Embed Size (px)
Citation preview

HIP AND THIGHCommon Injuries

STRAINS Quad, Hip Flexor, and
groin strains commonly occur from explosive movement
c/o “popping” or “pulling” feeling. Typically athlete can not continue activity. Strains that RTP too soon,
or are left untreated with RTP can result in avulsion fx
Signs and Symptoms Pain, swelling, decreased ROM secondary to pain
Treatment Rest, ice, ROM activities, electrical stimulation
for tissue regeneration, Progressive Resistive Strength Training

CONTUSIONS
Quadriceps Contusion - Results from a traumatic or repetitive impact to a
relaxed quad muscle, compressing the muscle against the femur

Quadriceps Contusion Cont’d Signs and Symptoms –
Pain, temporary loss of function, capillary bleeding, swelling, pain to the touch
Treatment – Immediately placed in flexion to stretch the
muscle (to prevent shortening), with ice pack to minimize swelling/bleeding and moderate pain. RICE and NSAIDs prescribed as needed
ROM (mild stretching), WBAT, and PRE within pain free ROM Heat, aggressive massage, and ultrasound are all
contraindicated

Hip Pointer – Occurs from a
blow to an inadequately protected hip (iliac crest and abdominal musculature)
Considered one of the most debilitating and hard to manage injuries in contact sports.
Hip pointer cont’d Signs and Symptoms –
Immediate pain, spasms, temporary paralysis of muscles. As a result, Ath is unable to rotate trunk, or flex the thigh without pain.
Treatment – RICE Ice cup massage Initially, steroid injection to manage pain,
followed by oral NSAIDs Recovery 1 to 3 wks
MOI is same as Iliac crest fx, Ath must be seen for Xray to RO

MYOSITIS OSSIFICANS
Occurs from a severe blow or repeated blows to quadriceps muscle. Failure to control initial
bleeding from quad contusion, or tx that it too aggressive can produce calcification in the muscle.
Signs and Symptoms – Pain, weakness, soreness,
swelling, decreased ROM Treatment –
Sx excision 1 yr post injury.

FEMORAL FRACTURE
Acute – Occurs in middle aged athletes, and elderly
patients. Osteoporosis is a pre-disposing condition High incident of Avascular Necrosis in adolescent
patients due to skeletal immaturity and inadequate blood supply
Fx w/o obvious deformity: c/o pain, no ROM, inability to WB. Ath is muscle-gaurding and resists any attempts to be moved. Hip is often EXTERNALLY rotated and slight adducted. Shortening of the limb is sometimes evident.

FEMORAL FX
http://www.youtube.com/watch?v=rO_nSjF_Jl0

FEM FX CONT’D
FEM FX CON’T
Treatment – Immobilized and transported for immediate
medical care. Physician will either do a close reduction, or open reduction, depending on placement of fracture and number of fracture sites. ORIF (open Reduction Internal Fixation) requires pins
and rods Following surgery, ath will be immobilized in
hinge brace and will require PT. Rehabilitation typically takes 4 months

FEM FX CON’T
Stress fracture Fairly uncommon, occurring most often in
endurance athletes, and are more common in FEMALE athletes (MOI Overuse)
Signs and symptoms – Pain in groin or anterior thigh, pain increasing
during activity; pain may be referred to knee. Positive Trendelenburg’s sign. Early x rays may not show fracture.
Treatment – Complete rest with calcium and Vitamin D
supplementation. Untreated stress fx can result in displaced femoral fx, then requiring sx

LEG LENGTH DISCREPANCY
Simply put: one leg is shorter than the other In non-active individuals,
a LLD of 1” will produce symptoms. In highly-active individuals, an LLD of 1/8” will produce symptoms.
3 types: True (Anatomical) Apparent Functional

LLD CONT’D
True: Either Femur or Tibia is shorter when compared bilaterally. In some cases BOTH Femur and Tibia are shorter. To Measure: Ath is supine, measurements taken
from medial malleoli to ASIS
Apparent: Not a true LLD. Bone length is the same when measured. Apparent shortening is caused by pelvic rotation. Can be fixed/treated.
Functional: Deformity in bone causes LLD, such as Genu Valgum/Genu Varum (bow-legged, Pigeon-toed). Can not be fixed. Measurements taken from medial malleoli to umbilicus

Left: Genu Valgum (Knock-kneed)Bottom: Genu Varum (bow-legged)

TROCHANTERIC BURSITISInflammation of the bursae caused by friction from the muscle or tendons surrounding the area.
Signs and Symptoms: c/o P in lateral hip which may radiate down to knee. TTP over greater trochanter. AT must r/o ITB tightness
Treatment: RICE, NSAIDS, ROM, and PRE. Avoid running on inclined surfaces. LLD and female athletes w/ increased Q-angle are more at risk
HIP DISLOCATION
https://www.youtube.com/watch?v=vXLLdU8-jO8
MOI: Traumatic force along axis of femur when knee is flexed. Can displace anteriorly or posteriorly. Posterior
dislocation are more common. Posterior dislocations cause femoral shaft to
adduct and flex


