Embed Size (px)
Citation preview

involvement .
In my new role as GCSHP president, I have the challenge of increasing our membership, especially the pharmacy technician section. The GCSHP Board of Directors has a definite commitment to meet our technician member-ship needs, but we need your involvement in the society to help identify how to best ac-complish this important goal in the upcoming year. I welcome your feedback and look forward to seeing increased involvement for pharmacists and technician members! Up-coming events for our local chapter are also included in this newsletter, so please mark your calendars to attend these educational offerings! GCSHP has a new website that is linked to TSHP website so just go to the TSHP website and click on the GCSHP link.. You can review information on our society, officer information, future events, and newsletters. I am looking forward to meeting the member-ship at upcoming events and welcome your comments ([email protected]) regarding chapter ideas, future program-ming or new opportunities in health-system pharmacy. Please join me in acknowledging the hard work of Monica Robinson Green who truly deserves a very big “Thank You” for volunteering to be our newsletter editor – they continue to be very well done!
Richard Cadle
Happy Spring fellow colleagues and new members! Welcome to our spring newslet-ter intended to provide you with updates within our membership, information on upcoming meetings, and clinical updates for the practicing pharmacist. We had a suc-cessful half-day GCSHP Seminar at Moody Gardens in February 2009 with tremendous speakers. The results from our attendees’ evaluations confirmed they enjoyed their trip to Galveston and gained valuable knowl-edge from the presentations. We also received many great topic ideas for future seminar presentations. On behalf of the GCSHP Board of Directors, I would like to acknowledge all the hard work of our semi-nar committee including Eddie Lee, Monica Green, Ogechi Eshleman, Allison Wilson, Roland Harris, Randall, Dausin, Todd Can-ada, Janeca Malveaux, Gina Beanes, Ashley Scott, Christi Parker, as well as our many pharmaceutical exhibitors for making this an excellent and flawless meeting.
The GCSHP Board of Directors was proud to recognize our annual award winners this year at the Seminar that included the following individuals:
Outstanding Pharmacist – Nicole McMaster-Baxter
Outstanding Technician — Gina Beanes
Outstanding Student – Ann Marie Prazak
Industry Service – Randall Dausin
Please congratulate these recipients for their prestigious professional awards, which were presented in recognition of their contribution to our society and phar-macy community. We are planning to have our new officer installation at our May 28th 2009 continuing education meeting with TSHP President, Todd Canada performing the induction. This will be a tremendous CE program organized by Jennifer Christen-sen, the GCSHP Education Council Chair . It is for preceptors of pharmacy students and pharmacy residents and will focus on preceptor development which is free to GCSHP members. Our new officers to be installed include:
Jennifer Nguyen, Pharm.D.,BCPS Presi-dent elect
Andy Laegeler, Pharm.D. Director
Katy Hanzelka, Pharm.D, BCPS Member-ship Secretary
Our other officers will continue to serve in their positions. Please start thinking now about becoming more involved in your local GCSHP chapter and running for one of our officer or committee positions in the com-ing year. It is a wonderful commitment to your own professional development and an excellent opportunity to work with industry, pharmacists, technicians, residents and students from the Galveston and Houston areas. Remember the way to improve and strengthen our profession is your active
P R E S I D E N T ’ S R E P O R T
Richard Cadle, R.Ph., Pharm.D., BCPS, FASHP
SPRIN
G ISSUE
A P R I L / M A Y 2 0 0 9
G U L F C O A S T S O C I E T Y O F H E A L T H - S Y S T E M P H A R M A C I S T S
I N S I D E T H I S I S S U E :
P R E S I D E N T ’ S R E P O R T
1
C A L E N D A R O F E V E N T S
2
P R E C E P T O R C E P R O G R A M
3
S T U D E N T S E C T I O N
4
R E S I D E N T S E C T I O N
9
P H A R M A C Y R E V I E W
1 1
A N N O U N C E M E N T
CONTINUING EDUCATION FOR PRECEPTORS
Thursday, MAY 28, 2009
5:30 PM
M.D. Anderson Cancer Center
Hickey Auditorium
See page 3 for details!

2
G U L F C O A S T S O C I E T Y O F H E A L T H - S Y S T E M P H A R M A C I S T S
Sun Mon Tue Wed Thu Fri Sat
1 2
3 4 5 7 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23
24
31 25 26 27 28 29 30
May 2009
SUN MON TUE WED THU FRI SAT
1 2 3 4
5 6 7 8 9 10 11
12 13 14 15 16 17 18
19 20 21 22 23 24 25
26 27 28 29 30
April 2009 S C H E D U L E
⇒ April 16-19, 2009
61st TSHP Annual Seminar
⇒ May 10, 2009
Mother’s Day
⇒ May 16, 2009
TSU/UH Graduation!!!!!!
