Embed Size (px)
Citation preview

I?HARMACOI~NETICS AND DRUG DISPOSITION
Grapefruit juice-terfenadine single-dose interaction: Magnitude, mechanism, and relevance
Objective: To investigate the single dose-response effects of grapefruit juice on terfenadine disposition and electrocardiographic measurements. Methods: Twelve healthy males received 250 ml water or regular- or double-strength grapefruit juice with 60 mg terfenadine in a randomized crossover trial. Plasma concentrations of the cardiotoxic agent ter- fenadine and the active ant&&mink metabolite terfenadine carboxylate were deternked over 8 hours. The QT, interval was monitored. Re&ts:Terfenadine concentrations were measurable ( > 1 rig/ml) in 27 (20%; p < 0.001) and 39 (30%; p < 0.001) samples from mdividuals treated with regular- and double-strength grapefruit juice, respectively, compared to only four (3%) samples with water. Terfenadine plasma peak drug concentration (C,) was also higher. Terfenadine carboxylate area under the plasma drug concentration-time curve (AUC), C,,,,, and time to reach C, (t-) were increased by both strengths of juice. However, terfenadine carboxylate apparent elimination half-life (t& was not altered. The magnitude of the interaction of terfenadine carboxylate AUC and C, ranged severalfold and correlated among individuals for regular-strength (3 = 0.87; p < 0.0001) and double-strength (12 = 0.78; p < 0.0001) grapefruit juice. No differences in the pharmacokinetics of terfenadine and terfenadine carboxylate were observed between the two strengths of grapefruit juice. QT, interval was not altered. G~nclus~ons: A normal amount of regular-strength grapefruit juice produced maximum single-dose effects on terfenadine and carboxylic acid metabolite pharmacokinetics. The mechanism likely involved reduced presys- temic drug elimination by inhibition of more than one metabolic pathway. The extent of the interaction was not su&ient to produce electrocardiographic changes. However, the pharmacokmetic e&cts were highly variable among individuals. This study further enhances the awareness of the potential for a serious interaction between grapefruit juice and terfenadine. (Clin Pharmacol Ther 1997;61:401-9.)
Susan E. Rau, MSc, John R Bend, PhD, J. Malcolm 0. Arnold, MD, Lan T. Tran, BSc, J. Da@d Spence, MD, and David G. Bailey, PhD / London, Ontario, Canada
From the Department of Pharmacology and Toxicology, Univer- sity of Western Ontario, and the Department of Medicine, Victoria Campus, London Health Sciences Centre.
Supported by the Medical Research Council of Canada (grant MA- 11584) and the Victoria Hospital Research Development Fund.
Presented in part at the Tenth International Symposium on Microsomes and Drug Oxidations, July 18-21, 1994, To- ronto, Ontario, and the Canadian Society for Clinical Inves- tigations Meeting, Sept. 15-17, 1995, Montreal, Quebec.
Received for publication Aug. 5, 1996; accepted Nov. 17, 1996.
It is often recommended that medications be ad- ministered at mealtimes to aid in patient compliance to the treatment regimen.’ However, this creates the
Reprint requests: David G. Bailey, PhD, Department of Medi- cine, Victoria Campus, London Health Sciences Centre, 37.5 South St., London, Ontario, N6A 4G.5, Canada.
Copyright 0 1997 by Mosby-Year Book, Inc. 0009-9236/97/$5.00 + 0 13/l/79320
401

402 Rau et al. CLINICAL PHAFSAACOLOGY & THEF-uU’EUTICS
APRIL 1997
Terfenadine
CYP3A4
Azacyclonol
J
Ketone-Acid Metabolite
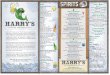
Fig. 1. Proposed scheme for the oxidative biotransformation of terfenadine in humans.
opportunity for food-drug interactions. Grapefruit juice has been shown to produce a severalfold in- crease in the bioavailability of multiple drugs, mak- ing this type of interaction particularly relevant.2s The extent of the interaction between grapefruit juice and felodipine was variable but reproducible within individuals, indicating that the effect was largely dependent on subject characteristics.4 The mechanism of action appears to be reduced presys- temic felodipine elimination by inhibition of cyto- chrome P450 3A4 (CYP3A4) monooxygenase activ- ity.5
Terfenadine is a widely used antihistamine be- cause of its low propensity to impair cognitive func- tion and produce sedation6 It is well absorbed sub-
sequent to oral administration but undergoes nearly complete presystemic elimination by CYP3A4 to two primary metabolites, terfenadine carboxylate and azacyclonol (Fig. 1). 7,8 Normally, terfenadine is not detected in plasma. It is the metabolite, terfen- adine carboxylate, that confers antihistaminic activ- ity in vivo.
