Embed Size (px)
Citation preview
GUIDELINES FOR DIABETIC RETINOPATHY
EXECUTIVE SUMMARY Diabetic retinopathy remains the major sight threatening eye disease in the working age population in the developed world and is increasing as a cause of blindness in other parts of the world. Recent information from major population studies (DCCT, UKPDS) regarding the importance of optimal management of diabetes, and its associated conditions, on the development of complications, is beginning to change the epidemiology of visual handicap. However, this is offset by the increase in the prevalence of diabetes overall. Current therapies for diabetic retinopathy are effective particularly for proliferative disease. These guidelines represent a consensus document outlining the epidemiology, clinical features and recommendations for population screening, detection, diagnosis and management of various forms of diabetic retinopathy. Some special problems are discussed as well as aspects of counselling for patients at different stages of the disease. The Guidelines are advisory and are not intended as a set of rigid rules, since individual patients will require tailored treatment for their particular condition. However, it is hoped that if used appropriately, they will lead to a uniformly high standard of management of patients with diabetic retinopathy.
2
PREFACE
Diabetic retinopathy is a potentially blinding disease affecting many individuals in the working age group. The aim of the guidelines is to provide advice on best management of different aspects of diabetic eye disease, based on evidence taken form the literature and published trials of therapies plus consensus opinion of an expert panel convened by the Royal College of Ophthalmologists which was representative of a range of groups with an interest in this condition. In addition opinion was taken from the consultant body of practicing ophthalmologists within the UK, registered with the College of Ophthalmologists.
EVIDENCE is graded on three levels:
Level 1 evidence was based on results of randomised controlled trials (RCTS)
power calculations or other recognised means were used to determine statistical validity of the conclusion.
Level 2 evidence was based on results of case studies, case series or other non-randomise prospective or retrospective analysis of patient data.
Level 3 evidence was based on expert opinion, consensus opinion or current recognised standard of care” criteria where no formal case series analysis was available.
RECOMMENDATIONS for practice are based on treatment protocols and
measures which were recognised to improve patient care and/or quality of life based on Level A strength of evidence was universally agreed Level B where the probability of benefit to the patient outweighed the risks Level C where it was recognised that there was difference of opinion as to
the likely benefit to the patient and decision to treat would be based after discussion with the patient
3
CONTENTS
SECTION 1. TERMINOLOGY AND DISEASE DEFINITION
1.1 Definition of Diabetic Retinopathy 1.2 Classification of Diabetic Retinopathy 1.3 Definitions of the Complications of Diabetic Retinopathy
SECTION 2. THE EPIDEMIOLOGY OF DIABETIC EYE DISEASE
2.1 Introduction 2.2 Prevalence of eye disease in people with diabetes 2.3 Incidence of Eye Disease in People with Diabetes
SECTION 3. RISK FACTORS AND THEIR MANAGEMENT, INCLUDING
COUNSELLING FOR DIABETIC RETINOPATHY 3.1 Introduction 3.2 Duration of Diabetes 3.3 HbA1c and glycaemic control 3.4 Hypertension 3.5.Age 3.6 Pregnancy 3.7 Renal Disease 3.8.Hyperlipidaemia 3.9. Smoking 3.10. ACE Inhibition 3.11. Aspirin and thrombolytic therapy 3.12. Antioxidants. 3.13. Alcohol 3.14. Counselling for Diabetic Retinopathy
SECTION 4. CLINICAL FEATURES OF DIABETIC RETINOPATHY 4.1 Non-proliferative (background/pre-proliferative) retinopathy 4.2 Proliferative diabetic retinopathy 4.3 Maculopathy SECTION 5. SCREENING FOR DIABETIC RETINOPATHY 5.1 Introduction 5.2 Development of screening for diabetic retinopathy 5.3 Evidence for the effectiveness of screening 5.4 Organisation of screening services
5.5 Screening methodology 5.6 Grading and referral 5.7 Population to be screened 5.8 Frequency of screening 5.9 Quality standards 5.10 Role of ophthalmologist
SECTION 6. LASERS and LENSES
4
6.1 Method of laser application 6.2 Lasers 6.3 Side effects of lasers SECTION 7. MANAGEMENT OF DIABETIC MACULOPATHY
7.1 Introduction 7.2 Definition
7.3 Recommendations for treatment 7.4 Treatment protocols for diabetic maculopathy
SECTION 8. MANAGEMENT OF NVE 8.1 Introduction
8.2 Definition 8.3 Evidence for current standard of treatment 8.4 Recommendations for treatment 8.5 Treatment protocols 8.6 New vessels on the iris (Rubeosis iridis)
SECTION 9. MANAGEMENT OF NVD 9.1 Introduction
9.2 Definition 9.3 Evidence for current standard of treatment
9.4 Recommendations for treatment 9.5 Treatment protocols
SECTION 10. VITRECTOMY IN DIABETIC EYE DISEASE
10.1 Indications 10.2 Vitreous / subhyaloid haemorrhage 10.3 Haemolytic ghost-cell glaucoma 10.4 Retinal detachment 10.5 Severe widespread fibrovascular proliferation 10.6 Iris / angle neovascularisation with vitreous opacity
10.7 Anterior hyaloidal fibrovascular proliferation / retrolental fibrovascular proliferation
10.8 Vitrectomy for diabetic macular disease SECTION 11. CATARACT 11.1 Introduction
11.2. Aims of surgery for Cataract 11.3 Cataract Surgery in patients with diabetes
11.4, Cataract surgery and vitrectomy in patients with diabetes 11.5. Cataract surgery, new vessels, rubeosis and risk of worsening
retinopathy 11.6. Visual outcomes of cataract surgery
11.7 Cataract surgery and progression of diabetic retinopathy APPENDIX
5
SECTION 1. TERMINOLOGY AND DISEASE DEFINITION
1.1 DEFINITION OF DIABETIC RETINOPATHY
Diabetic retinopathy is a chronic progressive sight-threatening disease of the retinal microvasculature associated with the prolonged hyperglycaemia and other conditions linked to diabetes mellitus such as hypertension. 1.2 CLASSIFICATION OF DIABETIC RETINOPATHY Diabetic retinopathy is a potentially blinding disease in which the threat to sight comes through two main routes: growth of new vessels leading to intraocular haemorrhage and possible retinal detachment with profound global sight loss, and localised damage to the macula / fovea of the eye with loss of central visual acuity. Classification and severity grading of diabetic retinopathy have historically been based on ophthalmoscopically visible signs of increasing severity, ranked into a stepwise scale from no retinopathy through various stages of non-proliferative or preproliferative disease to advanced proliferative disease. However, this may not accurately reflect functionally severe disease since maculopathy with severe visual loss may occur in the presence of moderate ophthalmoscopic signs. Two different approaches to classification have emerged: (a) those designed to cover the full range of retinopathy and aimed at the ophthalmologist that are based on the original Airlie House / EDTRS classification and (b) those which are proposed for use in population screening. 1.2.1 Full disease classifications
These have developed from the original Airlie House classification developed for the Early Treatment Diabetic Retinopathy Study (ETDRS)(1) aimed at grading retinopathy in the context of overall severity of ophthalmoscopic signs. Modified and simplified versions have been developed and used for research programmes and in clinical practice. A simplified version was developed for the first version of these guidelines in 1997 (2). A reduced version of the ETDRS classification aimed at countries without systematic screening programmes has recently been endorsed by the American Academy of Ophthalmology Guidelines Committee(3) and used in clinical trials (eg ETDRS, see later). The latter classification was developed in recognition of the need for a clinical grading system that would reflect the vision threatening risk of diabetic retinopathy. This describes three stages of low risk non-proliferative retinopathy, a fourth stage of severe non-proliferative retinopathy and a fifth grade of proliferative retinopathy. In addition macular oedema is determined as absent or present and further sub-classified on the basis of involvement of the centre of the macula.
1.2.2 Population screening classifications
The National Screening Committee(NSC) (4)has adopted a classification for use in England and Wales aimed at detection of that level of retinopathy
6
sufficiently severe to merit referral of the patient for expert ophthalmological opinion and possible treatment. A Scottish Diabetic Retinopathy Grading Scheme has also recently been introduced(5). The NSC classification adopts a simplified approach to grading retinopathy based on features which a non-ophthalmologist / accredited photographic grader might be faced with in a population of diabetic patients. This classification identifies four types of presentation of fundus disease, namely retinopathy (R), maculopathy (M), photocoagulation (P) and unclassifiable (U) (see Appendix).
1.2.3 Differences between classification systems
There is considerable overlap between the various classifications. They all recognise the two basic mechanisms leading to loss of vision: retinopathy (risk of new vessels) and maculopathy (risk of damage to the central fovea).
The differences between classifications relate mainly to levels of retinopathy and also to terminology used. Below are described the similarities and differences in both classifications, with the aim of permitting ready cross-reference. Where alternative terminology is in common use this is shown in parentheses. 1.2.3.1 Retinopathy Diabetic retinopathy is classified according to the presence or absence of abnormal new vessels as: • non-proliferative (background/preproliferative) retinopathy • proliferative retinopathy Each has a different prognosis for vision. 1.2.3.2 Non-proliferative diabetic retinopathy (NPDR) (background/pre-proliferative) In the international (AAO) classification, NPDR is graded as: • mild • moderate • severe In the NSC-UK classification, NPDR is graded as: • background (Level R1) • pre-proliferative (Level R2) In the Scottish Diabetic Retinopathy Grading Scheme, NPDR is graded as: • mild background (Level R1) • moderate background (Level R2) • severe background (Level R3) 1.2.3.3 Proliferative diabetic retinopathy (PDR)
7
PDR (Level R3 in the NSC-UK grading and R4 in Scotland) is described according to (a) location • new vessels on the disc (NVD) or within 1 disc diameter (DD)of the margin of
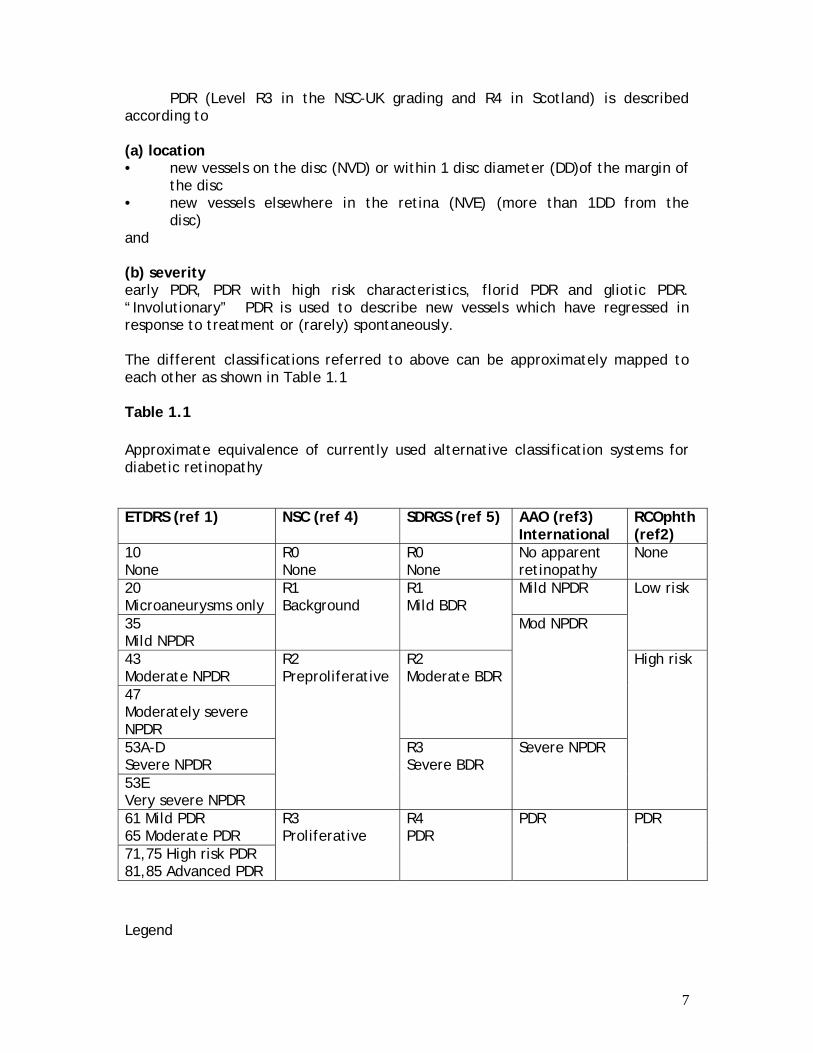
the disc • new vessels elsewhere in the retina (NVE) (more than 1DD from the disc) and (b) severity early PDR, PDR with high risk characteristics, florid PDR and gliotic PDR. “Involutionary” PDR is used to describe new vessels which have regressed in response to treatment or (rarely) spontaneously. The different classifications referred to above can be approximately mapped to each other as shown in Table 1.1 Table 1.1 Approximate equivalence of currently used alternative classification systems for diabetic retinopathy
Legend
ETDRS (ref 1) NSC (ref 4) SDRGS (ref 5) AAO (ref3) International
RCOphth (ref2)
10 None
R0 None
R0 None
No apparent retinopathy
None
20 Microaneurysms only
Mild NPDR
35 Mild NPDR
R1 Background
R1 Mild BDR
Low risk
43 Moderate NPDR 47 Moderately severe NPDR
R2 Moderate BDR
Mod NPDR
53A-D Severe NPDR 53E Very severe NPDR
R2 Preproliferative
R3 Severe BDR
Severe NPDR
High risk
61 Mild PDR 65 Moderate PDR 71,75 High risk PDR 81,85 Advanced PDR
R3 Proliferative
R4 PDR
PDR
PDR
8
ETDRS = Early Treatment Diabetic Retinopathy Study; AAO = American Academy of Ophthalmologists; NSC = National Screening Committee; SDRGS = Scottish Diabetic Retinopathy Grading Scheme; NPDR = Non-proliferative diabetic retinopathy; BDR = Background diabetic retinopathy; PDR = Proliferative diabetic retinopathy; HRC = high risk characteristics 1.2.4. Diabetic maculopathy (DM) Retinopathy which affects the macula is separately described as diabetic maculopathy. DM is further classified as: • focal oedema • diffuse oedema • ischaemic or • mixed DM may be tractional due to vitreoretinal pathology or non-tractional (intraretinal). In the classification systems described above various definitions of maculopathy have been given. EVIDENCE LEVEL 1 1.3 DEFINITIONS OF THE OCULAR COMPLICATIONS ASSOCIATED WITH DIABETIC RETINOPATHY The ocular complication of diabetes may be specific to progression of the ocular disease or, more commonly, may be non-specific recognised associations of diabetes in the eye. ------------------------------------------------------------------- Table 1.2 Complications linked to Diabetic Retinopathy Specific Non-Specific Retinal Detachment Cataract Rubeosis Iridis Glaucoma Cataract Retinal Vein Occlusion/ Optic Disc Swelling Optic Neuropathy --------------------------------------------------------------------- 1.3.1 Non-specific ocular disease associations 1.3.1.1 Cataract
9
Cataract is defined as opacification of the lens and is common in older age populations. Age-related cataract occurs earlier in patients with diabetes. 1.3.1.2 Glaucoma
Glaucoma is defined as loss of vision due to raised intraocular pressure and occurs in two forms: primary or secondary. Primary glaucoma may present as acute glaucoma or chronic glaucoma. Patients with diabetes may have a greater risk of developing primary chronic glaucoma with loss of visual field (side vision). Patients with PDR are at risk of developing secondary glaucoma, particularly rubeotic glaucoma (see below). 1.3.1.3 Retinal Vein Occlusion / Optic disc swelling
Patients with diabetes are at higher risk of developing optic nerve disease due to vascular occlusion, which is distinct from diabetes-specific optic neuropathy (see below) and usually occurs in older patients with Type 2 diabetes and hypertension. This may be a form of ischaemic optic neuropathy. 1.3.2 Specific complications 1.3.2.1 Retinal Detachment
Retinal detachment is caused by the accumulation of fluid between the neural retina and the retinal pigment epithelium and in non-diabetic patients most commonly results from a tear in the retina (rhegmatogenous retinal detachment). In patients with PDR, tractional retinal detachment may occur due to condensation and contraction of the vitreous gel in association with haemorrhage and fibrosis (plus gliosis). Tractional retinal detachment may progress to combined tractional and rhegmatogenous retinal detachment. Central vision is lost when the macula is involved. 1.3.2.2 Rubeosis iridis and rubeotic glaucoma Rubeosis iridis is the growth of new vessels on the iris in eyes with advanced retinal ischaemia. Rubeosis may induce a severe form of intractable glaucoma (see below) due to closure by fibrovascular tissue of the aqueous fluid drainage route in the anterior chamber angle of the eye. 1.3.2.3 Cataract A specific form of “snow-flake” cataract is recognised in younger diabetics. In addition, a rare form of “osmotic” reversible cataract occurs in young diabetic patients, including infants, due to rapid changes in fluid electrolyte balance in severe uncontrolled diabetes. 1.3.2.4 Optic neuropathy
10
Patients with diabetes may rarely experience optic neuropathy, which presents as swelling of the optic discs associated with gradual reduction in visual acuity. 1.3.2.5 Other ocular pathology in diabetes Ocular muscle palsies are not uncommon in association particularly with Type 2 diabetes. In addition, corneal epitheliopathy is common and a cause of poor epithelial wound healing especially after ocular surgery.
11
SECTION 2 THE EPIDEMIOLOGY OF DIABETIC EYE DISEASE 2.1 INTRODUCTION
Diabetes mellitus results in considerable morbidity and mortality, affecting about 180 million people worldwide(6). The disease is classified according to two distinct groups of patients: type 1 diabetes (previously known as ‘insulin dependent’ or ‘juvenile onset’) and type 2 diabetes (non-insulin dependent, adult-onset) which is characterized by insulin resistance in peripheral tissues and an insulin secretory defect of the beta-cell(7). Type 2 diabetes is classified also by clinical stage, to those controlled by healthy living, those who need oral medication, and those who need insulin. The new WHO classification also recognises other types of secondary diabetes eg after pancreatic disease and a fourth category of gestational diabetes but these conditions are not considered in this document.
Between 70 to 90% of known diabetic patients have type 2 diabetes(8). An
estimated 50% more remain undiagnosed(9, 10). In the UK white population, rates of known diabetes range from 2 - 4%. Type 2 diabetes is commoner in ethnic minority peoples and those who are socio-economically deprived.
Diabetes increases risk for developing many irreversible complications(11).
These can be largely divided into macrovascular and microvascular complications. The macrovascular complications include cerebro-vascular disease, coronary heart disease and peripheral vascular disease. The microvascular complications include eye disease (diabetic retinopathy), nerve disease (diabetic neuropathy) and kidney disease (diabetic nephropathy). The other main eye complication, cataract, is usually not specific to diabetes, but the risk of developing cataract is greater in people with diabetes.
The prevalence of these complications in a general population relates to the
prevalence, type and duration of diabetes. Therefore, the predicted rise in numbers of adults with diabetes will be accompanied by an increase in the number of diabetic complications.
In people with diabetes, cataracts and retinopathy are the most significant cause of visual impairment and blindness, and people with diabetes are 25 times more likely than the general population to become blind(12). In developed countries, diabetic eye disease represents the leading cause of blindness in adults under 65 years(13). 2.2. PREVALENCE OF EYE DISEASE IN PEOPLE WITH DIABETES 2.2.1 Definitions
Point prevalence: the proportion of cases of a disorder or disease in a particular population at a particular point in time.
12
Lifetime prevalence: the proportion of the population who have a history of a given condition at a particular point in time. 2.2.2 Prevalence of diabetic retinopathy
There is a wide range of prevalence estimates. Those studies that specifically report the prevalence of retinopathy at diagnosis (rather than pooled prevalence data from patients who may have had varied exposure to the disease), suggest that the prevalence of retinopathy of any severity in people with newly diagnosed diabetes is dependent upon the type of diabetes (type 1 or type 2). Generally, the prevalence of retinopathy at diagnosis of type 1 diabetes is reportedly low, between 0% and 3% (14-17), while a higher proportion of those with newly diagnosed type 2 diabetes have evidence of DR (6.7–30.2%)(14, 18-25).
Studies not confined to newly diagnosed diabetes show the prevalence of DR
in type 1 and type 2 diabetes strongly correlates with duration of disease, and in type 2 diabetes with the clinical stage as shown by the need for insulin.
Sub-clinical diabetic retinopathy, shown by retinopathic changes on fluorescein angiography in people with no photographic abnormalities are common, and of patients so defined in the Diabetes Control and Complications Trial (DCCT, see below), 67% had retinopathy within 5 years of diabetes onset.
The United Kingdom Prospective Diabetes Study (UKPDS, see below) found a higher prevalence of retinopathy (39% in men and 35% in women) in newly diagnosed type 2 diabetes than have other studies.
Population based studies from the UK generally show lower rates of
retinopathy: of 10,709 diabetes patients identified through health district audit and data linkage, 16.5% had retinopathy(26). In addition, more recent UK prevalence studies suggest that improvements in treatment of diabetes have led to lower rates of retinopathy, particularly of the sight threatening type(27-31).
2.2.3. Prevalence of diabetic macular oedema
The prevalence of macular oedema has also been found to be related to the duration of the disease and in type 2 diabetes the clinical stage as shown by the need for insulin treatment(32).
The prevalence of clinically significant MO (i.e. MO which threatens central
visual function; CSMO) is reportedly low in patients with type 1 diabetes (5%)(33, 34) and type 2 diabetes (2%)(35) in the first years following diagnosis. However, this increases to more than 20% in people who have had type 1 diabetes for 25 years(33). 2.2.4. Effect of gender on prevalence of diabetic retinopathy
There is little evidence of a difference in prevalence of retinopathy between genders. One UK report has suggested a higher prevalence of visual impairment in females based on data of blind or partially sighted registrations(36).
13
2.2.5. Effect of ethnicity on prevalence of diabetic retinopathy
This has been studied in the US where in the third National Health and Nutrition Examination Survey in the USA, the prevalence of retinopathy was 46% higher in blacks and 84% higher in Mexican-Americans than whites with diabetes(37).
The studies in the UK report either a similar prevalence of retinopathy
between people of African, Black West Indians, Jamaicans, European and Indian origin with type 2 diabetes(38), or in one report less in Indian Asians compared with White Europeans(39).
Rates of blindness or visual loss are also variously reported: one report has
suggested an ethnic and gender difference in the likelihood of being registered blind or partially sighted, with an interaction between gender and ethnicity: there was a higher proportion of visually impaired females than males (P < 0.05), but rates were lower than expected in female Indo-Asians. 2.2.6 Prevalence of cataract in people with diabetes The point prevalence of cataract increases with age, and is higher in ethnic minority groups such as the Indo Asian person, compared to the prevalence in the general population. One report indicated a prevalence of 30% compared to 3% in people aged under 60 years and 78% compared to 54% in those aged 60 years and over(36). The age of onset of cataract seems to be earlier in Asians. 2.3. INCIDENCE OF EYE DISEASE IN PEOPLE WITH DIABETES 2.3.1 Definition
Disease incidence is the number of new cases of a particular disease occurring over a defined time period. It may also be expressed as the percentage of cases progressing to the next stage of a disease over a defined time period. It may also be expressed as the number of patients per 100 or per 1000 patient years (see below). 2.3.2 Incidences of diabetic retinopathy in people with diabetes
The 4-year incidence of any retinopathy with type 1 diabetes enrolled in the WESDR was 59%(40). The 4-year incidence of any retinopathy in type 2 patients was 34%, and if on insulin, 47.4%. Progression of retinopathy is more frequent in type 1 diabetes (41% over 4 years) and insulin needing type 2 diabetes (34%) than non –insulin treated (25%).
Progression to proliferative retinopathy (PDR) was 10% over 4 years in type
1,and 7% and 2% in type 2 treated with or without insulin respectively. In type 1, insulin-treated type 2 and non-insulin-treated type 2, the 4-year incidence of
14
CSMO was 4%, 5% and 1%, and the incidence of legal blindness was found to be 1.5%, 3% and 2.5%, respectively(40).
The 10-year incidence of any retinopathy, macular oedema or visual loss in
the WESDR was 90%, 20% and 9% in type 1 diabetes, 79%, 25% and 33% in insulin-treated type 2 diabetes and 67%, 14% and 21% in non-insulin-treated type 2 diabetes, respectively(41). In subjects who have since been followed-up for 14 years(34), regression occurred in 17% of patients.
In the UKPDS, 22% of those with no sign of DR at baseline developed DR at 6
years, and in 29% of patients with baseline DR, DR progressed 2 or more steps on the ETDRS scale after 6 years’ disease duration(42). The risk of photocoagulation increased in relation to baseline DR severity.
Recent studies have suggested that the data from these early studies does
not reflect current incidences which are lower in frequency, mostly related to improvements in management of diabetes rather than of the retinal complications(29, 32, 43). In addition, there are a number of more recent incidence studies relevant to the population of diabetic patients in the UK(43, 44). 2.3.3. Incidence of cataract in people with diabetes
The incidence of cataract was 29 (17-46) 1000-person-years-1 in one study(45), another of hospital diabetic clinic attenders showed the incidence of cataract was 10.4 (95% confidence interval, 9.0, 11.9) per 1000 person-years, higher in females(46).
The incidence of cataract in Type 1, non-insulin-treated and insulin-treated
Type 2 was 7, 12 and 18 per 1000 person-years, respectively(47, 48) but this was confounded by age. Age poor metabolic control and any retinopathy were significant independent predictors of cataract. Duration of diabetes was a significant independent predictor of cataract for type 1 patients.
