-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
1/24
Circulation Journal Vol.75, May 2011
CirculationJournal
OfficialJournaloftheJapaneseCirculationSociety
http://www.j-circ.or.jp
AaDO2: alveolar-arterial oxygen differenceACE: angiotensin
converting enzymeAPTT: activated partial thromboplastin timeBNP:
brain natriuretic peptideCABG: coronary artery bypass graftingCDT:
catheter-directed thrombolysisCT: computed tomographyCTEPH: chronic
thromboembolic pulmonary hypertensionCTR: cardiothoracic ratioDBP:
diastolic blood pressureDVT: deep vein thrombosisHIT:
heparin-induced thrombocytopeniaHLA: human leukocyte antigenHOT:
home oxygen therapyICU: intensive care unitINR: international
normalized ratioIPC: intermittent pneumatic compressionIVC:
inferior vena cavaMDCT: multi-detector CTMHLW: Ministry of Health,
Labour and WelfareMRA: magnetic resonance angiography
MRV: magnetic resonance venographyMSCT: multi-slice CTNHI:
National Health InsuranceNO: nitric oxideNYHA: New York Heart
AssociationPaCO2: partial pressure of arterial carbon dioxidePaO2:
partial pressure of arterial oxygenPCPS: percutaneous
cardiopulmonary supportPE: pulmonary embolismPEA: pulmonary
thromboendarterectomyPEEP: positive end-expiratory pressurePG:
prostaglandinPH: pulmonary hypertensionPT: prothrombin timePTCA:
percutaneous transluminal coronary angioplastyPTE: pulmonary
thromboembolismSBP: systolic blood pressureSpO2: peripheral oxygen
saturationUK: urokinaseVTE: venous thromboembolism
Abbreviations Used in the Guidelines
Released online March 25, 2011
Mailing address: Scientific Committee of the Japanese
Circulation Society, 8th Floor CUBE OIKE Bldg., 599 Bano-cho,
KarasumaAneyakoji, Nakagyo-ku, Kyoto 604-8172, Japan. E-mail:
[email protected]
This English language document is a revised digest version of
Guidelines for the Diagnosis, Treatment and Prevention of
PulmonaryThromboembolism and Deep Vein Thrombosis reported at the
Japanese Circulation Society Joint Working Groups performed in
2008.(website:
http://www.j-circ.or.jp/guideline/pdf/JCS2009_andod_h.pdf)
Joint Working Groups: The Japanese Circulation Society, The
Japan Radiological Society, The Japanese Association for Thoracic
Surgery,The Japanese Society for Vascular Surgery, The Japanese
Society on Thrombosis and Hemostasis, The Japanese Respiratory
Society,The Japanese Society of Phlebology, The Japanese Society
for Cardiovascular Surgery, The Japanese College of Cardiology
ISSN-1346-9843 doi: 10.1253/circj.CJ-88-0010
All rights are reserved to the Japanese Circulation Society. For
permissions, please e-mail: [email protected]
Guidelines for the Diagnosis, Treatment andPrevention of
Pulmonary Thromboembolism and
Deep Vein Thrombosis (JCS 2009)
Digest Version JCS Joint Working Group
Table of Contents
Abbreviations Used in the Guidelines 1258
Introduction to the Revised Guidelines 1259
I General Descriptions 1259 1. Acute Pulmonary Thromboembolism
1259 2. Chronic Pulmonary Thromboembolism 1261 3. Deep Vein
Thrombosis 1262
II Descriptions of Individual Diseases1263 1. Acute Pulmonary
Thromboembolism 1263
2. Chronic Pulmonary Thromboembolism 1268 3. Deep Vein
Thrombosis 1272 4. Prevention of Pulmonary Thromboembolism/
Deep Vein Thrombosis (VenousThromboembolism) 1275
References 1277
(Circ J 2011; 75:1258 1281)
JCS GUIDELINES
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
2/24
1259
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
The Japanese Circulation Society (JCS) has already
providedguidelines for the diagnosis and treatment of major
cardio-vascular diseases. The JCS decided to revise the
Guidelinesfor the Diagnosis, Treatment and Prevention of
PulmonaryThromboembolism and Deep Vein Thrombosis, which werefirst
completed in April 2004, to include new advanced tech-
niques of diagnosis and treatment of these conditions that
havebeen developed since publication of the first guidelines. Aswas
the case for the previous guidelines, the Working Groupsfor the
present guidelines consisted of cardiologists and car-diovascular
surgeons who have been involved in research onthe diagnosis,
treatment and prevention of pulmonary throm-boembolism (PTE).
Although the etiology and pathology of PTE have yet to
becompletely determined, it is known that deep vein thrombosis(DVT)
plays an important role in the development of PTE.PTE may thus be
considered a complication of DVT, and theseconditions are regarded
as a single disease entity that shouldbe called venous
thromboembolism (VTE). Treatment forPTE differs significantly
depending on whether the conditionis acute or chronic. Although
acute PTE is an emergent con-dition especially prevalent in Europe
and the United States, itis becoming increasingly prevalent in
Japan as well becauseof Westernization of Japanese lifestyle, the
rapid increase inpopulation of the elderly, increased recognition
of this dis-ease, and advancement of diagnostic techniques. Acute
PTEhas received much media attention as an economy-class syn-drome
and an unexpected secondary disaster following earth-quakes. It is
also a postoperative complication that shouldbe careful monitored
for in patients with prolonged bed restfollowing gastrointestinal
surgery, gynecologic treatment, ororthopedic surgery. Patients with
acute PTE require promptdiagnosis and appropriate treatment.
Patients with acute PTEoften respond well to thrombolytic therapy
and anticoagula-tion therapy, and new drugs have been approved and
are avail-able for this patient population. Patients with large
amountsof thrombus or circulatory collapse can be treated
effectivelywith catheterization and surgery. Inferior vena cava
(IVC)filters are used to prevent PTE, and the use of
non-permanentfilters (also referred to as temporal filters and
removable fil-ters) has become increasingly common. Chronic PTE
associ-ated with pulmonary hypertension (PH) is a serious
conditionthat causes right heart failure and respiratory failure
and doesnot respond well to conventional medical treatment.
However,
its prognosis has been improved by new drugs efficaciousin the
treatment of PH. Pulmonary thromboendarterectomy(PEA) with
cardiopulmonary bypass and deep hypothermicintermittent circulatory
arrest is performed as radical treat-ment of PTE, and has
significantly improved the outcome ofsurgery, clinical symptoms,
and cardiopulmonary hemody-
namics as well as the QOL of patients with central type
ofchronic PTE. Prevention of perioperative VTE by physicaltherapy
is quite important, and new drugs have becomeavailable for this
purpose.
The Working Groups revised the present guidelines, plac-ing
emphasis on currently available evidence whenever possi-ble, but it
should be noted that the present guidelines includeup-to-date
information that may be utilized by cardiologists,cardiovascular
surgeons, and other surgeons involved in sur-gical treatment of VTE
in the clinical setting as guidance fordiagnosis and treatment of
this disease. It should also be notedthat determination of
treatment by attending physicians basedon the specific conditions
and circumstances of their patientsshould take precedence over the
guidelines, and that the pres-ent guidelines provide no grounds for
argument in cases oflegal prosecution. The guidelines may be
revised in the futureto include description of newer methods of
diagnosis andtreatment of VTE.
We hope that the guidelines will aid physicians in thediagnosis,
treatment, and prevention of VTE.
In the present guidelines, levels of recommendation arerated
according to the following classification as used in
otherguidelines for the Diagnosis and Treatment of
CardiovascularDiseases.
Class I: Conditions for which there is evidence for
and/orgeneral agreement that the procedure or treatmentis useful
and effective.
Class II: Conditions for which there is conflicting
evidenceand/or a divergence of opinion regarding the
use-fulness/efficacy of a procedure or treatment.
Class IIa: The weight of evidence/opinion is in favor
ofusefulness/efficacy.
Class IIb: Usefulness/efficacy is less well established
byevidence/opinion.
Class III: Conditions for which there is general agreementthat a
procedure/treatment is neither useful norindicated and may be
harmful.
I General Descriptions
1. Acute Pulmonary Thromboembolism
1 EpidemiologyPTE becoming prevalent in Japan, and should no
longer beconsidered a rare condition. In 2006, PTE occurred in
7,864patients in Japan. The number of patients has increased
2.25-fold in the past decade,1and the incidence of this condition
isestimated to be 62 cases/million population. Since the inci-dence
of PTE in the United States is about 500 cases/millionpopulation,
that in Japan in 2006 is about one-eighth that inthe United
States.
The incidences of perioperative PTE in Japan were 4.41,
4.76, 3.62, and 2.79 cases/10,000 surgeries in 2002, 2003,2004,
and 2005, respectively. The incidence began to decreasein 2004 when
the guidelines for the prevention of PTE werepublished and
healthcare costs for preventive treatment beganto be covered by the
National Health Insurance (NHI) ofJapan.2
In Japan, acute PTE develops more frequently in femalesthan in
males. The most common age of onset is in the sixthand seventh
decades.3
2 Risk FactorsMajor risk factors for PTE are listed in Table 1.
Virchowstriad, ie, the presence of (1) interrupted blood flow, (2)
endo-
Introduction to the Revised Guidelines
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
3/24
1260
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
thelial dysfunction, and (3) hypercoagulability, is a
veryimportant set of factors that affect susceptibility to
thrombusformation.
3 Conditions of OnsetAcute PTE often occurs when patients stand
up or begin walk-ing or during micturition or defecation after
resting.3,4Sincethe major source of emboli is thrombi in veins of
the lowerlimbs or intrapelvic veins, it is believed that muscle
contrac-tion in the lower limbs increases venous return, with
themuscles acting in pump-like fashion to push blood, resultingin
release of thrombi that cause PTE.
