Embed Size (px)
Citation preview

SPRING 2008 www.hemophilia.ca VOL 43 NO 2
Canadian Hemophilia SocietyServing the Bleeding Disorders Community
Hem philiaTODAY
WORLD HEMOPHILIA DAY • RESEARCH • CHAPTER SPOTLIGHT • OUR STORIES • MEDICAL NEWS
Our MissionThe Canadian Hemophilia Society strives toimprove the health and quality of lifefor all people with inherited bleeding disorders,and to find a cure.
Research1960
2008
Nikolas and Patrick Muinonen
Eddy and Donald Burns
has made great strides in lessthan 50 years, but a curehas yet to be found.
SPRING 2008 • VOL 43 • NO 2
Hemophilia Today625 President Kennedy Avenue, Suite 505Montreal, Quebec H3A 1K2www.hemophilia.caPhone: 514 848-0503Fax: 514 848-9661Toll-free: 1 800 [email protected]
Hemophilia Today is the official publication of the Canadian HemophiliaSociety (CHS) and appears three times yearly.
The Canadian Hemophilia Society strives to improve the health andquality of life for all people with inherited bleeding disorders and to find acure. Its vision is a world free from the pain and suffering of inheritedbleeding disorders.
The purpose of Hemophilia Today is to inform the hemophilia andbleeding disorders community about current news and relevant issues.Publications and speakers may freely use the information contained herein,provided a credit line including the volume number of the issue is given.Opinions expressed are those of the writers and do not necessarily reflectthe views of the CHS.
The CHS consults medical professionals before distributing anymedical information. However, the CHS does not practice medicine and inno circumstances recommends particular treatments for specificindividuals. In all cases, it is recommended that individuals consult aphysician before pursuing any course of treatment.
Brand names of treatment products are provided for informationonly. They are not an endorsement of a particular product or company bythe writers or editors.
www.hemophilia.ca
We would like to thank the followingcompanies, corporate foundations andemployee fund programs for theirgenerous support. Our way of recognizingthem for their generosity is through ourNational Corporate Giving Program.
3M - CanadaCanadian Blood ServicesDelta Hotel WinnipegDe Luca’s Specialty FoodsFondation de Bienfaisance T.A. Germain (La)Great-West Life Assurance CompanyHarold E. Ballard FoundationHéma-QuébecJean Coutu Group (PJC) Inc. (The)John Brouwer Foundation (The)
We would also like to thank our numerous additional donors – individuals, corporations
and foundations – who each year express their confidence in us by making substantial
supporting donations.
Working together with individuals and the corporate sector in Canada helps the CHS
accomplish its mission and vision by extending our reach and reinforcing our messages.
CSL BehringEdwards Charitable FoundationF.K. Morrow FoundationJ.P. Bickell Foundation
Dewdney Family Charitable Foundation
Lillian and Don Wright Foundation (The)Manitoba Liquor Control CommissionOctapharmaPower Corporation of CanadaPuma CanadaSchering CanadaScotiaBankStandard Limestone QuarriesToronto Star Fresh Air FundWinnipeg Free Press (The)
P L A T I N U M
G O L D
S I L V E R
B R O N Z E
H E M O P H I L I A T O D AY S P R I N G 2 0 0 82
CONTRIBUTING WRITERSDr. Ronald BarrBrent BuchananSarah BradshawKaren DunnAnn English, PhDNicole Graham, PTDr. Wenda L. GreerDr. Gonzalo HortelanoDr. Paula JamesDr. Robert KlaassenFrançois LarocheDr. David LillicrapLisa LittleMichel LongMaurice MaretteJoAnn K. Nilson, PTDr. Maha OthmanDavid PageJohn PlaterDr. Bruce RitchieDr. Elianna SaidenbergDr. William P. SheffieldMarion StolteDr. Irwin WalkerPam Wilton, RNEmil WijnkerDr. Rochelle Winikoff
EDITORFrançois Laroche
PRESIDENTPam Wilton, RN
EXECUTIVE DIRECTORDavid Page
EDITORIAL COMMITTEEHélène BourgaizeClare CecchiniFrançois LarocheMichel LongDavid PageChantal RaymondPatricia Stewart
PRODUCTIONCOORDINATORChantal Raymond
GRAPHIC DESIGNERPaul Rosenbaum
COPY EDITORDebbie Hum
TRANSLATORSRoy KeysLine LadouceurMarie Préfontaine
Canadian Hemophilia SocietyServing the Bleeding Disorders Community
Hem philiaTODAY

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 3e d i t o r i a l p a g e s
Wordfromtheeditor
François Laroche
IN THIS ISSUESPRING 2008 VOL 43 NO 2
Alarge part of this issue of Hemophilia Today is dedicated to research.Thanks to the research and advances over the past 50 years or so, the quality of life ofpeople affected by inherited bleeding disorders has improved immensely. A greater
variety of treatment options, more effective and safer treatments, as well as the introduction ofhome treatment, self-infusion and prophylaxis have all helped preserve joints and muscles,prolong the lives of those affected and contribute to better quality of life. Treatment, however,remains difficult and complicated for cases where inhibitors are involved, and muchinvestigation remains to be done in this area. Apart from those who develop inhibitors, peoplecoping with bleeding disorders today are active and productive individuals who have the sameopportunities—or nearly so—as the rest of the population.
Supported by funds from the Hemophilia ResearchMillion Dollar Club—whose endowment isnearing $2 million—the CHS Dream of a Cure Program now provides research grants andscholarships in basic or clinical sciences related to advancing hemophilia treatment and findinga cure. The Peer Review Committee, which approves the projects for funding, actually receivedclose to twice the number of applications in 2008 as in 2007, which is very encouraging.
In this issue, you can also learn more about the projects supported by two other CHSprograms: Care Until Cure, in association with Wyeth, and the Fellowship in Congenital&Acquired Bleeding Disorders, in conjunction with the Association of Hemophilia Clinic Directorsof Canada and Novo Nordisk. The issue also includes research by partners in the pharmaceuticalindustry, who assure us that several new, more effective products for various bleeding disorderswill be on the market soon.
All this is part of the CHS’s primary commitment and its vision—that is, to help bring abouta world without the pain and suffering caused by inherited bleeding disorders, and eventuallyfind a cure for these conditions. In the light of recent advances in research, we can definitelysay that we are on the right track.
LETTER TO THE EDITORSubject: Kogenate® FS and Helixate® FS - Two distinct productsDear François,
In the winter issue of Hemophilia Today, both in the Word From the Editor and in theIntroduction of Helixate® FS article on page 21, Kogenate® FS and Helixate® FS are referred to as“identical” products.
Bayer HealthCare Pharmaceuticals would like to clarify that Kogenate® FS supplied withBIOSET and Helixate® FS are in fact two distinct products on a number of fronts:
1) Bayer manufactures both of the recombinant factor eight (rFVIII) (lyophilized / freeze driedpowder) preparations, fills and seals the product vial. However, all subsequent steps forHelixate® FS, including those described in Point 2, are not conducted in a Bayer facility.
2) Important components of Kogenate® FS supplied with BIO-SET, including the product label,package insert, infusion set and diluent are not the same as those provided with Helixate® FS.
3) Only Kogenate® FS is supplied with the Bio-Set reconstitution system which is integrated withthe Kogenate rFVIII vial.
4) Our complete product offering extends beyond the actual product and package to includeprograms like the EZ-log patient diary system, Kogee/Kojo Club Newsletters, etc.
As the manufacturer and distributor of Kogenate® FS, Bayer firmly believes that Canadiansliving with hemophilia A should have a clear and accurate understanding of the differences whichmake Kogenate® FS and Helixate® FS distinct products.
Should your readers have any questions about Kogenate® FS, they may contact the Bayer Inc.Medical Information hotline at 1 800 265-7382.
Thank you,
Alan BirrellVP, Hematology / CardiologyBayer HealthCare PharmaceuticalsBayer Inc.
F RE ESubscription toHEMOPHILIA TODAY
Call us now or send us an e-mailto receive your copy of Hemophilia Today.
1 800 [email protected]
WWOORRDD FFRROOMM TTHHEE EEDDIITTOORR................................................33Letter to the Editor ..............................................................33
MMEESSSSAAGGEE FFRROOMM TTHHEE PPRREESSIIDDEENNTT AANNDD EEXXEECCUUTTIIVVEE DDIIRREECCTTOORR..............................................44Letter to the President ........................................................44
CCOOMMMMUUNNIITTYY NNEEWWSSBayer recognized as platinum donor ..............................552008 World Hemophilia Day..............................................552008 CHS Board of Directors ............................................77Chapter Spotlight..................................................................88Historical overview of MPTAP indexation......................99May 19: World Hepatitis Day ............................................99What was wrong with the Armour trial decision?....1100Teen Ambassador at Alberta Children’s Hospital ......1111Quebec’s no-fault bill for blood injury ........................1122Hemophilia, a disease that changed the world ........1122New CTAS triage guidelines ............................................1122Upcoming Events ................................................................1133What’s new on the CHS Web site?................................1133
YYOOUUTTHH FFIILLEE // VVOOLLUUNNTTEEEERR FFIILLEE....................................1144
FFUUNNDDRRAAIISSIINNGGDare to Dream for Hemophilia ......................................11552008 Ron Fellows/Mosport Hockey Challenge ..........1155
FFOOCCUUSS OONN RREESSEEAARRCCHHResearch means hope........................................................1166Hemophilia Research Million Dollar Club ..................1166Dream of a Cure, CHS Research Program....................1188Care Until Cure....................................................................2200Novo Nordisk Fellowship ..................................................2222
OOUURR SSTTOORRIIEESSFull Moon Wish ..................................................................2233
MMEEDDIICCAALL NNEEWWSSHepatitis C Press Review..................................................2244Opportunities to participate in research ....................2255AHCHC-Baxter Canada research partnership ............2266Physio Corner – the meaning of “spontaneous” ......2266
TTHHEE BBLLOOOODD FFAACCTTOORRNews from around the world..........................................2277Important Safety Information on PREZISTATM ..........2277
AA GGLLOOBBAALL PPEERRSSPPEECCTTIIVVEECHS continues to support valuable projects in 2008 ..2288Letter of commendation for our twinnings ................2288

