Upload
interaction
View
217
Download
0
Embed Size (px)
Citation preview
7/28/2019 GlobalHealthBriefingBook FINAL Web
1/66
113th Congress
GLOBAL HEALTH:Investing in Our Future
7/28/2019 GlobalHealthBriefingBook FINAL Web
2/66
InterAction IA United Voice for Global Change
1400 16th Street, NW, Suite 210
Washington, D.C. 20036
InterAction is the largest alliance of U.S.-based nongovernmental international organizations, with more
than 180 members. Our members operate in every developing country, working with local communities
to overcome poverty and suffering by helping to improve their quality of life. Visit www.interaction.org.
The following individuals contributed to the development of this briefing book:
Danielle Heiberg, InterAction
Erin Jeffery, InterAction
Ashley Bennett, Global Health Technologies Coalition
Lisa Brandt, InterActionMichelle Brooks, Sabin Vaccine Institute
David Bryden, RESULTS
Amanda Carroll, PATH
Catherine Connor, Elizabeth Glaser Pediatric AIDS Foundation
Erin Fry Sosne, PATH
Filmona Hailemichael, Management Sciences for Health
Tom Harmon, International AIDS Vaccine Initiative
Marielle Hart, Stop AIDS Alliance
Caitlin Horrigan, Population Action International
Jennifer Katz, Drugs for Neglected Diseases initiative
Crystal Lander, Management Sciences for HealthKatie Lapides Coester, Elizabeth Glaser Pediatric AIDS Foundation
Jeff Meer, Public Health Institute
Mike OBrien, American Refugee Committee
Loyce Pace Bass, LIVESTRONG Foundation
Mary Pack, International Medical Corps
Lauren Reliford, PATH
Mannik Sakayan, 1,000 Days
Cover photo: Cameron Calabrese
http://www.interaction.org/http://www.interaction.org/7/28/2019 GlobalHealthBriefingBook FINAL Web
3/66
Global Health Briefing Book
Contents
Introduction to Global Health 3
HIV/AIDS 7
Malaria 11
Tuberculosis 15
Neglected Tropical Diseases 19
Non-Communicable Diseases 23
Maternal and Child Health 27
Nutrition 31
Family Planning and Reproductive Health 35
Water, Sanitation and Hygiene (WASH) 39
Health in Humanitarian Response 43
Vaccination 47
Health Research and Development 51
Millennium Development Goals
& Post-2015 55
Health Systems Strengthening 59
7/28/2019 GlobalHealthBriefingBook FINAL Web
4/66
Many organizations, governments and private donors devote significant resources and expertise to improvingthe health and well-being of individuals worldwide. Several of the NGOs that focus daily on global healthissues, including those that have contributed to this briefing book, are listed below. While each organizationthat appears here may not specialize in every area of health or, for conscience or other reasons, may notfully agree with the views expressed in every brief collectively they recognize the importance of integratingand coordinating health programs in an effort to improve the overall health of individuals worldwide. Thesebriefs are not meant to be consensus documents, but provide a general overview and specificrecommendations on some of the most vital topics in global health.
InterAction always strives to find common ground and shared principles among its members. This approachroutinely unites our diverse membership around a very broad array of topics and policy positions focused onpoor and marginalized populations. There are, however, a range of issues where our members reflect thediffering views within U.S. society, or simply different approaches to global engagement. In such cases, in theinterest of holding our community together without prejudice to one side or the other, InterAction adopts aneutral position on a range of issues, including but not limited to abortion, approaches to aid reform, food aidand military interventions.
Supporting organizations include:
American Red CrossAmerican Society of Tropical Medicine and Hygiene (ASTMH)amfAR, The Foundation for AIDS ResearchCARE USACenter for Health and Gender Equity (CHANGE)Drugs for Neglected Diseases initiative (DNDi)Electronic Health Records InternationalElizabeth Glaser Pediatric AIDS FoundationFriends of the Global Fight Against AIDS, Tuberculosis and MalariaGlobal Health CouncilGlobal Health Technologies CoalitionIMA World HealthIntraHealth International, IncInternational AIDS Vaccine InitiativeInternational HIV/AIDS AllianceInternational Medical CorpsInternational Rescue CommitteeManagement Sciences for HealthMercy CorpsMillennium Water AlliancePATHPopulation Action InternationalPopulation Services International (PSI)Public Health InstituteRESULTSSabin Vaccine Institute
Save the ChildrenSierra Care IncStop AIDS AllianceThe Hunger ProjectThe TB Alliance1,000 DaysU.S. Fund for UNICEFWASH AdvocatesWaterAid AmericaWorld Vision
7/28/2019 GlobalHealthBriefingBook FINAL Web
5/66
Summary
Through critically-needed
investments for global health
programs, the United States
has helped save millions of
lives, as well as contributed to
making the world healthier,
safer and more secure.
Global health programs seek to
address the physical and
mental health needs of
individuals; treat and preventthe spread of infectious
diseases; strengthen the
capability of health workers
and health systems; and
increase access to healthcare
services to improve the overall
well-being of individuals,
families and communities.
Introduction to Global Health
Overview
Why is global health critical?
Americans have always valued caring for those in need, including the
poor, those who are sick and the most vulnerable populations. These
values have been reflected in the United States consistent investment
in global health. To this end, the U.S. has been successful in reducing
child deaths, slowing the spread of AIDS and other infectious or
chronic conditions, responding quickly to health emergencies in times
of disasters, and preventing and treating malnutrition.
National borders do not stop the spread of disease. As such,
addressing global health issues and working to prevent outbreaks
directly impacts the health and well-being of Americans.Investing in the health care needs of individuals reduces the cost of
future pandemics, long-term disability and premature death, and
improves the ability of individuals in developing countries to contribute
to their own economies. A healthy community leads to a healthy
workforce that misses fewer days of work and can continually provide
for their families.
Investing in global health allows developing nations to move toward aid
independence and increase their participation in the global economy.
Now is no time to shy away from our health investments. Scientific innovation
continues to produce miracles at an accelerating pace. International donors are
stepping up to the plate. Many traditional aid recipients are putting more
resources into their own domestic health. The U.S. investment less than 1
percent of our federal budget saves and transforms hundreds of thousands of
lives every year. Its hard to imagine a better return on investment.