4 PathophysiologyAcute PTE is caused by abrupt blockage of
pulmonary vesselsby thrombi that has formed in the veins or the
heart and hastraveled through the blood stream. The source of
emboli is theveins of the lower limbs or pelvis in more than 90% of
cases.The main manifestations of acute PTE are sudden onset of
PHand hypoxemia.5,6 Since the mean pulmonary arterial pres-
sure that can be generated by the right ventricle is 40 mmHgin
individuals without cardiopulmonary disease,7when pul-monary
arterial pressure exceeds 40 mmHg during the acutephase of PTE,
physicians should suspect acute-on-chronicPTE, ie, acute
exacerbation of chronic PTE due to the occur-rence of acute PTE, or
chronic PTE. Pulmonary infarction,which occurs as a hemorrhagic
infarction, develops in about10 to 15% of patients with acute
PTE,8,9often as a result ofocclusion of a peripheral pulmonary
artery.
5 Severity ClassificationSince the prognosis and rate of
recurrence of acute PTE differsignificantly by the presence or
absence of echocardiographicfindings of pressure overload in the
right ventricle, the sever-ity of acute PTE is commonly classified
according to clinicalsigns/symptoms and echocardiographic
findings,10as outlinedin Table 2.
6 Prognosis and Clinical CourseAccording to available data in
Japan, the mortality rate of
Table 1. Risk Factors for Pulmonary Thromboembolism
Acquired factors Congenital factors
Interrupted blood flow Prolonged bed
restObesityPregnancyCardiopulmonary disease (eg, congestive
heart
failure, chronic cor pulmonale)General anesthesiaAnesthesia of
the lower limbs
Plaster bandage of the lower limbsVaricose veins in the lower
limbs
Endothelial dysfunction SurgeriesTrauma, fracturesCentral venous
catheterizationCatheter test/interventionVasculitisAntiphospholipid
syndromeHyperhomocysteinemia
Hyperhomocysteinemia
Hypercoagulability Malignant tumorsPregnancySurgeries, trauma,
fracturesBurnsDrugs (eg, oral contraceptives,
estrogens)InfectionsNephrotic syndromeInflammatory bowel
disease
Myeloproliferative disorders, polycythemiaParoxysmal nocturnal
hemoglobinuriaAntiphospholipid syndromeDehydration
Antithrombin deficiencyProtein C deficiencyProtein S
deficiencyAbnormal plasminogenAbnormal fibrinogenIncrease in tissue
plasminogen activator inhibitorAbnormal thrombomodulinActivated
protein C resistance (Factor V Leiden)*
Prothrombin gene mutation (G20210A)*
*Not observed in Japanese population.
Table 2. Classification of Clinical Severity of Acute Pulmonary
Thromboembolism
HemodynamicsRight heart overload observed
on echocardiography
Cardiac arrestCollapse
Cardiac arrest or circulatory collapse Present
Massive UnstableShock or hypotension (defined as a systolic
blood
pressure of 15 minutes or adecrease in blood pressure by >40
mmHg, regard-less of the presence/absence of new onset
ofarrhythmia, dehydration or sepsis)
Present
Submassive Stable (absence of the above findings) Present
Non-massive Stable (absence of the above findings) Absent
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
4/24
1261
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
acute PTE is 14% overall, 30% among patients with cardio-genic
shock (20% among those receiving thrombolytic ther-apy and 50%
among those not receiving it), and 6% amongpatients without
cardiogenic shock.3 According to data inEurope and the United
States, the mortality rate of acute PTEis as high as 30% when it is
not diagnosed and treated prompt-ly, but decreases to 2 to 8% when
appropriate treatment isperformed.11,12It is known that early
diagnosis and appro-priate treatment decrease the mortality rate
substantially.
Independent determinants of mortality of acute PTE includeright
ventricular dysfunction on echocardiography, advancedage (70
years), cancer, congestive heart failure, chronic ob-structive
pulmonary disease, hypotension, and tachypnea.13
In a follow-up study in Japan, PH developed in 3.7% inpatients
with acute PTE.14In the United States, it has beenestimated that PH
secondary to chronic PTE develops in 0.1to 3.8% of patients with a
history of acute PTE.1517
2. Chronic Pulmonary Thromboembolism
1 DefinitionChronic PTE develops as a result of chronic
occlusion of pul-monary arteries by organized thrombi. In Japan,
chronic PTEis defined as abnormal pulmonary blood flow
distributionand pulmonary circulation hemodynamics that persist
for6 months without substantial changes.18Some patients withchronic
PTE exhibit clinical manifestations such as shortnessof breath
during exercise (exertional dyspnea) due to throm-botic occlusion
of several pulmonary arteries, which causesPH. This condition is
referred to as chronic thromboembolicpulmonary hypertension
(CTEPH). CTEPH is classified byclinical course into two types, ie,
recurrent CTEPH with ahistory of signs/symptoms suggestive of acute
PTE, and latentCTEPH with progression of PH but without clear
clinicalfindings of acute PTE. Patients with mild CTEPH are
treatedwith medical treatment mainly consisting of anticoagula-tion
therapy to prevent progression of disease, while patientswith
severe PH may also have right heart failure and a
poorprognosis.19,20In 1998, the Ministry of Health, Labour
andWelfare (MHLW; formery Ministry of Health and Welfare)of Japan
termed CTEPH idiopathic chronic PTE with PHand designated it a
specific disease for which healthcare costsare covered by public
expenditure. In the present guidelines,however, the term CTEPH is
used.
2 EpidemiologyThe incidence of PTE, including acute and chronic
PTE, inJapan is believed to be lower than in Europe and the
UnitedStates. According to data in annual reports on
pathologicautopsy cases, the incidence of acute PTE in Japan is
aboutone-tenth that in the United States,21although these data
arerather old. In the United States, it is estimated that acute
PTEoccurs in 0.5 to 0.6 million individuals each year, and
thatCTEPH occurs in about 0.1 to 0.5% of patients surviving
theacute phase of PTE.15,16However, a recent report noted thatCTEPH
occurred in 3.8% of patients with a history of
acutePTE.17Physicians should be aware of the risk of progressionto
CTEPH when treating patients with acute PTE.
In Japan, the Specific Disease Respiratory Failure StudyGroup of
the MHLWestablished criteria for the diagnosis ofCTEPH and
conducted a nationwide survey in 1997.22Thenumber of patients with
CTEPH was estimated to be 450(95% confidence interval: 360 to
530).23,24The MHLW thendesignated CTEPH a specific disease and has
conducted an
annual epidemiological survey of it. In 2006, a total of 800
pa-tients with CTEPH were provided with medical care certifi-cates
for the treatment of a specific disease. Assessment ofcase reports
on 520 of the 800 patients with CTEPH revealedthat female patients
were predominant, with a female to maleratio of 2.8:1, and that the
mean age of patients was 6213 years. Female patients were
predominant, especially amongthose over 40 years of age, with no
gender difference observedin younger patients.25
3 EtiologyThe mechanisms of onset of CTEPH are still uncertain.
InEurope and the United States, CTEPH is considered a
chroniccondition occurring in patients with a history of acute
PTEcaused by DVT. In a nationwide survey in Japan, only 28%of
patients with CTEPH had DVT.24Although some patientswith CTEPH had
known risk factors for DVT, such as coagu-lopathy (such as presence
of antiphospholipid antibodies anddeficiency of antithrombin,
protein C, or protein S), heart dis-ease, and malignant tumors,
43.9% of patients assessed hadno apparent underlying conditions.
Frequencies of human leu-kocyte antigen (HLA)-B*5201 and
HLA-DPB1*0202 werehigh among patients with a particular type of
CTEPH, and inpatients carrying HLA-B*5201 and/or -DPB1*0202, the
fre-quency of DVT was significantly lower than in other
patients.26These findings suggest that there may be a different
mecha-nism of onset of CTEPH in the Japanese population not
sharedby Western populations. Some patients with CTEPH mayremain
asymptomatic for several months to years followinga period with
findings suggestive of acute PTE. This asymp-tomatic period is
referred to as a honeymoon period.15Although the mechanism of
latent progression of PH isunknown, several hypotheses, including
repetition of latentthrombosis and progression of thrombosis in the
pulmonaryarteries, have been suggested. Recently, the involvement
ofsmall vessel disease in the pathogenesis of CTEPH has
beenhypothesized.27
4 Clinical ManifestationsAlthough there are no symptoms specific
to CTEPH, almostall patients experience exertional dyspnea. Abrupt
dyspneaand chest pain develop repeatedly in patients with
repetitiveCTEPH, while exertional dyspnea becomes severe over
timein patients with latent CTEPH without apparent recurrence.Other
symptoms such as chest pain, dry cough, and syn-cope, may develop
as well, and bloody sputum and fever maydevelop in patients
complicated by pulmonary bleeding andpulmonary infarction. Patients
with right heart failure due toPH may exhibit abdominal distension,
body weight gain, andedema of the lower legs.
5 DiagnosisThe diagnosis of CTEPH is made according to the
criteriafor diagnosis of idiopathic chronic PTE with PH
describedbelow. Contrast multi-slice computed tomography
(termedmulti-slice CT [MSCT] or multi-detector CT [MDCT]) isuseful
in the diagnosis and differential diagnosis of CTEPH.However,
pulmonary angiography is required to determinewhether surgery is
indicated.
6 PrognosisAccording to a report by Riedel et al and the results
of asurvey of CTEPH in Japan, the prognosis of patients witha mean
pulmonary arterial pressure during the stable periodof 30 mmHg is
poor.19,20 The prognosis of patients under-
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
5/24
1262
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
going medical treatment has recently improved. However,since
there are patients whose QOL and vital prognosis areimproved
significantly following surgery (PEA), accuratediagnosis and
severity classification are essential in consider-ing whether
patients are indicated for surgery, including thedetermination
whether lesions are surgically accessible andwhether significant
disorder of major organs is present.
