for working with stable isotope labeled analogs
of vitamin A 51.1.1 Facilities, equipment, and support 51.1.2 Personnel 5
1.2 Theoretical basis of the stable isotope dilution technique of vitamin A 51.3 Three-day stable isotope dilution procedure 61.4 Procedures for estimating total body vitamin A pool size 6
1.4.1 Choice of labeled vitamin A analog 71.4.2 Dose of labeled vitamin A 71.4.3 Preparation of labeled vitamin A doses 81.4.4 Administration of labeled vitamin A doses 81.4.5 Blood collection, processing, and transport procedures 9
1.5 Rationale for blood sampling times for measurement of plasma isotopic ratios of labeled to non-labeled retinol 9
1.6 Measurement of plasma isotopic ratios of labeled to non-labeled retinol 101.7 Factors that may affect plasma isotopic ratios
of labeled to non-labeled retinol 101.8 Assessing adequacy of vitamin A status using the stable isotope
dilution technique 11
2|Study protocols for using the paired stable isotope dilution technique 11
2.1 Site selection 112.2 Selection of study participants 112.3 Subject inclusion and exclusion criteria 122.4 Full study protocols for the paired stable isotope dilution technique 122.5 Partial study protocols for the paired stable isotope dilution technique 142.6 Estimation of duration of an intervention 172.7 Sample size calculation 182.8 Statistical analysis 18

3|Paired stable isotope dilution technique for estimating relative vitamin A equivalency factors for β-carotene 19
3.1 Site selection 193.2 Selection of study participants 193.3 Subject inclusion and exclusion criteria 193.4 Study design and protocol 203.5 Selection of high β-carotene and low vitamin A foods 203.6 Estimation of duration of an intervention 213.7 Procedures for estimating vitamin A equivalency of β-carotene 213.8 Sample size calculation 22
4|Monitoring the effectiveness of vitamin A intervention programs 224.1 Selection of study participant 224.2 Sample size calculation 224.3 Subject inclusion and exclusion criteria for studies monitoring
program effectiveness 224.4 Importance of periodic monitoring of vitamin A status
in intervention programs 224.5 Subject inclusion and exclusion criteria for periodic monitoring
of vitamin A status in intervention programs 23
5|Studies on vitamin A requirements 23
Summary 23
References 24
3HarvestPlus

4HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
Bangladesh, Guatemala, China, Philippines, Peru, andNicaragua, and to evaluate the efficacy and effective-ness of vitamin A interventions.
The purpose of these guidelines is to assistresearchers in designing and carrying out studiesusing the stable isotope dilution technique to assessthe efficacy and effectiveness of vitamin A interven-tions aimed at improving vitamin A status inpopulations at risk of deficiency. Although other stableand radiolabeled isotopic techniques are available forstudying vitamin A and carotenoid metabolism, theseguidelines focus on the stable isotope dilution tech-nique for assessment of vitamin A status. Thistechnique has been validated against liver vitamin Aconcentrations in surgical patients with low toadequate liver vitamin A stores (Furr et al. 1989,Haskell et al. 1997). Results of those studies indicatethat the technique provides an accurate quantitativeestimate of mean total body vitamin A pool size forgroups of subjects. It is important to note that thetechnique does not provide precise estimates ofvitamin A pool size for individual subjects, and henceit is not intended for use as a diagnostic method forassessing vitamin A status in individuals.
The paired stable isotope dilution technique consistsof estimating total body vitamin A pool size before andafter an intervention to assess the change in vitamin Apool size in response to supplementation with vitaminA or provitamin A carotenoids. The paired stableisotope dilution technique has been used to assess theefficacy and effectiveness of vitamin A interventions forvitamin A status in populations at risk of deficiency.These guidelines describe the theoretical basis of thestable isotope dilution technique and include studyprotocols for using the paired isotope dilution techniquein field settings. Information is also provided on thetechnical aspects of working with stable isotopes ofvitamin A, recognizing that specific technical procedures will vary depending on the choice of labeledvitamin A analog and analytical instrumentation. Forthis reason, it is important for field and laboratoryresearchers to work closely together during the plan-ning phase of a study to ensure that the choice oflabeled vitamin A analog(s) and analytical methods areappropriate to address the specified research question.
IntroductionVitamin A deficiency is a serious public health problemaffecting ~140 million children and ~20 million preg-nant women annually in many developing nationsworldwide. Vitamin A deficiency can result in anemia,reduced resistance to infection, impaired cellulardifferentiation, xerophthalmia, and ultimately blind-ness and death. Because of the detrimental effects ofvitamin A deficiency on human health, accurateassessment of vitamin A status is necessary to makeinformed decisions regarding intervention programs.
Vitamin A is stored primarily in the liver, and thus livervitamin A concentration is considered to be the bestindicator of vitamin A status. However, becauseobtaining liver specimens is difficult and usually notjustified, indirect assessment techniques such asserum retinol concentration and the relative doseresponse tests are commonly used to assess vitamin Astatus. Another indirect assessment method is thestable isotope dilution technique, which provides aquantitative estimate of the size of the exchangeablebody pool of vitamin A. The ‘exchangeable body poolof vitamin A’ refers to the vitamin A in the body that isin a dynamic state. Hereafter, the exchangeable bodypool will be referred to as the total body vitamin Apool. By using assumptions regarding the liver to bodyweight ratio, estimates of liver concentrations ofvitamin A can also be obtained. The stable isotopedilution technique has the advantage that it is the onlyindirect assessment method that provides a quantita-tive estimate of vitamin A status across the continuumof status, from deficient to excessive vitamin A poolsizes. Thus, the technique can also be used forassessing vitamin A pool size in populations at risk ofexcessive status because of exposure to too muchvitamin A either through the use of dietary vitamin Asupplements and/or excessive consumption of vitaminA-rich or fortified foods. The analogs of vitamin A thatare used for assessing vitamin A pool size are labeledwith stable isotopes (deuterium or 13C) and are notradioactive. There is no known health risk associatedwith ingestion of stable isotope labeled vitamin A. Thestable isotope dilution technique has been usedsuccessfully to assess total body vitamin A pool size inchildren and/or adults in the United States,

5HarvestPlus
the safe disposal of hazardous chemical and biologicalwastes. Additionally, laboratory personnel must be ableto quantitatively analyze human plasma or serum forretinol and carotenoids by HPLC, and be familiar withHPLC methods for analyzing food samples for vitaminA and carotenoid contents. Experience with GC-MS orGC-C-IRMS is desirable, although initially the MSanalyses can be done in collaboration with researchersand institutions with the necessary expertise andinstrumentation.
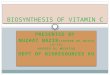
1.2 Theoretical basis of the stable isotopedilution technique
The stable isotope dilution technique for estimatingthe total body vitamin A pool is based on the principleof isotope dilution, as shown in Figure 1. A knowndose of stable isotope labeled vitamin A is adminis-tered orally. After a mixing period (~20 days in adults),during which the labeled vitamin A mixes with theendogenous vitamin A pool, a blood sample isobtained for measurement of the plasma or serumisotopic ratio of labeled to non-labeled retinol. (Eitherplasma or serum can be used; for simplicity, “plasma”will be used hereafter.) Total body vitamin A pool size(mmol retinol) is estimated quantitatively using themeasured plasma isotopic ratio of labeled to non-labeled retinol and the equation developed by Olson
1|Description of the StableIsotope Dilution Technique
1.1 Requirements for working with stableisotope labeled analogs of vitamin A
1.1.1 Facilities, equipment, and supportA relatively sophisticated biochemistry laboratory isrequired for working with stable isotope labeled analogsof vitamin A. Specifically the laboratory must be clean,dust-free, and well-ventilated, with temperature andlighting control. It must be equipped with a biosafetycabinet and a chemical fume hood for safe handling ofbiological and chemical materials; a digital balance(0.0000 g); a UV/VIS spectrophotometer (preferably ascanning UV/VIS spectrophotometer to assess degrada-tion of compounds); an HPLC with a UV/VIS detector;and freezers (–20oC for retinoids and/or –80oC forcarotenoids and retinoids). A suitable mass spectrom-eter is required for stable isotope analyses. The type ofmass spectrometry (i.e., gas chromatography-massspectrometry [GC-MS] or gas chromatography-combus-tion-isotope ratio mass spectrometry [GC-C-IRMS]) willvary depending on the type of labeled compound used.Other necessary supplies include positive displacementpipettes and general laboratory supplies such as acentrifuge, vortex mixer, sonicator, glassware, vacuumflasks and nitrogen or argon gas. It is important for thelaboratory to have mainte-nance contracts for theanalytical instruments(HPLC and MS) and easyaccess to replacement parts.
1.1.2 PersonnelLaboratory personnel musthave extensive experiencewith basic biochemical andanalytical chemistry tech-niques and training in thesafe handling of chemicalsand human biologicalsamples (blood, breastmilk, urine, stool) as well as
����� ���� ����� � ����
���� ������ �� �� ���� � �������
����� ��������
����� �� �������
�� ���������
����� �
��������� ����
�� �������
����� �
PRINCIPLE OF ISOTOPE DILUTION
FIGURE 1

6HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
technique can be used to detect quantitative changesin total body vitamin A pool size in response tosupplementation or dietary intervention. InBangladeshi men, the technique detected increases intotal body vitamin A pool size in response to threedifferent levels of vitamin A supplementation, and theincreases in pool size were similar to the expectedtheoretical increases based on the amounts of vitaminA provided (Haskell et al. 1999).
The Olson equation provides a quantitative estimate oftotal body vitamin A pool size for non-pregnant andnon-lactating adults and school-age children. For preg-nant and/or lactating women, estimates of retention ofthe dose of labeled vitamin A and the system catabolicrate have yet to be defined; thus the Olson equation isnot recommended for these groups. To date, no equa-tion has been developed to quantitatively estimatetotal body vitamin A pool size during pregnancy andlactation. However, the stable isotope dilution tech-nique can be used to obtain qualitative estimates ofvitamin A status in these population groups, asdescribed below.
1.3 Three-day stable isotope dilutionprocedure
The conventional stable isotope dilution techniqueprovides a quantitative estimate of vitamin A pool sizebased on the plasma isotopic ratio of labeled to non-labeled retinol after the labeled vitamin A dose hasmixed with endogenous vitamin A. However, studies inrats indicate that the fraction of the dose of labeledvitamin A in plasma at 3 days after dosing is highlycorrelated with liver vitamin A stores, and that thisfraction of the labeled dose in plasma accuratelypredicts vitamin A pool size in rats with low to highliver vitamin A stores (Adams and Green 1994). Similarly,preliminary studies in adults and children indicate thatserum or plasma isotopic ratios of labeled to non-labeled retinol measured at 3 days after dosing are highlycorrelated with estimated vitamin A pool size, and thusthat predictive equations can be developed to estimatetotal body vitamin A pool size using day-3 plasmaisotopic ratios. Strong linear correlations have beenreported in adults between serum isotopic ratios oflabeled to non-labeled retinol measured at 3 and 20 days
and coworkers (referred to hereafter as the Olsonequation) (Furr et al. 1989):
Total body vitamin A pool size (mmol) = F × dose × (S × a ×{(1/D:H)−1})
where F is a factor for the efficiency of storage of anorally administered dose, and is assumed to be 0.5based on the work of Bausch and Rietz (1977); dose isthe amount of labeled vitamin A administered in mmolretinol equivalents; S corrects for the inequalitybetween the plasma and liver ratios of labeled to non-labeled retinol; a is used to correct for irreversible lossof labeled vitamin A during the mixing period; D:H isthe isotopic ratio of labeled to non-labeled retinol inplasma; and finally, the value –1 corrects for the con-tribution of the mass of the labeled dose to the totalbody vitamin A pool. The oral dose of labeled vitaminA does not truly equilibrate with the endogenousvitamin A pool because of continuous intake of un-labeled dietary vitamin A and catabolism of the dose oflabeled vitamin A during the 20-day mixing period.Newly absorbed dietary vitamin A is preferentiallysecreted into the blood stream (Loerch et al. 1979),and thus labeled vitamin A in the plasma is diluted toa greater extent than labeled vitamin A in the liver. Thefactor S in the Olson equation corrects for theinequality of the isotopic ratios of labeled to non-labeled vitamin A in plasma versus liver. A value of0.65 is used for the factor S, which is based on themean observed plasma to liver ratio of the specificactivities of radiolabeled vitamin A in rats with varyinglevels of dietary vitamin A intake and liver vitamin Astores (Hicks et al. 1984). The factor a is included toadjust for catabolism of the dose of labeled vitamin Aduring the mixing period. This factor is calculatedbased on the half-life of vitamin A turnover, which isestimated as 140 days in adults, and is assumed to beindependent of the size of the liver reserves of vitaminA, and to be time-invariant (a = e–kt, where k = ln 2/140 days and t = time in days since dosing).
The stable isotope dilution technique has been vali-dated against hepatic vitamin A concentrations insurgical patients in the US and Bangladesh with low toadequate vitamin A pool sizes (Furr et al. 1989,Haskell et al. 1997). In addition to its use in estimatingtotal body vitamin A pool size, the stable isotope dilution

7HarvestPlus
are generally larger than doses of 13C-labeled vitamin Abecause of differences in the sensitivities of the analyt-ical instruments. Thus, doses of deuterium labeledvitamin A are more likely to perturb the endogenousvitamin A pool than doses of 13C-labeled vitamin A. Inaddition, the minimum number of blood samplesrequired for the paired stable isotope dilution techniquewill differ depending on which labeled compound isused. An additional blood sample is required whenGC-C-IRMS is used to correct for residual 13C in plasmafrom the first dose of 13C-labeled vitamin A (this isdescribed in detail below). Because differently substi-tuted analogs of deuterium vitamin A compounds areavailable (i.e., 2H4, 2H8), pre- and post-interventionpool sizes can be estimated using different deuteriumlabeled analogs, obviating the need to collect a bloodsample prior to administration of the second dose ofdeuterium labeled vitamin A. In target groups in whichit is desirable to minimize the number of bloodsamples collected (i.e., children), this may be animportant consideration when selecting the labeledvitamin A compound. Finally, availability of instrumen-tation and cost will also affect the choice of labeledcompound. Thus, field and laboratory researchersshould carefully consider the target group, instrumen-tation, and costs before deciding on which labeledvitamin A compound to use.
1.4.2 Dose of labeled vitamin AThe dose of labeled vitamin A will vary depending onthe labeled compound used, the target group, and thedetection limit of the mass spectrometer. Oral doses ofdeuterium labeled retinyl acetate are typically 5–10 mgretinol equivalents (RE) for adults and 2.5–5 mg RE forchildren. The use of 13C-labeled vitamin A is relativelynew. In the one study performed to date, an oral doseof 5.0 mg RE of 13C-retinyl acetate was used for anadult subject (Tanumihardjo 2001). However, becausethe 13C was still detectable at 4 years after dosing,smaller doses of 13C-retinyl acetate can be used infuture studies (Tanumihardjo 2003). If plasma isotopicratios are measured only at 3 days after dosing, thedeuterium labeled doses can be reduced to 2.5–5 mgfor adults and to 1.25–2.5 mg for children. The specified doses are appropriate for the GC-MS andGC-C-IRMS methods that are currently used
after dosing, with correlation coefficients (r) of 0.94and 0.90 in two separate populations (Ribaya-Mercado et al. 2003). Similar observations regardingthe potential usefulness of isotopic ratios measured at3 days after dosing have been made in children aged7–13 years (Ribaya-Mercado et al. 2000, Tang et al.2002) and in children aged 1-2 years (Haskell et al.2003). The 3-day stable isotope dilution procedure isadvantageous because of the shorter blood samplingtime. However, the predictive equations for quantita-tive estimation of total body vitamin A pool size usingday-3 serum or plasma isotopic ratios have not yetbeen validated against direct measurements of livervitamin A concentrations in humans. Nevertheless,because the plasma isotopic ratios of labeled to non-labeled retinol measured at 3 days after dosing arehighly correlated with estimated vitamin A pool size,the ratios provide a qualitative estimate of vitamin Apool size and can be used to assess qualitativechanges in vitamin A pool size in response to an inter-vention. This has been demonstrated among Filipinochildren who were fed controlled diets containingcarotene-rich fruits and vegetables (Ribaya-Mercado etal. 2000), and among elderly Guatemalans who werefed controlled diets plus vitamin A supplements(Ribaya-Mercado et al. 1999).
1.4 Procedures for estimating total body vitamin A pool size
1.4.1 Choice of stable isotope labeled analog of vitamin AThe choice of labeled analog(s) of vitamin A willdepend on the target group, available instrumentation,and cost. Deuterium labeled vitamin A or 13C-labeledvitamin A can be used to estimate total body vitamin Apool size using the stable isotope dilution technique.Deuterium labeled vitamin A compounds are commer-cially available (Cambridge Isotopes, Andover, MA),and 13C-labeled vitamin A compounds can be special-ordered as a custom synthesis from commercialsuppliers of isotopically labeled pharmaceuticals. GC-MS is used to analyze deuterium labeled vitamin A(Handelman et al. 1993, Tang et al. 1998); GC-C-IRMScan be used to analyze 13C-labeled vitamin A(Tanumihardjo 2000). The doses of deuterium labeledvitamin A that are used to estimate vitamin A pool size

8HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
transferred to a new, clean vial and ethanol is evapo-rated in the dark under nitrogen or argon gas. Anappropriate amount of corn oil is added to the residueto achieve the desired concentration, and the vial isshaken vigorously using a vortex mixer or sonicator todissolve the labeled vitamin A thoroughly in the cornoil. For example, if the desired dose of labeled vitaminA is 5 mg RE in 200 µL of corn oil, a solution of 25 mgRE/mL is needed. To determine the concentration, adilution of the solution of labeled vitamin A in corn oilis carefully prepared in hexane to achieve an ODreading of between 0.5 and 1.0 absorption units, andthe concentration is determined by UV/VIS spec-trophotometry as described above, that is, by using themolar extinction coefficient for retinol in hexane of51,770 M–1 cm–1, the molecular weight of 290 for [2H4]-retinol, and adjusting for the dilution factor. Thevolume required for a dose is determined based on theconcentration of the labeled vitamin A in corn oil. Apositive displacement pipette is used to carefully placethe desired volume of labeled vitamin A into opaquegelatin capsules. Alternatively, a positive displacementpipette can be used to administer the desired volumeof the solution of labeled vitamin A directly into themouths of subjects, as described below. The vialcontaining the corn oil solution of labeled vitamin A isflushed with nitrogen or argon gas, protected fromlight, and stored at ≤ –20oC. Under these conditions,the labeled vitamin A is stable for at least 2 years.
1.4.4 Administration of labeled vitamin A dosesFor adults and school-age children, an oral dose oflabeled vitamin A dissolved in vegetable oil is adminis-tered in a gelatin capsule; for infants and preschool-agechildren, doses are administered directly into themouth using a positive displacement pipette with adisposable tip. In both cases, a low vitamin A/high-fatsnack is provided immediately following administrationof the labeled vitamin A to enhance absorption.Examples of snacks for adults and school-age childrenare peanut butter on a cracker, deep-fried curriedpotato pastries, or other low vitamin A deep-friedpastries. Infants should be breastfed after administra-tion of the dose, even though breast milk containsvitamin A. For non-breastfed infants, animal milk orinfant formula should be provided after administration.
(Handelman et al. 1993, Tang et al. 1998,Tanumihardjo 2000). However, it is likely that thesensitivity of mass spectrometers will improve withtime; thus it may be possible to administer lowerdoses in the near future. Because the sensitivity of theinstrument impacts the size of the dose required, it isimportant to know the capabilities of the mass spectrometer when deciding on the dose.
1.4.3 Preparation of labeled vitamin A dosesCommercially available analogs of vitamin A labeledwith stable isotopes are usually provided in powderform. For administration to human subjects, doses oflabeled vitamin A are prepared in vegetable oil. Thefollowing is a brief description of procedures forpreparing deuterium labeled retinyl acetate in corn oil.Because vitamin A is light-sensitive, it is very impor-tant that all procedures be conducted in dim light orunder gold fluorescent lighting (Barua and Furr 1998).As an example, a known amount of [2H4]-retinyl acetateis carefully dissolved in ethanol in a volumetric flask sothat the concentration is ~40 mg/mL (e.g., 1.0 g in25 mL). A careful dilution of the stock solution isprepared in ethanol to achieve an optical density (OD)reading between 0.5 and 1.0 absorption units usingUV/VIS spectrophotometry at 325 nm. The concentra-tion of the stock solution of [2H4]-retinyl acetate isdetermined using the molar extinction coefficient forretinol in ethanol of 52,770 M-1 cm-1 and the molecularweight of [2H4]-retinol of 290, and adjusting for thedilution factor. The concentration of the stock solutionis based on the [2H4]-retinol content and is expressedas mg retinol equivalents (mg RE), rather than mgretinyl acetate. The chemical purity of the labeledcompound can be assessed by reverse-phase HPLC byinjecting an aliquot of the solution of labeled vitamin A(~1–2 µg RE of [2H4]-retinyl acetate), monitoring theabsorbance at 325 nm, and collecting spectra from200–800 nm using a photodiode array detector. Theisotopic purity can be checked by MS. After checkingthe isotopic and chemical purity, α-tocopherol (~2 µgper mg of vitamin A acetate) is added as an antioxidantto the stock solution of [2H4]-retinyl acetate in ethanol.
To prepare the labeled vitamin A in corn oil, a knownamount of [2H4]-retinyl acetate in ethanol is carefully