Former Senator Bill Frist (R-TN)
Global Health Briefing Book 2013 | 3
7/28/2019 GlobalHealthBriefingBook FINAL Web
6/66
Making Progress
U.S. global health programs have treated
approximately 5.1 million people living
with HIV and prevented the transmission
of HIV to millions more.1
In FY2011, the Presidents Malaria
Initiative (PMI) and its partners
distributed more than 42 million long-
lasting insecticide-treated mosquito
nets and provided treatment to 45
million individuals.2
Immunization programs save more than
3 million lives each year.3
Each year, USAID interventions help
save the lives of more than 6 million
children under the age of 5 and significantly reduce maternal deaths from pregnancy-related causes.4
Over the past five years, the U.S. government has leveraged taxpayer dollars and $4 billion in donated medicines
to provide over 600 million safe and effective neglected tropical disease treatments to approximately 251 million
people cumulatively.5
Centers for Disease Control and Prevention (CDC) programs helped reduce the number of new polio cases
globally by more than 99 percent between 1988 and 2010 ,6 and the CDC-led global campaign to eradicate
guinea worm disease has helped reduce the disease burden from 3.5 million cases per year in 1986 to near
eradication today.7
U.S. Response and Strategy
The U.S. is at the forefront of global health, with targeted initiatives like the Child Survival Call to Action (led by USAIDto end preventable child deaths) and Saving Mothers, Giving Life (a public-private partnership to reduce maternal
mortality). The President's Emergency Plan for AIDS Relief (PEPFAR) and PMI, are helping to create an AIDS-free
generation and reduce the burden of malaria. The U.S. government has also prioritized global health within its
development programs through its Global Health Initiative (GHI). GHI looks to increase the impact of global health
investments and achieve sustainable health outcomes.
At the same time, the U.S. government is not alone in its efforts to improve global health. Significant contributions are
made by other nations, as well as multilateral organizations such as the World Health Organization; public-private
partnerships such as the Global Fund to Fight AIDS, Tuberculosis and Malaria and the Global Alliance for Vaccines
and Immunization (GAVI); private foundations; and civil society organizations. These donor partnerships allow global
health funding to be leveraged across multiple health sectors to benefit and reach those who are in most need.
The U.S. is at a critical juncture in its global health efforts: budget pressures threaten the global health gains that havebeen made and jeopardize programming despite the growing consensus within Congress, across government
agencies and throughout the broader global health community about what is working and what remains to be done.
Capitalizing on our successes and meeting emerging global health challenges will require increased and sustained
commitments by all donors.
Benoit Darrieux
Global Health Briefing Book 2013 | 4
7/28/2019 GlobalHealthBriefingBook FINAL Web
7/66
Recommendations
The Administration should:
Maintain U.S. government support for overall global health programs and initiatives, including support for
health systems strengthening.
Continue partnerships with other donors, such as the private sector and civil society organizations , to
most effectively leverage donor contributions to global health.
Ensure that its global health efforts are aligned with the priorities of developing nations so that U.S.
investments are effective, sustainable and focused on building the capacity of local communities to provide for
their future health needs.
Work to reduce inequities in access to quality health care as it invests in lower-income countries. This
requires increased engagement with vulnerable and traditionally marginalized populations, including women, youth
and persons with disabilities.
Ensure that humanitarian health programs during crises lay a foundation for effective health systems so
nations can successfully transition from providing relief to development programs. Fragile states often lack the
ability to partner with development agencies to deliver care and provide basic security to access health services,
which is crucial to developing sustainable, lasting health systems.
Congress should:
Maintain appropriate funding level for all health accounts. If the U.S. fails to live up to its commitments, the
gains made in reducing incidences of maternal mortality, tuberculosis, malaria, HIV and other diseases in
developing countries could stagnate or even reverse. Sustained U.S. investments in global health programs and
health systems strengthening are crucial health problems will only be more expensive and difficult to resolve in
the future, especially with the rise of chronic non-communicable diseases (cancers, lung and heart disease, and
diabetes) in all populations.
Continue to invest in global health research and evaluation programs that develop and implement new
technologies and tools to assist countries anticipate future health challenges.
Encourage federal agencies to ensure that their global health programs are integrated, recorded,
monitored and evaluated so efficiency improvements can continue to be made throughout the global health
sector.
Provide adequate funding in order to train a capable health workforce.
Benoit Darrieux
Global Health Briefing Book 2013 | 5
7/28/2019 GlobalHealthBriefingBook FINAL Web
8/66
Contributors
InterAction
Erin Jeffery
Danielle Heiberg
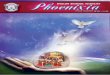
Global Health Appropriations Chart ($ in thousands)
1 World AIDS Day 2012 Update, PEPFAR. http://www.pepfar.gov/funding/results/index.htm.2 The Presidents Malaria Initiative, Sixth Annual Report to Congress. http://pmi.gov/resources/reports/pmi_annual_execsum12.pdf.3 Combination Prevention in PEPFAR: Treatment, PEPFAR. http://www.pepfar.gov/documents/organization/ 183299.pdf.4 USAID Maternal and Child Health, USAID. http://www.usaid.gov/what-we-do/global-health/maternal-and-child-health.5 USAIDs Neglected Tropical Diseases Program, USAID. http://www.neglecteddiseases.gov/about/index.html.6 National Institute of Neurological Disorders and Stroke: Post-Polio Syndrome Face Sheet. http://www.ninds.nih.gov/disorders/post_polio/
detail_post_polio.htm.7 Guinea Worm Frequently Asked Questions, CDC. http://www.cdc.gov/parasites/guineaworm/gen_info/faqs.html.
a Estimate based on assumption of proportional increases or decreases from FY2012 levels for the global health subaccounts.b Global Fund totals include $300 million (FY2010) and $297.3 million (FY2011) from Labor-HHS appropriations accounts.c Due to a $250 million shift from bilateral to multilateral funding, the Global Fund received $1.3 billion in FY12 and PEPFAR received $4.243 billion.
Accounts FY2010 FY2011 FY2012
FY2013 CR Post
-Sequestration
Estimatea
Global Health Initiative (GHP USAID & State) 7,874,000 7,829,310 7,917,860 8,038,030
Global Health Programs (USAID) 2,515,000 2,495,000 2,625,000 2,609,750
Maternal and Child Health 549,000 548,900 605,550 594,155
Family Planning/Reproductive Health
in all accounts 648,500 613,770 610,000 598,521
The GAVI Alliance 78,000 90,000 130,000 123,370
Nutrition 75,000 89,800 95,000 93,212
Vulnerable Children (USAID) 15,000 15,000 17,500 17,171
HIV/AIDS (USAID) 350,000 349,300 350,000 343,414
Other Infectious Diseases (USAID) 981,000 968,100 1,033,000 1,013,561
Malaria 585,000 618,800 650,000 637,768
Tuberculosis 225,000 224,600 236,000 231,559
Neglected Tropical Diseases 65,000 76,800 89,000 87,325
Global Health Programs State (PEPFAR Only) 4,609,000 4,585,800 4,243,000 3,862,430
Global Fund to Fight HIV/AIDS, Malaria & TB 1,050,000b
1,045,800b
1,300,000c
1,565,850
NIH Global Health 587,610 520,700 581,000 551,369
CDC Global Health 354,403 340,300 347,600 329,872
Water in all accounts 315,000 314,370 315,000 329,037
Global Health Briefing Book 2013 | 6
7/28/2019 GlobalHealthBriefingBook FINAL Web
9/66
Summary
The HIV/AIDS epidemic
continues to be a major global
health challenge, but with U.S.
support and leadership, an
AIDS-free generation is within
reach.
HIV/AIDS impacts the overall
development in many of the
most vulnerable countries
because it undermines efforts
to reduce poverty, improve
access to education and
healthcare, address gender
inequalities and maintain
national security.