7 TreatmentSince the prognosis of patients receiving medical
treatmentalone is poor, physicians should consider PEA when the
or-ganized thrombi are surgically accessible and no
significantdisorders are observed in other major
organs.15,16,18,2834 Inpatients in whom the proximal ends of the
organized thrombiare located in lobe arteries or main pulmonary
arteries, sig-nificant improvement of pulmonary hemodynamics,
QOL,and prognosis may be obtained after successful PEA.3034Ithas
also been reported that surgery may improve the pulmo-nary
hemodynamics and QOL of patients in whom thrombi arelocated in
segmental arteries.32,34Recent reports have notedthat drugs for the
treatment of pulmonary arterial hyperten-sion are effective in the
treatment of patients with CTEPHnot indicated for surgery.3337
3. Deep Vein Thrombosis
1 DefinitionThe veins of the extremities are classified into
superficialveins that lie above the fascia and deep veins that lie
underthe fascia. Acute venous thrombosis is thus classified as
DVTaffecting deep veins and thrombophlebitis affecting superfi-cial
veins. The manifestations of DVT depend on the locationof affected
veins. The present guidelines mainly describeDVT in the veins of
the pelvis and lower limbs.38
2 EpidemiologyAt autopsy, DVT is observed in 24 to 60% of
patients
who died in hospital in Europe and the United States and0.8% of
those in Japan.3941In an epidemiological survey, theVenous Disease
Survey Committee of the Japanese Societyof Phlebology in 1997
reported that DVT occurred in 506 pa-tients per year,42while the
number of new patients with DVTwas estimated to be 14,674
patients/year,1 ie, 12/100,000population/year, in a questionnaire
survey conducted by theJapanese Society of Pulmonary Embolism
Research in 2006.These findings reflects the fact that the
incidence of DVT
has increased about 30-fold during the last decade. On theother
hand, the annual incidence of DVT in Europe and theUnited States
were calculated as 50/100,000 population/yearon the basis of
reports published between 1976 and 2000.43The incidence of DVT in
Japan has increased rapidly to aboutone-fourth those in Europe and
the United States.
3 Etiology and Risk FactorsThe major causes of venous thrombus
are venous endo-thelial dysfunction, hypercoagulability, and
interruption ofvenous blood flow.44 The development of DVT
involvesthese major causes as well as various other risk factors
ofvarious strengths38,45 (Table 3). Most cases of DVT in theveins
in the neck and upper limbs are iatrogenic, and causedby the
placement of an intravenous line, pacemaker catheter,or
hemodialysis shunt, and cases of thoracic outlet syndromeare also
observed. DVT in the superior vena cava developsin patients with
superior vena cava syndrome in whom DVTis typically caused by
mechanical compression of this vein bymediastinal tumor. DVT in the
IVC often develops as a resultof extension of thrombus from veins
in the pelvis or lowerlimb. Cases of IVC filter thrombosis and of
Budd-Chiari syn-drome are also observed. In the veins in the pelvis
and lowerlimb, DVT may develop as a result of venous compressiondue
to congenital iliac bands and webs in the pelvis, iliaccompression
by the iliac artery, insertion or placement of acatheter into the
femoral vein, or bed rest with limited legmovement. Cases of DVT in
the lower legs are predomi-nant.45,46DVT in the lower leg often
develops in the veins ofthe soleus muscle,38,47which receive blood
from the medial,central, and lateral parts of the lower leg,4851
and the veinrunning through the central portion of the soleus
muscle islargest and the main location of DVT.48
4 PathophysiologyThrombus in a vein adheres to the venous wall
over a periodof several days after thrombus formation as a result
of in-flammatory changes, and then regresses due to
organization.Although venous valves included within the lesion may
bedamaged, some valves maintain function.38,45 Blood flowrecovers
after lysis or regression of thrombi during the acutephase. During
the chronic phase, recovery of blood flowoccurs after organization
or recanalization of thrombi. Thrombiin the popliteal vein and the
distal veins disappear almostcompletely in several days to several
weeks, while thrombiin the proximal leg veins remain as fibrotic
bands, althoughabout 50% of such thrombi regress within one year
after for-mation.52The central edge of thrombus can become
embolicor a source of emboli. While white thrombi and mixedthrombi
tend to adhere to the venous wall, red thrombi donot adhere to the
venous wall tightly and are easily detachedfrom the vascular wall
and cause embolism.53Thrombus inveins in the pelvis and lower limbs
are detached duringmovement of the hip and knee joints in the
supine or sittingposition. During walking, thrombi are detached
from the wallas a result of calf muscle pump function.49Embolism
often
Table 3. Risk Factors for Deep Vein Thrombosis
Risk factors
Demographics/environment
ElderlyProlonged sitting: During trips and duringdisasters
Pathology Trauma: Leg fractures, leg palsy, spinal
injuriesMalignant tumorsCongenital hypercoagulability: Coagulation
in-
hibitor deficiencies
Acquired hypercoagulability: Following surgeryHeart
failureInflammatory bowel disease, antiphospholipid
syndrome, vasculitisVaricose veins of lower
limbsDehydration/polycythemiaObesity, pregnancy, postpartum
statusCongenital iliac bands and webs, iliac compres-
sion by the iliac arteryHistory of venous thromboembolism:
Vein
thrombosis, pulmonary thromboembolism
Treatment Surgeries: Orthopedic surgery, neurosurgery,abdominal
surgery
Drugs: Female hormone, hemostatics, cortico-steroids
Catheter test/interventionProlonged bed rest: Management of
severe
patients, postoperative patient management,patients with
cerebrovascular disorders
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
6/24
1263
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
occurs within one week after formation or progression
ofthrombus, but may recur depending on the amount of move-ment of
the lower limbs and blood flow in the central edgeof
thrombus.47,50The severity of PTE correlates with the sizeof emboli
and frequency of formation of emboli. Severe PTEis often caused by
thrombus in leg veins above the popli-teal vein, especially the
femoral vein, but may be caused bythrombi in soleus
veins.47,49,50Although the source of emboliis uncertain in 30 to
60% of patients with PTE,38,45autopsy
has frequently revealed the presence of new and old sourcesof
emboli in the veins of lower limbs.50
5 Typing and Staging of DVTDVT in the pelvis and lower limb is
classified into centraltype of DVT (iliac DVT and femoral DVT),
which occurs inveins above the popliteal vein, and peripheral type
of DVT(lower leg DVT), which occurs in popliteal vein and
distalveins. In the present guidelines, DVT is also classified
basedon clinical signs/symptoms and severity of anomalous
venousdrainage into acute and chronic phases. Signs and symptomsof
acute anomalous venous drainage include swelling, pain,and skin
color change in patients with central type of DVT.In patients with
iliac DVT with diffuse occlusion, venousnecrosis due to poor
arterial perfusion develops in the acutephase. It is of practical
use to classify the severity of clinicalsigns/symptoms according to
the presence/absence of pain-ful swelling, painful swelling with
discoloration (phlegmasiaalba dolens [milk leg], phlegmasia cerulea
dolens [blue leg]),and venous necrosis.38,54 Although peripheral
type of DVTtypically causes pain, many patients are asymptomatic.
Impor-tant findings of physical examination include the presence
of
thrombosed veins or tenderness on palpitation (direct find-ings)
and hard lower leg muscles (indirect finding).38,54WhenDVT recurs
during the chronic phase, the patient exhibitssigns and symptoms
characteristic both the acute and chronicphases of DVT.
6 Prognosis and RecurrenceThe short-term prognosis of DVT in the
pelvis and lowerlimb depends on the presence/absence and severity
of acute
anomalous venous drainage, acute PTE, and arterial embo-lism.
Acute anomalous venous drainage often subsides withinseveral months
after onset. Acute PTE is the most serious con-dition,45,55and
requires both primary and secondary preven-tion. In patients with
arterial embolism, the presence/absenceof patent foramen ovale must
be confirmed.56The long-termprognosis of DVT depends on the
presence/absence and sever-ity of post-thrombotic syndrome,
recurrent DVT, chronic PTE,and arterial embolism.38,45,54
Post-thrombotic syndrome de-velops in about 40% of patient with
central type of DVT,57and is caused by abnormal valves in
perforating arteries andsuperficial veins. When DVT recurs, acute
manifestationsare observed, and the incidences of PTE and
post-throm-botic syndrome are increased.58Early treatment improves
theprognosis of patients with DVT. Patients with recurrent
DVTfollowing anticoagulation therapy must be assessed for
throm-bophilia.59,60To ensure prevention of recurrent DVT,
patientsmust continue exercise and compression therapy as well
asanticoagulation therapy for an appropriate length of time.
Theduration of anticoagulation therapy should be
determinedconsidering the reversibility of risk factors and whether
thecondition is idiopathic and/or permanent.45,60
II Descriptions of Individual Diseases
1. Acute Pulmonary Thromboembolism
1 DiagnosisAccurate diagnosis of acute PTE is difficult, since
no physical
or laboratory findings are specific to acute PTE.
Physiciansshould suspect acute PTE when the following
non-specificfindings are present. Acute PTE should be included in
thedifferential diagnosis if patients have dyspnea that cannot
beexplained by other causes.
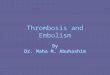
Figure 1. Steps in the diagnosis of acute pulmonary
thromboembolism. Start heparin therapy when pulmonary embolism
issuspected. Examine for deep vein thrombosis at once. *1Screen the
patient with chest X-ray, ECG, arterial blood gas
analysis,transthoracic echocardiography, and blood chemistry.
*2When PCPS is not available, maintain circulation with cardiac
compres-sion and vasopressors. CT, computed tomography; PCPS,
percutaneous cardiopulmonary support. Adapted from
TherapeuticResearch2009; 30:744 747.
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
7/24
1264
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
(1) SymptomsThe absence of symptoms specific to acute PTE is a
majorreason for delay or lack of diagnosis of this disease. Its
com-mon and major symptoms are dyspnea and chest
pain.3,6164Typically, such symptoms develop when patients begin
walk-ing after bed rest, when they urinate or defecate, or whenthey
change posture.
(2) Clinical FindingsTachypnea and tachycardia are frequently
present.62,65Shockand hypotension may develop as well. DVT may
cause swell-ing of the lower legs and Homans sign, etc.
(3) ExaminationsFigure 1 illustrates the recommended steps in
diagnosis. Itshould be noted that the flow chart reflects currently
avail-able techniques.66
[Levels of Recommendations]1. MSCT, pulmonary angiography,
pulmonary scintigraphy,
arterial blood gas analysis, D-dimer: Class I2. Transthoracic
echocardiography, magnetic resonance an-
giography (MRA): Class IIa3. Transesophageal echocardiography:
Class IIb
2 Treatment(1) IntroductionIn the treatment of acute PTE, it
should be noted that (1)prompt diagnosis and treatment are
essential, since the prog-nosis after successful treatment during
the acute phase isexcellent, and that (2) after achievement of
stable hemody-namics patients should be carefully followed for
recurrence ofPTE and should be treated promptly when DVT develop.
