Embed Size (px)
Citation preview

Hurricanes continue to affect us in the Gulf Coast region, but it can-not stop our membership growth – we continue to recruit new stu-dent and technician members with our directed efforts and continuing education (CE) programs. The student membership drives peaked in August and September at Texas Southern University and the Uni-versity of Houston colleges of pharmacy. GCSHP is honored to provide our support to future members and leaders in our soci-ety. We are also sponsoring a Texas Medical Center pharmacy residency program social on Sep-tember 25th for area PGY-1 and PGY-2 residents.
Our Educational Council, under the direction of Jennifer Christen-sen, PharmD, continues to identify CE programs of relevance for our membership. We are planning to explore a technician CE program on Women’s Health within the
next 6 months and a preceptor CE program for pharmacists within the region. If you have specific topics of interest, please send y o u r C E i d e a s t o tcanada@ mdanderson.org.
The Board of Directors is working with the executive director for TSHP to have our website be a component of TSHP’s homepage as a link. We have not received any feedback from the member-ship regarding specific features you would like to see on our web-site to date (www.gcshp.org) so the Board of Directors is compil-ing the items we hope the mem-bership would find most useful. We are hoping this will influence our local members to join TSHP for the added benefit of CE, as we have to pay an additional fee for non-TSHP members attending local CE programs in this region. The added benefits of joint mem-bership would provide you with
the weekly TSHP electronic news-letter, the TSHP quarterly journal with original articles and practice-oriented information, as well as periodic special mailings about new regulations or developments in practice. You will still, of course, receive our GCSHP quar-terly newsletter!
Save the Date – our next Annual
Seminar is set for Saturday, Feb-
ruary 7th, 2009 with the topics to include new drug updates in on-cology, HIV/AIDS, gastrointesti-nal disorders and endocrinology, as well as a sterile compounding update and technician town hall. We will also offer a Career Panel for students after lunch. If you are interested in assisting with the seminar or serving on the future committee, please contact Eddie Lee, PharmD, BCPS at 409-747-3181 or email: lelee@ utmb.edu
President’s Report Todd Canada, PharmD, BCNSP, FASHP
The University of Houston Col-lege of Pharmacy (UHCoP), through the Practice Programs Office, offers several P4 rotation sites with the Indian Health Ser-vice (IHS) in New Mexico, Ari-zona, and Alaska. I had the privi-lege of spending twelve weeks in Sitka, AK, from May 25 – August 16, 2008. Simply stated – it was a phenomenal, life-changing experi-ence!
The rotation site, where I com-pleted my institutional medicine and family medicine rotations, is
called Mt. Edgecumbe Hospital and is the largest facility of the SouthEast Alaska Regional Health Consortium (SEARHC – pro-nounced “Search”). SEARHC serves 18 native communities of the Tlingit, Haida, Tsimshian, and other Native people of Southeast Alaska. With a population of approximately 9000, Sitka is the second largest of these communi-ties, after Juneau.
I shared the summer with another Pharmacist intern named Marc Brancaccio from the Wingate
University School of Pharmacy in Charlotte, NC; Steve Ellis, an optometry intern from Southern
An Alaskan VACATION ROTATION -Ann Marie Prazak
August
September
2008
President’s Report 1
Alaskan Rotation 1,3
Calendar of Events 2
Mentor Program 2
Student Section 4
Resident Section 8
Inside this issue:
HealthSystemCE.org
The e-learning center for Health-System Pharmacy
Society Members!
Easy access to home study programs!
——————————-
Has your contact infor-mation changed?
Please send all changes to
Allison Wilson at
GULF COAST SOCIETY OF
HEALTH-SYSTEM
PHARMACISTS
KAYAKED TO PIRATE’S COVE AND CAUGHT THE BEACH VIEW SUNSET
-Continued on page 3

Calendar of Events
• September 25 - 26
UH Clinical Skills Competi-
tion
• October 16
3rd Annual TSU/ UH Fall
Seminar
• November 7
UH College of Pharmacy Resi-
dency Showcase
• December 7 - 11
43rd ASHP Midyear Clinical
Meeting, Orlando, Fl
Page 2 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS
Mentors shall :
•Cultivate a professional relationship with the protégé
•Encourage and facilitate thought-provoking questions
•Communicate via phone, email, and/or one-on-one visit
•Provide positive feedback and constructive criticism
•Offer support through listening and sharing
•Contribute to the professional growth of future pharmacists
The Gulf Coast Society of Health-System Pharmacists (GCSHP) is ex-cited to continue to student and phar-macist members the GCSHP Mentor-ship Program!
The GCSHP Mentorship Program fosters networking and communica-tion experiences between practicing pharmacist members and energetic student members who are interested in furthering their commitment to student development and obtaining a greater understanding of the phar-macy profession, respectively. The establishment of this relationship between pharmacists and students provides a framework for students to explore their potential as well as de-velop visibility within the organiza-tion.
This program allows student mem-bers the opportunity for networking, professional development and career guidance to ensure the advancement of the pharmacy profession, which is our mission. For pharmacist mem-bers, the program represents another avenue for contributing towards to development in the profession, out-side of the preceptor-student relation-ship.
Participation in the program is strictly voluntary.
Mentors act as role models for their protégés. They facilitate and foster the development of a protégé through teaching, coaching, counsel-ing and championing. Pharmacist mentors will be paired with students to provide a greater understanding of a variety of career paths within the pharmacy profession.