The U.S. is the largest funder of
HIV/AIDS programs worldwide
through support for the
Presidents Emergency Plan for
AIDS Relief (PEPFAR) and the
Global Fund to Fight AIDS,
Tuberculosis and Malaria
(Global Fund).1
HIV/AIDS
Overview
In 2011, approximately 34 million people worldwide, including 3.4million children under 15, were living with HIV/AIDS. However, the
number of new HIV infections and deaths from the disease are on the
decline in many of the hardest-hit countries.2
In 2011, 1.7 million people died of AIDS-related illnesses and 2.5
million people were newly infected with HIV.3 In fact, 39 countries have
seen new infections among adults decrease by more than 25 percent
between 2001 and 2011, and deaths from AIDS have fallen by one-
third in the past 6 years.4
The HIV/AIDS pandemic disproportionately affects sub-Saharan Africa,
where almost three out of every four new infections occur.5
Millions of HIV-infected individuals lack the treatment services they
need to survive and thrive. The number of children accessing
treatment is especially troubling, with only 28 percent of eligible
children on treatment compared to 54 percent of eligible adults.6
The majority of those living with HIV do not know they are infected.7
Women represent more than half of all current cases of HIV. Women
also often have less power in relationships and during sexual
encounters, leaving them vulnerable to coercion and gender-based
violence. HIV/AIDS is the leading cause of death among women of
reproductive age.8
Stigma, discrimination, legal barriers and the violation of human rights
pose major obstacles for key populations including men who have
sex with men, sex workers and people who use drugs to access HIV
prevention, treatment and care services in many countries around the
world.
PEPFAR is the largest commitment by a nation to combat a single
disease internationally, both programmatically and scientifically.
Additionally, the U.S. is responsible for 72 percent of global spending
on HIV/AIDS research and development.9
The Global Fund was created in 2002 to raise and disburse large sums
of money around the world to prevent and treat AIDS, tuberculosis andmalaria, diseases that together kill 5 million people every year. An
innovative public-private partnership, the Global Fund leverages $2 for
every $1 invested by the U.S. government while maximizing impact by
working in close coordination with PEPFAR and other U.S. programs.
James Pursey
Global Health Briefing Book 2013 | 7
7/28/2019 GlobalHealthBriefingBook FINAL Web
10/66
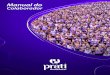
Making Progress
As of the end of FY2012, U.S.
assistance directly supported
more than 5.1 million patients on
life-saving antiretroviral
treatment, and more than 46.5
million people with counseling and
testing programs.10
PEPFAR provided resources and
funding for the prevention of
mother-to-child HIV transmission
for more than 11 million HIV-
positive pregnant women, allowing
more than 230,000 infants to be
born HIV-free in FY2012. Globally over 57 percent of women received the necessary treatment and services
to reduce transmission from mother to child, up from 15 percent in 2005.11
As of December 2012, the Global Fund had provided HIV/AIDS treatment to 4.2 million people, as well as
services to 1.7 million pregnant women. On average, the Global Fund saves 100,000 lives each month with
its work on HIV, tuberculosis and malaria.
Recent scientific advances have reinforced the fact that putting HIV-positive individuals on treatment is not only
good for their own health, but also reduces the likelihood of transmission to others.
PEPFAR plays a fundamental role in reaching key populations with targeted services and creating an enabling
environment for working with stigmatized groups in both generalized and concentrated epidemics.
To ensure that countries are able to sustain and build on progress to date, PEPFAR programs continue to invest in
building strong health and community systems that increase national capacity to implement country-led HIV/AIDS
programs.
PEPFAR has begun to transition from an emergency response to one of long-term sustainability through
partnerships and country ownership. U.S. investment has been leveraged with other bilateral and multilateral
partners to create a truly global response.
U.S. Response and Strategy
Since President George W. Bushs announcement of PEPFAR in 2003, the U.S. has invested more than $40 billion in
the global AIDS response. The program was most recently reauthorized through the Tom Lantos and Henry J. Hyde
United States Global Leadership Against HIV/AIDS, Tuberculosis and Malaria Reauthorization Act of 2008.
Implemented through the Office of the Global AIDS Coordinator (OGAC) in the Department of State, PEPFAR is a
multiagency effort supporting HIV/AIDS programs mainly through USAID and the Centers for Disease Control and
Prevention, with additional programming through the Department of Defense, the Department of Health and HumanServices and the Peace Corps. The program works closely with other major bilateral and multilateral donors such as
the Global Fund.12
Scientific advances since the beginning of PEPFAR have improved how we respond to the global HIV/AIDS epidemic,
and in turn have made U.S.-funded programming more efficient and effective. The PEPFAR program now has a clear
plan how the U.S. government is going to lead the world towards the end of AIDS in the recent Blueprint Towards an
AIDS-Free Generation. The Blueprint has a simple goal: make smart investments based on sound science with a
shared global responsibility in order to achieve an AIDS-free generation.
Source: AIDSInfo
Global Health Briefing Book 2013 | 8
7/28/2019 GlobalHealthBriefingBook FINAL Web
11/66
Recommendations
Congress should maintain strong funding levels for the PEPFAR program. We recognize that these are
challenging economic times. However, U.S.-funded global HIV/AIDS programs have shown a consistent return on
investment measured in lives saved, costs avoided through infections prevented and the generation of goodwill
among global partners. Strong support from Congress, including policies that support the effectiveness of HIV/
AIDS programming, is critical to advancing the global AIDS response.
Congress should continue to support the Global Fund. Multilateral funding complements bilateral funding by
leveraging investments from other donors, helping build country-level commitment and strengthening capacity at
all levels to deliver programs. U.S. leadership has been and remains the most important leveraging tool available
to the Global Fund. In the lead up to the Fourth Replenishment of the Global Fund, scheduled for fall 2013, it is
critically important for the U.S. government to signal to the international community its continued strong support by
providing robust funding for the Global Fund in FY2014.
Support scientific advances towards the end of HIV/AIDS. Even with amazing strides toward ending the global
AIDS crisis, many undiscovered breakthroughs remain. A vaccine and a cure are on the horizon. New
technologies and treatments could be game changers. Ten years of global HIV/AIDS programming experience will
pave the way towards an AIDS-free generation if we can harness lessons learned. U.S. support for HIV/AIDSresearch is critical, not just for those suffering from and at risk for HIV/AIDS around the world, but also for the more
than 1 million people living with HIV in the United States.
Source: 2012 Country Progress Reports (www.unaidsorg
Global Health Briefing Book 2013 | 9
7/28/2019 GlobalHealthBriefingBook FINAL Web
12/66
Contributors
Elizabeth Glaser Pediatric AIDS Foundation
Katie Lapides Coester
International HIV/AIDS Alliance
Marielle Hart
International AIDS Vaccine Initiative (IAVI)
Jennie Aylward
1 Neglected disease R&D: A five-year review, G-FINDER, 2012. Pg. 28.2 Report on the Global AIDS Epidemic, UNAIDS, 2012. Pg. 8.3 Ibid. Pg. 8.4 Ibid. Pg. 11.5
Ibid. Pg. 11.6 Ibid. Pg. 47.7 Progress Report 2011: Global HIV/AIDS Response, WHO/UNAIDS/UNICEF, 2011.8 Women and Health: Today's Evidence Tomorrow's Agenda, The World Health Organization, 2009.9 Neglected disease R&D: A five-year review, G-FINDER, 2012. Pg. 28.10 World AIDS Day 2012 Update, PEPFAR. http://www.pepfar.gov/funding/results/index.htm.11 On the Road to an AIDS-Free Generation, Dipnote. http://blogs.state.gov/index.php/site/entry/on_the_road_to_aids_free_generation.12 Report on the Global AIDS Epidemic, UNAIDS, 2012. Pg. 11.