⇒ May 28, 2009
Preceptor CE

3
C O N T I N U I N G E D U C A T I O N F O R P R E C E P T O R S M A Y , 2 8 , 2 0 0 9
E D U C A T I O N A L G O A L :
P R O V I D E P R E C E P T O R S I N A V A R I E T Y O F S E T T I N G S W I T H T O O L S T O E N H A N C E T H E I R A B I L I T Y T O E D U C A T E S T U D E N T S O F P H A R M A C Y .
E D U C A T I O N A L O B J E C T I V E S :
I D E N T I F Y U N I Q U E C H A R A C T E R I S T I C S O F S M A L L H O S P I T A L S A N D A C T I V I T I E S T H A T A D D D I V E R S I T Y A N D C H A L L E N G E T O R O -T A T I O N S
• Describe how effective preceptors, learners and patients benefit from the rotation experience
• Design a strategy to individualize the learning experience to the student’s knowledge and experience
• Describe the difference between feedback and evaluation and apply the R.I.M.E. tool to facilitate feedback
• Understand your teaching style and how to adapt teaching styles to student learning preferences
• Recognize key elements of a meaningful evaluation, and tools available to prepare meaningful evaluations
P R O G R AM :
E V A L U A T I N G Y O U R E V A L U A T I O N S : S T E P S F O R P R E P A R I N G M E A N I N G F U L S T U D E N T A P P R A I S A L S
Dr. Susannah Koontz 156-999-09-027-L04-P 0.5 contact hours (0.05 CEU’s)
Customizing the learning experience
Dr. Steven Pass 156-999-09-028-L04-P 0.5 contact hours (0.05 CEU’s)
Challenges and opportunities with student rotations in small hospitals
Dr. Sharon Brown 156-999-09-036-L04-P 0.5 contact hours (0.05 CEU’s)
Practical tips for providing learners with feedback on clinical rotations
Dr. Michael Liebl 156-999-09-037-L04-P 0.5 contact hours (0.05 CEU’s)
Assessing student learning preferences and adapting preceptor teaching styles
Dr. Todd Canada 156-999-09-038-L04-P 0.5 contact hours (0.05 CEU’s)
Effective precepting: a win-win relationship for all
Dr. Jeffrey Bryan 156-999-09-039-L04-P 0.5 contact hours (0.05 CEU’s)
RSVP no later than 12pm, Monday, May 11, 2009 to [email protected]. Only one person may RSVP per email. RSVPs for groups of people will not be accepted.
Continuing education credits will be provided to GCSHP members at no charge. A $40 fee will be assessed at the door for non-GCSHP members (this includes GCSHP membership).
To receive a certificate of attendance, a program evaluation form must be completed, signed, and returned to the registration desk at the end of the program. A certificate will be mailed within 30 days of the program.
The Texas Society of Health-System Pharmacists is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. This pro-gram provides a total of 3.0 contact hours (0.3 CEUs) of continuing pharmaceutical education for pharmacists. This program has been reviewed by the Joint Committee on Internship Programs and has been designated as preceptor education and training for Texas preceptors.
Location:
Hickey Auditorium
(Main building - elevator B to 11th floor) M.D. Anderson Cancer Center
1515 Holcombe Blvd
Time:
5:15 GCSHP Officer Installation
5:30 CE Program
8:30 Program conclusion
Box lunch will be provided

4
2009. A total of six TSU SSHP student members represented the pharmacy department during the student poster session on Monday, March 31: Joyce Forlemu, Allyson Davis, Linda Ho, Abigail Okeke, Ashley Scott and Candice Wig-gins. Research Week is an opportunity for both faculty and staff to present their year’s research and progress to other faculty, staff, administrators, students and visitors of the entire TSU commu-nity. Last year only three students pre-sented during the 2008 Research Week and we have increased our numbers of participating student members. TSU SSHP is very proud of all student mem-bers who have shown an interest in health-system pharmacy and have chosen to explore its many options.
On April 13, 2009, the chapter visited Dodson Elementary for the TSHP Antibiotic Awareness Project. The project was initiated by the TSHP Student Section Executive Committee (SSEC) where TSU SSHP members Pam Dyer, Candice Wig-gins and Ashley Scott serve as TSU repre-sentatives. Chapter members shared information to all 5th grade classes on
It has been an exciting and busy Spring semester for Texas Southern University’s SSHP!