Themain component of treatment of PTE is pharmacological
anti-thrombotic therapy, and anticoagulants and thrombolyticsshould
be used appropriately based on the severity of thepatients
condition. Patients with a high risk of bleeding shouldadditionally
be treated with non-permanent IVC filters andcatheter intervention
to support drug treatment, and percuta-neous cardiopulmonary
support (PCPS) and surgical throm-bectomy should be performed for
patients with severe condi-tion. Physicians should also assess
whether any DVT remainsas soon as possible to consider whether IVC
filters are indi-cated. Figure 2shows an example of an algorithm of
treat-ment during the acute phase of PTE. It should be noted
thatthis algorithm involves basic concepts and should be
modifiedappropriately according to the condition of individual
patientsand hospital policies.
(2) Cardiopulmonary ManagementThe main pathological feature of
acute PTE is acute cardio-
Figure 2. An example of a treatment algorithm for acute
pulmonary thromboembolism. *1When risk of bleeding is high.
*2Treatcomplications appropriately with available methods.
*3Unstable hemodynamics consistent with shock or prolonged
hypo-tension. *4Condition requiring cardiopulmonary resuscitation
or prolonged severe shock. *5Consider PCPS according to
hospitalequipments and patient condition. *6Select appropriate
treatment according to hospital equipments and patient
condition.*7Evaluate based on right ventricular enlargement on
echocardiography and severity of pulmonary hypertension. *
8Presence/absence of DVT which may have serious effects if it
releases emboli causing recurrent embolism. The above algorithm is
an ex-ample. Each institution should select appropriate methods
according to its healthcare resources. DVT, deep vein
thrombosis;PCPS, percutaneous cardiopulmonary support; IVC,
inferior vena cava.
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
8/24
1265
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
pulmonary failure. Since mortality is particularly high
imme-diately after the onset of PTE,67appropriate
cardiopulmonarymanagement is quite important.
1) Respiratory ManagementPatients with acute PTE typically
exhibit hypoxemia andhypocapnia (type I respiratory failure).68
Oxygen therapyshould be initiated for patients with an partial
pressure ofarterial oxygen (PaO2) of 60 Torr (mmHg) (or a
peripheraloxygen saturation [SpO2] of 90%).
Nasal cannulas, an oxygen mask, or an oxygen mask withreservoir
bag should be used as appropriate.
When oxygen therapy does not achieve a PaO2of 60 Torr(SpO290%),
intubation and mechanical ventilation shouldbe initiated.69During
mechanical intubation, the tidal volumeshould be set at a low
level, 7 mL/kg, to avoid increase inintrathoracic pressure.10
2) Circulatory ManagementAlthough severity varies depending on
the degree of occlu-sion in the pulmonary vascular bed, patients
often exhibit PH,right heart overload, decreased right cardiac
output, decreasedleft cardiac output, and/or shock. Theoretically,
treatmentshould include drugs that have cardiotonic effects and
widenthe pulmonary artery.
There is no evidence to recommend volume loading. It hasbeen
pointed out that excessive volume loading in the rightventricle may
compress the left ventricle and decrease leftcardiac output.70Drug
treatment (the drugs of first choice aredopamine and
dobutamine;71norepinephrine72is effective inpatients with
hypotension; phosphodiesterase III inhibitorsrequire further
evaluation to accumulate clinical data), nitricoxide (NO)
inhalation, and other appropriate treatment shouldbe performed.
Patients with cardiopulmonary arrest and those not re-sponding
well to drug treatment (patients with progressivehypotension)
should be treated promptly with PCPS and beconsidered for surgical
thrombectomy.73,74
[Levels of Recommendations]1. Respiratory management (oxygen
therapy and low tidal
volume ventilation): Class I2. Circulatory management Volume
loading: Class III Dopamine: Class IIa Dobutamine: Class IIa
Norepinephrine: Class IIa Use of PCPS in severe patients: Class
I
Table 4. Dose Adjustment Table for Unfractionated Heparin for
Continuous Infusion*1
APTT(sec)
Bolus(units)
Hold(min)
Rate change(mL/hr)*2
Dose change(units/24 hr)
Repeat APTT
120 0 60 4 3,840 6 hrs later
Unfractionated heparin should be administered intravenously as
an initial bolus dose at 5,000 units, followed bycontinuous
infusion at 1,400 units/hr. Six hours after the initial
administration of unfractionated heparin, APTT shouldbe determined
for adjustment of the dose according to the above table.*1Use this
table for APTT reagents with a therapeutic range of 1.9 to 2.7
times the control.*2
When unfractionated heparin is administered at a concentration
40 units/mL.APTT, activated partial thromboplastin time; Bolus,
bolus dose for repeated administration; Hold, duration of
suspen-sion of continuous infusion; Rate change, change in infusion
rate during continuous infusion; Dose change, change indose during
continuous infusion.Adapted from Cruickshank MK, et al. A standard
heparin nomogram for the management of heparin therapy. Arch
InternMed1991; 151:333 337, with permission from American Medical
Association. Added Dose change to this table.
Table 5. Contraindications to Thrombolytic Therapy
Absolute contraindications
Active internal bleeding
Recent spontaneous intracranial bleeding
Relative contraindications
Major surgery, delivery, organ biopsy or puncture of
non-compressible vessels within 10 days
Ischemic stroke within 2 months
Gastrointestinal bleeding within 10 days
Severe trauma within 15 days
Neurosurgery or ophthalmologic surgery within 1 month
Uncontrolled severe hypertension (SBP >180 mmHg,DBP >110
mmHg)
Recent cardiopulmonary resuscitation
Platelet count
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
9/24
1266
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
(3) Drug Treatment
1) Initial TreatmentThe major components of the treatment of
acute PTE are anti-coagulation therapy and thrombolytic therapy.
The treatmentof choice is anticoagulation therapy using
unfractionatedheparin.75,76This should be performed in all patients
unlessanticoagulation is contraindicated. When acute PTE is
strong-ly suspected or a long period of time is required to
confirm
the diagnosis, treatment may be initiated before confirmingthe
diagnosis. Unfractionated heparin should be administeredas a single
intravenous dose of 80 units/kg or 5,000 units,followed by
continuous intravenous infusion at 18 units/kg/hror 1,300 units/hr.
The dose should be adjusted to maintainan activated partial
thromboplastin time (APTT) of 1.5 to2.5 times the control value
(Table 4).77Infusion of unfrac-tionated heparin should be continued
until control of anti-coagulation with warfarin is established.
Thrombolytic therapy is performed to promptly improvepulmonary
circulation by dissolving thromboemboli, and isalso used for the
treatment of patients with massive acute PTEwith unstable
hemodynamics or echocardiography-provenenlargement of the right
heart.78Monteplase, a recombinanttissue plasminogen activator, is
the only drug officially indi-cated for the treatment of acute PTE
in Japan.79The recom-mended regimen in adults is intravenous
administration of13,750 to 27,500 units/kg over about 2 minutes.
Table 5listscontraindications to thrombolytic therapy.10Although
throm-bolytic therapy has been proven to be clearly superior to
anti-coagulation therapy in ensuring prompt dissolution of
thrombiand improvement of hemodynamics,7983 no difference
inprognosis has been observed in randomized studies of
throm-bolytic therapy and anticoagulation therapy.
The current criteria for drug treatment for acute PTE areas
follows:(1) Anticoagulation therapy is the treatment of choice
for
normotensive patients without right heart dysfunction.(2)
Normotensive patients with right heart dysfunction should
be carefully assessed for expected benefits and risk ofbleeding
in considering whether thrombolytic therapy isa treatment
option.
(3) Thrombolytic therapy is the treatment of choice for
pa-tients with persistent shock and hypotension unless it
iscontraindicated.
2) Long-Term TreatmentFollowing treatment with unfractionated
heparin, warfarintherapy is used. Warfarin therapy should be
initiated duringthe early phase of treatment with unfractionated
heparin, andthe dose of warfarin should be adjusted to achieve an
optimalprothrombin time and international normalized ratio
(PT-INR).The initial dose is 3 to 5 mg in many cases. Warfarin
therapyshould be continued when the risk of recurrent PTE is
higherthan the risk of bleeding, and the duration of warfarin
therapywill vary depending on the presence and types of risk
factors(Table 6). The optimal target range of warfarin therapy is
2.0to 3.0 PT-INR in foreign countries84,85but is 1.5 to 2.5
PT-INRin Japan because of the risk of bleeding.
[Levels of Recommendations]Class I
1. During the acute phase of acute PTE, unfractionatedheparin
should be administered to achieve an APTT of1.5 to 2.5 times the
control value for a period of timeuntil the effects of warfarin are
stabilized.
2. Warfarin should be administered during the chronicphase of
acute PTE. The duration of warfarin therapyshould be 3 months for
patients with reversible risk fac-tors and at least 3 months for
patients with congenitalcoagulopathy and those with idiopathic VTE.
Warfarinshould be administered for a longer period of time
topatients with cancer and those with recurrent PTE.
3. In patients with persistent shock, hypotension, and un-stable
hemodynamics, thrombolytic therapy should be
performed during the acute phase of acute PTE.Class IIa
1. During the acute phase of acute PTE, thrombolytictherapy
should be performed in normotensive patientswith right heart
dysfunction.
Class IIb1. During the treatment of acute PTE, the dose of
warfarin
should be adjusted to achieve a PT-INR of 1.5 to 2.5.
(4) Catheter InterventionCatheter intervention is indicated for
patients with acute mas-sive PTE with unstable hemodynamics despite
other appro-priate treatment.86,87Catheter interventions include
catheter-directed thrombolysis (CDT) and catheter
fragmentation/aspiration thrombectomy.
1) Catheter-Directed ThrombolysisUse of catheters to inject
thrombolytics directly to thrombusin the pulmonary arteries is not
currently supported.88Appro-priate methods of injection such as the
pulse-spray techniqueshould be used to ensure the efficacy of
treatment.