Enthusiasm for terfenadine has been tempered more recently by reports that it can cause a serious ventricular arrhythmia, torsades de pointes.9-18 Ap- proximately 125 deaths have been reported.” Ter- fenadine is known to be as potent a blocker of the delayed rectifier potassium current in cardiac myo- cytes as quinidine,‘8,20,21 whereas terfenadine car- boxylate is devoid of this activity. Blockade of this

CLINICAL PHARMA COLOGY & THERAPEUTICS VOLUME 61. NUMBER4 Rau et al. 403
potassium channel by terfenadine and quinidine is the likely explanation for prolongation of the QT, interva1,18’20’21 which predisposes to the develop- ment of this arrhythmia complex.22-25 Case reports of torsades de pointes were associated with concom- itant administration of medications that inhibit CYP3A4, with overdose, or with liver disease,‘-18 and under these conditions plasma terfenadine con- centrations were measurable.10,26 Thus conditions in which the presystemic metabolism of terfenadine is reduced appear to put individuals at risk for tor- sades de pointes.
Because grapefruit juice is widely available, an interaction with terfenadine may have significant impact in the general population. Also, grapefruit juice consumption is not subject to the same regu- lations as prescription medications, which further emphasizes the need for a clear understanding about the consequences of concomitant grapefruit juice and terfenadine administration. Recent clinical investigations have shown that grapefruit juice aug- mented plasma terfenadine concentrations and pro- longed the QT, interva1.27,28 However, subjects were administered double-strength grapefruit juice and the juice was given twice daily for 1 week with terfenadine, which may not reflect routine use. The purpose of this study was to investigate the effects of regular- and double-strength grapefruit juice on the disposition of terfenadine and its metabolite terfen- adine carboxylate during single-dose administration. Electrocardiographic monitoring was also per- formed.
METHODS Study population. Twelve healthy white males (age
range, 23 to 40 years) were tested. An evaluation before the study showed that subjects had normal physical findings and laboratory test results, includ- ing routine 1Zlead electrocardiogram, hematology, serum chemistry, and urinalysis. One subject (sub- ject 11) had laboratory results outside the normal at prestudy evaluation and did not undergo testing with grapefruit juice and terfenadine. Individuals provided written informed consent for the study, which had been approved by the Health Sciences Standing Committee on Human Research at the University of Western Ontario (London, Ontario).
Experimental design. Subjects received 60 mg ter- fenadine (Seldane, Marion Merrell Dow Canada, Inc., Lava& Quebec) with either 250 ml water, regular-strength grapefruit juice (President’s Choice, Loblaws [the same lot number was used
throughout the study]), or double-strength grape- fruit juice (single dilution from concentrate) in a randomized crossover trial. The interval between testing was 1 week. Subjects abstained from alcohol for 48 hours and fasted for 10 hours before testing. Blood was sampled for determination of plasma terfenadine and terfenadine carboxylate concentra- tions just before dosing and at 1/2, 1, 11/2, 2, 21/2, 3, 4, 5, 6, and 8 hours after administration. A standard 1Zlead electrocardiogram was recorded by the same technician with a MAC 6 (Marquette Electronics, Milwaukee, Wis.) before each blood sampling after each subject rested for 5 minutes in the supine position. The position of the electrodes was fixed to subjects during each study day. Mean QT, interval was determined by electrocardiographic digital readout. The largest QT, interval was determined by a trained technician who was blinded to subject, treatment, and order and who manually measured the QT interval and divided it by the square root of the RR interval. The electrocardiograms were also reviewed for variations in ST segment or T-wave morphology, which were confirmed by a cardiolo- gist. Subjects consumed a standardized lunch 4 hours after drug administration. Caffeine-containing beverages and smoking were not allowed, but water was permitted from 3 hours after dosing.