One of the chapter’s highlights thus far was the clinical skills competition held on campus in March. A total of six teams made up of second, third and fourth year students competed in the Spring 2009 Clinical Skills Competition on TSU COPHS campus. The event was separated into two phases: 1) the written “pharmacist’s care plan” and 2) the oral presenta-tion. Students were able to participate in hopes of receiving proper feedback from the judges to prepare them for the 61st TSHP Annual Seminar Clinical Skills Com-petition. The TSU COPHS competition was a great opportunity for students to also increase their presentation skills. The first place winners of the TSU SSHP Spring 2009 competition were third year students Regina Ramirez and Sania Sul-tan. The TSU chapter would like to recognize student members that participated in the 2009 TSU Research Week held on campus during the week of March 31 – April 6,
bacterial vs. viral infections, how to properly wash hands, stressed the importance of appropriate antibiotic use and storage and the role of their pharmacist. Goodie bags were given to the elementary students that also contained pamphlets, flyers for parents and magnets that were designed and created by the TSHP SSEC. Members of two other student organizations, TSU SNPhA and Phi Delta Chi, joined TSU SSHP in the event to educate on the importance of vaccinations and smoking cessation. This community service event became a wonderful opportu-nity for pharmacy student organizations at TSU to come together and work as a team to educate younger generations.
Four teams of students represented TSU COPHS at the 61st TSHP annual seminar in the Clinical Skills Competition and three students also competed in the Disease State Manage-ment Competition. We also participated in the TSHP SSEC Teddy Bear Drive and col-lected teddy bears for a children’s hospital which were given during the weekend of the seminar.
Ashley Scott
T E X A S S O U T H E R N U N I V E R S I T Y S S H P
A S H L E Y S C O T T , P R E S I D E N T
American Diabetes Association Super Power Event
Sunnyside Multi-Service Center
TSU and UH participate in the ADA Super Power Event at the
Sunnyside Multi-Service Center
TSU students assist with Blood Pressure
checks and Blood Glucose screenings

5
TSHP Antibiotic Awareness Project
April 13, 2009
Dodson Elementary
TSU SSHP
TSU-SSHP
Jamilla Hicks (pre-pharm)
Arezo Noormohammadi (P3)
Frank North (P3)
Ashley Scott (P3)
Thu Pham (P3)
Dodson
Elementary
students
demonstrating
how to properly
wash their hands
Antibiotic
Awareness
Lessons for
children at
Dodson
Elementary
by Arezo
Noormohammadi
Jimella Hicks
Frank North
Ashley Scott
Future
Pharmacists
At
Dodson
Elementary
1st place TSU
Clinical Skills Competition Winners
Spring 2009
Sania Sultan (P3) Regina Ramirez (P3)

6
Hospital Administration - Perry Flowers, RPh, MS, Memorial Hermann Hospital
Ambulatory Care - Monica Robinson-Green, PharmD, BCPS, Harris County Hospital District - Acres Home Health Center
Solid Organ Transplant - Rebecca Benslar, PharmD, RPh, St. Luke’s Episcopal Hospital
Cardiology - David Putney, PharmD, The Methodist Hospital
The GCSHP annual seminar was a great success and incredibly student-focused by featuring a career panel for students which included practitioners in nuclear pharmacy, ambulatory care, critical care/nutrition support, and investiga-tional drugs.
This semester, our chapter has been promoting World TB Day which took place on Tuesday, March 24, 2009. This cam-paign has a special place in Amy Moss, our President-elect’s heart. UH-SSHP set up at the UC-Satellite on the UH Main Campus to hand out fact sheets and festive World TB Day cookies. This was a great opportu-nity for pharmacy students to promote
The Spring 2009 semester has been a busy one for the University of Houston SSHP chapter.
The semester began with the very suc-cessful UH-TSU SSHP Fourth Annual Residency Mentoring Social on Thursday, January 22, 2009 from 5:00 – 8:00 PM at the UH Alumni Center O’Quinn Great Hall. Dr. Ryan Roux from the Harris County Hospital District was our keynote speaker for the night. Local residency programs and student members were invited to enjoy a catered meal and a keynote ad-dress. Students also had the opportunity to speak with residents and program directors from Houston area residency programs. The event was made possible by the generous financial support of GCSHP.
Practitioners who have been extremely supportive of our chapter by taking time out of their schedules to speak at our Main Campus meetings this semester included:
Organizational Involvement - Todd Canada, PharmD, BCNSP, FASHP, University of Texas MD Anderson Cancer Center
awareness, celebrate people who had been cured, and support those who were currently undergoing treatment.