Determination and perseverance pay off
The Canadian Hemophilia Society has long been known for its determination and perseverance. Perhaps this character trait originated in the chronic nature of bleedingdisorders and the never-ending challenge of individuals and families to cope with them.
Although results sometimes seem slow in coming, our determination and perseverance hasclearly paid off over the last four seasons.
After a decade-long effort to obtain financial compensation for those infected by hepatitis Cfrom blood and blood products, this past summer saw the first payments in the pre-86/post-90 hepatitis C class action settlement. This meant help for all people infectedthrough the blood system, regardless of the date of transfusion. The CHS can be proud thatafter the 86-90 class action settlement was announced in 1998, the organization contin-ued to work on behalf of those who had been left out.
The five remaining provinces – Saskatchewan, British Columbia, New Brunswick, Quebecand Alberta – indexed the Multi-Provincial/Territorial Assistance Program to the cost ofliving for those infected with HIV through blood and blood products. All this was the resultof determination and perseverance.
The criminal prosecution of certain individuals at the heart of the tainted blood tragedy ofthe 1980s came to an end this winter. While some may fault the judgment, the CHS haskept its promise to those affected that we would shine light on these terrible events to theutmost of our ability. And to remember the people who lost their lives, we launched theCommemoration of the Tainted Blood Tragedy with a memorial tree planting in Ottawa.
The CHS is more involved than ever in today’s questions of blood safety and supply. Tomark the 10th anniversary of the Final Report of the Commission of Inquiry on the BloodSystem in Canada, we produced the Fourth Edition of the CHS Report Card on Canada’sBlood System.
This past year, the CHS and the four professional associations representing bleeding disor-der healthcare providers endorsed the First Edition of the Canadian Comprehensive CareStandards for Hemophilia and Other Inherited Bleeding Disorders. This process began 29years ago with the groundbreaking 1978 Winnipeg Conference on Comprehensive Care.Implementation of these Standards will help ensure high-quality care for all Canadianswith bleeding disorders.
Over last summer and fall we launched the All About Carriers booklet and program, andtrained a committed group of women to do von Willebrand disease outreach with the pro-gram called Raising Awareness, Changing Lives. These are landmarks in a long struggle torecognize the care and treatment needs of carriers of hemophilia and women with otherinherited bleeding disorders. Again, determination and perseverance paid off.
And we saw renewed determination to push forward the research agenda to improvetreatment and find a cure. The CHS Research Summit brought together clinicians and re-searchers, who re-affirmed CHS’ key role in this area. Perhaps as a direct result, the CHSreceived double the number of research applications in 2007 compared to 2006 and is in-vesting a record amount of funds in research in 2008.
A major effort is being made to invest in our current volunteers and in our youth, and toattract new volunteers. They will be the next generation of leaders to carry on our tradi-tion of determination and perseverance.
H E M O P H I L I A T O D AY S P R I N G 2 0 0 84 e d i t o r i a l p a g e s
Message from the Presidentand the Executive Director
Pam Wilton, RNPresident
David Page Executive Director
LETTER TO THE PRESIDENT
April 14, 2008
Dear Ms. Wilton,
This April 2008, the Alberta MPTAPrecipients received word from the ProvincialHealth Minister, Ron Liepert, that the Provinceof Alberta is granting cost of living indexing ofthese payments. Further to that, they haveincluded retroactivity to 1994/1995. This wasgreat news as it has been seven years sinceOntario provided indexing, the first province todo so. Now, as of this April, all the provinceshave indexed their MPTAP packages for all oftheir citizens who were infected with HIVthrough the use of blood or blood products.The province of Nova Scotia created its ownseparate program.
As representatives of the HIV-transfusedcommunity of Canada, (individuals whoreceived HIV-infected blood or blood productsfor surgery, childbirth, trauma or other medicalreasons unrelated to bleeding disorders) wewould like to thank the Canadian HemophiliaSociety. We know that it took a lot of effortand perseverance to convince the provinces,one by one, to provide us with indexation.Indexation was an important issue becausemany of us have lived with HIV and itsdebilitating effects for more than 20 years andthe cost of living has risen considerably in thattime. We are grateful to the Presidents, theHIV/HCV Task Force, staff and individualmembers of the CHS at the national level whokept up this effort over so many years.
Also, we would like to thank all those inthe CHS provincial chapters who never gave upand kept on writing letters, meeting withMinisters, MLAs, candidates for parties, andgovernment officials on our behalf.
We would like to thank the provincialgovernments for providing us with theindexing of the MPTAP payments and theCanadian Blood Agency for their efficient andsympathetic administration.
Although we are very pleased to receiveindexation, we are also aware of the inequalityamong the provinces with regards toretroactivity and hope that the CanadianHemophilia Society will continue to pressthose provincial governments to make thesituation fair and equal across all the provincesof Canada and grant retroactivity to all datingback to 1994/1995.
In closing, we would like to express oursincere appreciation to the Canadian HemophiliaSociety for including the HIV-transfusedcommunity in all of its advocacy efforts and forits continued support over the years.
Sincerely,Members of the HIV-transfused communityof Canada
H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 5c o m m u n i t y n e w s
CommunityNews 2008 World Hemophilia Day
Manitoba Chapter
The Manitoba Chapter celebrated WorldHemophilia Day with an awareness table atthe Health Sciences Centre (HSC) in Win-nipeg. HSC is the home of the ManitobaBleeding DisordersProgram for bothadults and chil-dren. We were for-tunate to haveCBC Radio comeby and conduct aninterview with ourExecutive Director, Christine Keilback, andwith Manitoba Board Member, Ingrid Olson.The awareness table was an excellent wayto educate the general public about inher-ited bleeding disorders.
The Canadian Hemophilia Society providesspecial recognition to donors who con-tributed over $450,000 to the work of theorganization at the national and chapter lev-els in the previous year. For 2007, the CHS ispleased to recognize Bayer HealthCare as aPlatinum level donor. A donor at this levelcontributes between $450,000 and $650,000to the organization’s efforts.
“Bayer has long been a major donor tothe CHS,” said Pam Wilton, CHS President.“Their support is truly valued; without it, wewould not be able to provide the level ofprograms and services to the bleeding disor-der community that we do today.”
In 2007, Bayer contributed $400,000 inunrestricted funding at the national and
CHS recognizes Bayer as platinum level donor for 2007
Northern Alberta Region
� HHeemmoopphhiilliiaa DDaayy aatt 774422 SSiiggnnaallssSSqquuaaddrroonn,, EEddmmoonnttoonn,, AAllbbeerrttaa
bbyy BBrreenntt BBuucchhaannaannIt was April 17. I came in early, because it
was a special day for “the bleeder” or as myold Commanding Officer used to call me “themutant.” It was World Hemophilia Day and Iwas starting to set up my display I had justreceived the day before.
Before I get too far in my article, let megive you a quick background on how I gothere. I joined the Military in 1987 and wasmedically released in 2005, after totallyfalling apart due to some major bleeds andsurgeries to stop bleeds, etc. I found out Ihad hemophilia in October 2000, henceearning the new nickname “the mutant.” Iknow one thing is for sure, the military andbeing a bleeder don’t mix and my body re-minds me of it everyday.
So there I was, setting up my display,and I already had people asking me whatwas going on. I thought to myself… goodstart. After I finished the display I put asign up that read, “If you have any ques-tions about bleeding disorders ask Bucky”(my real nickname), and I was actually sur-prised by how many people talked to methroughout the day. continued on page 6
chapter levels. These funds were critical in theability of the CHS to fulfill its mission in the areasof care and treatment, education and support, asafe and secure blood supply, and advocacy.
In addition to the unrestricted funding, Bayersponsored the following programs and activitiesin whole or in part: the CHS Research Summitheld in February 2007 organized to solicit advicefrom the medical and scientific community onhow the CHS could maximize its impact in thearea of research; Rendez-vous Québec, a 4-dayCongress that included the biennial CHS – Asso-ciation of Hemophilia Clinic Directors of CanadaMedical/Scientific Symposium, New Team Work-shop, annual meetings and consumer work-shops; and the Step by Step Program for Parentsthat provides critical tools of support and edu-
cation to families of newly diagnosed chil-dren with hemophilia.
“Our partnership with the CHS is very im-portant to Bayer,” said Alan Birrell, Vice Pres-ident, Hematology/Cardiology. “Bayer hassupported the CHS for over 15 years, and isproud to be recognized as a Platinum sponsor.”
Editor’s note: The philanthropic relationshipbetween Bayer and the CHS is governed, forthe CHS, by its Policy on Relations withCompanies in the Pharmaceutical Industryand its National Corporate Giving Program;and, for Bayer, by the Collaborative PartnershipGuiding Principles developed by RX&D, thenational association representing Canada’sresearch-based pharmaceutical companies.
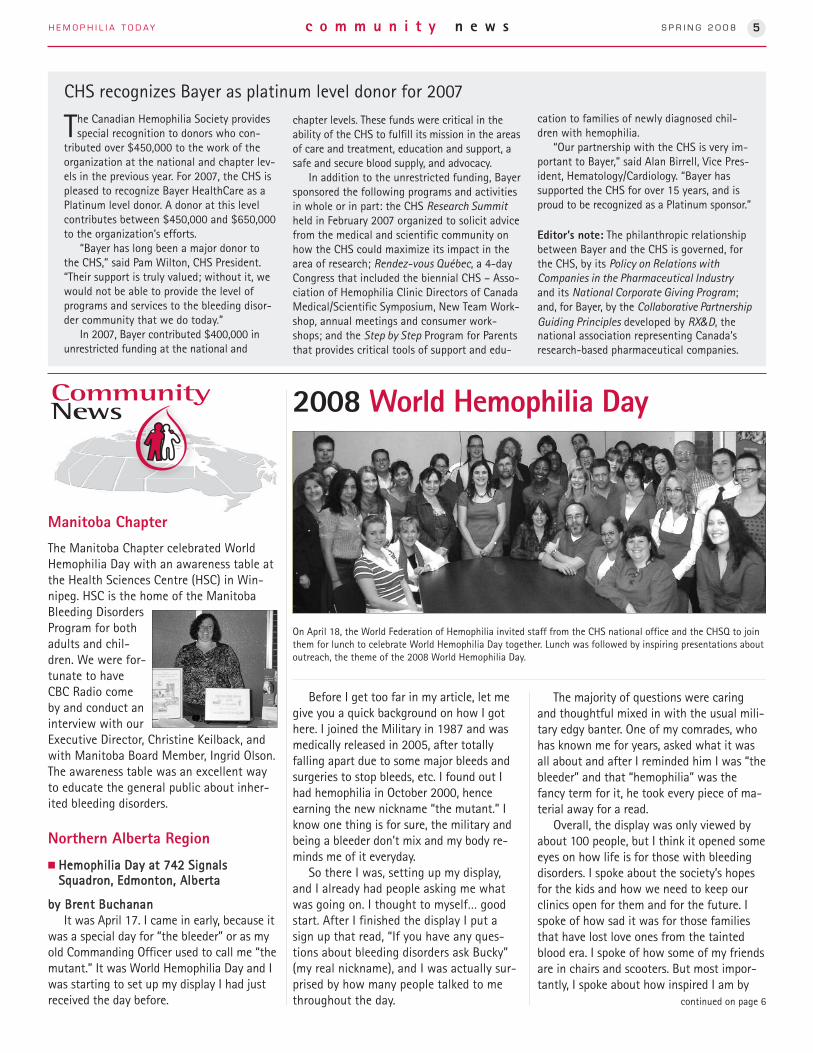
On April 18, the World Federation of Hemophilia invited staff from the CHS national office and the CHSQ to jointhem for lunch to celebrate World Hemophilia Day together. Lunch was followed by inspiring presentations aboutoutreach, the theme of the 2008 World Hemophilia Day.
The majority of questions were caringand thoughtful mixed in with the usual mili-tary edgy banter. One of my comrades, whohas known me for years, asked what it wasall about and after I reminded him I was “thebleeder” and that “hemophilia” was thefancy term for it, he took every piece of ma-terial away for a read.
Overall, the display was only viewed byabout 100 people, but I think it opened someeyes on how life is for those with bleedingdisorders. I spoke about the society’s hopesfor the kids and how we need to keep ourclinics open for them and for the future. Ispoke of how sad it was for those familiesthat have lost love ones from the taintedblood era. I spoke of how some of my friendsare in chairs and scooters. But most impor-tantly, I spoke about how inspired I am by

H E M O P H I L I A T O D AY S P R I N G 2 0 0 86 c o m m u n i t y n e w s
others in the society who possess so muchdedication and pure guts to get throughtheir daily lives and still make the time to dowhat they need to do to, ensuring that oursociety is here for a long, long time.
I came in early; it was a special day forhemophilia, and it didn’t hurt as much today.
� Donalda School participates in Red,White & You Day April 17, 2008
My name is Mary Mueller and my sonAlden Mueller has severe hemophilia A.When I was asked by the Alberta Chapter toparticipate in spreading awareness of hemo-philia in my community I jumped at thechance to give back to the society. We havenever participated in a Red, White & You Dayin our school before so the plans were underway. Alden’s friend, Morgan Baker, has anephew with severe hemophilia so we gother planning the day with us.
Alden and Morgan made posters and putthem up around the school, asking the stu-dents and staff towear red and white,and to please give aloonie or toonie tohelp find a cure forhemophilia. Theschool included theevent on the April calendar and I put a dis-play up in the hallway. I never dreamt thatthe day would have turned out so successful.At least 60 out of 75 people wore red, whiteor both and the students that forgot worered pinnies to support the day. One studenttold me it was just like Halloween. With hav-ing such a small school, I thought that if wetook in one dollar for every student we wouldbe successful, but we surpassed that by fourtimes!!!
Alden’s classmate Jessica Nelson is a littlegirl we all should model our lives upon. Shepresented Alden with an envelope that morn-ing and inside the envelope were two 50-dol-lar bills. A note was attached saying that shehoped this money will help find a cure for herbest friend. It was so awesome the donationshe gave. I talked with her mom later that dayand she told me that Jessica has been savingfor a laptop. She willingly gave her savings inhopes to help find a cure for her friend. Shewants to help make the world a better placeto live in when she grows up, her mom Lauratold me – but she should realize that she al-ready has been doing just that. May we allgive as freely as Jessica, so a cure for hemo-philia is closer to be being found.
Southern Alberta Region
National office provided an excellent kitthat included the Fact Sheet and brochures.We set up an information display in the Uni-versity of Calgary Medical School, near oneof the amphitheatres, and chatted withpassersby, including students, staff and thegeneral public.
As we only had a few seconds to get ourmessage out, we had a big bowl of Kit Katsto draw the students over. The informationabout von Willebrand disease generated alot of questions. We emphasized that theWeb site is a wonderful resource.
We hope that some of these students willwant to learn more about blood disorders orconsider a hematology specialty.
� BBrreeaakkffaasstt TTeelleevviissiioonn SShhooww
A couple of people in Edmonton also ap-peared on a local Breakfast Television Showon April 17 to raise public awareness onbleeding disorders. It wasn’t a long inter-view but enough for us to provide the ba-sics and the CHS contact information.
� RReedd,, WWhhiittee && YYoouu aatt MMootthheerr TTeerreessaaCCaatthhoolliicc SScchhooooll
Anika and Korri Spruyt organized a Red,White & You Day at school for April 17. Theygo to Mother Teresa Catholic School in SylvanLake which is grades 3 to 9. The girls made anannouncement about World Hemophilia Dayand asked that everyone wear red and white. A lot of kids did wear red and white. We didnot have a fundraiser with this day, but quite afew of the kids did ask about the blood disor-ders and most of the teachers also worered. Sheri, their older sister, also had a Red,White & You Day at the Royal Bank whereshe works in Strathcona (Edmonton). All ofthe employees wore red and she had aninfo session with the employees.
continued from page 5
An enthusiastic group at Donalda School.
Eager students at Mother Teresa Catholic School.
Jessica, Alden and Morgan