Assay of terfenadine. An assay was modified to improve the sensitivity. 29 The method involved solid-phase extraction and HPLC. In brief, an ali- quot (1.5 ml) of plasma was applied to a 100 mg octadecyl preparatory solid-phase extraction column (Burdick and Jackson, Muskegon, Mich.) after pre- conditioning with methanol and then water. The column was washed once with methanol/water (65:35 vol/vol), and the sample was eluted with methanol/water (9O:lO vol/vol) and evaporated to dryness under nitrogen. Recovery of terfenadine from plasma was >95%. The coefficient of variation of recovery was 3%. This was determined by com- parison of the peak height of terfenadine extracted from four plasma samples (10 &ml) to the peak height of terfenadine dissolved in HPLC mobile phase. The residue was dissolved in a mobile phase (100 ~1) that consisted of methanol/water (75:25 vol/vol) and triethylamine (5 ml/L; Fischer Scien- tific, Fairlawn, N.J.), adjusted to pH 3.2 with phos- phoric acid, and contained the internal standard cetirizine hydrochloride (Pfizer, Kirkland, Ontario). An aliquot (80 ~1) was injected onto a 3 pm octa- decyl 15 cm X 0.46 cm analytical column (CSC ODS2, Chromatographic Specialties, Brockville,

404 Rau et al. CLINICAL PHARMACOLOGY &THERAPEUTICS
APRIL 1997
Table I. Individual terfenadine (T) pharmacokinetic data after administration with water (W), regular-strength grapefruit juice (RS), and double-strength grapefruit juice (DS)
Subject
No. of samples containing terfenadine*
No. T+W T+RS T+DS T+W T+RS T+DS T+W T+RS T+DS
1 1 4 2 0 4 3 0 5 4 0 2 5 0 1 6 0 1 I 0 1 8 2 1 9 0 2
10 1 3 12 0 2 13 0 1
5 I 5 0 5 2 3 2 2 7 1 0
2.1 3.9 - 3.4 - 1.9 - 1.7 - 4.3 - 1.6 - 1.7 1.6 1.4 - 1.8 3.0 2.9 - 1.6 - 1.1
2.8 2.6 6.7
2.3 2.7 6.3 1.3 2.3 2.2 1.0 -
2.0 2.0 - 1.5 - 2.0 - 2.0 - 1.0 - 1.0 - 1.0 1.0 1.5 - 4.0 2.5 1.5 - 1.5 - 2.0
2.0 1.5 4.0 - 1.5 1.5 4.0 2.0 5.0 8.0 2.5 -
*Number of plasma samples in which terfenadine was detected, i.e. >l n&n1 (maximum of 11 per subject for each treatment); C,,, Peak concentration; c,, time to C,,
Ontario) with a mobile phase flow rate of 0.3 ml/ min. Eluate was monitored with a Waters 470 scan- ning fluorescence detector (Waters Chromatogra- phy, Milford, Mass.) at an excitation wavelength of 223 nm and an emission wavelength of 290 nm. The retention times of terfenadine and cetirizine were 9.0 and 13.0 minutes, respectively. The coefficients of variation for plasma terfenadine concentration at 5.0 rig/ml and at the limit of quantitation (1.0 rig/ml) were 7% and 22%, respectively. Plasma terfenadine concentrations less than 1.0 r&ml were detectable. This represents about a fivefold improvement over the former method.
Assay of te@enadine carboxylae. This analytical procedure was also modified from a previous meth- od.2g An aliquot (250 ~1) of plasma and internal standard solution (100 ~1) of diphenhydramine (Parke-Davis, Scarborough, Ontario) was applied to a 100 mg octadecyl preparatory solid-phase extrac- tion column (Waters Chromatography) after pre- conditioning with methanol and then O.OlN hydro- chloric acid. The column was washed with methanol/ water (20:80 vol/vol), and the sample was eluted with methanol/water (75:25 vol/vol) and evaporated to dryness under nitrogen. Recovery of terfenadine carboxylate (Marion Merrell Dow Inc.) and internal standard was >95%. The residue was dissolved in a mobile phase (100 ~1) that consisted of methanol/ water (50:50 vol/vol) and triethylamine (200 ul/L) adjusted to pH 3.0 with phosphoric acid. An aliquot (80 ~1) was injected onto a 3 urn o&y110 cm X 0.32 cm analytical column (Sperisorb, PhaseSep, Clwyd,
England) at a flow rate of 1.4 ml/min. Eluate was monitored by fluorescence detection at an excitation wavelength of 223 nm and an emission wavelength of 290 nm. Retention times of terfenadine carboxy- late and diphenhydramine were 3.0 and 5.0 minutes, respectively. The assay was sensitive to 10 rig/ml (coefficient of variation at 50 rig/ml = 5%).
