Embed Size (px)
Citation preview

Diabetic Foot UlcerA Complete Solution
Therapy Approachwith Adapted Products

A Complete Solution for Diabetic Foot Ulcers
This booklet focuses on the recommended treatment of diabetic foot ulcers. Diabetes is regarded as the health crisis of the 21st century. Did you know that:
n 285 million people worldwide are affected by diabetes1
n Each year a further 7 million develop diabetes1
n More than 9 million Canadians live with diabetes or prediabetes1
n 15% of persons with diabetes will develop a foot ulcer2-3
n Every 30 seconds a lower limb is lost due to diabetes somewhere in the world4
n The total costs for treating a diabetic foot ulcer can range from $10,000 to $60,0005-6
The diabetic foot ulcer is one of the most severe effects of diabetes. BSN Medical offers a full package of primary dressings, fixation products and casting products for pressure offloading to help you help your patients.
Today, diabetes is extremely widespread. The disease is increasingly a result of lifestyle choices, in particular lack of exercise, excessive blood pressure and excess weight. Early recognition and taking a proactive stance help to keep the late effects in check.
1 Canadian Diabetes Association2 National Institute of Diabetes and Digestive and Kidney Diseases: Diabetic Neuropathy: The Nerve Damage of Diabetes. Washington, DC, US Department of Health and Human Services, 1995.3 Mayfield JA, Reiber GE, Sanders LJ, et al.: Preventive foot care in people with diabetes. Diabetes Care 1998; 21:2161-2177.4 Kshitij Shankhdhar, MBBS, Dip Diab, A World of Difference in Diabetic Foot Care, Podiatry Today, Volume 21 Issue 11, November 2008.5 Glover JL, Weingarten MA, Buchbinder DS, Poucher RL, Deitrick GA 3rd, Fylling CP: A 4-year outcome based retrospective study of wound healing and limb salvage in patients with chronic wounds. Adv Wound Care 10:33–38, 1997.6 Apelqvist J, Ragnarson-Tenmvall G, Persson U, Larsson J: Diabetic foot ulcers in a multidisciplinary setting: an economic analysis of primary healing and healing with amputation. J Intern Med 235:463–471, 1994.
2

Assessment and Treatment of the Diabetic Foot Ulcer
1 Heather L. Orsted, RN, BN, ET, MSc; Gordon Searles, OD, MD, FRCPC, FACP; Heather Trowell, BSC, OT (c); Leah Shapera, RN, MSN; Pat Miller, RN, ET; and John Rahman, Certified Orthotist.2 Sibbald RG, Orsted HL, Schultz GS, Coutts P, Keast D. Preparing the wound bed 2003: Focus on infection and inflammation. Ostomy/Wound Management. 2003;49(11):24-51.3 Nursing Best Practice Guideline: Assessment and Management of Foot Ulcers for People with Diabetes. Toronto: RNAO. 2004
Assessment and Treatment
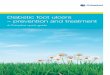
The Canadian Association of Wound Care has developed Best Practice Recommendations for the Prevention, Diagnosis and Treatment of Diabetic Foot Ulcers1 and recommends the following treatment algorithm2, in which pressure redistribution is a key component in treating the cause.
The importance of offloading
Pressure is a factor in 90 percent of diabetic plantar ulcers, and the pressure must be modified or removed. Pressure-induced ischemia occurs in tissues over bony areas of weight-bearing during ambulations and standing. Neuropathy prevents the perception of protective pain, resulting in a increased potential for tissue breakdown. Diabetic plantar ulcerations require aggressive and effective downloading in order to achieve wound healing.3
Person withDiabetic Foot Ulcer
Identify and Treatthe Cause
Vascular flowAwareness of neuropathic
changesPressure redistribution
Glycemic controlLipid control
Local Wound Care
Patient-CenteredConcerns
Adherence toplan of care
Quality-of-life issuesrelated to lifestyle
changes
Debridement
Callus andnecrotic tissue
Moisture Balance
Control exudate
Infection Control
Rule out/treat osteomyelitis
3