9HarvestPlus
1.5 Rationale for blood sampling times formeasurement of plasma isotopic ratiosof labeled to non-labeled retinol
Blood samples are collected at 24 hours, 3 days, and20 days after dosing. The 24 hour sample is collectedto provide qualitative information on absorptionand/or mobilization of the dose of labeled vitamin Afrom the liver. Plasma kinetic studies indicate that theplasma isotopic ratio of labeled to non-labeled retinolpeaks at approximately 24 hours after dosing (Haskellet al. 1998). Thus, if the plasma ratio of labeled to non-labeled vitamin A is low at this time point, it can beinterpreted as an indication of reduced absorptionand/or reduced mobilization of labeled vitamin A fromthe liver. This information is useful in analyzing thedata and interpreting the results. Specifically, the 24-hour plasma isotopic ratios are examined usingdescriptive statistics to identify outliers, and the 24-hour ratios are compared with estimates of vitaminA pool size to determine whether there is an associa-tion between the two variables.
The day-3 sample is collected because the plasmaisotopic ratio of labeled to non-labeled retinol measuredon day 3 is highly correlated with estimates of vitaminA pool size and provides a qualitative estimate of thetotal body pool of vitamin A, as described in Section1.3. Pre- and post-supplementation day-3 plasmaisotopic ratios of labeled to non-labeled vitamin A canbe used to assess whether vitamin A status haschanged in response to an intervention. Because theOlson equation has not yet been verified in pregnantand lactating women, it is currently recommended thatchanges in vitamin A status be assessed in thesepopulation groups using plasma isotopic ratios oflabeled to non-labeled retinol measured 3 days afterdosing. Also, in population groups that are known tohave high infection rates, it may be desirable to usethe day-3 plasma isotopic ratios in addition to the day-20 ratios to assess vitamin A status, because infectionis less likely to occur within a 3-day sampling periodthan within a 20-day sampling period. The day-20plasma isotopic ratio provides a quantitative estimate ofthe total body vitamin A pool size using the Olson equa-tion in school-age children and adults, as described inSection 1.2. A shorter sampling time of 14 days is
1.4.5 Blood collection, processing, and transportproceduresVenous blood samples are collected into evacuated,foil-wrapped, blood collection tubes specificallydesigned for the collection of serum (no additive) orplasma (containing EDTA as an anticoagulant). Theamount of blood required will vary by age group andsensitivity of the analytical method. Generally, 3–5 mLof blood is collected from infants and preschool-agechildren, and 7–10 mL of blood is collected fromschool-age children and adults. It is important toprotect the blood from light to minimize photodegra-dation (by using foil-wrapped tubes and working indim or gold fluorescent light), to keep the samplescool, and to handle the samples gently during allprocedures to prevent hemolysis. If serum is used, theblood is allowed to clot prior to centrifugation. Ifplasma is used, the tubes are inverted gently to mixthe blood with the anticoagulant. The foil is removedand the tubes are centrifuged at 2800 x g for 15minutes to separate serum or plasma. Equal portionsof serum or plasma are transferred to two screw-capvials, and flushed with nitrogen or argon gas. The vialsare wrapped in foil to protect the samples from lightand are stored in opaque boxes at ≤ –20oC. Twoaliquots of serum or plasma are prepared so that thereis a back-up sample in case one sample is damaged orlost. It is very important to clearly label vials and boxeswith waterproof markers. If the samples are to beshipped to another institution for analysis, they mustbe kept frozen during shipment. The samples can bepacked in dry ice or shipped on liquid nitrogen inspecially designed containers for biological materials.It is important to check with the local shippingcompany to determine specific regulations for ship-ping biological samples on dry ice or liquid nitrogen.
Biological waste that is generated during the bloodcollection and processing procedures must be handledand disposed of according to regulations for safehandling of biological materials and safe disposal ofbiological waste.

10HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
method, with selected ion monitoring carried out forfragment ions of the tBDMS derivatives at m/z 255(retinol) and m/z 263 ([2H8]-retinol).
1.7 Factors that may affect plasmaisotopic ratios of labeled to non-labeled retinol
Factors that may potentially affect the plasma isotopicratio of labeled to non-labeled vitamin A, as well asestimates of vitamin A pool size, are dietary vitamin Aintake during the mixing period, intestinal parasites,infection, inflammation, iron and zinc status, andintestinal malabsorption. Because newly absorbeddietary vitamin A is preferentially secreted into plasma,it is desirable to maintain dietary vitamin A intake at alow and constant level during the 20-day mixing periodafter administration of the labeled dose to minimizethe effect of dietary vitamin A on the plasma isotopicratio of labeled to non-labeled vitamin A. In commu-nity settings, dietary vitamin A intake cannot usually becarefully controlled; however, it is assumed that intakeis low and relatively constant in populations in whichvitamin A deficiency is endemic, and that the effect ofdietary vitamin A intake on the plasma isotopic ratio isminimal. Nevertheless, assessment of dietary vitamin Aintake during the 20-day mixing period is recommended.
Intestinal parasites may reduce absorption of thelabeled vitamin A dose. For efficacy studies, subjects aretreated with antihelminthics 1 to 2 weeks prior to begin-ning the study procedures. For effectiveness studies,subjects are not treated for intestinal helminths.
Subjects with clinical symptoms of infections areexcluded from participating in a study. However, it ispossible that subclinical infection or inflammation mayaffect the plasma isotopic ratio of labeled to non-labeledvitamin A. At present, there is no known associationbetween plasma concentrations of C-reactive protein(CRP) and plasma isotopic ratios of labeled to non-labeled retinol. Nevertheless, it is recommended thatplasma concentrations of CRP and α1-acid glycoprotein(AGP) be measured to examine whether there is anassociation between subclinical infection or inflamma-tion and plasma isotopic ratios of labeled to non-labeledvitamin A. When possible, iron and zinc status should
recommended for preschool-age children (Haskell etal. 2003); the optimal blood sampling time for infantsaged 0–12 months is not known.
1.6 Measurement of plasma isotopic ratiosof labeled to non-labeled retinol
Plasma isotopic ratios of deuterium labeled retinol tonon-labeled retinol are measured by GC-MS using electron ionization (Handelman et al. 1993) or elec-tron capture negative chemical ionization (Tang et al1998) as previously described; 13C/12C in retinol ismeasured by GC-C-IRMS (Tanumihardjo 2000). Thereferenced analytical methods provide detailed informa-tion on the procedures for carrying out the analyses.The following is a brief description of the proceduresfor measurement of plasma isotopic ratios of [2H4]-labeled retinol to unlabeled retinol using GC-MS andelectron ionization (Handelman et al. 1993). Retinol isextracted from plasma (1.0 mL) and purified by HPLC,and the tert-butyldimethylsilyl (tBDMS) derivative ofretinol is formed. An advantage of transforming retinolto its tBDMS derivative is that this derivative is stablefor at least one year; thus the GC-MS analyses do notneed to be performed immediately after isolating theretinol from the plasma. Nevertheless, it is recom-mended that the derivatized samples be analyzed byGC-MS as soon as possible. Plasma isotopic ratios of[2H4]-retinol to retinol are determined by GC-MS usinga quadrupole mass spectrometer and 70 eV electronionization. Selected ion monitoring is carried out forfragment ions of the tBDMS derivatives at m/z 255(retinol) and m/z 259 ([2H4]-retinol). A set of calibra-tion standards with [2H4]-retinol/retinol weight ratiosof 0.00, 0.0167, 0.050, 0.167 and 0.50 is analyzed witheach set of plasma samples. A linear regression equa-tion is calculated between the weight ratios of thecalibration standards and the integrated areas for m/z 259 and m/z 255. The area ratios for retinol fromthe plasma samples are substituted into the regressionequation to solve for weight ratios. The within-runprecision of the isotopic ratio measurements is esti-mated by periodically analyzing standards with eachset of plasma samples. The coefficient of variation forthe mean isotopic ratio measurements for the stan-dards is typically <5%. Plasma isotopic ratios of[2H8]-retinol/retinol are measured using the same