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 7c o m m u n i t y n e w s
Sitting, from left to right: Venanz D’Addario (Ontario),Craig Upshaw (Vice-President), Dr. Bruce Ritchie(MSAC Representative), David Pouliot (Vice-President).Standing, from left to right: Eric Stolte (Past-President),Jeff Beck (Ontario), James Kreppner, LLB (Secretary),Ann Wood (Saskatchewan), Martin Kulczyk (Quebec),Mylène D’Fana (Quebec), Aline Landry (New Brunswick),Bill Featherstone (Manitoba), Dianna Cunning (NovaScotia), Mike Beck (Vice-President), Clare Penner (Alberta), Maureen Brownlow, RSW (Vice-President),Pam Wilton, RN (President), Colleen Barrett (New-foundland and Labrador). Missing from the picture:Norman Locke (Treasurer), Elaine MacRae (Prince Edward Island), Gabriel Ramos (British Columbia),Bruce Rempel (British Columbia), Julia Sek (Ontario),Emil Wjinker (National Youth Committee Representative).
22000088 CCHHSS BBooaarrdd ooff DDiirreeccttoorrss
Lastly, a radio program on hemophiliafeaturing resource persons from the CHSQand the CHS and the medical communitywas broadcast on April 17 and will soon beavailable on the CHS Web site.
Nova Scotia ChapterQuebec Chapter
On World Hemophilia Day a number ofpublic outreach tables were set up to pro-mote the cause we work for. In conjunctionwith the CHS national office, and the WorldHemophilia Federation (WFH), we are proudto have held our very first information dayfor the general public on April 17.
The CHSQ also had an outreach table ata hospital, and another at the Quebec Na-tional Assembly, where badges marking theevent were handed out to all the MNAs.The Minister of Health and Social Services,Philippe Couillard, tabled an unannouncedmotion to recognize World Hemophilia Day.
Prince Edward Island Chapter
Dianna Cunning of the Nova Scotia Chapter set up atable in front of the Royal Bank branch where sheworks, with tons of info. Employees all wore redand/or white. And they asked each client to buy acolouring book for that day only.
Bayer marks Hemophilia DayBayer was a sea of red and white as
employees at the Toronto head officecelebrated Red, White & You Day on April 17(World Hemophilia Day), raising over $900for the Canadian Hemophilia Society.
The first ever “Run For It” event was heldin Charlottetown on April 19, to raiseawareness about inherited bleeding disor-ders and to fundraise for the PEI Chapter. It was a 13km run along the ConfederationTrail, on a cool but sunny spring day, andabout 75 people showed up to run or walkthe 13km, or 5, 3 and 1km which were alsomarked. It was uplifting to see people unre-lated to the cause show their support. De-spite a few minor glitches, it was declared asuccess by all, so next year should be biggerand better!
On World Hemophilia Day, Chapter VP,Elaine MacRae, held a Red, White & You Dayat the high school where she is a teacher.The package sent along by the CHS nationaloffice was used to raise awareness amongher colleagues.
CHSQ, CHS and WFH at Montreal Central Train Station.
World Hemophilia Day celebration at IWK Health Centre in Halifax.
CHSQ at the Quebec National Assembly.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 88 c o m m u n i t y n e w s
Prince Edward Island Chapter
A local group of sportsmen decided toshow support to the PEI Chapter as theirannual “charity of choice” and held awildlife dinner open to the public. Dona-tions were made at the door where we hada small display of CHS brochures and pam-phlets. This unique event raised over $1,000and was a truly fun and heartfelt afternoon!
QQuueebbeecc CChhaapptteerr4th edition of the Bowl-a-Thon
The Quebec Chapter has held another ofits traditional Bowl-a-Thons, which havebrought in over $10,000 gross in Victoria-ville, Montreal and Quebec City! A firstBowl-a-Thon was held in Victoriavillethanks to a volunteer who handled organi-zation for the event. It is important to notethat the work done byall our volunteersacross Quebec in set-ting up these eventshas been amazing, andwe can only encourageinitiatives of this kindeverywhere in Canada!
CHSQ pensWe now have a new promotional item:
a pen with CHSQ logo! Easy to sell and verypractical, the pen is already a big successwith our members, many of whom havepromised to promote it to their friends andacquaintances. This will help diversify oursources of funding and, at the same time,help raise awareness about hemophilia.
Hemophilia OntarioJeff Beck, President, is pleased to
announce that Heather Heagle hasaccepted the position of Executive Director,Hemophilia Ontario, as of May 20, 2008.
Heather has had significant experiencein senior management positions, providingleadership in developing a diverse array offund development programs, sponsorshipcampaigns and events. Those opportunitieshave served a range of concerns,municipally for Vaughan, Ontario,provincially for the Ontario Association ofLandscape Architects, and nationally for theOntario Association of Chiefs of Police -York Region Police Services and for theCanadian Association for CommunityLiving.
As a community member, Heather hasbeen an active volunteer and boardmember in organizations such as TDCanada Trust – Friends of the Environment,Wings of Hope – Eating Disorders of YorkRegion, Opera York, and the Ontario SpecialOlympics.
The Board and staff of Hemophilia Ontario invite you to join us inwelcoming Heather to the bleedingdisorders community.
South Western Ontario Region (SWOR)
On March 29, 2008, SWOR hosted amember conference, “Let’s Talk AboutMe.” This educational conference was de-signed to provide access to speakers andinformation sessions for carriers, youthwith hemophilia, adults with hemophiliaand individuals with von Willebrand dis-ease. The conference was a huge success.Overwhelmingly participants have re-quested that as a region, SWOR continue toprovide access to educational opportunities.As a result, we are in the process of devel-
Central West Ontario Region(CWOR)
On April 6, 2008, members came out toenjoy the artistic scenery at the Art Galleryof Hamilton for CWOR’s 2008 AGM. Guestspeakers included Nigel Small, ProvincialHIV/HCV Program Manager, and PediatricHematologist Dr. Anthony Chan of theHamilton-Niagara Regional HemophiliaClinic. The children who attended the eventalso enjoyed a private tour of the gallerywith an artsy craft session to end the day.An enjoyable time was had by all!
TToorroonnttoo aanndd CCeennttrraall OOnnttaarriiooRReeggiioonn ((TTCCOORR))This year TCOR held their annual AGM at
the Playdium in Mississauga. The day wascomplete with presentations and reports,many awards, and entertainment for thechildren. It concluded with a buffet andplay time at the Playdium.
ChapterSpotlight
Board member Luke Kilner and TCOR Board PresidentMike Beck presented the Karttik Shah Award to JamesKreppner and Antonia Swann for long standingcommitment and advocacy.
Newfoundland and Labrador oping a plan that will continue to bring ed-ucation to our members. Without your sup-port, this would not have happened. Thankyou very much for your continued supportof SWOR and our efforts to enhance sup-ports and programming within the region.
Norman Locke, from the NL Chapter, receiving a RedWhite & You donation from Chris Ryan, NL AccountManager for Genworth Financial Canada.
H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 9c o m m u n i t y n e w s
May 19: World Hepatitis Day
by Michel Long, CHS ProgramDevelopment Coordinator
In 2008, the CHS along with otherconcerned Canadian organizations,healthcare professionals and patients joinedthe World Hepatitis Alliance (WHA) to launchthe first ever global WORLD HEPATITIS DAY.
The WHA is a global coalition committedto changing the fate of more than 500million peopleliving with viralhepatitis B or Cworldwide. Theinternationalcampaign themeAm I Number 12?was designed tocommunicate thestatistic that one in 12 people worldwide hasviral hepatitis B or C. “12 asks for 2012” werepresented to governments around the world,6 internationally mandated and 6 nationallyfocused.
To reduce the health and socialimpact of hepatitis B and C on the liverhealth of Canadians, we ask federal,provincial and territorial governments ofCanada to adopt, by 2012, a coordinatednational strategy that:� Promotes prevention of hepatitis B andC through expanded education,immunization and harm reductionprograms all across Canada.
� Improves access to comprehensive careand treatment programs in all areas ofthe country.
� Increases knowledge and innovationthrough interdisciplinary research andsurveillance to reduce the burden ofhepatitis B and C on Canadians.
� Creates awareness about risk factors,stigma and the need for testing amongthe general population and at-riskgroups.
� Builds capacity through training andrecruitment of qualified healthprofessionals.
� Supports communities and community-based groups in developing, deliveringand evaluating peer-driven and focusedinitiatives.
For more information, please visitwww.aminumber12.org.
Historical overview of Multi Provincial/Territorial AssistanceProgram (MPTAP) indexation
by Michel Long, CHS Program Development Coordinator
In May 1990, the Government of Canada established its Extraordinary Assistance Plan(EAP) to provide financial assistance to an estimated 1,250 individuals (or their estates)who were infected by HIV through the transfusion of tainted blood or blood products in
Canada between 1978 and 1989. This assistance plan was funded solely by the federalgovernment and consisted of compensation of $120,000, tax free. Qualifying individualshad to apply before December 31, 1990, in order to receive an indemnity of $30,000 forfour years. Indemnities were paid out by Health and Welfare Canada in April in the years1990, 1991, 1992 and 1993.
On the 15th of September, 1993, provincial and territorial Health Ministers announcedthe creation of the Multi Provincial/Territorial Assistance Program (MPTAP) to provide fi-nancial support to people who have contracted HIV through tainted blood transfusions orcomponents received in Canada. Only Nova Scotia is not part of this program, having setup its own plan earlier that same year.
The MPTAP program took over from the EAP, with compensation administered by theprovincial and territorial health ministries instead of federally. Improvements to this planwere made on the 1st of December, 1993. Individuals approved for financial assistancethrough the EAP were eligible for additional assistance through MPTAP, which provides$30,000 per annum for life. In all jurisdictions, this amount has been linked to the cost ofliving and the actual annual payment is over $30,000.
The CHS and its members have fought long and hard across Canada to ensure the pay-ments are indexed to the cost of living. Below is a table which summarizes when the in-dexations were obtained in all provinces and results, except for Nova Scotia. All nineprovinces base the increased payments on the difference in the cost of living between1994 and the present.
Date indexation agreed upon Province /Territory Retroactivity
May 4, 2001 Ontario YES. As of 1994, year of the beginning of the program
July 2005 Manitoba No
October 2005 Newfoundland and Labrador No
March 2006 Prince Edward Island No
May 2007 Saskatchewan No
July 2007 British Columbia No
September 2007 New Brunswick No
November 2007 Quebec No*
March 2008 Alberta YES. From 1994/95 to 2007/2008
* Retroactivity was offered as of April 1, 2007. Quebec chapter members are still negotiating to obtainbetter retroactivity.
The CHS HCV/HIV Task Force is currently verifying if there are any victims in the Yukon,Northwest Territories and Nunavut regions to determine if indexation requests should be made.
Assistance Program for HIV Secondarily Infected Individuals In December 1998, the federal, provincial and territorial governments agreed on a joint
program to provide ex gratia payments of $240,000 per individual to Canadians who weresecondarily infected with HIV by a primary recipient (spouse/partner or mother to child).This program supplements the financial assistance provided to Canadians directly infectedwith HIV from the blood supply (“primary infections”) under the federal Extraordinary As-sistance Program (EAP) and the Multi Provincial/Territorial Assistance Program (MPTAP).Estates of secondarily infected individuals can also apply for benefits. The program is ad-ministered by the federal government (Health Canada) on behalf of the federal/provincial/territorial governments.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 810 c o m m u n i t y n e w s
by John Plater, Chair of the CHS HIV/HCVTask Force
As I stood in front of the SuperiorCourt of Ontario building andexpressed my outrage at the not
guilty verdict that had just beenpronounced by the Honourable MadameJustice Benotto, it was a struggle toarticulate why there was suchdisappointment. The day had been longanticipated and though the verdict was notcompletely unexpected, the tears andanguished faces of many who spilled out ofthe room weighed heavily on everyoneinvolved with the case. The media wantedanswers and, given the few minutes we hadto digest the 63-page decision, it wastough to articulate just what was so wrongwith the verdict.
There were obvious errors. MadameJustice Benotto referred to the freezing ofplasma as “lyophilizing [so that] factor VIIIcould be separated from other bloodcomponents.” Lyophilizing is actually afreeze drying step used towards the end ofthe process of producing FVIII concentratethat allows it to be stored at highertemperatures than cryoprecipitate. Thejudgment may not have hung on thismistake but it does speak to a lack ofdetailed understanding.
The same can be said for the descriptionof the situation that the defendants faced;Madame Justice Benotto suggested that“they were forced to choose betweendistributing a product that was not risk-free and leaving hemophiliacs without alife-saving treatment.” During the time inquestion, the vast majority of bloodproducts used by hemophiliacs were not forlife-saving circumstances. There is nomention in the judgment as to whether thefour identified victims received product forlife-saving reasons. I spent a lot of time infront of the media explaining that this casewas about a limited set of circumstancesrelated to one product distributed for ashort period of time in the mid-1980s. Is itpossible that this point was not made clearin court during the one and a half yearsthis trial was prosecuted?
Justice Benotto dismissed in three shortparagraphs what I suspect many people
viewed as the least serious of all thecharges in the case, but which was in myopinion the key to the whole case. Thepharmaceutical company Armour wascharged with failing to immediately notifythe Canadian Minister of Health of adeficiency or an alleged deficiency in itsproduct. The allegation referred to studiesdone by Dr. Alfred Prince, retained byArmour to conduct studies on its heattreatment process. Justice Benotto foundthese facts. Dr. Prince did those studies and“concluded that the efficacy of dry heat byArmour was somewhat limited.” He wantedto publish but Armour refused. Then JusticeBenotto concluded that there wereproblems with the studies, finding theywere unreliable, confusing andinconclusive. She decided that his findings“could not reasonably be construed toallege deficiencies in the viral inactivationprocess.”
History of course proved Dr. Prince rightbut, in fairness, the benefit of hindsightcannot be relied on to prove criminalliability. But is that the issue? The judgment
implies that it is up to a company to decidewhether research that appears to raisedoubt about the safety of its productshould or should not be reported to thegovernment. I submit that this is notacceptable. This conclusion also meant thatthe defendants had not failed to dischargea legal duty, a finding necessary to provecriminal negligence or public nuisancerelated to the bodily harm that was causedto the victims. The case fell apart.
Would anything have changed if theinformation had been reported? Would thegovernment officials (who were also foundultimately not guilty) have acted any fasterto save the lives at issue? We will neverknow. But again that is not the point.Failing to report is a crime. I would arguethat companies that make a profit fromtheir products should not be in a positionto decide what should be reported andwhat should not. It appears as thoughJustice Benotto, based on herunderstanding of the facts, felt thedefendants worried about a global shortageof hemophilia products more than theyworried about their company’s share of themarket of those products. I would prefer asystem that requires a company to providethe results of internal research toregulators for evaluation. Rules of privilegeand confidentiality can protect theirinterest in intellectual knowledge while ourpublic servants protect our safety.
Would it have been satisfactory for onlyArmour to have been convicted of thelimited charge of failing to notify theMinister? For many people I suspect not.Unfortunately, they viewed this case as anindictment of the whole system, which itwas not. Clearly, the outcome of theArmour case led to the dropping of chargesagainst Dr. Roger Perrault, in the trial thatwas to take place in Hamilton. That trialwould have looked at a broader range ofissues but still would not have been acomplete review of everything that wentwrong. The Krever Report (Commission ofInquiry on the Blood System in Canada)tells the story of the tragedy as a wholeand speaks to how the system failed us.
I do believe such a conviction wouldhave been a better outcome for Canadianhealthcare.
What really was wrong with the Armour criminal trial decision?
Justice Benotto dismissed
in three short paragraphs
what I suspect many
people viewed as the least
serious of all the charges
in the case, but which was
in my opinion the key to
the whole case.
The pharmaceutical
company Armour was
charged with failing to
immediately notify the
Canadian Minister of
Health of a deficiency or
an alleged deficiency in
its product.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 11c o m m u n i t y n e w s
Dr. Poon (...) eventually
diagnosed Justin with
severe hemophilia A.
After his first few factor
treatments, he developed
inhibitors. Unfortunately,
Justin did not respond to
the effective immune
tolerance treatment that
is generally administered
to hemophiliacs with
inhibitors.
Calgary’s Justin Shenher appointed as the new TeenAmbassador for the AlbertaChildren’s Hospital
by Lisa Little, Calgary, Alberta
During a luncheon organized by theAlberta Children’s Hospital (ACH) onFriday, February 29, Justin Shenher
was “sworn in” as the 2008 Children’sMiracle Network Champion Child by JustineClay, Communications and MarketingCoordinator of the ACH Foundation. In thiscapacity, Justin will serve as the ACHFoundation’s official teen ambassador tothe Children’s Miracle Network ChampionsAcross Canada Program, which is sponsoredby Wal-Mart Canada. The 14 ChampionChildren selected from across the nationgathered in Ottawa with their families tomeet each other and exchange stories. Theywill then fly to Disneyland to meet their“Champion Child” counterparts from theUS, the UK and Ireland.
Many of Justin’s friends and familymembers attended the luncheon along withmedia representatives, Morna Brown andAndrea Pritchard (two hemophilia nurses)and other medical and hospital staff. Therewere several guest speakers, including Dr.Man-Chiu Poon, Hemophilia Clinic Director(Calgary), Brad Baker, District Manager,Wal-Mart Canada, and Paul Lethbridge, Director, Corporate Development, Children’sMiracle Network.
On this occasion, Dr. Poon presented amoving speech and video about Justin,whom he has known since he was threedays old. When Justin was born, he had aroutine blood test on his heel that bled for10 consecutive hours. At that time, Dr. Poon was called in and eventuallydiagnosed Justin with severe hemophilia A.After his first few factor treatments, hedeveloped inhibitors. Unfortunately, Justindid not respond to the effective immunetolerance treatment that is generallyadministered to hemophiliacs withinhibitors. A variety of very expensiveproducts with inconsistent efficacy wereused on Justin. One of these products hadto be injected every two hours. For nearlyfive years, Justin was in so much pain anddiscomfort from ankle bleeds that he was inand out of a wheelchair.
About four years ago, there was anunexpected turn of events when Dr. Poonand several other Canadian specialists got together and decided to try anexperimental drug called Rituximab®, whichis used to treat lymphoid cancer. Therewere several reports indicating that this
chemotherapy drug could be used to treatsome immune problems associated withunwanted antibodies. This team ofphysicians developed a protocol and tried iton Justin to see if it would crash hisimmune system and destroy his inhibitor.Justin was one of the first Canadianpatients to receive this experimentaltreatment that must be repeated every sixto eight months. Rituximab has not curedJustin of the inhibitors, but their level hasbecome low enough that factor VIII can beadministered to prevent bleeding. He hasgone from having multiple bleeds everyother week to only twice a year. Andalthough he experiences some fear aboutthe treatment losing its effectiveness, it hasnot stopped him from living a very activeand fulfilling life. In essence, this miracledrug has given him his life back.
Without this treatment, Justin wouldnot have been well enough to serve thisyear as the teen ambassador for theAlberta Children’s Hospital. During Justin’sspeech, he thanked the staff in thehemophilia treatment centre and all othermedical personnel that have helped himalong the way. His desire to become thespokesperson for the seventy-six thousandchildren who visit the Alberta Children’sHospital every year was motivated in partby wanting to shine a light on theextraordinary care that the hospital staffhas provided to him and all of the otherchildren that pass through the hospital’sdoors. It is also a way of giving back to acommunity that has been by his side eversince he was three days old.
As Justin spoke during his acceptancespeech, it became abundantly clear toeveryone in the audience that he is a witty,smart and articulate young man who haswisdom beyond his years. His wisdom stemsin part from his suffering and the medicalstruggles he has experienced in his shortlife. Whatever the source of his character,his positive attitude and caring dispositionmake him a perfect role model andspokesperson for the hemophiliacommunity and the larger hospitalcommunity. There was not a dry eye in thehouse when Justin completed his speech. Itis an honour to know this young man andto be part of the hemophilia communitythat we all share.
For more information about theChildren’s Miracle Network, please visittheir Web site atwww.childrensmiraclenetwork.ca.
Dr. Poon presented a moving speech and video about Justin.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 812 c o m m u n i t y n e w s
� Quebec re-introduces no-faultcompensation bill for bloodinjury
QUEBEC CITY, March 17, 2008 - Thegovernment of Quebec has re-introducedno-fault compensation legislation asrecommended by the Commission of Inquiryon the Blood System in Canada (the KreverCommission) in 1997. An earlier bill died onthe order table when an election wascalled.
Bill 67 would provide for compensationfor injuries caused by a blood productdistributed by Héma-Québec, regardless offault. It would not, however, indemnifyagainst negligence on the part of ahealthcare professional.
In the absence of any claims againstHéma-Québec, such a program would savethe blood operator several million dollars ayear in insurance costs. Quebec would bethe first province in Canada to introducesuch legislation.
� Hemophilia, one of the 12 diseases that changed the world
In his book Twelve Diseases ThatChanged Our World, Irwin Sherman, aprofessor emeritus of biology at theUniversity of California Riverside,describes how bacteria, parasites andviruses have swept through cities anddevastated populations, felled greatleaders and thinkers, and in their waketransformed politics, public health andeconomies.He also describes how hemophilia
had serious effects on the crownedheads of Europe. According to Sherman,the rise of Spanish dictator FranciscoFranco in the 1930s can be traced tothe lack of an heir to the thronebecause of hemophilia. Anotherexample is the collapse of the Romanovdynasty in Russia, in part caused by thefamily’s distraction of having to carefor young Alexei, heir to the throne,who had severe hemophilia. This set thestage for the rise of the Bolsheviks andthe Russian Revolution in 1917.Irwin W. Sherman, Twelve Diseases
That Changed Our World, AmericanSociety for Microbiology, ISBN-10:1555814662
RRoobbeerrtt KKllaaaasssseenn,, MMDD,, FFRRCCPP((CC))Director, Hemophilia ProgramChildren’s Hospital of Eastern Ontario, OttawaCo-Chair CHS ER Advisory Group
An important update regarding emer-gency care for patients with bleed-ing disorders was published in the
March edition of the Canadian Journal ofEmergency Medicine. Dr. Michael Bullard,who had worked with the CHS EmergencyAdvisory Group, was the principal author ofthe article on the revisions to the CanadianEmergency Department Triage and AcuityScale (CTAS) adult guidelines.
The revised guidelines include a new“first-order modifier” for the triage ofadults with inherited or acquired bleedingdisorders who present to the emergencydepartment. Life- or limb-threateningbleeds are assigned a CTAS level 2 (2/5 - 2nd
highest acuity), which indicates emergentcare is needed. Mild or moderate bleeds areassigned a CTAS level 3, which indicates ur-gent care is recommended. Other first-order modifiers may apply that may affecttriage level such as those relating to hemo-dynamic stability or level of consciousness.CTAS levels range from level 1 (resuscita-tion) to level 5 (non urgent). What thismeans is that only patients who need ac-tive resuscitation will be prioritized aheadof level 2 patients, such as bleeding disor-der patients with life- or limb-threateningbleeds. This is the same level of acuity as-signed to pregnant women in active labour,individuals presenting with significantchest pain, hemodynamically unstabletrauma patients or head-injury patientswith a Glasgow Coma Scale (GCS) score of10-13.
Patients with bleeding disorders whohave a major or moderate bleed requirerapid factor replacement, and it has longbeen known that the key to avoiding long-term damage to joints is prompt treatment.Ideally, treatment should begin within anhour of the injury. These revised guidelineswill improve emergency department triageand treatment of bleeding disorder patients.
The revisions focusing on bleeding disor-
ders came about through discussions be-tween the CHS ER Advisory Group and Dr.Bullard, who is Co-Chair of the CTAS Na-tional Working Group. The Advisory Groupwas in the process of revising the FactorFirst card for patients with bleeding disor-ders, which outlines the individual’s diag-nosis and therapy and can be presented totriage nurses to facilitate appropriate
emergency care. Dr. Bruce Ritchie, the pre-vious chair of the advisory group, in-vited Dr. Bullard to participate in the dis-cussion, which in turn led to the inclusionof bleeding disorder patients in the newCTAS guidelines.
The new Factor First cards are ready andpatients can expect to receive new cardswhen they come for their next clinic visit. It isalso important that patients and their familiesadvocate for adequate system capacity tohelp eliminate inpatient and emergency de-partment overcrowding which is limiting theability to deliver acceptable quality of care.
Now that we have the new Factor Firstcards and a new CTAS first-order modifier,patients should be prepared to show theircards when they go to the emergency de-partment and help to introduce thechanges to the ED staff. It may take up to ayear to disseminate and educate the entireemergency community about these CTASrevisions across Canada and even longer forthe broad introduction of CTAS electronicdecision support tools. It is hoped and an-ticipated that the updated and standard-ized CTAS guidelines will result in bettercare for bleeding disorder patients.
�Optimizing care for patients presenting with bleedingdisorders to the emergency department: the impact of thenew CTAS triage guidelines
These revised guidelines
will improve emergency
department triage and
treatment of bleeding
disorder patients.
Bernard-Soulier Syndrome – An Inherited Bleeding Disorder
The latest in the series on Rare FactorDeficiencies, this document is a generalinformation booklet about Bernard-SoulierSyndrome for patients, families andhealthcare providers. This booklet wasdeveloped by the Quebec hemophilia clinicnurses of the Canadian Association ofNurses in Hemophilia Care (CANHC) andpublished by the CHS. You can download it at www.hemophilia.ca/en/printed_documents.
H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 13c o m m u n i t y n e w s
Upcoming EventsCanadian Hemophilia Society
▪ August 20, 2008 – The 2008 Ron Fellows/Mosport Hockey Challenge in support of the Canadian Hemophilia Society will be held at Campus Ice Centre in Oshawa, Ontario. For more details, please contact the CHS national office at 1 800 668-2686.
▪ September 5-7, 2008 - National Youth Leadership Workshop at the YMCA Geneva Park,Orillia, Ontario.
▪ November 2008 (Date to be confirmed) – The 1st CHS National Workshop for Patients withRare Factor Deficiencies will take place in Montreal.
Manitoba Chapter▪ June 30, 2008 - Deadline for Scholarship/Bursary Applications.▪ July 13-22, 2008 - Family Camp at Luther Village, Ontario.▪ September 5-7, 2008 - Men’s Retreat at Lake Manitoba Narrows Lodge.▪ October 9, 2008 - Member Meeting (Location to be confirmed).
Alberta Chapter▪ September 19-21, 2008 - The CHS Alberta Chapter Annual Family Retreat will be held at theGoldeye Centre near Nordegg.
▪ October 2008 (Date to be confirmed) - Both Regions are in the early planning stages of anevent to celebrate the 30th anniversary of the establishment of our clinics in Alberta.
Toronto and Central Ontario Region (TCOR)▪ June/July 2008 - Families In Touch Summer Picnic – A day where families and friends can connect, learn and picnic in a relaxed outdoor setting. Watch for more details.
▪ June 29-July 12, 2008 - YMCA Camp Wanakita Summer Camp – A place for children with inherited bleeding disorders to enjoy regular camp activities while learning to manage theircondition with the help of clinic staff.
▪ August 23, 2008 - John Plater Lamb Roast – A great opportunity for members within theTCOR community to meet and join together for an afternoon of fun and fantastic food! Thisspecial event is generously provided and planned by Mr. and Mrs. John Plater. For moreinformation please call 416 972-0641.
▪ September 19-21, 2008 - Just the Guys weekend – A weekend for fathers and their sons tohave an opportunity to learn and play together. This weekend is held in conjunction with twoother regions (SWOR and CWOR). If you are interested in participating in this weekend pleasecall 416 972-0641.
▪ October 2008 (Date to be confirmed) - Transition Program Evening – The transition programevening is designed to help transitioning families familiarize themselves with the entiretransition process from the Hospital for Sick Children to the St. Michael’s Hospital adult clinic.The program is open to families or individuals 17 years of age who will be transitioning thefollowing year.
▪ October 2008 (Date to be confirmed) - Women In Touch Group – A day for women to learn,gather, share and express their thoughts, life lessons and ideas. Please call 416 972-0641 if youwish to attend.
Ottawa & Eastern Ontario Region (OEOR)▪ August 9, 2008 - The 14th Annual Shawn Duford Golf Tournament for Hemophilia will be heldat the Meadows Golf Course in Ottawa. Early Bird Registration Fee is $95 per person, whichincludes, golf, cart, box lunch, buffet roast beef dinner, prizes and FUN. Book early if you don’twant to miss this event. For registration please contact Colin Patterson at [email protected] or call 613 739-3845.
Central West Ontario Region (CWOR)▪ July 20, 2008 - This year, CWOR will be holding their annual Summer BBQ & Education Day atAfrican Lion Safari. The day will be packed with family fun and a picnic-style barbeque lunch.Members are encouraged to bring their families to this event for a walk on the wild side!
Quebec Chapter (CHSQ)▪ August 10-15, 2008 – Children’s summer camp in Saint-Raymond-de-Portneuf, Quebec.▪ Summer 2008 (Date to be confirmed) – A one-day activity for young adults.▪ Mid-October 2008 – Family weekend for families dealing with inhibitors.
Prince Edward Island Chapter▪ A fall meeting is planned for the PEI Chapter in Charlottetown, with an invited guest speaker.Location and date to be confirmed.
CHS 2007 Annual ReportThe CHS 2007 Annual Report and the com-plete Financial Statements are available atwww.hemophilia.ca/en/1.5.php.
What’s new on the CHS Web site?
www.hemophilia.ca
determinationperseverance
TheCanadianHemophiliaSociety
2007annualreport
You can also order copies by contacting the CHS office at 1 800 668-2686 [email protected].