Mentor requirements:
To mentor a pharmacy student
please complete the mentor profile
form provided in the Au-
gust/September 2008 GCSHP
Newsletter and submit via email
to the address below. (page 10)
Protégé Requirements:
To apply for the program, please
complete the application provided
by your pharmacy school repre-
sentative, and submit via email a
letter of interest and Curriculum
Vitae or Resume to the address
below.
Monica Robinson Green PharmD
Protégés Shall :
•Cultivate a professional relationship with the mentor
•Demonstrate strengths and explore potential
•Communicate via phone, email, and/or one-on-one visit
•Integrate feedback and grow professionally
•Make a commitment to your professional development
•Communicate current goals and objectives to mentor
Pharmacy School Representatives Ashley Scott, Texas Southern University Christi Parker, University of Houston
MENTOR PROGRAM

California School of Optometry in Fullerton, CA; and Al Kahal, an Environmental Health MS student from Tulane University in New Orleans, LA. The program is structured so that Marc and I ro-tated between the inpatient and outpatient services at two-week intervals. In other words, if I were inpatient, he would be outpatient. By Houston standards, Mt. Edgecumbe is an inconceivably small facility. The hospital has 27 beds – 3 on the critical care service (CCS), 17 on the acute medicine service (AMS), and 7 in OB-GYN/surgery service (OSS). The outpatient pharmacy fills about 5000 prescriptions per month.
Because of the unique setup of the rotation site, I experienced the full range of patient care – from chart review for refill requests, to tele-pharmacy and mail order, to the more traditional pharmacist role in the outpatient setting to caring for all levels of patient acuity in the inpatient setting. In addition, I
was able to tailor the rotations to my interest in critical care, and I actively participated in codes, direct cardio conversion, and an extubation.
Since the average day length for
the summer is at least 17 hours, when the work day was complete we had plenty of time remaining each day to enjoy the outdoors.
My fellow interns and I biked, hiked, mountain climbed, kayaked, fished, and practiced Anusara yoga.
Most remarkable of our adven-tures was completing the Baranof Cross-Island Trail, where I learned a completely new skill set/language and fell in love with mountaineering! !
For more information about the trail, visit http://en.wikipedia.org/wiki/Baranof_Cross-Island_Trail.
If you are interested in learning more about interning at SEARHC and the incredible lifestyle that is unique to Sitka, please email me at abprazak@ uh.edu. For a different perspective, I also recommend contacting Constance Reyes at cmreyes2@ uh.edu, who is cur-rently on rotation in Sitka through November 2008. Finally, look for a more detailed article in the No-vember issue of the TSHP Journal. I’d like to extend a special thank you to all of the pharmacy staff at SEARHC, and especially Joel and Jessica Hinckley, Jeff Chamberlain, Mary and Bryant Mackey, Eric Skan, Jill Reid, and Tracy Gale.
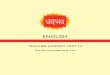
JULY 26 - STARRIGAVAN BAY A SUMMER IN ALASKA WOULD NOT
BE COMPLETE WITHOUT FISHING FOR SALMON!
August 9, 2008 - MT. BASSIE
—3900FT. The beautiful sunset on the ridge of Mt. Bassie on Baranof Cross-Island Trail, a difficult 16-mile informal trail that took two nights and two days to complete.
Left to right: Steve Ellis, Optometry Intern, Southern California College of Optometry; Jeff Chamberlain, PharmD, Mt. Edgecumbe Hospital; Marc Brancaccio, Pharmacist Intern, Wingate School of Pharmacy; and Ann Marie Prazak, Pharmacist Intern, University of Houston College of Pharmacy
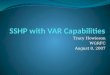
August 10, 2008 - BARANOF CROSS-ISLAND TRAIL
Paused to take a photos of a large cornice, an overhanging mass of snow along the crest of a ridge. The steep slope below a cornice is often the starting point for an avalanche.
Page 3 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS

The new officers of TSU SSHP are very ex-cited about the upcoming year and following in the footsteps of those who came before them. The new officers are:
President: Ashley Scott (P3) President-elect: Celia Fenceroy (P2) Vice President: Chitakone Liankeo (P3) Treasurer: Kristine Aquino (P3) Secretary: Arezo Normoohadi (P3) Historian: Thu Pham (P3)
The 2008-2009 academic year for TSU SSHP began with a community service project at Acres Home Health Center in Houston, TX. Third and fourth year students participated in the Annual Acres Home Health Fair, counsel-ing patients on their current medications and answering any questions that the patients may have. During the first week of school, the officers conducted a membership drive en-couraging pharmacy students to become in-
volved in SSHP and its affiliated organizations, GCSHP, TSHP, and ASHP. The officers are working to increase their membership numbers and reach out to students on a more personal level by hosting socials and other off campus activities. The first general meeting of the year was held on Wednesday, September 3 and the highlighted speaker was Todd Canada, GCSHP president. Other special guests were Ogechi Eshleman, immediate past president of GCSHP and Pam Dyer, immediate past presi-dent of TSU SSHP. Dr. Canada presented an informative speech on the importance of be-coming actively involved and the benefits that both students and pharmacists can gain from joining the organizations. He also touched upon the different types of jobs that fall under the title of Health System Pharmacists and answered questions regarding residency pro-grams.