Data adysis. Plasma drug concentrations were analyzed by a noncompartmental method. The ter- minal elimination rate constant (kJ was determined by log-linear regression of the final data points (at least three). The apparent elimination half-life of the log-linear phase (t,,,) was calculated as 0.693/k,. The area under the plasma drug concentration-time profile was calculated from 0 to 8 hours [AUC(O-S)] by the linear trapezoidal method. The AUC(8-m) was determined by dividing the final concentration by k,. Plasma peak drug concentration (C,,) and the time to reach C,, (t,=) were obtained directly from the experimental data.
Statistical analyses of frequency data (number of samples and subjects with detectable plasma terfen- adine concentrations) were performed with non- parametric methods. Comparisons among the three treatments first used complex x2 analysis. If p < 0.05, the analysis was repeated between the three sets of treatments corrected for multiple compari- sons @ < 0.016 significant). Comparison of terfen- adine C,, between treatments used the Wilcoxon signed-rank test. For subjects in whom terfenadine was not measured, the value of the limit of detection (1.0 r&ml) was assigned. Parametric data analysis

CLINICAL PHARMACOLOGY &THERAPEUTICS VOLUME 61, NUMBER 4 Rau et al. 405
+RS -+DS *w
2 4 6 8
TIME (h)
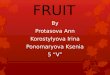
Fig. 2. Mean plasma terfenadine carboxylate concentration-time profiles for individuals (n = 12) administered 60 mg terfenadine with 250 ml regular-strength (RS) or double-strength (DS) grapefruit juice or water (W). Bars represent the SEM. Comparisons were made at each measurement time between the two grapefruit juice treatments and water: **p < 0.01; ***p < 0.001.
was performed on other data with use of ANOVA for repeated measures for initial contrasts among the three groups. For those analyses wherep < 0.05, the effect of the two grapefruit juice treatments was compared with that of water by the paired t test corrected for multiple comparisons (p < 0.025 sig- nificant). Data are presented as mean values t stan- dard error.
RESULTS Plasma terfenadine concentrations. A total of 27
samples (20%;~ < 0.001) from the group that was given terfenadine plus grapefruit juice and 39 sam- ples (30%; p < 0.001) from those given terfenadine plus double-strength grapefruit juice had detectable plasma terfenadine concentrations, in contrast to only four samples (3%) from the group given terfen- adine alone (Table I). This represented all 12 indi- viduals given terfenadine plus grapefruit juice (p < 0.001) and 10 subjects given terfenadine plus double-strength grapefruit juice (p < 0.005) com- pared with three subjects given terfenadine alone. Terfenadine C,, was also higher with regular- strength @ < 0.01) and double-strength @ < 0.05) grapefruit juice than with water. However, the num- ber of samples and subjects with detectable plasma terfenadine concentrations and terfenadine C,, were not different between the two grapefruit juice treatments. The highest plasma terfenadine concen-
trations were observed in two subjects given double- strength grapefruit juice. Terfenadine t,, most fre- quently occurred within 4 hours after dosing.
Te$enadine carboxylute pharmucokinetics. Plasma terfenadine carboxylate concentrations with both strengths of grapefruit juice initially were lower and then exceeded those with water (Fig. 2). This re- sulted in a greater terfenadine carboxylate AUC(O- 9 Cm,, and t,, compared with water (Table II). Calculated terfenadine carboxylate AUC(O-a) with regular-strength (2672 k ng - hr/ml; p < 0.001) and double-strength (2740 _t 35 ng * hr/ml; p < 0.001) grapefruit juice was also greater than that with water (1747 -+ 147 ng * hr/ml). However, terfenadine carbox- ylate t,/, was not different among the three treatments.
The extent of change in terfenadine carbovlate AUC(O-8) and C,, by grapefruit juice relative to water was variable among individuals (Fig. 3). There was a high correlation between these variables by regular-strength (I’ = 0.87;~ < 0.0001) and double- strength (I” = 0.78; p = 0.0001) grapefruit juice. However, a corresponding relationship was not ob- served between terfenadine carboxylate AUC(O-8) and t,,* for either regular-strength (3 = 0.11; p = 0.29) or double-strength (2 = 0.10;~ = 0.31) grape- fruit juice.