H E M O P H I L I A T O D AY S P R I N G 2 0 0 814 y o u t h f i l e / v o l u n t e e r f i l e
by Marion StolteChair of the CHS Volunteer Development Committee
Welcome to the first article onvolunteerism. Our story began inthe spring of 2006 when ten
wonderful volunteers desiring to help“grow” the ability of the CHS to successfullyrecruit, train and recognize volunteers gottogether and formed the VolunteerDevelopment Committee. Hélène Bourgaize,the CHS Director of Volunteer Developmentand Human Resources has proven to be aninvaluable asset and leader in helping thecommittee develop a variety of tools for useby chapters and regions.
Not only do the volunteers on thiscommittee have the heart, so do all thevolunteers across our country, in each of ourchapters, on each committee. What aprivilege to volunteer together – to see themission and vision of the CanadianHemophilia Society fulfilled – to see liveschanged and quality of life improved for allwith bleeding disorders.
Over the past two years we havesuccessfully developed a number of tools forour chapters and regions. They range fromtemplates of job descriptions, skills andinterest surveys, planning calendars, how andwhere to recruit volunteers, crafting yourrecruitment message, evaluation forms, termsof reference templates, recognition ideas. Inaddition, a new volunteer brochure has beendesigned and can be used by Chapters. The
items listed abovehave all beencompiled togetherinto an “easy to use’binder that eachchapter/region hasbeen given.
Members of thecommittee havegiven presentations
at CHS AGMs, at chapter AGMs, as well as atthe World Federation of Hemophilia’s NMO(National Member Organization) trainingsession in 2006. Hélène was also invited topresent on volunteering at one of Ireland’sHemophilia meetings. Earlier this month, wepresented a poster at the World Congress inIstanbul.
Moving forward we are creating a CHSvolunteer Web page which will be usable byboth chapters and national levels. Volunteer
YouthFile
Sarah Bradshaw
Emil Wijnker
National Youth Committee Co-Chairs
It’s official! The National Youth Committee (NYC) will be holdingits first Youth Leadership Retreat at Geneva Park in Ontario fromSeptember 5 to 7, 2008. This event is limited to 40 participantsaged 15 to 25 from all corners of Canada, so be sure to applythrough your local chapter ASAP!
The retreat will provide an opportunity to develop leadershipskills, better understand what it means to be involved in the CHS,participate in great team-building activities and meet peers fromacross the country. Not to mention the presence of an amazingguest speaker.
In other news, the NYC is busy planning events for 2009. Theupcoming year will prove to be a big step towards new youth pro-gramming and promises to be very exciting. If you have any ideas,be sure to share them with your local representatives before thecommittee meets in mid-November.
Keep checking the Web site for upcoming national youthevents and stay in touch with your local chapter for all of their future events.See you in September!
The Canadian Hemophilia Society
September 5 to 7,2008.
A WEEKEND RETREAT FOR YOUNG PEOPLE
opportunities can be posted on the Web andpeople can regularly go there to see what isavailable and where they might like tovolunteer. We are in the process ofresearching some type of volunteer database,which could be used by both chapter andnational levels. This would facilitate trackingvolunteers and their hours, both of which arenecessary to obtain certain types of funding.
We have a tremendous committee – andit’s a privilege to work with each member.Often committee work is seen as drudgeryand not a lot of fun. However, one of ourcommittee members said, “This is myfavourite committee!” It’s great workingtogether to see volunteers across our countryempowered to continue succeeding. Theabundant achievements we’ve made over theyears were made possible due to theremarkable volunteers that have workedtoward a common vision. We will continue towork diligently to strengthen ourorganization – so that quality of life for allwith bleeding disorders will be improved.
Indeed, the volunteers on this committee,and those of you who participate in someway in the organization, “have the heart”.
To find out more about the committee’swork or to obtain a copy of the toolsmentioned above, please contact HélèneBourgaize at [email protected].
“Volunteers donot necessarilyhave the time;they just havethe heart.” – Elizabeth Andrew
VolunteerFile
Are you between 15-25 years old and would like to make a difference in your community while building your professional and social skills and having fun?
Mark your calendar for
September 5 to 7, 2008
The Canadian Hemophilia Societywill be holding a weekend leadership retreat for young people
from around the country with the purpose of learning,personal growth and building relationships.
This workshop will take place at the YMCA Geneva Park in Orillia, Ontario, with themain focus being on leadership training and activities to help you build self-esteem,develop concrete thinking abilities, and make decisions that reflect true leadership qualities. Participation and travel for selected candidates will be covered by the CHS, but please apply early, as spaces are limited!
For more information or to obtain an application form please contact
Hélène Bourgaize at either 1 800 668-2686 or by e-mail at [email protected]
H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 15f u n d r a i s i n g
FUNdraising
FINAL DRAW: August 28, 2008
BIG EVENT: September 19, 2008
Keep raising pledges at www.idaretodream.ca and for every $100raised your name will be entered into the next draw to win your veryown seat in the new Van Diemen Formula SCCA Race car at theBridgestone Racing Academy.
PLUS!... EXCITING NEWSAll participants who were encouraged to register by another participantplease rush to your event profile and answer the question – Who asked youto register for the Dare to Dream for Hemophilia event? The person whoasked you to join will receive an extra ballot for the next draw if yousuccessfully raised at least $100.
Be part of an amazing day when YOU
Dare to Dream for Hemophiliaand when YOU become a race car driver!
The CHS is proud to be
selected as the benefiting
charity for the 2008 Ron
Fellows/Mosport Hockey
Challenge. Hosted by Ron
Fellows, world-renowned road racer for the factory
Corvette team, this exciting hockey challenge will feature
current and retired professional hockey players (NHL & AHL),
along with race car drivers and crew from the American
Le Mans Series.
FEEL the speed…
HEAR the engine…
DRIVE the hairpin turn, and…
DARE to Dream for Hemophilia
Don’t wait! Invite your friendsnow to register and raise
pledges! YOU could be behindthe wheel of a Race car faster
than YOU think!
Winners so far…Derek Gates, Matthew D’Addario, Sarah Bradshaw, John Mullan…YOU?
2008 Ron Fellows/Mosport Hockey Challenge in support of the Canadian Hemophilia Society
WHEN: Wednesday, August 20, 2008
WHERE: OUIT Campus Ice Centre in Oshawa, Ontario
TICKETS: $25 General Admission $125 VIP Ticket $500 “Play with the Greats” Experience
For more information and to find out how you canparticipate please contact 1 800 668-2686.
Our thanks to Ron Fellows and Mosport for theirsupport of the CHS!
Christine Ford of PriceWaterhouseCoopers andDr. Georges-Étienne Rivard participating in theMarch 27 draw.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 816 f o c u s o n r e s e a r c h
by David Page, CHS Executive Director
The mission of the Canadian Hemophilia Society is to strive to improve thehealth and quality of life for all people with inherited bleeding disorders,and to find a cure. Therefore, research is at the heart of our activities.Over the past 17 years, thanks to the Hemophilia Research Million DollarClub endowment, generous individual donors, committed corporate
sponsors, and CHS chapters and regions across the country, the Society hasinvested more than four and a half million dollars in both clinical and basic peer-reviewed research in Canada. The cure may not yet have been achieved but it iscloser every year.
In 2007 and 2008, the CHS is operating three research programs: � the CHS Dream of a Cure Research Program with funding from the HemophiliaResearch Million Dollar Club, generous public donations and Bayer HealthCare;
� the Care until Cure Research Program in collaboration with Wyeth� and the Novo Nordisk Canada Inc. – CHS – Association of Hemophilia Clinic Directors of Canada Fellowship in Congenital and Acquired Bleeding Disorders.
Descriptions of the programs and the research projects funded in 2007 and 2008follow on pages 18 to 22.
The goal of this special feature on research is to inform the community of thetremendous work being accomplished and to acknowledge the commitment of theresearchers who have worked to improve the quality of life of people withbleeding disorders over the last year. For those affected by bleeding disorders,research means hope.
We would also like to highlight the behind-the-scenes work of the scientists whohave volunteered their time on the Peer Review Committees to evaluate the grantapplications. Without them, the CHS would not be able to operate its researchprograms. They are:
Dr. Patricia McCusker, Chair, CancerCare ManitobaDr. Anthony Chan, McMaster University Medical CentreDr. Michael Delorme, Kelowna, BCDr. Christine Demers, Hôpital de l’Enfant-Jésus, Quebec CityDr. Lawrence Jardine, Children’s Hospital of Western OntarioDr. Michael Nesheim, Queen’s UniversityDr. Fred Ofosu, McMaster UniversityDr. Bruce Ritchie, University of AlbertaDr. Mary-Frances Scully, Memorial University of NewfoundlandDr. Jean St-Louis, CHUM – Hôpital Maisonneuve-Rosemont, Montreal
We thank you for your dedication.
HemophiliaResearchMillion Dollar Clubby Maurice Marette, Chair
The Hemophilia Research GrantsReview Committee, under thechairmanship of Dr. Patricia McCusker,
met earlier this year and announced the2008 CHS Dream of a Cure ResearchProgram grant recipients. Summaries oftheir projects can be seen on pages 18 to20. These grants total $222,000 and weremade possible by funding provided by theHemophilia Research Million Dollar Club,Bayer and the Canadian Hemophilia Society.The Million Dollar Club and the CHS havecontributed close to $3,000,000 in supportof hemophilia research in Canada since 1991.
The Hemophilia Research Million DollarClub endowment fund has now surpassed$1,800,000 and our dream is that by theend of 2010 the endowment will reach the$2 million mark. In partnership with theCHS, we hope we can generate even moremoney each year towards ongoing research.
The Million Dollar Club is the mosteffective way in which you can supportbleeding disorders research in Canada. Thisis “our” fund – it is a tangible and visibleevidence of our commitment to research.Every single dollar, whether you purchase amembership or make a donation, goes toresearch (there are no administration orfundraising costs) and is tax deductible.
To benefit new families and members ofour community who don’t know about theMillion Dollar Club we have included in thisissue of Hemophilia Today, a brochuredescribing the Club and how you can makea difference by investing in hemophilia andother bleeding disorder research.
We would like to acknowledge theCanadian Hemophilia Society and all itschapters and regions, and the individuals,families and groups who are members ofthe Million Dollar Club or have supportedus through donations. Our supporters arealso recognized in the Administrators’Annual Report to the members, and at theAnnual General Meeting of the CanadianHemophilia Society. Once again, we thankall of you who are dedicated to supportingbleeding disorder research.
ResearchFor those affected by bleeding disorders, research means hope
1960 2008