15
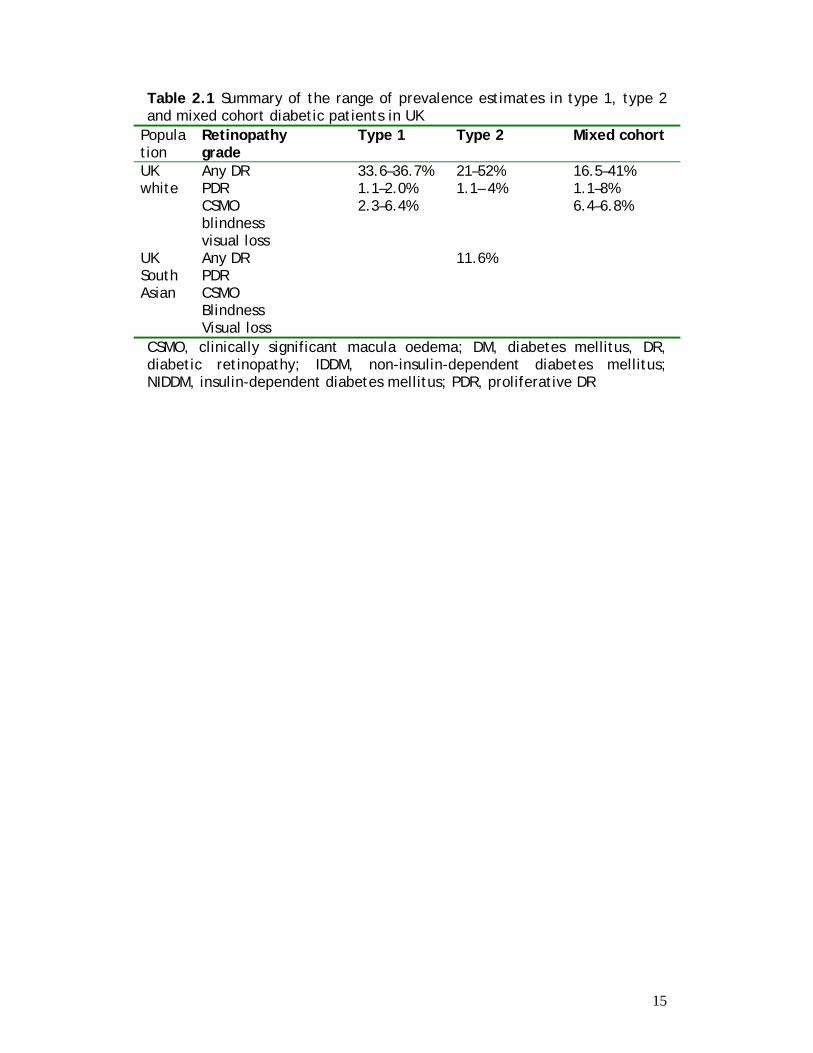
Table 2.1 Summary of the range of prevalence estimates in type 1, type 2 and mixed cohort diabetic patients in UK
Population
Retinopathy grade
Type 1
Type 2
Mixed cohort
UK white
Any DR PDR CSMO blindness visual loss
33.6–36.7% 1.1–2.0% 2.3–6.4%
21–52% 1.1– 4%
16.5–41% 1.1–8% 6.4–6.8%
UK South Asian
Any DR PDR CSMO Blindness Visual loss
11.6%
CSMO, clinically significant macula oedema; DM, diabetes mellitus, DR, diabetic retinopathy; IDDM, non-insulin-dependent diabetes mellitus; NIDDM, insulin-dependent diabetes mellitus; PDR, proliferative DR
16
SECTION 3 RISK FACTORS AND THEIR MANAGEMENT
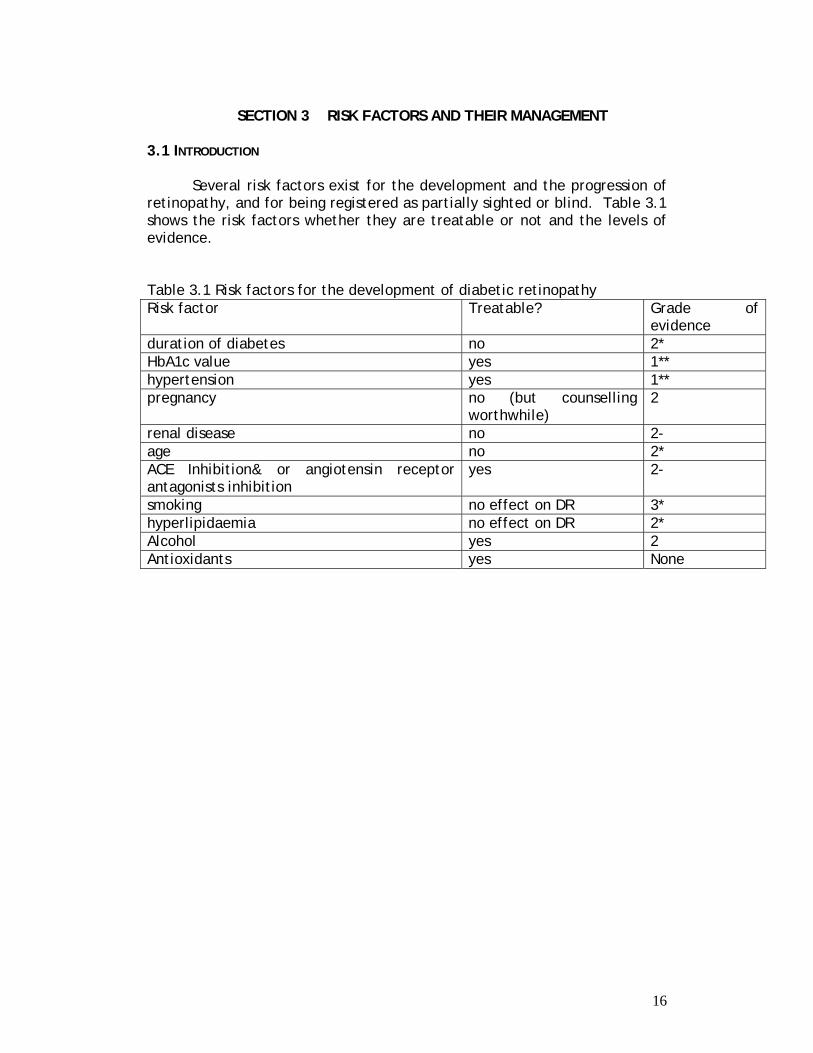
3.1 INTRODUCTION
Several risk factors exist for the development and the progression of retinopathy, and for being registered as partially sighted or blind. Table 3.1 shows the risk factors whether they are treatable or not and the levels of evidence. Table 3.1 Risk factors for the development of diabetic retinopathy Risk factor Treatable? Grade of
evidence duration of diabetes no 2* HbA1c value yes 1** hypertension yes 1** pregnancy no (but counselling
worthwhile) 2
renal disease no 2- age no 2* ACE Inhibition& or angiotensin receptor antagonists inhibition
yes 2-
smoking no effect on DR 3* hyperlipidaemia no effect on DR 2* Alcohol yes 2 Antioxidants yes None
17
3.2 DURATION OF DIABETES 3.2.1 Introduction
The onset of diabetes can be exactly timed in childhood (type 1 diabetes). However, there is evidence of delay from onset of diabetes to diagnosis in adult onset type 1, and considerable delay of about 8 years in type 2(49). 3.2.2 Definition
Duration of diabetes is defined for clinical purposes as the time from Diagnosis of Diabetes. However, it is recognised that sub-clinical diabetes may be present for a considerable time prior to diagnosis. 3.2.3 Relationship between duration of diabetes and retinopathy. There is a clear relationship between the duration of diabetes and the development of retinopathy, in both types 1 and 2 diabetes. In type 1 this is has been demonstrated in both the US Diabetes Control and Complications Trial (DCCT) results (see later) and in a UK study (29, 50). The relationship is not so clear in type 2 diabetes but has been shown to be important in the United Kingdom Prospective Diabetes Study (UKPDS) modelling of risk factors, particularly since with continuing duration there is continuing exposure to high HbA1c values(42). The duration of diabetes is also an important risk factor for progression of retinopathy to sight-threatening eye disease in both types 1 and 2 diabetes(43). EVIDENCE LEVEL 1 3.3. HBA1C AND GLYCAEMIC CONTROL 3.3.1. Introduction
In most studies glycosylated haemoglobin HbA1c (DCCT aligned) is used to estimate glycaemic control. 3.3.2. Relationship between HbA1c of diabetes and retinopathy.
In both types 1 and 2 diabetes, observational studies and randomised controlled trials (RCT) demonstrate that for both type 1 and type 2 diabetes improved glycaemic control (as measured by HbA1c) reduces the development of retinopathy and reduces the chance of progression of existent retinopathy. The benefits of treatment are directly shown in both the DCCT (Fig.1) and UKPDS studies which are randomized controlled studies of sufficient size to be robust for both type 1 and type 2 diabetes(51, 52). The UKPDS glycaemic study was an incidence study which examined intensive monotherapy for safety profiles as well as differences in glycaemic
18
control. An earlier study(53) treated people with type 2 diabetes who had failed on oral therapy and in whom insulin treatment was added to control their glycaemia; the insulin therapy was either conventional or intensive.
The DCCT observational study(54) showed that the higher the initial
HbA1c, and the shorter the duration of diabetes at entry, the greater was the benefit of intensive therapy and improved glycaemic control. The mean HbA1c during the trial was the dominant predictor of retinopathy, a 10% lower HbA1c (e.g. 7.2% versus 8%) was associated with a 44% lower risk. This risk gradient applied over all the HbA1c values seen with no threshold value for rapid deterioration. The change in risk is compounded by the duration of exposure – total glycaemic exposure being most important.
In both DCCT and UKPDS studies, those treated intensively initially
had a worsening in the chance of developing and progression of retinopathy, followed some three years later by a significant and increasingly significant improvement in the chance of developing new or progression of existent retinopathy.
In the DCCT study(51), 1441 patients were followed for a mean of 6.5
years. Intensive control achieved a mean HbA1c of 7.3%, with conventional control a mean of 9.1%. This intensive control resulted in risk reduction of 76% (95% confidence intervals 62 – 85%) or and 54% (39 – 66%) in worsening of retinopathy by 54% (39 to 66%); the development of new vessels was retarded by 47% (14 to 67%)(51, 54). On completion of the study, the intensive and controlled groups continued to be observed. Within one year the HbA1c values in each group were similar and the difference was insignificant at 3 years (8.1 versus 8.2%, P = 0.09) but over the continuing 7 years of the observational study the patients in the intensive control group continued to have less risk of developing retinopathy when compared with the control group(55).
The advantages of improved glycaemic control applied to all ages
studied and both genders. In particular a small subset of adolescents showed the same findings(56). In the Kumamoto study(53), 55 type 2 patients without retinopathy and 55 with retinopathy were assigned to either conventional (CIT) or intensive therapy (MIT). Progression of retinopathy in the secondary prevention group was 19.2% for MIT and 44% for CIT; in the primary prevention it was 7.7% for MIT and 32% for CIT. The authors concluded that progression was unlikely if HbA1c was below 6.5%.
In the UKPDS, Type 2 patients demonstrated an increased risk of the
chances of developing retinopathy for 3 – 5 years followed by a gradually increasing risk reduction of developing retinopathy(52). The observational data were analysed by a proportional hazards model which concluded that duration of diabetes and HbA1c values were best thought of as 2 components of glycaemic exposure(57).
There were 3867 newly diagnosed patients randomised to
conventional or more intense therapy. The mean HbA1c values achieved
19
over the following 10 years was 7% (6.2-8.2) in the more intense, and 7.9% (6.9-8.8) in the conventional. Intensive glycaemic control conferred a 34% risk reduction in development of retinopathy. There were no differences between the glycaemic treatment modalities for risk of developing retinopathy except for chlorpropamide which appeared deleterious. The risk of needing photocoagulation, and cataract extraction were significantly reduced. Initial post-study monitoring observational data (as yet unpublished) show a similar pattern to the DCCT with continuing improvement in the more intensively treated group. EVIDENCE LEVEL 1 3.3.3 Recommendations
Any reduction of HbA1c is beneficial in reducing the development of new and progression of existing retinopathy.
The following recommendations are made:
- patients should be aware of their HbA1c, what it means, and how to lower it.
- patients should be encouraged to lower their HbA1c, and be given the necessary treatment and support to allow this.
- if retinopathy is present HbA1c should be maintained at a level below 7% but caution should be exercised if high risk retinopathy is present.
- patients should be aware of the potential temporary worsening of retinopathy should diabetes control improve dramatically, but long term benefits should be emphasised
- Establishment of local links between ophthalmologists and physicians should be encouraged, in order to facilitate early referral for management of risk factors in progressive cases.
RECOMMENDATION LEVEL A 3.4. HYPERTENSION 3.4.1 Introduction
In Type 1 diabetes, hypertension is associated with developing abnormal renal function, including the early stages of abnormal urinary protein excretion. Hypertension is exceedingly common in Type 2 diabetes, with a prevalence of 80 – 85% in cohort studies. 3.4.2 Definitions
The definition of hypertension depends in part on the methods used to measure blood pressure.
The current British Hypertension Society guidelines define Hypertension in Diabetes Mellitus as systolic blood pressure greater than/equal to 140 mm Hg, and/or diastolic blood pressure greater than/equal to 90 mm Hg. Treatment targets should be systolic level <130
20
mm Hg and diastolic < 80 mm Hg. Lower levels may be required for younger patients with Type 1 diabetes and micrvascular complications. 3.4.2.1 Methods used to measure blood pressure.
In the UKPDS an electronic sphygmomanometer was used, the patient sat in a quiet room, on their own, and after 5 minutes rest, had a series of 4 readings separated by 2 minutes. The first reading was discarded, and the mean taken of the others. Similar methods were used in all other studies to prevent chance casual high readings. 3.4.2.2 Systolic or Diastolic blood pressure
To determine whether intensive diastolic blood pressure control offers additional benefit over moderate control, the Appropriate Blood
Pressure Control in Diabetes (ABCD) Trial(58) randomised patients to either intensive or moderate blood pressure control. Hypertensive subjects, defined as having a baseline diastolic blood pressure of 90 mmHg, were randomised to intensive blood pressure control (diastolic blood pressure goal of 75 mmHg) versus moderate blood pressure control (diastolic blood pressure goal of 80–89 mmHg). A total of 470 patients were randomised to either nisoldipine or enalapril and followed for a mean of 5.3 years. The mean blood pressure achieved was 132/78 mmHg in the intensive group and 138/86 mmHg in the moderate control group. Changes in retinopathy were a secondary outcome. Although intensive therapy demonstrated a lower incidence of deaths (5.5 vs. 10.7%, P = 0.037) (Fig.2), there was no difference between the intensive and moderate groups with regard to the progression of diabetic retinopathy and neuropathy. . At present, there is no definitive evidence suggesting increased benefits accruing from the treatment of systolic versus diastolic BP levels.
3.4.3 Relationship between hypertension and diabetic retinopathy
Hypertension has been found to be very important in determining the chances of developing retinopathy in observational studies. In Type 1 patients, antihypertensive treatment with ACE inhibitors resulted in a 23% reduction in the progression of retinopathy (13). In Type 2 diabetes, in the UKPDS study, tight control of blood pressure (144/82 mm Hg) versus ‘less’ tight control (152/87) resulted in 34% and 47% reduction in significant deterioration of retinopathy and visual acuity, respectively(59). This observational relationship can be applied throughout the entire blood pressure range with no apparent worsening of retinopathy with low blood pressure.
The beneficial effects of anti-hypertensive medication are
immediate, as are the deleterious effects of further increases in blood pressure or of stopping treatment, therefore regular measurement of blood pressure levels is needed, especially in the presence of established retinopathy.
21
3.4.4 Type of antihypertensive therapy.
The EURODIAB Controlled Trial of Lisinopril in Insulin Dependent Diabetes (EUCLID) study group(60) investigated the effect of lisinopril on
retinopathy in type 1 diabetes compared with placebo. Eligible patients were not hypertensive, and were normoalbuminuric (85%) or microalbuminuric. Patients assigned to lisinopril had significantly lower HbA1c at baseline. Treatment reduced the development of retinopathy, but the effect may have been due to its pressure-lowering effect(60). The ABCD study was unable to demonstrate any significant differences between ACE inhibitors and dihydropyridine calcium channel blockers(58).
Studies are currently in progress to examine the effects of blocking the Renin Angiotensin system in reducing the development/progression of retinopathy over and above the protection afforded by blood pressure control. Until then, reduction of blood pressure per se with any appropriate group of antihypertensive is of paramount importance. It may, however, be appropriate to utilise ACE inhibitors or angiotensin receptor antagonists as a part of the antihypertensive regimen, as many of the patients with retinopathy will have concomitant renal disease, where these agents do appear to posses a specific renoprotective effect, over and above blood pressure control. The beneficial effects of control of hypertension are immediate on starting treatment. However, the effects wear off as soon as control is lost as shown after cessation of the UKPDS: when blood pressure returned to control levels in the intensive treated group of patients at the end of the study, the chances of developing retinopathy were identical. 3.4.5 Recommendations
The following recommendations are made: - correct blood pressure measurement methodology should be used,
and not casual clinic measurements. - any reduction in blood pressure, especially systolic blood pressure is
beneficial. - patients should be aware of their blood pressure, what it means, and
how to lower it. - patients should be aware of the potential harm if they stop their
therapy and their blood pressure increases. - patients should be encouraged to lower their blood pressure, and be
given the necessary treatment and support to allow this. - there should be regular measurement of blood pressure, to ensure
continuing control. - if retinopathy is present systolic blood pressure should be below
130mm Hg. - an ACE inhibitor or angiotensin receptor antagonist antihypertensive
drug may be considered since it provides additional benefit, over and above its blood pressure lowering effect.
22
RECOMMENDATION LEVEL A 3.5.AGE 3.5.1 Relationship of age to vision impairment in diabetic patients
Older patients with diabetes have a greater risk of visual impairment(36). 3.6. PREGNANCY 3.6.1 Relationship of pregnancy to worsening diabetic retinopathy
Most pregnant patients with background retinopathy will not experience a worsening of their retinopathy during pregnancy. A small and unpredictable group of patients will progress rapidly to PDR; in addition, they remain at risk for a year post partum(61). It is difficult to separate the various likely factors for this since predictive factors include poor pre-pregnancy control of diabetes, rapid improvement of glycaemic control intensively during the early stages of pregnancy, and the development of pregnancy complications such as pregnancy-related hypertension, pre-eclampsia and fluid retention.
There is limited evidence that counselling to improve control before conception is beneficial, in terms of deterioration of retinopathy during pregnancy. 3.6.2. Recommendations
The following recommendations are made: - patients should have access to pre-pregnancy counselling, especially
for improvement in glycaemic control. - eyes should be screened before conception, in each trimester and
between 3-9 months post-natally. RECOMMENDATION LEVEL A 3.7. RENAL DISEASE 3.7.1. Introduction
There is an association between retinopathy and all levels of abnormal renal function, independent of duration of diabetes and level of glycaemic control, in both types 1 and 2 diabetes, especially in some ethnic groups. The commonest means of evaluating renal function is the measurement of urinary albumin excretion rates. In both Types 1 and 2 diabetes, renal disease evolves through a stage of normoalbuminuria, progressing to abnormal levels with microalbuminuria and finally to
23
persistent albuminuria (established nephropathy). Traditional measurements of renal function, such as urea and creatinine, may well remain normal until well into the established nephropathy stage (persistent proteinuria). All stages of abnormal renal function with abnormal urinary albumin excretion are associated with increased incidence of retinopathy. Deteriorating renal function is also invariably associated with hypertension, including patients with early nephropathy, as manifest by microalbuminuria, with further deleterious effects on the development and progression of retinopathy. 3.7.2. Definition
End stage renal failure is defined as a creatinine of greater than 500 µmol/l or requiring dialysis or transplantation. 3.7.3. Relationship between renal failure and worsening of diabetic retinopathy.
Patients with renal failure develop worsening of their retinopathy particularly affecting the macula (macular oedema), but are also at risk of PDR(62). This may relate to mode of therapy with haemodialysis being a stronger associated risk factor. Conversely treatment of the renal disease may be associated with an improvement in the retinopathy and a more beneficial response to treatment, as seen for instance after renal transplantation, particularly if combined with pancreas transplantation.
Patients with developing nephropathy as determined by the presence of microalbuminuria invariably have a rise in blood pressure, which may be the cause of the increased risk of retinopathy. 3.7.4. Recommendations
The following recommendations are made: - patients with retinopathy in the presence of established renal
dysfunction require more regular supervision of retinopathy. - aggressive blood pressure control is essential for reduction of the rate
of progression of both retinopathy and nephropathy. RECOMMENDATION LEVEL A 3.8. HYPERLIPIDAEMIA 3.8.1 Relationship between hyperlipidemia and diabetic retinopathy
In the WESDR and Hoorn(23, 63) studies there was a correlation between high cholesterol blood levels and risk of retinopathy in the diabetic population. This was not found in the UKPDS and as yet no randomised control trial has shown a benefit of lowering elevated cholesterol levels in
24
terms of risk reduction of development and progression of retinopathy or blindness. EVIDENCE LEVEL 1 3.9 SMOKING 3.9.1. Relationship between smoking and diabetic retinopathy
The relationship between cigarette smoking and microvascular complications of diabetes is complex. However, it appears that cigarette smoking is not a risk factor for the development or progression of retinopathy in observational studies(64). It is not clear if this is a direct causative relationship or a survivor artefact. Discontinuation of smoking is recommended for reducing the development other complications of diabetes, especially cardiovascular disease EVIDENCE LEVEL 1 3.10 ACE INHIBITION 3.10.1 Relationship between ACE inhibition and diabetic retinopathy
Several studies which are not placebo controlled have shown benefit of ACE Inhibition to diabetic retinopathy over and above blood pressure lowering(65), for instance the MICROHOPE study. In the UKPDS, there was no difference between those assigned to captopril compared with those assigned to atenolol(59). The effective mechanism for the benefits of blockade of the renin angiotensin system may be reduced intracapillary pressures, which may also apply to beta blockade. ACE inhibitor or angiotensin 2 receptor antagonist inhibition is beneficial in delaying progression of nephropathy and it is likely that ACE inhibition, beta-blockade and angiotensin 2 inhibition all have an effect at reducing the risk of developing retinopathy. EVIDENCE LEVEL 2 3.11. ASPIRIN AND THROMBOLYTIC THERAPY 3.11.1 Relationship of aspirin and thrombolytic therapy to diabetic retinopathy
Aspirin therapy does not reduce the risk of developing retinopathy, but also does not increase the incidence of retinal haemorrhages(66). Reperfusion therapy for acute myocardial ischaemia, with thrombolytic therapy, does not increase the risk of retinal haemorrhages. EVIDENCE LEVEL 1
25
3.11.2. Recommendation
The following recommendation is made: - retinopathy should not be a contraindication for aspirin therapy or
thrombolytic therapy for myocardial infarction. RECOMMENDATION LEVEL A 3.12 ANTIOXIDANTS. 3.12.1. Relationship of antioxidant therapy to diabetic retinopathy
Antioxidants are currently under evaluation for several age related and other diseases such as macular degeneration and cataract. The role of antioxidants in developing retinopathy, and changing existing retinopathy to more aggressive disease has been investigated with observational studies. There is no evidence of effectiveness(67). EVIDENCE LEVEL 2 3.13 ALCOHOL 3.13.1 Relationship of alcohol to worsening of diabetic retinopathy.
There is no consensus about the effects of alcohol consumption and the development or progression of diabetic retinopathy. One observational study reports worsening in some groups(68); whilst another found improvement(69). 3.14 COUNSELLING FOR DIABETIC RETINOPATHY 3.14.1 Introduction The management of the diabetic patient with retinopathy requires teamwork and close liaison between physicians, ophthalmologists, specialist diabetes nurses, general practitioners, practice nurses and paramedical staff including chiropodists, dieticians, screeners and many other personnel including psychologists. The patient and the health care team need to be kept informed. Only in this way will the risk factors be managed adequately. 3.14.2 Evidence for value of Counselling
The UKPDS Quality of Life study(70) showed that no particular treatment produced an adverse psychological event, but that complications did. Treatment for complications such as photocoagulation was an example of this effect, producing long term anxiety. Another observational population based study of Type 1 and 2, showed a significant and enduring elevation of anxiety and depression, above that normally presented in
26
community samples in people with diabetes who were newly registered blind or visually handicapped(71).
Screening for psychological distress and managing psychological
morbidity is therefore important. All health and social care professionals working with retinopathy need to be vigilant to the presence of psychological morbidity. This is currently not standard practice but if sufficient and timely could prevent psychological and physical deterioration, social exclusion and dependency. Such screening may be a desirable annual adjunct to attendance at an eye clinic and would require training of professionals both in identification and management of distress(72).
The latter study also showed that certain demographic features, coping styles and thinking style were predictive of poorer psychological outcome (lower age, poorer physical health status, perception of increased symptoms, denial, self-blame and lack of acceptance). It may be appropriate to focus assessment in these areas to develop early intervention strategies, particularly since avoidant coping strategies may interfere with the rehabilitative process. EVIDENCE LEVEL 1 3.14.3 Recommendations 3.14.3.1 Risk Factor Reduction Due to the chronic nature of and insidious development of diabetic complications many patients fail to appreciate the seriousness of the condition and the life-shortening effects of the disease, in particular, the clear evidence of the importance of establishing good glycaemic control to delay significantly the complications. This is especially true for retinopathy. The potential explanation of newly diagnosed retinopathy will depend on the pre-existent level of education. It is equally the remit of all medical personnel caring for one or more aspects of the diabetic state that they explain not only the value of good control of diabetes but that diet, exercise, avoidance of cigarette smoking and attention to weight will all have beneficial effects on the prevention of complications generally. Even in cases of advanced DR with maculopathy, it is not too late to institute a change of life-style which will benefit the end-organ disease.
Educational aids and advice on how to improve glycaemic and blood pressure control are now widely available, and in particular can be accessed from the Diabetes UK web site(73). For those who prefer other languages than English, the Australian web site is useful. 3.15.3.2. The Young Diabetic
27
A small sub-group of young, patients with type 1 diabetes appears to be susceptible to a particularly aggressive rapidly advancing form of PDR. In some cases, even extensive laser therapy fails to control the proliferative disease and extensive vitreo-retinal surgery is performed with limited functional success.
It is unclear whether poor compliance and/or poor attention to their diabetes is the main factor in the progression of the disease or whether other factors such as hormone dysfunction particularly growth hormone/IGF-1, have a part in this serious condition. These patients require special attention and monitoring and the value of frequent, positive counselling cannot be overstated. Alteration of their therapeutic regimen, including insulin therapy, may improve adherence, and consequently glycaemic control. 3.15.3.3. Driving and Visual Fields It is now recognised that panretinal photocoagulation (see Section 6,8 and 9) may have damaging effects on visual field function, in addition to the effects of retinopathy itself. In the UK, the Driving and Vehicle Licensing Authority (DVLA) has set minimal standards of visual field function which are required for permission to hold a Driver's License. All patients who require retinal photocoagulation should be asked to provide informed written consent to therapy as for any surgical procedure. It is the ophthalmologist's duty to explain clearly the reasons for laser therapy, the type of therapy to be undertaken and the likely effects on the patient's vision. In the UK, it is the patient's responsibility to inform the DVLA that he/she has had laser therapy for diabetic retinopathy. If this is not possible, then the patient's next of kin or GP should inform the DVLA of the patient's visual status. As a last resort the ophthalmologist is duty-bound to inform the Medical Adviser of the DVLA. Advice regarding driving restrictions on patients with diabetic retinopathy may best be provided in the form of an information leaflet. 3.15.3.4 Pregnancy Patients with diabetes who are considering pregnancy should preferably attend a pre-pregnancy clinic, with their husband / partner if possible, where the risks of pregnancy for the eyes can be carefully explained within the context of each patient's particular state of health. In particular, the potential deleterious effects of tightening control on retinopathy can be explained and the need for frequent monitoring of the retinopathy throughout the pregnancy. In addition, the safety of fluorescein angiography and or laser therapy if required during the pregnancy, can be emphasised.
28
The minimum recommendations suggested by Diabetes UK are that fundus examination should be performed at pre-pregnancy, at the diagnosis of pregnancy, at the end of each trimester and 9 – 12 months post-natally. More frequent examinations are recommended if active disease is detected. Patients who have become pregnant sometime after scatter PRP laser therapy for proliferative diabetic retinopathy are considered not at significant risk of developing reactivation of proliferative disease but should be monitored and counselled during their pregnancy. 3.15.3.5. Social Services for the Visually Handicapped In spite of appropriate treatment a small group of patients will fail to respond and progress inexorably to severe visual impairment and blindness. It is important that such patients are advised fully concerning the support services which are available to them through the Social Services and in particular what benefits are available to them to enable them to lead as normal a life as possible. In particular with appropriate visual aids they should be encouraged to maximise the residual vision which they possess. The ophthalmologist’s role is to ensure that such patients are referred to the appropriate professionals and services for their individual needs. Early registration with the Social Services will minimise the handicapping effects of visual impairment through the use of appropriate low visual aids for use at home and at work, including CCTV's (closed circuit television). Young people in particular benefit from mobility and rehabilitation support services of this nature. There should also be close liaison with the diabetes specialist nurse and often district nurse to ensure that treatment can be given easily without needing extra effort: dosette boxes for tablets, and different injection devices and insulin regimen can be helpful. RECOMMENDATION LEVEL A
29
SECTION 4 CLINICAL FEATURES OF DIABETIC RETINOPATHY
4.1 NON-PROLIFERATIVE DIABETIC RETINOPATHY (NPDR)(BACKGROUND AND PRE-PROLIFERATIVE) NPDR includes all forms of retinopathy which precede the development of new vessels. The AAO classification describes three grades (mild , moderate, severe) while the NSC-UK system describes two grades: background (Level R1) and pre-proliferative (Level R2) (see Section 1.2 and Appendix). Background retinopathy may consist of microaneurysms only (Fig. 3), progressing to microaneurysms and small haemorrhages ("dots”), and then to larger haemorrhages (blots") (Fig.4) which can be of various degrees (Fig.5). Flame shaped haemorrhages are also seen in combined hypertensive/diabetic retinopathy (Fig 6). Exudates (background retinopathy, Level 1), more common in Type II diabetes, are waxy yellow deposits with discrete edges, extending sometimes to the equatorial fundus often in clusters or forming circinate patterns whose centre may be a leaking microaneurysm (Fig 7). “Cotton wool spots” (CWS) (preproliferative retinopathy, Level 2), are fluffy white lesions representing ischaemia-associated lesions of the nerve fibre layer - hence are only found in the posterior retina where the nerve fibre layer is of appreciable thickness (Fig.8). They may appear suddenly during periods of changing glucose regulation and in association with hypertension. Venous dilatation may occur as an early sign (see Fig.5) but becomes more pronounced as more of the capillary bed is closed. A general dilatation of the veins is observable even when the retinopathy is mild and is to be distinguished from venous beading, which is a sign of preproliferative retinopathy (Level 2) (Fig.9). Beading is indicative of extensive non-perfusion (due to capillary closure) of the retina and manifests fusiform bulges in the wall of the vein (Fig 9). Fluorescein angiography will invariably show closure of the capillary bed on either side of the vessel (Fig. 10). A further important FFA sign of pre-proliferative disease is 360 degree of mid-peripheral non-perfusion which demarcates the ischaemic interface and guides future treatment protocols for photocoagulation (see Section 9)(74). Other signs of severe / preproliferative retinopathy are dilated capillaries which can mimic new vessels but are better described as intraretinal microvascular abnormalities (IRMA) (see Fig. 6). They frequently occur adjacent to CWS’s, and may be associated with other signs such as “omega” venous loops (Fig. 11,12), venous reduplication and white lines which represent occluded arterioles (Fig 13). According to the Early Treatment for Diabetic Retinopathy Study (ETDRS) report, severe / pre-proliferative retinopathy is definitely present if the signs conform to the following rule: ie the presence of venous beading and/or IRMA and /or large blot haemorrhages in 1-3 quadrants of the fundus(1).