What is a total contact cast?
A composite, anatomically conforming, below knee cast that is applied with minimal padding, enclosing the toes.
How does total contact casting work?
It effectively reduces plantar pressure and redistributes pressure to the cast:
Why is TCC Gold Standard?
n It allows for healing while ambulating
n It forces compliance*
n It provides an intimate “total contact” with forefoot, arch, heel, Achilles tendon, and lower leg
n It eliminates the propulsive phase of gait
n It shortens the stride length
n It protects the affected limb from trauma
n It minimizes vertical (ground reactive pressures) and shear stresses
*Total contact casting forces compliance
Armstrong et al.5 demonstrated that patients using removable cast walker for off-loading wore their device on average during only 28% of their total daily activity, and even the subset most adherent to their off-loading regimen still only wore the device for a total of 60% of their total daily activity. This highlights a key advantage of the total contact cast: it is a non-removable device, which the patient must wear 100% of the time, therefore increasing treatment efficacy.
Treating the Cause with Pressure Redistribution
Most diabetic foot specialists consider total contact casting as the pressure offloading Gold Standard in the treatment of non-infected DFU, neuropathic foot wounds and Charcot foot.1
1 American Diabetes Association. Consensus development conference on diabetic foot wound care. Diabetes Care 1999;22:1354-60.2 Shaw, J.E., et al. The mechanism of plantar unloading in total contact casts: implications for design and clinical use. Foot Ankle Int, 1997. 18(12): p. 809-17.3 Hartsell HD, Fellner C, Frantz R, et al. The repeatability of total contact cast applications: implications for clinical trials. J Prothèses et orthèses 13 (1) :4-7, 2001.4 Birke, JA, Sims DS, Buford WL. Walking casts: effect on plantar foot pressures. J Rehabil Res Dev 22:18-22, 1985.5 Armstrong DG, Lavery LA, Kimbriel HR, et al. Activity patterns of patients with diabetic foot ulceration: patients with active ulceration may not adhere to a standard pressure off-loading regimen. Diabetes Care 2003;26:2595-7.
Up to 30% of load is distributed to the cast wall2
Average forefoot offloading is 65%3
Pressure is reduced up to 84% at metatarsal heads4
4

Total Contact Casting is the Gold Standard
1 Armstrong DG, Nguyen HC, Lavery LA, et al. Off-loading the diabetic foot wound: a randomized clinical trial. Diabetes Care 2001;24:1019-1022.2 Mueller MJ, Diamond JE, Sinacore DR, et al. Total contact casting in treatment of diabetic plantar ulcers: controlled clinical trial. Diabetes Care 1989L12(6):384-8.3 Myerson M, Papa J, Eaton K, et al. The total-contact cast for management of neuropathic plantar ulceration of the foot. J Bone and Joint Surg; 74-A(2):261-269, 1992.
Total Contact Casting is the most effective offloading device in healing neuropathic foot wounds, as overwhelmingly validated by clinical results.
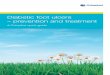
A study by Armstrong et al.1, involved 63 patients with non-infected neuropathic plantar foot ulcers and compared the TCC with a removable cast walker and a half shoe. All patients were followed for 12 weeks and had weekly visits for wound care and debridement.
Mueller et al.2 also compared the TCC with another treatment modality. Patients were randomized to receive TCC treatment or to avoid weight bearing and use sterile saline wet-to-dry dressings. The group treated with TCC showed 90.4% healed in an average of 33.5 days, as the non-TCC group showed 31.5% healed in an average of 65.0 days.
Myerson et al.3 used TCCs on 71 plantar ulcers. 90% of the ulcers healed at a mean duration of 5.5 weeks.
Those are just a few examples of the clinical evidence available supporting the use of total contact casting as pressure offloading device. In short:
n 18 studies (4 randomized) show total contact casting results in consistent healing of active diabetic foot wounds from 36-52 days for 85-95% of patients.
n A meta-analysis of 526 ulcers in 493 patients presented by Peter Cavanagh at the 2000 American Diabetes Association 60th Scientific Sessions, showed TCC use resulted in 88% healing in mean time of 43 days.
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
70
60
50
40
30
20
10
0
50.489.5%
33.5
61.0
65.0%58.3
Total Contact Cast
Removable Cast Walker
Half Shoe
Percent Healed
Mean Days to Healing
5