During the month of March, before the 61st TSHP annual seminar, we held the well-known Teddy Bear Drive at both the UH Main Cam-pus and Texas Medical Center Campus to donate new stuffed animals to a local chil-dren’s hospital in the city which the seminar takes place. Approximately 16 students from the University of Houston competed in the clinical skills competition at the seminar. Allison Palmer (P3) and Christi Parker (P3) took first place in the competition, and Con-nie Reyes (P4) and Aimee Hammerstrom (P4) took second. Students also participated in the disease state management competition. Both Aimee Hammerstrom (P4) and Allison Palmer (P3) took honorable mention awards in the competition.
We would also like to congratulate all fourth-year pharmacy students who successfully matched to their desired residency program. We hope that you enjoy your time as a PGY1 Resident at your institution.
Christi Parker
U N I V E R S I T Y O F H O U S T O N S S H P
C H R I S T I P A R K E R , P R E S I D E N T
American Diabetes Association Super Power Event
Sunnyside Multi-Service Center
TSU and UH students participate in the
ADA Super Power Event at the Sunnyside Multi-Service Center
UH assist with blood glucose screenings

7
UH-TSU SSHP
4th Annual Mentoring Social
UH Alumni Center

8
Pamela Dyer-Price, PharmD Candidate 2009
Texas Southern University College of Pharmacy & Health Sciences
Michael E DeBakey VA Medical Center VALOR Student
Hepatitis B Immune Globulin (HBIG) in Liver Transplantation
In November 2007, the Micheal E. DeBakey V.A. Medical Center began offering liver transplantation services. Since inception, a total of six liver transplan-tations have been performed. This article reviews Hepatitis B Immune globu-lin (HBIG) for the prevention of hepatitis B recurrence following liver trans-plantation.
Hepatitis B (HBV) is a virus transmitted by blood and blood-derived fluids, and is one of the most common causes of hepatitis, cirrhosis, and hepatocel-lular carcinoma. It is estimated that 800,000 to 1.4 million people in the US have hepatitis B infection. For patients with HBV-induced liver failure, liver transplantation is a viable treatment option. HBV-induced liver disease accounts for 5-10% of all liver transplantations.
Without preventative intervention, there is an approximately 80% risk for HBV recurrence of the transplanted liver (graft) because the virus can still be present within the body. Hepatitis B surface antigens (HBsAg) and HBV DNA are markers for HBV. Patients positive for these markers are at risk for HBV recurrence. In addition to pre- and post-operative oral antiviral medications, HBIG is used to prevent the recurrence of HBV post-transplantation in HBsAg positive patients. HBIG is prepared from plasma donated by individuals with high titers of antibodies to HBsAg. Several stud-ies have confirmed the role of HBIG in preventing graft HBV infection. HBIG administration has become the standard of care at transplant centers worldwide. Research also supports long-term intravenous administration of HBIG.
The intramuscular HBIG preparation can be diluted in normal saline and infused intravenously (IV), usually over 4 hours. At the time of transplanta-tion, HBIG, dosing typically consists of 10,000 units IV, then 10,000 units IV daily for the first six days following the surgery. As determined by monthly to bimonthly hepatitis B surface antibody (anti-HBs) titer results, 10,000 units is administered IV every one to two months, with the goal of keeping HBsAg and HBV DNA negative and the anti-HBs titers greater than 300 mIU/MI. Pre-medication with acetaminophen and diphenhydramine can reduce adverse effects during and immediately following the infusion, such as myal-gia, back pain, skin rash, nausea, headache, hypotension, fever, chills, and tremors. However, HBIG is generally well tolerated, with mild adverse reac-tions. Long-term treatment with HBIG is expensive. Cost-effective strate-gies are being evaluated to determine potential alternatives to indefinite HBIG IV administration.
For more information, please contact Pamela Dyer-Price at [email protected] or Dr. Shelia Sandberg at [email protected]
Maggie Dinh, PharmD Candidate 2009
University of Texas College of Pharmacy
Immediate, extended and sustained-release niacin:
Differences in side effect profiles
Niacin, or nicotinic acid, is a popular drug used in dyslipidemia. Niacin raises
high-density lipoprotein (HDL) cholesterol by 15-35% which is more than the
HMG CoA-reductase inhibitors (statins), bile acid sequestrants, or fibrates.