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 17f o c u s o n r e s e a r c h
VOTING MEMBERSHIPS
Ken, Darlene and Tony PoyserTerry DouglasLynne Kubin & FamilyC. Kang TanMr. and Mrs. Joe LaxdalAudrey Irene Saigeon Poyser, Schultz & GlassHemophilia Ontario Manitoba ChapterThe IsaacsNorthern Alberta Region Toronto & Central Ontario Region Ray & Helen PoyserNova Scotia Chapter Central West Ontario Region British Columbia Chapter Dr. and Mrs. Ron GeorgeDesharnais-Pépin FamilyHemophilia SaskatchewanMarcel & Aline LaFranceEstate of Mary Ann OlsonShaun Aaron BernsteinMrs. R.W. RuddMrs. Pat LaxdalAlex, Ken Little & Lisa Sorrenti-LittleDr. Martin InwoodEnid & Douglas PagePoyser, O’Shaughnessy & CHSSusan Anderson (In Memory of Dorothy Kidd)Ken HannaGlass FamilyClam Chops c/o Lois LindnerDWK EnterprisesBlanche Summers (In Memory of Stuart Johnson)Quebec Chapter Southern Alberta RegionNorth Western Ontario RegionEstate of Janet RuddNew Brunswick ChapterG.W. Cooper FamilyNorth Eastern Ontario RegionAurore Mercure Fournier Northern Alberta Region (In Memory of Frank Schnabel)Art & Leona OlsonO’Shaughnessy – MolinaIan & Gail Austin (Jeff & Tim Austin)Canadian Hemophilia Society Ottawa & Eastern Ontario Region South Western Ontario Region Clam Chops II (Dr. Gerry Growe, Lois Lindner, Diane Rudd, George Stephenson,Cheong K. Tan)Frank Bott & Family (In Memory of Gregory Bott) Jamie Hill L. Faye StephensonOttawa & Eastern Ontario Region (In Memory of Shawn Duford)
NON-VOTING MEMBERSHIPS
Dr. S.K. AliMontreuil FamilyMr. Normand CampeauRalph Murray Jacques D. FournierDavid PageJohn FultonRobert C. PedersenClaire B. GagnonQuebec Chapter Mrs. B. RoseDonat & M-Paule GendronClaire & Éric RoussinGlenys & Ed GurneySavoie FamilyRev. Stephen H. HillElon O. ScottJo-Ann KubinBlanche SummersGhislaine LandrevilleBernice & Henry Triller
Ottawa & Eastern Ontario Region South Western Ontario RegionToronto & Central Ontario RegionToronto & Central Ontario Region (On Behalf of the Estate of Ann Lois Brown) Tom & Marvin OlsonFrancine O’MearaBert and Joan Rebeiro Candace Terpstra
HONOREES
Dr. Agathe BarryGisèle Bélanger and her TeamLorraine Bernier and her TeamHelen and Hunter BishopIn Memory of Martin BottIn Memory of Ann Lois BrownDr. Robert Card, Caryl Bell and Elena KaniganComprehensive Care Team of Southern AlbertaKathy ConliffeIn Memory of Clifford Roy CrookRay and Pat DanielIn Memory of Ken DanielDr. Barry L. DeVeberBill FeatherstoneIn Memory of Raymond Joseph FontaineFor Persons with Hemophilia who have Died from AIDS “So We Never Forget”Pierre Fournier In Memory of Robert GibsonMuriel Girard and her TeamDr. Gerry GroweIn Memory of Frank HaslamAnn HarringtonIn Memory of Glen Michael HoferDr. Martin InwoodDr. François JobinIn Memory of Stuart JohnsonFamily of David Joy Marie JutrasDr. Garner King and Dr. John AkubutuDr. Nathan KobrinskyIn Memory of Bradley KoloskiIn Memory of Charles Joseph (C.J.) KubinIn Memory of Barry Waines KubinIn Memory of Edward KubinNormand Landry FamilyIn Memory of Pierre LatreilleIn Memory of Bill LaxdalDr. Mariette Lepine and her TeamIn Memory of James “Jimmy” Alan LoveIn Memory of Gary MacLeanIn Memory of Dr. Douglas, Mark, Paul and Norine MaynardIn Memory of Art OlsonIn Memory of Ray O’MearaBob O’NeillOttawa & Eastern Ontario RegionDr. Mohan PaiJohn PeachPersons with Hemophilia from South Western Ontario RegionPauline Peters and Duncan ConradGary N. PetrickIn Memory of John PooleKen PoyserRay Poyser In Memory of Allan E. QuartermainIn Memory of Brian RebeiroIn Memory of Darryl RebeiroDr. Georges-Étienne RivardJoyce Rosenthal and Lois BedardIn Memory of Howard SayantDr. Brent SchacterIn Memory of Kenneth ShewchukIn Memory of Frank SchnabelMarthe SchnabelIn Memory of Glen SprengerIn Memory of John StrawaDr. Hanna StrawczynskiFrank and Candy TerpstraIn Memory of Frank TerpstraIn Memory of Troy Christian TrépanierDr. Chris TsoukasIn Memory of Neil Kerr Van DusenDr. Irwin WalkerBarbara WebsterGlen Webster
DONORS
THE FOLLOWING REPRESENT GENERAL DONATIONS, AND THOSE MADE IN HONOR OF MARY MACLEOD, AND MARJORIE CALDERWOOD, AND IN MEMORY OFRAY ABATE, NORMAN BABINEC, MARTIN BOTT, GEORGE FORBES-BENTLEY, MICHAEL CONLIFFE, SHAWN DUFORD, JOHN FULTON, JACQUELINE HÉBERT,REVEREND STEPHEN HILL, DR. BARRY ISAAC, WILLIAM LINDNER, HAZEL MACDONALD, ART OLSON,CLAYTON PETRICK AND ODAS WHITE
Valerie Alexander and Greg RumpelJames Joseph BarretteFrank BottHélène Bourgaize and Normand Latulippe Catherine CalderwoodCan-Ital Ladies SocietyMargaret CracknellCV Labs – FMC University of CalgaryMargaret DoaneJoan FultonDr. Ron & Leni GeorgeJacqueline and Peter GilbertJoyce ArgallJeannine HébertChris Grant and Judy PattersonMike and Joanne HaydenManitoba ChapterHemophilia OntarioIan DeAbreuDr. A. James and Helen BlackGrace JasperDaniel LangloisLinda LaxdalPatricia LaxdalJennifer LelièvreDr. David LillicrapErma Chapman and James LoveBrian and Stephanie LucasLorne MacDonaldJacqueline V. MacIntyreShirley and John MacKillopLawry MacLeod and FamilyFriends and Family of Mary MacLeodLorraine J. MarkoticEldene MillerWilliam MindellJudith A. MorganMike & Mary MuellerNewfoundland and Labrador ChapterNorthern Alberta RegionDaniela & John O’FeeOttawa & Eastern Ontario RegionDouglas PageLorraine Calderwood-ParsonsFaith and Kip PanesarLolita PelletierMarlene PermanandMary-Lou and Garnet PlanteDarlene & Ken PoyserPrince Edward Island ChapterQuebec ChapterJoan RobertsRuth RushtonAudrey I. SaigeonApollonia SteeleHenry TrillerToronto & Central Ontario RegionJanice YoungDr. Gershon GroweCanadian Hemophilia SocietyEileen LucasJeffrey WhitakerMargaret Whitaker
THE FOLLOWING REPRESENT CONTRIBUTIONS MADE TO THEMARJORIE CALDERWOOD MEMORIAL FUND:
Mr. & Mrs. Fred BrineEva DipasqualeMary Alice FinchFlorence GilbertMargaret GoodacreMary GoodacreJean & Reginald HealJeannette LuiseAdrian MeeuwissenJean & Ed MaskiewichRuth MesichEverett PersonLouise WatsonCarole & Dan Young
Ferdinand Labonté (In Memory of Luc Labonté)Oliver Tulk FamilyJean-Guy LavigneAnthony & Maxime VeilleuxAntoine L’HéraultJoseph WaldnerLouise MainvilleLionel MercierSusan E. Anderson Guy-Henri Godin Jamie Hill David L. Holmes François Laroche Elaine Reid (In Memory of Marvin Louis Olson) Friends and Family of Mary MacLeod Nova Scotia Chapter (In Memory of Martin Bott) Dr. and Mrs. Ron George (In Memory of Dr. Barry Isaac)(In Memory of Cecil and Pat Harris) Friends and Family of Dr. Barry Isaac (In Memory of Dr. Barry Isaac) Dr. David Lillicrap Margaret Cracknell (In Memory of George Forbes-Bentley) Godin Family: Fernande, Donald and Guy-Henri Northern Alberta Region British Columbia Chapter (In Memory of Captain Dick Rudd) Catherine Hordos (In Memory of Andras J. Hordos) Volunteers from the 1st Annual Road HockeyTournament (In Honor of Trevor Sauvé and JamieVilleneuve) Friends and Family of Marjorie Calderwood (In Memory of Marjorie Calderwood)Tanya and Flavio Antenucci(In Honour of Andris Antenucci)Dr. Bruce RitchieKen Poyser In honour of his “Angel” Darlene PoyserJeff Beck In honour of his “Angel” Heather MollerTom Alloway In honour of his “Angel” James BeckwithDavid PageIn honour of his “Angel” Patricia StewartCraig UpshawIn honour of his “Angel” Gayle Achtymichuk James KreppnerIn honour of his “Angel” Antonia Swann Tony NiksicIn honour of his “Angel” Loretta NiksicDr. and Mrs. Ron GeorgeIn honour of their “Angels” Dr. Martin Inwood, Dr. Irwin Walker,Dr. J. Cranby, and the Hemophilia Nurse CoordinatorsBlanchette-D’Fana FamilyIn honour of their “Angel” Kevin BlanchetteCan-Ital Ladies SocietyOttawa & Eastern Ontario Region(In Memory of Michel Frank)Frank Bott(In Memory of Martin and Gregory Bott)
HONORARY MEMBERSHIPS
Frank Bott and Family Canadian Hemophilia Society British Columbia Chapter Southern Alberta RegionNorthern Alberta Region Manitoba ChapterNew Brunswick ChapterNewfoundland and Labrador ChapterNova Scotia ChapterPrince Edward Island ChapterQuebec ChapterHemophilia SaskatchewanHemophilia Ontario Hemophilia Ontario (On Behalf of the Maynard Family) Central West Ontario RegionNorth Western Ontario Region