TSU SSHP has already begun planning events in collaboration with other professional phar-
macy organizations recognized on TSU’s campus, such as the TSU APhA-ASP chapter, Kappa Psi Pharmaceutical Fraternity and SNPhA. Other upcoming events include the Fall Seminar with U of H SSHP in October, the clinical skills competition and the Midyear Clinical Meeting in Orlando, Florida.
Although we are starting a new academic year, with new officers, our mission is the same, “… to increase the students knowledge and awareness of pharmacy practice in health systems; provide information to students regarding career options in and credentials needed for pharmacy practice in health sys-tems; and encourage membership and partici-pation in TSHP and ASHP as a student and after graduation.”
Ashley Scott
TSU SSHP President
Texas Southern University
University of Houston
Page 4 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS
UHSSHP would like to welcome the Class of 2012! Congratulations on beginning your jour-ney through pharmacy school. We hope it will be a great one. It will be over before you know it, and you will begin an invigorating career in health-system pharmacy.
First, SSHP would like to congratulate a few of our members for their acceptance into an ASHP Advisory Group this year!
Membership Advisory Group – Allison Palmer (P3) and Daniel Ortiz (P2)
Student Society and Leadership Development Advisory Group – Tri Nguyen (P4)
Communications Advisory Group – Christi Parker (P3)
Meetings and Programming Advisory Group – Stephanie Weightman (P3)
As the Fall 2008 semester begins, the dedicated officers of UHSSHP anticipate a phenomenal year. Over the summer, officers held a Fall Planning Meeting to prepare for the Class of 2012 New Student Orientation and upcoming year. The officers introduced the P1s during New Student Orientation via a short presenta-tion, where we handed out Disney fruit snacks to promote the Midyear Clinical Meeting in
Orlando, FL! We also participated in the or-ganizational fair on the last day of orientation where P1s purchased items from different organizations and learned more about the vari-ous student organizations. We sold clipboards with pertinent lab values and various UHCoP and SSHP t-shirts.
UHSSHP held our first UH Main Campus Meeting of the semester on Tuesday, August 26, 2008. Over 100 P1 and P2 students were in attendance to learn about the benefits of SSHP membership and various leadership opportuni-ties that the organization has to offer. Officers handed out membership forms and raffled off medical dictionaries to P1s. On August 27, 2008, we held our 3rd Annual SSHP Down-town Aquarium Social, which allowed us to welcome the incoming first-year students and celebrate the beginning of the fall semester.
This year we will host UHSSHP meetings on the UHCoP Main Campus on the second and fourth Tuesday of each month. This semester’s meetings will feature topics from speakers in research, oncology, new practitioner, critical care, ambulatory care, and residencies. We will also hold meetings on our Texas Medical Cen-ter Campus on the first and third Monday of each month. These meetings will include jour-
nal club, pediatric cardiology, and Midyear Clinical Meeting preparation. Our first journal club meeting was held on Monday, Septem-ber 8, 2008 where Dr. Jeff Sherer introduced the literature evaluation process.
On Thursday, October 16, 2008 the Univer-sity of Houston College of Pharmacy will be joining Texas Southern University to hold the 3rd Annual Fall Seminar at the Alumni Center in the Great Hall. The UH Clinical Skills Competition will be held on September 25 - 26, 2008 at the UHCoP TMC Campus. On Friday, November 7, 2008, from 3:00 PM – 5:00 PM, we will host the UH College of Pharmacy Residency Showcase at the UH TMC Campus where UH, TSU, and UT pharmacy students are invited to learn about Texas residency programs in a smaller setting than ASHP Midyear.
UHSSHP is looking forward to another out-standing year. We would like to thank our members for their continued support and wish everyone the best of luck this year!
Christi Parker
UH SSHP President

Page 5 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS
TSU SSHP participates in
the annual
Acres Home Community
Center
Health Fair
August 2008
TSU SSHP
General Meeting
September 2008
Guest Speaker
Todd Canada GCSHP
President
——————————
Left to right: Ashley Scott; Todd Canada, PharmD, BCNSP,
FASHP; Chad Hardy, PharmD, MS; Ogechi Eshleman, PharmD;
Chitakone (Anny) Liankeo
UH SSHP
2008-2009 Officers
Left to Right: Mary Helen Chaplin, Gerald Kim, Dan Truong-le, Jeffrey Joe, Daniel Ortiz, Amanda Garcia, Minhtri Nguyen, April Morgan, Allison Mosely, Allison Palmer Front Row: Ann Marie Prazak, Christi Parker, Amy Moss, Stephanie Weightman

Page 6 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS
Nebivolol Efficacy and Safety
Van Tran, Pharm.D. Candidate 2009
University of Houston College of Pharmacy
Hypertension is an increasingly important health issue for both the public and healthcare professionals. In order to help guide clinicians in the management of this disease, the Seventh Re-port of the Joint National Committee on Prevention, Detec-tion, Evaluation, and Treatment of High Blood Pressure (JNC 7) was developed. The ultimate goal of antihypertensive ther-apy is to reduce morbidity and mortality of the cardiovascular and renal system.1