In addition, it also lowers low-density lipoprotein (LDL) cholesterol and
triglycerides.1 Niacin has been used since the mid-1950’s and is available
over-the-counter as well as by prescription.2
There are three different formulations: immediate-release (IR), sustained-
release (SR), and extended-release (ER). The immediate-release form is
available by prescription (Niacor®) and over-the counter and is FDA-
approved for dyslipidemia. The disadvantages of this formulation are that it
needs to be administered two or three times daily and also has a higher
incidence of cutaneous flushing than the other formulations. The sustained-
release form is available over-the-counter (non FDA-approved, sold as a
dietary supplement). The SR version has a decreased incidence of cutaneous
flushing, but was later found to have higher incidences of hepatotoxicity and
gastrointestinal intolerance. The last formulation is the extended-release
niacin (Niaspan®) which is available by prescription only and is FDA-
approved for dyslipidemia. The ER version has a dissolution rate in between
that of IR and SR and has a better tolerability and side effect profile.2
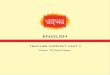
The cutaneous flushing and hepatotoxicity seen in certain formulations of
niacin are related to its dissolution rates and metabolic pathway. Niacin has
two different metabolic pathways: the amidation pathway, and the conjuga-
tive pathway. The amidation pathway is a high-affinity, low-capacity pathway
and produces nicotinamide and pyrimidine metabolites which are responsible
for the hepatotoxicity seen with SR niacin. The conjugative pathway on the
other hand, is a low-affinity, high-capacity pathway. It is used only when the
amidation pathway is saturated and produces nicotinuric acid which is asso-
ciated with vasodilation and flushing and is responsible for the adverse
effects seen with IR niacin.2
Percentages of niacin going through each metabolic pathway
It is important for pharmacists to know the different formulations of niacin
that are available and counsel patients on the different adverse effects that
can occur with each one. For the immediate-release formulation, taking
aspirin 45-60 minutes before niacin, avoiding hot liquids with niacin admini-
stration, and taking niacin in divided doses with small meals can reduce the
cutaneous flushing.2
References
McKenny J. Niacin for dyslipidemia: Considerations in product selection. Am J Health-
Syst Pharm 2003; 60:995-1005.
Pieper JA. Overview of niacin formulations: Differences in pharmacokinetics, efficacy,
and safety. Am J Health-Syst Pharm 2003; 60:S9-S14.
0% 50% 100%
SR
ER
IR
Amidation
Conjugation

9
Carrie Shuman, PharmD Pharmacy Practice Resident
Harris County Hospital District
Post-Cardiac Arrest Therapeutic Hypothermia: The Pharmacist’s Role
After return of spontaneous circulation (ROSC) in patients experiencing sudden cardiac arrest, anoxic brain injury can persist for several hours and is an important cause of morbidity and mortality in patients who are resusci-tated1. In an attempt to reduce injury caused by the generation of free radicals, induced therapeutic hypothermia has been a proposed means to reduce oxygen demand and improve neurologic outcomes in these patients1,2. The Hypothermia After Cardiac Arrest (HACA) Study Group conducted a multicenter, randomized, controlled trial in which 275 patients were random-ized to receive normothermia or hypothermia, with cooling to 32-34°C for 24 hours, after ROSC following ventricular fibrillation. A greater proportion of patients receiving treatment with hypothermia had a favorable neurologic outcome, as defined by a Pittsburgh cerebral-performance score of 1 or 2 (39% normothermia vs. 55% hypothermia; p = 0.009). Additionally, fewer patients receiving hypothermia died when compared to patients in the nor-mothermia group (56 and 76 patients, respectively; p = 0.02). Based upon the results of this trial, as well as an additional study conducted in a similar population1, the American Heart Association recommends the use of thera-peutic hypothermia in adult patients who experience ROSC after out-of-hospital ventricular fibrillation cardiac arrest3.
While therapeutic hypothermia potentially improves the neurologic outcome and mortality of patients experiencing cardiac arrest, there are several pharmacologic and physiologic factors that must be managed throughout the cooling process. Neuromuscular blocking agents are often utilized during cooling to prevent shivering. Shivering will increase metabolic heat produc-tion, resulting in increased cooling time, oxygen demand and carbon dioxide production4. Although it is essential to prevent shivering in order to ade-quately cool the patient, it is important to recognize that lowered core body temperatures will alter the pharmacokinetics of most medications. Caldwell and colleagues conducted a trial in healthy volunteers utilizing vecuronium, in which they found the clearance to be reduced by 11.3% for every 1°C re-duction in body temperature. Additionally, there was an inverse relationship between the core body temperature and the duration of action of the medi-cation (i.e. the lower the temperature, the longer the duration of action)5. Because hypothermia reduces the metabolic processes of the body, this principle should be considered for all medications utilized during hypother-mia, not exclusively the neuromuscular blocking agents.
Therapeutic hypothermia is a complex process that requires intense moni-toring by various members of the healthcare team, including a pharmacist. Pharmacists play a vital role in monitoring for and preventing toxicities that may be caused by altered pharmacokinetics of the various medications utilized throughout the hypothermic period. In addition to altering the phar-macokinetics of medications, hypothermia also causes variations in the body’s natural physiologic processes. Although there are multiple physiol-ogic changes that take place, there are specific areas of potential interven-tion by the pharmacist, such as management of hyperglycemia, electrolyte imbalances and infection control.