11HarvestPlus
vitamin A concentrations in deficient and marginallydeficient populations by making the assumption that<90% (for example 50% or 70%) of total body vitaminA is in the liver (Ribaya-Mercado et al. 2004a).
2|Study Protocols for Usingthe Paired Stable IsotopeDilution Technique
The paired stable isotope dilution technique consistsof estimating total body vitamin A pool size before andafter a vitamin A intervention in order to assess theimpact of the intervention on vitamin A status. Briefly,the mean change in vitamin A pool size (final pool sizeminus initial pool size) is calculated, and the meanchange in vitamin A pool size of the vitamin A supple-mented group(s) is compared with the mean changein vitamin A pool size of a negative control group.Procedures for carrying out a study using the pairedstable isotope dilution technique are described below.
2.1 Site selectionWhen choosing a study site, it is important to considerfactors that can affect the feasibility of successfullycarrying out the study procedures in the study popula-tion. Such factors include, 1) religious and/or culturalpractices that affect food intake and access to thestudy population, 2) the political climate and how thatmay affect study logistics and safety of study personneland participants, and 3) seasonal differences that mayaffect food availability and logistics, such as trans-portation difficulties due to increased probability offlooding and landslides.
2.2 Selection of study participantsThe population groups that are considered to be athigh risk of vitamin A deficiency are infants (6–12months of age), young children, and pregnant andlactating women in low-income communities in devel-oping countries. A recent study in the Philippinesshowed that the elderly are also at risk of vitamin Adeficiency (Ribaya-Mercado et al. 2004a). The studypopulation should be well defined, and subjectsshould be similar with respect to age, socio-economicstatus, and physiological status.
also be assessed because absorption and/or mobiliza-tion of vitamin A from the liver may be reduced iniron- and/or zinc-deficient subjects.
Because intestinal malabsorption affects plasmaisotopic ratios of labeled to non-labeled vitamin A, anindicator of intestinal absorption is useful. Intestinalpermeability tests or fat absorption tests can beperformed to obtain information on intestinal absorp-tion. However, these tests will not provide specificinformation on the absorption efficiency of the dose oflabeled vitamin A. Absorption of the dose of labeledvitamin A can be assessed qualitatively by collecting ablood sample 24 hours after the labeled vitamin A isadministered, as described in Section 1.5. Moresophisticated tracer techniques exist for assessingabsorption quantitatively (Green and Green 1997,Dueker et al. 2000), but these methods are not feasiblefor routine use in community settings.
1.8 Assessing adequacy of vitamin A status using the stable isotope dilution technique
Vitamin A deficiency is defined as a liver vitamin Aconcentration <0.07 µmol/g, and excessive vitamin Astatus is defined as >1.05 µmol/g (Olson 1987a).Estimates of total body vitamin A pool size obtainedby the stable isotope dilution method can be convertedto liver vitamin A concentrations by assuming thatliver weight is 2.4% of body weight in adults, 3% ofbody weight in children, and 4.2% of body weight ininfants (Olson 1987b). It is also assumed that the livercontains 90% of total body vitamin A, although theproportion of total body vitamin A in the liver varieswith vitamin A status. In well-nourished individuals, itis estimated that the liver contains ≥ 90% of total bodyvitamin A; in poorly or marginally nourished persons,the kidneys and other tissues contain an appreciableamount (10-50%) of total body vitamin A, thus theamount in liver can range from 50-90% (Olson 1987b).Thus, this method for converting total body pool sizeto liver vitamin A concentration is less than ideal, butuntil a cut-off value is determined for assessing theadequacy of vitamin A status based on total bodyvitamin A pool size, this method is recommended.Additional calculations can be done to estimate liver

12HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
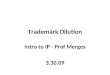
vitamin A pool size. During the 20-day mixing period,subjects consume their usual diets. The intervention isimplemented on study day 21, and, in this example,ends on study day 81. Thereafter subjects resume theirusual diets. After a 10-day stabilization period, asecond dose of labeled vitamin A is administered toparticipants (study day 92); blood samples areobtained at 24 hours, and 3 and 20 days after dosing(study days 93, 95, and 112) for qualitative and quanti-tative estimation of final vitamin A pool size.
The full study protocol for preschool-age children issimilar (Figure 3). However, because the dose oflabeled vitamin A mixes with endogenous vitamin Awithin 8–12 days after dosing in this age group, ablood sample is collected at 14 days after dosing forquantitative estimation of vitamin A pool size. Forpreschool-age children, a shorter stabilization periodof 7 days is recommended prior to administration ofthe second dose of labeled vitamin A.
The number of blood samples collected will differdepending on which analog of labeled vitamin A isused. If different forms of labeled vitamin A are usedto assess initial and final vitamin A pool sizes (e.g.,[2H4]-retinyl acetate and [2H8]-retinyl acetate), it is notnecessary to collect an additional blood sample priorto administering the second dose of labeled vitamin A.However, if the same form of labeled vitamin A is usedto estimate initial and final pool sizes (e.g., 13C-retinylacetate or [2H4]-retinyl acetate), it is necessary tocollect an additional blood sample prior to adminis-tering the second dose to correct for residual labeledvitamin A in plasma from the first dose (study day 92,Figure 2; study day 83, Figure 3).
Various approaches can be used to assess the plasmaretinol response to an intervention. The first approach isto measure plasma retinol concentrations on study days20 and 82, immediately before and after an interventionconsisting of daily administration of a source ofvitamin A. The mean change in plasma retinol concen-tration of the vitamin A supplemented group(s) iscompared with that of the negative control group toassess the effect of the intervention on plasma retinolconcentration. However, if subjects have marginal
2.3 Subject inclusion and exclusion criteria
Potential study subjects are recruited from communi-ties in which vitamin A deficiency is known to be apublic health problem. Subjects are examined by aphysician to assess their current state of health and toobtain their medical histories. A finger prick bloodsample is obtained for measurement of hemoglobinconcentration. Subjects with fever, chronic disease,diarrhea within the past week, malaria within the past2 weeks, severe anemia, or signs or symptoms ofxerophthalmia are excluded from the study. Participantswith severe anemia are treated with iron and those withxerophthalmia are treated with vitamin A according toWHO guidelines (WHO 1989, WHO/UNICEF/IVACGTask Force 1988). The study protocol must be approvedby the research and ethical review boards of the partici-pating institutions, and informed consent to participatein the study must be obtained from the study partici-pants or their legal guardians.
2.4 Full study protocols for using thepaired stable isotope dilutiontechnique
The study protocol will vary depending on the researchquestion(s) and the target group. The full studyprotocol is presented first, recognizing that it may notbe feasible or appropriate to use this protocol incertain situations. Partial study protocols appropriatefor certain target groups are presented later. Theadvantage of the full protocol is that it provides quali-tative information on apparent absorption and/ormobilization of the dose of labeled vitamin A, andboth qualitative and quantitative estimates of vitaminA pool size.
As shown in Figure 2, the full protocol for non-preg-nant, non-lactating adults and school-age childrenconsists of using the paired isotope dilution techniqueto assess total body vitamin A pool size before andafter a vitamin A intervention. Subjects are randomlyassigned to the intervention and control groups. Anoral dose of labeled vitamin A is administered toparticipants on study day 0 and blood samples arecollected at 24 hours, and 3 and 20 days after dosingfor qualitative and quantitative estimation of initial

13HarvestPlus
If small amounts of vitamin A are provided dailyduring the intervention (study days 21-81), the plasmaretinol concentration on study day 82 may reflect recentintake of supplemental vitamin A to some extent. Thus,the plasma retinol concentration can also be measuredon study day 92, after the 10-day stabilization period.
vitamin A status initially, it is possible that the firstdose of labeled vitamin A will increase their plasmaretinol concentrations. In that case, the plasma retinolconcentration measured on day 20 may be higher thanthe initial plasma retinol concentration at baseline. Ifthe plasma retinol concentration increases to withinthe normal homeostaticrange on day 20, the meanchange in plasma retinolconcentration betweenstudy days 20 and 82 inresponse to the interven-tion may be lower thanexpected. The secondapproach is to measureplasma retinol concentra-tion at baseline (study day0) before the first dose oflabeled vitamin A is admin-istered, and immediatelyfollowing the interventionon study day 82. In thiscase, the change in plasmaretinol concentrationreflects the effect of the firstdose of labeled vitamin Aplus the vitamin A providedduring the intervention. Thethird approach is to estimatethe effect of the interven-tion on plasma retinolconcentration by measuringplasma retinol concentra-tions immediately beforeand after the intervention,on study days 20 and 82, ina separate group ofsubjects who are notadministered labeledvitamin A but are exposedto the same intervention.
����� �� �� �� ������ �� � ���
�� � �
� ������� ������� �
� � ��� ����
��� � �
� ������� ������� �
� � ���
���� ��� � �
����������� �
� ��� � ��
��� ���� ��� ���� �
! ���������
� � �"�� ����#
! ����������
� � �"�� �����#
��� ���� ��� ���� �
! ���������
� � �"�� ����#
! ����������
� � �"�� �����#
� �# ��#$ �� ����
$ ������� � ���������� � $ �� ��# ������"��� � ���� �
� � ��� ����
FULL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN A INTERVENTION IN NON-PREGNANT, NON-LACTATING ADULTS
AND SCHOOL-AGE CHILDREN
FIGURE 2
� ����� �� ����� � ��
�� ����
�� ������� �� ���� �
��� ���� �� ���
������� ��� ��� �����
�� ����
�� ������� �� ���� �
� �� ��
��� ���� �� ��
������� ���
��� �����
! � �� � �����"� ��� ������! ����� ���
! �� ���� � �� ����� ���
��� ����
�� �� ����� �
������� �� ���
�� �� ����#
FULL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN A INTERVENTION IN PRESCHOOL-AGE CHILDREN
FIGURE 3

14HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
protocols that require fewer blood samples are recom-mended. Because the Olson equation has not beenverified to estimate vitamin A pool size in lactating andpregnant women, it is more appropriate to use the day-3 isotope dilution procedure for qualitative assessmentof vitamin A pool size in these population groups.
For non-pregnant, non-lactating adults and school-agechildren, a partial protocol that consists of collectingblood samples at 24-hours and 20 days after dosing isrecommended (Figure 4A) for quantitative estimationof vitamin A pool size. However, if blood can beobtained at only one time point, the blood sampleshould be collected at 3 or 20 days after dosing withlabeled vitamin A for qualitative or quantitative estima-tion of vitamin A pool size, respectively (Figure 4B).
For pregnant and lactating women, a 3-day isotopedilution procedure that consists of collecting bloodsamples at 24 hours and 3 days after dosing (Figure4C, 4D, pg 16) is recommended (These protocols canalso be used for non-pregnant, non-lactating adults andschool-age children.) However, if blood can be obtainedat only one time point, the blood sample should becollected at 3 days after dosing with labeled vitamin Afor qualitative estimation of vitamin A pool size.
For preschool-age children, a partial protocol thatconsists of collecting blood samples at 24 hours and14 days after dosing is recommended (Figure 5A, pg 17)for quantitative estimation of vitamin A pool size.However, if blood can be obtained at only one timepoint, the blood sample should be collected at 3 or 14days after dosing with labeled vitamin A for qualitativeor quantitative estimation of vitamin A pool size,respectively (Figure 5B, pg 17). Partial protocols using the 3-day isotope dilution procedure can also be used forpreschool-age children (Figures 5C, 5D, pg 18).
Whenever possible, the full protocol is recommended(except for pregnant and lactating women). A partialprotocol that includes a blood sample at 24 hours afterdosing with labeled vitamin A is preferable to aprotocol that consists of only a single blood sample at3, 14, or 20 days after dosing.
The plasma retinol concentration measured on studyday 92 may be a better indicator of the effect of theintervention on vitamin A status because at that timepoint the supplemental vitamin A that was providedduring the 60-day intervention had 10 days to mix withthe exchangeable vitamin A pool.
Plasma carotenoid concentrations reflect dietaryintake; therefore plasma carotenoid concentrations aremeasured on study days 20 and 82, immediatelybefore and after the intervention. If possible, plasmaconcentrations of ferritin and zinc are also measuredbecause iron and zinc status may affect vitamin Aabsorption and/or mobilization. It is important tomeasure plasma concentrations of CRP and AGP toevaluate the effect of subclinical infection or inflam-mation on plasma concentrations of retinol,carotenoids, ferritin and zinc, and on the isotopicratios of labeled to non-labeled retinol.
In preschool-age children, approaches the same asthose described above can be used to assess the effectof an intervention on plasma retinol concentration.Briefly, plasma retinol concentrations can be measuredimmediately before and after the intervention (studydays 14 and 76), or at baseline (study day 0) andimmediately after the intervention (study day 76).Alternatively, the initial plasma retinol concentrationcan be measured at baseline (study day 0), or immedi-ately before the intervention (study day 14), and thefinal plasma retinol concentration can be measuredfollowing the intervention after the 7-day stabilizationperiod (study day 83). Alternatively, plasma retinolconcentrations can be measured before and after theintervention in a separate group of children who areexposed to the same intervention but are not givenlabeled vitamin A.
2.5 Partial study protocols for using the paired stable isotope dilution technique
In certain situations, it may be necessary to use apartial version of the full study protocol. It is recog-nized that in some cultures it may not be possible tocollect blood at more than one time point after dosingwith labeled vitamin A. In these situations, partial study

15HarvestPlus
the plasma retinol concentration on study day 20, theeffect is likely to be less than on day 3 because by 20days after dosing the labeled vitamin A will have mixedto a greater extent with the endogenous vitamin A pool.The final plasma retinol concentration can be measuredimmediately following the intervention (study day 82),
When a 3-day isotope dilution protocol is used foradults and school-age children (Figures 4C-D, pg 16),the effect of the intervention on plasma retinol concen-trations can be assessed using several approaches. Ifthe initial dose of labeled vitamin A is relatively large (5–10 mg RE) and the subjects have marginal vitaminA status at baseline, it islikely that the plasmaretinol concentration onstudy day 3 will increasetransiently in response tothe dose of labeledvitamin A. Because thistransient increase willdepend on an individual’sinitial vitamin A status, itcannot be assumed thatthe mean increase inplasma retinol on day 3 inresponse to the labeleddose will be similar in alltreatment groups. For thisreason, when the inter-vention begins on studyday 4 (Figure 4C, pg 16),measurement of plasmaretinol concentration atbaseline (study day 0) ispreferable to measure-ment at 3 days afterdosing. The final plasmaretinol concentration canbe measured immediatelyfollowing the intervention(study day 65), or after the10-day stabilization period(study day 75). If the inter-vention begins on studyday 21 (Figure 4D, pg 16),the pre-interventionplasma retinol concentra-tion can be measured atbaseline (study day 0) oron day 20. Although theinitial dose of labeledvitamin A may still affect
� �� �� �� ������ �� ���
��� ���
� ������ ������� �
�� ���
� ������ ������� �
���� ��
� �� �� ������������� �����
�������� ������
������� �� ������������� ������ ���
���� �� �����
� ����� ���
� ������� � ������������
��������
����� ����� ��
�������������
� �� ����
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN AINTERVENTION IN NON-PREGNANT, NON-LACTATING ADULTS AND
SCHOOL-AGE CHILDREN USING 24-HOUR AND 20-DAY ISOTOPIC RATIOS
FIGURE 4A
� �� �� �� ������ �� ���
�� ���
� ������ ������ �
�� ���
� ������ ������ �
��� ��
� �� �� ����������� �����
������� �����
���� �� ������������ �����
���� �� �����
� ����� ��
� ������ � ����������
�������
���� ����� �
�����������
� �� ����
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN AINTERVENTION IN NON-PREGNANT, NON-LACTATING ADULTS AND
SCHOOL-AGE CHILDREN USING 3-DAY OR 20-DAY ISOTOPIC RATIOS
FIGURE 4B

16HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
retinol response to a particular intervention based onthe advantages and disadvantages of the differentapproaches, as described above.
For preschool-age children, the approaches are similarfor assessing the effect of the intervention on plasma
retinol concentrations whena 3-day isotope dilutionprotocol is used. When theintervention begins on studyday 4 (Figure 5C, pg 18), it ispreferable to measure theinitial plasma retinol concen-tration at baseline (study day0). The final plasma retinolconcentration can be meas-ured immediately followingthe intervention (study day65), or after the 7-day stabi-lization period (study day72). When the interventionbegins on study 15 (Figure5D, pg 18), the initialplasma retinol concentra-tion can be measured atbaseline (study day 0) or theday before the interventionbegins (study day 14). Thefinal plasma retinol concen-tration can be measuredimmediately following theintervention (study day 76)or after the 7-day stabiliza-tion period (study day 83).
In addition to the bio-chemical data, informationon anthropometry, dietaryintake, and morbidity iscollected. Measurements ofweight, height (or length)and mid-upper arm circum-ference are recommended.Dietary intake can beassessed weekly by foodfrequency questionnaires;morbidity can be assessedweekly by questionnaire.
or after the 10-day stabilization period (study day 92;Figure 4D). The rationale for the different approaches isthe same as that described for the full study protocol.The choice of a day-3 protocol will depend on whether aprotocol of shorter duration is desirable, and whichmethod is considered optimal for assessing the plasma
������ � �� �������� �
�� ��
�� ������
������� �
�� ��
�� ������ ������� �
�� � ��
� �� �� ������������ �����
������ ������
���!��� �� �� ��
������
������ ���!���
�� �� ��
� ���� ���
� ������� � ������������
������
����� ����� ��
� �����������
�� �� ��"
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN A INTERVENTION USING 3-DAY ISOTOPE DILUTION PROCEDURE IN ALL ADULTS
AND SCHOOL-AGE CHILDREN (INTERVENTION BEGINS ON STUDY DAY 4)
FIGURE 4C
� �� �� �� ������ �� ��
�� ���
�� ��� � � ������ �
��� ���
�� ��� � � ������ �
���� ���
� �� ��� ����������� � ����
������� �����
������� ��� ����������� �����
������� ��� ����
� ����� ��
� ������ � �� �� ����
�������
���� ����� �
������������
�� ��� ��� !
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN A INTERVENTION USING 3-DAY ISOTOPE DILUTION PROCEDURE IN ALL ADULTS
AND SCHOOL-AGE CHILDREN (INTERVENTION BEGINS ON STUDY DAY 21)
FIGURE 4D

17HarvestPlus
can be estimated by using liver vitamin A concentra-tions and estimates of liver weight as a proportion ofbody weight, as described in Section 1.8. In general,interventions that provide close to the RDA(FAO/WHO 2002) of vitamin A, 5–7 days/week, are8–12 weeks in duration.
2.6 Estimation of duration of intervention
The duration of an intervention will vary depending onthe amount of vitamin A provided and the frequencywith which the vitamin A is administered. Theexpected effect of supplementation with vitamin A onvitamin A pool size inadults and school-age children can be estimatedby assuming that 50% ofsupplemental vitamin A isretained in the body and~0.5%/d of the vitamin Apool is catabolized. Forpreschool-age children, itcan be assumed that ~50%of supplemental vitamin Ais retained and ~2.2%/d ofthe vitamin A pool is catab-olized (Haskell et al. 2003).These assumptions areused to estimate theexpected effect on vitaminA pool size of adminis-tering a particular amountof supplemental vitamin Afor a particular period oftime. Initial estimates ofvitamin A pool size can beobtained from the scientificliterature for different agegroups with low or highsocio-economic status(Olson et al. 1984, Olson1979, Flores and de Araujo1984, Dahro et al. 1983,Dorea et al. 1984,Suthutvoravoot and Olson1974). Most of the publisheddata on liver vitamin Aconcentrations are basedon direct measurement ofliver vitamin A in specimensobtained at autopsy. Totalbody vitamin A pool size
� ����� �� ����� � ��
�� ����
�� ������� �� ���� �
��� ���� �� ���
������ ��� �����
�� ����
�� ������� �� ���� �
� �� ��
��� ���� �� ���
������ ���
�����
! � �� � �����"� ��� ������! ����� ���
! �� ���� � �� ����� ���
��� ����
�� �� ����� �
������� �� ���
�� �� ����#
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN A INTERVENTION IN PRESCHOOL-AGE CHILDREN
USING 24-HOUR AND 14-DAY ISOTOPIC RATIOS
FIGURE 5A
� ����� �� ����� � ��
�� ����
�� ������� �� ���� �
��� ���� �� ���
���� �� ������
�� ����
�� ������� �� ���� �
� ��� ���
��� ���� �� ��
���� �� ������
� ��� � �����!� ��� ������ ����� ���
�� ���� � �� ����� ���
��� ����
�� �� ����� �
������� �� ���
�� �� ����"
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A
VITAMIN A INTERVENTION IN PRESCHOOL-AGE CHILDREN
USING 3-DAY OR 14-DAY ISOTOPIC RATIOS
FIGURE 5B

18HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
change in vitamin A pool size. Estimates of initialvitamin A pool size can be obtained from the scien-tific literature. The expected change in vitamin A poolsize can be estimated from results of previous studiesor by estimating the expected changes, based onassumptions regarding retention and catabolism of
vitamin A, as describedabove. An estimate of thestandard deviation of thechange in vitamin A poolsize can be obtained fromprevious studies that reportmean changes in vitamin Apool size in response to anintervention. The estimatedsample size should beincreased to adjust forpotential drop-outs andpossible loss of data due tofield or laboratory errors, orother causes during thecourse of the study.
2.8 Statisticalanalysis
Descriptive statistics arecalculated for all variablesto check for outliers.Variables that are notnormally distributed areappropriately transformedto approximate a normaldistribution. Change invitamin A pool size andchange in plasma retinolconcentration are examinedin relation to plasmaconcentrations of CRP andAGP to determine whetherthere is an associationbetween the indicators ofvitamin A status and indica-tors of subclinical infectionand inflammation.
2.7 Sample size calculationThe sample size calculation and plan for data analysisare performed in consultation with a statistician. Tocalculate the sample size, information is needed oninitial vitamin A pool size, the expected change invitamin A pool size, and the standard deviation of the
������ � �� ������� ��
�� ��
�� ������
������� �
� ��
�� ������ ������� �
�� � ��
� � �� ������������ �����
������� ������
�� ��� �� �� ���������
������ �� ���
�� �� ��
� ���� ���
� ������� � ������������
�������
����� ����� ��
� �����������
�� � ��!
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN A INTERVENTION USING 3-DAY ISOTOPE DILUTION PROCEDURE IN
PRESCHOOL-AGE CHILDREN (INTERVENTION BEGINS ON DAY 4)
FIGURE 5C
� ����� �� ����� � ��
��� ����
�� ������� ������� �
�������� ������
������ ��� ����
�� ����
�� ������� ������� �
����� ���
�������� �����
������ ����
� ��� �������!����� ������ ����� ����
������� � ������������
��������
����� ����� ��
��������������
�� �� ����"
PARTIAL PROTOCOL FOR ASSESSING IMPACT OF A VITAMIN A INTERVENTION USING 3-DAY ISOTOPE DILUTION PROCEDURE IN
PRESCHOOL-AGE CHILDREN (INTERVENTION BEGINS ON DAY 15)
FIGURE 5D

19HarvestPlus
sources, the diet is carefully controlled throughout theentire study period. This requires that the study becarried out in a controlled setting with access to dieticians and a research kitchen where foods can becarefully prepared using standardized recipes.
3.1 Site selectionThe considerations for selection of the study site arethe same as those described in Section 2.1. In addi-tion, adequate facilities and trained personnel must beavailable for careful preparation of controlled diets andcareful monitoring of food consumption. Access toclinical staff is also required to monitor the healthstatus of the participants throughout the study period.
3.2 Selection of study participantsBecause the study diets must be carefully controlled andfood consumption must be monitored, access to thestudy participants is necessary throughout the day forthe entire study period. Thus, a study group should beselected that is willing to consume their daily meals andsnacks under supervision at the study facility (i.e., meta-bolic wards/out-patient facilities, boarding schools, etc.).
3.3 Subject inclusion and exclusion criteria
Relative vitamin A equivalency factors may vary withvitamin A status. Thus, the initial vitamin A status ofthe subjects selected for the study should be similar. Ifthe purpose of the study is to estimate vitamin Aequivalency factors in populations at risk of vitamin Adeficiency, study subjects are recruited from communi-ties in which vitamin A deficiency is known to be apublic health problem. The subjects are screened forplasma concentrations of retinol, CRP and AGP, andfor hemoglobin concentration. The subjects are exam-ined by a physician to assess their current state ofhealth and to obtain their medical histories; exclusioncriteria are the same as those described in Section 2.3.Eligible subjects with the lowest plasma retinolconcentrations and normal CRP and AGP concentra-tions are selected for the study.
Correlation analysis is used to determine whether thereis an association between 24-hour plasma isotopicratios and day-3 plasma isotopic ratios and/or estimatesof total body vitamin A pool size. Final mean vitamin Apool sizes or final mean day-3 plasma isotopic ratiosbetween the supplemented and non-supplementedgroups are compared using analysis of covariance withinitial values and any other variables as covariates.Final mean plasma retinol and carotenoid concentra-tions between the supplemented andnon-supplemented groups are compared using analysisof covariance with initial values and any other variablesas covariates. The relationship between change inplasma retinol concentration and change in vitamin Apool size is examined using regression analysis.
3|Paired Stable IsotopeDilution Technique for Estimating Relative Vitamin A EquivalencyFactors for β-carotene
The paired isotope dilution technique can be used to estimate the relative vitamin A equivalency of β-carotene from plant source foods (Haskell et al. 2004).The study design consists of an intervention group(s)(high β-carotene vegetables or fruit), a negative controlgroup (low vitamin A vegetables or fruits), and a posi-tive control group (retinyl palmitate). Vitamin A poolsize is estimated before and after approximately 60days of intervention. The mean change in vitamin Apool size is estimated for each treatment group (finalpool size minus initial pool size). The relative vitaminA equivalency of β-carotene from plant sources ofvitamin A is estimated by comparing the mean changein vitamin A pool size of the plant group(s) with thatof the retinyl palmitate group, as described below. It isalso possible to assess the efficacy of supplementationwith plant sources of vitamin A for improving vitaminA status by comparing the mean change in vitamin Apool size of the plant group(s) with that of the nega-tive control group. To obtain accurate estimates of therelative vitamin A equivalency of β-carotene from plant

20HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
3.5 Selection of high β-carotene and low vitamin A foods
A low vitamin A diet is developed in consultation witha dietician. The diet is based on foods typicallyconsumed by the study population and is replete in allnutrients except vitamin A, which is present in lowamounts (~25% of the RDA). The plant source food(s)is carefully selected based on the β-carotene content,and availability and acceptability to the study population.To determine which high β-carotene foods (dark greenleafy vegetables, dark orange vegetables and fruits) toinclude in the study, focus group discussions areconducted to determine which foods are locally availableand acceptable to the study population, and to obtaininformation on usual food preparation techniques.
The food preparation techniques that are used in thestudy will depend on the research question. If thepurpose of the study is to assess the vitamin A equivalency of β-carotene from plant sources of vitaminA as the foods are typically consumed, the food isprepared according to the traditional food preparationtechniques. If the purpose of the study is to assess theeffect of food preparation techniques on estimates ofvitamin A equivalency, a variety of preparation methodsare used. In either case, the foods are prepared in theform they will be consumed by the study participants,and samples of each food are analyzed by HPLC todetermine the carotenoid content. The portion sizerequired to supply ~80–100+ % of the RDA for the studypopulation is determined based on the all-transβ-carotene content of the food and the currently recom-mended vitamin A equivalency factor of 12:1.Cis-β-carotenes and the other provitamin A carotenoidsare quantified, but because of uncertainty regarding thebioavailability and vitamin A equivalency of thesecarotenoids, they are not included in the determinationof the portion size. An acceptability trial is conducted todetermine whether the study population is willing toconsume the specified portion size of the selectedfood(s). It may be necessary to provide the food(s) morethan once daily if the portion size is too large. Theselected plant source food(s) is obtained from thesame supplier throughout the study period to minimizevariability in the β-carotene content. Samples of theprepared foods are collected weekly for analysis of thecarotenoid content.
3.4 Study design and protocolThe study design consists of a group(s) that receiveshigh β-carotene vegetables or fruit and a corn oil capsule,a negative control group that receives low β-carotenevegetables or fruit and a corn oil capsule, and a positivecontrol group that receives low β-carotene vegetables orfruit and a capsule containing corn oil in which isdissolved an amount of retinyl palmitate equivalent tothe amount of vitamin A in the high β-carotene vegeta-bles or fruit, as estimated by assuming 1 µg retinol =12 µg β-carotene (Institute of Medicine 2001); foodand capsule supplements are provided daily:
Capsule Food supplementPlant source food(s)
corn oil High β-carotenevegetable or fruit
Negative controlcorn oil Low vitamin A
vegetable or fruitPositive control
retinyl palmitate Low vitamin A in corn oil vegetable or fruit
The full study protocol described above is thepreferred study design; however, a partial version ofthe protocol can be used if it is not feasible to collectall of the blood samples required in the full protocol.Note that this study design differs from that of the fullprotocol for community-based studies in that the dietis controlled. As shown in Figure 6, subjects consumea controlled low vitamin A diet during the 20-daymixing periods after administration of the initial andfinal doses of labeled vitamin A and during the 10-daystabilization period following the intervention. Duringthe intervention period, subjects consume the lowvitamin A diet in addition to their assigned food andcapsule supplements.
In addition to the biochemical data, anthropometricdata are collected and subjects are monitored formorbidity weekly. Because the diet is carefullycontrolled, it is not necessary to obtain information ondietary intake.
InterventionGroup