Global Health Briefing Book 2013 | 10
7/28/2019 GlobalHealthBriefingBook FINAL Web
13/66
Summary
Malaria control is a model of
cost-effective success.
Increased funding directly
correlates with a drop in
malaria.
Malaria cases have been cut in
half in more than 40 countries
worldwide, saving over a
million lives in the past decade.
Malaria is at a tipping point:
history shows that if we scaleback funding, malaria will
reemerge worse than ever,
especially since populations
with reduced immunity will face
an increase in morbidity. If we
act now, we can build on our
past decade of success. The
U.S. has been a global leader in
the fight against malaria. Its
imperative the U.S. continues
to build upon its legacy and
support countries working to
eliminate malaria and the
needless deaths and disability
of children around the world.
Malaria
Overview
Malaria is a serious and sometimes fatal disease caused when a
mosquito infected with the malaria parasite feeds on humans. People
with malaria suffer from high fevers, shaking chills and flu-like
symptoms and, in severe cases, death.
Despite progress, malaria continues to be one of the leading killers of
children under 5.
In 2010, there were an estimated 219 million cases of malaria per year
and 660,000 deaths. An estimated 91 percent of deaths in 2010 were
in Africa, followed by Southeast Asia and the Eastern Mediterranean.
Approximately 86 percent of deaths globally were among children.
Malaria typically occurs in tropical and subtropical areas of the worldwhere the parasite thrives. Half of the worlds population is at risk of
malaria infection.
The economic cost of malaria is estimated at a minimum of $12 billion
in lost productivity each year in Africa alone. Research from the UN
Secretary-Generals Special Envoy for Malaria has indicated that for
every $1 invested in malaria control in Africa $40 is generated in GDP.
Preventing malaria is crucial for protecting U.S. and other nations
troops serving in countries where malaria is prevalent.
The progress achieved to date is at risk of stalling. International
funding for malaria control has leveled off in recent years.1
The numbeof long-lasting insecticide-treated nets (LLINs) procured in 2012 was
66 million far fewer than the 92 million procured for distribution in
2011, and less than half of the 145 million procured in 2010.
Lifesaving LLINs cost only $2.20 per person per year, but the average
lifespan of an LLIN is only 2 to 3 years. LLIN distribution and
replacement are vital. We must uphold coverage levels until malaria is
actually eliminated, community by community. The mass scale-up of
LLIN coverage over the last decade from 3 percent in 2000 to 53
percent in 2012 is working.
Progress is also threatened by increasing resistance of the mosquito to
insecticides and of the parasite to drugs.
PATH MACEPA
Global Health Briefing Book 2013 | 11
7/28/2019 GlobalHealthBriefingBook FINAL Web
14/66
Making ProgressInterventions against malaria over the past decade have averted over 274 million malaria cases and saved 1.1
million lives.
Under the leadership of President George W. Bush, the Presidents Malaria Initiative (PMI) was launched in 2005,
a five-year, $1.265 billion expansion of the U.S. governments response to malaria control. PMIs initial objective
was to reduce malaria-related deaths by 50 percent in 15 African focus countries. This was in addition to the U.S.
being the largest contributor to the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), which to
date has distributed over 310 million insecticide treated nets.2
Since its establishment, PMI has funded the distribution of more than 31 million bednets, 92 million
lifesaving antimalarial treatments, 24 million rapid diagnostic tests and 12 million intermittent preventive
treatments for pregnant women.Successful malaria interventions can improve the treatment of other diseases that afflict the same population. For
example, U.S.-funded malaria control efforts in Zambia led to an increase in diagnoses of respiratory infections in children
under the age of 5, prompting better and appropriate treatment and bolstering the effectiveness of local health systems.
Past investments in R&D resulted in the development of the drugs, insecticides and diagnostic tools that are in use
today and brought the world closer to its first-ever malaria vaccine.
U.S. Response and Strategy
Under the Tom Lantos and Henry J. Hyde United States Global Leadership Against HIV/AIDS, Tuberculosis and
Malaria Reauthorization Act of 2008, PMI was extended and its goal was broadened to achieve Africa-wide impact by
halving the burden of malaria in 70 percent of at-risk populations in sub-Saharan Africa. Specifically, PMI has
expanded to two new focus countries (Guinea and Zimbabwe), and expanded its programs in Nigeria and the
Democratic Republic of the Congo.
In 2011, PMI commissioned an External Evaluation of its first five years a rare undertaking for a government agency.
The Evaluation Team, after site visits, partner interviews and review of documentation, declared PMI to be a very
successful, well-led component of the U.S. government Global Health Initiative that quickly reoriented a problematic
U.S. government malaria program, took it to a large scale quickly, efficiently and effectively complemented the larger
global malaria program, and contributed to the apparent reduction in child mortality.3
Source: Kaiser Family Foundation
Global Health Briefing Book 2013 | 12
7/28/2019 GlobalHealthBriefingBook FINAL Web
15/66
Recommendations
Congress and the Administration should maintain strong support for PMI and the Global Fund . Sustained
support is needed to capitalize on this unique moment in history. With past investments, we have backed malaria
into a corner. We are at a tipping point and must build on the progress achieved to create a malaria-free future and
eliminate the threat of resurgence.
Congress should continue its investment in the research and development of new tools and approaches
that hold the promise of eliminating the disease and combating drug resistance. Consideration must be given to
the long-term benefits of U.S. leadership in R&D and the need for new tools to accelerate progress towards ending
malaria.
Donors should continue to support elimination efforts in specific geographies. Elimination means the end of
recurring costs of controlling and treating the disease; an end to school and work days lost while sick with malaria
and an end to the needless deaths and disability of children around the world. Today, with new tools on the
horizon and strong partnerships and programs in endemic countries, we are closer than ever to achieving our
elimination goals.
USAID must continue to promote the linkages between malaria and other leading causes of death for
children under 5. Linking with pneumonia and diarrhea prevention efforts in particular will help maximizeefficiencies and achieve greatest results.
Global Health Briefing Book 2013 | 13
7/28/2019 GlobalHealthBriefingBook FINAL Web
16/66
Contributors
PATH
Amanda Carroll
Sally [email protected]
Kammerle Schneider
American Society of Tropical Medicine and Hygiene (ASTMH)
Erin Morton
Jodie Curtis
1 World Malaria Report 2012, World Health Organization. http://www.who.int/malaria/publications/world_malaria_report_2012/en/index.html.2 Global Fund support extends antiretroviral treatment to 4.2 million people, The Global Fund. 2012. http://www.theglobalfund.org/en/mediacenter/newsreleases/2012-11-29_Global_Fund_support_extends_antiretroviral_treatment_to_4,2_million_people/.3External Evaluation of the Presidents Malaria Initiative: Final Report, Pg. 67.