Beta-blockers, as one of the most important classes of anti-hypertensive drugs, have proven to reduce morbidity and mortality of cardiovascular diseases.2 Nebivolol, a new third-generation β-adrenergic-blocking agent, was recently approved by the FDA in 2008.3 Nebivolol is unique because it has a greater degree of beta-1 cardioselectivity than other agents available in this class.3 In addition to the other beta-1 blocker mechanisms of action, it also has nitric oxide mediated vasodi-latory effects.3 The FDA approval of nebivolol was based on three randomized, multicenter, double-blind, placebo-controlled twelve week clinical trials in patients with mild to moderate hypertension.4
In the trial of Weiss and colleagues, 909 patients were random-ized to placebo or once daily nebivolol 1.25, 2.5, 5, 10, 20, or 40 mg. Treatment with nebivolol resulted in a statistical sig-nificant reduction in sitting systolic and diastolic blood pres-sure and an increase in responder rates (p<0.001). The trial’s results also showed equal side effect tolerability in both groups. Common adverse effects usually associated with beta-blockers, such as fatigue, erectile dysfunction, bradycardia, depression, and decreased libido, were low in nebivolol groups.5
Saunders and colleagues conducted another study with 300 African American patients with mild-to-moderate hyperten-sion. They were randomized to placebo or once daily nebivo-lol 2.5, 5, 10, 20, or 40 mg. Like the previous trial, treatment with nebivolol resulted in a statistical significant reduction in systolic and diastolic blood pressure with higher responder rates than placebo (p<0.001). This trial’s promising results also showed that nebivolol was not associated with adverse metabolic effects.6
In a third study by Gradman and colleagues, 669 patients were randomized to placebo or once-daily nebivolol 5, 10, or 20 mg in addition to ongoing antihypertensive therapy (Angiotensin-Converting Enzyme Inhibitor (ACEI), Angiotensin II Recep-tor Blocker (ARB), Diuretic, ACEI+Diuretic, or ARB+Diuretic). Nebivolol showed a statistical significant reduction in blood pressure when added to ongoing therapy in the management of mild to moderate hypertension (p<0.001).7
These clinical trials have demonstrated that nebivolol is effec-tive and safe to use in the treatment of mild to moderate hy-pertension. Also, data collected from clinical trials showed that nebivolol was not associated with adverse metabolic ef-fects.8 Furthermore, its beneficial hemodynamic profile of high β1 cardioselectivity and nitric oxide vasodilatory effect has distinguished nebivolol from other beta-blockers in its class.3,4
These studies have supported the tolerability and efficacy of nebivolol as monotherapy or in combination with other anti-hypertensive drugs. Even though nebivolol show promising
results, larger clinical studies need to be conducted to prove its place in antihypertensive therapy. Also, its long term safety and efficacy to improve clinical outcomes have yet to be deter-mined and reported. In conclusion, nebivolol may play an important role in addition to conventional antihypertensive treatment, but more clinical studies must be conducted in order to use it as the drug of choice in antihypertensive ther-apy.
References
National Heart, Lung, and Blood Institute. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure guidelines. NIH. 2004;04-5230.
Saseen JJ, Carter BL. Hypertension. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, editors. Pharmacotherapy: a patho-physiologic approach. New York: McGraw Hill; 2005. p. 207-8.
Weiss RJ. Nebivolol: A novel beta-blocker with nitric oxide-induced vasodilatation. Dove Medical Press. 2006;2(3):303-8.
Nebivolol [package insert]. St. Louis, MO: Forest Pharmaceuticals, Inc., 2007.
Weiss RJ, Weber MA, Carr AA, Sullivan WA. A randomized, double-blind, placebo-controlled parallel-group study to assess the efficacy and safety of nebivolol, a novel β -blocker, in patients with mild to moderate hypertension. J Clin Hypertens. 2007;9:667-76.
Saunders E, Smith WB, DeSalvo KB, Sullivan WA. The efficacy and tolerability of nebivolol in hypertensive African American patients. J Clin Hypertens. 2007;9:866-75.
Gradman AH. Addition of the β -blocker nebivolol to ongoing therapy in the management of mild to moderate hypertension. American Society of Hypertension (ASH) 22nd Annual Meeting; Chicago, IL; May 19-22, 2007.
Schmidt AC, Graf C, Brixius K, Scholze J. Blood pressure-lowering effects of nebivolol in hypertensive patients with type 2 diabetes mellitus. Clin Drug Invest 2007;27(12):841-9.
Folgari R, Zoppi A, Lazzari P, Mugellini A, Lusardi P, Preti P, et al. Comparative effects of nebivolol and atenolol on blood pressure and insulin sensitivity in hypertensive subjects with type II diabetes. J Hum Hypertens. 1997;11:753-7.
Nodari S, Metra M, Dei Cas L. β -blocker treatment of patients with diastolic heart failure and arterial hypertension. A prospective, random-ized, comparison of the long-term effects of atenolol vs. nebivolol. Eur J Heart Fail. 2003;5:621-7.
Grassi G, Trevano FQ, Facchini A, Toutouzas T, Chanu B, Mancia G, et al. Efficacy and tolerability profile of nebivolol vs atenolol in mild-to-moderate essential hypertension: results of a double-blind randomize multicentre trial. Blood Press. 2003;12:35-40.
Urlir O, Fejfusa M, Havranek K, et al. Nebivolol versus metoprolol in the treatment of hypertension. Drug Intest. 1991;3:107-10.