21HarvestPlus
(µg β-carotene consumed per day in the vegetableor fruit groups/µg RE consumed per day in theretinyl palmitate group) * (mean ∆ in net vitaminA pool size [relative to the negative control group]of the retinyl palmitate group/mean ∆ in netvitamin A pool size [relative to the negative controlgroup] of the vegetable or fruit groups)
The relative vitamin A equivalency factor provides anestimate of the equivalency of β-carotene from aparticular food source in relation to retinyl palmitate.Thus, an estimated relative vitamin A equivalencyfactor of 10:1 for a particular plant source food meansthat 10 µg of β-carotene from that food is equivalentto 1 µg of retinol as retinyl palmitate.
The impact of supplementation with plant sources ofvitamin A on vitamin A status is assessed bycomparing the mean change in vitamin A pool size inthe supplemented group(s) with the mean change invitamin A pool size in the negative control group.
3.8 Sample size calculationThe sample size is calculated using procedures thesame as those described in Section 2.7.
The low vitamin A vegetables or fruits should also belocally available and acceptable to the study popula-tion. Procedures the same as those described abovecan be used to select the low vitamin A plant sourcefoods. The types and amounts of fiber in the portion oflow vitamin A vegetables or fruits should be similar tothat of the high β-carotene vegetables or fruits. It maybe necessary to adjust the amounts of low vitamin Acontaining foods in the diet to achieve similar typesand amounts of dietary fiber in all treatment groups.
3.6 Estimation of duration of intervention
The duration of the intervention can be estimated asdescribed in Section 2.6.
3.7 Procedures for estimating relativevitamin A equivalency factors
The relative vitamin A equivalency of β-carotene fromplant source foods is estimated by comparing themean changes in vitamin A pool size in the groupsthat receive plant sources of vitamin A with that in thegroup that receives retinyl palmitate. First, the meanchange in vitamin A pool size is determined for eachtreatment group, controlling for initial values. Second,the mean change in vitamin A pool size in the negativecontrol group is subtractedfrom the mean change invitamin A pool size in eachof the groups that receiveda vitamin A source toobtain the net mean changein vitamin A pool size inrelation to the negativecontrol group. Third, thenet mean changes invitamin A pool size in thegroups that receive plantsources of vitamin A arecompared with the netmean change in vitamin Apool size in the retinylpalmitate group to estimatethe relative vitamin A equiv-alency of the plant sourcesof vitamin A, using thefollowing equation:
� �� �� �� �������� ���
��� ���
� ������ ������� �
�� ���
� ������ ������� �
���� ��
� �� �� ������������� �����
�������� ������
������ �� � �� �� ��
�������� ������
�� ��� �� �
�� �� ��
� �� ������� � ���
� ������� � ������������
��������
����� ����� ��
�������������
� �� ���!
PAIRED ISOTOPE DILUTION TECHNIQUE: ESTIMATING THE RELATIVE
VITAMIN A EQUIVALENCY OF β-CAROTENE AND IMPACT OF AN
INTERVENTION IN NON-PREGNANT, NON-LACTATING ADULTS
AND SCHOOL-AGE CHILDREN (RESEARCH SETTING)
FIGURE 6

22HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
In addition, the elderly are also at risk of vitamin A deficiency, as has been documented in a recent studyin rural Philippines, where 14.5% of men and womenbetween 60 and 88 years old had low liver vitamin Aconcentrations (<0.07 µmol/g) as assessed by stableisotope dilution methods (Ribaya-Mercado et al. 2004a).
4.2 Sample size calculation.The sample size is calculated using the proceduresdescribed in Section 2.7.
4.3 Subject inclusion and exclusioncriteria for studies monitoringprogram effectiveness
The subject inclusion and exclusion criteria are similarto those of other labeled vitamin A studies mentionedin Section 2.3. That is, the participants should be ingeneral good health, with no major chronic diseases,acute illnesses, or gastrointestinal problems. Becausethe goal of the study in Nicaragua was to documentwhether the new national program of sugar fortifica-tion with vitamin A had an impact on the vitamin Astatus of school-age children during the inaugural yearof the program, it was important that the results werenot confounded by other existing vitamin A interven-tion programs such as the Nicaraguan National HealthCampaign, which administers high-dose vitamin A(200,000 IU or 60,060 µg vitamin A) twice a year tochildren <5 years of age. Thus, in that study (Ribaya-Mercado et al. 2004b), only children who did notreceive a high-dose vitamin A supplement during theprevious year were included as study participants.
4.4 Importance of periodic monitoring of vitamin A status in interventionprograms
Periodic monitoring of the vitamin A status of targetgroups is desirable to document the continued effec-tiveness of intervention programs in maintaining anadequate vitamin A status in vulnerable groups. Inaddition, periodic monitoring is done to ensure thatliver vitamin A stores remain at safe levels. Althoughthe upper safe limit of liver vitamin A stores is unknown,a physiologic range of liver vitamin A concentration isbetween 0.07 and 1.05 µmol/g liver (between 20 and300 µg/g liver) (Olson 1984). It would be prudent toperiodically monitor liver vitamin A concentrations in
4|Monitoring theEffectiveness of Vitamin AIntervention Programs
The stable isotope dilution technique has been shownto be very useful for monitoring the effectiveness ofprograms designed to improve the vitamin A status ofpopulations. For example, when the Republic ofNicaragua initiated a national program of vitamin Afortification of table sugar for domestic consumption,the effectiveness of the program was monitored in 21school-age children by measuring their total bodyvitamin A pool sizes using the stable isotope dilutiontechnique at baseline and 1 year after the start of theavailability of fortified sugar in their local markets(Ribaya-Mercado et al. 2004b). To avoid seasonal vari-ability in carotene-rich foods, the study was conductedduring the same calendar month, albeit 1 year apart. Noattempt was made by the investigators to influence thesubjects’ consumption of sugar or other aspects of theirdiet. An oral dose of [2H4]-retinyl acetate was providedat baseline, and [2H8]-retinyl acetate after 1 year, in orderto distinguish [2H8]-retinol from any residual [2H4]-retinol. In this study, the minimum of 1 blood draw wasobtained at baseline and at the repeat test 1 year later.The blood was obtained 21 days after dosing with thelabeled vitamin A and was used for estimation of totalbody vitamin A pool size using the Olson equation andfor determination of plasma retinol. Total body vitaminA increased in all of the 21 study participants during theyear, with a median increase of 112%. In contrast,plasma retinol increased in 16 subjects and decreasedin 5 subjects; the median change was an increase of18.6%. Thus, plasma retinol changes were small andinconsistent, unlike the changes in total body vitamin Apool size obtained using stable isotope dilutionmethodology, making the latter the method of choicefor monitoring the effectiveness of vitamin A programs.
4.1 Selection of study participantsIn monitoring program effectiveness, it is important tochoose subjects who are representative of the program’sintended target groups. In vitamin A interventionprograms, the target groups are those who are at risk forvitamin A deficiency, i.e., children and pregnant orlactating women, especially those residing in poor areas.

23HarvestPlus
aged >60 years, acceptable vitamin A intakes were esti-mated to be 490 and 393 µg RAE/d, respectively. Thesenumbers may be rounded to 500 and 400 µg RAE/d,respectively. On the basis of these results, the 1989Philippine recommendations of 525 and 450 µg RE/d,and the 2002 FAO/WHO recommendations of 600 and500 µg RE/d for elderly men and women appearadequate, whereas the current US recommendations of900 and 700 µg RAE/d for elderly men and women arehigh. The procedure of estimating vitamin A require-ments described above is possible only in populationswith minimally adequate vitamin A status. It will not bevalid in populations with liver vitamin A stores thatgreatly exceed the minimum adequate value of 0.07µmol/g because their vitamin A intakes are presumablywell above the vitamin A requirements. It is of interestto note that total body vitamin A and/or liver vitamin A(both estimated using stable isotope dilution tech-niques), correlated with dietary RAE, preformed vitaminA, β-carotene, fat, and protein; in contrast, serumretinol was unrelated to any of these dietary intakes(Ribaya-Mercado et al. 2004a). The above technique ofobtaining information regarding dietary vitamin Arequirements relied primarily on dietary intake data andassessment of liver vitamin A stores by stable isotopedilution. Other more sophisticated isotope techniques(e.g., model-based compartmental analysis) (Green andGreen 1990) are available which can be used forobtaining information about dietary vitamin A require-ments based on kinetic methods for studying vitamin Adynamics in vivo.
SummaryVitamin A tracer dilution methodology is a powerfultool for assessing vitamin A status and for evaluatingthe efficacy and effectiveness of vitamin A interventionprograms. The method can be applied in both clinicaland field settings. It is useful for estimating relativevitamin A equivalency factors for β-carotene, and couldbe used to obtain information on vitamin A require-ments. It is useful for assessing a wide range of humanvitamin A status, from deficiency to sub-toxicity. It isthe only indirect measure of vitamin A status thatprovides a quantitative estimate of total body vitaminA pool size and liver vitamin A concentration.
a small number of subjects, especially when multiplevitamin A intervention programs are in place, toconfirm that continued increased intakes of vitamin Afrom all sources pose no risk of adverse health effects.Stable isotope dilution methods are the only indirectmethods available for the quantitative estimation ofliver vitamin A stores. The fortified food used invitamin A programs should be continuously moni-tored for quality control to ensure that vitamin Alevels do not shift outside the desired range of safeand efficacious levels.
4.5 Subject inclusion and exclusion criteriafor periodic monitoring of vitamin Astatus in intervention programs
Because in a national vitamin A fortification programeveryone is exposed to the nutrition intervention, peri-odic monitoring of vitamin A status by stable isotopedilution methods is recommended in a small cross-sectional sample of subjects not only from poorcommunities, but also from higher-income communi-ties. The study participants should include children,women of reproductive age, and the elderly. Theyshould be generally healthy with no major chronicdiseases, acute illnesses, or gastrointestinal problems.
5|Studies on Vitamin ARequirements
The stable isotope dilution methodology has the poten-tial to provide useful information regarding the dietaryvitamin A requirements of various age groups. Forexample, the dietary vitamin A intakes (retinol activityequivalents, RAE) of >60-year-old Filipinos with adequate(>0.07 µmol/g or >20 µg/g) or low (<0.07 µmol/g) livervitamin A concentrations have been studied (Ribaya-Mercado et al. 2004a). An acceptable or sufficientdietary vitamin A intake value (in µg RAE/kg body wt)associated with adequate liver vitamin A was estimatedby taking the mean RAE ± 2 SDs consumed by subjectswhose liver vitamin A concentrations were adequate anddividing this value by their mean body weight. Adding2 SDs to the mean RAE gives a margin of safety to coverthe needs of most healthy elders. The acceptable dailydietary vitamin A intake associated with adequate livervitamin A reserves was estimated to be 6.4 µg RAE/kgbody wt. For a reference 76-kg man and a 61-kg woman