Hyperglycemia is usually present after cardiac arrest, which is further perpetuated by hypothermia3. In patients experiencing ROSC post-cardiac arrest, it is important to manage hyperglycemia, as it has been shown to be associated with worsened neurologic outcomes and increased mortality6. In order to maintain tight blood glucose control, patients will often require an insulin drip. While tight glucose control is the goal, it is imperative to keep inmind that the signs and symptoms of hypoglycemia will be masked by the administration of neuromuscular blocking agents, sedatives and the hypo-thermic process. For these reasons, the blood glucose must be frequently and closely monitored.
Electrolyte abnormalities will also usually present with the induction of hypothermia due to an increase in diuresis. This will result in the global depletion of potassium, magnesium, calcium and phosphorus. Very few randomized, controlled clinical trials have been conducted to evaluate how and when electrolyte replacement should occur in this patient population. Animal models of post-cardiac arrest support have shown that maintaining normal levels of magnesium can prevent further neurologic injury, which is the ultimate goal of the therapeutic hypothermia process. It is desirable to maintain potassium levels in the lower range of normal because once the rewarming process begins, potassium will shift extracellularly and poten-tially lead to hyperkalemia if not appropriately managed. Once the rewarm-ing process begins, it is crucial to ensure that all potassium supplementa-tion, including IV fluids, have been discontinued4.
A final physiologic effect of therapeutic hypothermia in which a pharmacist could assist in monitoring and managing is the risk for infection. During hypothermia, immune system function is impaired and the release of pro-inflammatory cytokines is inhibited. The risk of infection is further increased by the presence of hyperglycemia during the post-cardiac arrest period. Two randomized clinical trials have evaluated the risk of developing an infec-tion in patients undergoing post-cardiac arrest therapeutic hypothermia. The HACA study group reported that a higher proportion of patients in the hypothermia group developed an infection when compared to patients in the normothermia group (37% vs. 29%; p = NS)2. In contrast, a similar study conducted by Bernard and colleagues indicated that no clinically significant infections developed in either group1. Although the inconsistency observed between the two studies may be attributed to differences in the duration of hypothermia or follow-up, controversy exists on how to properly address the risk of infection in patients receiving therapeutic hypothermia. Some clini-cians feel that prophylactic antibiotics should be administered during the hypothermic period, while others believe that an infection should be treated upon development. Regardless of the option chosen, when assessing the risk of or monitoring for the development of infection, one should consider that the usual clinical manifestations of infection will not be reliable while the patient is hypothermic. For example, it will not be possible to determine if the patient has been febrile and the white blood cell count will not be an accurate indication of immune response4.
Although post-cardiac arrest therapeutic hypothermia is not yet common practice, it is slowly gaining support. As more institutions utilize therapeutic hypothermia, there will be an increasing opportunity for the pharmacist to develop protocols that ensure the discontinuation of potassium supplemen-tation, ensure the proper dosing of medications, monitor for toxicities caused by the altered pharmacokinetics of medications, manage hyperglyce-mia and electrolyte imbalances and provide therapeutic recommendations for the prevention of infection.
References
Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors with out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002;346:557-63.
The Hypothermia After Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002;346:549-56.
Part 7.5: Postresuscitation Support. Circulation 2005;112:IV84-8.
Arpino PA, Greer DM. Practical Pharmacologic Aspects of Therapeutic Hypothermia After Cardiac Arrest. Pharmacotherapy 2008;28:102-11.
Caldwell JE, Heier T, Wright PM, et al. Temperature-dependent Pharmacokinetics and Pharmacodynamics of Vecuronium. Anesthesiology 2000;82:84-93.
Mullner M, Sterz F, Binder M, et al. Blood Glucose Concentration After Cardiopulmon-
ary Resuscitation Influences Functional Neurologic Recovery in Human Cardiac Arrest
Survivors. J Cereb Blood Flow Metab 1997;17:430-6.

10
Rina Patel, Pharm.D.
Pharmacy Practice Resident
Michael E DeBakey VA Medical Center
Diabetes and Herbal Supplements
Herbal supplements are plants or parts of plants used for their scent, flavor and/or therapeutic properties. However, herbal supplements are not with-out risk. The active ingredients of herbal supplements are often unknown, and one herbal supplement can contain multiple active ingredients. Another problem associated with herbal supplements include that studies regarding safety, efficacy and quality are not required by the FDA before a supplement is marketed.