Celik T, Iyisoy A, Kursaklioglu H, Kardesoglu E, Kilic S, Turhan H, et al. Comparative effects of nebivolol and metoprolol on oxidative stress, insulin resistance, plasma adiponectin and soluble P-selectin levels in hypertensive patients. J Clin Hypertens. 2006;24:591-6.
Brixius K, Middeke M, Lichtenthal A, Jahn E, Schwinger RG. Nitric oxide, erectile dysfunction and beta-blocker treatment (MR NOED STUDY): benefit of nebivolol versus metoprolol in hypertensive men. Clin Exp Pharmacol Physiol. 2007; 34:327-31.
Doumas M, Tsakiris A, Douma S, Grigorakis A, Papadopoulos A, Hounta A, et al. Beneficial effects of switching from β -blockers to ne-bivolol on the erectile function of hypertensive patients. Asian J Androl. 2006; 8:177-82.
Rosei EA, Rizzoni D, Comini S, et al. The nebivolol-lisinopril study group. Evaluation of the efficacy and tolerability of nebivolol versus lisinopril in the treatment of essential arterial hypertension: a randomized, multicenter, double blind study. Blood Press. 2003;12:15-23.
Van Bortel, LM, Bulpitt CJ, Fici F. Quality of life and antihypertensive effect with nebivolol and losartan. Am J Hypertens. 2005;18:1060-66.
Mazza A, Bil-Extremera B, Maldonato A, et al. Nebivolol vs amlodipine as first-line treatment of essential arterial hypertension in the elderly. Blood Press. 2002;11:182-8.
Flather MD, Shibata MC, Coats A, Van Veldhuisen DJ, Parkhomenko A, Borbola J, et al. Randomized trial to determine the effect of nebivolol on
mortality and cardiovascular hospital admission in elderly patients

Page 7 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS
Doripenem (DoribaxTM): the Newest Addition to the Carbapenem Family
Denisse I. Martinez, Pharm.D.
Pharmacy Resident 2007-2008
The University of Texas Medical Branch
Carbapenems are a potent class of beta-lactam antibiotics with broad spectrum activity against gram-positive, gram-negative, and anaerobic pathogens. These agents are usually reserved for severely ill, hospitalized patients for the treatment of noso-comial pneumonia, complicated urinary tract infections (UTIs), complicated intra-abdominal infections, febrile neutro-penia, septicemia, complicated skin and soft-tissue infections, meningitis, and pulmonary infections in patients with cystic fibrosis.1
Antimicrobial resistance is a serious problem that is associated with increased health-care costs and increased rates of morbid-ity and mortality.2 With the increase in rates of infection with multi-drug resistant (MDR) pathogens, including Pseudomonas aeruginosa and extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae species, the use of carbapenems has increased.1 Health-care providers are faced with the chal-lenge of treating these pathogens resistant to almost all avail-able antibiotics.2 Therefore, the development of new antibiot-ics is essential to improve outcomes in patients infected with MDR pathogens.1
Doripenem is the newest member of the carbapenem class. It was approved in the U.S. in 2007 for the treatment of compli-cated UTIs and intra-abdominal infections.3 Similar to the other anti-pseudomonal carbapenems, doripenem has broad spectrum activity against many MDR pathogens, including ESBL-producing organisms. Like the other carbapenems, doripenem lacks activity against methicillin-resistant Staphylococ-cus aureus, methicillin-resistant coagulase-negative staphylo-cocci, Enterococcus faecium and Stenotrophomonas maltophilia.3 Doripenem has demonstrated greater activity against gram-positive organisms compared to meropenem and greater activ-ity against gram-negative pathogens compared to imipenem.2,3 Doripenem also has greater activity against P. aeruginosa than the other carbapenems, including strains that have acquired resistance to imipenem or meropenem.2,3
Another advantage of doripenem versus other available car-bapenems is its increased stability in solution. Both imipenem and meropenem are considered to be relatively unstable in solution with considerable degradation after 3.5 and 5.5 hours, respectively. Therefore, they should not be infused for longer than 2 to 3 hours. Doripenem, however, appears to be stable in solution for up to 12 hours, which should allow for a longer duration of infusion.1 As with other beta-lactams, carbap-enems exhibit a time-dependent killing effect. Therefore, their efficacy is related to the time above the minimum inhibitory concentration (MIC). The ability to prolong the infusion of doripenem will increase the time above the MIC.
Doripenem’s safety profile differentiates it from other carpa-benems.1,2 All beta-lactams have the potential to cause sei-zures when dosages are not adjusted for impaired renal func-tion or small body mass. Carbapenems are believed to cause seizures by binding directly to the GABAA receptor.2 Horiuchi et al. evaluated the convulsive activity of doripenem compared to other beta-lactam antibiotics. Compared to imipenem and
meropenem, doripenem displayed the least affinity for GABAA receptors (95%, 49%, and 10%, respectively).4 Addi-tionally, in phase III clinical trials, seizures have not been re-ported with doripenem.1
The efficacy of doripenem in the treatment of complicated UTIs and intra-abdominal infections has been evaluated in several studies. Three trials have been conducted in patients with abdominal infections and two in patients with UTIs. However, these trials have only been published in abstract form.2,5
Doripenem is approved for the treatment of complicated UTIs caused by E. coli, Klebsiella pneumoniae, Proteus mirabilis, P. aeruginosa, and Acinetobacter baumannii. Naber et al. conducted an international, prospective, randomized, double-blind, multi-center, non-inferiority study comparing the efficacy of doripenem 500 mg IV every 8 hours to levofloxacin 250 mg IV daily in 748 patients with complicated UTIs or pye-lonephritis.6 Patients in both groups could be switched to levofloxacin 250 mg orally once daily when clinically stable. The results of the study showed that doripenem was non-inferior to levofloxacin when clinical cure rates (95.1% vs. 90.2%, respectively) and microbiological cure rates (79.2% vs. 78.2%, respectively) were compared. A prospective, open-label, international, multicenter, single-arm study of doripenem (n=423) was conducted to assess its efficacy in patients with complicated UTIs.6 All patients in this study received doripenem and were compared to the patients who had re-ceived levofloxacin in the previously described study by Naber and colleagues. Doripenem was found to be non-inferior to levofloxacin with respect to clinical cure rates (93% vs. 90.2%, respectively).