30
A classification of NPDR as mild, moderate and severe has been proposed as an International Diabetic Retinopathy Severity Scale (see American Academy of Ophthalmology Web site: available at: http://www.aao.org/aao/education/library/) (3, 75, 76) and provides classification criteria used in several large studies including the DCCT(77) and the UKPDS(59, 78, 79). However, NPDR severity grading using the additional classification of mild, moderate, severe and very severe has been used for major studies such as the ETDRS and is based on standard photographs of fundus lesions set by the Airlie House Grading system (1, 80). Precise classifications for the purposes of clinical trials and other studies based on the Airlie House grading system have used the following criteria to define each of the grades of NPDR: • mild: at least one microaneurysm • moderate: severe retinal haemorrhages in at least one quadrant, or
CWS, venous beading or IRMA definitely present • severe: severe retinal haemorrhages in four quadrants; or
venous beading in 2 quadrants; or extensive IRMA in one quadrant • very severe: any two of the features of severe NPDR. This has later been simplified to three grades(1) as follows: Mild NPDR: at least one microaneurysm, but not as severe as moderate NPDR. Moderate NPDR: extensive intraretinal haemorrhages and/or microaneurysms, and/or cotton wool spots, venous beading or intraretinal microvascular abnormalities definitely present but not as severe as severe NPDR. Severe NPDR: cotton-wool spots, venous beading and IRMA all present in at least two quadrants; or two of them present in at least two quadrants with intraretinal haemorrhages and microaneurysms present in all quadrants; or IRMA present in each quadrant, being severe in at least one of them, but no PDR. However, such classifications are difficult to use in clinical practice on a routine basis since certain features such as venous beading are common to both moderate and severe retinopathy. It is preferable, therefore, to consider NPDR as either mild or "low risk" (ie not requiring regular close observation by an ophthalmologist) and severe or "high risk" (ie requiring regular close observation as a prelude to scatter panretinal photocoagulation (PRP)). This simple approach has been described previously(2) approximating to Level R1 (background) and Level R2 (pre-proliferative) using the NSC-UK system and may be of more value in practice (See Section 1, Table 1.1 and Appendix).
31
Therefore, for the purposes of defining those patients at risk of developing new vessels, the features of "low risk" (mild/moderate) NPDR (background DR) are : • mildly dilated veins, • microaneurysms, • dot haemorrhages, • exudates, • occasional CWS’s. and the features of "high risk", pre-proliferative (severe) NPDR are • IRMA, • venous beading and “omega” loops,
• clusters of large "blot" or "blotch" haemorrhages, • multiple CWS’s.
(Note, maculopathy is covered in section 2.4.) EVIDENCE LEVEL 1 RECOMMENDATION LEVEL A 4.2. PROLIFERATIVE DIABETIC RETINOPATHY (PDR) Proliferative retinopathy (PDR) usually appears late in the disease. However, PDR may occur with little warning in young adolescent or post-adolescent individuals and have a particularly aggressive course usually because of poorly controlled diabetes and often failure to attend for ophthalmological review. The retinopathy in these individuals may be “florid” see Section 9.5.3).
New vessels mostly arise from the venous side of the circulation and are recognisable by their abnormal location and their unusual pattern (Figs. 14, 15). Unlike normal vessels which have a branching pattern that divides dichotomously, new vessels form loops or rete (arcades). While normal vessels appear to supply or drain an area of retina, it may be difficult to identify such a role for new vessels. For example, a rete of vessels may arise from the main trunk of a vein and criss-cross the vessel randomly or a venule may arise from the disc and after forming a tortuous loop wind back towards the disc (Figs. 16,17,18). Early new vessels usually lie flat on the surface of the retina, but as the vitreous detaches, they are drawn forward.
Patients with new vessels individuals require extensive counselling (see Section 3). It is important to emphasise that new vessels by themselves rarely produce symptoms; their sequelae are the cause of visual loss.
New vessels are classified by (a) location and (b) severity (see Section 1.2.2). (a) Location. New vessels arise from the retina (NVE) (Figs 14,17) or the disc (NVD) (Figs.18-20). Most new vessels arise from veins in a central, circular
32
area about 31/2 disc diameters from the disc margin in any of 4 quadrants. New vessels may also arise peripherally and be missed on examination. In such patients there may also be evidence of rubeosis (iris new vessels, see below). Where there is sectoral ischaemia, new vessels characteristically arise at the junction of the perfused and non-perfused area as demonstrated on fluorescein angiograms (Figs. 21,22). In eyes with widespread ischaemia, NVD are common. Disc NVD may be flat or forward depending on the position of the posterior vitreous face. (b) Severity. New vessels per se do not cause visual loss. However, their sequelae may. Accordingly in attempts to define risk of visual loss, major treatment studies such as the DRS, the ETDRS and the DRVS(81-99) combined the dual risk of developing new vessels and of developing visual loss in a continuous grading system of retinopathy from preproliferative (severe and very severe retinopathy) to proliferative (early PDR, high risk PDR and severe PDR). Only the high risk PDR and severe PDR were recommended for pan-retinal photocoagulation in all cases. Severe PDR included cases of retinal fibrosis and tractional retinal detachment. Involutionary PDR is also a late form of PDR which has responded to treatment or regressed spontaneously (rare). EVIDENCE LEVEL 1 Untreated NV (D or E) lead to vitreous haemorrhage (VH) and blindness. VH may be subhyaloid before the vitreous is fully detached and present as small boat-shaped “crescents” with a level superior border where the PVD is present (Figs. 23-25).
In the late stage of the natural history of proliferative disease, fibrous tissue (gliosis) gathers around the new vessels and contraction of this tissue causes repeated bleeding and eventually, tractional retinal detachment. Occasionally, fine epiretinal gliosis occurs with minimal traction on the retina but this is uncommon. 4.3 MACULOPATHY Visual loss in diabetic maculopathy is usually the result of macular oedema but there is no direct correlation of the clinical appearance and degree of visual loss. Macular oedema may be difficult to detect; characteristically it appears as “retinal thickening” on binocular, stereoscopic slit lamp examination. Retinal thickening at the macula can be confirmed objectively by imaging techniques such as scanning laser ophthalmoscopy (100) and optical coherence tomography (OCT)(101-106) but most of these techniques have not as yet been validated in large multicentre studies.
When maculopathy occurs within one disc diameter of the fovea, it is termed clinically significant macular oedema (CSMO)(107) (See Section 7) since under these conditions it is considered to be visually threatening. This term was introduced to facilitate studies of laser therapy for macular oedema. However, the term itself is somewhat confusing since each of the
33
different types of CSMO may have different outcomes and the evidence for progression to sight loss is not clear since definitive natural history studies have not been performed. Current clinical trials of new medical therapies for macular disease may provide data on the natural history of macular disease.
Fluorescein angiography also reveals vessels with abnormal permeability causing leakage and pooling of dye in the late phase but this does not consistently correlate with CSMO(107, 108). A classification of maculopathy based on ophthalmological features is detailed below. However it is important to note that the terms “focal” and “diffuse” are used to convey a sense of the extent of macular involvement, and if the ophthalmological findings are interpreted in conjunction with the corrected visual acuity a more accurate impression of the severity of disease will be obtained. For instance, diabetic maculopathy with reduced vision may occur in the relative absence of CSMO and fluorescein dye leakage on angiography. In this condition, ischaemia is the likely pathology.
Maculopathy may also be tractional ie where there is vitreo-retinal adhesion and there is forward contraction of the vitreous gel from the retinal surface. This can be visualised by optical coherence tomography (OCT) and may constitute a component of mixed maculopathy (see below) 4.3.1 Clinical types of diabetic maculopathy 4.3.1.1. Focal maculopathy The characteristic features of focal maculopathy are well circumscribed, leaking areas associated with complete or incomplete rings of hard exudates. These are often related to micro-aneurysms, particularly in the centre of exudative rings (Figs 7,26,27). The exudative rings have a predilection for the perifoveal area where the retina is thickest. The focal areas of leakage are thickened by retinal oedema and fluorescein angiography is usually not necessary to identify them. 4.3.1.2 Diffuse maculopathy Diffuse maculopathy consists of generalised thickening of the central macula caused by widespread leakage from dilated capillaries in this area. Severe oedema is a feature and it is often associated with cystic changes. The other features of diabetic retinopathy may not be present and in particular there may be no exudates. In severe cases it may be impossible to identify the fovea due to the diffuse retinal thickening. The fluorescein angiogram may provide more definitive evidence of maculopathy than the ophthalmoscopic picture (Figs. 28,29). . There is evidence also that retinal pigment epithelial damage may contribute to the macular oedema probably by failing to remove the tissue fluid accumulating in the retina from the leaking capillaries(109). 4.3.1.3 Ischaemic maculopathy
34
Ischaemic maculopathy may be suspected, based on unexplained visual loss in the presence of a relatively normal looking macula. Blot haemorrhages in the paramacular region may be indicative of ischaemic maculopathy. There may be associated haemorrhages and exudates elsewhere. The exact extent of the ischaemia can only be seen on fluorescein angiography as shown by an increase in the foveal avascular zone (FAZ) (Fig. 30-32). It is therefore important that patients with maculopathy in which ischaemia is suspected are investigated with this technique. There does not appear to be a direct correlation between the visual acuity and the degree of ischaemia. Perifoveal microaneurysms in the absence of retinal thickening may indicate ischaemic maculopathy. In addition, sometimes there may be patches of ischaemia present within an area of exudative maculopathy indicated by a cotton wool spot (Fig.33). 4.3.1.4 Tractional maculopathy
Previously it has been accepted that vitreoretinal maculopathies are
due to traction caused by vitreoretinal adhesions or by membrane formation either as epiretinal membranous sheets or distinct transretinal bands. Tractional retinoschisis may also occur and may be one form of severe macular oedema. In the extreme form traction retinal detachment occurs (110).
Since the introduction of optical coherence tomography (OCT) imaging, it has become clear that a tractional element may apply to many diabetic maculopathies which appear predominantly intraretinal (101, 103, 106), and that the distinction between the two classes of maculopathy may be blurred. Difficulties relate to the interpretation of OCT images. Currently, several reports have established in-house methodologies for evaluation of the normal macula. Clear evidence of macular thickening has been demonstrated but the sensitivity and specificity of the technology has been validated in only a few centres and different centres adopt different criteria for examination (105, 111). However, it appears to be possible to differentiate between tractional and non-tractional macular pathology(101, 104, 105, 111). 4.3.1.3 Mixed maculopathy Many cases do not fit exactly into the groups described above. Frequently, there is combined pathology particularly of diffuse oedema and ischaemia. Variable degrees of traction may also be involved. Nevertheless, classifying the maculopathy according to its predominant features is useful from a therapeutic and prognostic point of view.
35
SECTION 5 SCREENING FOR DIABETIC RETINOPATHY
5.1 INTRODUCTION
Several guideline groups have published in recent years on various aspects of diabetic retinopathy, including NICE(112), SIGN(113) and HTBS (5, 114). This section of the revised RCOphth guidelines covers background issues in screening and makes specific recommendations of relevance to ophthalmologists. 5.2 DEVELOPMENT OF SCREENING IN THE UK
The development of screening in Europe was first encouraged by the St. Vincent Declaration which in 1992 set a target for reduction of new blindness by one third in the following 5 years (115). The British Diabetic Association (now Diabetes UK) supported the establishment of mobile photographic screening in a number of UK centres which has been shown to be effective with high sensitivities and specificities(116, 117). At the same time a number of optometry based programmes were reporting various levels of success. This led to calls for the introduction of screening in the UK(118, 119) which was taken up by the National Screening Committee (NSC) of the Department of Health with a proposed National Risk Reduction Programme(120). In late 2002 the National Service Framework for Diabetes was published which includes the specific requirement for the introduction of a national programme for screening for diabetic retinopathy in England and Wales(121). At the same time the Health Technologies Board of Scotland (HTBS) published its recommendations with detailed guidance on implementation(114) followed by the adopted grading scheme(5). At the time of publication an implementation process was underway in all four UK nations with the aim of 80% coverage by 2006 and 100% coverage by the end of 2007. A consensus grading protocol has been developed(4) and details are available on the NSC website(122). 5.3 EVIDENCE FOR THE EFFECTIVENESS OF SCREENING The evidence of effectiveness of screening is based on evidence of treatment efficacy presented later in Sections 7.3.1 and 9.3, especially after early detection, and of cost- effectiveness. Screening for diabetic retinopathy has been shown to be cost-effective in health economic terms(123-125). A Department of Health (DoH) commissioned three-centre study of cost-effectiveness in diabetic eye screening reported relatively high costs per true positive case detected(126, 127). This was improved in later studies using screening techniques with higher sensitivity and specificity(117). A health economics study of the effectiveness of changing from opportunistic to systematic screening reported a small incremental cost for a large increase in cases of sight threatening diabetic retinopathy (STDR) detected(128). Diabetic retinopathy therefore represents an
36
excellent paradigm for screening as laid out in the principles for screening of human disease described by Wilson and Junger in 1968(129). 5.4 ORGANISATION OF SCREENING SERVICES
The introduction of National Screening Standards by 2006 will alter significantly the delivery of screening in the UK. The key feature of these standards is the need for rigorous quality control at all stages and for all personnel. Internal and external quality control are requirements for screening services and will be monitored through regional quality assurance centres with submission of outcome data as a minimum data set to a central data quality network.
A key requirement for the introduction of systematic screening in the UK is the need for disease registers in all Primary Care Trusts. This will be essential to achieve full coverage of the target population. 5.5 SCREENING METHODOLOGY
Various screening methods have been employed in the past depending on local expertise and staff availability(117, 130). Because of the need for quality control the NSC has determined that the method of screening for England and Wales will be digital photography through dilated pupils. Scotland has adopted a non-mydriatic protocol with the option of pupil dilatation if images are poor.
Two options exist for the delivery of NSC/HTBS standard screening: (1) ambulant primary care based screening by teams of retinal screening technicians and (2) optometry based with photography in optometry practices. In each case grading will be performed using trained and quality controlled graders either in central grading units or in optometry based grading practices. During the transition to photographic screening slit lamp biomicrosopy will continue to be used by optometry screening systems.
Opportunistic screening should continue in diabetic clinics and elsewhere for case detection of patients who fail to attend or are missed from systematic screening.
It is recognised that photography cannot detect all cases of oedema particularly if not associated with exudates but these cases are relatively rare and should be detectable if the patient has symptoms of reduced vision. With rapid advancements in technology new approaches to screening may prove effective including computerised methods for detection and assessment of retinopathy(5, 131-133).
37
5.6 GRADING AND REFERRAL
A national consensus grading protocol has recently been agreed for England and Wales(4) with the following key principles :
- to detect any retinopathy - to detect the presence of sight threatening diabetic retinopathy
(STDR) - to allow precise quality assurance at all steps - to minimise false positive referral to the hospital eye service
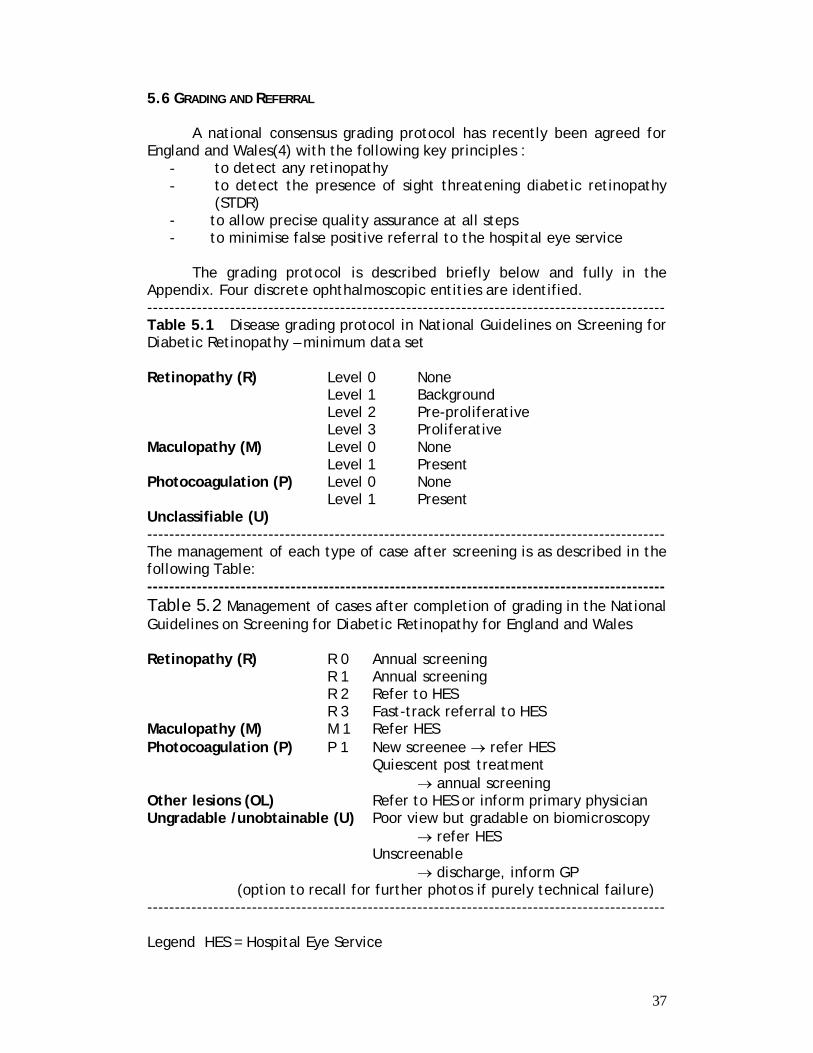
The grading protocol is described briefly below and fully in the
Appendix. Four discrete ophthalmoscopic entities are identified. ---------------------------------------------------------------------------------------------- Table 5.1 Disease grading protocol in National Guidelines on Screening for Diabetic Retinopathy – minimum data set Retinopathy (R) Level 0 None Level 1 Background Level 2 Pre-proliferative Level 3 Proliferative Maculopathy (M) Level 0 None Level 1 Present Photocoagulation (P) Level 0 None Level 1 Present Unclassifiable (U) ---------------------------------------------------------------------------------------------- The management of each type of case after screening is as described in the following Table: ---------------------------------------------------------------------------------------------- Table 5.2 Management of cases after completion of grading in the National Guidelines on Screening for Diabetic Retinopathy for England and Wales Retinopathy (R) R 0 Annual screening R 1 Annual screening R 2 Refer to HES R 3 Fast-track referral to HES Maculopathy (M) M 1 Refer HES Photocoagulation (P) P 1 New screenee → refer HES
Quiescent post treatment → annual screening
Other lesions (OL) Refer to HES or inform primary physician Ungradable /unobtainable (U) Poor view but gradable on biomicroscopy → refer HES Unscreenable
→ discharge, inform GP (option to recall for further photos if purely technical failure)
---------------------------------------------------------------------------------------------- Legend HES = Hospital Eye Service
38
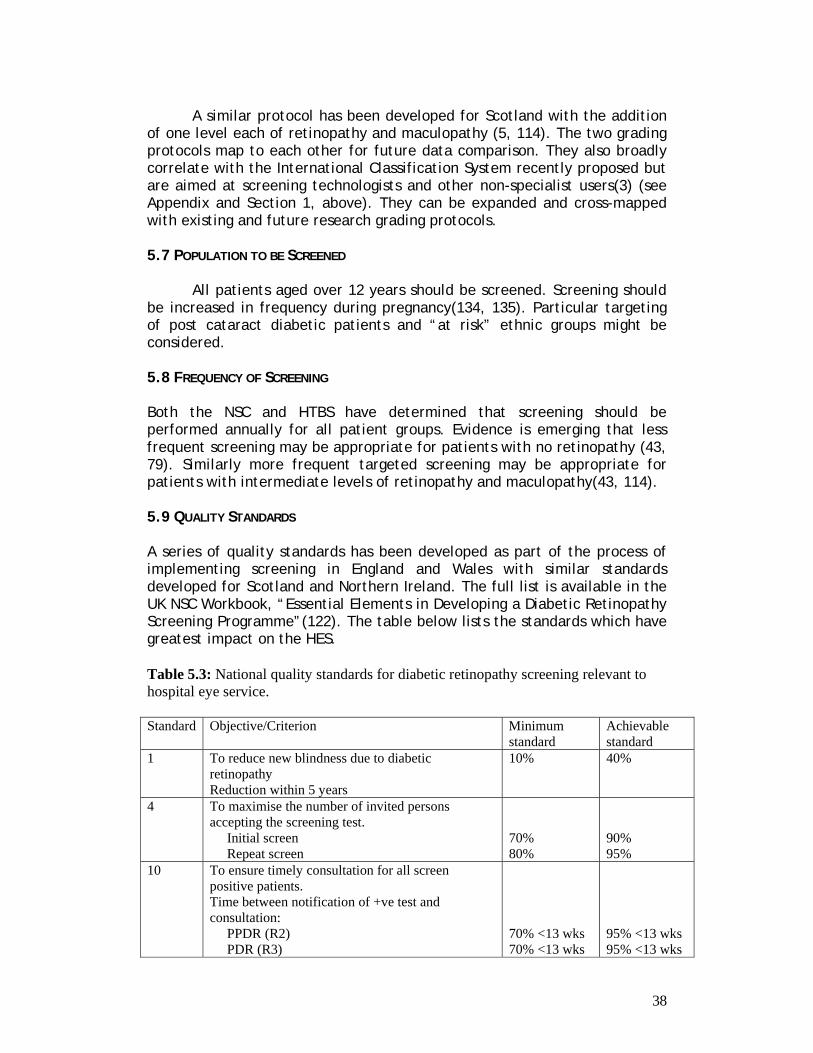
A similar protocol has been developed for Scotland with the addition of one level each of retinopathy and maculopathy (5, 114). The two grading protocols map to each other for future data comparison. They also broadly correlate with the International Classification System recently proposed but are aimed at screening technologists and other non-specialist users(3) (see Appendix and Section 1, above). They can be expanded and cross-mapped with existing and future research grading protocols. 5.7 POPULATION TO BE SCREENED
All patients aged over 12 years should be screened. Screening should be increased in frequency during pregnancy(134, 135). Particular targeting of post cataract diabetic patients and “at risk” ethnic groups might be considered. 5.8 FREQUENCY OF SCREENING Both the NSC and HTBS have determined that screening should be performed annually for all patient groups. Evidence is emerging that less frequent screening may be appropriate for patients with no retinopathy (43, 79). Similarly more frequent targeted screening may be appropriate for patients with intermediate levels of retinopathy and maculopathy(43, 114). 5.9 QUALITY STANDARDS A series of quality standards has been developed as part of the process of implementing screening in England and Wales with similar standards developed for Scotland and Northern Ireland. The full list is available in the UK NSC Workbook, “Essential Elements in Developing a Diabetic Retinopathy Screening Programme”(122). The table below lists the standards which have greatest impact on the HES. Table 5.3: National quality standards for diabetic retinopathy screening relevant to hospital eye service. Standard Objective/Criterion Minimum
standard Achievable standard
1 To reduce new blindness due to diabetic retinopathy Reduction within 5 years
10% 40%
4 To maximise the number of invited persons accepting the screening test. Initial screen Repeat screen
70% 80%
90% 95%
10 To ensure timely consultation for all screen positive patients. Time between notification of +ve test and consultation: PPDR (R2) PDR (R3)
70% <13 wks 70% <13 wks
95% <13 wks 95% <13 wks
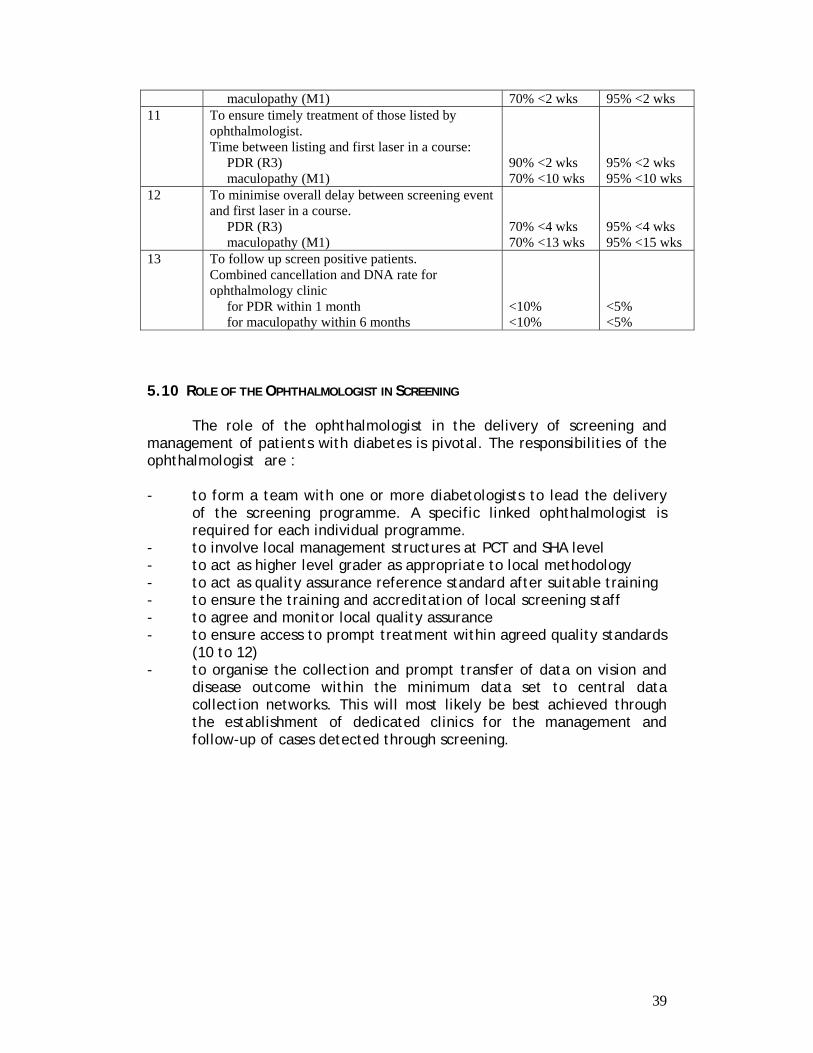
39
maculopathy (M1) 70% <2 wks 95% <2 wks 11 To ensure timely treatment of those listed by
ophthalmologist. Time between listing and first laser in a course: PDR (R3) maculopathy (M1)
90% <2 wks 70% <10 wks
95% <2 wks 95% <10 wks
12 To minimise overall delay between screening event and first laser in a course. PDR (R3) maculopathy (M1)
70% <4 wks 70% <13 wks
95% <4 wks 95% <15 wks
13 To follow up screen positive patients. Combined cancellation and DNA rate for ophthalmology clinic for PDR within 1 month for maculopathy within 6 months
<10% <10%
<5% <5%
5.10 ROLE OF THE OPHTHALMOLOGIST IN SCREENING
The role of the ophthalmologist in the delivery of screening and management of patients with diabetes is pivotal. The responsibilities of the ophthalmologist are :
- to form a team with one or more diabetologists to lead the delivery
of the screening programme. A specific linked ophthalmologist is required for each individual programme.