HIP DISLOC CONT’D
Signs and Symptoms: Presents with a flexed, adducted, and internally
rotated femur, extreme pain and no ROM available
Treatment: Immediately reduce by medical professional.
Immobilize and rest for 2 weeks. Use of crutches for ambulation approx 4 weeks
Complications: Serious tearing to capsular ligaments, fracture to
femur (head or neck) Sciatic Nerve damage, later development of osteoarthritis, avascular necrosis of femoral head due to interrupted blood supply

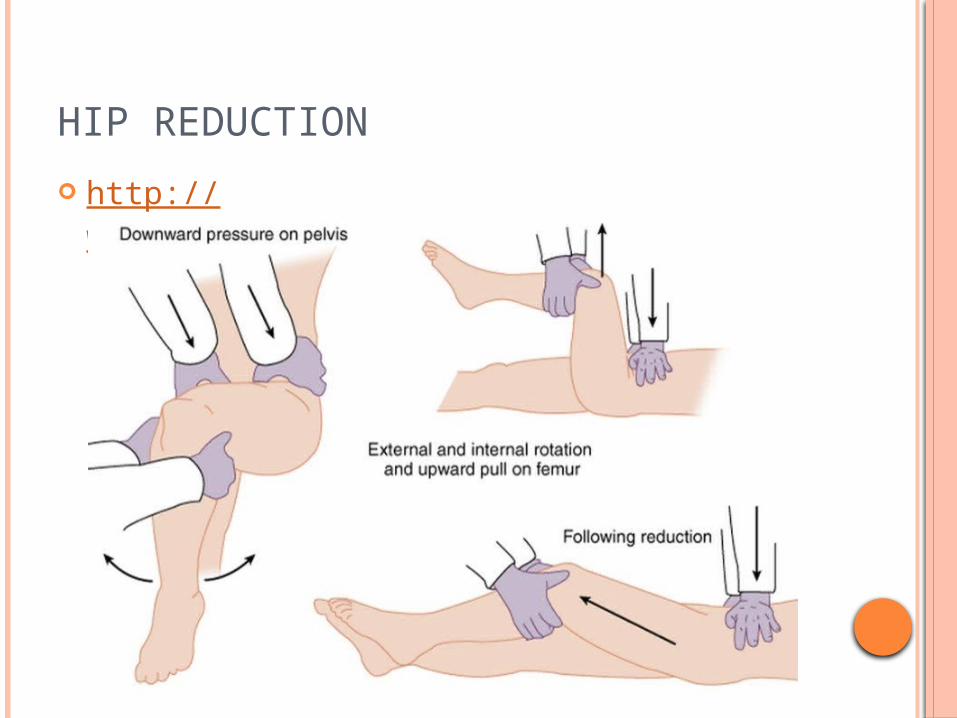
HIP REDUCTION
http://www.youtube.com/watch?v=sGQZaqB48rw

HIP DISLOCATION OVERVIEW
https://www.youtube.com/watch?v=mAL-Szu7qAc
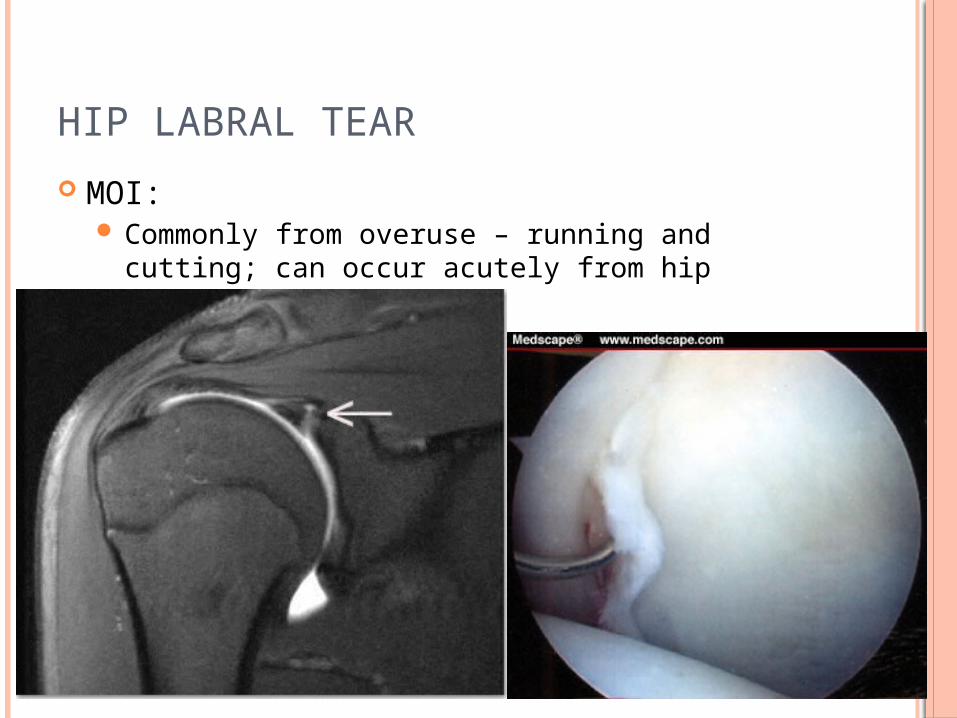
HIP LABRAL TEAR
MOI: Commonly from overuse – running and cutting;
can occur acutely from hip dislocation

