Embed Size (px)
Citation preview
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 1/18
Click to edit Master subtitle style
4/22/12
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 2/18
4/22/12
NAME:Gopinath
AGE:13 years
SEX:Male
CHIEF COMPLIANTS:
C/O Hematuria for the past 2 days.
C/O Left loin pain for the past 2 days.
HISTORY OF PRESENT ILLNESS:
H/O Hematuria associated with loinpain.
No H/O frequency of micturition.
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 3/18
4/22/12
No H/O intake of any anticoagulants.
No H/O edema.
No H/O trauma.No H/O fever.
No H/O bleeding from other sites of the body.
PAST HISTORY:
H/O similar episode-1yr back-3days-spontaneously resolved.
No H/O TB.
No other relevant past history.
FAMILY HISTORY:
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 4/18
4/22/12
PERSONAL HISTORY:
Consumes a mixed diet.
Normal bladder and bowel habits.
GENERAL EXAMINATION:
Conscious,oriented,afebrile.Not anaemic,not icteric.
No cyanosis,no clubbing, no pedal edema.
No generalised lymphadenopathy.VITALS:
RR: 14/min,
PR: 82/min,
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 5/18
4/22/12
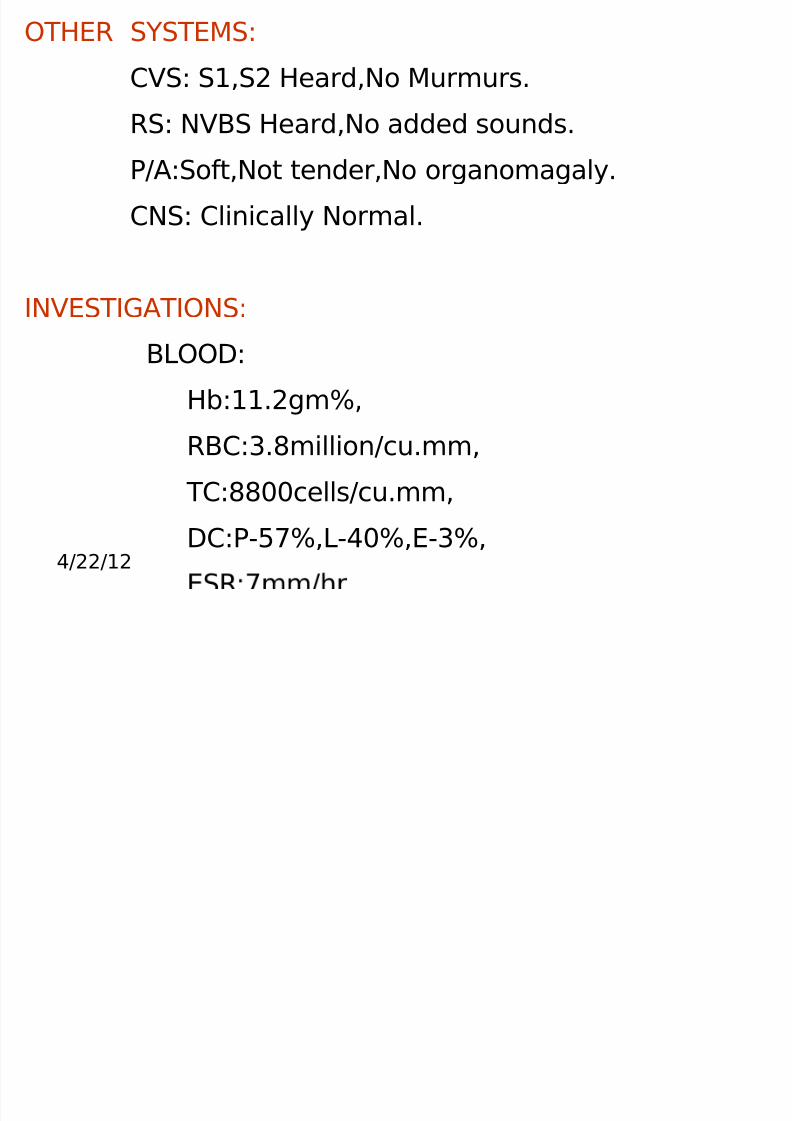
OTHER SYSTEMS:
CVS: S1,S2 Heard,No Murmurs.