- to involve local management structures at PCT and SHA level - to act as higher level grader as appropriate to local methodology - to act as quality assurance reference standard after suitable training - to ensure the training and accreditation of local screening staff - to agree and monitor local quality assurance - to ensure access to prompt treatment within agreed quality standards
(10 to 12) - to organise the collection and prompt transfer of data on vision and
disease outcome within the minimum data set to central data collection networks. This will most likely be best achieved through the establishment of dedicated clinics for the management and follow-up of cases detected through screening.
40
SECTION 6 LASERS Photocoagulation for diabetic retinopathy is now performed almost exclusively with the use of ophthalmic lasers. There are various types of lasers currently in use and others under development. 6.1 METHOD OF LASER APPLICATION
Laser energy may be applied to the retina either through the dilated pupil using a contact lens or the indirect ophthalmoscope, or externally through the sclera. Transpupillary laser is normally applied using the slit-lamp bio-microscope and a contact lens. The modern wide-angled contact lenses are superior to the 3 mirror contact lens although the mirrors on the 3 mirror may enable laser to be applied more peripherally to the retina. Contact lenses such as the VOLK or MAINSTER or RODENSTOCK lenses give a good view of the macula, the equatorial and pre- and post- equatorial regions. These lenses give an inverted image but provide easy access to the retina even in the presence of media opacity such as mild to moderate cataract.
Lasers can also be applied using a non contact indirect method such as the 90 dioptre or 66 dioptre or superfield lenses again using a bio-microscopy technique with the slit-lamp. They may also be used with special adaptation of an indirect ophthalmoscope and this enables good access to peripheral retina and is the method of choice when applying laser during a general anaesthetic. It is very important to remember that the spot size may vary with the different types of lenses that are used and the operator should be familiar with the lens he or she normally uses. A sample of different spot sizes achieved with different lenses is shown in the table Table 6.1 at the end of this document
Trans-scleral laser therapy may also be used and a special
attachment for the DIODE laser is available for this application. The laser intensity is monitored through an indirect ophthalmoscope and lens. 6.2 LASERS
Optical radiations produced by gas or solid lasers are unique in that they are emitted at effectively one wavelength. DYE lasers are produced with inorganic dyes and have varying wavelengths (Fig. 34). Gas lasers (ARGON and KRYPTON) produce optical radiations in the visible spectrum while the newer DIODE lasers produce energy in the infrared band. The infrared lasers can be either continuous or multipulsed (MICROPULSE). Lasers act by inducing thermal damage after absorption of energy by tissue pigments. The three main pigments are luteal pigment, haemoglobin and melanin and the appropriate laser wavelength can be used to be selectively absorbed in one or more of these three pigments. The main target cell however is the pigment epithelium and this is site where much of the tissue damage is induced.
41
6.2.1 The ARGON Laser
The ARGON laser is the commonest and main source of laser energy for treating diabetic retinopathy. The ARGON laser produces two major peaks of energy in the 488 and 514 wavelengths (Figure 22). The 488 wavelength has been shown by reflection off the contact lens to cause operator blue colour vision damage and this wavelength is now filtered out of the system(136-139). The 514 wavelength has a potential for causing similar damage but this has as yet not been proven; to prevent reflection of this waveband there is a barrier filter and the aiming beam is replaced with a HeNe (helium neon) laser which is coaxial with the treating laser beam. This green laser energy is absorbed both by haemoglobin and by pigment epithelium. It is therefore possible with this wavelength to directly close microaneurysms or close new blood vessels and if applied over a retinal vessel, may cause spasm or closure of the vessel. However in clinical practice, although it is possible to close vessels, the main application of the laser is to the underlying pigment epithelium where it produces a visible burn. A burn if gently applied causes a blanching of the outer neural retina; a more intense laser burn will produce marked whitening of the entire retinal thickness with a surrounding pigment ring developing later. The energy applied to the pigment epithelium raises the temperature by approximately 10 degrees C with a temperature gradient from the centre of the burn to the adjacent retina resulting in enlargement of the visible area of RPE cell loss, damage to the neural retina and progressive choriocapillaris atrophy. It is therefore important that the laser energy should be set to induce a minimal reaction at the time of application.
Although the second peak from the ARGON laser is in the 488 this wavelength has now fallen into disuse. The disadvantages of this wavelength was that it is absorbed by the luteal pigment in the nerve fibre layer in the macular area risking damage to the perimacular nerve fibre layer. The 514 nm wavelength is minimally absorbed by the luteal pigment and therefore is safer for treatment of retina close to the macula(140-142). 6.2.2. The KRYPTON laser
KRYPTON laser peaks at 647 nm and 568 nm and thus emits in the red and yellow wavebands. The red waveband was initially thought to be useful in treating parafoveal lesions because it is not absorbed by luteal pigment. However, this colour is no longer used because of the super-sensitivity of the pigment epithelium to changes in power. A small increase in power changed a white RPE reaction either to a haemorrhage or to disruption of the pigment epithelium. A slight tilting of the lens leading to a change in the spot size had the same effect. The yellow peak of the KRYPTON laser is similar to the yellow of the DYE laser.
42
6.2.3. The DYE laser
The Dye laser (570nm – 630nm) was developed in order to give a variable wavelength laser in the green, yellow and red wavebands. In the green waveband it had no advantage over the ARGON laser and the red waveband is similar to the KRYPTON and has the same complications. However the yellow wavelength (577 nm) has gained some popularity because it is absorbed by haemoglobin and therefore direct closure of microaneurysms and blood vessels can be achieved. In addition, much less power is required compared to the ARGON laser to achieve a satisfactory burn and therefore in those patients with a low pain threshold or very thin retinas, this wavelength can be very helpful(143, 144). Some operators feel that they are most comfortable treating with this wavelength. The yellow wavelength can be obtained either with the KRYPTON laser or with the DYE laser. 6.2.4. The DIODE Laser
The DIODE laser at 810 nm in the infrared or invisible spectrum is delivered via a portable machine. The lack of a bright flash provides increased patient comfort. Also because of the minimal bleaching of the retina, rapid recovery from the laser treatment occurs. However with the DIODE laser the end point is more difficult to assess being a greyish lesion at the level of the pigment epithelium rather than more obvious white lesion produced by other wavelengths. If the laser surgeon is unaware of this difference, there may be a tendency to raise the power of the DIODE laser to produce a white lesion similar to that produced with the ARGON laser and that this more intense lesion may cause pain and excessive damage to the retina(145, 146). Around 9% of the energy from the diode laser is absorbed by the pigment epithelium, the remaining energy penetrating into the choroid to be absorbed by choroidal melanocytes compared to the 50% energy uptake by the RPE from the ARGON laser(147, 148)
The DIODE laser has been adapted to fire in a rapid sequence micropulse mode (THE MICROPULSE LASER). In this mode there are short applications of laser of approximately 100 micro-seconds in length with an interval in the region of 1900 micro-seconds. Thus 100 micro-bursts of the laser can be put into an envelope of 0.2 of a second. The method of application of this laser is to increase the power of the laser to achieve a whitening of the retina and then to reduce the energy levels by around 50% to continue treatment. The effect of this laser is to raise the temperature within the pigment epithelium by only thus minimising collateral damage to both neuroretina and choroid. In addition, unlike the DIODE laser in which pain may occur, with the MICROPULSE there is no associated pain. Initial non-randomised clinical studies in particular for diabetic maculopathy are encouraging(149, 150) and there is currently a large multi-centre study in progress comparing this laser with the ARGON laser.
43
6.2.5 The Frequency-doubled YAG laser Recent application of the frequency doubled YAG laser has shown that it is as effective in treatment of diabetic macular oedema as other laser types and that it is gaining some popularity(151, 152). 6.2.6 Lasers in Development The YLF laser (Yitrium Lithium Fluoride) is in the infrared wavelength. It is a picosecond multipulse laser which selectively destroys melanosomes within the pigment epithelial cells, leading to dysfunction but not death of the RPE cells. Thus, the YLF laser appears to induce even less collateral damage than the MICROPULSE laser. This laser is currently under clinical trial for treatment of diabetic maculopathy. 6..3. LASER APPLICATION : GENERAL PROTOCOLS
Laser treatment can be carried out either as a single application or in repeated sessions. Both eyes can be treated in the same session both for the macula and for the peripheral retina. Caution should be taken when treating in the macular area when there are associated exudates lying immediately adjacent to the fovea as sometimes when the oedema has been treated, the exudates increase and these can encroach into the fovea and permanently affect foveal function. Under these circumstances, the treatment should be fractionated. The aim of treatment of panretinal photocoagulation (PRP) is to destroy the areas where there is capillary non-perfusion / retinal ischaemia. In some eyes this may mean an initial treatment of over 2000 burns of 500 microns size, or more if the burn size is smaller. If there is an inadequate response without full regression of new vessels, then re-treatment can be carried out. This re-treatment can be performed within one month to three months of the initial treatment. If there has been insufficient laser prior to vitrectomy, then further laser can be applied during the vitrectomy via the indirect ophthalmoscope or the endolaser (see section on vitrectomy). RECOMMENDATION LEVEL A 6.4. SIDE EFFECTS OF LASERS 6.4.1 Pain
Delivery of laser energy to the ocular fundus may in some cases be associated with pain. Diode lasers may be more painful than conventional lasers. The cause of the pain is unclear but may be due to direct thermal damage to branches of the posterior ciliary nerves. Pain may be prevented with the use of simple analgesia but on occasion may require entonox, peribulbar anaesthesia, or less frequently general anaesthesia, to achieve a satisfactory full PRP particularly in patients with florid proliferative retinopathy in whom a delay in therapy may be risky. Pain may also be felt by patients who have had previous laser treatment if the new laser burns
44
encroach on the previously treated areas. It is therefore important when applying repeat laser therapy to try to avoid the previously treated areas. 6.4.2. Vitreous haemorrhage
Laser therapy in patients with forward new vessels may be sufficient to cause marked regression of vessels which separate from the posterior hyaloid face and produce vitreous and subhyaloid haemorrhage. In most cases this is a rare event but patients require information concerning this risk prior to initiation of therapy. 6.4.3. Effect on visual function
There is now good evidence that the risk of causing reduction in visual field is around 40-50% after full PRP. This has implications for fitness to drive and should form part of the information provided to patients prior to treatment(153-156). There may also be other more subtle effects of PRP on visual function such as some degree of loss of contrast sensitivity and a reduction in the ERG(157). Finally, it must be remembered that visual function may also be lost through inadvertent laser application to the foveal and parafoveal regions, or through the development of secondary neovascular membranes after focal treatment of microaneurysms. EVIDENCE LEVEL 1
Other persistent side effects that may occur following laser treatment are some loss of visual acuity, a possible reduction in accommodative power, some dimness of vision like looking through a neutral density filter, some patients may complain of nyctalopia(158). Loss of colour vision in the blue spectrum may occur following extensive peripheral laser treatment and photophobia may also occur after laser therapy. This photophobia is due to halation and although it may be helped by dark glasses, it is possibly helped more by shading the eyes. 6.4.4 Secondary choroidal neovascularisation
If laser application is applied very close to the macula and is of a high energy, then there is a risk of loss of central vision due to disruption of the pigment epithelium and Bruch’s membrane, giving rise to foci of chorioretinal neovascularistation, such as occurs spontaneously in exudative age-related macular degeneration (the disciform response). This may occur rapidly following laser treatment and may result in loss of central vision. There is an increased risk of choroidal neovascularisation when moving from a peripheral region to a more central region without appropriately reducing the power of the laser or taking account of possible effects of lens tilt. 6.4.5. Macular Burn It is very important to prevent the development of a foveal burn by constantly referring back to the macula to be sure that the laser does not
45
stray into the macular area. In addition, recognition is growing of the risk of extension of laser burn size with time into the foveal zone. 6.4.6. Macular oedema
Scatter peripheral pan-retinal photocoagulation has been reported to be followed by development or worsening of macular oedema which fortunately is transient but it is important to warn the patient that there may be some loss of vision following the laser treatment. It is important to treat the maculopathy either at the same time or prior to peripheral scatter retinal photocoagulation (PRP)(159-162). 6.4.7 Other side effects
Rare complications such as corneal burns, raised intraocular pressure or angle closure (associated with shallowing of the anterior chamber, choroidal effusion and accompanying myopia)(163) and preretinal or subretinal fibrosis have been reported. Full panretinal laser photocoagulation is commonly followed by pallor of the optic disc as a result of loss of some of the nerve fibre layer, particularly with relatively heavy burns. Such patients have poor pupillary reactions and dilate poorly with short-acting mydriatics. This can compromise examination of the fundus and increase difficulty with intraocular surgery, if required post laser. There is also the recognised potential risk of traction retinal detachment with PRP.
46
SECTION 7 MANAGEMENT OF DIABETIC MACULOPATHY The use of lasers to treat diabetic retinopathy is an invasive and destructive procedure and it is essential to obtain informed consent for each new treatment course as for any surgical procedure. 7.1 INTRODUCTION Diabetic maculopathy (DM) causes gradual and largely irreversible loss of central vision. Many patients with DM are elderly; thus assessment and treatment may be complicated by co-existing ocular pathology, such as cataract, glaucoma or poor mydriasis response. Medico-social problems may also militate against optimal management . Diabetic maculopathy is caused by oedema from leaking capillaries and/or ischaemia due to capillary loss. Diabetic changes in the choroidal vasculature may also worsen the ischaemia and contribute to the oedema by reducing retinal pigment epithelial function. Visual loss is largely due to disruption of the fovea and perifoveal neuro-retina by oedema. The ETDRS(107) and the British Multi-centre Photocoagulation Study(164) showed that macular photocoagulation was effective in slowing the cumulative rate of central visual loss due to macular oedema. The aim of treatment is to prevent further visual loss; since visual acuity rarely improves following treatment, best results are achieved by applying treatment before central vision deteriorates. Loss of central vision due to macular ischaemia or generalised oedema cannot be prevented by photocoagulation. Many cases of diabetic maculopathy involve co-existing macular oedema and ischaemia. In such cases the prognosis depends on the extent of the oedema and the severity of the ischaemia 7.2 DEFINITION Diabetic maculopathy is classified as focal, diffuse, ischaemic, tractional or mixed (see Section 1). For the purposes of treatment, laser therapy is recommended where there is evidence of clinically significant macular oedema (CSMO) despite the recognised difficulties with the definition of CSMO (see Section 4). CSMO has been defined by the ETDRS group as retinal thickening involving the centre of the macula in one of three ways(165): 1. thickening of the retina at or within 500 microns of the centre of the macula 2 . hard exudates at or within 500 microns of the centre of the macula, if associated thickening of the adjacent retina (not residual hard exudates remaining after disappearance of retinal thickening)
47
3. a zone or zones of retinal thickening one disc area or larger, any part of which is within one disc diameter of the centre of the macula
Retinal thickening is determined clinically by slit lamp biomicroscopy / indirect ophthalmoscopy or by evaluation of stereoscopic fundus photographs of the macular area. Fluorescein angiography is useful to evaluate leakage, while newer technology such as optical coherence tomography (OCT) may assist in objectively determining increases in retinal thickness (See Section 4). 7.3 EVIDENCE SUPPORTING TREATMENT RECOMMENDATIONS 7.3.1 Photocoagulation
Two RCTs have reported beneficial effects of focal argon laser to microaneurysms in the treatment of maculopathy. Blankenship and colleagues reported lower frequency of visual loss after 2 years in patients with symmetrical macular oedema and preproliferative retinopathy(166). The ETDRS found a significant reduction in moderate visual loss at 3 years in patients with macular oedema plus mild to moderate retinopathy compared to observation(165). Subgroup analysis found that treatment was significantly more effective in eyes with clinically significant macular oedema (CSMO), particularly in people in whom the centre of the macula was involved or imminently threatened(92, 167). In a third RCT, Olk found significant improvement in VA at 1 and 2 years in patients with diffuse maculopathy with or without CSMO treated with grid laser to zones of retinal thickening(168). Overall, photocoagulation reduced the risk of moderate visual loss (defined as a doubling of the visual angle, equivalent to loss of about two Snellen lines) by 50-70%(165, 168). However, it is clear that photocoagulation therapy does not per se lead to an improvement in vision and, while it reduces the risk of visual loss in a majority of patients particularly those with PDR, a significant proportion do not benefit from photocoagulation especially for macular disease. Despite this, there are currently no alternative validated therapies (see Section 7 below).
According to the ETDRS(165) which is the largest reported study
involving a control untreated group, treatment of diabetic maculopathy is indicated when there is clinically significant macular oedema (CSMO) involving the centre of the macula ie where retinal thickening has encroached to within <500 nm of the fovea. Although patients with normal central vision and CSMO were included in the study, clear benefit was achieved when pre-treatment visual acuity was < 6/9 and was most beneficial when vision was between 6/12 and 6/24. Controversy exists as to whether laser therapy is beneficial when CSMO co-exists with normal vision ie 6/6 or better. It is important to note that benefit in the ETDRS was taken as a delay in progression of visual loss ie that even when photocoagulation treatment was applied there was still an increasing, albeit at a slower rate, incidence of visual loss. While the ETDRS data indicated a trend towards benefit ie a 10% to 5% reduction in incidence of visual loss of 2 lines of
48
Snellin acuity equivalent in patients with CSMO and normal visual acuity, there was no statistical analysis to indicate that this was significant. Although the ETDRS study represents the main body of evidence demonstrating the value of laser therapy in the management of macular oedema, several points should be noted:
1. the study was designed to compare no therapy with any type of photocoagulation therapy, panretinal and/or focal, in the treatment of diabetic retinopathy, including maculopathy; subgroup analysis of different types of retinopathy was performed as the overall data was accumulated
2. focal photocoagulation referred to focal treatment in the macular area and included both direct laser therapy for focal lesions at the macula and grid therapy for diffuse macular oedema
3. treatable lesions ie leaking microaneurysms or diffuse macular leakage, were identified by fluorescein angiography Fluorescein angiographic evidence of retinal oedema in the absence of clinically obvious retinal thickening (Clinically Significant Macular Oedema, CSMO in the ETDRS(165) is not normally regarded as an indication for treatment. EVIDENCE LEVEL 2 7.3.2 Treatment of Systemic Risk Factors Data from the UKPDS (Type II diabetes)(42, 52, 57, 59, 78, 79, 169-173) and the DCCT (Type I diabetes)(174-182) indicate that the progression of non-proliferative diabetic retinopathy including maculopathy is significantly delayed by attention to general measures such as diabetes and blood pressure control, dietary (especially lipid) intake, and the taking of regular exercise if possible, combined with regular clinical observation (see Section 3). EVIDENCE LEVEL 1 7.3.3 Intravitreal Steroids Intraocular injections of crystalline steroid preparations (Triamcinolone) has been advocated for treatment of refractory CSME which has not responded to laser therapy(102, 183-187). Most studies are single case reports or open label interventional case series. No randomised control study of intravitreal steroids has yet been reported. The evidence to date is that retinal thickening as evaluated by optical coherence tomography as well as by clinical techniques can be reduced and there is some improvement in vision in some cases. A prospective study comparing a group of 20 patients treated by intravitreal steroid injection with a group of 16 patients treated with laser therapy indicated an beneficial effect on vision in the steroid treated group with no improvement in the laser treated group(184). Difficulties with control of intraocular pressure and
49
development of cataract have been experienced. In addition, the effect of treatment is transient and repeat injections are required. EVIDENCE LEVEL 2 7.3.4 Medical Treatment of Diabetic Maculopathy Considerable research is currently in place to determine the value of several pharmacologic approaches to the treatment of macular oedema. The EUCLID study of lisinopril indicated that there was 50% reduction in progression of retinopathy following use of the drug(60, 188) but the UKPDS data indicated that this effect was due predominantly to control of the hypertension(59, 169) and not primarily to effects of these drugs on the renin-angiotensin system(173, 189). Accordingly a larger trial is underway to determine whether there is an effect for delay in retinopathy progression in normotensive patients.
A further approach has been to determine whether inhibitors of protein kinae C may be beneficial for treatment of diabetic maculopathy on the basis of the anti-growth factor effects of the inhibitor. Initial results from a randomised controlled multicentre trial are inconclusive(190) and further trials are in progress. EVIDENCE LEVEL 1 7.3.5 Vitrectomy for treatment of tractional maculopathy (diffuse non-responsive macular oedema) Severe diffuse macular oedema which is non-responsive to grid laser photocoagulation or repeated grid laser photocoagulation, may benefit from vitrectomy with removal of the attached posterior hyaloid face. Cases likely to benefit have an appearance which may be very subtle, but presents as posterior hyaloid face thickening, surface wrinkling and a detectable sheen, or abnormal reflex from the inner limiting lamina (46). Evidence for the value of vitrectomy in tractional diabetic macular oedema comes mostly from interventional case series in cases of severe CSMO refractory to laser therapy(101, 103, 104, 106, 191-194). There has been one non-randomised control trial in which a small series of seven cases with previously untreated bilateral symmetrical tractional macular oedema were assigned to vitrectomy in one eye and laser to the second eye(193). The results showed some resolution of CSMO by OCT in both groups but with visual improvement only in the vitrectomised group. Approximately 50% of patients may experience modest improvement of vision, up to 2 lines or more. EVIDENCE LEVEL 2
50
7.4 RECOMMENDATIONS FOR TREATMENT 7.4.1 Photocaogulation
The cumulative evidence to date indicates that photocoagulation therapy remains the mainstay of therapy for sight-threatening diabetic macular oedema. Based on the evidence of the ETDRS(107, 108, 167, 195-200) and previous less extensive studies the following recommendations for the laser treatment of diabetic macular oedema, as identified as retinal thickening by clinical stereoscopic viewing on biomicroscopy or by stereoscopic fundus photographs, are proposed:
Laser therapy for maculopathy is recommended (1) where the centre of the macula is involved) in which vision is 6./9
or less. Laser treatment may be considered (2) only after counselling with regard to potential side effects and
risks of treatment for patients in patients where vision in 6/6 or better Laser therapy should involve scatter treatment in the area of leaking
lesions 500 microns or more distant from the centre of the macula. Where there are no discrete identified lesions ie where leakage is diffuse, a grid of laser therapy should be applied. Areas of leakage may be identified by fluorescein angiography RECOMMENDATION LEVEL A 7.4.2 Medical Treatment
Currently there are no recommendable pharmacological agents for treatment of diabetic retinopathy. In all patients but especially in those patients with maculopathy and vision of 6/6 or better, attention to possible systemic risk factors should be made (see Section 4). RECOMMENDATION LEVEL A 7.4.3 Intravitreal steroid therapy
No firm recommendations regarding the use of intravitreal steroids for diffuse non-responsive macular oedema can be made at this time but it should be noted that benefit is usually transient. RECOMMENDATION LEVEL B 7.4.4 Vitrectomy for diabetic macular oedema
51
Vitrectomy may be considered in selected cases of tractional severe macular oedema not responsive to other therapies (see Section 10). RECOMMENDATION LEVEL B 7.5 TREATMENT PROTOCOLS FOR DIABETIC MACULOPATHY
The aims of treatment are (a) to delay the progression of visual loss and (b) to promote resolution of maculopathy. These two aims overlap but are not necessarily equivalent. 7.5.1 Photocoagulation
The current standard of care for sight threatening diabetic maculopathy is focal laser photocoagulation, a term used to differentiate this form of treatment from pan-retinal photocoagulation. Focal treatment may be directly to leaking microaneurysms or administered as a grid to the macular area. Treatment is normally delivered via a slit-lamp / contact lens system involving topical corneal anaesthesia and placement of a hand-held contact lens.
Photocoagulation therapy for diabetic retinopathy is currently performed using custom-designed ophthalmic lasers (see Section 6). Safe treatment depends on accurate identification of the fovea and avoidance of excessively intense burns. The fovea can be difficult to identify if there is considerable oedema. Excessively intense burns can be avoided by starting treatment with very low powered burns, and gradually increasing the intensity until a satisfactory moderate blanching of the retina is achieved. Energy uptake varies, depending on the degree of the retinal oedema, so it is important to reduce power when treating less oedematous areas.
Satisfactory results can be achieved with a number of different light wavelengths (see elsewhere in these guidelines). The most frequently used wavelengths are 514nm (the “Green” component of the Argon Blue/Green laser) and 810nm (from the infra-red diode laser). The Argon blue/green laser should not be used for treatment of microaneurysms that are very close to the central area. This is because the blue light from this laser (487 nm) is absorbed by xanthophyll pigment overlying the parafoveal area. This can cause nerve fibre layer damage and parafoveal scotomata (see Section 6). In general, the blue laser waveband is not recommended due to its possible deleterious effects on the user (see Section 6). 7.5.1.1 Treatment of focal leaking areas at the macula (focal maculopathy) This type of maculopathy responds most readily to photocoagulation. Areas of focal leakage, usually at the centre of circinate exudative rings, (identifiable by fluorescein angiography), are treated using a 50-100 micron beam of 0.1 sec duration at sufficient power level to obtain moderate
52
blanching of the retina. Repeated "hits" can be applied to large microaneurysms (>40mm) When the microaneurysm is close to the fovea, a short (0.05sec) superficial burn just sufficient to blanch it may be used. However the treatment of microaneurysms within 300 �icrons of the centre of the fovea should be undertaken with caution because of the significant risk of closure of the perifoveal arcade or of direct foveolar coagulation.
An alternative to direct treatment of focal leakage is to apply a gentle grid to the entire circinate ring, including the margin, in a fashion similar to that used for diffuse maculopathy. RECOMMENDATION LEVEL A 7.5.1.2 Treatment of diffuse maculopathy Diffuse maculopathy is a more difficult form of diabetic retinopathy to treat. However, scatter laser photocoagulation has been accepted as the mainstay of therapy in the ETDRS(165). The technique consists of applying 100-200 micron burns delivered at a power level sufficient to obtain a minimum blanching reaction at the pigment epithelium in a scatter pattern over the central macula avoiding the fovea itself. Spacing of lesions by intervals of one burn diameter is recommended. Gentle treatment within the papillomacular bundle is safe to within one disc diameter of the optic disc and the centre of the macula provided microaneurysmsare not directly treated and re-treatment of the same spot is not performed. RECOMMENDATION LEVEL A 7.5.1.3 Treatment of Mixed maculopathy Focal and diffuse areas of oedema should be identified and treated as described above. RECOMMENDATION LEVEL A 7.5.1.4 Treatment of Ischaemic maculopathy Although the ETDRS included patients with perifoveal capillary closure in the design of the study and have recommended treatment of ischaemic maculopathy, there is no evidence that laser therapy is of value in isolated forms of this condition. However, if the degree of ischaemia is sufficiently large that it forms part of proliferative retinopathy, then this of itself may warrant therapy. RECOMMENDATION LEVEL C 7.5.2 Recommendations regarding vitrectomy for tractional macular oedema
53
The evidence in favour of this therapy is restricted to cases of tractional macular oedema not responsive to other means and in which there is evidence of a clear tractional component to the maculopathy with significant elevation of the retina. Preference is for objective clinical evidence via OCT or high resolution ultrasound in case selection and subsequent monitoring of results. The surgical goal should be the removal of all thickened posterior hyaloid and cortical gel material via a three port pars plan vitrectomy (see below). RECOMMENDATION LEVEL C 7.5.3 Diffuse maculopathy in the presence of neovascularistion. Occasionally maculopathy co-exists with disc or retinal neovascularisation. Whether to treat the new vessels with PRP or to treat the maculopathy first depends on the age of the patient and the relative severity of the retinopathy. In young patients with active new vessels it is generally recommended to treat the new vessels first with PRP since new vessels in these patients can advance rapidly with devastating consequences. In older patients, with NIDDM it is better to treat the maculopathy first or at least at the same time since PRP itself in these patients can hasten the progression of the maculopathy. Fractionating PRP into sessions of 700-800 burns separated by 2-3 weeks reduces the risk of this progression. RECOMMENDATION LEVEL C 7.6. FOLLOW-UP AFTER TREATMENT FOR DIABETIC MACULOPATHY Patients with diabetic maculopathy should be reviewed 3-4 months after treatment. If oedema persists, or if the visual acuity worsens, repeat fluorescein angiography may be helpful in identifying areas of residual focal leakage which should then be retreated. Treatment of leaking areas associated with exudates may cause regression of the exudates over many months. Since focal maculopathy can recur, patients with treated maculopathy should be followed for a sufficient time to ensure that the condition is inactive. Patients with cataracts and treated diabetic retinopathy should have the maculopathy reassessed before cataract surgery since surgery can induce recurrence or advance of existing macular oedema. Any persistent areas of oedema should be retreated either before or soon after surgery.