2) Catheter Fragmentation/Aspiration ThrombectomyCatheter
interventions other than catheter-directed throm-bolytic therapy
include aspiration thrombectomy, thrombusfragmentation, and
rheolytic thrombectomy. These techniquesare followed by
thrombolytic therapy in most cases. It hasbeen suggested that the
clinical results of these techniquesare comparable to that of
surgical thrombectomy.89Efficacyevaluation should be based on
improvement of hemody-namics and oxygenation, and angiographic
findings shouldnot be overemphasized.90 Physicians should be aware
thatcomplications 91 such as injury of vascular walls,
peripheralembolism, recurrent thrombosis, traumatic hemolysis,
andblood loss may occur.
(a) Aspiration ThrombectomyThe Greenfield embolectomy device has
not yet been approvedin Japan. Aspiration thrombectomy using
guiding cathetersfor percutaneous transluminal coronary angioplasty
(PTCA)has attracted attention because of its simplicity and
excellentclinical results.92 On the other hand, catheters designed
topercutaneously remove thrombus from the coronary arteriesare not
useful in the treatment of acute PTE because of theirlow suction
power.
(b) Thrombus FragmentationThrombus fragmentation is performed to
directly break athrombotic mass in a proximal pulmonary artery and
redis-tribute microemboli into peripheral vessels.93 Although
thethrombi are not recovered, small fragments of a thromboticmass
will respond better to thrombolytic therapy because thetotal
surface area exposed with thrombolytics will be in-creased
significantly. Currently used methods of fragmenta-tion include
cutting a thrombotic mass by rotating a pigtailcatheter94 and
crushing it with a balloon catheter. Hybrid
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
10/24
1267
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
treatment techniques combining fragmentation and
aspirationthrombectomy using guiding catheters have been proposedto
prevent distal emboli associated with fragmentation, andhave
achieved excellent results.95
(c) Rheolytic ThrombectomyRheolytic thrombectomy is a
theoretically safe method sincethrombi are removed, but is in many
cases ineffective whenused alone to treat acute PTE.
[Levels of Recommendations]1. CDT: Class IIb The efficacy of
simple injection of a thrombolytic agent
into the affected pulmonary artery does not differ fromthat of
systemic administration of the drug.
2. Catheter fragmentation/aspiration thrombectomy: ClassIIb
Aspiration thrombectomy Thrombus fragmentation Rheolytic
thrombectomy
(5) Surgical Treatment
1) Indications for Surgery
(a) Treatment Strategies for Acute PTEWhen a diagnosis of acute
PTE is made, anticoagulationand/or thrombolytic therapy should be
promptly initiated.However, since exacerbation of acute PTE may be
observedand cardiac arrest may occur during the course of
throm-bolytic therapy, patients should be carefully monitored
andconsidered for surgery throughout medical treatment. Manyreports
have indicated that surgical treatment improves thecondition of
patients with unstable hemodynamics due to mas-sive PTE, and recent
surgical techniques may achieve favor-able results in patients with
massive PTE.9698 Treatmentstrategies for patients who develop PTE
following surgeryshould be determined in accordance with the type
of surgeryand the general condition of patients.
(b) Indications for Surgical ThrombectomyIn patients with
circulatory failure or shock due to acute mas-sive PTE causing
rapid occlusion of the pulmonary arterialtrunk or both right and
left main pulmonary arteries, promptrecanalization of the occluded
pulmonary arteries is essen-tial.99Surgical pulmonary thrombectomy
under cardiopulmo-nary bypass is indicated for these patients. In
patients with-out shock, conventional surgical pulmonary
thrombectomyis indicated, among other conditions, (1) when
tachycardiapersists in the absence of hypotension and medical
treatmentis not effective; (2) when thrombus is observed in the
pul-monary arterial trunk or both right and left main
pulmonaryarteries, and heart failure and/or respiratory failure is
rapidlyprogressive; (3) when thrombolytic therapy is
contraindicated;and (4) when free thrombus is present in the right
atriumand/or ventricle.100
When post-surgical patients or bedridden patients experi-ence
the abrupt onset of circulatory collapse before the diag-nosis of
acute PTE and medical treatment is not effective,PCPS must
immediately be initiated in the ward.101 Whensuch patients are
confirmed not to have fatal cerebral com-plications and are
diagnosed with shock due to acute PTE,pulmonary thrombectomy should
be performed.
2) Methods of SurgerySurgical thrombectomy for the treatment of
acute PTE in-volves incision of the affected pulmonary artery to
removethrombus under cardiopulmonary support.74When poor
car-diopulmonary kinetics are observed before surgery,
femoralveno-arterial cardiopulmonary support should be
initiatedpromptly as a supportive measure. When shock develops ina
patient in the ward, PCPS should be initiated before thepatient is
transferred to the operating room.
Following median sternotomy, cardiopulmonary support
isinitiated. An incision is made into the pulmonary arterial
trunkand, when necessary, the right main pulmonary artery to
re-move thrombus. In patients with acute PTE, soft,
rod-shaped,relatively fresh red thrombi may be removed. Although
throm-bus in peripheral arteries should also be removed
wheneverpossible, postoperative thrombolytic therapy is effective
indissolving peripheral thrombus when most central thrombusis
removed during surgery. Surgical thrombectomy may beperformed
during a beating heart procedure. However, whensmall thrombi are
located in many segmental arteries orthrombi are tightly adherent
to the vascular wall, thrombec-tomy should be performed during an
arrested heart procedure.
3) Results of Surgical Pulmonary ThrombectomyStein et al
reviewed 46 reports on 1,300 cases of surgical pul-monary
thrombectomy performed from 1985 to 2006, andreported that the
mortality of patients undergoing pulmo-nary thrombectomy was
20%.102According to annual reportsby the Japanese Association for
Thoracic Surgery, a total of539 patients with acute PTE underwent
surgical pulmonarythrombectomy during the 7-year period between
2000 and2006, and the in-hospital mortality was 21.2%. The results
inJapan are similar to or better than those in foreign
countries.The results are fairly good given the severe condition
ofpatients. During the period between August 1996 and October2006,
the Japanese Society of Pulmonary Embolism Researchconducted a
survey in 60 institutions in Japan, and a total of32 patients who
underwent pulmonary thrombectomy forthe treatment of acute PTE were
registered.103Mean age was5717 years, and 21 patients (66%) were
female. The initialpresentation was shock in 23 patients,
cardiopulmonary arrestin 3 patients, and syncope in 11 patients.
Underlying con-ditions included trauma in 3 patients, malignant
tumors in3 patients, cerebrovascular disorder in 3 patients, heart
diseasein 1 patient, central line placement in 2 patients, and
preg-nancy in 1 patient. Acute PTE developed after surgery in13
patients and during prolonged bed rest status in 8
patients.Seventeen patients were inpatients when PTE
developed.Before surgical pulmonary thrombectomy, thrombolytic
ther-apy was performed in 10 patients and catheter interventionsfor
pulmonary embolus in 4 patients. Ten patients underwentPCPS before
surgery. Six patients (18.8%) died in hospital,and 3 patients (30%)
under PCPS died. IVC filters were usedin 16 patients (50%).
[Levels of Recommendations]1. Surgical pulmonary thrombectomy
under cardiopulmo-
nary bypass in patients with acute massive PTE withcirculatory
collapse: Class I
2. Surgical pulmonary thrombectomy for the treatment ofacute
massive PTE in patients without shock: Class IIa
(6) Inferior Vena Cava FiltersAlthough the indications for and
efficacy of IVC filters haveyet to be fully determined and
demonstrated, IVC filters have
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
11/24
1268
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
been increasingly recognized as effective in preventing PTEand
its complications.104106
1) Indications of Permanent IVC Filters107,108
Class I: Among patients with VTE,Those who are contraindicated
for anticoagulation therapyThose who exhibit treatment-related
complications and
adverse drug reactions to anticoagulation therapyThose with
recurrent VTE during adequate anticoagulation
therapyThose who are unable to continue anticoagulation
therapy
Class IIa: Among patients with VTE,Those with venous thrombosis
in intrapelvic veins or
branches of the IVCThose with large free thrombi in proximal
veinsThose undergoing thrombolytic therapy or thrombectomy
for the treatment of PTEThose with VTE with poor cardiopulmonary
reserveThose with recurrent PTE following placement of filtersThose
with high risk of complications related to anti-
coagulants (such as ataxia and frequent falls)Those undergoing
PEA for the treatment of chronic PTE
Class IIb: Among patients without VTE,Those with trauma
associated with a high risk of VTEThose undergoing surgery with a
high risk of VTEThose with other conditions associated with a high
risk of
VTEClass III:
Patients with acute PTE with neither right heart failurenor DVT
who are undergoing anticoagulation therapy
Patients with peripheral type of DVT who are
undergoinganticoagulation therapy
Contraindications:Patients with no access to the vena
cavaPatients without space to place a filter
*Use of a non-permanent IVC filter may be considered forpatients
with conditions for which an IVC filter will nolonger be required
after several weeks.
2) Indications for Non-Permanent IVC109111
Class I: NoneClass IIa:
Patients indicated for the placement of a permanent IVCfilter
but who need the filter for only several weeks toprevent acute
PTE.
Class IIb:Long-term placement of removable filters
Class III:Patients with acute PTE with neither right heart
failure nor
DVT who are undergoing anticoagulation therapyPatients with
peripheral type of DVT who are receiving
anticoagulation therapy*Since permanent placement of IVC filters
increases therisk of venous thrombosis, removable IVC filters
should beremoved whenever possible.
[Levels of Recommendations]The indications for permanent and
non-permanent IVC filtersare listed as above.
2. Chronic Pulmonary Thromboembolism
1 DiagnosisDiagnosis of idiopathic chronic PTE with PH (CTEPH)
as
a condition requiring treatment should be made according tothe
criteria for diagnosis provided by the Specific DiseaseRespiratory
Failure Study Group of the MHLW (Table 7).CTEPH should be suspected
in patients with exertional dys-pnea. Patients in whom CTEPH is
suspected should be iden-tified based on the typical symptoms and
clinical findingslisted in Table 7. Arterial blood gas analysis
should be per-formed not only in patients with abnormal chest X-ray
find-ings but also in those without remarkable X-ray findings.
