Embed Size (px)
Citation preview

Gold Standards Framework
Dr Mohammed Javid

Aims
• Deaths– Why, where, how
• End Of Life Care– EoLC, ACP, PPC, PPD, GSF, LCP
• Gold Standards Framework– 3 steps– 5 goals– 7 Key tasks

Deaths
• 500, 000 per year in the UK• 1% of the population dies each year• Cause of death
- 25% cancer- 20% heart disease- 15% respiratory disease- 10% strokes and related disorders- 30% other

Place of Death
• Where do people want to die ?– 55% Home– 25 % Hospice– 10 % Hospital– 5 % Care Home
• Where do people die ?– 55 % Hospital– 20% Care Home– 20% Home– 5% Hospice


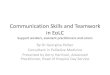
End Of Life Care
supportive andpalliative care
deterioration death/bereavement
ACP / PPC LCPOne year Last days
ACP Advanced care PlanPPC Preferred priorities of care PPD Preferred place of deathGSF Gold standards FrameworkLCP Liverpool Care PathwayEoLC End of Life Care

Gold Standards Framework
IdentifyWhich patients may be in the last year of life + their stage?
Use of register+ planning meeting (PIG, NB Coding ) .
AssessCurrent and Future Clinical needs and Personal needs
(assessment tools, Advance care planning )
Plan Planning care in line with needs -cross boundary Plan care in final days (eg LCP) + action plans

Cancer
Dementiaand
decline
Organ
failure
Sudden death
GSF Step 1: Identify



Assess• Symptom assessment• Personal needs• Preferred priorities of care
– Place of care– Place of death– Advanced Care planning
• Statement of wishes and preferences• Advance decisions• Power of attorney
• Patient focussed – Needs based– Voluntary



Plan
• Communication• Out of hours handover• Drugs in home
– What drugs– DN prescribing– Pharmacy– Syringes, diluents
• OOH bypass number• Crisis prevention

5 GoalsPatients are enabled to have a ‘good death’
1) Symptoms controlled2) Preferred place of care 3) Safe + secure with fewer crises4) Carers feel supported, involved, empowered, and satisfied.5) Staff confidence, teamwork, satisfaction, co-working with specialists and communication better.

7 CC1 Communication
Register, PHCT Meetings, care plan Advanced care planning (ACP) eg PPC
C2 Co-ordinationIdentified co-ordinator for GSF, keyworker for patient
C3 Control of SymptomsAssessment tools,
C4 Continuity Out of HoursHandover form + OOH protocol
C5 Continued LearningLearning about conditions on patients seen, SEA / reflective practice
C6 Carer SupportPractical, emotional, bereavement, National Carer’s Strategy
C7 Care in dying phase- Protocol LCP / ICP

What should we do ?
Level 1 – register, PHCT meeting, co-ordinator C1,2
Level 2 – Assessment tools, OOHs handover, education, audit and reflective practice
C3,4,5Level 3 – Carer/family support, bereavement plan and
protocol for final daysC6,7
Level 4 – Sustain and build on developments, practice protocol, extend

Indicator Points
Payment stage
s
Palliative Care (PC1)The practice has a complete register available of all
patients in need of palliative care/support.
3 —
Palliative Care (PC2)The practice has regular (at least 3 monthly) multidisciplinary
case review meetings where all patients on the palliative care register are discussed.
3 —
Cancer (Cancer 1)The practice can produce a register of all cancer patients
defined as a 'register of patients with a diagnosis of cancer excluding non-melanotic skin cancers from 1 April 2003'.
5 —
Cancer (Cancer 3)The percentage of patients with cancer, diagnosed within
the last 18 months, who have a patient review recorded as occurring within 6 months of the practice receiving confirmation of the diagnosis.
6 40–90%

Records and information (Records 13)There is a system to alert the out-of hours service or duty doctor
to patients dying at home.
2 —
Practice management (Management 9)The practice has a protocol for the identification of carers and a
mechanism for the referral of carers for social services assessment.
3 —
Education and training (Education 7)The practice has undertaken a minimum of 12 significant event
reviews in the past 3 years which could include:New cancer diagnosesDeaths where terminal care has taken place at home
4 —
Education and training (Education 10)The practice has undertaken a minimum of 3 significant event
reviews within the last year.
6 —

Mr W death • GP and DN ad hoc arrangements - no PPoD
discussed or anticipated• Problems with symptom control - high anxiety• Crisis call OOHs - no plan or drugs available in the
home• Admitted to hospital • Dies in hospital • Carer given minimal support in grief• No reflection by PHCT team on care given• ? Inappropriate use of hospital bed?

Mr W with GSF• On GSF Register - discussed at PHCT meeting (C1)• DS1500 and info given to pt + carer (home pack) (C1,
C6)• Regular support, visits phone calls - proactive (C1, C2) • Assessment of symptoms, partnership with SPC -
customised care to pt and carer needs (C3)• Carer assessed incl psychosocial needs (C3, C6)• Preferred place of care noted and organised (C1, C2)• Handover form issued – care plan and drugs issued for
home (C4)• End of Life pathway/LCP/minimum protocol used (C7)• Pt dies in preferred place - bereavement support Staff
reflect-SEA, audit gaps improve care, learn (C5, C6)

Take Home message
• Identify patients in last year of life– Prognostic indicators
• Assess needs– GSF tools
• Plan for deterioration and death

Any Questions
• http://www.endoflifecareforadults.nhs.uk/
• http://www.goldstandardsframework.nhs.uk









![EOLC [EPEC/G ELNEC] Staffcomfortcarechoices.com/wp...iii.pain-educ.-2015.pdf · EOLC [EPEC/G–ELNEC] Staff Education [End-of-Life Nursing Education Consortium - Geriatrics] Eliza](https://img.pdfslide.us/doc/110x75/5f024d4c7e708231d403978f/eolc-epecg-elnec-sta-eolc-epecgaelnec-staff-education-end-of-life-nursing.jpg)