Global Health Briefing Book 2013 | 14
7/28/2019 GlobalHealthBriefingBook FINAL Web
17/66
Summary
Tuberculosis (TB) is a bacterial
infection that is airborne and
spread mainly by coughing. It
kills three people a minute, is a
threat to the United States and
puts health care personnel at
risk. Yet, it is one of the best
buys in global health, since it
can usually be cured with
inexpensive drugs.
People with TB, especiallywomen, often suffer from
discrimination and rejection.
Stigma inhibits people from
accessing treatment, leading to
needless death, or may
interfere with treatment
completion, leading to the
development of drug
resistance.
U.S. aid is helping the world
score impressive gains against
TB. USAID provides assistance
to 28 countries, boosts the
supply chain and supports
research into new tools to fight
TB.
Tuberculosis
Overview
TB strikes adults in their most productive years and often pushes
families deeper into poverty. In India, an estimated 100,000 women are
abandoned each year by their families as a result of TB stigma. 1
TB treatment is long and arduous, ranging from six months to two
years, and requires multiple medications. Side effects of treatment for
drug-resistant TB can include acute pain and hearing loss.
Most of the current TB drugs were developed more than 40 years ago.
The existing TB vaccine, more than 90 years old, does not protect
against the most common, contagious form of the disease and has
failed to halt the epidemic. New and better tools will transform the fight
against TB.TB often goes undetected in children, though progress is being made.
Children are more likely to develop the most deadly forms of TB, such
as TB that affects the brain. In 2010, there were about 10 million
orphaned children as a result of TB deaths among parents. 2
Healthcare workers have a two to three times greater risk of
contracting TB than the general population, yet protection is
inadequate.
Shortages of medication and improper or incomplete treatment have
led to often-deadly multidrug-resistant (MDR) and extensively drug-
resistant (XDR) strains.
Progress against multidrug-resistant TB has been slow, with only one
in five patients being diagnosed and even fewer starting treatment fo
the disease.
In South Africa, drug resistant TB consumed about 32 percent of the
countrys estimated 2011 national TB budget of $218 million.3
TB is a serious threat to public health in United States, and is reported
in every state. In 2011, 62 percent of the reported U.S. cases occurred
in foreign-born persons.4 Drug resistant TB in the U.S. costs anywhere
from $100,000 to $1 million per patient.
TB is the leading infectious killer of people with HIV/AIDS, andthreatens the substantial gains made through The Presidents
Emergency Plan for AIDS Relief (PEPFAR) and the Global Fund to
Fight AIDS, Tuberculosis and Malaria (Global Fund). However,
progress toward the integration of TB and HIV services into one
seamless service is helping to save lives.Aeras
Global Health Briefing Book 2013 | 15
7/28/2019 GlobalHealthBriefingBook FINAL Web
18/66
Making Progress
An estimated 20 million people are alive today as a direct result of TB programs.5 Since 2002, with U.S.support, Cambodia has achieved a 45 percent drop in TB, while expanding services to children.
A new, U.S.-developed technology, called Xpert, is revolutionizing the TB response. It can diagnose TB withintwo hours, even among people whose TB is often hard to detect, such as those living with HIV. It can also detectresistance to one of the primary TB drugs.
TB-related deaths among people living with HIV in Africa have declined by 28 percent since 2004.6Providing access to antiretroviral drugs soon after HIV diagnosis has been proven to lower new TB casesby 63 percent.
Major innovations in TB treatments that will reduce suffering, cut treatment time and save money are on thehorizon. However, there is a $25.6 million shortfall in USAID funding for drug development, which could lead todelays in the roll out of new medications.
Vaccines that prevent adolescents and adults from developing infectious TB would be one of the single greatestadvances in the global fight against the disease. Enormous progress has been made, with more than a dozenvaccine candidates in clinical trials. Expanded U.S. support for vaccine R&D is crucial to preserving thismomentum.
U.S. Response and Strategy
The USAID TB program, while modestly funded, has proven effective and essential. In addition, PEPFAR makes a
critical contribution to addressing TB-HIV coinfection and recently issued the Blueprint for an AIDS-Free Generationwith strong commitments on TB-HIV. The U.S. is also a major backer of the Global Fund, which provides 82 percent
of international financing for TB and, to date, has detected and treated 9.7 million cases of TB.7 The U.S. also backs
the World Health Organization and its partnerships, which provide essential global leadership and assistance in the
fight against TB, and the Global Drug Facility, which supplies lifesaving TB treatments. Finally, the U.S. supports
research programs through USAID, the National Institutes of Health (NIH), the Food and Drug Administration (FDA)
and the Centers for Disease Control and Prevention, which are developing innovative TB products and approaches.
Source: Global Tuberculosis Report 2012. WHO, 2012.
Global Health Briefing Book 2013 | 16
7/28/2019 GlobalHealthBriefingBook FINAL Web
19/66
Recommendations
The global fight against TB remains fragile and the momentum to break this disease is at risk of faltering. Since TB
knows no borders, this puts lives at risk globally as well as in the U.S., where cases among foreign-born persons have
remained high. We recommend several steps to stay on course and ultimately overcome the global TB epidemic.
U.S. agencies should provide technical assistance and support to countries that are showing boldleadership and national plans on TB. South Africa, for instance, has produced its first ever joint TB and HIV
strategy and is aiming, along with other countries in the region, to eliminate TB and HIV deaths.7
The U.S. government should back innovation in TB programming, including community-centered approaches
and the latest technology, which TB REACH an initiative of the Stop TB Partnership has demonstrated can be
used to reach many more patients.
U.S. agencies should combine TB prevention and care with other services, including those for mothers and
children. Making TB services an integral part of HIV, prenatal care, family planning and immunization programs will
prevent millions of unnecessary deaths among women and children.
Congress should provide $400 million in FY2014 for USAIDs global TB program, including vital TB research,
and $1.65 billion for the U.S. contribution to the Global Fund. We recognize that these are challenging economic
times, however these complementary programs are well positioned to make effective use of these resources, while
leveraging contributions from other donors as well as affected-country governments.
Congress should maintain current funding for NIH to preserve its crucial biomedical research on TB and new TB
tools which could radically accelerate efforts to eliminate the disease. Congress should also maintaining funding for
the FDA to preserve the Critical Path Initiatives support for the development of new TB drugs and vaccines.