Patients with diabetes are 1.6 times more likely to use herbal supplements than those without diabetes, and as the incidence of diabetes increases, the use of herbal supplements for the treatment of diabetes also increases. Despite this, the American Diabetes Association does not support the use of dietary supplements due to the lack of long-term safety and efficacy trials.
Four herbal supplements that may have a potential role in diabetes and have clinical studies supporting or rejecting their use include: ivy gourd, ginseng, fenugreek and cinnamon. Ivy gourd’s possible mechanism of action (MOA) is insulin-mimetic, and 1800 mg tablets of dried ivy gourd leaves have been studied. Ginseng is thought to have multiple MOA, including delaying gastric emptying, increasing glucose transport and uptake, increasing glycogen storage and modulating insulin secretion. Multiple dosage forms have been studied, including 100-200 mg tablets of dried leaves and 1 g capsules of ginseng extract taken three times daily. Fenugreek’s possible MOA include delaying gastric emptying, slowing carbohydrate absorption and increasing peripheral glucose utilization. Like ginseng, multiple dosage forms of fenu-greek have been used in studies including 1 g capsules of extract and 50 g of defatted powder baked into bread. Finally, cinnamon is thought to be insulin-mimetic and may enhance glucose uptake. Studies have used both powder (1, 3, 6 g) and 112 mg extract capsule formulations taken three times daily.
Data from clinical trials suggests that these herbal supplements may have a possible effect in lowering BG (blood glucose) levels in diabetic patients. However, one limitation of studies regarding herbal supplements is that baseline fasting BG levels and A1C are rarely provided. Also, studies are limited by small sample sizes and short trial durations, which may not allow adequate assessment of long-term adverse effects and effects on A1C.
Several other herbal medications have been found to have effects on BG. Some herbals that may raise BG include: angelica root, devil’s claw, ginseng, licorice and ma huang. Herbals that may lower BG include: aloe vera, cinna-mon, fenugreek, fig leaf, garlic, ginger, ginseng, gurmar, holy basil, ivy gourd, milk thistle, nettle, nopal or prickly pear cactus, sage and vanadium. The use of antidiabetic agents with herbal supplements that are thought to lower BG is not recommended as this can increase the likelihood of hypoglycemia.
More research is needed to establish the safety and efficacy of herbal sup-plements in the treatment of diabetes. As healthcare professionals, pharma-cists should be aware of the available data supporting or rejecting the use of various herbal supplements in diabetes to be able to relay this information to their patients.
For a complete list of references or more details regarding herbal supplement studies, email Rina Patel at [email protected].
Daina Wells, Pharm.D.
Pharmacy Practice Resident
Michael E. DeBakey VA Medical Center
Acromegaly: Treatment for a Rare Disease
On August 31, 2007 the FDA approved Somatuline depot (lanreotide acetate injection) for the long-term treatment of acromegaly in patients who have failed treatment with or who are not candidates for surgery and/or radia-tion therapy.1
Somatuline depot acts by lowering the levels of growth hormone and insulin-like growth factor in the body.1 Somatuline depot should be injected at 4 week intervals for 3 months via the deep subcutaneous route in the buttock.3 Side effects seen with Somatuline depot include diarrhea, gallstones, skin reactions such as itching, slow heart rate, and changes in blood sugar.1
Acromegaly is a syndrome caused by excessive secretion of growth hor-mone, which acts through insulin-like growth factor.2 Excessive secretion is most commonly caused by a benign tumor in the pituitary gland.1 The mani-festations of acromegaly most noticeably include enlargement of the hands, feet, and facial bones, but can also include the overgrowth/enlargement of many tissues such as skin, connective tissue, cartilage, and vital organs.2
Acromegaly affects approximately 15,000 people in the United States and Canada and is most commonly diagnosed around age 40-45.1,2 Due to the slow onset and progression of the syndrome, the interval from the onset of symptoms until diagnosis is usually about 12 years.2 Acromegaly has been known to reduce life expectancy by 5 to 10 years.1
References
U.S. Food and Drug Administration. FDA News. FDA Approves New Drug to Treat Rare Disease, Acromegaly. Available at: http://www.fda.gov/bbs/topics/NEWS/2007/NEW01692.html. Accessed September 10, 2007.
Melmed S. Clinical manifestations of acromegaly. UpToDate online. Available at: http://www.utdol.com/utd/content/topic.do?topicKey=pituitar/6039. Accessed September 10, 2007.
U.S. Food and Drug Administration. Highlights of prescribing information, Somatuline Depot (lanreotide) injection. Available at: http://www.fda.gov/cder/foi/label/2007/022074lbl.pdf. Accessed September 10, 2007.
HealthSystemCE.org
The e-learning center for
Health-System Pharmacy
Society Members!!!!