Doripenem is also approved for the treatment of complicated intra-abdominal infections caused by E. coli, K. pneumoniae, P. mirabilis, P. aeruginosa, Bacteroides caccae, Bacteroides fragilis, Bacter-oides thetaiotaomicron, Bacteroides uniformis, Bacteroides vulgatus, Strep-tococcus intermedius, Streptococcus constellatus, and Peptostreptococcus micros. In two identical, randomized, multinational, multicen-ter, double-blind studies, the efficacy of doripenem 500 mg IV administered over 1 hour every 8 hours was compared to mer-openem 1 g IV administered over 3-5 minutes every 8 hours in 946 patients.6 Doripenem was found to be non-inferior to meropenem with regard to clinical cure rates. In the first study, the clinical cure rates in the microbiologically evaluable patients were 82.8% vs. 85.9%, respectively. In the second study, the rates were 81% vs. 82.1%, respectively.
Although not an FDA-approved indication, doripenem has also been shown to be effective in the treatment of ventilator-associated pneumonia (VAP). In a large, prospective, random-ized phase III clinical trial, Chastre et al. tested the efficacy of doripenem 500 mg IV every 8 hours via a 4-hour infusion versus imipenem 500 mg IV every 6 hours via a 30-minute infusion or imipenem 1000 mg IV every 8 hours via a 60-minute infusion in 531 patients with VAP.7 Clinical cure rates with doripenem were non-inferior to imipenem (68.3% vs. 64.2%, respectively). Therefore, the authors concluded that doripenem is clinically effective and non-inferior to imipenem in the treatment of VAP. Doripenem is currently being evalu-ated in 3 other clinical trials for VAP and health-care associ-ated pneumonia.5
Note: Denisse Martinez currently works at Harris County Hospital District as a Critical Care Pharmacist

Page 8 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS
The rise in infections caused by MDR pathogens in the health-care setting makes the carbapenems an important class of antibiotics. Doripenem’s expanded antimicrobial activity, improved stability in solution compared to other carbapenems, and decreased propensity to cause seizures may be advanta-geous in hospital and ICU settings where the prevalence of nosocomial infections is increasing and the use of broad-spectrum antibiotics is more frequently required. However, to attempt to minimize the development of resistance, doripenem should be reserved for severe, life-threatening infections where other antimicrobial options are limited.
References
Nicolau D. Carbapenems: a potent class of antibiotics. Expert pin Pharmacother 2008;9(1):23-37.
Lister PD. Carbapenems in the USA: focus on doripenem. Expert Rev Anti Infect Ther 2007;5(5):793-809.
Anderson DL. Doripenem. Drugs of Today 2006;42(6):399-404.
Horiuchi M, Kimura M, Tokumura M, et al. Absence of convulsive liability of doripenem, a new carbapenem antibiotic, in comparison with �-lactam antibiotics. Toxicology 2006;222:114-124.
http://www.clinicaltrials.gov. Search term: Doripenem. Ac-cessed 5/16/08.
Doribax (Doripenem for injection). Full prescribing informa-tion. Ortho-McNeil-Janssen Pharmaceuticals, Inc; Raritan, NJ: January 2008.
Chastre J, Wunderink R, Prokocimer P, et al. Efficacy and safety of intravenous infusion of doripenem versus imipenem in ventilator-associated pneumonia: a multicenter, randomized study. Crit Care Med 2008;36(4):1089-96.
Raltegravir for the Treatment of Human
Immunodeficiency Virus
Sylvia L. Best, Pharm.D.
Pharmacy Practice Resident
Harris County Hospital District
Human Immunodeficiency Virus (HIV) is a leading cause of death in minorities, especially African-Americans. Over 1 million people are currently living with the disease and there is an estimated 56,300 new cases each year in the United States.1,2 HIV is an infectious disease in which patients may present with a sore throat, fever, myalgia, night sweats, nausea and vomiting. Suspected cases of HIV may be verified by the enzyme-linked immunosorbent assay (ELISA) and confirmed by a positive western blot test.