Ekxtrocardiographic effects. Mean and longest baseline QT, intervals for regular-strength grape- fruit juice (393 -+ 4 and 395 k 5 msec, respectively),

406 Rati et al. CLINKAL PHARMACOLOGY &THERAPEUTICS
APRIL 1997
Table II. Individual and mean pharmacokinetics of terfenadine carboxylate after terfenadine (T) administration with water (W), regular-strength grapefruit juice (RS) and double-strength grapefruit juice (DS)
Subject AUC(O-8) (ng - hrlml) C,, bM4 t,, VN b2 (hr) No. T+W T+RS T+DS T+W T+RS T-tDS T+ W Tt-RS T+DS T+W T+RS T+DS
1 1504 1637 1237 301 361 277 4.0 5.0 5.0 4.1 2.9 6.0 2 1185 2137 1570 209 404 313 2.5 5.0 6.0 3.2 4.3 5.4 3 1476 1559 1729 302 346 359 3.0 5.0 5.0 3.9 6.1 4.1 4 1063 1367 1871 234 253 433 2.5 5.0 5.0 3.4 4.5 3.0 5 777 1532 1364 151 317 266 4.0 3.0 5.0 5.7 2.1 2.8 6 1089 1511 2210 278 312 451 3.0 3.0 4.0 3.6 3.2 4.9 7 1092 1850 1623 254 402 342 1.0 3.0 3.0 5.0 3.2 3.7 8 1327 2079 1608 263 424 343 1.5 4.0 4.0 4.0 3.4 3.5 9 1274 1331 1311 231 251 296 3.0 5.0 5.0 3.0 3.8 4.2
10 1154 1524 1240 181 274 265 2.0 5.0 5.0 9.0 5.3 9.2 12 689 1595 1470 128 294 293 1.5 2.5 4.0 3.5 3.1 3.4 13 1006 1345 912 216 241 187 1.5 4.0 5.0 3.0 7.4 3.2
Mean 1136 1622 1512 229 323 319 2.5 4.1 4.7 4.3 4.1 4.4 SEM 71 77 98 16 18 21 0.3 0.3 0.2 0.5 0.4 0.5 p Value - <O.ool co.01 - <O.OOl <O.OOl - <O.OOl <O.OOl - NS NS
AUC(O-S), Area under the curve from 0 to 8 hours; C,,, peak concentration; t,,; time to C,,,,; tlR, elimination half-lie. Comparisons were made between water and other treatments.
double-strength grapefruit juice (392 t 2 and 404 + 5 msec, respectively), and water (398 ? 2 and 403 ? 5 msec, respectively) were not different among treat- ments. Subsequently, neither strength of grapefruit juice increased mean or longest QT, interval com- pared with water at any measurement time. No relationship was observed between QT, interval and plasma terfenadine concentration in any individual. Variations in T-wave morphology were observed in five subjects but were evident with all treatments.
DISCUSSION This study establishes that even a single glass of
normal-strength grapefruit juice can augment plasma concentrations of both the cardiotoxic par- ent compound terfenadine and its active antihista- minic metabolite terfenadine carboxylate. Double- strength grapefruit juice did not produce a greater interaction, indicating that an amount of grapefruit juice that could be taken occasionally with terfena- dine produced the maximum single-dose pharmaco- kinetic effect.
Because grapefruit juice likely inhibited the pre- systemic metabolism of terfenadine, it might be an- ticipated that plasma concentrations of terfenadine carboxylate would be reduced. This was evident dur- ing the initial 2 hours after dosing, particularly with the double-strength grapefruit juice. However, ter- fenadine carboqlate concentrations were higher
from 4 to 8 hours for both strengths of grapefruit juice compared with water. The net effect was in- creased terfenadine carboxylate t,, and AUC. This has also been observed in other grapefruit juice- terfenadine studies,27-28 but these publications did not elucidate the mechanism(s) for the changes in the terfenadine carboxylate concentration-time pro- file.
Double-strength grapefruit juice has the highest viscosity of the three solutions tested in this study. For this reason it would be most likely to extend gastric emptying time and thereby lengthen the pe- riod of drug absorption.30’31 Thus protracted gastric emptying time by grapefruit juice could explain the initially lower terfenadine carboxylate concentra- tions and the prolonged t,,. However, this inter- pretation cannot explain the enhanced terfenadine carboxylate AUC.