H E M O P H I L I A T O D AY S P R I N G 2 0 0 818 f o c u s o n r e s e a r c h
DREAM OF A CUREThe role of X-inactivation in the expression of hemophilia A in women
2007 - 2008Dr. Wenda L. Greer, FCCMGProfessor, Department of PathologyDalhousie University - Halifax, Nova Scotia
Hemophilia A is an X-linked bleeding disorder
resulting from mutations inthe FVIII gene. One functionalFVIII gene is sufficient fornormal clotting. Thus,typically XY males who inheritone mutated FVIII gene are affected whileheterozygous XX females are not. Rarely,heterozygous females with Hemophilia Ahave been described. These can arise due tounfavourably skewed X chromosomeinactivation. This is a dosage compensationmechanism that causes one X in everyfemale cell to be inactivated early indevelopment. In most females,approximately half of their cells inactivatetheir maternal and half their paternal X. Inrare cases, X chromosome inactivation isskewed. If it is skewed toward the activationof a mutated gene, a heterozygous femalecan be affected. A family has presentedwith several males and several femalesaffected with Hemophilia A. In the females,most cells were expressing the mutatedpaternal X chromosome. It is unlikely thatchance could account for the dramaticskewing of X chromosome inactivationleading to three affected females.
Our objective is to understand why thesefemales are expressing Hemophilia A. Ourhypothesis is that it is due to skewed Xchromosome inactivation ratios resultingfrom an inherited predisposition for themutated X-chromosome to remain active.
Dream of a Cure CHS Research ProgramSupporting research towards improving the quality of life for persons withhemophilia and finding a cure have been goals of the Canadian Hemo-philia Society (CHS) since it was founded in 1953. Since 1990, throughfunds provided by the Hemophilia Research Million Dollar Club and the CHS, the Societyprovides basic scientific research grants and studentships aimed at developing treatmentsfor hemophilia and finding a cure.
The following reports describe the projects funded in 2007 and 2008.
Our aims are to:▪ determine X chromosome inactivationpatterns and correlate these with diseaseexpression
▪ determine whether X chromosomeinactivation ratio skewing is moreconsistent with genetically influenced orrandom X chromosome inactivation.
▪ delineate, through microsatelliteanalysis, a region of the X-chromosomethat is associated with variedsusceptibility of X chromosomeinactivation.
▪ consider potential candidate genes fromthis region.
▪ identify the clinical symptoms andstandards of care of carrier females, andtheir experiences with medical treatmentby interviewing carrier females andhealthcare professionals.
We believe that this family provides aunique opportunity to study X chromosomeinactivation and its role in the expressionof Hemphilia A in heterozygous females. Italso provides an opportunity to documentthe clinical phenotype of female carrierswho differ in their factor VIII activitiesaccording to their respective X chromosomeinactivation ratios.
DREAM OF A CUREGene therapy of hemophilia A
2007 - Second year fundingDr. Gonzalo HortelanoAssistant Professor, Department of Pathology McMaster University - Hamilton, Ontario
We will evaluate the feasi-bility of cell transplanta-
tion therapy to reverse severehemophilia A in mice. Althoughcurrent factor VIII (FVIII) prod-ucts are safe, patients must endure life-long regular FVIIIinfusions. Thus, a safe and more economictreatment is desirable.
Gene therapy is an alternative. Gene ther-apy strategies use virus as vehicles to intro-duce the FVIII gene, but they are associatedwith undesirable immune responses. Alterna-tively, transplanted cells producing FVIII areonly temporarily functional. We propose thetransplantation of non-autologous cells (notfrom the patient) genetically engineered tocontinuously produce FVIII. To avoid rejectionof the transplanted cells, they are enclosed intiny microcapsules (less than 1mm in diame-ter) before being transplanted. The microcap-sules allow the free flow of FVIII, but areimpermeable to immune cells, therefore pro-tecting the enclosed cells.
We found that mice transplanted with mi-crocapsules containing muscle cells engi-neered to secrete factor IX contained highamounts of factor IX in the blood for at least120 days and did not mount an immune re-sponse to human FIX. More importantly, thistreatment was able to reverse the disease insevere hemophilia B mice. If this wereachieved in humans, it would eliminate severeand moderate hemophiliacs. Therefore, we willapply the same strategy to hemophilia A.
Initially, we will engineer muscle cells toproduce FVIII, and determine the amount ofFVIII they produced. Second, we will encloseFVIII-producing cells in microcapsules that willthen be transplanted into mice to determinehow much FVIII is found in blood, and for howlong. Any immune responses to FVIII will bestudied. Finally, the correction of the disease inhemophilia A mice will be investigated.
This transplantation therapy could reduceand ultimately eliminate the need for regularFVIII injections. Importantly, the microcapsulescan be removed, increasing the safety of thetreatment.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 19f o c u s o n r e s e a r c h
DREAM OF A CUREPlatelet type von Willebrand disease: An underdiagnosed cause of excessivemucocutaneous bleeding?
2008 - Second year fundingDr. Maha OthmanAdjunct Assistant Professor, Department ofPathology and Molecular MedicineQueen’s University - Kingston, Ontario
Platelet type von Willebranddisease (PT-VWD) and type
2B von Willebrand diseasehave similar clinical as well aslaboratory features while re-sulting from abnormalities intwo different genes. Type 2BVWD results from a defective von Willebrandfactor (VWF) and PT-VWD is caused byplatelet GP1BA gene defect. The discrimina-tion between the two disorders is often achallenge. The general tests necessary for theidentification require particular technical ex-perience and necessitate fresh blood samples.Definitive diagnoses can be made by reveal-ing the gene defect in either the VWF or theGP1BA. The correct diagnosis and discrimina-tion between the two disorders has impor-tant implication on treatment decision. TheVWF/FVIII concentrate, the major treatmentin type 2B-VWD, may worsen platelet countand bleeding conditions in PT-VWD. Plateletconcentrate is the ideal treatment for PT-VWD.In this study, we propose that patients withPT-VWD are being under/misdiagnosedamong type 2B VWD and we adopt the useof a genetic approach for a definitive diagno-sis of PT-VWD. The DNA analysis will includethe related area of the VWF gene responsiblefor type 2B VWD and also the platelet GP1BAgene responsible for PT-VWD in 100 patientsinitially diagnosed with type 2B VWD fromCanada and worldwide. Under the auspicesof the International Society for Thrombosisand Hemostasis: Scientific and Standardiza-tion Committee on von Willebrand Factor, weestablished an online database/disease reg-istry now accessible at www.pt-vwd.org. The project/registry will address the ques-tion of how many PT-VWD cases are beingmisdiagnosed among the type 2B VWDcases, increase awareness among physi-cians, specialists and patients about this di-agnostic problem and will indicate thesignificance of the genetic analysis in thesepatients with subsequent implication ontreatment decision.
DREAM OF A CUREFactor VII(a) clearance behaviour
2008 - Second year fundingDr. William P. SheffieldAssociate Professor, Department of Pathology and Molecular MedicineMcMaster University - Hamilton, Ontario
The hemophilia communityknows all too well that
the replacement therapy thatcan restore hemophiliacs toan active life is not alwaysproblem-free. For individualswith hemophilia A, replace-ment therapy with purified recombinantfactor VIII (FVIII) can sometimes be compli-cated by inhibitor formation. Inhibitors areantibodies directed against the injectedFVIII. Fortunately, administration of recom-binant factor VIIa (FVIIa) can bypass thispotentially serious problem. However, FVIIis one of the coagulation factors thatleaves the circulation the most rapidly. Thisclearance behaviour is not completely un-derstood. For this reason, Drs. Bill Sheffieldand Bryan Clarke, of McMaster Universityand Canadian Blood Services have receiveda CHS research grant to study the clearanceof FVII(a) in mice genetically altered tohave hemophilia A. The investigators willuse DNA and cell culture technology tomake both human FVII identical to currentclinical products, and new forms of FVII intheir laboratories. Once purified, how longthe FVII-related proteins last in the mousecirculation, and how well they controlbleeding will be determined. The most un-usual products to be tested are “fusions” -in which FVII and human serum albumin,ordinarily separate proteins, are combinedinto a single chain. The researchers proposethat FVII will continue to work in this newformat, and will remain in the circulationfor much longer than the current product.The longer it remains, the more effective itshould be in combating bleeding. Sheffieldand Clarke hope that their research willlead to better understanding of the mecha-nism of action of rFVIIa, and to the designof improved rFVII(a) products to providecaregivers with novel tools to help hemo-philiac patients with inhibitors.
DREAM OF A CUREStructural and genetic analysis of thecomplexes between factor VIII and lowdensity lipoprotein receptor-related protein: Toward a long-acting factor VIII
2008 - First year fundingAnn English, PhDDepartment of Chemistry and BiochemistryConcordia University – Montreal, Quebec
Scientific developmentshave provided a new
generation of safer factor VIII(FVIII) biopharmaceuticalsthat are free of blood-bornpathogens. However, the highcost of FVIII still remains abig hurdle in hemophilia treatment. Onlycertain countries can afford prophylaxis oron-demand treatment while many otherscannot even meet on-demand require-ments. Clearly, FVIII has to be further devel-oped to yield a product with a prolongedhalf-life.
Our project that is being supported bythe CHS Dream of a Cure Research Programwill provide the critical structural informa-tion to inform the development of longeracting FVIII. It is well known that low-den-sity lipoprotein receptor-related protein(LRP), a receptor molecule, is responsiblefor eliminating FVIII from blood. FVIII clear-ance by LRP requires that the two proteinsbind to each other. Thus, if the FVIII-LRPbinding interaction is decreased, FVIII willremain in the blood stream longer. How-ever, FVIII/LRP binding mechanisms have tobe well understood to avoid possible sideeffects such as the induction of inhibitoryantibodies. We will generate a 3D model ofthe FVIII/LRP binding interfaces using x-raycrystallography. Complexes between spe-cific FVIII domains and LRP clusters willelucidate at the molecular level how LRPbinds and eliminates FVIII. Such atomic-level structural details of the binding inter-faces will indicate how the sequence ofFVIII should be modified to decrease its interaction with LRP. Reduced affinity be-tween FVIII and LRP will be evaluated usingstate-of-the art biophysical techniques. Theresults will guide the development of thenext generation of FVIII biopharmaceuticalswith a prolonged biological half-life. Longerlasting FVIII will allow treatment for all andbring us one step closer to a cure.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 820 f o c u s o n r e s e a r c h
DREAM OF A CUREAn evaluation of the prevalence andfunctional significance of non-neutralizing antibodies to factor VIII
2008 - First year fundingFunded through a research grant to theCanadian Hemophilia Society from BayerHealthCare
Dr. David LillicrapDepartment of Pathology and MolecularMedicine Queen’s University – Kingston,Ontario
The development of anti-bodies to factor VIII (FVIII)
represents the main treat-ment-related complication ofcurrent therapies for hemo-philia A. For the past 30years, this complication hasbeen evaluated by a laboratory test thatdetects only those antibodies that interferewith FVIII’s clotting function. There is grow-ing evidence to suggest that in addition toantibodies that inhibit the functional activ-ity of FVIII, some “non-neutralizing” anti-bodies are also generated by FVIII exposure.The prevalence of these antibodies, theiroverlap with neutralizing inhibitors andtheir clinical significance are all factorsthat are very poorly characterized and formthe basis for the studies proposed in thisresearch project. In this project, we will es-tablish a laboratory test to detect andquantify the levels of antibodies that bindto FVIII in plasma. The test plasma sampleshave already been characterized with afunctional antibody test (the Bethesdaassay) and thus overlapping patterns of re-activity will be apparent. Finally, when de-tected, we will attempt to correlate thepresence of non-neutralizing antibodieswith in vivo FVIII recovery and half-life.
CARE UNTIL CURE
Creating meaningful messages for individuals with mild hemophilia
2007 - Second year fundingJoAnn K. Nilson, PTPhysiotherapistSaskatchewan Bleeding Disorders ProgramSaskatoon, Saskatchewan
This multi-phased projectbrings individuals with
mild hemophilia and physio-therapists together to createmore meaningful educationalmaterials specifically for peo-ple with mild hemophilia. TheCanadian Physiotherapists in HemophiliaCare (CPHC) have serious concerns aboutgaps in patients’ understanding of mild he-mophilia. Young adults with mild hemo-philia are often seen in the emergencyroom days after a traumatic incident withan uncontrolled bleed which then takesweeks or months to totally resolve. Theseclinical experiences suggest that the edu-cational materials and strategies currentlyin use, that target individuals with severehemophilia, are not effective in providinginformation that facilitates those with mildhemophilia to seek care in a timely manner.
The purpose of this study is to consultyoung adults with mild hemophilia, parentsof children or adolescents with mild hemo-philia and PTs from across Canada in orderto identify appropriate communicationstrategies to be used in educational mate-
rial about health and healthcare specificallyfor people with mild hemophilia. In Phase 1we will focus on the lived experiences ofyoung adults with mild hemophilia fromfour locations in Canada. Through semi-structured interviews, we will learn aboutparticipants’ internal ‘processes’ andchoices that they make in accessing med-ical care after injury, learn about messages,information and knowledge that partici-pants feel would motivate them to seekcare in a timely manner. During Phase 2,the knowledge gained in Phase 1 will beused to guide a group of PTs from acrossCanada. They will identify educationalstrategies that are grounded both in theexperiences and attitudes of individualswith mild hemophilia and in the realities ofthe health care system. In Phase 3, thesestrategies will be further refined duringfocus groups of young adults and PTs andparents of children with mild hemophiliaand PTs in both French and English. Thisphase will also include written or telephoneconsultation with young adults with mildhemophilia who live in rural settings. Par-ticipants from each phase will be invited tocontinue their involvement in the projectthrough written or verbal feedback aftereach phase.
This research will help to develop amodel that demonstrates a viable way ofintegrating the perspectives and knowl-edge of patients and health care profes-sionals in order to create the mostmeaningful, client centered, realistic edu-cational strategies specifically for personswith mild hemophilia.
Care Until CureThe Care Until Cure Research Program was established inthe year 2000 in collaboration with Wyeth Canada.Wyeth Canada is engaged in the discovery, development,and commercialization of human pharmaceuticalsthrough recombinant DNA and other technologies. This program allows Canadianinvestigators to conduct research on various medical and psychosocial aspects ofbleeding disorders. Grants are given for clinical research, including outcome evalu-ation, in fields relevant to improving the quality of life of persons with hemophilia,persons with von Willebrand disease or other inherited bleeding disorders, personswith related conditions such as HIV or hepatitis C as well as carriers of an inher-ited bleeding disorder.
The following reports describe projects funded in 2007 and 2008.

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 21f o c u s o n r e s e a r c h
CARE UNTIL CURE
The prevalence of symptomatic pediatricVWD
2008 - Second year funding Dr. Paula James, FRCPCAssistant ProfessorQueen’s University - Kingston, Ontario
Von Willebrand disease(VWD) is an inherited
bleeding disorder that causesbleeding from mucousmembranes (ie: nosebleeds,bleeding gums and heavymenstrual periods) and easybruising. Diagnosing the condition can bevery difficult, particularly in children.Although bruises and nosebleeds arecommon among children with VWD, veryyoung children may not have had a chanceto manifest other characteristic bleedingsymptoms, such as heavy menstrual periodsor bleeding after surgery. To compound this,it is often difficult for patients to recognizewhether certain symptoms are normal orabnormal and most of the attempts toaddress this by creating standardizedbleeding questionnaires have been focusedon the adult population.
In the current study, we propose toaddress the issue of the symptomaticprevalence of VWD in children byinvestigating children who have symptomsof bleeding or bruising for VWD.Additionally, we propose to validate acommonly used (modified) adult bleedingquestionnaire in children during the courseof this study. We will accomplish this byscreening between 10,000 and 15,000children attending a pediatric outpatientcentre for bleeding or bruising symptoms.Those that report a problem with bleedingor bruising symptoms will be furtherevaluated using a bleeding questionnaire.Children with positive bleeding scores willthen be investigated with VWF laboratorystudies. The bleeding questionnaire will alsobe administered to a group of ~300 normalchildren to allow for the validation of thequestionnaire. This study will be carried outby investigators who have recentlycompleted a complementary study,performed primarily on adults, evaluatingthe prevalence of VWD at the level ofprimary care.
CARE UNTIL CURE
Non-steroidal anti-inflammatory drugsand menorrhagia revisited
2008 - Second year fundingDr. Rochelle Winikoff, FRCPStaff hematologistCHU Sainte-Justine - Montreal, Quebec
Menorrhagia is a commonclinical problem to
which there is no standardmedical treatment approach.It is estimated that about30% of women complain ofmenorrhagia and it is themain presenting complaint in women re-ferred to gynecologists. Non-steroidal anti-inflammatory drugs (NSAIDS), whichnon-specifically inhibit cyclooxygenase(COX), are effective in approximately 50 to60% of women with menorrhagia, with re-ductions in menstrual blood loss (MBL) ofthe order of 30 to 40%. Clinical studieshave shown that NSAIDs are more effectivein women who have higher baseline MBL. Asubset of women with menorrhagia haveincreased MBL related to overproduction ofprostacyclin (PGI2) and increased localuterine vasodilatation, which may be tar-geted by NSAID therapy.
Among women with menorrhagia, thosewho produce higher baseline levels of PGI2are more likely to have a better response tonon-specific COX inhibition by NSAIDSthan women who secrete lower levels. Thevariability and degree of response toNSAIDS observed in the literature may, atleast in part, depend on the baseline levelsof PGI2 production in women with menor-rhagia. Other clinical factors such as age,weight, parity and dysmenorrhea may alsopredict a favourable response to NSAIDtherapy. The main objective of this study isto identify clinical predictors of response toNSAID therapy in women with menorrha-gia. We will also determine if higher base-line levels of PGI2 in women withmenorrhagia correlate with their clinicalresponse to COX inhibition by NSAIDS.
Women between the ages of 18 and 40with primary menorrhagia will be treatedwith an NSAID for two consecutive men-strual periods and the MBL will be recordedusing the Pictorial Blood Assessment Chart(PBAC). Recruitment for this study will takeplace over 18 months. Potential clinicalpredictors of response to NSAIDS will be
collected. Baseline levels of PGI2 urinarymetabolites will be measured in all eligiblewomen. Logistic regression will be used toassess various clinical variables and PGI2 asa predictor of significant response to NSAIDtherapy. A significant response will be de-fined as a ≥ 30% decrease in PBAC score.The average baseline PBAC score will becompared with an average of 2 post-treat-ment PBAC scores.
The results of this study should help cli-nicians identify women for whom NSAIDtherapy should be considered upfront totreat menorrhagia. Clinical indices includ-ing baseline PGI2 measurements could be apart of the initial clinical evaluation formenorrhagia and could help distinguish be-tween women with menorrhagia who arelikely to respond to treatment with NSAIDSand those who are not, in whom alternativetherapies may be more beneficial. A similartreatment strategy could eventually be ap-plied to women with menorrhagia relatedto bleeding disorders
CARE UNTIL CURE
Bleeding disorders, menorrhagia and iron deficiency: An examination of quality of life
2008 - First year fundingDr. Ronald BarrDepartment of Clinical Epidemiology andBiostatisticsHealth Sciences centre - McMasterUniversity, Hamilton, Ontario
The Canadian HemophiliaSociety has awarded Dr.
Ronald Barr of McMasterUniversity, and co-investiga-tors at three other Canadiancentres, a research grant toanalyze data from a nationalsurvey of women and men with inheritedbleeding disorders. The survey was under-taken because a pilot study had shown thatwomen with the most common bleedingdisorder, von Willebrand disease, had muchpoorer overall health than men with thesame disease and about the same level ofpoor health as severe hemophiliacs who areinfected with the AIDS virus. It was pro-posed that bleeding disorders in women, bycausing heavy menstrual bleeding, lead tochronic iron deficiency, poor overall healthand low educational achievement. All re-