Since the discovery of zidovudine (AZT) in 1987, six drug classes have been approved by the Food and Drug Admini-stration (FDA) for the treatment of HIV. These drug classes consist of nucleoside reverse transcriptase inhibitors (NRTI), non-nucleoside reverse transcriptase inhibitors (NNRTI), protease inhibitors (PI) and fusion inhibitors. Within the past 12 months, FDA approved three novel agents which include, etravirine (Intelence): a non-nucleoside reverse transcriptase inhibitor; maraviroc (Selzentry): a new class called CCR5 an-tagonists; and raltegravir (Isentress): another new class, inte-grase inhibitors.3
Within the HIV life cycle, the enzyme HIV-1 integrase allows viral DNA to incorporate into the host cell for replication. Raltegravir inhibits this process making it effective against resistant HIV strains.4 Merck & Co., Inc. obtained FDA ap-proval to market raltegravir in the U.S. in October 2007. This approval was a pivotal step in infectious disease because this new class of agents provides an oral alternative for treatment experienced patients.
Steigbigel et al. conducted two identical double-blind, random-ized, phase III trials in various geographic regions. BENCHMRK-1 and BENCHMRK-2 are ongoing trials which assess if raltegravir 400mg twice a day with optimized back-ground therapy for HIV is superior to placebo with optimized background therapy in patients who have at least one drug class failure. New England Journal of Medicine recently pub-lished an interim analysis which displayed data through the first 48 weeks. Both trials are expected to continue until 156 weeks of data is collected. A total of 703 patients combined were randomized into the studies. Data from the combined trials at 16 weeks discovered HIV-1 RNA was suppressed to undetectable levels of less than 50 copies per milliliter in 61.8% of raltegravir recipients as opposed to 34.7% of placebo recipients (P<0.001). Analysis at 48 weeks found 62.1% of raltegravir patients achieved undetectable HIV-1 RNA levels compared to 32.9% of placebo patients (P<0.001). In summa-tion, authors discovered raltegravir combined with optimized drug therapy provided better HIV suppression than optimized drug therapy alone.5
HealthSystemCE.org
The e-learning center for Health-
System Pharmacy Society Members!
Easy access to home study
programs!
——————————-
Has your contact information
changed?
Please send all changes to
Allison Wilson at

Page 9 GULF COAST SOCIETY OF HEALTH-SYSTEM PHARMACISTS
The most common side effects include nausea (2.4%), diarrhea (4.3%) and headache (2.6%).3,5,6 Patients in clinical trials ex-perienced increased creatnine kinase (5.4%), cholesterol (8%), triglycerides (8.4%) and aminotransferase (3.5-4.3%) values.5
Raltegravir should be initiated in treatment-experienced adults who have failed therapy in other medication classes.6 Nearly all HIV agents are metabolized by the CYP 450 system, which makes raltegravir very unique. Raltegravir undergoes hepatic glucuronidation through uridine diphospate glucoronsyltrans-ferase, therefore drug interactions are limited.7 Patients con-comitantly using rifampin or atazanavir should be monitored more frequently. Dose adjustments are unnecessary for hepatic or renal dysfunction. Raltegravir is a pregnancy class Category C drug and has not been tested in children less than 16 years old. Raltegravir is available in 400mg strength tablets and should be dispensed as one tablet twice daily. Raltegravir may be taken without regard to food.7 A one month supply of ther-apy will cost patients approximately $970.3
Prior to the approval of raltegravir and maraviroc, there were no oral options for patients in need of salvage therapy. Either agent may benefit patients resistant to HIV without signifi-cantly increasing pill burden.
References
1 Department of Health and Human Services: Centers for Disease Control and Prevention. www.cdc.gov. Accessed: September 1, 2008
2 Hall PhD, H. et al. Estimation of HIV Incidence in the United States. JAMA 2008 August 6; 300(5):520-529
3 Lexi-Comp Online. www.crlonline.com Accessed: July 29, 2008
4 Two New Drugs for HIV Infection. Med Lett Drug Ther 2008 Jan 14; 50(1277):2-4
5 Steigbigel MD, R. et al. Raltegravir with Optimized Back-ground Therapy for Resistant HIV-1 Infection. N Engl J Med 2008 July 24; 359(4):339-354
6 New HIV Drug: Raltegravir (Isentress). Pharmacist’s Letter/Prescriber’s Letter 2007; 23(11):231103
7 Guidelines for the Use of Antiretroviral Agents in HIV-1 Infected Adults and Adolescents. Bethesda, MD: Department of Health and Human Services (DHHS) 2008 Jan 29; p1-112
Breakfast/Exhibits
Opening Remarks
New Drug Update in Oncology
Wendy Smith, PharmD, BCPS
Drug Update in HIV/AIDS Management
Teddy Zerai, PharmD
Questions
Break/Exhibits
Sterile Compounding Update
Paul Holder, PharmD
Questions
Break/Exhibits
Drug Update in GI Disorders
Fred Sutton, MD
Drug Update in Endocrinology
Jose Garcia, MD
Questions
Lunch
Technician Town Hall
Paul Holder, PharmD
Career Panel for Students
Afternoon Break
Gulf Coast Society of Health-System Pharmacist
Annual Seminar February 2009
If you are interested in serving on any of the councils,
please contact the appropriate chairperson. (pg 11) Get involved today!
Get Involved!