54
SECTION 8 MANAGEMENT OF NEW VESSELS ELSEWHERE (NVE)
8.1 INTRODUCTION NVE may occur on any vessel but usually are restricted to the major arcades of the posterior pole. Their presence can be verified by fluorescein angiography if there is doubt as to whether they are truly present and active. Panretinal photocaogaulation of the peripheral retina is the current standard of care based on several large treatment trials (see below). NVE may vary in their severity depending on age, glucose control, and other associated vascular disease and in minimal or early stages there is not the same urgency to treat as with NVD according to the ETDRS data (81-85, 87-92, 94-97, 157, 201-206). 8.2 DEFINITION NVE are defined as any abnormal collection of leaking vessels occurring on the retina outwith an area circumscribed by the distance of one disc diameter from the rim of the optic disc. They usually occur in the post-equatorial retina with a predilection for the vascular arcades. However, NVE in the nasal retina also occur, often as an initial focus, and may be easily missed. Untreated NVE in particular are associated with tractional retinal detachment, hence the importance of their early detection and treatment.
Rubeosis iridis also represents a form of neovascularisation occurring on the iris and may present in severe forms of diabetic ocular ischaemia. A short note on rubeosis is included at the end of this Section. 8.3 EVIDENCE FOR CURRENT STANDARD OF TREATMENT OF NVE The evidence for treatment of NVE is derived from the ETDRS and DRS studies(81, 85, 92, 206). EVIDENCE LEVEL 1 8.4 RECOMMENDATIONS FOR TREATMENT OF NVE PRP should be given with fully informed consent (see above under counselling, Sections 3 and 6) and can be tailored to the nature of the NVE in order to minimise effects on the visual field.
55
Based on the available evidence these guidelines recommend the following: --------------------------------------------------------------------------------------------- Condition observe PRP Vitrectomy ---------------------------------------------------------------------------------------------- Flat (early) NVE sometimes usually no Flat (mature / florid) NVE no yes sometimes Flat "stable" (treated) NVE yes +/- "fill-in" no Forward NVE no yes sometimes Forward NVE with VH no yes sometimes Forward NVE with traction RD no yes yes --------------------------------------------------------------------------------------------- RECOMMENDATION LEVEL A 8.5 TREATMENT PROTOCOLS
Treatment of NVE (and NVD, see Section 9) is by pan-retinal laser photocoagulation (PRP). Treatment is normally delivered via a slit-lamp / contact lens system involving topical corneal anaesthesia and placement of a hand-held contact lens as for laser therapy of macular oedema. To minimise discomfort in some patients peribulbar or retro-bulbar anaesthesia may be offered under appropriate expert control (see RCOphth Guidelines on Anaesthesia in Ophthalmology). For patients unable to comply with a slit-lamp delivery system, PRP may be delivered via a head-mounted binocular indirect ophthalmoscope system. Using this system it may be possible to deliver bilateral PRP in a single session.
Areas of retinal ischaemia as determined by fluorescein angiography should be preferentially treated and a more peripheral application of the laser burns helps to preserve more of the visual field. 8.5.1 Early NVE. Early NVE responds to a basic scatter PRP, defined as treatment of all four quadrants, by regression within days to weeks (Figs.35,36). A basic PRP comprises 1500-2000, 200-500 micron laser burns applied pre- and post- equatorially outside the vascular arcades. Lesions should normally be applied leaving lesion-wide (ie 200-500 micron) intervals throughout the fundus to preserve visual field. Some practitioners prefer routinely to use a smaller spot size such as 200�m but a correspondingly larger number of burns is required to achieve an effect. In addition, spot size will vary with the lens used (see Section 6). Sufficient energy should be applied to achieve "blanching" (ie a greyish white lesion) of the retina without producing
56
visible necrosis. The amount of energy required will vary for each patient and also at different retinal locations in the same eye depending on factors such as retinal thickness, oedema and degree of melanisation of the retinal pigment epithelium (the main energy absorbing tissue in this procedure) (see Section 6 on Lasers). 8.5.2 Progressive NVE. NVE may present as relatively advanced abnormal vascular structures (Fig. 11) which require a full PRP with particular attention being paid to the area of ischaemic retina in the proximity of the NVE but avoiding direct application to the new vessels (Fig.37). 8.5.3 Florid NVE. NVE may develop rapidly and in more than one site (Fig. 14). This condition requires aggressive management as for florid NVD (see below), attention being paid to the regions of ischaemic retina. 8.5.4 Non-responding NVE. On occasion, NVE may not fully respond to PRP and persist as foci of leaking vessels. Attempts should be made to close down such vessels with the application of further laser, particularly around the site of the NVE, in a series a short focal applications. The active vessels should be monitored every 2-3 weeks. 8.5.5 NVE with gliosis. NVE particularly on the vascular arcades may form firm vitreo-retinal adhesions which may promote the development of gliosis (Fig 38). Such lesions may act as the focus for traction on the retina, with retinal detachment, which, if treated too aggressively with laser therapy, may develop retinal holes and lead to rapidly extending, rhegmatogenous retinal detachment. Application of the laser some distance from the site of the gliotic NVE may help to induce regression of the new vessels. If the condition progresses however, for instance with vitreous haemorrhage or retinal detachment, vitrectomy may be required (see below). 8.5.6 NVE with vitreous haemorrhage. NVE are frequently the cause of vitreous haemorrhage but the site of bleeding may be masked by the blood (Figs. 24,25). NVE may be tracked to the point or tip of a subhyaloid haemorrhage. NVE with vitreous haemorrhage should be treated as for NVD with vitreous haemorrhage (see next Section).
57
8.6 NEW VESSELS ON THE IRIS (RUBEOSIS IRIDIS) 8.6.1 Introduction
Rubeosis iridis (Fig. 39) is a manifestation of severe retinal ischaemia and heralds the onset of rubeotic glaucoma. In the presence of clear media, further immediate photocoagulation should be applied since regression can be induced although this is perhaps better documented following central retinal vein occlusions(207). However rubeosis is often associated with advanced PDR rendering it impossible to apply further laser due to vitreous haemorrhage. In these circumstances prompt vitreous surgery is required to enable peroperative photocoagulation to be carried out (see Section 10 below). The results of the Early Vitrectomy Study show the benefits of surgery in eyes with severe neovascularisation and vitreous haemorrhage; thus, the presence of rubeosis indicates that surgery cannot be further delayed(208). Ultrasound examination is mandatory to exclude a retinal detachment, since co-existing rubeosis implies a poorer prognosis for surgery (see above). Utrasound biomicroscopy also may be of value to examine the peripheral retina and vitreous base / pars plana. EVIDENCE LEVEL 1 8.6.2 Therapy / Management
Glaucoma due to rubeosis responds poorly to standard trabeculectomy procedures(209). When trabeculectomy is combined with mitomycin-C however, the results are more encouraging(210), and compares favourably with other anti-proliferative agents such as 5-Fluorouracil(211) as well as other surgical procedures such as Molteno tubes and Cyclocryotherapy. When it is possible to apply further photocoagulation, trabeculectomy with mitomycin may be delayed to allow as much regression of the rubeosis as possible prior to surgery(209). However, many ophthalmologists believe that urgent aggressive management of rubeotic glaucoma, involving vitrectomy and extensive PRP are required to control the process, particularly if there is a minimal response to non-surgical approaches. In extreme cases cycloablation( destruction of the aqueous producing cells of the ciliary body may be necessary either by cylco-diode or cryotherapy. In eyes which are already blinded by rubeotic glaucoma, the aim is to achieve a pain-free condition. Under these circumstances, topical steroids together with atropine is the appropriate palliative treatment. EVIDENCE LEVEL 3 RECOMMENDATION LEVEL B
58
SECTION 9 MANAGEMENT OF NEW VESSELS ON THE DISC (NVD) 9.1 INTRODUCTION NVD usually indicate a measure of global retinal ischaemia which can be confirmed on fluorescein angiographic assessment of the peripheral fundus. Consequently, panretinal photocaogaulation of the peripheral retina is the current standard of care based on several large treatment trials as for NVE(76, 81, 83-85, 87-89, 91, 93, 95-97, 144, 157, 198, 202, 206, 212-215). NVD may however vary in their severity depending on age, glucose control, and other associated vascular disease(42, 52, 57, 59, 60, 75, 76, 79, 86, 89, 91, 108, 120, 169, 171, 188, 203, 216-233). 9.2 DEFINITION NVD are defined as any abnormal collection of leaking vessels occurring on the optic disc or within one disc diameter of the optic disc. They may be distinguished from collateral vessels by the presence of dye leakage on fluorescein angiography. 9.3 EVIDENCE FOR CURRENT STANDARD OF TREATMENT The initial evidence for the effectiveness of panretinal photocoagulation (PRP) was based on a number of uncontrolled or small clinical trials(163, 213, 214). The first definitive evidence for PRP in PDR-NVD was provided by the DRS / ETDRS in the USA and by the British Multicentre Study Group in Europe (see references cited in Section 9.1 above). The risk of severe visual loss in patients with high risk characteristics is reduced by 50% at 2 and 5 years by this therapy and by up to 70% in moderate risk patients(81). However, a reduction of the risk of severe visual loss in patients with early NVD or with severe or very severe ischaemic background retinopathy was not observed in these studies. Despite this, many ophthalmologists institute PRP at an earlier stage than recommended by the DRS or ETDRS
Scatter peripheral retinal photocoagulation (PRP) has been shown to be effective in six RCTs(84, 93, 164, 202, 214). Two British RCTs from the 1970s recruited patients with proliferative diabetic retinopathy and found that peripheral photocoagulation versus no treatment significantly reduced the risk of blindness after 2 or 3 years(164, 202). The Diabetic Retinopathy Study(84) found that early versus deferred argon treatment decreased the risk of severe visual loss at 5 years in patients with either preproliferative or proliferative retinopathy. A subgroup analysis(204) of the Early Treatment Diabetic Retinopathy Study (ETDRS)(93) found that the benefit was significant in people with type 2 diabetes and with severe preproliferative or early proliferative retinopathy without high risk characteristics. The British Multicentre Study(164) and the ETDRS(85) recruited patients with preproliferative disease most of whom had maculopathy; both found that
59
PRP significantly reduced the risk of visual deterioration at 5 years compared to no treatment. EVIDENCE LEVEL 1 9.4 RECOMMENDATIONS FOR TREATMENT PRP should be given with fully informed consent (see above under counselling, Section 3) and can be tailored to the nature of the NVD in order to minimise effects on the visual field.
Based on the available evidence these guidelines recommend the following: ---------------------------------------------------------------------------------------------- Condition observe PRP Vitrectomy ---------------------------------------------------------------------------------------------- Very severe (ischaemic) BDR yes no no Flat (early) NVD no yes no Flat (mature / florid) NVD no yes sometimes Flat "stable" (treated) NVD yes +/- "fill-in" no Forward NVD no yes sometimes Forward NVD with VH no yes sometimes Forward NVD with traction RD no yes yes ---------------------------------------------------------------------------------------------- RECOMMENDATION LEVEL A 9.5 TREATMENT PROTOCOLS Treatment of NVD (and NVE, see Section 8) is by pan-retinal laser photocoagulation (PRP). Treatment is delivered uniformly to the retina with particular attention to obvious areas of retinal ischaemia, frequently detectable in the temporal paramacular area. Treatment is usually restricted to retinal areas outside the vascular arcades unless the NVD is particularly active. 9.5.1 Early NVD. Newly-developing flat "early" new vessels usually respond well to a basic PRP comprising 1500-2000, 200-500 micron laser burns applied pre- and post- equatorially outside the vascular arcades as described above for NVE (Figs.40,41).
60
9.5.2 Established NVD. "Established" new vessels are those which have developed into mature branching and/or arcade formations, but are still "flat" ie they lie on the retinal surface, and have not led to haemorrhage. Established NVD may require a full PRP (>2000 laser burns) applied over more than one session. The precise number of burns will depend on the response to treatment which should be monitored at 2-3 weekly intervals. 9.5.3 Florid NVD. NVD in young adolescents may progress rapidly to extensive sheets of vessels occupying a wide region of the peripapillary retina (Fig 18). (Such vessels require urgent, aggressive management which should comprise a full PRP applied in a single session if possible. In appropriate circumstances this may require PRP delivery through a head-mounted binocular indirect ophthalmoscope system under general anaesthetic. Laser lesions should be sufficiently strong in florid retinopathy which may be difficult to achieve in the presence of vitreous opacities and retinal ischemia and is also difficult in lightly pigmented fundi. Further laser should be applied at weekly intervals until regression of vessels is achieved. If the neovascularisation cannot be controlled, vitrectomy with endolaser may be required (see Section 10). 9.5.4 Stable (quiescent, treated) NVD. NVD respond to PRP either by regressing completely (especially in older subjects and if treated early) or by "maturing" into non-leaking smaller vascular formations which do not progress. These can be described as "stable" NVD which require observation and monitoring, if necessary with fluorescein angiography, but probably do not require further photocoagulation. These patients can be followed in an accredited, systematic screening programme. 9.5.5 Non-responding NVD. In a proportion of patients, NVD fail to regress and/or mature into an inactive stable state. Inadequate laser therapy is a frequent cause, often due to poor patient compliance with the PRP procedure. This may be improved by performing the laser with local or general anaesthetic (see Section 6 above). In the latter case, the laser may be applied via the binocular indirect ophthalmoscope with good effect and a larger burn size (see above). Even if fully treated as described above, certain patients still fail to respond. Re-treating treated areas of the retina may then be performed, usually however at the expense of the visual field. This will affect the patient's fitness to drive and appropriate counselling is essential. Recourse to vitrectomy may be necessary if the neovascularisation cannot be controlled (see below).
61
9.5.6 Forward NVD Patients may present with untreated "forward" NVD or the NVD may project into the vitreous cavity during the course of treatment as a result of posterior vitreous detachment (PVD). In the absence of vitreous haemorrhage forward NVD should be treated urgently with a full PRP with the proviso that an overly aggressive PRP may induce too rapid a regression of the forward vessels and cause vitreous bleeding. In such circumstances vitrectomy and intra-operative endolaser therapy is likely to be the treatment of choice (see below). 9.5.7 NVD with vitreous haemorrhage. Treatment of NVD in the presence of small collections of subhyaloid or intra-gel blood should be aimed at performing a basic PRP (2000 laser burns, 500 micron) followed by careful application of further brief laser applications (200-300 laser burns per session) until regression of the NVD is achieved. However, this may not be successful and vitrectomy with endolaser may be required. RECOMMENDATION LEVEL A/B
62
SECTION 10 VITRECTOMY IN DIABETIC EYE DISEASE 10.1 SURGICAL OBJECTIVES Vitrectomy is a specialised procedure which is the domain of appropriately trained vitro-retinal surgeons. Vitrectomy surgery is used to achieve specific goals, which may limit or halt the progress of advanced diabetic eye disease. These are: • to remove vitreous opacity (commonly vitreous haemorrhage, also intra-ocular fibrin, or cells) and/or fibrovascular proliferation (severe extensive proliferative retinopathy; anterior hyaloidal fibrovascular proliferation) • to allow completion of panretinal laser photocoagulation (with the endolaser, introduced into the vitreous cavity or with the indirect laser ophthalmoscope), or direct ciliary body laser photocoagulation • to relieve retinal traction, tractional displacement or ectopia, traction detachment by removal or dissection of epiretinal membranes, in cases of non-rhegmatogenous retinal detachment • to achieve retinal reattachment by closure of breaks and placement of internal tamponade (in cases of combined traction/rhegmatogenous detachments). • to remove the posterior hyaloid face in some cases of diffuse macular oedema with posterior hyaloid face thickening 10.2 VITREOUS / SUBHYALOID HAEMORRHAGE 10.2.1 Definition
Vitreous haemorrhage is defined as bleeding into the vitreous cavity from ruptured normal or new retinal vessels, usually caused by forward detachment of the vitreous gel and leading to loss of vision from vitreous opacification. Vitreous haemorrhage may be intragel (ie into the vitreous substance) or retrogel (subhyaloid) when it occurs into the space between the detached vitreous gel and the retinal surfacce 10.2.2 Simple vitreous haemorrhage.
Simple vitreous haemorrhage occurs in the absence of other intravitreal pathology. It is a relative indication for vitreous surgery. DRS studies(234, 235) have shown that several factors should be considered: the patient’s age, the rapidity of progress and degree of severity of diabetic eye disease, the patient’s appreciation of risks, and benefits, of surgery, and the patient’s ability to co-operate with surgery, and in particular with post-operative positioning, and supplemental laser photocoagulation where indicated. Various types of simple vitreous haemorrhage occur as discussed below: 10.2 3. Severe non-clearing vitreous haemorrhage.
63
Vitreous haemorrhage often clears within a matter of days to weeks, and it is usually possible to achieve delivery of initial or supplemental panretinal laser photocoagulation without vitrectomy (see Section 6 on lasers). If laser photocoagulation is not possible, or vitreous haemorrhage persists for more than one month then vitrectomy should be considered since maculopathy and/or proliferative disease may progress unchecked, thus compromising the final visual result . Patients with Type II diabetes are less likely to have severe progressive proliferative retinopathy and while they also gain benefit from early surgery, as opposed to deferred surgery (surgery deferred for more than 6 months) the benefit is less. These patients should nonetheless have surgery within 3 to 6 months from onset of persistent non-clearing vitreous haemorrhage. Regular (2-4) weekly ultrasonic examinations are required to ensure early detection of retinal detachment, and clinical biomicroscopy to detect iris or iridocorneal angle neovascularisation, or haemolytic/ghost cell glaucoma. Patients with any of these complications should be considered for early vitrectomy(234-236). RECOMMENDATION LEVEL A Surgical Goals and Procedure For this indication the surgical goal is to remove the vitreous opacity through a 3-port pars plana vitrectomy procedure. The posterior hyaloid face should be removed (this is a structural support for fibrovascular proliferation and its removal usually prevents subsequent re-proliferation), and initial or supplemental panretinal laser photocoagulation should be performed to help prevent re-bleeding, re-proliferation, anterior hyaloidal fibrovascular proliferation, entry site complications (fibrovascular ingrowth) and rubeosis. 10.2.4 Non-clearing Post-vitrectomy Haemorrhage Post-operative inrtavitreal blood is common in the early post-vitrectomy period (~ 2-4 weeks) but usually clears spontaneously within a short time. Usually it takes the form of a diffuse vitreous haze generated by widespread fibrin deposition. Clearance is associated with spontaneous fibrinolysis which is often delayed in patients with diabetes. In all cases where the retina cannot be adequately visualised, it is essential to confirm the absence of underlying retinal detachment with ultrasonography. If cavity haemorrhage does not clear within the first few post-operative weeks, revision surgery should be considered. RECOMMENDATION LEVEL A Surgical Goals and Procedures
64
The surgical goal is to remove the haemorrhage, and treat the cause. Revision normally requires a 3-port pars plana vitrectomy to allow an adequate internal search for the source of bleeding. In particular, examination of the previous entry sites is important to search for possible bleeding sources, and top up PRP is indicated if previous phototherapy is found to be inadequate. 10.2.5 Dense Pre-macular Haemorrhage Subhyaloid premacular haemorrhages may be seen with or without associated intra-gel vitreous haemorrhage (Fig.42) usually in immediate vicinity of neovascular complexes. Limitation of blood to this site indicates incomplete vitreous detachment, providing a ready surface for continued forward proliferation of the new vessels and risk of tractional (tabletop) retinal detachment. Consequently, early vitrectomy should be considered to clear premacular haemorrhage. While temporising, PRP to visible, untreated areas of retina should be performed(237). Some surgeons also promote the use of YAG laser vitreolysis based on a number of small case series(238-244) (Figs. 43,44). Intravitreal tissue plasminogen activator has also been used to clear premacular haemorrhages(245).
Indications for vitrectomy in this type of haemorrhage include severe visual loss (for example in only eyes), failure of regression or resumption of haemorrhage after supplemental laser photocoagulation and the presence of significant subhyaloid pre-macular haemorrhage in eyes with good pre-existing panretinal laser photocoagulation. RECOMMENDATION LEVEL B Surgical Goals and Procedures A 3-port pars plana vitrectomy is performed taking care to remove the posterior hyaloid face, particularly from the posterior pole and the temporal arcades. Haemorrhage is removed, residual membrane dissected and supplemental panretinal endolaser photocoagulation is placed if needed. Long standing cases are more likely to require significant membrane dissection with its attendant risk of iatrogenic retinal break formation. 10.3 HAEMOLYTIC GHOST-CELL GLAUCOMA Elevated intra-ocular pressures may be caused by partially lysed red cells (red cell ghosts or “erythroclasts”) particularly in those eyes with a disrupted anterior hyaloid face after previous vitrectomy for vitreous haemorrhage(245), or in aphakic eyes with vitreous haemorrhage. "Erythroclasts" pass from the vitreous cavity into the anterior chamber and obstruct the trabecular meshwork. After a vitrectomy for diabetic vitreous haemorrhage, ghost cell glaucoma should be suspected in patients with elevated intraocular pressure in the early post-operative period(246). It is important to differentiate this condition from steroid induced glaucoma, since many of these patients may also be using topical steroid drops. The
65
physical signs of fine pigmented (cells) and flare in the anterior chamber indicate ghost cell glaucoma and may be subtle. Ghost cell glaucoma ia particularly common if vitrectomy is performed for removal of dense vitreous haemorrhage (ochre membrane). If the intra-ocular pressure remains elevated despite medical therapy after one to 3 weeks, surgery should be considered. RECOMMENDATION LEVEL B Surgical Goals and Procedures Revision pars plana vitrectomy with removal of all vitreous cavity and anterior chamber haemorrhage is the preferred surgical procedure. Glaucoma filtering surgery is usually not required. 10.4 RETINAL DETACHMENT 10.4.1 Tractional Macular Ectopia and Detachment Traction retinal detachment (TRD) arises from tension caused by contraction of the fibrovascular proliferations.(Fig 28.) The hazards of surgery are high in this condition, and thus vitrectomy in TRD is generally limited to those eyes with one of: a) involvement of the macula in the TRD; (b) evidence of a progressive, extensive extra-macular traction retinal detachment; (c) combined traction rhegmatogenous retinal detachment which threatens to involve the macular area (see below). Traction retinal detachment involving the macula is major indication for vitrectomy surgery if present for less than six months. Surgery in cases with macular involvement for more than 6 months is usually associated with little or no functional improvement and is not recommended(236, 247, 248). RECOMMENDATION LEVEL B Surgical Goals and Procedures In addition to removal of media opacity, specific goals include release of tractional components by removal of cortical vitreous and the posterior hyaloid vitreous face, dissection and removal of fibrovascular membranes, closure of persistently bleeding vessels and treatment of any iatrogenic retinal breaks. Cases with pure tractional elevation will experience spontaneous post-operative retinal reattachment and macular remodelling as a result of successful surgery. Anatomic success has been reported in between 64% to 80% or patients (with a 6 month follow-up) with visual function improvement in 26% to 65%(49, 52). 10.4. 2 Combined Traction - Rhegmatogenous Retinal Detachment Most extra-macular traction retinal detachments are only relative indications for surgery since they may remain stable for indefinite periods. In some patients the force of the fibrovascular traction is sufficient to create a retinal tear, often in relation to previous laser photocoagulation scars. These tears are frequently difficult to identify pre-operatively.
66
Clinically, a rhegmatogenous retinal detachment caused by fibrovascular proliferation presents with a convex configuration rather than the concave contour of a tractional, non-rhegmatogenous detached retina. In addition, white (hydration) lines in the inner retina, are more characteristic of a rhegmatogenous component. Surgery is indicated if there is sudden visual loss, evidence of progressive peripheral combined traction/rhegmatogenous retinal detachment, or evidence of progressive iris rubeosis. RECOMMENDATION LEVEL B Surgical Goals and Procedures Pars plana vitrectomy techniques are used to gain access to the retinal surface, to dissect fibrovascular membranes and thickened hyaloid face structures and thereby to relieve traction on and around retinal breaks. Vitrectomy also allows the performance of an internal search to help the actually identification of the retinal breaks. Subretinal fluid is removed and the retina reattached, followed by delivery of per-operative laser both locally to the break(s) and peripherally as supplemental or initial panretinal photocoagulation. Internal tamponade (gas, or silicone oil) will be necessary, and scleral buckles may be placed in some cases to support peripheral pathology, particularly if there has been extensive anterior hyaloid/pars plana proliferation. Care, however, should be taken to leave these patients phakic if at all possible. Accurate post-operative positioning is of critical importance. 10.5 SEVERE WIDESPREAD FIBROVASCULAR PROLIFERATION Some patients (typically young adult type 1 diabetics with a history of diabetes since childhood) are seen with a pattern of active fibrovascular proliferation that progresses despite extensive panretinal laser photocoagulation. These eyes have a high risk of severe visual loss and blindness. The Diabetic Retinopathy Vitrectomy Study Group(208) compared standard laser and vitrectomy indications (with vitrectomy for vitreous haemorrhage, or traction macular detachment) in a randomised fashion with early vitrectomy surgery, in a total of 370 eyes. The number of patients experiencing preservation of good visual function (20/40 or better) was almost twice as high in the early vitrectomy group (44%) compared to the conventional management group (28%) after 4 years of follow-up. However, the proportion of eyes with severe visual loss or blindness was similar in both groups and this stage was reached earlier in the early vitrectomy group. Clinical characteristics which warrant referral for early vitrectomy, even in the absence of extensive laser photocoagulation, include widespread fibrovascular proliferation (three disc diameters or more of fibrovascular tissue). It is to be emphasised that these patients frequently have extensive proliferation as their sole indication and do not necessarily have vitreous haemorrhage or macular tractional displacement. While these patients
67
should receive panretinal laser photocoagulation, the presence of high risk characteristics should indicate vitreoretinal referral at an early stage. RECOMMENDATION LEVEL B Surgical Goals and Procedures A 3-port pars plana vitrectomy is performed, with great care being taken to remove all detectable posterior hyaloid face which is typically adherent to the retina. 10.6 IRIS / ANGLE NEOVASCULARISATION WITH VITREOUS OPACITY Anterior segment neovascularisation which is mild and non-progressive may be safely monitored. Progressive iris or angle neovascularisation requires panretinal laser photocoagulation, and if vitreous haemorrhage prevents adequate and effective panretinal laser photocoagulation, vitrectomy with endolaser photocoagulation is indicated. Patients with established neovascular glaucoma may undergo combined surgery, comprising pars plana vitrectomy, with extensive endolaser photocoagulation and in some cases with additional direct ciliary body photocoagulation. This surgery is combined with silicone oil exchange in some eyes or with glaucoma filtration surgery in others. RECOMMENDATION LEVEL C 10.7 ANTERIOR HYALOIDAL FIBROVASCULAR PROLIFERATION / RETROLENTAL FIBROVASCULAR PROLIFERATION
Fibrovascular proliferation on the anterior hyaloidal surface or its remnant is typically seen after vitrectomy in severely ischaemic eyes of patients with type 1 diabetes mellitus. This fibrous tissue, which causes contraction of adjacent tissue and may cause peripheral traction retinal detachment, posterior iris displacement and lens displacement or recurrent vitreous haemorrhage, is highly vascular and difficult to treat. In some patients this process may be localised to the area of the entry site and is associated with typical sentinel vessels on the adjacent episclera and sclera(249). Anterior hyaloidal fibrovascular proliferation may also occur after cataract extraction in patients with active proliferative disease(250). RECOMMENDATION LEVEL B Surgical Goals and Procedure The surgical goal is to remove all fibrovascular tissue. This requires basal vitrectomy, lensectomy, membrane dissection and extensive, confluent laser photocoagulation to the peripheral retina and pars plana, often combined with scleral buckling surgery and silicone oil exchange. 10.8 VITRECTOMY FOR DIABETIC MACULAR OEDEMA

68
Vitrectomy for removal of hard exudates has been proposed, but
apart from an initial report(251) there have been no further studies for this indication alone.