Patients with hypoxemia associated with hypocapnia shouldbe
assessed with ECG, echocardiography, and pulmonaryfunction tests to
exclude other cardiopulmonary diseases andto confirm the
presence/absence of findings of right heartoverload such as right
ventricular enlargement and right ven-tricular hypertrophy. In
making the diagnosis of CTEPH,physicians should confirm that (1)
pulmonary ventilation/per-fusion scintigraphy has revealed
maldistribution of pulmonaryblood flow without abnormal ventilation
distribution thathas persisted for 6 months; or the patient
exhibits at leastone of the five typical findings of pulmonary
artery angiog-raphy,112ie, (a) pouch defects (the presence of round
pouch-like shadows of thrombi that have been smoothed by bloodflow,
(b) webs and bands (band-like stenosis with pulmonaryrecanalization
associated with organization of thrombi, (c)intimal irregularities,
(d) abrupt narrowing, and (e) completeobstruction; and (2) right
heart catheterization reveals normalpulmonary artery wedge pressure
and a mean pulmonary arte-rial pressure of 25 mmHg. Cardiac
catheterization is usefulfor measurement of pulmonary vascular
resistance to deter-mine prognosis.
Although contrast CT (MSCT) has been reported to beuseful in the
diagnosis of CTEPH,113pulmonary angiographyis required to assess
the condition of subsegmental arteriesand to determine whether
surgery is indicated.114
2 TreatmentCTEPH is treated with medical and surgical therapy,
andthe results with current methods of PEA are excellent. Onlya few
reports have described catheter interventions for thetreatment of
CTEPH; use of them is not expected to becomecommon in the future,
if they are used at all.
(1) Medical TreatmentThe pathophysiology of CTEPH includes PH
due to occlu-sion of pulmonary arteries by organized thrombi,
intractableright heart failure, and hypoxemia. Accordingly,
surgicalremoval of organized thrombi (PEA) is the only radical
treat-ment for CTEPH. However, PEA is limited to the treatmentof
central type of CTEPH. Patients with peripheral type ofCTEPH, those
with relatively mild CTEPH who do not needsurgery, and those with
CTEPH with persistent PH followingsurgery are treated with medical
treatment.
In medical treatment, patients with CTEPH who are notindicated
for surgery receive anticoagulants for the treatmentof VTE, which
is considered the cause of CTEPH, oxygentherapy for hypoxemia,
pulmonary vasodilators for PH, andcardiotonics and diuretics for
right heart failure, whenevernecessary.
1) Anticoagulation TherapyThe prognosis of untreated CTEPH
depends on pulmonaryhemodynamics. It has been reported that even
patients withmild CTEPH may exhibit exacerbation of pulmonary
hemo-dynamics over time.19 Such exacerbation is believed to
becaused by recurrent acute PTE, and to involve mechanisms
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
12/24
1269
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
Table 7. Guidelines for the Diagnosis of Idiopathic Chronic
Pulmonary Thromboembolism With Pulmonary Hypertension
Chronic pulmonary thromboembolism with pulmonary hypertension is
defined as the presence of chronic obstruction of pulmonary
arteriesdue to organized thrombi and pulmonary hypertension causing
severe exertional dyspnea.
(1) Major symptoms and other clinical findings
1) Exertional dyspnea (Hugh-Jones Grade II or more severe) or
fatigability has been observed for >3 months.
2) Clinical symptoms typically associated with acute pulmonary
thromboembolism (abrupt onset of dyspnea, chest pain, syncope,
etc.)have occurred at least once.
3) Clinical symptoms (swelling in the lower limbs and pain)
suspected deep vein thrombosis in the lower limbs have
occurred.
4) Pulmonary bruit is auscultated over the lungs. 5) Chest
auscultation reveals abnormal sounds suggestive of pulmonary
hypertension (including at least one of the following four
find-
ings: (1) increase in the pulmonary component of the second
heart sound, (2) a fourth heart sound, (3) noise at the pulmonary
arterialorifice during the diastolic phase, and (4) noise at the
tricuspid orifice during the systolic phase
(2) Laboratory findings
1) Arterial blood gases
(a) Hypoxemia associated with hypocapnia (PaCO218 mm)
(b) Enlargement of cardiac shadow (CTR >50%)
(c) Local differences in pulmonary artery shadows (right vs.
left lung, upper vs. lower lung)
3) ECG
(a) Right axis deviation and pulmonary P wave
(b) R >5 mm at V1 or R/S >1, or S >7 mm at V5 or R/S 6
months evenafter thrombolytic or anticoagulation therapy. When
findings appear to have persisted, scintigraphy should be repeated
6 months laterto confirm the findings.
6) Pulmonary angiography
As changes due to chronic thrombi, at least one of five
findings, including (a) pouch defects, (b) webs and bands, (c)
intimal irregulari-ties, (d) abrupt narrowing, and (e) complete
obstruction, is observed.
7) Right heart catheterization
(a) Mean pulmonary arterial pressure during the chronic stable
phase is >25 mmHg. (b) Pulmonary arterial wedge pressure is
normal (
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
13/24
1270
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
of formation of thrombus in situ. Accordingly, life-long
anti-coagulation therapy with warfarin is required for patients
withCTEPH. Warfarin is often administered with a target INR of1.5
to 2.5, which is also recommended for patients with acutePTE.
2) Thrombolytic TherapyPatients with CTEPH may exhibit rapid
progression of dis-ease. When levels of coagulation/fibrinolytic
molecular
markers such as D-dimer are high during disease
progression,thrombolytic therapy may yield improvement.
Physiciansshould be aware of this possibility.
3) HypoxemiaAlthough there is no conclusive evidence for it,
oxygen ther-apy is expected to improve both the QOL and prognosis
ofpatients with CTEPH. In Japan, home oxygen therapy (HOT)for
patients with PH including CTEPH is covered by theNHI.
4) Treatment of Right Heart FailureThe presence of clinically
significant right heart failure is animportant determinant of the
prognosis in CTEPH. Patientswith right heart failure who exhibit
pleural effusion, hepa-tomegaly/abnormal hepatic function,
thrombocytopenia, legedema, or other typical signs/symptoms are
treated with con-ventional regimens for heart failure including bed
rest, restric-tion of water intake, diuretics, and oral
cardiotonics. Patientsin severe condition also require intravenous
administrationof catecholamines such as dopamine and dobutamine as
wellas milrinone.
5) VasodilatationAlthough use of classic vasodilators such as
calcium blockers,nitrates, and angiotensin converting enzyme (ACE)
inhibi-tors to treat CTEPH has been attempted, the efficacy of
thesedrugs in patients with CTEPH has not been
demonstrated.However, recent studies have evaluated the effects of
bera-prost35and epoprostenol,115 drugs indicated for
pulmonaryarterial hypertension, on CTEPH. Open-label studies
andplacebo-controlled studies of bosentan36,116and sildenafil37have
revealed that these drugs may significantly improvepulmonary
hemodynamics, six-minute walking distance, andbrain natriuretic
peptide (BNP) level, and so on. The efficacyof regimens combining
these drugs has also been reported.However, use of these drugs for
the treatment of CTEPH iscurrently not covered by NHI in Japan.
[Levels of Recommendations]1. Anticoagulation therapy: Class
IIa2. Oxygen therapy/HOT: Class IIb3. Vasodilatation for the
treatment of PH: Class IIb4. Cardiotonics and diuretics for right
heart failure: Class IIb
(2) Surgical Treatment
1) PEA by Lateral ThoracotomyPEA is almost fully established as
a method of treatment ofCTEPH. Lateral thoracotomy had been used
before PEA bymedian sternotomy with cardiopulmonary bypass and
deephypothermic intermittent circulatory arrest was establishedas
the standard technique. The indications for PEA by
lateralthoracotomy are similar to those for the method by
mediansternotomy, though this procedure is currently considered
foronly a limited number of patients.117123
a) SurgeryIncision along the fourth or fifth rib is made to
approach thepulmonary artery. Dissection is started from the
interlobarfissure to expose the segmental arteries. Taping is
performedto control back flow of blood from peripheral vessels.
Dissec-tion must be performed carefully so as not to injure the
pul-monary parenchyma. After administration of heparin, eitherthe
right or left main pulmonary artery is clamped
withoutcardiopulmonary bypass to monitor changes over time in
pul-
monary arterial pressure for about 5 minutes. After confirm-ing
that pulmonary arterial pressure does not exceed systemicblood
pressure, an incision is made into the affected lobeartery to
initiate thromboendarterectomy. The dissecting planeis determined
as in the median sternotomy technique. Thetarget organized thrombus
and the intima are held and pulledalong the direction to each
segmental artery without cuttingoff the thrombus and the intima.
Following removal of thethrombus and the intima, the peripheral
taping is removed toconfirm back flow of blood. The incision over
the lobe arteryis closed by suturing or using an autologous
pericardial patch.
b) Results of Surgery by Masuda et alSince 1986, Masuda et al
have performed PEA by lateral tho-racotomy in 16 patients. In all
patients, a right lateral tho-racotomy incision was used to access
the pulmonary arteries.No patients exhibited serious arrhythmia or
right heart failure.No patients required emergency cardiopulmonary
bypass forthe treatment of hypoxemia. Two patients underwent
throm-boendarterectomy by left lateral thoracotomy as a
second-stage procedure in a two-staged operation. Two
patients(12.5%) died of surgical complications, due to
postoperativepneumonia and postoperative pulmonary edema in one
caseeach. The patients who survived surgery exhibited prompt
im-provement in mean pulmonary arterial pressure, cardiac index,and
pulmonary vascular resistance, and gradual improve-ment in PaO2
over time, resulting in significant improvement6 months after
surgery. Three patients died 4,220, 1,891, and1,173 days after
surgery, due to sudden death in 2 patientsand heart failure in 1
patient. Relationships were suspectedto exist between these
late-phase deaths and CTEPH.
c) SummaryMedian sternotomy, which enables PEA in both right
andleft pulmonary arteries in one stage, is used as the
standardprocedure for treatment of CTEPH, and has yielded
favor-able results, particularly in patients with central type
ofCTEPH.16,124 The lateral thoracotomy technique should
beconsidered only for patients with predominantly unilateraldisease
with peripheral pulmonary lesions.