H E M O P H I L I A T O D AY S P R I N G 2 0 0 822 f o c u s o n r e s e a r c h
gional hemophilia centres in Canada sup-ported the national survey that collectedinformation and blood samples (to deter-mine iron levels) from a total of 408 peo-ple. A questionnaire asked about 14important aspects of overall health, highestlevel of education and use of iron supple-ments. Women in the survey answered a setof questions about their menstrual bleedingpattern. A state-of-the art measurementsystem was used to measure the overallhealth of each person. Statistical tests willshow whether women with bleeding disor-
ders have poorerhealth and lowereducationalachievementthan comparisongroups, such asmen with similarbleeding disor-ders and whetherthese deficits arerelated to irondeficiency. Re-sults from thestudy may justifya large random-ized clinical trialof iron supple-ments to improveoverall healthand educationalachievement in
women with excessive menstrual blood lossassociated with inherited bleeding disorders.This study is important because iron sup-plements are inexpensive to make, easy totake, and could greatly improve the qualityof life for millions of such women aroundthe world.
Novo Nordisk FellowshipThe Novo Nordisk Canada Inc. – Canadian HemophiliaSociety – Association of Hemophilia Clinic Directors of CanadaFellowship in Congenital and Acquired Bleeding Disorders is afellowship program established in the fall of 2001. Novo Nordisk has a leading positionwithin areas such as coagulation disorders, and manufactures and markets pharmaceuticalproducts and services that make a significant difference to patients, the medical profes-sion and society.
The goal of this fellowship program is to provide fellows in hematology or other rele-vant fields the opportunity to acquire clinical or research skills necessary to improve thecare and quality of lives of patients with hemophilia and other congenital or acquiredbleeding disorders.
The following report describes the project funded in 2007.
NOVO NORDISK FELLOWSHIP
Quality assurance of special coagulationlaboratory practices
2007 fundingDr. Elianna SaidenbergChief Resident in HematologyMcMaster University - Hamilton, Ontario
It is a pleasure for me tohave this opportunity to in-troduce myself to the hemo-philia community of Canada.I am presently in my sixthpostgraduate year of medicaltraining and am enrolled in atransfusion medicine fellowship at the University of Ottawa. Concurrent with thistraining I am working in the coagulationlaboratory and with the clinical hemophiliaand bleeding disorders service. Given thenecessity of treating many haemostatic defects with human and recombinant bloodproducts, the connection between transfu-sion medicine and hemostasis medicinefeels very natural.
This year I am the very fortunate andgrateful recipient of the Novo Nordisk -Canadian Hemophilia Society - Associationof Hemophilia Clinic Directors of CanadaFellowship in Hemophilia. I aim to use theopportunities afforded to me by thisfellowship to gain the skills needed toeffectively manage a coagulationlaboratory. Availability of prompt, preciseand accurate measurements of hemostaticparameters is vitally important in theprovision of medical care to patients withbleeding disorders. To further my knowledge
and understanding of procedures andprocess in the coagulation lab I amplanning several quality assurance projects.
The first project I have undertaken relates to creation of normal ranges forplatelet aggregation and secretion testsdone at our site. These tests are very impor-tant in the diagnosis of congenital and ac-quired disorders of platelet function as wellas other disorders of coagulation such asvon Willebrand disease. The testing ma-chines used are called aggregometers. Theyprovide a visual representation of the testresults as a graph and also provide meas-urements of the slope and amplitude of thecurve. Interpretation of these tests reliesheavily on the interpreting physician’sreading of the curve. Thus, the results couldvary based on the eye of the interpreter. Toimprove the accuracy of these test results itis recommended by the Clinical LaboratoryStandards Institute that every laboratorycalculate normal ranges for their own ag-gregometers. To comply with these recom-mendations, I have begun the task ofcompiling data on aggregation test resultsdone on healthy volunteers at our centre.This information will then be evaluated by a statistician who will apply the necessarymathematical processes to determine thenormal ranges.
Subsequent projects I have plannedwill evaluate the quality of other testsdone in the coagulation lab to help ensuretheir quality. Through assessment of theseprocedures, I will gain vital skills in labo-ratory management which will hopefullyhelp me ensure that I can provide the bestpossible care for my patients with bleed-ing disorders.
This study isimportantbecause ironsupplementsare inexpensiveto make, easyto take, andcould greatlyimprove thequality of lifefor millions ofsuch womenaround theworld.

Our Stories
H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 23o u r s t o r i e s
Ialways looked up to my older brotherPatrick. He was older, smarter, and bet-ter than me at just about everything. He
had what people call “The Midas Touch” orbetter yet, “The Patrick Touch”. Most broth-ers and sisters fight – and sometimes evendislike each other – not us.
For the first ten years of my life, every-thing was just right. It even seemed normalto watch Patrick giving himself needles atthe kitchen table. Patrick had a bleedingdisorder called hemophilia. This rare condi-tion is passed down from parent to child atbirth. Some parents may not even knowthey are carriers. My mom did not knowshe would give hemophilia to my brother.
The blood of people with hemophiliadoes not clot normally and they can bleedfor long periods of time, usually into theirmuscles and joints. To make his blood clot,Patrick had to get a needle into his vein.
Despite having this serious condition,my big brother never wanted – nor did hesettle for – a protected life inside ourhome. He faced every day head on, even ifit meant enduring pain from internalbleeding. Patrick skied, skated, and evenraced down the toboggan hill. I never gavemuch thought to his bleeding disorder untilI was old enough to learn the truth and de-tails about his condition.
Patrick lived with a secret. I learned thathe needed large amounts of blood productsto survive. With each needle he put into hisbody, Patrick was accepting someone else’s
blood. Unfortunately – and tragically – it was a time when some people donatedblood contaminated with HIV. At age 7,Patrick became HIV-positive, which meanthe had a great chance to someday developthe full-blown, life-threatening diseasecalled AIDS.
When I realized that Patrick’s illnesswould lead to his death, my world camecrashing down. I could not imagine my lifewithout him. Why would the blood that heneeded to survive take his life away? Theselife-and-death issues and unansweredquestions were too much for a 10 year oldwho liked to play and havefun with her big brother.
Patrick sensed the shockI felt upon learning his se-cret and engulfed me in hisarms with a “hug of love”,welcoming me as one of his“secret keepers”. My brotherhad not changed, but I had.I realized that each minutespent with him was veryprecious.
Full moons became our symbol of hope.Patrick taught me to wish upon every fullmoon in the hopes that a cure for AIDS wouldbe found before he took his last breath.
Patrick entered high school and his ac-complishments mounted: trophies, awards,and early university acceptance. To theoutside world, Patrick had it all. But the se-cret of living with AIDS continued to cast adark shadow over his many successes andhe knew that this shadow had to be lifted.Patrick decided to make his journey withAIDS public, knowing that many peoplewere afraid of this disease because they didnot understand it. He revealed that he hadcontracted HIV through tainted blood, likemany other Canadians. Patrick told hisstory so that people would realize that HIVand AIDS are preventable.
Although he was very sick, my dearbrother, friend and teacher never stoppedsharing his gift of love and laughter witheveryone. As days turned into weeks, it wassoon apparent that our full moon wishwould never come true. His medical careintensified while his smile and gracebrought us peace.
Patrick never complained about his painor expressed anger about dying. He didn’tquestion God about his imminent death; he accepted what was to be. Patrick’s opti-mistic outlook taught me FAITH, LOVE andACCEPTANCE.
The day Patrick died waslike no other day in my life.My mom woke me up to saygoodbye to my brother, for-ever. It was a cold, rainy, November morning. When Ientered his hospital room,tears poured down my face. I said goodbye to his bodythat day but I will never saygoodbye to his spirit.
I wear the precious rosary ring thatPatrick left me with pride. It is a simple goldband with ten knots for prayer, one for eachyear I lived without knowing his secret.
Having a brother like Patrick andwatching him die changed me. It has em-powered me to dispel the myths about HIVand AIDS. Patrick taught me the impor-tance of talking about HIV and AIDS as ameans of prevention. He shared his jour-ney and faced his death with bravery. He paved the way for us to continue histeachings and eradicate HIV and AIDS.Patrick left me with the hope that some-day AIDS will no longer take the lives ofbrothers, sisters, mothers, fathers andfriends.
With each full moon I still wish for acure for AIDS. This was Patrick’s wish. It ismine. And I hope that it is now also yours.
In the story Full Moon Wish Lyanne Fortin-Foster tells us in her own words about herexperience with her older brother Patrick, a young hemophiliac who contracted HIV and AIDS.
Lyanne shares this story of love, courage, and compassion. With each full moon, Patrickmade a wish: a wish that a way would be found to eliminate HIV and AIDS before he drewhis last breath.
Patrick0AIDS, the dream, remains alive through the organization dedicated to his memory,Patrick4Life, and the annual Partici-Patrick project in schools. Through awareness raising,education, and dialogue we will make Patrick’s wish come true one day. Visitwww.patrick4life.org.
Full Moon Wishby Karen Dunn
H E M O P H I L I A T O D AY S P R I N G 2 0 0 824 m e d i c a l n e w s
MedicalNews
Hepatitis C Press Review
by Michel Long, CHS Program Development Coordinator
� Study shows positive findings in treatingpatients with advanced hepatitis C
April 24, 2008 – The hepatitis C therapypeginterferon alfa-2b, when given as low-dose maintenance therapy, can preventdisease progression in certain patients whofailed previous interferon-based hepatitis Ctherapies and have advanced liver disease,according to findings from a large, four-year study. The study, called COPILOT(Colchicine versus Peg-Intron Long-Term),showed that low-dose peginterferon alfa-2b was superior to colchicine in improvingthe disease-free survival of patients withcirrhosis and portal hypertension, especiallyin patients who stayed on treatment.“These findings make a strong case forconsidering low-dose peginterferon alfa-2bas a maintenance therapy in patients withcirrhosis and portal hypertension who havefailed hepatitis C eradication therapy,” saidprincipal investigator Nezam Afdhal, MD.“While other interferon maintenancetherapies have been studied in the past fewyears in previous interferon nonresponders,these findings show, for the first time, aclinical benefit in a specific population withadvanced disease,” he said.
For more information: www.medicalnewstoday.com/articles/105346.php
� Alcohol, Tobacco and Cannabis All MayPromote Liver Disease Progression inPeople with Chronic Hepatitis C
In the April 2008 Journal of Hepatology,three hepatology experts reviewedenvironmental factors associated withaccelerated liver fibrosis progression inchronic hepatitis C (HCV) patients. Theynoted than these factors have been
investigated in order to improve clinicaloutcomes, especially for “difficult-to-treat”patients who tend to respond poorly tointerferon-based therapy. The authorswrote, “Several studies have shown that acombination of HCV infection and highlevels of alcohol abuse results in synergisticacceleration of liver fibrogenesis.” Inaddition, more recent data indicate thateven light alcohol consumption may alsoworsen fibrosis progression. Some studieshave suggested that tobacco smoking mayenhance histological activity in chronichepatitis C patients, thereby promotingfibrosis progression. This may be due tocytokine changes triggered by low oxygenlevels. Cannabis use is increasingly emergingas a novel factor linked to liver diseaseprogression in patients with chronichepatitis C. Studies have shown that regularcannabis smoking is an independentpredictor of both fibrosis and steatosisseverity in HCV-infected patients. Theauthors concluded, “Patients should beinformed of the deleterious impact ofalcohol, tobacco and cannabis use, andshould be offered appropriate support toachieve abstinence.”
For more information: www.hivandhepatitis.com/hep_c/news/2008/032808_a.html
� Use of CT Scans to Monitor LiverFibrosis in People with Hepatitis C
January 15, 2008 – Liver biopsy is regardedas the “gold standard” for diagnosing andstaging liver fibrosis in people withhepatitis C, but the procedure isunpleasant, costly, and carries a small riskof complications. Thus, researchers haveexplored a variety of non-invasive methods,including blood tests and external imaging,to monitor liver disease progressionwithout repeated biopsies.
Spanish researchers reported the resultsof study of one such method – computedtomography, or CT scans – in the December20, 2007 advance online edition of thejournal Hepatology. This study evaluated animage-processing method for assessingliver fibrosis using conventional CT scans inpatients with chronic hepatitis C.
Based on their findings, the authorsconcluded, “Optical digital analysis of CTimages of the liver is effective in
determining the stage and distribution ofliver fibrosis in chronic hepatitis C.” Theyadded, “Fibro-CT is a simple to use, readilyavailable and useful method for thediagnosis of fibrosis in patients with chronichepatitis C.”
For more information: www.hivandhepatitis.com/hep_c/news/2008/011408_b.html
� Liver Transplant Outcomes in HIVPositive Patients with Viral Hepatitis
April 29, 2008 – Until a few years ago, HIV-positive individuals were typicallyconsidered ineligible for organ transplantsdue to a high risk of poor outcomes. Thischanged, however, with the advent ofcombination antiretroviral therapy thatenabled full HIV suppression, good immunerecovery and longer life expectancy. At the43rd Annual Meeting of the EuropeanAssociation for the Study of the Liver(EASL) held in Milan in April, researcherspresented data on outcomes of livertransplantation among HIV-positiveindividuals in Italy, most of whom werecoinfected with the hepatitis C virus (HCV)or hepatitis B virus (HBV).
To evaluate possible extension of theindication for orthotopic livertransplantation to include HIV-infectedindividuals, the Italian National Centre forTransplantation nominated a committee ofexperts to design a protocol to be appliedon a national basis. The program wasvoluntarily adopted by six Italian livertransplant centres. Between September2002 and November 2007, 60 HIV-positiveindividuals with liver cirrhosis underwenttransplantation using cadaver donors. Theinvestigators concluded that, “The short-term results of orthotopic liver transplantin HIV-infected individuals are slightlyinferior when compared with thoseobserved in HCV or HBV monoinfectedorthotopic liver transplant recipients.”
For more information: www.hivandhepatitis.com/2008icr/easl/docs/042908_g.html