Vitrectomy with posterior hyaloid face removal, with or without inner limiting lamina removal(252) has been advocated for non-ischaemic diffuse diabetic macular oedema which is not responsive to at least one macular grid laser treatment, and who have an attached posterior hyaloid. Vitrectomy surgery has been documented to be associated with improved visual acuity in other types of macular oedema, including pseudophakic macular oedema(253),and retinitis pigmentosa(254). In vitrectomy for diabetic macular oedema, case selection has varied, with initial studies attempting only to include cases with a taut posterior hyaloid, while later studies have not used this criterion.
Surgery is associated with a reduction in foveal thickness, as measured with optical coherence tomography, in many studies(101, 104, 193, 255-257). One study reports that the mean perifoveal capillary blood flow velocity was significantly increased after vitrectomy for macular oedema (2.19 mm per second to 2.68 mm per second postoperatively, P =.02), and that this was associated with complete regression of oedema in the 9 eyes studied(258). Many studies report visual benefit(194, 259) and approximately 40 to 50% of cases experience an improvement in acuity of 2 lines or more (LogMAR)(104, 193, 259-261). A recent study reports encouraging results with the final visual acuity improved by 2 or more lines in 32 of 65 eyes (45%), while remained unchanged in 49%, and worse in 6%(104). These apparently encouraging results were from a retrospective study with no control cases. There is a small fellow eye study(193) using cases with bilateral macular oedema, one eye operated. A controlled study of 15 operated eyes and 16 controls found an improvement in acuity in the treatment group, although the numbers were small and differences not statistically significant(260).
Most studies have significant design flaws. Most have been retrospective, or lacking in controls, and there are no randomised controlled studies reported to date. Statistical significance at the level of 0.02 or better is reported in most studies, but the small numbers mean that the confidence intervals are large. Since significant numbers of eyes are undergoing this surgery, with one group reporting follow up data on 485 eyes of 325 patients(262), the need for a prospective randomized controlled trial is apparent. EVIDENCE LEVEL 2 RECOMMENDATION LEVEL B
69
SECTION 11 CATARACT 11.1 INTRODUCTION
Cataract is common in diabetic patients, with prevalence rates of 8% of younger patients, and 25% of older-onset diabetic patients, over a 10 year study period(263). Acute metabolic cataract remains rare(264) . Indications for cataract surgery in diabetic eyes are similar to those in non-diabetic eyes. In addition, surgery may be indicated to allow accurate assessment of retinal disease, or to allow delivery of laser photocoagulation(265). 11.2 AIMS OF CARTARACT SURGERY IN PATIENTS WITH DIABETIC RETINOPATHY.
While the primary aim of cataract surgery is to restore vision, the recent trend towards lens extraction for early cataract raises issues for patients with diabetes, since it is recognized that there is a risk of progression of retinopathy after surgery (see below). In such situations, it is advisable to treat any retinopathy prior to surgery if possible. However, in the presence of cataract which precludes an adequate view of the fundus, a primary aim of surgery may be to permit fundus visualization. In such circumstances, it may be advisable to perform PRP with indirect laser at the time of surgery. 11.2 CATARACT SURGERY IN PATIENTS WITH DIABETES The major determinant of visual acuity outcome and complication rate are the level of maculopathy and the degree of underlying retinopathy, plus the overall care of the diabetes. It is therefore essential that these aspects are dealt prior to addressing other variables.
In general, cataract surgery and intraocular lens implant materials are well tolerated in patients with diabetes(266) and there are no obvious differences in post-surgical inflammation in eyes receiving hydrophobic acrylic lenses, or heparin surface-modified rigid polymethylmethacrylate lens implants(267). However, hydrophilic acrylic intraocular lens implants from some manufacturers have been associated with opacification in diabetic eyes(268, 269). Caution should be exercised if a hydrophilic intraocular lens implant is to be used in diabetic eyes.
Diabetic eyes, particularly those which have been treated with PRP,
may have poor pupil function and so may not dilate well at cataract surgery (20). Microscope-associated retinal phototoxicity is usually associated with prolonged operating times (usually in excess of 100 minutes), but has been described in short cases (operating times less than 30 minutes) in diabetic eyes(270). Care should be taken to ensure that diabetic cataract surgery is not prolonged, and that posterior pole illumination is minimised (pupil occlusion).
There is evidence that the size of the capsulorrhexis opening in cataract surgery may shrink in diabetic eyes, as opposed to non-diabetic
70
eyes(271-273). These changes were not apparent in the early post-operative period, but were present by 3 months follow-up. Silicone intraocular lens implants are also associated with significant anterior capsule fibrosis and shrinkage(274-277), sometimes leading to capsulophimosis or lens decentration, and are thus contra-indicated in diabetic eyes.
Diabetic eyes have a significantly higher rate of posterior capsule opacity requiring YAG laser capsulotomy(271, 278), although this does not correlate with degree of retinopathy. Massive proliferation of lens epithelial remnants has been reported in rare diabetic eyes after YAG laser capsulotomy(279).
Diabetic eyes undergoing combined cataract and glaucoma filtering
surgery have a similar course to non-diabetic eyes(280). EVIDENCE LEVEL 2 RECOMMENDATION LEVEL B 11.3 CATARACT SURGERY AND VITRECTOMY IN PATIENTS WITH DIABETES
Cataract may develop in as many as 75% of patients after diabetic vitrectomy (273). Consideration may therefore be given to performing combined lensectomy / vitrectomy routinely in diabetic patients requiring vitrectomy surgery since such patients respond well to combined vitrectomy and cataract surgery(281-284).
Although combined cataract and vitrectomy surgery achieves good
results, diabetic eyes undergoing this surgery are more likely than non-diabetic eyes to develop uveitis of varying degrees with posterior iris symechiae(285). EVIDENCE LEVEL 2 RECOMMENDATION LEVEL C 11.4 Cataract surgery, new vessels, rubeosis and risk of worsening retinopathy
Cataract surgery may precipitate aggressive iris neovascularisation, and if not recognised or treated swiftly and aggressively, may result in irreversible blindness(286). It is important that eyes with ischaemic retinopathy are identified and are treated with pan-retinal laser photocoagulation in the preoperative or per-operative period, as it may not be possible to deliver adequate laser treatment postoperatively(287).
Cataract surgery can be safely undertaken in diabetic eyes with iris
neovascularisation, with an acceptable complication rate (hyphaema,

71
fibrin), provided care is taken to treat the retinopathy in the preoperative or per-operative period(288). EVIDENCE LEVEL 3 RECOMMENDATION LEVEL C 11.5 Visual outcomes of cataract surgery
The presence and degree of maculopathy is the main predictor of final visual acuity after cataract surgery, while severity of retinopathy is also a significant factor(289, 290). Maculopathy present at the time of cataract surgery is unlikely to resolve spontaneously, while macular oedema developing after cataract surgery in non-diabetic patients is likely to resolve. Eyes with advanced diabetic retinopathy are much less likely to experience resolution of any post-cataract surgery macular oedema(291).
The risk of macular oedema(292) rises with severity of
retinopathy(293) and may occur in as many as 30% of patients with severe retinopathy(294, 295). Specific risk factors include severe retinopathy, known or pre-existing macular oedema, hypertension(295), and elevated aqueous growth factors such as VEGF [vascular endothelial growth factor] levels(295, 296). EVIDENCE LEVEL 2 11.6 Cataract surgery and progression of diabetic retinopathy
The question of whether cataract surgery causes more rapid progression of diabetic retinopathy has been raised in many studies(293, 297-304). There is evidence that progression is associated with longer operating times(302, 305). For patients with mild to moderate retinopathy, cataract surgery is a safe procedure with no significant risk of progression to sight-threatening complications(306). However, since early fluorescein leakage at the macula is common after cataract surgery, the differentiation of post-operative pseudophakic leakage and incipient diabetic maculopathy may be difficult. Careful monitoring is therefore required (see 11.5 above). EVIDENCE LEVEL 2

72
List of Working Party Members J.V.Forrester (Chair), F.Burden, A.H.M.Hamilton, M.Lavin, S.P.Harding, S.H.D.Wong, J.F.Talbot, J.Vora, R.Williams, Heidi Packer (College secretary).
73
REFERENCES
1. 1991. Grading diabetic retinopathy from stereoscopic color fundus photographs--an extension of the modified Airlie House classification. ETDRS report number 10. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98:786.
2. Royal College of Ophthalmologists. 1997. Guidelines for the management of diabetic retinopathy., London.
3. Wilkinson, C. P., F. L. Ferris, 3rd, R. E. Klein, P. P. Lee, C. D. Agardh, M. Davis, D. Dills, A. Kampik, R. Pararajasegaram, and J. T. Verdaguer. 2003. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 110:1677.
4. Harding, S., R. Greenwood, S. Aldington, J. Gibson, D. Owens, R. Taylor, E. Kohner, P. Scanlon, and G. Leese. 2003. Grading and disease management in national screening for diabetic retinopathy in England and Wales. Diabet Med 20:965.
5. Leese, G. P., A. D. Morris, and J. Olson. 2003. A national retinal screening programme for diabetes in Scotland. Diabet Med 20:962.
6. World Health Oragnisation. 2002. The World Health Report. In http://www/who.int/whr/en/.
7. Report of the Expert Committee on teh Diagnosis and Classification of Diabetes Mellitus. 1997. Diabetes Care 20:1183.
8. Bennett, N., T. Dodd, J. Flatley, S. Freeth, and K. Bolling. 1995. Health Survey for England, 1993. HMSO, London.
9. Nabarro, J. D. 1988. Diabetes in the United Kingdom: some facts and figures. Diabet Med 5:816.
10. Simmons, D., D. R. Williams, and M. J. Powell. 1991. The Coventry Diabetes Study: prevalence of diabetes and impaired glucose tolerance in Europids and Asians. Q J Med 81:1021.
11. Donnelly, R., A. M. Emslie-Smith, I. D. Gardner, and A. D. Morris. 2000. ABC of arterial and venous disease: vascular complications of diabetes. Bmj 320:1062.
12. National Society to Prevent Blindness. 1980. Visual Problems in the US: data analysis definitions. Data
74
sourcces, Detailed Data Tables, Anlysis, Interpretation., New York.
13. National Institutes of Health, and Natioanl Institute of Diabetes and Digestive and Kidney Diseases. 1995. Diabetes in America., Bethesda, MD.
14. Wan Nazaimoon, W. M., R. Letchuman, N. Noraini, A. R. Ropilah, M. Zainal, I. S. Ismail, W. B. Wan Mohamad, I. Faridah, M. Singaraveloo, I. H. Sheriff, and B. A. Khalid. 1999. Systolic hypertension and duration of diabetes mellitus are important determinants of retinopathy and microalbuminuria in young diabetics. Diabetes Res Clin Pract 46:213.
15. Dorf, A., E. J. Ballintine, P. H. Bennett, and M. Miller. 1976. Retinopathy in Pima Indians. Relationships to glucose level, duration of diabetes, age at diagnosis of diabetes, and age at examination in a population with a high prevalence of diabetes mellitus. Diabetes 25:554.
16. Frank, R. N., W. H. Hoffman, M. J. Podgor, H. C. Joondeph, R. A. Lewis, R. R. Margherio, D. P. Nachazel, Jr., H. Weiss, K. W. Christopherson, and M. A. Cronin. 1980. Retinopathy in juvenile-onset diabetes of short duration. Ophthalmology 87:1.
17. Klein, R., M. Palta, C. Allen, G. Shen, D. P. Han, and D. J. D'Alessio. 1997. Incidence of retinopathy and associated risk factors from time of diagnosis of insulin-dependent diabetes. Arch Ophthalmol 115:351.
18. Ramachandran, A., C. Snehalatha, V. Vijay, and M. Viswanathan. 1996. Diabetic retinopathy at the time of diagnosis of NIDDM in south Indian subjects. Diabetes Res Clin Pract 32:111.
19. Aiello, L. P., T. W. Gardner, G. L. King, G. Blankenship, J. D. Cavallerano, F. L. Ferris, 3rd, and R. Klein. 1998. Diabetic retinopathy. Diabetes Care 21:143.
20. Chang, C. J., C. C. Fu, M. S. Chen, C. L. Yang, Y. J. Chen, L. M. Chuang, T. J. Wu, and T. Y. Tai. 1990. A comparison of newly and previously diagnosed diabetics in Taiwan. J Formos Med Assoc 89:264.
21. Davis, T. M., I. M. Stratton, C. J. Fox, R. R. Holman, and R. C. Turner. 1997. U.K. Prospective Diabetes Study 22. Effect of age at diagnosis on diabetic tissue damage during the first 6 years of NIDDM. Diabetes Care 20:1435.
75
22. Hu, Y. H., X. R. Pan, P. A. Liu, G. W. Li, B. V. Howard, and P. H. Bennett. 1991. Coronary heart disease and diabetic retinopathy in newly diagnosed diabetes in Da Qing, China: the Da Qing IGT and Diabetes Study. Acta Diabetol 28:169.
23. Klein, R., B. E. Klein, S. E. Moss, and K. L. Linton. 1992. The Beaver Dam Eye Study. Retinopathy in adults with newly discovered and previously diagnosed diabetes mellitus. Ophthalmology 99:58.
24. Kohner, E. M., S. J. Aldington, I. M. Stratton, S. E. Manley, R. R. Holman, D. R. Matthews, and R. C. Turner. 1998. United Kingdom Prospective Diabetes Study, 30: diabetic retinopathy at diagnosis of non-insulin-dependent diabetes mellitus and associated risk factors. Arch Ophthalmol 116:297.
25. Wirta, O. R., A. I. Pasternack, H. H. Oksa, J. T. Mustonen, T. A. Koivula, H. J. Helin, and Y. E. Lahde. 1995. Occurrence of late specific complications in type II (non-insulin-dependent) diabetes mellitus. J Diabetes Complications 9:177.
26. Morgan, C. L., C. J. Currie, N. C. Stott, M. Smithers, C. C. Butler, and J. R. Peters. 2000. The prevalence of multiple diabetes-related complications. Diabet Med 17:146.
27. Prasad, S., G. G. Kamath, K. Jones, L. G. Clearkin, and R. P. E.-. Phillips. 2001. Prevalence of blindness and visual impairment in a population of people with diabetes. Eye 15:640.
28. Sparrow, J. M., B. K. McLeod, T. D. Smith, M. K. Birch, and A. R. Rosenthal. 1993. The prevalence of retinopathy and maculopathy and their risk factors in the non-insulin-treated diabetic patients of an English town. Eye 7:158.
29. Younis, N., D. M. Broadbent, S. P. Harding, and J. R. Vora. 2002. Prevalence of diabetic eye disease in patients entering a systematic primary care-based eye screening programme. Diabet Med 19:1014.
30. McLeod, B. K., J. R. Thompson, A. R. Rosenthal, and e. al. 1988. The prevalence of retinopathy in the insulin-requiring diabetic patients of an English town. Eye 2:424.
31. Broadbent, D. M., J. A. Scott, J. P. Vora, and S. P. Harding. 1999. Prevalence of diabetic eye disease in an inner city population: the Liverpool Diabetic Eye Study. Eye 13:160.
32. Younis, N., D. M. Broadbent, S. P. Harding, and J. P. Vora. 2002. Prevalence of Diabetic Eye Disease in Patients
76
Entering a Systematic Primary Care Based Eye Screening Programme. Diabetic Medicine 19:1014.
33. Klein, R., B. E. Klein, S. E. Moss, M. D. Davis, and D. L. DeMets. 1984. The Wisconsin epidemiologic study of diabetic retinopathy. IV. Diabetic macular edema. Ophthalmology 91:1464.
34. Klein, R., B. E. Klein, S. E. Moss, and K. J. Cruickshanks. 1998. The Wisconsin Epidemiologic Study of Diabetic Retinopathy: XVII. The 14-year incidence and progression of diabetic retinopathy and associated risk factors in type 1 diabetes. Ophthalmology 105:1801.
35. Mitchell, P., W. Smith, J. J. Wang, and K. Attebo. 1998. Prevalence of diabetic retinopathy in an older community. The Blue Mountains Eye Study. Ophthalmology 105:406.
36. Hayward, L. M., M. L. Burden, A. C. Burden, H. Blackledge, N. T. Raymond, J. L. Botha, W. S. Karwatowski, T. Duke, and Y. F. Chang. 2002. What is the prevalence of visual impairment in the general and diabetic populations: are there ethnic and gender differences? Diabet Med 19:27.
37. Harris, M. I., R. Klein, C. C. Cowie, M. Rowland, and D. D. Byrd-Holt. 1998. Is the risk of diabetic retinopathy greater in non-Hispanic blacks and Mexican Americans than in non-Hispanic whites with type 2 diabetes? A U.S. population study. Diabetes Care 21:1230.
38. Kalk, W. J., J. Joannou, S. Ntsepo, I. Mahomed, P. Mahanlal, and P. J. Becker. 1997. Ethnic differences in the clinical and laboratory associations with retinopathy in adult onset diabetes: studies in patients of African, European and Indian origins. J Intern Med 241:31.
39. Das, B. N., J. R. Thompson, R. Patel, and A. R. Rosenthal. 1994. The prevalence of eye disease in Leicester: a comparison of adults of Asian and European descent. J R Soc Med 87:219.
40. Klein, R., B. E. Klein, and S. E. Moss. 1990. The Wisconsin epidemiologic study of diabetic retinopathy: an update. Aust N Z J Ophthalmol 18:19.
41. Klein, R., B. E. Klein, and S. E. Moss. 1996. Relation of glycemic control to diabetic microvascular complications in diabetes mellitus. Ann Intern Med 124:90.
42. Stratton, I. M., E. M. Kohner, S. J. Aldington, R. C. Turner, R. R. Holman, S. E. Manley, and D. R. Matthews. 2001. UKPDS 50: risk factors for incidence and progression of
77
retinopathy in Type II diabetes over 6 years from diagnosis. Diabetologia 44:156.
43. Younis, N., D. M. Broadbent, S. P. Harding, and J. P. Vora. 2003. Incidence of sight-threatening retinopathy in Type 1 diabetes in a systematic screening programme. Diabet Med 20:758.
44. Younis, N., D. M. Broadbent, J. P. Vora, and S. P. Harding. 2003. Incidence of sight-threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 361:195.
45. Prasad, S., G. G. Kamath, K. Jones, L. G. Clearkin, and R. P. Phillips. 2001. Prevalence of blindness and visual impairment in a population of people with diabetes. Eye 15:640.
46. Janghorbani, M. B., R. B. Jones, and S. P. Allison. 2000. Incidence of and risk factors for cataract among diabetes clinic attenders. Ophthalmic Epidemiol 7:13.
47. Cohen, D. L., H. A. Neil, J. Sparrow, M. Thorogood, and J. I. Mann. 1990. Lens opacity and mortality in diabetes. Diabet Med 7:615.
48. Cohen, D. L., H. A. Neil, M. Thorogood, and J. I. Mann. 1991. A population-based study of the incidence of complications associated with type 2 diabetes in the elderly. Diabet Med 8:928.
49. 1990. UK Prospective Diabetes Study 7: response of fasting plasma glucose to diet therapy in newly presenting type II diabetic patients, UKPDS Group. Metabolism 39:905.
50. 1995. The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the diabetes control and complications trial. Diabetes 44:968.
51. 1993. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 329:977.
52. 1998. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 352:837.
53. Ohkubo, Y., H. Kishikawa, E. Araki, T. Miyata, S. Isami, S. Motoyoshi, Y. Kojima, N. Furuyoshi, and M. Shichiri. 1995.
78
Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract 28:103.
54. 1995. Progression of retinopathy with intensive versus conventional treatment in the Diabetes Control and Complications Trial. Diabetes Control and Complications Trial Research Group. Ophthalmology 102:647.
55. 2002. Effect of intensive therapy on the microvascular complications of type 1 diabetes mellitus. Jama 287:2563.
56. White, N. H., P. A. Cleary, W. Dahms, D. Goldstein, J. Malone, and W. V. Tamborlane. 2001. Beneficial effects of intensive therapy of diabetes during adolescence: outcomes after the conclusion of the Diabetes Control and Complications Trial (DCCT). J Pediatr 139:804.
57. Stevens, R. J., I. M. Stratton, and R. R. Holman. 2002. UKPDS58--modeling glucose exposure as a risk factor for photocoagulation in type 2 diabetes. J Diabetes Complications 16:371.
58. Estacio, R. O., B. W. Jeffers, N. Gifford, and R. W. Schrier. 2000. Effect of blood pressure control on diabetic microvascular complications in patients with hypertension and type 2 diabetes. Diabetes Care 23 Suppl 2:B54.
59. 1998. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. Bmj 317:703.
60. Chaturvedi, N., A. K. Sjolie, J. M. Stephenson, H. Abrahamian, M. Keipes, A. Castellarin, Z. Rogulja-Pepeonik, and J. H. Fuller. 1998. Effect of lisinopril on progression of retinopathy in normotensive people with type 1 diabetes. The EUCLID Study Group. EURODIAB Controlled Trial of Lisinopril in Insulin-Dependent Diabetes Mellitus. Lancet 351:28.
61. 2000. Effect of pregnancy on microvascular complications in the diabetes control and complications trial. The Diabetes Control and Complications Trial Research Group. Diabetes Care 23:1084.
62. Skyler, J. S. 2001. Microvascular complications. Retinopathy and nephropathy. Endocrinol Metab Clin North Am 30:833.
79
63. van Leiden, H. A., J. M. Dekker, A. C. Moll, G. Nijpels, R. J. Heine, L. M. Bouter, C. D. Stehouwer, and B. C. Polak. 2002. Blood pressure, lipids, and obesity are associated with retinopathy: the hoorn study. Diabetes Care 25:1320.
64. Moss, S. E., R. Klein, and B. E. Klein. 1996. Cigarette smoking and ten-year progression of diabetic retinopathy. Ophthalmology 103:1438.
65. 2000. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet 355:253.
66. Chew, E. Y., M. L. Klein, R. P. Murphy, N. A. Remaley, and F. L. Ferris, 3rd. 1995. Effects of aspirin on vitreous/preretinal hemorrhage in patients with diabetes mellitus. Early Treatment Diabetic Retinopathy Study report no. 20. Arch Ophthalmol 113:52.
67. Mayer-Davis, E. J., R. A. Bell, B. A. Reboussin, J. Rushing, J. A. Marshall, and R. F. Hamman. 1998. Antioxidant nutrient intake and diabetic retinopathy: the San Luis Valley Diabetes Study. Ophthalmology 105:2264.
68. McKay, R., C. A. McCarty, and H. R. Taylor. 2000. Diabetic retinopathy in Victoria, Australia: the Visual Impairment Project. Br J Ophthalmol 84:865.
69. 1994. UK Prospective Diabetes Study (UKPDS). XI: Biochemical risk factors in type 2 diabetic patients at diagnosis compared with age-matched normal subjects. Diabet Med 11:534.
70. 1999. Quality of life in type 2 diabetic patients is affected by complications but not by intensive policies to improve blood glucose or blood pressure control (UKPDS 37). U.K. Prospective Diabetes Study Group. Diabetes Care 22:1125.
71. Robertson, N., F. Burden, M. L. Burden, K. Caesar, and J. Allen. 2003. Psychological adjustment and coping in visual loss associated with diabetes, a longitudinal study. Diabetic Medicine 20 suppl:24.
72. RNIB. 2003. See change. Improving the way health and social care organisations provide services for older people with sight problems.
73. Diabetes UK. 2003. web site. http://www.diabetes.org.uk.
80
74. Shimizu, K., Y. Kobayashi, and K. Muraoka. 1981. Midperipheral fundus involvement in diabetic retinopathy. Ophthalmology 88:601.
75. Aiello, L. P., M. T. Cahill, and J. S. Wong. 2001. Systemic considerations in the management of diabetic retinopathy. Am J Ophthalmol 132:760.
76. Aiello, L. M. 2003. Perspectives on diabetic retinopathy. Am J Ophthalmol 136:122.
77. Malone, J. I., A. D. Morrison, P. R. Pavan, and D. D. Cuthbertson. 2001. Prevalence and significance of retinopathy in subjects with type 1 diabetes of less than 5 years' duration screened for the diabetes control and complications trial. Diabetes Care 24:522.
78. Kohner, E. M., I. M. Stratton, and S. J. Aldington. 1993. Prevalence of diabetic retinopathy at diagnosis of NIDDM in the UKPDS. Investigative Ophthalmology and Visual Science 34:713.
79. Kohner, E. M., I. M. Stratton, S. J. Aldington, R. R. Holman, and D. R. Matthews. 2001. Relationship between the severity of retinopathy and progression to photocoagulation in patients with Type 2 diabetes mellitus in the UKPDS (UKPDS 52). Diabet Med 18:178.
80. Fransen, S. R., T. C. Leonard-Martin, W. J. Feuer, and P. L. Hildebrand. 2002. Clinical evaluation of patients with diabetic retinopathy: accuracy of the Inoveon diabetic retinopathy-3DT system. Ophthalmology 109:595.
81. 1978. Photocoagulation treatment of proliferative diabetic retinopathy: the second report of diabetic retinopathy study findings. Ophthalmology 85:82.
82. 1979. Four risk factors for severe visual loss in diabetic retinopathy. The third report from the Diabetic Retinopathy Study. The Diabetic Retinopathy Study Research Group. Arch Ophthalmol 97:654.
83. 1981. Photocoagulation treatment of proliferative diabetic retinopathy: relationship of adverse treatment effects to retinopathy severity. Diabetic retinopathy study report no. 5. Dev Ophthalmol 2:248.
84. 1981. Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. The Diabetic Retinopathy Study Research Group. Ophthalmology 88:583.
81
85. 1991. Early photocoagulation for diabetic retinopathy. ETDRS report number 9. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98:766.
86. 1991. Effects of aspirin treatment on diabetic retinopathy. ETDRS report number 8. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98:757.
87. Bailey, C. C., J. M. Sparrow, R. H. Grey, and H. Cheng. 1998. The National Diabetic Retinopathy Laser Treatment Audit. II. Proliferative retinopathy. Eye 12 ( Pt 1):77.
88. Bailey, C. C., J. M. Sparrow, R. H. Grey, and H. Cheng. 1999. The National Diabetic Retinopathy Laser Treatment Audit. III. Clinical outcomes. Eye 13 ( Pt 2):151.
89. Cantrill, H. L. 1984. The diabetic retinopathy study and the early treatment diabetic retinopathy study. Int Ophthalmol Clin 24:13.
90. Chew, E. Y., F. L. Ferris, 3rd, K. G. Csaky, R. P. Murphy, E. Agron, D. J. Thompson, G. F. Reed, and A. P. Schachat. 2003. The long-term effects of laser photocoagulation treatment in patients with diabetic retinopathy: the early treatment diabetic retinopathy follow-up study. Ophthalmology 110:1683.
91. Davis, M. D., M. R. Fisher, R. E. Gangnon, F. Barton, L. M. Aiello, E. Y. Chew, F. L. Ferris, 3rd, and G. L. Knatterud. 1998. Risk factors for high-risk proliferative diabetic retinopathy and severe visual loss: Early Treatment Diabetic Retinopathy Study Report #18. Invest Ophthalmol Vis Sci 39:233.
92. Early Treatment Diabetic Retinopathy Study Research Group. 1991. Early photocoagulaqtion for diabetic retinopathy. ETDRS report No.9. Ophthalmology 98:110.
93. Flynn, H. W., Jr., E. Y. Chew, B. D. Simons, F. B. Barton, N. A. Remaley, and F. L. Ferris, 3rd. 1992. Pars plana vitrectomy in the Early Treatment Diabetic Retinopathy Study. ETDRS report number 17. The Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 99:1351.