Proportional increases were observed between terfenadine carboxylate AUC and C,,, but not AUC or t1,2, with both strengths of grapefruit juice among individuals. Also, grapefruit juice did not prolong terfenadine carboxylate t,,z. Consequently, grapefruit juice likely altered other events during the drug absorption phase. Terfenadine is likely converted to terfenadine carboxylate through alco- hol and aldehyde intermediates.32733 Because terfen- adine carboxylate likely undergoes further oxidative metabolism to a ketone carboxylic acid metabolite,

CLINICAL P HABMACOLOGY & THERAPEUTICS VOLUME 61. NUMBER4 Rau et al. 407
0 RS
l DS
0 100 200 300
Relative Terfenadine Carboxylate AUCo43 (%)
Fig. 3. Relative terfenadine carboxylate area under the plasma drug concentration-time profile from 0 to 8 hours [AUC(O-8); grapefruit juice relative to water] plotted against relative terfenadine carbovlate plasma peak drug concentration (C,,) for each individual. The diagonal represents the line of unity.
grapefruit juice may also inhibit this metabolic step during presystemic elimination. An alternative in- terpretation resides in the fact that terfenadine has two primary metabolic pathways, both of which are mediated by CYP3A4.’ Grapefruit juice may aug- ment the terfenadine carboxylate AUC by preferen- tially inhibiting presystemic metabolism by the other route, that is, the N-dealkylation of terfenadine to azacyclonol. However, direct evidence of the effect of grapefruit juice on the disposition of the ketone carboxylic acid metabolite and azacyclonol is cur- rently lacking, and these interpretations should be currently viewed as hypotheses for testing.
Electrocardiographic changes were not found in this study. These results differ somewhat from re- cent trials in which a glass of double-strength grape- fruit juice and 60 mg terfenadine were administered twice daily for 1 week. In the one investigation, mean QT, interval over the 1Zhour dosing interval was increased from 420 + 6 to 432 f 6 msec 0) < 0.05) when grapefruit juice was added to the dosing regimen of six healthy volunteers.27 Plasma terfena- dine C,, concentrations were augmented from un- detectable (~5 @ml) to 7 + 1 r&ml, respectively. In the other trial, six slow metabolizers of terfena- dine (i.e., detectable plasma terfenadine concentra- tions after 1 week of medication) were tested.28 Maximum QT, interval was 415 + 5 msec at base- line, 430 + 5 msec after 1 week of terfenadine (‘JJ = NS), and 434 2 8 msec after 1 week of terfenadine and grapefruit juice @ < 0.05). Plasma terfenadine
C concentrations were quantified in three sub- jeFt;after terfenadine alone (10,8, and 6 @ml) and in all subjects after terfenadine with grapefruit juice (12 + 2 rig/ml). Grapefruit juice has been shown to augment plasma drug concentrations up to 24 hours after a single glass,34 indicating the potential for a cumulative effect of the juice with repeated admin- istrations. Also, terfenadine was given twice daily for 1 week. Therefore it might be reasoned that elec- trocardiographic changes would likely occur only during long-term use of grapefruit juice and terfen- adine. However, the magnitude of the single-dose pharmacokinetic interaction was highly variable among individuals. Consequently, it may not be pos- sible to exclude that the development of electrocar- diographic changes, which predisposes to the devel- opment of torsades de pointes, may also occur under conditions of concomitant single-dose administra- tion of grapefruit juice and terfenadine.
Is there a real clinical risk with grapefruit juice and terfenadine? Data of other terfenadine interac- tions can serve as a guide. The best documented example is the ketoconazole-terfenadine interac- tion. Case reports of torsades de pointes, cardiac arrest, and mortality were the first to signal risk,10Y12 which was confirmed in a large historical cohort evaluation.35 A prospective clinical trial showed that ketoconazole could markedly augment QT, interval, depending on plasma terfenadine concentration.26 Torsades de pointes1’15 and prolongation of the QT, interval with accumulation of terfenadine36’37

408 Rau et al. CLINICAL PHARMACOLOGY & THER4l’EUTIC.S
APRIL 1997
have been reported in combination with itracon- azole, another antifungal agent, and with the mac- rolide antibiotic erythromycin. However, the extent of the interaction appeared to be less than that with ketoconazole. In contrast, to our knowledge there are no reports of torsades de pointes when flucon- azole and azithromycin are combined with terfena- dine. In controlled clinical trials, fluconazole and azithromycin did not produce changes in cardiac repolarization or detectable plasma terfenadine concentrations.38339 Nevertheless, fluconazole and azithromycin are not recommended for concurrent administration with terfenadine because of the sim- ilarities of these drugs to those that are contraindi- cated.