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 25m e d i c a l n e w s
� The differential identification of platelet type von Willebrand disease (VWD) from its non-identical twintype 2B VWD: A significant impact on treatment decision
Canadian PT-VWD molecular study and international database/registry
Opportunit ies to part ic ipate in research
SASKATOON, Sask, May 3, 2008 – At the annual meeting of the Associa-tion of Hemophilia Clinic Directors of Canada (AHCDC), an internationalHIV research collaboration was proposed between AHCDC and CHAVI.CHAVI is the Center for HIV/AIDS Vaccine Immunology and is currentlyone of two implementation projects under the Global HIV Vaccine Enter-prise. In July 2005, the National Institute for Allergy and Infectious Dis-eases (NIAID) awarded the CHAVI grant to a consortium of investigatorsfrom Duke University, the Dana-Farber Cancer Institute, Beth Israel Dea-coness Medical Center, Oxford University, and the University of Alabama-Birmingham, led by Dr. Barton Haynes.
The achievements of CHAVI can be viewed on their Web site(www.chavi.org). In a recent paper, they showed that both control ofviral load and control of disease progression could be tracked to specificDNA polymorphisms.
The project would investigate whether resistance to HIV infection canbe tracked to differences in genes (polymorphisms) among individuals. Itis sometimes said that HIV-negative individuals with hemophilia were“lucky” to have escaped HIV infection, but maybe they have an in-bornresistance that could be traced to their genes. If there were more knowl-edge about this resistance, there could be opportunities to develop vac-cines and drugs to enhance this resistance for people around the worldstill faced with HIV exposure.
The specific project, Investigations of Gene Variants Associated withResistance and Susceptibility to HIV-1 infection in HIV-1 Exposed but Un-infected Individuals with Severe Hemophilia A, has been funded and ap-proved by the National Institutes of Health.
There is a growing concern about the appropriateness of the differ-ential identification between type 2B von Willebrand disease (2BVWD) and platelet type-VWD (PT-VWD). The two similar bleeding
disorders result from genetic defects at two different genes, the VWFand the platelet GP1BA genes.
The required platelet aggregation based phenotypic tests are poorlyapplied in the general hemostasis laboratory and requires fresh bloodsamples. The genetic analysis is a gold standard confirmatory test withfeasibility of sample transport.
Evidence exists that PT-VWD is being misdiagnosed among cases oftype 2B more often than not and even among cases of idiopathic throm-bocytopenic purpura (ITP) and possibly unexplained platelet disorders.There is an obvious critical impact on treatment decisions. We discussedthis diagnostic dilemma at the ISTH VWD subcommittee meeting inGeneva in July 2007 and an international online PT-VWD database/reg-istry was proposed and approved at the meeting. The database is cur-rently available at: www.pt-vwd.org.
This database represents a rich resource for PT-VWD and outlines theCanadian PT-VWD molecular study which is based mainly on geneticanalysis of the related region of the VWF gene in phenotypically diag-nosed type 2B VWD cases and, in mutation negative, the platelet GP1BA
gene where mutations responsible for the PT-VWD cases have beenreported. The study will address two major questions:1. Is PT-VWD truly rare or underdiagnosed?2. How many cases are being misdiagnosed among type 2B VWDcases?The Canadian molecular study is funded by the CHS, directed by
Dr. Maha Othman and carried out at David Lillicrap‘s laboratory facili-ties at Queen’s University. It aims to achieve a target of 100 cases be-fore the end of 2008.
We need collaboration from general practitioners, clinical direc-tors and all hematologists who may have identified cases with provi-sional diagnosis of type 2B VWD based on clinical and laboratory datato send in DNA samples together with phenotypic information. Thegenetic analysis will be performed to confirm the differential diagno-sis and results from the study will be reported back to the participat-ing laboratories and clinics.
Maha Othman, MD, PhDPathology and Molecular MedicineQueen’s [email protected]
� AHCDC-CHAVI: An international research collaboration on HIV proposed
by Drs. Irwin Walker and Bruce Ritchie
The hemophilia community that was so devastated by HIV nowhas an opportunity to contribute in an important way towards solvingthe world’s continuing problem of HIV infection. Individuals with he-mophilia A seem the most suited for this project as they were almostall infected within a period of five years and the infection rate washigh. Eligible individuals include those with severe hemophilia A(<1% factor VIII), who are HIV negative and who were born in or be-fore 1980.
Why select Canada?
Though other countries have been approached and will likely con-tribute, Dr. Lucy Dorrell, from Oxford University and coordinator ofthe CHAVI project, feels that Canada is best situated to kick-start theproject because of its up-to-date Canadian Hemophilia Registry andsample collection system, the Blood Borne Pathogens SurveillanceProject (BBPSP).
How can individuals take part in this research?
The project fits very well into the BBPSP project. For thoseindividuals who have donated samples to BBPSP and have signed thelatest consent form, nothing more needs to be done as the samples atBBPSP in Edmonton are entirely suitable. Those who signed an earlierversion of the consent form can re-consent on this latest version,with or without an extra blood sample. This form states, “I consent tosearch for genetic features that affect the predisposition to diseasecaused by blood borne pathogens described above.”

H E M O P H I L I A T O D AY S P R I N G 2 0 0 826 m e d i c a l n e w s
Rethinking the meaning of “spontaneous”
by Nicole Graham, PTVice-President, Canadian Physiotherapists in Hemophilia Care
The term “spontaneous bleed” is used extensively within the hemophilia community.Recently, the Canadian Physiotherapists in Hemophilia Care (CPHC) group has beendiscussing the meaning of this term and its implications.
“Spontaneous bleeding” is referred to in the medical literature; it is used by medicalprofessionals and is found in various printed materials. There are numerous scientific articles quoting the term, especially when referring to central nervous system (CNS)bleeds. Medical professionals including physicians, nurses, social workers and physiothera-pists also refer to the term “spontaneous bleed” when a bleed occurs for which the causeis unknown. In the resource binder All About Hemophilia: A Guide for Families, it states:“There is often no obvious cause for thebleeding – it just happens. This is calledspontaneous bleeding.” In addition, somebelieve that spontaneous bleeding canoccur in persons with severe hemophilia orin those with inhibitors.
The term “spontaneous” is defined as aprocess or event occurring withoutapparent external cause. This leads us tobelieve that a person with hemophilia cansustain a bleed for no good reason. Is thistrue? Is the problem in hemophilia not onlya lack of factor which affects thecoagulation cascade, but also a problem ofbleeding with no apparent cause, withoutstimulus or trauma? Is there a problemwith the integrity of the tissues? Is thereany evidence to show that normal tissuescan start bleeding without any disturbancein hemophilia?
In the absence of any evidence-baseddata on the topic, we do have long-termclinical follow-up. Take for example, a knee joint bleed. After an initial trauma followed bya bleed, the tissues are disrupted. Recurrent bleeding in the same joint may occur afterminimal trauma that may go unnoticed, leading one to believe that the resulting bleedhappened “spontaneously.” Perhaps it is semantics. Rather than using the term “sponta-neous bleed,” would it add clarity to say “a bleed with an unrecognized cause?” Gettingaway from the term spontaneous may help the person with hemophilia and those whotreat them to recognize that even minimal trauma can trigger a bleed and thus lead toprevention, better recognition and more timely response to treatment so that the health ofthe person with hemophila can be improved.
Perhaps more questions are raised than answers exist at this point. However, the CPHClooks forward to your opinions and ongoing discussion on the topic.
Canadian Physiotherapists in Physiothérapeutes canadiensHemophilia Care en hémophilie
AHCDC and Baxter Canadaannounce multi-yearresearch partnership
SASKATOON, Sask, May 3, 2008 – The Association of Hemophilia ClinicDirectors of Canada (AHCDC) and BaxterCorporation (Canada) have announced aresearch program called the Baxter-Canadian Hemophilia EpidemiologicalResearch Program (B-CHERP).
Through the B-CHERP program, Baxterwill provide$875,000 infunding overthree years. Thissupport will fundthe establishmentof a data analystposition tooversee keyresearch projectsutilizing theCHARMSdatabase, and theinitiation of anopen competitionfor researchgrants annuallyover the nextthree years. Threepeer-reviewedgrants will beawarded annually.
“We are verypleased to have this continued partnershipwith Baxter Canada,” said Dr. ManuelCarcao, a physician with the Hospital forSick Children, Division ofHaemotology/Oncology, in Toronto andoutgoing president of the Association ofHemophilia Clinic Directors of Canada. “The research grants and funding providedfor the CHARMS database are importantinvestments in necessary infrastructure and resources that allow researchers to askmeaningful questions about hemophiliacare and treatment.”
“Through our ongoing partnership withthe AHCDC we continue to gain a deeperunderstanding of what the hemophiliacommunity needs and how we can help,”said Serge Messerlian, Business UnitDirector, BioScience, Baxter Corporation.“The work the AHCDC does is invaluableand Baxter is proud to be their partner.”
“The research grants
and funding provided
for the CHARMS
database are
important
investments in
necessary
infrastructure and
resources that allow
researchers to ask
meaningful questions
about hemophilia
care and treatment.”
- Dr. Manuel Carcao
Rather than
using the term
“spontaneous
bleed,” would it
add clarity to say
“a bleed with an
unrecognized
cause?”

H E M O P H I L I A T O D AY S P R I N G 2 0 0 8 27t h e b l o o d f a c t o r
� Companies report on newdevelopments at AHCDC annualmeeting
SASKATOON, Sask, May 4, 2008 – At theannual meeting of the Association ofHemophilia Clinic Directors of Canada, held May 2-4, companies in the Canadianmarketplace reported on progress in thedevelopment of novel clotting factorconcentrates.
� Baxter to introduce 2000-IU vial sizeof Advate®
Baxter confirmed that the company willintroduce the 2000-IU vial size for itsrecombinant factor VIII product, Advate®, in late summer or early fall 2008.
It also presented news of products in its pipeline. Baxter has applied forInvestigational New Drug (IND) approval toproceed to clinical trials for its recombinantvon Willebrand factor. In addition, thecompany is engaged in pre-clinicaldevelopment of a longer half-liferecombinant factor VIII product.
� Bayer moving ahead with liposomefactor VIII
Bayer reported that it is moving ahead witha Phase III clinical trial of its novel factorVIII concentrate, BAY 79-4980. Thiscombination of Kogenate® FS andliposomes is intended to produce a longer-acting factor VIII which would reduce thefrequency of infusions for both prophylacticand on-demand therapy.
The randomized, double-blind, crossovertrial will recruit 250 patients fromcountries around the world, includingCanada. It will last three years and be thelargest trial of its kind ever conducted inthe field of hemophilia.
� CSL Behring refines Humate P®CSL Behring reported that it had madeseveral refinements to Humate P®, aplasma-derived product used to treat von Willebrand disease. Humate P is nowavailable in a formulation that requires lessvolume of diluent. It comes shipped withthe Mix2Vial® administration set and has
approval for room temperature storage.Helixate® FS, a recombinant factor VIII
product, will be introduced into Canada insummer 2008. (See Hemophilia Today, Vol 43, no 1.) The product will soon bemade available in the 2000 IU vial size.
CSL Behring also described its albufuse™technology, designed to extend the half-lifeof therapeutic proteins through geneticfusion to recombinant human albumin. Pre-clinical data suggest that fusion ofrecombinant factor VIIa (rFVIIa) torecombinant human albumin, usingalbufuse, extends the circulatory half-lifeof the recombinant protein six- to nine-fold.
� Novo Nordisk develops factor VIIa analogues
Among the products in the pipeline at NovoNordisk Canada is a long-acting analogueof factor VIIa, called NN1728. ThisGlycoPEGylated Factor VIIa, currently inpre-clinical development, is being developedby Novo Nordisk under a license from Neose.
Factor VIIa is used in the treatment ofbleeding episodes and for the prevention ofbleeding during surgery in hemophiliapatients with inhibitors to coagulationfactors VIII or IX.
Also in development at Novo Nordisk area short-acting, high-potency analogue offactor VIIa, called NN1731, and arecombinant factor VIIa, called VII-25, thatis stable at room temperature for 24 months.
� Octapharma introduces two new products Octapharma Canada Inc. announced thatWilate® and Octaplex® will be available inCanada as of May 2008.
Octaplex is a plasma-derivedprothrombin complex concentrate (PCC),containing human coagulation factors II,
VII, IX and X in combination. It is currentlylicensed in 26 countries worldwide, includingCanada, for the treatment and prophylaxisof bleeding in hereditary and/or acquiredcoagulation deficiencies of the prothrombincomplex factors. PCCs are used in thetreatment of factor II and X deficiency.
Wilate is Octapharma’s plasma-derivedvon Willebrand factor/FVIII concentrate. Itis licensed in 18 countries for the treatmentand prophylaxis of hemophilia A and/or vonWillebrand disease (VWD). In Canada,Wilate is currently approved for thetreatment and prophylaxis of bleeding inpatients with hemophilia A. Octapharma’ssubmission to Health Canada for a VWDindication is currently under review.
� Wyeth’s Xyntha® approved by HealthCanada
Wyeth reported that Health Canada’sBiologics, Radiopharmaceuticals andGenetic Therapies Directorate has approvedits new genetically engineered factor VIIIconcentrate, Xyntha®, for the treatment ofhemophilia A. Xyntha is a third-generationrecombinant factor VIII; the culture inwhich the cells are grown is free of anyhuman or animal material. In addition, thepurification process has been refined byutilizing a synthesized affinity ligand ratherthan a mouse monoclonal antibody.
Xyntha contains the identical B-domaindeleted factor VIII molecule as Refacto®,Wyeth’s other factor VIII concentrate. Inclinical trials, Xyntha was shown to beeffective at preventing or controllingbleeding, including preventing bleeding insurgery, for hemophilia A patients. It islicensed for routine and surgicalprophylaxis. The marketing date for Xynthain Canada is not known.
by David Page, CHS Executive Director
The
BloodFactor
Health Canada Endorsed Important Safety Information on PREZISTATM (darunavir)
On May 12, 2008, Health Canada issued a Public Communication providing patients withimportant new safety information about serious liver side effects that have been reportedwith PrezistaTM (darunavir).
Prezista, which is used in combination with another antiretroviral medication knownas ritonavir, is used to treat adult patients in whom other HIV therapy has failed.
The warning says that in clinical trials, 0.5 per cent of people who took the drugdeveloped hepatitis or inflammation of the liver.
The department says people on the drug should contact their doctor immediately ifthey have any of these symptoms: dark urine, yellowing of the skin, abdominal pain(especially on the right side below the ribs), general itchiness, decreased appetite, nauseaor vomiting and tiredness.
Patients should NOT discontinue their medication without consulting a doctor orpharmacist first.
Canadian Physiotherapists in Physiothérapeutes canadiensHemophilia Care en hémophilie

H E M O P H I L I A T O D AY S P R I N G 2 0 0 828 a g l o b a l p e r s p e c t i v e
by Michel Long, CHS Program Development Coordinator
The CHS International ProjectsCommittee, impressed with the qualityof the work being accomplished by the
national office, CHS Chapters and CanadianHTCs involved in World Federation of Hemo-philia twinning initiatives, is proud to be ableto continue to support the various Canadianand international partners who submittedfunding proposals in 2008. Grants have so farbeen confirmed for the following projects in2008. (The committee will continue to acceptproposals until June 30.)
� South African Hemophilia Foundation(SAHF) & Canadian Hemophilia Society(CHS)
$3,034 has been granted to SAHF to allowa South African youth to take part in theCHS Youth Leadership Training Workshop tooccur September 5-7, 2008.
� Tunisian Hemophilia Association (ATH)& Canadian Hemophilia Society -Quebec Chapter (CHSQ)
$7,000 has been granted to these partnersto support them in making possible variousactivities from their 2008 action plan, in-cluding medical and psychosocial work-shops, survey visits to 10 southern govern-orates, sponsorship of an ATH delegate toattend the WFH Congress and for CHSQmembers to travel to Tunisia to providetraining on strategic planning and the cre-ation of an efficient organizational structure.
� Jordanian Hemophilia and ThalassemiaSociety (JHTS) & Toronto and CentralOntario Region (TCOR) - HemophiliaOntario
$7,500 has been granted to these partnersto sponsor one JHTS delegate to attend the
WFH Congress. Furthermore, two membersof TCOR will travel to Jordan and two Jor-danians will travel to Canada to obtainknowledge and skills in patient education,volunteer development, recruitment andmanagement, strategic planning, leadershipdevelopment and succession planning.
� Shanghai, China HTC & SouthernAlberta Hemophilia Program, Calgary& Hemophilia Centre, Children’sHospital of Eastern Ontario
$15,000, for the next two years, has beengranted to these partners to complete thesecond part of a program to develop aneducational tool for teaching and self-learning for physiotherapists in China. The project will focus on trainingphysiotherapists as trainers to facilitatedissemination of this important disciplinein proper hemophilia care.
To learn about past and present accom-plishments of our twinning partners, our2008 action plan and more, please visit theinternational section of the CHS Web site:www.hemophilia.ca/en/international.
Letter of commendation for our 2007 international partnership work!We are proud to inform our readers thatour twinning project with South Africa andthe one between the CHSQ and Tunisiawere among the three finalists for the WFH2007 Twins of the Year Award. While wedid not win first place, this is still very encouraging news and will serve as a newsource of motivation for the work we accomplish through these projects.
Mr. Cesar Garrido, Chair of the WFH Hemo-philia Organization Twinning Committee,wrote: “The committee had the difficult taskof selecting a winner for the 2007 Twins ofthe Year Award. Though in the end your twin-nings were not selected for the award, I wouldlike to let you know that the committee wasvery impressed with your activities in 2007,and that you were among the three finalistsfor the award. On behalf of the entire com-mittee, I would like to thank you for your hardwork and dedication to twinning, and wishyou continued success in 2008.”
CHS continues to supportvaluable projects in 2008!
GlobalPerspectiveA
SAHF innovates with itsoutreach clinic on wheels!