94. Fine, S. L., and A. Patz. 1987. Ten years after the Diabetic Retinopathy Study. Ophthalmology 94:739.
95. Klein, R., B. E. Klein, S. E. Moss, M. D. Davis, and D. L. DeMets. 1987. The Wisconsin Epidemiologic Study of Diabetic Retinopathy. VI. Retinal photocoagulation. Ophthalmology 94:747.
82
96. Okun, E., G. P. Johnston, I. Boniuk, N. Arribas, R. F. Escoffery, and M. G. Grand. 1983. Xenon arc photocoagulation of proliferative diabetic retinopathy (a review of 2688 consecutive eyes in the format of the diabetic retinopathy study--DRS). Trans Am Ophthalmol Soc 81:229.
97. Okun, E., G. P. Johnston, I. Boniuk, N. P. Arribas, R. F. Escoffery, and M. G. Grand. 1984. Xenon arc photocoagulation of proliferative diabetic retinopathy. A review of 2688 consecutive eyes in the format of the Diabetic Retinopathy Study. Ophthalmology 91:1458.
98. Rand, L. I., G. J. Prud'homme, F. Ederer, and P. L. Canner. 1985. Factors influencing the development of visual loss in advanced diabetic retinopathy. Diabetic Retinopathy Study (DRS) Report No. 10. Invest Ophthalmol Vis Sci 26:983.
99. Vine, A. K. 1985. The efficacy of additional argon laser photocoagulation for persistent, severe proliferative diabetic retinopathy. Ophthalmology 92:1532.
100. Neubauer, A. S., U. C. Welge-Lussen, M. J. Thiel, C. Alge, S. G. Priglinger, C. Hirneiss, M. W. Ulbig, and A. Kampik. 2003. Tele-screening for diabetic retinopathy with the retinal thickness analyzer. Diabetes Care 26:2890.
101. Giovannini, A., G. Amato, C. Mariotti, and B. Scassellati-Sforzolini. 2000. Optical coherence tomography findings in diabetic macular edema before and after vitrectomy. Ophthalmic Surg Lasers 31:187.
102. Martidis, A., J. S. Duker, P. B. Greenberg, A. H. Rogers, C. A. Puliafito, E. Reichel, and C. Baumal. 2002. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology 109:920.
103. Massin, P., G. Duguid, A. Erginay, B. Haouchine, and A. Gaudric. 2003. Optical coherence tomography for evaluating diabetic macular edema before and after vitrectomy. Am J Ophthalmol 135:169.
104. Yamamoto, T., K. Hitani, I. Tsukahara, S. Yamamoto, R. Kawasaki, H. Yamashita, and S. Takeuchi. 2003. Early postoperative retinal thickness changes and complications after vitrectomy for diabetic macular edema. Am J Ophthalmol 135:14.
105. Strom, C., B. Sander, N. Larsen, M. Larsen, and H. Lund-Andersen. 2002. Diabetic macular edema assessed with
83
optical coherence tomography and stereo fundus photography. Invest Ophthalmol Vis Sci 43:241.
106. Panozzo, G., E. Gusson, B. Parolini, and A. Mercanti. 2003. Role of OCT in the diagnosis and follow up of diabetic macular edema. Semin Ophthalmol 18:74.
107. 1985. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol 103:1796.
108. 1991. Fluorescein angiographic risk factors for progression of diabetic retinopathy. ETDRS report number 13. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98:834.
109. Weinberger, D., S. Fink-Cohen, D. D. Gaton, E. Priel, and Y. Yassur. 1995. Non-retinovascular leakage in diabetic retinopathy. British Journal of Ophthalmology 79:728.
110. Stevens, T. S. 1981. Diabetic maculopathies. Int Ophthalmol Clin 21:11.
111. Sanchez-Tocino, H., A. Alvarez-Vidal, M. J. Maldonado, J. Moreno-Montanes, and A. Garcia-Layana. 2002. Retinal thickness study with optical coherence tomography in patients with diabetes. Invest Ophthalmol Vis Sci 43:1588.
112. Effectiveness, N. I. f. C. 2002. Inherited Clinical Guidelines E. Management of type 2 dibetes. Retinopathy - screening and early management. NICE, ed, London.
113. Intercollegiate Guidelines Network, S. 2001. Management of diabetes. A national clinical guideline. In SIGN Guidlenes. R. C. o. P. SIGN Executive, ed, Edinburgh.
114. Facey, K., E. Cummins, K. MAcpherson, A. Morris, L. Reay, and J. Slattery. 2002. Health Technology Assessment Report 1. Organisation of Services for diabetic retinopathy screening. H. T. B. f. Scotland., ed. Delta House, Glasgow.
115. St.Vincent Joint Task Force for Diabetes. 1994. Report of the Visual Impairment Subgroup. British Diabetic Association/Department of Health.
116. Taylor, R. 1996. Practical community screening for diabetic retinopathy using the mobile retinal camera: report of a 12 centre study. British Diabetic Association Mobile Retinal Screening Group. Diabet Med 13:946.
117. Harding, S. P., D. M. Broadbent, C. Neoh, M. C. White, and J. Vora. 1995. Sensitivity and specificity of photography and direct ophthalmoscopy in screening for sight
84
threatening eye disease: the Liverpool Diabetic Eye Study. Bmj 311:1131.
118. Owens, D. R., R. L. Gibbins, E. Kohner, G. M. Grimshaw, R. Greenwood, and S. Harding. 2000. Diabetic retinopathy screening. Diabet Med 17:493.
119. Hart, P. M., and S. Harding. 1999. Is it time for a national screening programme for sight-threatening diabetic retinopathy? Eye 13 ( Pt 2):129.
120. Garvican, L., J. Clowes, and T. Gillow. 2000. Preservation of sight in diabetes: developing a national risk reduction programme. Diabet Med 17:627.
121. Department of Health. The National Service Framework for Diabetes. T. D. o. Health, ed. RIchmond House, 79 WHitehall, London.
122. www.nscretinopathy.org.uk. 123. Rohan, T. E., C. D. Frost, and N. J. Wald. 1989. Prevention
of blindness by screening for diabetic retinopathy: a quantitative assessment. British Medical Journal 299:1198.
124. Javitt, J. C., J. K. Canner, and A. Sommer. 1989. Cost effectiveness of current approaches to the control of retinopathy in type I diabetics. Ophthalmology 96:255.
125. Dasbach, E. J., D. G. Fryback, and et.al. 1991. Cost effectiveness of strategies for detecting diabetic retinopthy. Medical Care 29:20.
126. Sculpher, M. J., M. J. Buxton, B. A. Ferguson, J. E. Humphreys, J. F. Altman, D. J. Spiegelhalter, A. J. Kirby, J. S. Jacob, H. Bacon, S. B. Dudbridge, and et al. 1991. A relative cost-effectiveness analysis of different methods of screening for diabetic retinopathy. Diabet Med 8:644.
127. Buxton, M. J., M. J. Sculphur, and B. A. Ferguson. 1991. Screening for treatable diabetic retinopathy. Diabetic Medicine 8:371.
128. James, M., D. A. Turner, D. M. Broadbent, J. Vora, and S. P. Harding. 2000. Cost effectiveness analysis of screening for sight threatening diabetic eye disease. Bmj 320:1627.
129. Wilson, J. M. G., and G. Junger. 1968. The principles and practice of screening for disease. Public Health Papers:WHO 34.
130. Gatling, W., A. J. Howie, and R. D. Hill. 1995. An optical practice based diabetic eye screening programme. Diabet Med 12:531.
85
131. Sharp, P. F., J. Olson, F. Strachan, J. Hipwell, A. Ludbrook, M. O'Donnell, S. Wallace, K. Goatman, A. Grant, N. Waugh, K. McHardy, and J. V. Forrester. 2003. The value of digital imaging in diabetic retinopathy. Health Technol Assess 7:1.
132. Cree, M. J., J. A. Olson, K. C. McHardy, P. F. Sharp, and J. V. Forrester. 1997. A fully automated comparative microaneurysm digital detection system. Eye 11 ( Pt 5):622.
133. Goatman, K. A., M. J. Cree, J. A. Olson, J. V. Forrester, and P. F. Sharp. 2003. Automated measurement of microaneurysm turnover. Invest Ophthalmol Vis Sci 44:5335.
134. Maloney, J. B. M., and M. I. Drury. 1982. The effect of pregnancy on the natural course of diabetic retinopathy. American JournaL of Ophthalmology 93:745.
135. Klein, B. E. K., S. E. Moss, and R. Klein. 1990. Effect of pregnancy on progression of diabetic retinopathy. Diabetes Care 13:34.
136. Gunduz, K., and G. B. Arden. 1989. Changes in colour contrast sensitivity associated with operating argon lasers. Br J Ophthalmol 73:241.
137. Arden, G. B., T. Berninger, C. R. Hogg, and S. Perry. 1991. A survey of color discrimination in German ophthalmologists. Changes associated with the use of lasers and operating microscopes. Ophthalmology 98:567.
138. Berninger, T. A., C. Canning, N. Strong, K. Gunduz, and G. B. Arden. 1990. [Color vision disturbance in laser operators and patients: comparison of argon and dye lasers]. Klin Monatsbl Augenheilkd 197:494.
139. Berninger, T. A., C. R. Canning, K. Gunduz, N. Strong, and G. B. Arden. 1989. Using argon laser blue light reduces ophthalmologists' color contrast sensitivity. Argon blue and surgeons' vision. Arch Ophthalmol 107:1453.
140. Smiddy, W. E., S. L. Fine, W. R. Green, and B. M. Glaser. 1984. Clinicopathologic correlation of krypton red, argon blue-green, and argon green laser photocoagulation in the human fundus. Retina 4:15.
141. Coscas, G., and G. Soubrane. 1983. The effects of red krypton and green argon laser on the foveal region. A clinical and experimental study. Ophthalmology 90:1013.
142. Marshall, J., and A. C. Bird. 1979. A comparative histopathological study of argon and krypton laser irradiations of the human retina. Br J Ophthalmol 63:657.
86
143. Vogel, M., F. P. Schafer, M. Stuke, K. Muller, S. Theuring, and A. Morawietz. 1989. Animal experiments for the determination of an optimal wavelength for retinal coagulations. Graefes Arch Clin Exp Ophthalmol 227:277.
144. Atmaca, L. S., A. Idil, and K. Gunduz. 1995. Dye laser treatment in proliferative diabetic retinopathy and maculopathy. Acta Ophthalmol Scand 73:303.
145. Ulbig, M. W., and A. M. Hamilton. 1993. [Comparative use of diode and argon laser for panretinal photocoagulation in diabetic retinopathy]. Ophthalmologe 90:457.
146. Friberg, T. R., and S. Venkatesh. 1995. Alteration of pulse configuration affects the pain response during diode laser photocoagulation. Lasers Surg Med 16:380.
147. Birngruber, R., and V. P. Gabel. 1983. Thermal versus photochemical damage in the retina--thermal calculations for exposure limits. Trans Ophthalmol Soc U K 103 ( Pt 4):422.
148. Gabel, V. P., R. Birngruber, W. Weinberg, R. McCord, and F. Hillenkamp. 1979. Comparison of temperature measurements and fundus reflectometry in laser coagulation. Mod Probl Ophthalmol 20:169.
149. Berger, J. W. 1997. Thermal modelling of micropulsed diode laser retinal photocoagulation. Lasers Surg Med 20:409.
150. Pollack, J. S., J. E. Kim, J. S. Pulido, and J. M. Burke. 1998. Tissue effects of subclinical diode laser treatment of the retina. Arch Ophthalmol 116:1633.
151. Saeed, M., D. Parmar, and D. McHugh. 2001. Frequency-doubled Nd:YAG laser for the treatment of exudative diabetic maculopathy. Eye 15:712.
152. Gupta, V., A. Gupta, R. Kaur, S. Narang, and M. R. Dogra. 2001. Efficacy of various laser wavelengths in the treatment of clinically significant macular edema in diabetics. Ophthalmic Surg Lasers 32:397.
153. Zaluski, S., G. Marcil, L. Lamer, and J. Lambert. 1986. [Study of the visual field using automated static perimetry following panretinal photocoagulation in the diabetic]. J Fr Ophtalmol 9:395.
154. Buckley, S. A., L. Jenkins, and L. Benjamin. 1992. Fields, DVLC and panretinal photocoagulation. Eye 6 ( Pt 6):623.
87
155. Pahor, D. 1998. Visual field loss after argon laser panretinal photocoagulation in diabetic retinopathy: full- versus mild-scatter coagulation. Int Ophthalmol 22:313.
156. Buckley, S., L. Jenkins, and L. Benjamin. 1992. Field loss after pan retinal photocoagulation with diode and argon lasers. Doc Ophthalmol 82:317.
157. Canning, C., P. Polkinghorne, A. Ariffin, and Z. Gregor. 1991. Panretinal laser photocoagulation for proliferative diabetic retinopathy: the effect of laser wavelength on macular function. Br J Ophthalmol 75:608.
158. Patel, J. I., L. Jenkins, L. Benjamin, and S. Webber. 2002. Dilated pupils and loss of accommodation following diode panretinal photocoagulation with sub-tenon local anaesthetic in four cases. Eye 16:628.
159. McDonald, H. R., and H. Schatz. 1985. Macular edema following panretinal photocoagulation. Retina 5:5.
160. McDonald, H. R., and H. Schatz. 1985. Visual loss following panretinal photocoagulation for proliferative diabetic retinopathy. Ophthalmology 92:388.
161. Francois, J., and E. Cambie. 1976. Further vision deterioration after argon laser photocoagulation in diabetic retinopathy. Ophthalmologica 173:28.
162. Meyers, S. M. 1980. Macular edema after scatter laser photocoagulation for proliferative diabetic retinopathy. Am J Ophthalmol 90:210.
163. Huamonte, F. U., G. A. Peyman, M. F. Goldberg, and A. Locketz. 1976. Immediate fundus complications after retinal scatter photocoagulation. I. Clinical picture and pathogenesis. Ophthalmic Surg 7:88.
164. British Multicentre Study Group. 1983. Photocoagulation for diabetic maculopathy. Diabetes 32:1010.
165. Early Treatment Diabetic Retinopathy Study Research Group. 1985. Photocoagulation for diabetic macular oedema. Archives of Ophthalmology 103:1796.
166. Blankenship, G. W. 1979. Diabetic macular edema and argon laser photocoagulation: a prospective randomised study. Ophthalmology 86:69.
167. 1995. Focal photocoagulation treatment of diabetic macular edema. Relationship of treatment effect to fluorescein angiographic and other retinal characteristics at baseline: ETDRS report no. 19. Early Treatment Diabetic
88
Retinopathy Study Research Group. Arch Ophthalmol 113:1144.
168. Olk, R. J. 1986. Modified grid argon (blue-green) laser photocoagulation for diffuse diabetic macular edema. Ophthalmology 93:938.
169. 1993. Hypertension in Diabetes Study (HDS): I. Prevalence of hypertension in newly presenting type 2 diabetic patients and the association with risk factors for cardiovascular and diabetic complications. J Hypertens 11:309.
170. 1998. Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. UK Prospective Diabetes Study Group. Bmj 317:713.
171. Colwell, J. A. 1996. Intensive insulin therapy in type II diabetes: rationale and collaborative clinical trial results. Diabetes 45 Suppl 3:S87.
172. Kohner, E. M., I. M. Stratton, S. J. Aldington, R. C. Turner, and D. R. Matthews. 1999. Microaneurysms in the development of diabetic retinopathy (UKPDS 42). UK Prospective Diabetes Study Group. Diabetologia 42:1107.
173. Strain, W. D., and N. Chaturvedi. 2002. The renin-angiotensin-aldosterone system and the eye in diabetes. J Renin Angiotensin Aldosterone Syst 3:243.
174. 1986. The Diabetes Control and Complications Trial (DCCT). Design and methodologic considerations for the feasibility phase. The DCCT Research Group. Diabetes 35:530.
175. 1987. Diabetes Control and Complications Trial (DCCT): results of feasibility study. The DCCT Research Group. Diabetes Care 10:1.
176. Boulton, A. J. 1993. DCCT: implications for diabetes care in the UK. Diabet Med 10:687.
177. Keen, H. 1994. The Diabetes Control and Complications Trial (DCCT). Health Trends 26:41.
178. Klein, R. 1995. Hyperglycemia and microvascular and macrovascular disease in diabetes. Diabetes Care 18:258.
179. Peterson, K. A., and C. K. Smith. 1995. The DCCT findings and standards of care for diabetes. Am Fam Physician 52:1092.
180. 1998. Early worsening of diabetic retinopathy in the Diabetes Control and Complications Trial. Arch Ophthalmol 116:874.
89
181. 2000. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. N Engl J Med 342:381.
182. Zhang, L., G. Krzentowski, A. Albert, and P. J. Lefebvre. 2001. Risk of developing retinopathy in Diabetes Control and Complications Trial type 1 diabetic patients with good or poor metabolic control. Diabetes Care 24:1275.
183. Roth, D. B., J. Chieh, M. J. Spirn, S. N. Green, D. L. Yarian, and N. A. Chaudhry. 2003. Noninfectious endophthalmitis associated with intravitreal triamcinolone injection. Arch Ophthalmol 121:1279.
184. Jonas, J. B., I. Kreissig, A. Sofker, and R. F. Degenring. 2003. Intravitreal injection of triamcinolone for diffuse diabetic macular edema. Arch Ophthalmol 121:57.
185. Jonas, J. B., and R. Degenring. 2002. [Intravitreal injection of crystalline triamcinolone acetonide in the treatment of diffuse diabetic macular oedema]. Klin Monatsbl Augenheilkd 219:429.
186. Jonas, J. B., and A. Sofker. 2001. Intraocular injection of crystalline cortisone as adjunctive treatment of diabetic macular edema. Am J Ophthalmol 132:425.
187. Beer, P. M., S. J. Bakri, R. J. Singh, W. Liu, G. B. Peters, 3rd, and M. Miller. 2003. Intraocular concentration and pharmacokinetics of triamcinolone acetonide after a single intravitreal injection. Ophthalmology 110:681.
188. Goa, K. L., M. Haria, and M. I. Wilde. 1997. Lisinopril. A review of its pharmacology and use in the management of the complications of diabetes mellitus. Drugs 53:1081.
189. Sjolie, A. K., and N. Chaturvedi. 2002. The retinal renin-angiotensin system: implications for therapy in diabetic retinopathy. J Hum Hypertens 16 Suppl 3:S42.
190. Frank, R. N. 2002. Potential new medical therapies for diabetic retinopathy: protein kinase C inhibitors. Am J Ophthalmol 133:693.
191. Lewis, H., G. W. Abrams, M. S. Blumenkranz, and P. V. Campochiaro. 1991. Resolution of diabetic macular oedema associated with a thickened and taut posterior hyaloid after vitrectomy (abstr). Ophthalmology 98 (suppl):146.
192. Tachi, N. 1998. Surgical management of macular edema. Semin Ophthalmol 13:20.
90
193. Otani, T., and S. Kishi. 2002. A controlled study of vitrectomy for diabetic macular edema. Am J Ophthalmol 134:214.
194. La Heij, E. C., F. Hendrikse, A. G. Kessels, and P. J. Derhaag. 2001. Vitrectomy results in diabetic macular oedema without evident vitreomacular traction. Graefes Arch Clin Exp Ophthalmol 239:264.
195. Chantelau, E. 2001. What may be gained from standard photocoagulation during early worsening of diabetic retinopathy? An observational study in type-1 diabetic patients after tightening of glycaemic control. Diabetes Metab 27:366.
196. Klein, R., S. E. Moss, B. E. Klein, P. Gutierrez, and C. M. Mangione. 2001. The NEI-VFQ-25 in people with long-term type 1 diabetes mellitus: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Arch Ophthalmol 119:733.
197. 1991. Classification of diabetic retinopathy from fluorescein angiograms. ETDRS report number 11. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98:807.
198. 1991. Early Treatment Diabetic Retinopathy Study design and baseline patient characteristics. ETDRS report number 7. Ophthalmology 98:741.
199. Kinyoun, J., F. Barton, M. Fisher, L. Hubbard, L. Aiello, and F. Ferris, 3rd. 1989. Detection of diabetic macular edema. Ophthalmoscopy versus photography--Early Treatment Diabetic Retinopathy Study Report Number 5. The ETDRS Research Group. Ophthalmology 96:746.
200. Folk, J. C., C. F. Blodi, and J. S. Pulido. 1990. Diabetic retinopathy. Iowa Med 80:525.
201. Bamroongsuk, P., Q. Yi, C. A. Harper, and D. McCarty. 2002. Delivery of photocoagulation treatment for diabetic retinopathy at a large Australian ophthalmic hospital: comparisons with national clinical practice guidelines. Clin Experiment Ophthalmol 30:115.
202. British Multicentre Study Group. 1984. Photocoagulation for proliferative diabetic retinopathy: a randomised controlled trial using the xenon arc. Diabetologia 26:109.
203. Early Treatment Diabetic Retinopathy Study Research Group. 1991. Fundus photographic risk factors for the progression of diabetic retinopahty. Report No.12. Ophthalmology 98:823.
91
204. Ferris, F. L., 3rd. 1996. Early photocoagulation in patients with Type I or II diabetes. Transactions of the American Academy of Ophthalmology 94:505.
205. Patz, A., and R. E. Smith. 1991. The ETDRS and Diabetes 2000. Ophthalmology 98:739.
206. The Diabetic Retinopathy Study Research Group. 1978. Photocoagulation treatment of proliferative diabetic retinopathy. Ophthalmology 85:82.
207. Murphy, R. P., and P. R. Egbert. 1979. Regression of iris neovascularization following panretinal photocoagulation. Arch Ophthalmol 97:700.
208. 1988. Early vitrectomy for severe proliferative diabetic retinopathy in eyes with useful vision. Results of a randomized trial--Diabetic Retinopathy Vitrectomy Study Report 3. The Diabetic Retinopathy Vitrectomy Study Research Group. Ophthalmology 95:1307.
209. Wand, M. 1989. Neovascular glaucomas. C.V. Mosby, St. Louis, Mo.
210. Palmer, S. 1991. Mitomycin as an adjunct chemotherapy with trabeculectomy. Ophthalmology 98:317.
211. Kitazwa, Y., K. Kawaze, H. Matsushita, and M. Minobe. 1991. Trabeculectomy with mitomycin-a comparative study with fluorouracil. Archives of Ophthalmology 109:1693.
212. Arun, C. S., N. Ngugi, L. Lovelock, and R. Taylor. 2003. Effectiveness of screening in preventing blindness due to diabetic retinopathy. Diabet Med 20:186.
213. Diabetic Retinopathy Study Research Group. 1976. Preliminary report on the effects of photocoagulation therapy. American Journal of Ophthalmology 81:383.
214. Hercules, B. L., Gayed, II, S. B. Lucas, and J. Jeacock. 1977. Peripheral retinal ablation in the treatment of proliferative diabetic retinopathy: a three-year interim report of a randomised, controlled study using the argon laser. Br J Ophthalmol 61:555.
215. Murphy, R. P., and P. R. Egbert. 1979. Regression of iris neovascularisation following panretinal photocoagulation. Archives of Ophthalmology 97:700.
216. 1991. Fundus photographic risk factors for progression of diabetic retinopathy. ETDRS report number 12. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98:823.
92
217. 1992. Aspirin effects on mortality and morbidity in patients with diabetes mellitus. Early Treatment Diabetic Retinopathy Study report 14. ETDRS Investigators. Jama 268:1292.
218. Chaturvedi, N., A. K. Sjoelie, M. Porta, S. J. Aldington, J. H. Fuller, M. Songini, and E. M. Kohner. 2001. Markers of insulin resistance are strong risk factors for retinopathy incidence in type 1 diabetes. Diabetes Care 24:284.
219. Chew, E. Y., M. L. Klein, F. L. Ferris, 3rd, N. A. Remaley, R. P. Murphy, K. Chantry, B. J. Hoogwerf, and D. Miller. 1996. Association of elevated serum lipid levels with retinal hard exudate in diabetic retinopathy. Early Treatment Diabetic Retinopathy Study (ETDRS) Report 22. Arch Ophthalmol 114:1079.
220. Chowdhury, T. A., D. Hopkins, P. M. Dodson, and G. C. Vafidis. 2002. The role of serum lipids in exudative diabetic maculopathy: is there a place for lipid lowering therapy? Eye 16:689.
221. Cunha-Vaz, J. 1998. Lowering the risk of visual impairment and blindness. Diabet Med 15 Suppl 4:S47.
222. Fuller, J. H., L. K. Stevens, and S. L. Wang. 2001. Risk factors for cardiovascular mortality and morbidity: the WHO Mutinational Study of Vascular Disease in Diabetes. Diabetologia 44 Suppl 2:S54.
223. Funderburk, R. L. 1989. Diabetes as a risk factor for retinal neovascularisation. Annals d'Opthalmologie 21:65.
224. Home, P. D. 2002. Therapeutic targets in the management of Type 1 diabetes. Diabetes Metab Res Rev 18 Suppl 1:S7.
225. Klein, R., B. E. K. Klein, and S. E. Moss. 1984. The Wisconsin epidemiologic study: II Prevalence and risk of diabetic retinopathy when age at diagnosis is less than thirty years. Archives of Ophthalmology 102:520.
226. Klein, R., B. E. K. Klein, and S. E. Moss. 1984. The Wisconsin epidemiologic study: II Prevalence and risk of diabetic retinopathy when age at diagnosis is thirty or more years. Archives of Ophthalmology 102:527.
227. Porta, M., A. K. Sjoelie, N. Chaturvedi, L. Stevens, R. Rottiers, M. Veglio, and J. H. Fuller. 2001. Risk factors for progression to proliferative diabetic retinopathy in the EURODIAB Prospective Complications Study. Diabetologia 44:2203.
93
228. Rand, L. I., A. S. Krolewski, and L. M. Aiello. 1985. Multiple factors in the prediction of risk of proliferative diabetic retinopathy. New England Journal of Medecine 313:1433.
229. Sen, K., A. Misra, A. Kumar, and R. M. Pandey. 2002. Simvastatin retards progression of retinopathy in diabetic patients with hypercholesterolemia. Diabetes Res Clin Pract 56:1.
230. Stephenson, J. M., J. H. Fuller, G. C. Viberti, A. K. Sjolie, and R. Navalesi. 1995. Blood pressure, retinopathy and urinary albumin excretion in IDDM: the EURODIAB IDDM Complications Study. Diabetologia 38:599.
231. Tapp, R. J., J. E. Shaw, C. A. Harper, M. P. de Courten, B. Balkau, D. J. McCarty, H. R. Taylor, T. A. Welborn, and P. Z. Zimmet. 2003. The prevalence of and factors associated with diabetic retinopathy in the Australian population. Diabetes Care 26:1731.
232. Vijan, S., T. P. Hofer, and R. A. Hayward. 1997. Estimated benefits of glycemic control in microvascular complications in type 2 diabetes. Ann Intern Med 127:788.
233. Wallberg-Henriksson, H., J. Rincon, and J. R. Zierath. 1998. Exercise in the management of non-insulin-dependent diabetes mellitus. Sports Med 25:25.
234. Diabetic Retinopathy Vitrectomy Study Research Group. 1985. Early vitrectomy for severe vitreous haemorrhage in diabetic retinopathy. Two year results of a randomised trial. DRVS report No2. Archives of Ophthalmology 103:1644.
235. Diabetic Retinopathy Vitrectomy Study Research Group. 1990. Early vitrectomy for sever vitreous haemorrhage in diabetic retinopathy. Four year results of a randomised trial. DRVS report No5. Archives of Ophthalmology 108:958.
236. Thompson, J. T., S. de Buistros, B. M. Glaser, and R. G. Michels. 1986. Results of vitrectomy for proliferative diabetic retinopathy. Ophthalmology 93:1571.
237. Smiddy, W. E., and H. W. Flynn, Jr. 1999. Vitrectomy in the management of diabetic retinopathy. Surv Ophthalmol 43:491.
238. Kroll, P., and H. Busse. 1986. [Therapy of preretinal macular hemorrhages]. Klin Monatsbl Augenheilkd 188:610.
239. Ulbig, M. W., G. Mangouritsas, H. H. Rothbacher, A. M. Hamilton, and J. D. McHugh. 1998. Long-term results after drainage of premacular subhyaloid hemorrhage into the
94
vitreous with a pulsed Nd:YAG laser. Arch Ophthalmol 116:1465.