Gulf Coast Soc iety of Health- System Pharmac ists
MENTOR PROGRAM
MENTOR PROFILE:MENTOR PROFILE:MENTOR PROFILE:MENTOR PROFILE:
GCSHP program is a volunteer opportunity between pharmacists and student members interested in obtaining a greater understandGCSHP program is a volunteer opportunity between pharmacists and student members interested in obtaining a greater understandGCSHP program is a volunteer opportunity between pharmacists and student members interested in obtaining a greater understandGCSHP program is a volunteer opportunity between pharmacists and student members interested in obtaining a greater understandinginginging
of the pharmacy profession. Please take the time to fill out the questionnaire below. This will allow GCSHP to create the bof the pharmacy profession. Please take the time to fill out the questionnaire below. This will allow GCSHP to create the bof the pharmacy profession. Please take the time to fill out the questionnaire below. This will allow GCSHP to create the bof the pharmacy profession. Please take the time to fill out the questionnaire below. This will allow GCSHP to create the bestestestest possible possible possible possible
match. For questions please contact Monica Robinson Green via email at [email protected] match. For questions please contact Monica Robinson Green via email at [email protected] match. For questions please contact Monica Robinson Green via email at [email protected] match. For questions please contact Monica Robinson Green via email at [email protected]
Name & Credentials: ________________________________________________________________________Name & Credentials: ________________________________________________________________________Name & Credentials: ________________________________________________________________________Name & Credentials: ________________________________________________________________________
Work Address: ____________________________________City: ____________ Zip Code: ________________Work Address: ____________________________________City: ____________ Zip Code: ________________Work Address: ____________________________________City: ____________ Zip Code: ________________Work Address: ____________________________________City: ____________ Zip Code: ________________
Phone (w): _______________________ (cell): _____________________ (other): ________________________Phone (w): _______________________ (cell): _____________________ (other): ________________________Phone (w): _______________________ (cell): _____________________ (other): ________________________Phone (w): _______________________ (cell): _____________________ (other): ________________________
EEEE----mail: ________________________________________Place of employment: ___________________________________________mail: ________________________________________Place of employment: ___________________________________________mail: ________________________________________Place of employment: ___________________________________________mail: ________________________________________Place of employment: ___________________________________________
Summary of Job Description: ___________________________________________________________________________________Summary of Job Description: ___________________________________________________________________________________Summary of Job Description: ___________________________________________________________________________________Summary of Job Description: ___________________________________________________________________________________
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
I would prefer to mentor (check or highlight all that apply):I would prefer to mentor (check or highlight all that apply):I would prefer to mentor (check or highlight all that apply):I would prefer to mentor (check or highlight all that apply):
In personIn personIn personIn person
EEEE----mailmailmailmail
PhonePhonePhonePhone
My best time to mentor a student is generally:My best time to mentor a student is generally:My best time to mentor a student is generally:My best time to mentor a student is generally:
MorningMorningMorningMorning
AfternoonAfternoonAfternoonAfternoon
EveningEveningEveningEvening
I am available to mentor (check or highlight all that apply):I am available to mentor (check or highlight all that apply):I am available to mentor (check or highlight all that apply):I am available to mentor (check or highlight all that apply):
During the weekDuring the weekDuring the weekDuring the week
WeekendsWeekendsWeekendsWeekends
What do you hope the student will gain from this relationship?What do you hope the student will gain from this relationship?What do you hope the student will gain from this relationship?What do you hope the student will gain from this relationship?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What do you hope to gain from this relationship?What do you hope to gain from this relationship?What do you hope to gain from this relationship?What do you hope to gain from this relationship?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
In matching you with a student, is there anything else we should take into account?In matching you with a student, is there anything else we should take into account?In matching you with a student, is there anything else we should take into account?In matching you with a student, is there anything else we should take into account?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Page 10

Office/Position Name Contact Information Reason to Contact
President Todd Canada tcanada@ mdanderson.org
President-Elect Richard Cadle cadle.richardmark@ med.va.gov
Immediate Past President Ogechi Eshleman Ogechi_eshleman@ hchd.tmc.edu
Directors Eddie Lee
Monica Robinson Green
lelee@ utmb.edu
monica_robinson@ hchd.tmc.edu
Annual Seminar
Recording Secretary W. Donovan Strader William.Strader@ memorialhermann.org
Treasurer Candy Eggleston creggleston@ yahoo.com Payment inquiries
Membership Secretary Allison Wilson awilson@ tmhs.org Membership status; Address change
Communication Council Monica Robinson Green monica_robinson@ hchd.tmc.edu Newsletter article submission
Mentorship program
Education Council Jennifer Christensen jennifer_christensen@ hchd.tmc.edu Continuing education events or credit
Professional and Legal Af-fairs
Ryan Roux ryan_roux@ hchd.tmc.edu
Technician Section Theresa Batiste
Kathleen Thomas
Gina Beanes
theresa_batiste@ hchd.tmc.edu
kathleen_thomas@ hchd.tmc.edu
gina.beanes@ va.gov
Technician membership
Student Section—TSU Ashley Scott ashley.randall@ yahoo.com Student membership
Student Section—UH Christi Parker christi.renee@ gmail.com Student membership
Members-at-Large Chad Hardy
Dan Metzen
Michael Pinon
Douglas Rasmussen
Chad_hardy@ hchd.tmc.edu
dmetzen@ tmhs.org
drmpinon@ sbcglobal.net
douglas.rasmussen@ cardinal.com
Website issues
Annual Seminar
Annual Seminar
Annaul Seminar
Industry Representative Rowland Harris Annual Seminar
GCSHP Newsletter is published quarterly
Submit contributions to
Monica Robinson Green, Pharm.D., Editor
phone: (281) 260-3375
e-mail: [email protected] We�re on the web!
www.gcshp.org
Page 11