Trends in TB Cases in Foreign-born Persons, U.S. 1991-2011
Source: Tuberculosis in the United States, 2011 (Slide Set), US Centers for Disease Control
Global Health Briefing Book 2013 | 17
7/28/2019 GlobalHealthBriefingBook FINAL Web
20/66
Contributors
RESULTSDavid Bryden
American Thoracic SocietyNuala S. Moore
With additional input and support from members of the Tuberculosis Roundtable:Aeras www.aeras.org
American Thoracic Society www.thoracic.org
Global Health Technologies Coalition www.ghtcoalition.org
IDSA Center for Global Health Policy www.idsaglobalhealth.org
Management Sciences for Health www.msh.org
PSI www.psi.org
RESULTS www.results.org
1 Rajeswari, R., et al. Socioeconomic impact of tuberculosis on patients and family in India, The International Journal of Tuberculosis and Lung
Disease, 1999. 3(10): 869-77. http://www.ingentaconnect.com/content/iuatld/ijtld.2 Tuberculosis Fact sheet N104, World Health Organization, October 2012.3 Pooran, A, et al. What is the Cost of Diagnosis and Management of Drug Resistant Tuberculosis in South Africa?, PLOS ONE, 2013. http://
www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0054587.4 Trends in Tuberculosis, U.S. Centers for Disease Control, 2011.5 20 million lives saved through TB care and control, World Health Organization, 17 October 2012. 6 Global Report 2012, UNAIDS. 2012. Pg. 58.7 Global Fund support extends antiretroviral treatment to 4.2 million people, The Global Fund. 2012. http://www.theglobalfund.org/en/mediacenter/
newsreleases/2012-11-29_Global_Fund_support_extends_antiretroviral_treatment_to_4,2_million_people/.
Global Health Briefing Book 2013 | 18
7/28/2019 GlobalHealthBriefingBook FINAL Web
21/66
Summary
Neglected Tropical Diseases
(NTDs) are tied to nearly every
major global health issue faced
today, including water and
sanitation, malnutrition, and
maternal and child health.
The U.S. government has
played a key role in NTD
control and elimination since
2007 by supporting the
cumulative delivery of over 600million treatments to over 251
million people in 25 countries
through USAIDs NTD program.
Addressing the link between
health and other sectors of
development, along with
increased research and
development (R&D), is
necessary to meet the 2020
control and elimination goals.
These efforts could improveand in some cases save the
lives of over 1 billion people
across the developing world,
assisting them to climb out of
poverty and live healthy,
productive lives.
Neglected Tropical Diseases
Overview
NTDs are a group of 17 infectious diseases and conditions afflicting
more than 1 billion of the worlds poorest people and threatening the
health of millions more.1
NTDs disproportionately affect poor and rural populations who lack
access to safe water, sanitation and essential medicines; they are
most prevalent in Africa, Asia, Latin America and the Caribbean.
NTDs cause sickness and disability, compromise maternal health and
fetal growth, inhibit childrens mental and physical development, and
can result in blindness and severe disfigurement. A number of NTDs
are fatal without treatment.
NTDs can lead to poverty and have an impact far beyond the healthsector, undermining efforts to improve education, empower women
and girls, and foster economic development. These diseases disable
and debilitate their victims, keeping children out of school and
preventing adults from working.
Since 2006, the U.S. has been an essential leading partner in
advancing control and elimination efforts for seven targeted NTDs:
lymphatic filariasis (elephantiasis), onchocerciasis (river blindness),
schistosomiasis (snail fever), soil transmitted helminthes (ascariasis
(roundworm), trichuriasis (whipworm) and hookworm) and trachoma.
The NTD program administered by USAID has made important and
substantial contributions toward the global fight to control and
eliminate these seven NTDs by 2020. Leveraging more than $4 billion
in donated medicines, USAID has supported the distribution of over
600 million treatments in 25 countries.2
While the most common NTDs have treatments that are easy to use
and effective, for the NTDs with the highest death rates, including
human African trypanosomiasis, visceral leishmaniasis and Chagas
disease, treatment options are extremely limited. New investments are
urgently needed to support research and development for new tools,
including diagnostics, drugs and vaccines, for all NTDs.
As the world becomes increasingly interconnected, the spread ofdisease across national borders poses a threat to all countries. NTDs,
including Chagas disease and dengue, have an increased prevalence
in the U.S.
In addition to USAID, other U.S. agencies involved in research and
control efforts for NTDs include the National Institutes for Health (NIH),
the Centers for Disease Control and Prevention (CDC) and the
Department of Defense (DoD).
Zubaedah Kendar, RTI International
Global Health Briefing Book 2013 | 19
7/28/2019 GlobalHealthBriefingBook FINAL Web
22/66
Making Progress
Over the past decade, the momentum behind the control and elimination of NTDs has increased dramatically. The
World Health Organization (WHO) developed its first Strategic Plan in 2003 and the U.S. government first
allocated $15 million in FY2006 for the creation of an integrated NTD control program administered by
USAID. The British government followed in 2008, with the development of its own NTD control program.
In January 2012, inspired by the WHO 2020 Roadmap for NTDs, a range of public and private partners including
pharmaceutical companies, donor governments, endemic countries, research organizations, the World Bank, and
the Bill and Melinda Gates Foundation, announced the London Declaration on NTDs, a new coordinated
commitment to control and eliminate 10 NTDs by 2020. By the end of 2012, over 40 countries had developed
NTD master plans outlining their strategies for achieving NTD control and elimination targets.
U.S. Response and Strategy
Support for NTD control has grown in recent years and has received widespread bipartisan support from U.S.
policymakers. Several U.S. agencies have programs focusing on NTDs:
USAIDs NTD program, in coordination with WHO and global partners, supports interventions for the control and
elimination of seven targeted NTDs including assistance for NTD program implementation led by Ministries of
Health; drug and diagnostic procurement; advising and training health personnel and community-based workers;
disease mapping; monitoring and evaluation for integrated NTD programs; and policy development.
NIH continues to be the largest funder globally of neglected disease early-stage R&D3 through the National
Institute of Allergy and Infectious Diseases and the Fogarty International Center.
CDC works to reduce the burden of NTDs through control programs, diagnostic research, capacity building in
endemic countries, progress evaluation and monitoring and identification of new tools.
DoD plays a significant role in NTD research and development for the U.S. military and is the only U.S. agency
that oversees research from basic science through product development.
It is essential that the U.S. continue its commitment to NTD control and elimination and to R&D programs across
government agencies. Investments are needed in late-stage product development to ensure that new discoveries make
it through the pipeline and become available to people who need them most. With investments like these, the U.S. can
save and improve hundreds of millions of lives and create a more economically prosperous global community.
Source: WHO 4
Global Health Briefing Book 2013 | 20
7/28/2019 GlobalHealthBriefingBook FINAL Web
23/66
Recommendations
Congress and the Administration should maintain strong funding levels for the USAID NTD Program. For
USAID to maximize the benefits of increased drug donations received from the pharmaceutical companies, the
U.S. government needs to support strong funding for this unique and successful public-private partnership.
The U.S. government should maintain U.S. leadership in NTD control and elimination by supporting thecommitments of the 2012 London Declaration on NTDs to achieve the 2020 NTD goals.
USAID should seek strategic cross-sectoral coordination of NTD treatment and control programs. The
inclusion of NTD control measures within other USAID programs or among broader U.S. government programming
will be necessary to advance NTD control and elimination goals. Opportunities for cross-sectoral coordination may
include maternal and child health services delivery platforms (e.g., childhood immunizations, vitamin supplements)
and/or water and sanitation projects.