RS: NVBS Heard,No added sounds.P/A:Soft,Not tender,No organomagaly.
CNS: Clinically Normal.
INVESTIGATIONS:
BLOOD:
Hb:11.2gm%,RBC:3.8million/cu.mm,
TC:8800cells/cu.mm,
DC:P-57%,L-40%,E-3%,
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 6/18
4/22/12
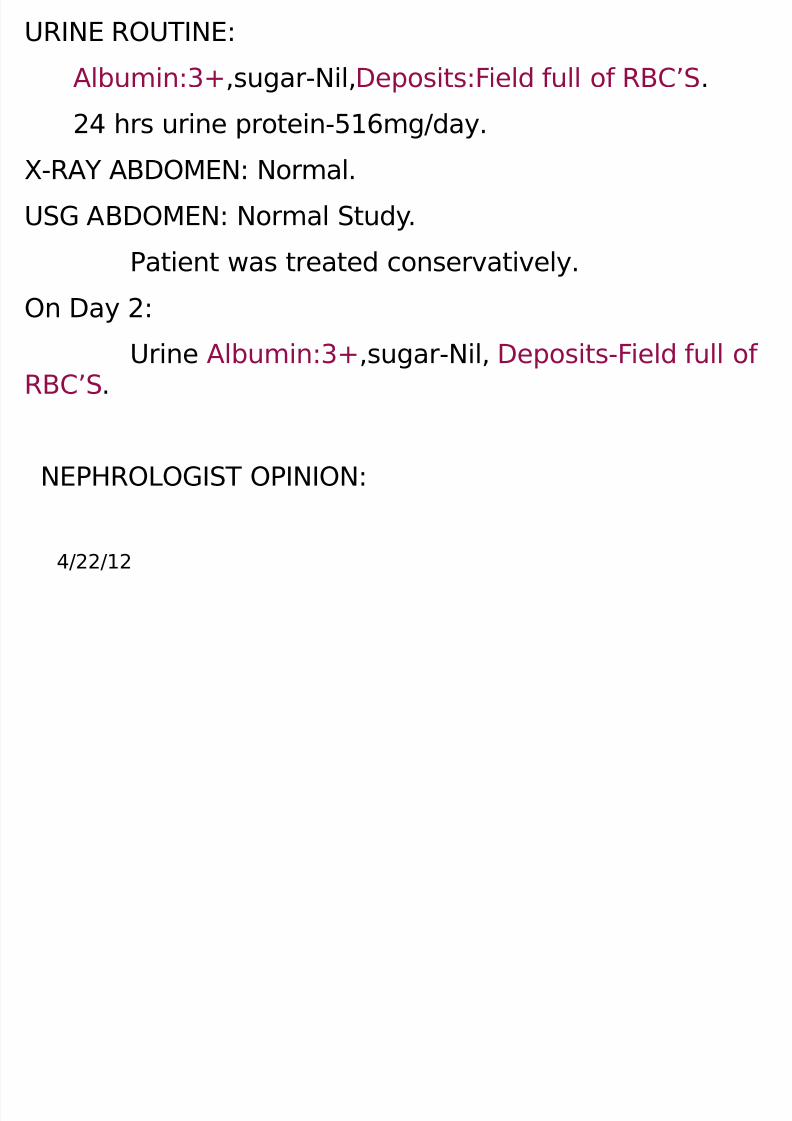
URINE ROUTINE:
Albumin:3+,sugar-Nil,Deposits:Field full of RBC’S.
24 hrs urine protein-516mg/day.X-RAY ABDOMEN: Normal.
USG ABDOMEN: Normal Study.
Patient was treated conservatively.On Day 2:
Urine Albumin:3+,sugar-Nil, Deposits-Field full of RBC’S.