To date, there have been no documented cases of torsades de pointes with grapefruit juice and terfen- adine. However, the reason for this may reside with a general lack of awareness of the potential for such an interaction2’ Indeed, the extent of the interac- tion of terfenadine with grapefruit juice approxi- mated that with itraconazole or erythromycin. Ulti- mately, it may be necessary to have at least one well-documented case of torsades de pointes, car- diac arrest, or mortality with grapefruit juice and terfenadine before there is sufficient evidence to satisfactorily prove clinical risk. On the other hand, there appears to be no benefit from taking grape- fruit juice with terfenadine and there is the potential risk of a serious adverse interaction, regardless of the frequency of occurrence. Thus it seems to be prudent to advise against grapefruit juice consump- tion during therapy with terfenadine or to recom- mend an alternative antihistamine until there is ad- equate data to justify the safety of this combination.
We thank Marie Krupa for electrocardiographic mea- surements.
References 1. Haynes R, Sackett D, Gibson E. Improvements of
medication compliance in uncontrolled hypertension. Lancet 1976;1:1256-68.
2. Bailey DG, Spence JD, Munoz C, Arnold JMO. In- teraction of citrus juices with felodipine and nifedi- pine. Lancet 1991;337:268-9.
3. Bailey DG, Arnold JMO, Spence JD. Grapefruit juice and drugs: how significant is the interaction? Clin Pharmacokinet 1994;26:91-8.
4. Bailey DG, Arnold JMO, Bend JR, Tran LT, Spence JD. Grapefruit juice-felodipine interaction: reproduc- ibility and characterization with the extended release drug formulation. Br J Clin Pharmacol 1995;40:135-40.
5. Bailey DG, Arnold JMO, Munoz C, Spence JD. Grapefruit juice-felodipine interaction: mechanism, predictability and effect of naringin. Clin Pharmacol Ther 1993;53:637-42.
6. McTavish D, Goa KL, Ferrill M. Terfenadine: an updated review of its pharmacological properties and therapeutic efficiency. Drugs 1990;39:552-74.
7. Garteiz DA, Hook RH, Walker BJ, Okerholm RA. Pharmacokinetics and biotransformation studies of terfenadine in man. Arzneimittelforschung 1982;32: 1185-90.
8. Yun CH, Okerholm RA, Guengerich FP. Oxidation of the antihistamine drug terfenadine in human liver microsomes: role of cytochrome P-4503A(4) in N-deallqlation and C-hydroxylation. Drug Metab Dispos 1993;21:403-9.
9. Davies AJ, Harindra V, McEwen A, Ghose RR. Car- diotoxic effect with convulsions in terfenadine over- dose. Br Med J 1989;289:325.
10. Monahan BP, Ferguson CL, Killeavy ES, Lloyd BK, Troy J, Cantilena LR. Torsades de pointes occurring in association with terfenadine use. JAMA 1990;264: 2788-90.
11. Matthews DR, McNutt B, Okerholm R, Flicker M, McBride G. Torsades de pointes occurring in associ- ation with terfenadine use. JAMA 1991;266:2375-6.
12. Zimmermann M, Duruz H, Guinand 0, Broccard 0, Levy P, Lacatis D, et al. Torsades de pointes after treatment with terfenadine and ketoconazole. Eur Heart J 1992;13:1002-3.
13. Crane JK Shih HT. Syncope and cardia arrhythmia due to an interaction between itraconazole and terfen- adine. Am J Med 1993;95:445-6.
14. Pohjola-Sintonen S, Viitasalo L, Toivonen L, Neu- vonen P. Torsades de pointes after terfenadine- itraconazole interaction [abstract]. Br Med J 1993; 306:186.
15. Paris DG, Parente TF, Bruschetta HR, Guzman E, Niarchos AP. Torsades de pointes induced by eryth- romycin and terfenadine. Am J Emerg Med 1994;12: 636-8.
16. Koh KK, Rim MS, Yoon J, Kim SS. Torsades de pointes induced by terfenadine in a patient with long QT syndrome. J Electrocardiol 1994;27:343-6.
17. Kamisako T, Adachi Y, Nakagawa H, Yamamoto T. Torsades de pointes associated with terfenadine in a case of liver cirrhosis and hepatocellular carcinoma. Intern Med 1995;34:92-5.
18. Woosley RL, Chen Y, Freiman JP, Gillis RA. Mech- anism of the cardiotoxic actions of terfenadine. JAMA 1993;269:1532-6.
19. Flockhart DA. Drug interactions, cardiac toxicity, and terfenadine: from bench to clinic? [editorial]. J Clin Psychopharmacol 1996;16:101-3.
20. Yang T, Prakash C, Roden DM, Snyders DJ. Mech- anism of block of a human cardiac potassium channel

CLINICAL PHARMACOLOGY &THERAPEUTICS VOLUME 61, NUMBER4 Rau et al. 409
by terfenadine racemate and enantiomers. Br J Phar- macol 1995;115:267-74.