HIP LABRAL TEAR CONT’D
Signs and Symptoms Most often asymptomatic. Occasionally: catching,
locking, or clicking, pain in the hip or groin, and feeling stiff or having decreased ROM
Treatment: Hips strengthening and proprioception, avoiding
movements that cause pain, NSAIDs, injections of corticosteriod. If pain persists longer than 4 weeks, sx considered to removed or repair

LEGG-CALVE-PERTHES DISEASE
Avascular necrosis of the femoral head Occurs in boys more than girls Occurs in ages 4 to 10
Etiology not always understood. Trauma only accounts for 25% on cases (femoral fx/hip dislocation)
Signs and Symptoms: Pain in groin, abdomen or knees. Limping is
common. Evaluations will only show limited ROM and pain. MRI/Xray needed

LEG
G-C
ALV
E-P
ERTH
ES
DIS
EA
SE

LEGG-CALVE-PERTHES DISEASE CONT’D
Treatment: Complete bed rest. If treated in time, femoral
head could re-vascularize and re-ossify
Complications: Head of the femur will become ill-shaped and
cause osteoarthritis in the future
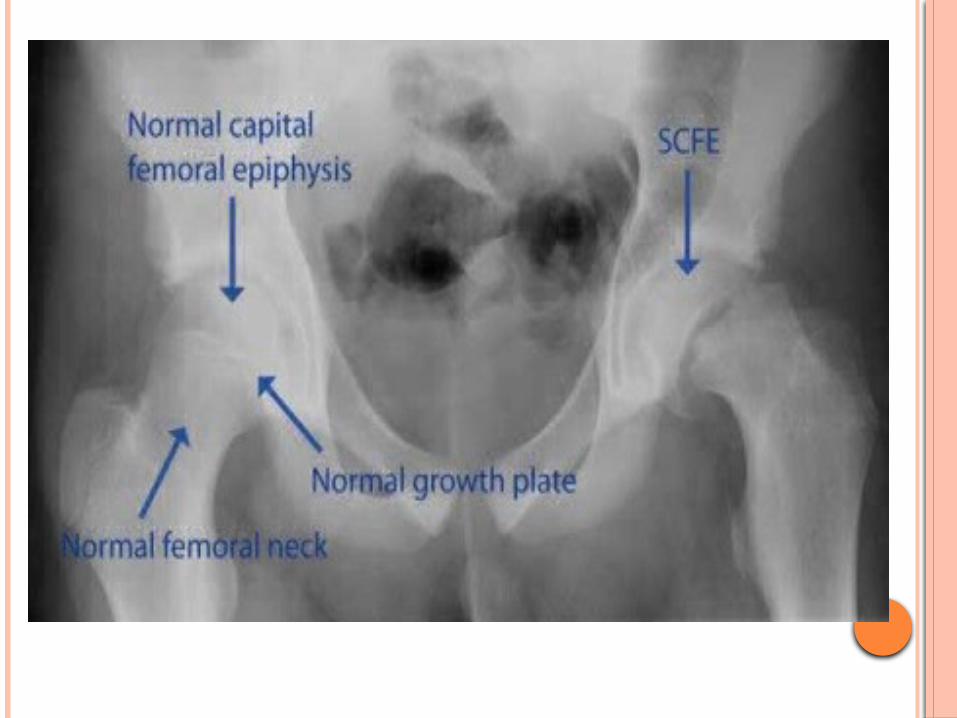
SLIPPED CAPITAL FEMORAL EPIPHYSIS
MOI: idiopathic potentially related to a growth hormone Mostly seen in boys, ages 10-17 Tall and thin, or obese Trauma only account for 25% of cases (femoral
fx/hip dislocation)
Signs and Symptoms: Similar to those of LCP
Treatment: Minor slippage: rest and NWB may prevent further
slippage Major displacement: corrective surgery required
LAST ONE!
SNAPPING HIP SYNDROME
ITB moving over the greater trochanter of the femur Excessive repetitive movements found in
athletes such as dancers, gymnasts, hurdlers, and sprinters – creates a muscle imbalance
Signs and Symptoms: Pain, with a visible “clunk” while patient re-
enacts motion
Treatment: Decrease inflammation and pain with ice,
NSAIDs, stretching and strengtheing
SNAPPING HIP SYNDROME
https://www.youtube.com/watch?v=SUXOqfT2zC4