NEPHROLOGIST OPINION:
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 7/18
4/22/12
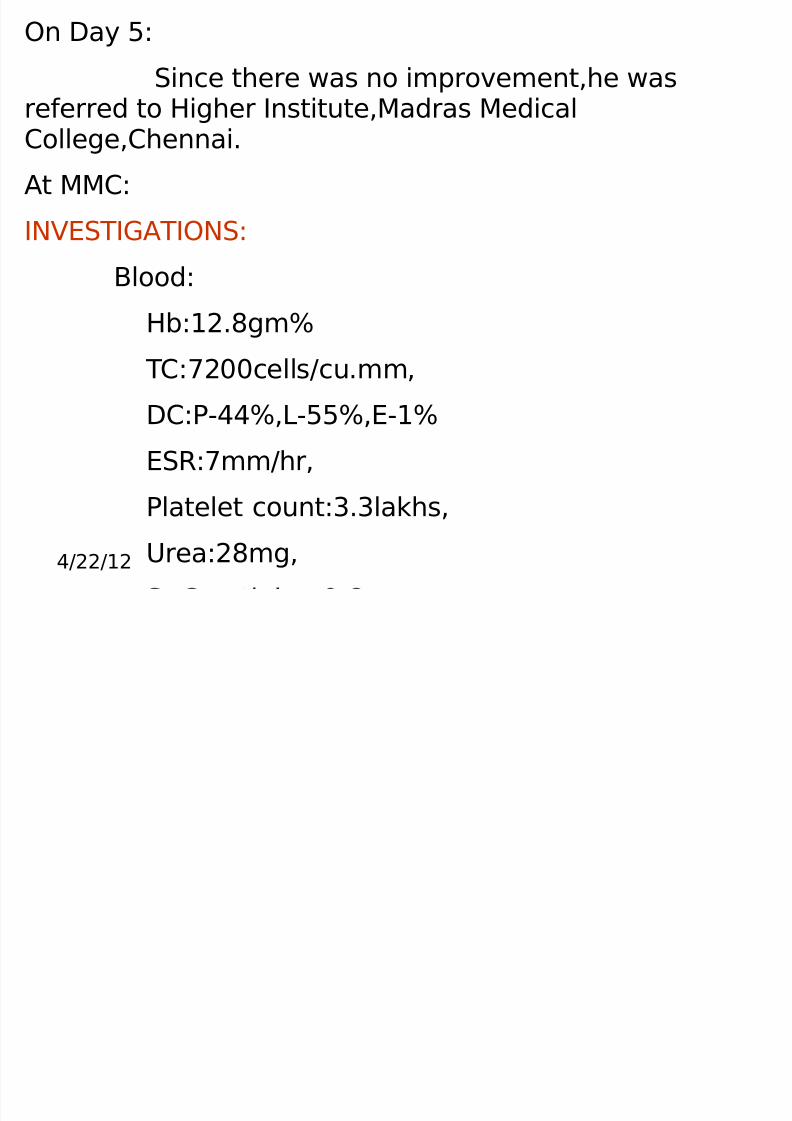
On Day 5:
Since there was no improvement,he wasreferred to Higher Institute,Madras Medical
College,Chennai.
At MMC:
INVESTIGATIONS:
Blood:
Hb:12.8gm%
TC:7200cells/cu.mm,
DC:P-44%,L-55%,E-1%
ESR:7mm/hr,
Platelet count:3.3lakhs,
Urea:28mg,
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 8/18
4/22/12
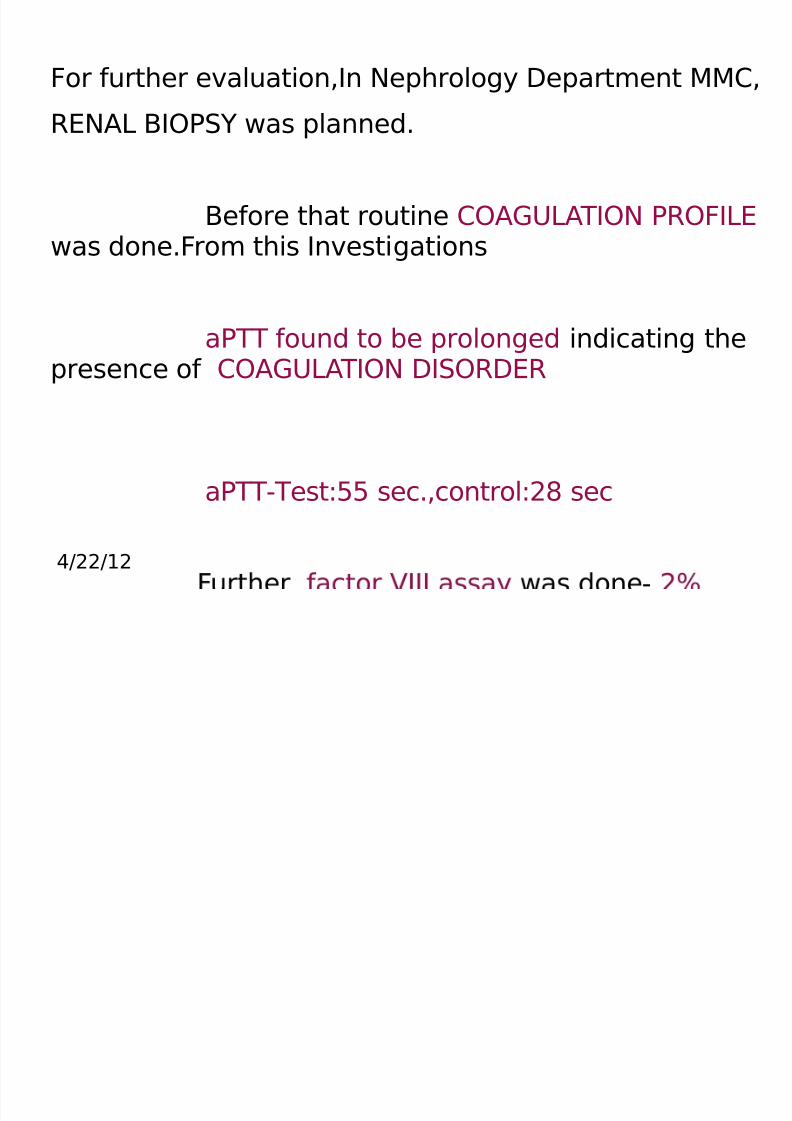
For further evaluation,In Nephrology Department MMC,
RENAL BIOPSY was planned.
Before that routine COAGULATION PROFILE was done.From this Investigations
aPTT found to be prolonged indicating thepresence of COAGULATION DISORDER
aPTT-Test:55 sec.,control:28 sec
-
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 9/18
4/22/12
DIAGNOSIS:
HEMOPHILIA A
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 10/18
4/22/12
Hence Renal Biopsy was deffered,
thus a MAJOR CATASTROPHY wasPREVENTED.
Once the Diagnosis was made,we persuethe case retrospectively and revealed the presence of family history.
Presence of similar illness in his younger brotherwhich was not
revealed during routine history taking at the time of admission.

8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 11/18
4/22/12
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 12/18
4/22/12
CASE DISCUSSION:
CAUSES OF HEMATURIA