24HANDBOOK ON VITAMIN A TRACER DILUTION METHODS TO ASSESS STATUS AND EVALUATE INTERVENTION PROGRAMS
Loerch JD, Underwood BA, Lewis KC. Response of plasma levels of vitamin Ato a dose of vitamin A as an indicator of hepatic vitamin A reserves in rats. J Nutr 1979;109:778–86.
Olson JA. Liver vitamin A reserves of neonates, preschool children and adultsdying of various causes in Salvador, Brazil. Arch Latinoam Nutr1979;29:524–45.
Olson JA, Gunning DB, Tilton RA. Liver concentrations of vitamin A andcarotenoids, as a function of age and other parameters, of American childrenwho died of various causes. Am J Clin Nutr 1984;39:903–910.
Olson JA. Serum levels of vitamin A and carotenoids as reflectors of nutritionalstatus. J Natl Cancer Inst 1984;73:1439–44.
Olson JA. Should RDA values be tailored to meet the needs of their users? J Nutr 1987a;117:220-2.
Olson JA. Recommended dietary intakes (RDI) of vitamin A in humans. Am J Clin Nutr 1987b;45:704–16.
Ribaya-Mercado JD, Mazariegos M, Tang G, Romero-Abal ME, Mena I,Solomons NW, Russell RM. Assessment of total body stores of vitamin A inGuatemalan elderly by the deuterated-retinol-dilution method. Am J Clin Nutr1999;69:278–84.
Ribaya-Mercado JD, Solon FS, Solon MA, Cabal-Barza MA, Perfecto CS, TangG, Solon JAA, Fjeld CR, Russell RM. Bioconversion of plant carotenoids tovitamin A in Filipino school-age children varies inversely with vitamin A status.Am J Clin Nutr 2000;72:455–65.
Ribaya-Mercado JD, Solon FS, Dallal GE, Solomons NW, Fermin LS,Mazariegos M, Dolnikowski GG, Russell RM. Quantitative assessment of totalbody stores of vitamin A in adults with the use of a 3-d deuterated-retinol-dilution procedure. Am J Clin Nutr 2003;77:694–9.
Ribaya-Mercado JD, Solon FS, Fermin LS, Perfecto CS, Solon JAA, DolnikowskiGG, Russell RM. Dietary vitamin A intakes of Filipino elders with adequate orlow liver vitamin A concentrations as assessed by the deuterated-retinol-dilution method: implications for dietary requirements. Am J Clin Nutr2004a;79:633–41.
Ribaya-Mercado JD, Solomons NW, Medrano Y, Bulux J, Dolnikowski GG,Russell RM, Wallace CB. Use of the deuterated-retinol-dilution technique tomonitor the vitamin A status of Nicaraguan schoolchildren 1 y after initiationof the Nicaraguan national program of sugar fortification with vitamin A. Am J Clin Nutr 2004b;80:1291–8.
Suthutvoravoot S, Olson JA. Plasma and liver vitamin A in a normal populationof urban Thai. Am J Clin Nut 1974;27:883–91.
Tang G, Qin J, Dolnikowski GG. Deuterium enrichment of retinol in humansdetermined by gas chromatography electron capture negative chemicalionization mass spectrometry. J Nutr Biochem 1998;9:408–14.
Tang G, Qin J, Dolnikowski GG, Hao L, Yin S, Russell RM. Use of a short-termisotope-dilution method for determining the vitamin A status of children. Am J Clin Nutr 2002;76:413–8.
Tanumihardjo SA. Vitamin A status assessment in rats with 13C4-retinyl acetateand gas chromatography/combustion/isotope ratio mass spectrometry. J Nutr 2000;130:2844–9.
Tanumihardjo SA. Application of 13C4-retinyl acetate and gas chromatography-combustion isotope ratio mass spectrometry to vitamin A assessment in thehuman. FASEB J 2001;15(4):A256; Abstract 228.5.
Tanumihardjo SA. A small physiological dose of vitamin A (17.5 µmol) takes4 years to disappear in healthy individuals. XXI International Vitamin AConsultative Group (IVACG) Meeting. Marrakech, Morocco. 2003. Abstract, p.31.
WHO. Preventing and controlling iron deficiency anaemia through primaryhealth care: A guide for health administrators and programme managers.Geneva: World Health Organization. 1989.
WHO/UNICEF/IVACG Task Force. Vitamin A supplements. A guide to their usein the treatment and prevention of vitamin A deficiency and xerophthalmia.Geneva: World Health Organization. 1988.
ReferencesAdams WR, Green MH. Prediction of liver vitamin A in rats by an oral isotopedilution technique. J Nutr 1994;124:1265–70.
Barua AB, Furr HC. Properties of retinoids: structure, handling, andpreparation. In: Redfern C, ed. Retinoid Protocols. Totowa, NJ: Humana Press1998:3–28.
Bausch J, Rietz P. Method for the assessment of vitamin A liver stores. ActaVitaminol Enzymol 1977;31:99–112.
Dahro M, Gunning D, Olson JA. Variations in liver concentrations of iron andvitamin A as a function of age in young American children dying of the suddeninfant death syndrome as well as of other causes. Int J Vit Nutr Res1983;53:13–18.
Dorea JG, Souza JA, Galvao MO, Iunes MAF. Concentration of vitamin A in theliver of foetuses and infants dying of various causes in Brasilia, Brazil. Int J VitNutr Res 1984;54:119–23.
Dueker SR, Lin Y, Buchholz BA, Schneider PD, Lame MW, Segall HJ, Vogel JS,Clifford AJ. Long-term kinetic study of β-carotene, using accelerator massspectrometry in an adult volunteer. J Lipid Res 2000;41:1790–1800.
FAO/WHO. Human vitamin and mineral requirements. Report of a jointFAO/WHO expert consultation. Rome: World Health Organization, Food andAgriculture Organization of the United Nations, 2002.
Flores H, de Araujo CRC. Liver levels of retinol in unselected necropsyspecimens: a prevalence survey of vitamin A deficiency in Recife, Brazil. Am J Clin Nutr 1984;40:146–52.
Furr HC, Amedee-Manesme O, Clifford AJ, Bergen III HR, Jones AD, AndersonDP, Olson JA. Vitamin A concentrations in liver determined by isotope dilutionassay with tetradeuterated vitamin A and by biopsy in generally healthy adulthumans. Am J Clin Nutr 1989;49:713–16.
Green MH, Green JB. Experimental and kinetic methods for studying vitamin Adynamics in vivo. Methods Enzymol 1 1990;190:304–17.
Green MH, Green JD. Use of a plasma dual isotope ratio method to measurevitamin A absorption. FASEB J 1997;11:A142.
Handelman GJ, Haskell MJ, Jones AD, Clifford AJ. An improved protocol fordetermining ratios of retinol-d4 to retinol isolated from human plasma. Anal Chem 1993;65:2024–8.
Haskell MJ, Handelman GJ, Peerson JM, Jones AD, Rabbi A, Awal MA, WahedMA, Mahalanabis D, Brown KH. Assessment of vitamin A status by thedeuterated retinol dilution technique and comparison with hepatic retinolconcentration in Bangladeshi surgical patients. Am J Clin Nutr 1997;66:67–74.
Haskell MJ, Islam MA, Handelman G, Peerson JM, Jones AD, Wahed MA,Mahalanabis, D, Brown KH. Plasma kinetics of an oral dose of [2H4] retinylacetate in adults with low or high total body stores of vitamin A. Am J ClinNutr 1998;68-90-5.
Haskell MJ, Mazumder RN, Peerson JM, Jones AD, Wahed MA, MahalanabisD, Brown KH. Use of the deuterated retinol dilution (DRD) technique to assesstotal body vitamin A stores of adult volunteers consuming different levels ofvitamin A. Am J Clin Nutr 1999;70:874–80.
Haskell MJ, Lembcke JL, Salazar M, Green MH, Peerson JM, Brown KH.Population-based plasma kinetics of an oral dose of [2H4]retinyl acetate amongpreschool-age Peruvian children. Am J Clin Nutr 2003;77:681–6.
Haskell MJ, Jamil KMA, Hassan F, Peerson JM, Hossain MI, Fuchs GJ, BrownKH. Daily consumption of Indian spinach (Basella alba) or sweet potatoes hasa positive impact on total body vitamin A stores of Bangladeshi men. Am J ClinNutr 2004;80:705–14.
Hicks VA, Gunning DB, Olson JA. Metabolism, plasma transport and biliaryexcretion of radioactive vitamin A and its metabolites as a function of liverreserves of vitamin A in the rat. J Nutr 1984;114:1327–33.
Institute of Medicine. Dietary reference intakes: vitamin A, vitamin K, arsenic,boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel,silicon, vanadium and zinc. Washington, DC: National Academy Press. 2001.

c/o International Food Policy Research Institute2033 K Street, NW, Washington, DC 20006-1002 USA Phone: 1-202-862-5600 • Fax: 1-202-467-4439 • HarvestP [email protected] rg
Breeding Crops for Better Nutrition