240. Rennie, C. A., D. K. Newman, M. P. Snead, and D. W. Flanagan. 2001. Nd:YAG laser treatment for premacular subhyaloid haemorrhage. Eye 15:519.
241. Raymond, L. A. 1995. Neodymium:YAG laser treatment for hemorrhages under the internal limiting membrane and posterior hyaloid face in the macula. Ophthalmology 102:406.
242. Isaacs, T. W., C. Barry, and I. L. McAllister. 1996. Early resolution of premacular haemorrhage following Nd:YAG laser photodisruption of posterior hyaloid. Aust N Z J Ophthalmol 24:365.
243. Celebi, S., and A. S. Kukner. 2001. Photodisruptive Nd:YAG laser in the management of premacular subhyaloid hemorrhage. Eur J Ophthalmol 11:281.
244. Gabel, V.-P., R. Birngruber, H. Gunther-koszka, and C. A. Puliafito. 1989. Nd:YAG laser photodisruption of haemorrgaic detachment of the internal limiting membrane. American Journal of Ophthalmology 107:33.
245. Chung, J., M. H. Kim, S. M. Chung, and K. Y. Chang. 2001. The effect of tissue plasminogen activator on premacular hemorrhage. Ophthalmic Surg Lasers 32:7.
246. Campbell, D. G., R. J. Simmons, F. I. Tolentino, and J. W. McMeel. 1977. Glaucoma occurring after closed vitrectomy. Am J Ophthalmol 83:63.
247. Thompson, J. T., S. de Buistros, R. G. Michels, and T. A. Rice. 1987. Results and prognostic factors for diabetic traction retinal detachment of the macula. Archives of Ophthalmology 105:497.
248. Rice, T. A., R. G. Michels, and E. F. Rice. 1983. Vitrectomy for diabetic traction retinal detachment involving the macula. American Journal of Ophthalmology 95:22.
249. Lewis, H., G. W. Abrams, and G. A. Williams. 1987. Anterior hyaloidal fibrovascular proliferation after diabetic vitrectomy. American Journal of Ophthalmology 104:607.
250. Ulbig, M., and A. M. Hamilton. 1994. Anterior hyaloidal fibrovascular proliferation. Current Opinion in Ophthalmology 5:54.
251. Takagi, H., A. Otani, J. Kiryu, and Y. Ogura. 1999. New surgical approach for removing massive foveal hard
95
exudates in diabetic macular edema. Ophthalmology 106:249.
252. Gandorfer, A., E. M. Messmer, M. W. Ulbig, and A. Kampik. 2000. Resolution of diabetic macular edema after surgical removal of the posterior hyaloid and the inner limiting membrane. Retina 20:126.
253. Wilkinson, C. P. 2000. Vitrectomy for chronic pseudophakic cystoid macular edema. Am J Ophthalmol 129:560.
254. Garcia-Arumi, J., V. Martinez, L. Sararols, and B. Corcostegui. 2003. Vitreoretinal surgery for cystoid macular edema associated with retinitis pigmentosa. Ophthalmology 110:1164.
255. Massin, P., A. Erginay, B. Haouchine, A. B. Mehidi, M. Paques, and A. Gaudric. 2002. Retinal thickness in healthy and diabetic subjects measured using optical coherence tomography mapping software. Eur J Ophthalmol 12:102.
256. Yamamoto, T., N. Akabane, and S. Takeuchi. 2001. Vitrectomy for diabetic macular edema: the role of posterior vitreous detachment and epimacular membrane. Am J Ophthalmol 132:369.
257. Otani, T., and S. Kishi. 2000. Tomographic assessment of vitreous surgery for diabetic macular edema. Am J Ophthalmol 129:487.
258. Kadonosono, K., N. Itoh, and S. Ohno. 2000. Perifoveal microcirculation before and after vitrectomy for diabetic cystoid macular edema. Am J Ophthalmol 130:740.
259. Sato, Y., Z. Lee, and H. Shimada. 2001. [Vitrectomy for diabetic cystoid macular edema]. Nippon Ganka Gakkai Zasshi 105:251.
260. Amino, K., and H. Tanihara. 2002. Vitrectomy combined with phacoemulsification and intraocular lens implantation for diabetic macular edema. Jpn J Ophthalmol 46:455.
261. Pendergast, S. D., T. S. Hassan, G. A. Williams, M. S. Cox, R. R. Margherio, P. J. Ferrone, B. R. Garretson, and M. T. Trese. 2000. Vitrectomy for diffuse diabetic macular edema associated with a taut premacular posterior hyaloid. Am J Ophthalmol 130:178.
262. Nakamura, S., N. Ogino, K. Kumagai, M. Furukawa, K. Atsumi, S. Demizu, H. Kurihara, H. Ishigooka, M. Iwaki, and S. Nishigaki. 2003. [The influence of hard exudates on the results of vitrectomy for macular edema due to diabetic retinopathy]. Nippon Ganka Gakkai Zasshi 107:519.
96
263. Klein, B. E., R. Klein, and S. E. Moss. 1995. Incidence of cataract surgery in the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Am J Ophthalmol 119:295.
264. Rajendram, R., J. A. Deane, M. Barnes, P. G. Swift, K. Adamson, S. Pearce, and G. Woodruff. 2003. Rapid onset childhood cataracts leading to the diagnosis of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. Am J Ophthalmol 136:951.
265. Edwards, M. G., A. P. Schachat, S. B. Bressler, and N. M. Bressler. 1994. Outcome of cataract operations performed to permit diagnosis, to determine eligibility for laser therapy, or to perform laser therapy of retinal disorders. Am J Ophthalmol 118:440.
266. Kruger, A. J., J. Schauersberger, V. Petternel, and M. Amon. 1999. Inflammation after phacoemulsification in patients with type 2 diabetes mellitus without retinopathy: prospective study. J Cataract Refract Surg 25:227.
267. Krepler, K., E. Ries, A. Derbolav, J. Nepp, and A. Wedrich. 2001. Inflammation after phacoemulsification in diabetic retinopathy. Foldable acrylic versus heparin-surface-modified poly(methyl methacrylate) intraocular lenses. J Cataract Refract Surg 27:233.
268. Lee do, H., Y. Seo, and C. K. Joo. 2002. Progressive opacification of hydrophilic acrylic intraocular lenses in diabetic patients. J Cataract Refract Surg 28:1271.
269. Pandey, S. K., L. Werner, D. J. Apple, and M. Kaskaloglu. 2002. Hydrophilic acrylic intraocular lens optic and haptics opacification in a diabetic patient: bilateral case report and clinicopathologic correlation. Ophthalmology 109:2042.
270. Kleinmann, G., P. Hoffman, E. Schechtman, and A. Pollack. 2002. Microscope-induced retinal phototoxicity in cataract surgery of short duration. Ophthalmology 109:334.
271. Hayashi, H., K. Hayashi, F. Nakao, and F. Hayashi. 1998. Area reduction in the anterior capsule opening in eyes of diabetes mellitus patients. J Cataract Refract Surg 24:1105.
272. Kato, S., T. Oshika, J. Numaga, Y. Hayashi, M. Oshiro, T. Yuguchi, and T. Kaiya. 2001. Anterior capsular contraction after cataract surgery in eyes of diabetic patients. Br J Ophthalmol 85:21.
273. Helbig, H., U. Kellner, N. Bornfeld, and M. H. Foerster. 1996. Cataract surgery and YAG-laser capsulotomy
97
following vitrectomy for diabetic retinopathy. Ger J Ophthalmol 5:408.
274. Dahlhauser, K. F., K. J. Wroblewski, and T. H. Mader. 1998. Anterior capsule contraction with foldable silicone intraocular lenses. J Cataract Refract Surg 24:1216.
275. Cochener, B., P. L. Jacq, and J. Colin. 1999. Capsule contraction after continuous curvilinear capsulorhexis: poly(methyl methacrylate) versus silicone intraocular lenses. J Cataract Refract Surg 25:1362.
276. Park, T. K., S. K. Chung, and N. H. Baek. 2002. Changes in the area of the anterior capsule opening after intraocular lens implantation. J Cataract Refract Surg 28:1613.
277. Subramaniam, S., and S. J. Tuft. 2001. Early decentration of plate-haptic silicone intraocular lenses. J Cataract Refract Surg 27:330.
278. Ionides, A., J. G. Dowler, P. G. Hykin, P. H. Rosen, and A. M. Hamilton. 1994. Posterior capsule opacification following diabetic extracapsular cataract extraction. Eye 8 ( Pt 5):535.
279. Jones, N. P., D. McLeod, and M. E. Boulton. 1995. Massive proliferation of lens epithelial remnants after Nd-YAG laser capsulotomy. Br J Ophthalmol 79:261.
280. Pollack, A., H. Katz, M. Oliver, and M. Zalish. 1996. The course after cataract extraction, intraocular lens implantation, and trabeculectomy for patients with diabetes. Ophthalmic Surg Lasers 27:595.
281. Huyghe, P., and J. Libert. 1994. Extracapsular lens extraction with posterior chamber lens implantation and vitrectomy for diabetic proliferative retinopathy in one operation. Bull Soc Belge Ophtalmol 254:49.
282. Jun, Z., S. Pavlovic, and K. W. Jacobi. 2001. Results of combined vitreoretinal surgery and phacoemulsification with intraocular lens implantation. Clin Experiment Ophthalmol 29:307.
283. Honjo, M., and Y. Ogura. 1998. Surgical results of pars plana vitrectomy combined with phacoemulsification and intraocular lens implantation for complications of proliferative diabetic retinopathy. Ophthalmic Surg Lasers 29:99.
284. Demetriades, A. M., J. D. Gottsch, R. Thomsen, A. Azab, W. J. Stark, P. A. Campochiaro, E. de Juan, Jr., and J. A. Haller. 2003. Combined phacoemulsification, intraocular
98
lens implantation, and vitrectomy for eyes with coexisting cataract and vitreoretinal pathology. Am J Ophthalmol 135:291.
285. Shinoda, K., A. O'Hira, S. Ishida, M. Hoshide, L. S. Ogawa, Y. Ozawa, K. Nagasaki, M. Inoue, and H. Katsura. 2001. Posterior synechia of the iris after combined pars plana vitrectomy, phacoemulsification, and intraocular lens implantation. Jpn J Ophthalmol 45:276.
286. Sadiq, S. A., A. Chatterjee, and S. A. Vernon. 1995. Progression of diabetic retinopathy and rubeotic glaucoma following cataract surgery. Eye 9 ( Pt 6):728.
287. West, J. A., J. G. Dowler, A. M. Hamilton, S. R. Boyd, and P. G. Hykin. 1999. Panretinal photocoagulation during cataract extraction in eyes with active proliferative diabetic eye disease. Eye 13 ( Pt 2):170.
288. Kuchle, M., A. Handel, and G. O. Naumann. 1998. Cataract extraction in eyes with diabetic iris neovascularization. Ophthalmic Surg Lasers 29:28.
289. Dowler, J. G., P. G. Hykin, S. L. Lightman, and A. M. Hamilton. 1995. Visual acuity following extracapsular cataract extraction in diabetes: a meta-analysis. Eye 9 ( Pt 3):313.
290. Somaiya, M. D., J. D. Burns, R. Mintz, R. E. Warren, T. Uchida, and B. F. Godley. 2002. Factors affecting visual outcomes after small-incision phacoemulsification in diabetic patients. J Cataract Refract Surg 28:1364.
291. Dowler, J. G., K. S. Sehmi, P. G. Hykin, and A. M. Hamilton. 1999. The natural history of macular edema after cataract surgery in diabetes. Ophthalmology 106:663.
292. Flesner, P., B. Sander, V. Henning, H. H. Parving, M. Dornonville de la Cour, and H. Lund-Andersen. 2002. Cataract surgery on diabetic patients. A prospective evaluation of risk factors and complications. Acta Ophthalmol Scand 80:19.
293. Chew, E. Y., W. E. Benson, N. A. Remaley, A. A. Lindley, T. C. Burton, K. Csaky, G. A. Williams, and F. L. Ferris, 3rd. 1999. Results after lens extraction in patients with diabetic retinopathy: early treatment diabetic retinopathy study report number 25. Arch Ophthalmol 117:1600.
294. Gupta, A., and V. Gupta. 2001. Diabetic maculopathy and cataract surgery. Ophthalmol Clin North Am 14:625.
99
295. Funatsu, H., H. Yamashita, H. Noma, E. Shimizu, T. Mimura, and S. Hori. 2002. Prediction of macular edema exacerbation after phacoemulsification in patients with nonproliferative diabetic retinopathy. J Cataract Refract Surg 28:1355.
296. Funatsu, H., H. Yamashita, H. Noma, T. Mimura, T. Yamashita, and S. Hori. 2002. Increased levels of vascular endothelial growth factor and interleukin-6 in the aqueous humor of diabetics with macular edema. Am J Ophthalmol 133:70.
297. Jaffe, G. J. 1993. Cataract extraction in the diabetic patient. Semin Ophthalmol 8:79.
298. Coyle, J. T. 1993. Progression of nonproliferative diabetic retinopathy and visual outcome after extracapsular cataract extraction and intraocular lens implantation. Am J Ophthalmol 115:824.
299. Schatz, H., D. Atienza, H. R. McDonald, and R. N. Johnson. 1994. Severe diabetic retinopathy after cataract surgery. Am J Ophthalmol 117:314.
300. Chiu, D. W., R. A. Meusemann, D. V. Kaufman, A. J. Hall, and M. D. Daniell. 1998. Visual outcome and progression of retinopathy after cataract surgery in diabetic patients. Aust N Z J Ophthalmol 26:129.
301. Kato, S., Y. Fukada, S. Hori, Y. Tanaka, and T. Oshika. 1999. Influence of phacoemulsification and intraocular lens implantation on the course of diabetic retinopathy. J Cataract Refract Surg 25:788.
302. Mittra, R. A., J. L. Borrillo, S. Dev, W. F. Mieler, and S. B. Koenig. 2000. Retinopathy progression and visual outcomes after phacoemulsification in patients with diabetes mellitus. Arch Ophthalmol 118:912.
303. Chung, J., M. Y. Kim, H. S. Kim, J. S. Yoo, and Y. C. Lee. 2002. Effect of cataract surgery on the progression of diabetic retinopathy. J Cataract Refract Surg 28:626.
304. Krepler, K., R. Biowski, S. Schrey, K. Jandrasits, and A. Wedrich. 2002. Cataract surgery in patients with diabetic retinopathy: visual outcome, progression of diabetic retinopathy, and incidence of diabetic macular oedema. Graefes Arch Clin Exp Ophthalmol 240:735.
305. Borrillo, J. L., R. A. Mittra, S. Dev, W. F. Mieler, S. Pescinski, A. Prasad, P. K. Rao, and S. B. Koenig. 1999. Retinopathy progression and visual outcomes after
100
phacoemulsification in patients with diabetes mellitus. Trans Am Ophthalmol Soc 97:435.
306. Schrey, S., K. Krepler, R. Biowski, and A. Wedrich. 2002. Midterm visual outcome and progression of diabetic retinopathy following cataract surgery. Midterm outcome of cataract surgery in diabetes. Ophthalmologica 216:337.
101
APPENDIX Grading Protocols for Diabetic Retinopathy 1. ETDRS Grading based on original Airlie House Classification The ETDRS grading protocol is based on fundus photographs of seven overlapping fields of view of the fundus which grade various aspects of retinopathy against a set of standard photographs. Field 1 is centred on the macula and field 2 is centred on the optic disc. Fields 3-8 two above, two below and on enasal to the discsuroound fields 1 and 2. The seven fields of view are centred around the disc and macula. Features graded in fileds 2-8 include haemorrhages and/or microaneurysms, hard exudates, cotton wool spots, venous calibre abnormalities, venous sheathing, perivenous exudates, arteriolar abnormalities, intraretinal microvascular abnormalities, arteriovenous nicking, NVE, fibrous proliferation, retinal elevation, preretinal haemorrhages, and vitreous haemorrhage. Features graded in field 1 only include NV, features graded in field 2 only include posterior vitreous detachment, macular oedema. Grading is based on a general protocol for each feature as follows: Grade 0 Grade 1a questionable presence Grade 1b definite presence but less than a specified size Grade 2a greater than a specified size but less than standard photo Grade 2b greater area than standard photo In this way, grades of retinopathy are determined by the cumulative severity of each of the features and an overall grading score applied as per the Table below. Table. ETDRS grading system for severity of retinopathy
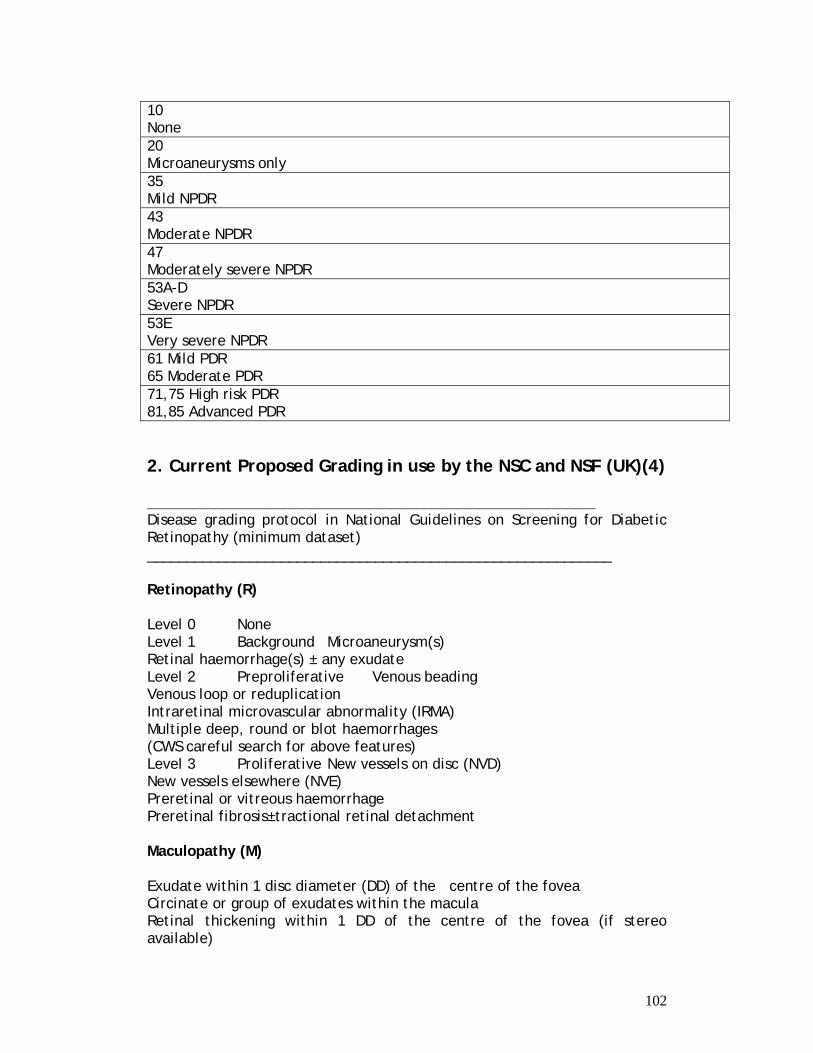
102
2. Current Proposed Grading in use by the NSC and NSF (UK)(4) ___________________________________________________ Disease grading protocol in National Guidelines on Screening for Diabetic Retinopathy (minimum dataset) ___________________________________________________________ Retinopathy (R) Level 0 None Level 1 Background Microaneurysm(s) Retinal haemorrhage(s) ± any exudate Level 2 Preproliferative Venous beading Venous loop or reduplication Intraretinal microvascular abnormality (IRMA) Multiple deep, round or blot haemorrhages (CWS careful search for above features) Level 3 Proliferative New vessels on disc (NVD) New vessels elsewhere (NVE) Preretinal or vitreous haemorrhage Preretinal fibrosis±tractional retinal detachment Maculopathy (M) Exudate within 1 disc diameter (DD) of the centre of the fovea Circinate or group of exudates within the macula Retinal thickening within 1 DD of the centre of the fovea (if stereo available)
10 None 20 Microaneurysms only 35 Mild NPDR 43 Moderate NPDR 47 Moderately severe NPDR 53A-D Severe NPDR 53E Very severe NPDR 61 Mild PDR 65 Moderate PDR 71,75 High risk PDR 81,85 Advanced PDR
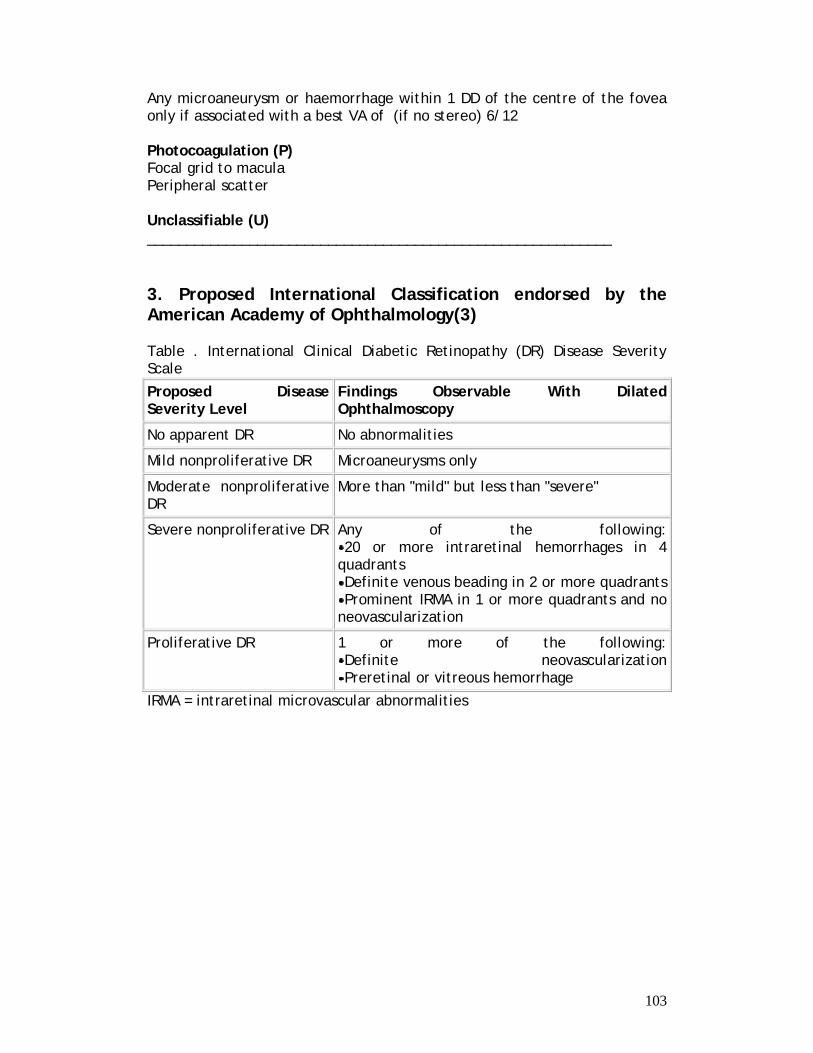
103
Any microaneurysm or haemorrhage within 1 DD of the centre of the fovea only if associated with a best VA of (if no stereo) 6/12 Photocoagulation (P) Focal grid to macula Peripheral scatter Unclassifiable (U) ___________________________________________________________ 3. Proposed International Classification endorsed by the American Academy of Ophthalmology(3) Table . International Clinical Diabetic Retinopathy (DR) Disease Severity Scale
Proposed Disease Severity Level
Findings Observable With Dilated Ophthalmoscopy
No apparent DR No abnormalities
Mild nonproliferative DR Microaneurysms only
Moderate nonproliferative DR
More than "mild" but less than "severe"
Severe nonproliferative DR Any of the following: 20 or more intraretinal hemorrhages in 4
quadrants Definite venous beading in 2 or more quadrants Prominent IRMA in 1 or more quadrants and no
neovascularization
Proliferative DR 1 or more of the following: Definite neovascularization Preretinal or vitreous hemorrhage
IRMA = intraretinal microvascular abnormalities
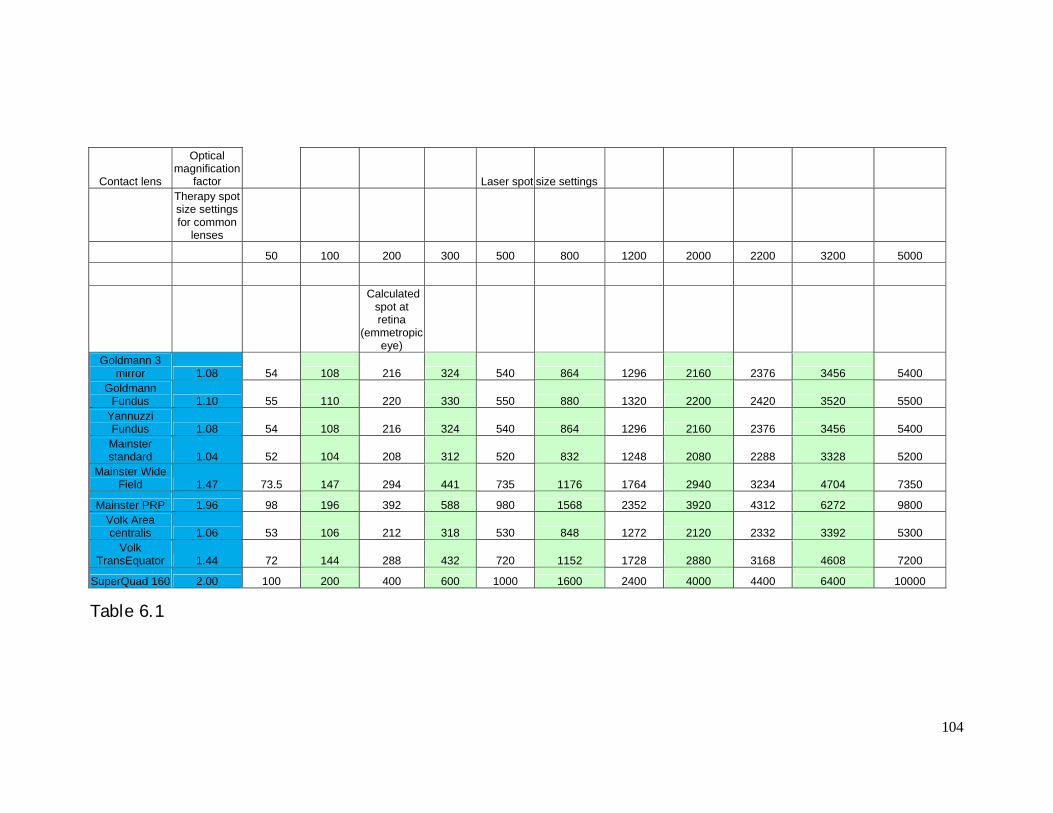
104
Contact lens
Optical magnification
factor Laser spot size settings
Therapy spot size settings for common
lenses
50 100 200 300 500 800 1200 2000 2200 3200 5000
Calculated spot at retina
(emmetropic eye)
Goldmann 3 mirror 1.08 54 108 216 324 540 864 1296 2160 2376 3456 5400
Goldmann Fundus 1.10 55 110 220 330 550 880 1320 2200 2420 3520 5500
Yannuzzi Fundus 1.08 54 108 216 324 540 864 1296 2160 2376 3456 5400 Mainster standard 1.04 52 104 208 312 520 832 1248 2080 2288 3328 5200
Mainster Wide Field 1.47 73.5 147 294 441 735 1176 1764 2940 3234 4704 7350
Mainster PRP 1.96 98 196 392 588 980 1568 2352 3920 4312 6272 9800 Volk Area centralis 1.06 53 106 212 318 530 848 1272 2120 2332 3392 5300
Volk TransEquator 1.44 72 144 288 432 720 1152 1728 2880 3168 4608 7200
SuperQuad 160 2.00 100 200 400 600 1000 1600 2400 4000 4400 6400 10000
Table 6.1






![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://img.pdfslide.us/doc/110x75/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)