21. Rampe D, Wible B, Brown AM, Dage RC. Effects of terfenadine and its metabolites on a delayed rectifier K+ channel cloned from human heart. Mol Pharma- co1 1993;44:1240-5.
22. Algra A, Tijssen JGP, Roelandt JRTC, Pool J, Lubsen J. QT, prolongation measured by standard 1Zlead elec- trocardiography is an independent risk factor for sudden death due to cardiac arrest. Circulation 1991;83:1888-94.
23. Bauman JL, Bauernfeind RA, Hoff JV, Strasberg B, Swiryn S, Rosen KM. Torsades de pointes due to quinidine: observations in 31 patients. Am Heart J 1984;107:425-30.
24. Zehender M, Hohnloser S, Just H. QT-interval pro- longing drugs: mechanisms and clinical relevance of their arrhythmogenic hazards. Cardiovasc Drugs Ther 1991;5:515-30.
25. Benedict CR. The QT interval and drug-associated torsades de pointes. Drug Invest 1993;5:69-79.
26. Honig PK, Wortham DC, Zamani K, Conner DP, Mullin JC, Cantilena LR. Terfenadine-ketoconazole interaction: pharmacokinetic and electrocardio- graphic consequences. JAMA 1993;269:1513-8.
27. Benton RE, Honig PK, Zamani K, Cantilena LR, Woos- ley RL. Grapefruit juice alters terfenadine pharmacoki- netics, resulting in prolongation of repolarization on the electrocardiogram. Clin Pharmacol Ther 199659383-8.
28. Honig PK, Wortham DC, Lazarev A, Cantilena LR. Grapefruit juice alters the systemic bioavailability and cardiac repolarization of terfenadine in poor metabo- lizers of terfenadine. J Clin Pharmacol 1996;36:345-51.
29. Coutant JE, Westmark PA, Nardella PA, Walter SM, Okerholm RA. Determination of terfenadine and ter- fenadine acid metabolite in plasma using solid-phase extraction and high-performance liquid chromatogra- phy with fluorescence detection. J Chromatogr 1991; 570:139-48.
30. Winstanley PA, Orme ML. The effect of food on drug bioavailability. Br J Clin Pharmacol 1989;28:261-8.
31. Welling PG. Effect of food on drug absorption. Phar- macol Ther 1989;43:425-41.
32. Chen TM, Chan KY, Coutant JE, Okerholm RA. Determination of the metabolites of terfenadine in hu- man urine by thermospray liquid chromatography-mass spectrometry. J Pharm Biomed Anal 1991;9:929-33.
33. Jurima-Romet M, Crawford K, Cyt T, Inaba T. Ter- fenadine metabolism in human liver. In vitro inhibi- tion by macrolide antibiotics and azole antifungals. Drug Metab Dispos 1994;22:849-57.
34. Lundahl J, RegHrdh CG, Edgar B, Johnsson G. Re- lationship between time of intake of grapefruit juice and its effect on the pharmacokinetics and pharmaco- dynamics of felodipine in healthy subjects. Eur J Clin Pharmacol 1995;49:61-7.
35. Pratt CM, Hertz RP, Ellis BE, Cromwell SP, Louv W, Moye L. Risk of developing life-threatening ventricular arrhythmia associated with terfenadine in comparison with over-the-counter antihista- mines, ibuprofen and clemastine. Am J Cardiol 1994;73:346-52.
36. Honig PK, Worthman DC, Hull R, Zamani K, Smith JE, Cantilena LR. Itraconazole affects single- dose terfenadine pharmacokinetics and cardiac re- polarization pharmacodynamics. J Clin Pharmacol 1993;33:1201-6.
37. Honig PK, Woosley RL, Samani K, Conner DP, Can- tilena LR. Changes in the pharmacokinetics and elec- trocardiographic pharmacodynamics of terfenadine with concomitant administration of erythromycin. Clin Pharmacol Ther 1992;52:231-8.
38. Honig PK, Worthman DC, Zamani K, Mullin JC, Conner DP, Cantilena LR. The effect of flucon- azole on the steady-state pharmacokinetics and electrocardiographic pharmacodynamics of terfena- dine in humans. Clin Pharmacol Ther 1993;53: 630-6.
39. Harris S, Hilligoss DM, Colangelo PM, Eller M, Oker- hohn R. Azithromycin and terfenadine: lack of drug interaction. Clin Pharmacol Ther 1995;58:310-5.