USAID should invest in late-stage product development for NTDs. Investments are needed in R&D,
particularly late-stage product development for new technologies, in order to achieve the goals of disease control
and elimination; address the urgent needs of particularly neglected patient populations, including those suffering
from NTDs with the highest death rates and respond to the potential challenge of drug resistance. Late stage
product development efforts could be made through the USAID NTD program or other USAID programs.
The DoD, CDC and NIH should expand current investments for NTD research and development. Additional
investments in R&D will ensure the availability of new tools and treatments for people living with NTDs.
Benoit Marquet, Drugs for Neglected Diseases initiative (DNDi)
Global Health Briefing Book 2013 | 21
7/28/2019 GlobalHealthBriefingBook FINAL Web
24/66
Contributors
Global Network for Neglected Tropical Diseases, Sabine Vaccine Institute
Michelle Brooks
Drugs for Neglected Diseases initiative (DNDi)
Jennifer Katz
RTI International
Jennifer Leopold
Research!America
Jennifer Chow
1 The current WHO list of NTDs is Buruli ulcer, Chagas disease, cysticercosis, dengue, dracunculiasis, echinococcosis/hydatidosis, endemic
treponematoses, foodborne trematodiases, human African trypanosomiasis (sleeping sickness), leishmaniasis, leprosy, lymphatic filariasis,onchocerciasis, rabies, schistosomiasis, trachoma and soil-transmitted helminths. Neglected Tropical Diseases, The World Health Organization.
http://www.who.int/neglected_diseases/en/.2 Bangladesh, Benin, Burkina Faso, Cambodia, Cameroon, Democratic Republic of Congo, Ghana, Guinea, Haiti, Indonesia, Lao PDR, Mali,
Mozambique, Nepal, Niger, Nigeria, Papua New Guinea, Philippines, Senegal, Sierra Leone, South Sudan, Tanzania, Togo, Uganda and Vietnam.3 2012 G-Finder Report: Neglected Disease Research and Development: A Five Year Review, Policy Cures. http://policycures.org/downloads/
GF2012_Report.pdf.4Sustaining the drive to overcome the global impact of neglected tropical diseases: second WHO report on neglected tropical d isease, The World
Health Organization. http://www.who.int/iris/bitstream/10665/77950/1/9789241564540_eng.pdf.
.
Global Health Briefing Book 2013 | 22
mailto:[email protected]:[email protected]:[email protected]:[email protected]7/28/2019 GlobalHealthBriefingBook FINAL Web
25/66
Summary
Accounting for almost two out
of three deaths worldwide,
there is no greater threat to
human health today than non-
communicable diseases
(NCDs). The four main NCDs
cardiovascular disease, cancer,
diabetes and chronic lung
diseases are caused largely
by exposure to four risk
factors: tobacco use, harmful
use of alcohol, inactivity and
poor diet. Urbanization, climate
and environmental factors also
impact NCDs by altering risk
factors.
The U.S. government
possesses state-of-the-art
expertise and capacity to fight
NCDs globally, through
prevention, detection,
treatment, rehabilitation and
palliative care. While the U.S.government has focused on
battling NCDs domestically, it
could do much more to apply
this knowledge to improve
global health for present and
future generations.
Non-Communicable Diseases
Overview
The World Health Organization (WHO) defines NCDs primarily as
cancer, cardiovascular disease, chronic lung diseases and diabetes.1
WHO also includes disabilities, injuries and mental health disorders in
its NCD-related focus areas. Many health organizations also include
birth defects, blindness, renal diseases, Alzheimers disease, dementia
and oral diseases in the definition.
WHO reports that, as of 2008, there were 36 million deaths globally due
to NCDs six times as many deaths as HIV/AIDS, malaria and
tuberculosis combined.2 Contrary to common misconceptions, the vast
majority of NCD deaths occur in low- and middle-income countries.The
impact of NCDs is increasing rapidly and will be overwhelming in allregions by 2020 unless action is taken urgently.3 NCDs not only cause
deaths, but can cause debilitating disabilities that place significant
strains on the individual and the economy. Disabilities from NCDs
account for approximately 78.6 percent of all years lived with a
disability. For example, at current rates of increase, unipolar depressive
disorders will become one of the top three disease burdens in all
countries by 2030.
These diseases have historically been associated with aging
populations in wealthy nations, but in todays world, they are striking
men and women in their most productive years and at all income levels
especially among youth and the poorest of the poor. There is no sharpdividing line between communicable disease and NCDs; many,
including rheumatic heart disease, Burkitts Lymphoma and cervical
cancer, begin with infections from communicable diseases. These
diseases are sapping the economic strength and social capital of
societies that are major U.S. partners for trade and development. Clear
evidence exists that social determinants, including poverty, lack of
education and poor housing, contribute significantly to NCD prevalence
For two consecutive years, the World Economic Forum (WEF) ranked
NCDs as one of the greatest risks to global well-being similar to fisca
crises and global governance gaps.4 WEF projects a cumulative loss of
$47 trillion to global GDP by 2030 as a result of NCDs. NCDs are
affecting increasingly younger populations in low- and middle-income
countries, furtherthreatening education outcomes, the global economy
and productive workforce, and undermining progress toward global
poverty eradication, including the UN Millennium Development Goals
(MDGs). The U.S. is not alone in underfunding work on NCDs; less tha
1 percent of global funding for health is applied toward addressing
NCDs or risk factors.5
Jeff Meer, Public Health Institute
Global Health Briefing Book 2013 | 23
http://api.ning.com/files/XbjgHYFq2wEyG*RXaVFTcOd*XZZZlFwBTjkmtk80TxJATdmQ38QOAXj75pucCt4Nf82HpJVFlusiWO-FbuOlyrwjRVwgoLMp/NCDPhotoatUN.JPG7/28/2019 GlobalHealthBriefingBook FINAL Web
26/66
Making Progress
There has been limited progress in
combating NCDs globally. The
wealthiest countries have had small
successes in reversing NCD trends,
including the U.S., which has
reduced heart attack incidence overthe last 50 years through improved
prevention, diagnosis and treatment.
Unfortunately, these have barely
made a dent in reversing the global
trend toward increased NCD rates.
The WHO Framework Convention on
Tobacco Control represented a
major NCD victory in 2003 and now
has 168 country parties. The U.S. signed in 2004, but has not ratified the treaty. 6
The 2011 UN High-Level Meeting on NCDs was a watershed moment and only the second time that the General
Assembly has met on a health issue. Nations unanimously adopted a Political Declaration, committing to reduce
the toll of NCDs.7
In 2012, the UN agreed to an ambitious target to reduce overall deaths from NCDs by 25 percent by the
year 2025. Member States also agreed to eight additional voluntary targets and 25 indicators. The United
States was instrumental in developing this global monitoring framework.
The Rio+20 Outcome Document, "The Future We Want," recognized that sustainable development requires
reductions in NCD and communicable disease prevalence.8 Discussions support including NCDs in a post-2015
MDGs framework.