[Levels of Recommendations]1. PEA by lateral thoracotomy: Class
IIb
2) PEA With Deep Hypothermia
(a) Indications for SurgeryFindings of various examinations
including pulmonary angi-ography, MSCT, pulmonary perfusion
scintigraphy and rightheart catheterization are important in
determining treatmentstrategies for CTEPH. Daily et
al125,126reported that surgicaltreatment of CTEPH is indicated for
patients with a pul-monary vascular resistance of 300 dyneseccm5in
whompulmonary angiography reveals occlusive lesions of the
lobearteries, while Jamieson et al28,127described this technique
asindicated for patients with (1) a mean pulmonary arterial
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
14/24
1271
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
pressure of 30 mmHg and a pulmonary vascular resistanceof 300
dyneseccm5; (2) central edges of thrombi locatedin surgically
accessible areas; and (3) without serious compli-cations. Important
determinants of the use of surgery for thetreatment of CTEPH are
the configuration of occluded pul-monary arteries and clinical
manifestations (New York HeartAssociation [NYHA] Class III or
higher without shock).31,128,129In terms of configuration of
affected pulmonary arteries, sur-gery is indicated for patients
with central type of CTEPH
that affects central pulmonary arteries including the
mainpulmonary artery, interlobar arteries, and segmental
arteriesand causes mural thrombi and intimal hyperplasia,
whileeffective surgical treatment may not be possible in
patientswith peripheral type of CTEPH affecting peripheral
portionsof segmental arteries and subsegmental arteries.
Appropriateselection of patients is thus important.130
(b) Surgical TechniquesUnlike acute PTE, the thrombi in CTEPH
are pale white, andorganized thrombi are attached firmly to the
pulmonary arte-rial wall. During surgical treatment of CTEPH,
organizedthrombi must be removed together with the intima.129The
SanDiego group including Daily et al125and Jamieson et
al28de-veloped a technique termed PEA in both lungs, which
involvesa median sternotomy with cardiopulmonary bypass and
deephypothermic intermittent circulatory arrest. PEA is the
stan-dard surgical technique for the treatment of
CTEPH,124,130134since CTEPH usually develops in both lungs; the
right andleft lungs can be approached simultaneously; cardiac
lesionscomplicated by CTEPH can be treated; and the risk of
pul-monary bleeding due to thoracotomy is low.
a) Important Aspects of PEATechniques to remove thromboemboli
alone without remov-ing the intima are completely ineffective in
the treatment ofCTEPH. In removing the intima, it is important
first to deter-mine the dissecting plane appropriately. Optimally,
the dis-secting plane should be located between the internal
elasticmembrane and the media. Second, since organized thrombiare
hard and not fragile, the target thrombus and intima shouldbe
slowly peeled peripherally to the segmental arteries bypulling the
thrombus to remove the tree-like organized throm-bus with intima.
Third, it is important to ensure a blood-freesurgical field.
Jamieson strippers are useful for this purpose,and intermittent
circulatory arrest should be performed asappropriate. The duration
of circulatory arrest should be15 minutes each time. When venous
oxygen saturation isdecreased to 90%, reperfusion should be
performed for atleast 10 minutes before restart of circulatory
arrest. Majorchallenges of PEA include the treatment of peripheral
occlu-sive lesions for which surgical thromboendarterectomy can-not
be performed by median sternotomy and treatment ofpatients with
fragile mural thrombi for which traction duringdissection is
difficult to perform.
b) Procedures for PEAa. Presurgical preparation: In patients
with DVT and those
with a history of it, an IVC filter is placed before PEA.During
surgery, patients should be monitored for deep bodytemperature
(pharyngeal temperature), arterial pressure, andpulse oximetry.
Transesophageal echocardiography andSwan-Ganz catheter placement
are performed. Endotrachealtubes are placed in the right and left
bronchi to prepare forpulmonary bleeding, and ice bags to wrap the
head arealso prepared. Autologous blood recovery systems (Cell
Saver) are used during surgery.b. Following a median sternotomy,
cardiopulmonary bypass
is performed with venous drainage from the superior venacava
(directly) and the IVC (through the right atrium) andarterial
return to the ascending aorta. When ventricularfibrillation occurs
after the initiation of cooling, a left atrialvent is inserted from
the right upper pulmonary vein.
c. Under hypothermia, the superior vena cava is freed
com-pletely from the right atrium to the innominate vein. The
frontal surface of the right main pulmonary artery is ex-posed
to the right superior pulmonary vein, and the leftmain pulmonary
artery to the pericardial reflection.
d. PEA of the right pulmonary artery: A retractor is
placedbetween the superior vena cava and the ascending aorta,and a
vertical incision of the right pulmonary artery is madefrom level
of mobilized aorta, past right upper lobe branch,and into the right
lower lobe artery. On the posterior wall,a dissecting plane is
developed to start PEA. In patientswith thrombus in the main
pulmonary artery, the dissect-ing plane can be identified at the
site of incision. Underhypothermia to a deep body temperature of
18C and inter-mittent circulatory arrest, PEA is performed distally
toeach segmental artery using a Jamieson stripper. Follow-ing PEA,
the right pulmonary artery is closed by doublerunning suture with
monofilament material.
e. PEA of the left pulmonary artery: Using a heart net, theheart
is tugged to the lower right-hand side, and the leftpulmonary
artery is exposed from the pulmonary trunkto the pericardial
reflection. The dissecting plane is de-veloped, and PEA is
performed to each segmental arteryunder intermittent circulatory
arrest. Following PEA, theleft pulmonary arterial wall is sutured
and closed.
f. When an atrial septal defect is present, it is closed.
Whencoronary artery bypass grafting (CABG) or surgical treat-ment
of valvular disease is required, it is performed duringrewarming.
Since tricuspid valve regurgitation is improvedwhen pulmonary
arterial pressure is decreased, no surgicaltreatment for it is
required, in principle.135
g. Following rewarming, withdrawal from cardiopulmonarybypass is
attempted. The patient can be safely withdrawnfrom cardiopulmonary
bypass when mean pulmonary arte-rial pressure is 30 mmHg or less.
However, when pulmonaryarterial pressure is identical to systemic
blood pressure orwhen severe bleeding from the respiratory tract is
observed,PCPS is introduced before withdrawal from cardiopulmo-nary
bypass, and protamine is administered thereafter.
h. Cardiac tamponade due to pericardial effusion may occurduring
the several weeks after surgery. To prevent it, peri-cardial
fenestration is performed on the left side, and adrainage tube is
inserted into the left thoracic cavity.
c) Postoperative ManagementWhen a patient with PCPS has returned
to the intensive careunit (ICU), withdrawal from PCPS is attempted
over 2 to3 days. Pulmonary edema and endotracheal bleeding due
toreperfusion injury are important postoperative
complicationsrequiring careful attention.136 When prolonged
respiratoryfailure develops, the patient should be carefully
ventilatedusing positive end-expiratory pressure (PEEP) for a
sufficientlength of time. After the risk of respiratory tract
bleeding orbloody drainage is decreased, the patient should begin
hepa-rin therapy and then be switched to oral warfarin. When
PHpersists, long-term management of right heart failure
withvasodilators (eg, prostaglandin [PG] E1and PGI2) and
cate-cholamines is required.
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
15/24
1272
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
(c) Results of Surgical TreatmentThe operative mortality of
patients undergoing PEA with car-diopulmonary bypass and deep
hypothermic circulatory arrestfor the treatment of CTEPH were 11.7%
(12/103)125 and12.6% (16/127)126in the case series reported by
Daily et al,8.7% (13/150)28and 5.1% as reported by Jamieson et
al,12710.1% (7/69) by Tscholl et al,1376% (66/1,100)138and
4.7%(52/1,100)139 by Thistlethwaite et al, 5% by Bonderman
etal,1408.0% (7/88) by Ogino et al,32and 8.3% (7 out of 84
pa-tients undergoing elective PEA) by Ando et al.141The resultsof
PEA have recently improved.
Although the long-term results of medical treatment ofCTEPH are
not favorable, PEA is expected to improve car-diopulmonary
hemodynamics and to yield a favorable long-term prognosis.134 It
has been reported that the 6-year and5-year postoperative survival
rate were 75%,2986%,32respec-tively, and so on. In the patients
with persistent PH follow-ing surgery, long-term results are
poor.124,131
(d) SummaryCTEPH does not respond to medical treatment. PEA is
quiteeffective in the treatment of central type of CTEPH. PEA
withcardiopulmonary bypass and deep hypothermic circulatoryarrest,
which is performed increasingly often now, signifi-cantly improves
pulmonary hemodynamics and pulmonarygas exchange, and is associated
with favorable results. How-ever, patients with peripheral type of
CTEPH should be care-fully evaluated to determine whether this
surgery is indicatedfor them.
[Levels of Recommendations]1. PEA with cardiopulmonary bypass
and deep hypother-
mic circulatory arrest for the treatment of central type
ofCTEPH: Class I
2. PEA with cardiopulmonary bypass and deep
hypothermiccirculatory arrest for the treatment of peripheral type
ofCTEPH: Class IIa
3. Deep Vein Thrombosis
1 Diagnosis
(1) Basic ApproachDiagnosis and treatment of DVT should always
be per-formed considering the risk of PTE (Figures 1,2). Patientsin
the acute phase should be evaluated for the presence andlocation of
thrombosis, the characteristics of possible sourcesof emboli, and
the severity of venous insufficiency in select-ing appropriate
treatment strategies.38,54,142Figure 3shows analgorithm for
diagnosis of DVT during the acute phase.142,143DVT should be
suspected on the basis of the history and phys-ical examination
signs/symptoms, and the presence/absenceof known risk factors.
Patients suspected to have acute-phaseDVT44 should be evaluated
with appropriate imaging tech-niques that enable the presence of
DVT to be promptly deter-mined. Noninvasive venous ultrasonography
is the exami-nation of choice for evaluation of DVT in the
extremities.53,144Minimally invasive contrast CT or magnetic
resonance venog-raphy (MRV) should be performed to evaluate
patients sus-pected to have abdominal or chest DVT.145147 When
thepresence/absence of DVT cannot be not confirmed with theabove
techniques, invasive contrast venography should beperformed.148
Differential diagnosis may be performed byquantitative assay.