MEDICAL CAUSE SURGICALCAUSE
Kidney
General cause Ureter
Disease of Renal Parenchyma Bladder
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 13/18
4/22/12
MEDICAL CAUSES:
GENERAL CAUSES:
Bleeding disorders
Anticoagulant Drugs
Sub Acute Bacterial
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 14/18
4/22/12
DISEASE OF RENAL PARENCHYMA:
Glomerulonephritis
Malignant Hypertension
Polycystic kidney
Renal Vein Thrombosis
Polyarteritis
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 15/18
4/22/12
SURGICAL CAUSES:
KIDNEY:
Wilms Tumor
Hypernephroma
Papilloma of Renal Pelvis
Hemorrhage into:hydronephrotic
kidney,renal cyst injury
URETER:
Stone
BLADDER
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 16/18
4/22/12
BLADDER:
Acute cystitis
Stone
Papilloma
Carcinoma
Trauma PROSTATE:
Tubercular prostatitis
Bleeding prostatic venous plexus URETHRA:
Trauma
Angioma
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 17/18
4/22/12
TAKE HOME MESSAGE:
This case illustrates the IMPORTANCE
OFROUTINE SCREENING of the individual before
any Invasive Diagnostic Procedure to preventserious complications.
A major part of DIAGNOSIS also relieson the HISTORY GIVEN BY THE PATIENT,so we
should try our level best to GET COMPLETEHISTORY from the atients.
8/3/2019 Safrin Hemophilia
http://slidepdf.com/reader/full/safrin-hemophilia 18/18
4/22/12 THANK
YOU





