Easy Access to home study pro-grams!!!!

11
Kimthy Phung, Pharm.D. Autumn Shuler, Pharm.D. Resident Aspen Wall, Pharm.D. Resident
Michael E. DeBakey VA Medical Center
CHEST GUIDELINES 2008 The American College of Chest Physicians publishes guidelines on antithrombotic and thrombolytic therapies every 3 to 4 years. The 8th Edition was pre-sented in the CHEST Journal Supplement June 2008. Several significant changes were made to the guidelines since its last publication in 2004. With respect to vitamin K antagonists (VKAs), the indications and International Normalized Ratio (INR) goals remain essentially the same with more details on specific cases and exceptions, permitting the clinician to individualize therapy. For example, with idiopathic deep-vein thrombosis (DVT), oral anticoagulation may be extended to long term therapy and the INR goal may be lowered to a range 1.5 to 1.9, allowing for less frequent monitoring. In the case of mechanical prosthetic valve with an embolic event despite anticoagulation, the INR goal may be increased to a range of 3.0-4.0 or 3.5-4.5 from the previous goal of 2.5 to 3.5. In this population, aspirin may also be added, except in patients with high bleeding risk or age > 80. Also of note, the dose of aspirin has been lowered to 81 mg across the board. Regarding the management of elevated INR’s, the recommendations remain the same with the exception of the dose lowering of vitamin K. For example, in patients with mild to moderately elevated INRs without major bleeding, vitamin K1 should be given orally rather than subcutaneously. Furthermore, in patients with INR >5 but <9, with no significant bleeding, a clinician may choose to omit one or two doses, monitor more frequently and resume at lower dose when INR is therapeutic, or omit one dose and give oral vitamin K1 (1-2.5mg). The guidelines also suggest the use of daily low-dose vitamin K (100 to 200mcg) for pa-tients receiving long term warfarin therapy with variable INR response not attributable to any usual known causes. Perhaps the most exciting aspect in the new CHEST guidelines is the specific recommendations for perioperative management of antithrombotic therapy. For the first time, an entire chapter is devoted to this topic. With a re-emphasis of the CHADS2 (congestive heart failure, hypertension, age>75, diabetes, and prior transient ischemic attack or stroke) score, risk stratification is more defined and systematic. Using some of the previous guidelines in combination with risk stratification, we now have a step-by-step approach for anticoagulation bridging during medical procedures. Recommendations also specify that for minor dental and dermatologic procedures or cataract surgery, warfarin and aspirin therapy should be continued. However, aspirin or clopidogrel should be held 7 to 10 days prior to all other types of surgery. Aspirin or clopidogrel should be continued in patients with bare metal or drug-eluting stent placement for 6 and 12 months, respectively. This is only a summary of the most pertinent recommendations for outpatient management of anticoagulants. More details of these guidelines, as well as inpatient dosing and recommendations for antithrombotic and thrombolytic therapies, are available for review in the CHEST June 2008 Supplement.
GCSHP has a new website that is linked to TSHP website. Log on to the TSHP website at
www.tshp.org and under the Links tab, click on GCSHP!!!
Has your contact information changed?
Please send all changes to
Katy Hanzelka at
GCSHP Newsletter is published quarterly
Submit contributions to
Monica Robinson Green, PharmD, BCPS, Editor
phone: (281) 260-3375
e-mail: [email protected]
S P R I N G I S S U E

12
Office/PositionOffice/PositionOffice/PositionOffice/Position NameNameNameName Contact InformationContact InformationContact InformationContact Information Reason to ContactReason to ContactReason to ContactReason to Contact
President Richard Cadle [email protected]
President-Elect Jennifer Nguyen [email protected]
Immediate Past President Todd Canada [email protected]
Directors Monica Robinson Green
Andy Laegeler
Annual Seminar
Recording Secretary W. Donovan Strader [email protected]
Treasurer Candy Eggleston [email protected] Payment inquiries
Membership Secretary Katy Hanzelka [email protected] Membership status; Address
change
Communication Council Monica Robinson Green [email protected] Newsletter article submission
Mentorship program
Education Council Jennifer Christensen [email protected] Continuing education events or
credit
Professional and Legal Affairs Ryan Roux [email protected]
Technician Section Kathleen Thomas
Gina Beanes
Technician membership
Student Section—TSU Celia Fenceroy [email protected] Student membership
Student Section—UH Amy Moss [email protected] Student membership
Members-at-Large Chad Hardy
Dan Metzen
Michael Pinon
Douglas Rasmussen
Website issues
Annual Seminar
Annual Seminar
Annaul Seminar
Industry Representative Randall Dausin Annual Seminar