The kit provides several advantages such as:
n Standardized technique
n Optimal effectiveness
n Time savings
n Convenient all-in-one kit
n Increased compliance
BSN Medical also provides hands-on educational sessions, training material and on-site support.
One example of success with Cutimed® Total Contact Cast Kit
Introducing the Cutimed® Total Contact Cast Kit
BSN Medical is simplifying the pressure offloading Gold Standard solution!
The Cutimed® Total Contact Cast Kit has been developed in partnership with healthcare professionals dealing with diabetic foot ulcers every day. The result is a recipe that offers the most effective and comfortable TCC through an easy standardized technique. It combines specifically chosen and proven casting materials to provide an intimate comfortable close fit and proper pressure redistribution for an optimized healing environment.
Day 1 Day 4 Day 7
Day 14 Day 33 Day 47
6

Local Wound Care
Discover Cutimed® advanced wound care products from BSN Medical, an innovative wound management range which reliably covers all wound healing phases.Once the diabetic foot ulcer is being addressed with pressure offloading, adequate local wound care is required for optimal healing conditions. Especially designed to aid in the treatment of chronic wounds such as diabetic foot ulcers, our new Cutimed® range offers a complete selection of effective and patient-friendly products.
Local Wound Care
Infection Control
Cutimed® Gel
Moisture BalanceDebridement
Cutimed® Cavity
Cutimed® Sorbact® gel
Fixation: Leukomed® T, Hypafix® transparent
Cutimed® Sorbact®
dressing / pad
7
The Cutimed® Sorbact range has proved effective in infected diabetic ulcers and in preventing an infection. By a unique mode of action the microbial load is effectively reduced without using a chemically active agent, such as silver. Cutimed® Sorbact is not linked to undesirable side effects or bacterial resistance and supports the natural wound healing process.

BSN Medical Inc. • 4455 Autoroute Laval West, Suite 255 • Laval (QC) Canada • H7P 4W6Tel. 1-877-978-5526 • Fax 1-877-978-9703
PE
1106
15TC
C R
2
Ordering Information
The Cutimed® range of products offers high flexibility in the therapy of chronic wounds. Choose your dressing with the easy-to-use pictograms according to exudate level, wound depth and wound phase:
Wound DepthShallow
Deep
Shallow + deep
ExudateDry to low
Low to medium
Medium to high
High to excessive
Wound PhaseNecrotic
Sloughy
Granulation
Epithelization
Infected
Impregnated acetate fabric with an additional absorbent core for exudate management
Impregnated acetate fabric primary wound dressing for deep or superficial wounds
Sorbact dressing impregnated with hydrogel for the promotion of autolytic debridement
Cutimed® Sorbact® dressing 7216401 4 cm x 6 cm 5 dressings 7216400 4 cm x 6 cm 40 dressings 7216501 7 cm x 9 cm 5 dressings 7216500 7 cm x 9 cm 40 dressings
Cutimed® Sorbact® pad 7216101 7 cm x 9 cm 5 dressings 7216100 7 cm x 9 cm 40 dressings 7216201 10 cm x 10 cm 5 dressings 7216200 10 cm x 10 cm 40 dressings 7216300 10 cm x 20 cm 20 dressings
Cutimed® Sorbact® gel 7261100 7.5 cm x 7.5 cm 10 dressings 7261101 7.5 cm x 15 cm 10 dressings
Cutimed® Gel 7261000 8 g 10 tubes 7261001 15 g 10 tubes 7261002 25 g 10 tubes
Cutimed® Cavity 7262100 5 cm x 6 cm 10 dressings 7262101 10 cm x 10 cm 10 dressings 7262103 15 cm x 15 cm 05 dressings
Cutimed® Total Contact Cast kit Code Dimensions Box Contents 7349900 - 1 kitEverything you need for one total
contact cast
Hydrogel used on dry wounds to promote autolytic debridement and create a moist wound environment
Foam dressing used to protect the wound and absorb exudates and moisture