D-dimer can be used for patients in whomthe possibility of
acute-phase DVT is low.149,150Patients withabnormal D-dimer levels
should be evaluated with imagingtechniques to confirm the
diagnosis. Physicians should beaware that the presence of normal
D-dimer levels can excludeacute-phase DVT but cannot exclude
chronic-phase DVT.Appropriate imaging techniques should be used to
excludethrombosis. Prior to treatment, the causes of DVT should
beinvestigated.
(2) History and Present IllnessDuring the history and physical
examination, physiciansshould look not only for the symptoms of
acute-phase DVTbut also those of PTE and arterial
embolism.38,54,142 Acute-phase DVT should be suspected when
swelling, pain, or colorchange of the extremities is present.
Central type of DVTshould be suspected when unilateral swelling is
noted. Cen-tral type of DVT is suspected in patients with femoral
pain,while central or peripheral type of DVT is suspected in
pa-tients with lower leg pain. Central type of DVT is suspectedwhen
red purple skin is observed in the femoral region orlower leg.
Patients with peripheral type of DVT are oftenasymptomatic.
Physicians should suspect peripheral type of
Figure 3. Algorithm for diagnosis of deep vein thrombosis.CT,
computed tomography; MRV, magnetic resonance ve-nography.
Figure 4. Diagnosis of deep vein thrombosis in the lowerlimbs by
venous ultrasonography.
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
16/24
1273
Circulation Journal Vol.75, May 2011
JCS Guidelines for Pulmonary Thromboembolism and DVT
DVT when patients present with dyspnea and/or chest
pain.Patients should be evaluated for common known risk factorsof
DVT (Table 3).
(3) Medical ExaminationPatients should be inspected visually for
color change andswelling in the extremities, and the extremities
should bepalpated for pathological changes in the deep veins
andmuscles.38,54,142 Central type of DVT should be suspectedwhen
color change or swelling is present in the extremities.The presence
of palpable thrombotic veins in the groin isa direct finding of
central type of DVT in the lower limbs.Stiff muscles in the lower
legs are an indirect finding of cen-tral type of DVT, while tender
muscles in the lower legs area direct finding of central or
peripheral type of DVT. Centraltype of DVT should be strongly
suspected when patientsexhibit skin color change and swelling as
well as stiffnessand/or tenderness of the lower leg
muscles.38,142Severe cen-tral type of DVT should be strongly
suspected when dermalnecrosis of the lower legs as well as skin
color change andswelling of the legs are present. A lower leg
arterial Dopplertest should then be performed to evaluate blood
flow inthe leg arteries. Patients in whom acute DVT recurs
duringthe chronic phase of DVT exhibit findings of both chronicand
acute DVT.
(4) Laboratory Examinations
1) Quantitative ExaminationsQuantitative examinations are used
for differential diagnosisof DVT on the basis of blood chemistry
findings and bloodflow. D-dimer is the most important item in
screening forDVT. Blood flow is evaluated with ultrasonography,
whichcan determine vessel blood flow, and plethysmography, whichcan
determine blood flow in the lower limbs. Among ultra-sonographic
techniques for diagnosis of DVT, continuouswave Doppler is used to
check for arterial perfusion dis-order, while color Doppler and
pulsed Doppler are used tocheck for occlusion and resumption of
blood flow.38,142Airplethysmography is commonly used to evaluate
lower limbsvein function.
2) Imaging TechniquesImaging techniques such as
ultrasonography,151contrast CT,152MRV, and venography are used to
confirm the morphologi-cal diagnosis of DVT. During lower limb
venous ultrasonog-raphy (Figure 4), the following four steps of
investigationshould be performed: (1) determination of the
presence/ab-sence of thrombus in lower limb veins; (2) when
thrombus is
detected, evaluation of its characteristics to stage disease;(3)
when acute-phase DVT is present, determination of theextent of
thrombus to determine the type of DVT; and (4)examination of the
central edge of the thrombus to evaluate itas a potential source of
emboli. Staging should be performedbased on comprehensive
evaluation of noncompressing veins,brightness of thrombus, and
perfusion defects, among otherfindings142(Table 8). Although venous
ultrasonography is ahighly reliable technique for diagnosis of
acute-phase DVT,it is of limited use in the diagnosis of chronic
DVT. On con-trast CT, the diagnosis of DVT can be made based on
findingsof venous filling defects. MRV can also provide findings
ofthrombosis useful in the diagnosis of DVT, though its
reli-ability is less than that of contrast CT. Since
venographyprovides findings of venous filling defects and
delineates theborder of thrombus, it can be used to diagnose DVT
reliablyand exclude other possible diseases.153,154
3) Etiological EvaluationEtiological evaluation includes blood
tests to check for ten-dency of thrombosis such as the presence of
thrombophiliaand autoantibodies. Coagulation/fibrinolytic markers
are use-ful in the determination of treatment strategies and the
pre-vention of recurrent DVT. Patients should be examined
forcongenital conditions such as protein S deficiency, protein
Cdeficiency, and antithrombin deficiency as well as for
acquiredconditions such as decrease in levels of coagulation
inhibi-tors and increase in levels of tissue factors.
Antiphospholipidantibodies, which are autoantibodies known to be
associatedwith DVT, should also be tested.
[Levels of Recommendations]1. D-dimer: Class IIa2. Venous
ultrasonography: Class I3. MRV: Class IIa4. Contrast CT: Class I5.
Venography: Class I
2 Treatment
(1) Introduction (Current Concepts)Whether a thrombus developing
in a deep vein will grow ornot depends on external factors as well
as the balance be-tween the intrinsic and extrinsic coagulation
systems and thefibrinolytic system surrounding the thrombus. In
order toensure effective treatment of thrombosis, physicians
shouldunderstand the effects of mechanical compression of veinssuch
as that in pregnancy/delivery and surgical treatment,effects of
tissue factors such as cancer on the coagulation
Table 8. Diagnosis of Acute and Chronic Deep Vein Thrombosis by
Venous Ultrasonography
Criteria Acute phase Chronic phase
Vein Stenosis (compressibility)
Distention
Occlusion (noncompressing)
Distended
Stenosis (partial compression)
Contracted
Clots Floating
Regression
Consistency
Surface character
BrightnessHomogeneity
Free
None/moderate
Soft
Smooth
Low/middleHomogeneous
Fixed
Severe
Hard
Irregular
High/middleHeterogeneous
Blood flow Defect
Recanalization (in thrombus)
Collateral (in branch)
Total
Absent
Absent
Partial
Present
Present
-
8/10/2019 Guidelines for the Diagnosis, Treatment and Prevention
of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2
17/24
1274
Circulation Journal Vol.75, May 2011
JCS Joint Working Group
system, and abnormality or deficiency of regulatory proteinssuch
as proteins C and S and antithrombin (Class I). Theoptimal method
of treatment of DVT involves a combinationof techniques to prevent
the development of PTE, eliminate ordissolve venous thrombus
promptly, and prevent recurrenceof thrombosis, maintain the patency
of veins, and preservethe function of venous valves. Physicians
must consider theclinical severity and natural course of DVT in
selecting drugtreatment, catheter interventions, and/or surgical
thrombec-
tomy, among other techniques (Class IIa).
(2) Drug TreatmentHeparin and warfarin are the essential
components of anti-coagulation therapy for patients with DVT (Class
I).78,155,156Since the anticoagulative effect of unfractionated
heparin,which is used in Japan, varies between individuals, the
effectof heparin should be monitored with APTT and blood hepa-rin
concentration. The target APTT in Europe and the UnitedStates is
1.5 to 2.5 times the control APTT.75,157159This levelappears
appropriate in Japanese patients, as well (Class I).Following
initial intravenous administration of 5,000 unitsof heparin, 10,000
to 15,000 units of heparin should be con-tinuously infused over 24
hours. The dose should be adjustedaccording to APTT values. When
bleeding complicationsoccur, heparin treatment should be suspended
or permanentlydiscontinued. Type II heparin-induced
thrombocytopenia(HIT) is a serious treatment-related complication
associatedwith arterial thrombosis and DVT caused by immune
reac-tions. When it is suspected, heparin therapy must be
discon-tinued immediately (Class I). Low molecular weight
heparin,which is commonly used in Europe and the United States,
isnot indicated for the treatment of DVT in Japan. However,
theindications for low molecular weight heparin have expanded,and
the prevention of VTE in patients undergoing total hipreplacement,
total knee replacement, surgery for hip fracture,or abdominal
surgery has recently been added to them.
When warfarin is administered to patients with throm-bosis,
heparin and warfarin should be combined for 5 daysbefore starting
warfarin monotherapy. The dose of warfarinshould be adjusted to
achieve a PT-INR of 1.5 to 2.5 (target2.0) (Class IIb). The risk of
bleeding complications increasesin patients with a PT-INR of 4.
Patients with de novo DVTwith no known risk factors should receive
warfarin for 3 to6 months (Class IIa), while patients with
recurrent DVT orlong-term risk factors such as cancer, antithrombin
deficien-cy, or antiphospholipid antibody syndrome should
receivewarfarin as long as the relevant risks continue (Class
IIa).Systemic thrombolytic therapy decreases the incidences ofDVT
and the sequelae of thrombosis (Class IIa).160163Uro-kinase (UK)
should be infused intravenously at a dose of60,000 to 240,000
units/day on Day 1 and at tapered dosesfrom Days 2 to 7 (Class
IIa).
[Levels of Recommendations]1. Combined use of of heparin and
warfarin in the treatment
of acute DVT: Class I2. Heparin control with a target APTT of
1.5 to 2.5 times
the control in the treatment of acute DVT: Class I3. Warfarin
control with a target PT-INR of 2.0 (1.5 to 2.5)
times the control in the treatment of acute DVT: Class IIb4.
Systemic thrombolytic therapy in the treatment of acute
DVT: Class IIa
(3) Physical Therapy (Exercise and Compression)During the acute
phase of DVT, physicians should carefully
consider clinical severity and the natural course of DVT
inselecting appropriate treatment such as drug treatment, cathe-ter
interventions, and/or surgical thrombectomy, among othertechniques.
Patients should following surgical thrombectomystart