U.S. Response and Strategy
NCD prevention, diagnosis, treatment and care programs are widespread within the U.S. However, U.S. federalagencies are at the early stages of developing and resourcing NCD interventions abroad. With the U.S. lacking an
overall international policy and funding stream for NCDs, global health programs that address them tend to be
piecemeal, resulting in short-term, tangential and uncoordinated activities with modest impact. The Department of
Health and Human Services (HHS) has demonstrated the most robust work in this area and recently released a global
strategy that includes NCDs. In addition to its leadership in global policy development, HHS efforts include Centers for
Disease Control and Prevention and National Institutes for Health research; surveillance and training programs,
exemplified by the chronic disease Centers of Excellence initiative; and the Global Youth Tobacco Survey.
The State Department has utilized public-private partnerships to drive its engagement in global NCDs. In 2011, the
Office of the Global AIDS Coordinator (along with other partners) announced the Pink Ribbon Red Ribbon Initiative, 9
which leverages the Presidents Emergency Plan for AIDS Relief (PEPFAR) platform to expand screening and
treatment for cervical cancer and promote breast cancer education. However, there has been little discussion as towhether PEPFAR could be similarly expanded for other NCDs. Additionally, the State Departments Global Partnership
Initiative helped launch the Global Alliance for Clean Cookstoves,10 which works to reduce the indoor air pollution and
resulting NCDs caused by cooking with biofuels in developing countries.
USAID targets NCDs through a small number of country programs and some grants addressing cancer and diabetes.
As of 2000, USAID ceased support for tobacco production and committed to identifying alternative cash crops for
economic development. Its new Office of Health Systems is positioned to encourage the integration of NCD
interventions as part of country-based health programs.
Source: WHO
Global Health Briefing Book 2013 | 24
7/28/2019 GlobalHealthBriefingBook FINAL Web
27/66
Recommendations
The Administration should reaffirm its policy commitments to NCDs and integrate NCD prevention, diagnosis
and treatment with existing international development programs such as the Global Health Initiative, PEPFAR,
Feed the Future and the Global Climate Change Initiative.
USAIDs new Office of Health Systems should develop guidance for integrating NCD interventions intoexisting country programs. USAID should adopt a widespread policy, that acknowledges the intersection of the
global NCD burden with key development priorities, including agriculture, gender equality and economic growth.
Likewise, the State Department Office of Global Health Diplomacy and Office of Global Womens Issues should
include NCDs in their programs and messaging.
The Administration should emphasize a whole of government approach to NCD prevention, diagnosis,
treatment, care and rehabilitation to ensure multisector coordination and supportive social or economic policies.
The President should seek Senate consent to ratifythe WHO Framework Convention on Tobacco Control.
The Administration should continue to support innovation for NCDs worldwide, by leading the creation,
testing and broad dissemination of global health technologies.
In intergovernmental negotiations, the Administration should champion NCD prevention, diagnosis and
treatment. The Administration should deliver on NCD-related pledges, and encourage other nations to do so. The
U.S. government should support nutritional science and consumerbehavior research11 and promote reduced
consumption of foods high in sugar and fat in an effort to produce a culture of wellness and healthy eating.
Programs that emphasize appropriate physical exercise at all ages are cost-effective. The U.S. should also
facilitate the availability of essential medicines for NCDs globally.
U.S. representatives at the UN should ensure the post-2015 MDG agenda includes NCDs within the context
of health, as well recognizing the link between NCDs and human development generally. U.S. government
negotiators should lead global NCD policy dialogue, including within the WHO NCD Action Plan and NCD
accountability mechanism. The Administration should also advocate for gender- and age-disaggregated NCD data
collection in global health programs to ensure the needs of children, adolescents, adults and the elderly are allconsidered. The Administration should share U.S. successes on NCDs with other governments, including in health
systems strengthening. Federal agencies should convene global multistakeholder partnerships and in-country
interagency collaborations on NCDs, excluding entirely the tobacco industry, to address social determinants of
health that affect NCDs.
...the global burden of NCDs constitutes one of the major challenges for
development in the twenty-first century...UN Political Declaration on NCDs
September 2011
Global Health Briefing Book 2013 | 25
7/28/2019 GlobalHealthBriefingBook FINAL Web
28/66
Contributors
Public Health Institute
Jeffrey Meer, lead author
Advancing SynergyArti Varanasi
Arogya World
Nalini Saligram
LIVESTRONG Foundation
Loyce Pace Bass
With additional input and support from members of the NCD Roundtable and its co-chairs, Medtronic, Inc. and the
Public Health Institute.
www.ncdroundtable.org
1 Global Status Report on Non-Communicable Diseases, World Health Organization. 2010. http://www.who.int/nmh/publications/ncd_report_full_en.pdf.2Global Burden of Disease Study 2010, The Lancet. December 13, 2012. http://www.thelancet.com/themed/global-burden-of-disease.3Mathers C.D., Loncar D. Projections of Global Mortality and Burden of Disease from 2002 to 2030, PLoS Med, 2006. Pg. 3(11). 4Global Risks 2010: A Global Risk Network Report, World Economic Forum. http://www3.weforum.org/docs/WEF_GlobalRisks_Report_2010.pdf.5Where have all the donors gone? Scarce donor funding for Non-Communicable Diseases, Center for Global Development. http://www.cgdev.org/files/1424546_file_Nugent_Feigl_NCD_FINAL.pdf.6The WHO Framework Convention on Tobacco Control, World Health Organization.http://www.who.int/fctc/about/en/index.html.7Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases, UnitedNations. http://www.un.org/ga/search/view_doc.asp?symbol=A/66/L.1&referer=http://www.un.org/en/ga/ncdmeeting2011/&Lang=E.8The Future We Want, Outcome Document from the UN Conference on Sustainable Development.http://sustainabledevelopment.un.org/futurewewant.html.9Pink Ribbon Red Ribbon Overview, U.S. Department of State. http://www.state.gov/r/pa/prs/ps/2011/09/172244.htm.10The Cookstove Story, Global Alliance for Clean Cookstoves. http://www.cleancookstoves.org/.11Communication Strategies to Help Reduce the Prevalence of Non-Communicable Diseases, Nutrition Reviews. http://www.foodinsight.org/LinkClick.aspx?fileticket=p5w1hnTGPbQ%3d&tabid=1440.
Global Health Briefing Book 2013 | 26
7/28/2019 GlobalHealthBriefingBook FINAL Web
29/66
Summary
Every day, 19,000 children die
from preventable diseases and
conditions such as pneumonia,
diarrhea, malaria, measles and
polio.1
Since 1990, U.S. investments
have contributed to a 40
percent decline in maternal and
child deaths.
In June 2012, the United States
committed to endingpreventable child deaths within
a generation and improving
maternal health. Continuing U.S.
efforts to address the leading
causes of maternal and child
mortality and morbidity will
dramatically accelerate progress
toward this ambitious goal.
Maternal and Child Health
OverviewSignificant progress has been made in improving maternal and child
health in recent years, in part due to increased U.S. leadership and
support. In 2011, fewer than 7 million children died before their fifth
birthday, compared to around 12 million in 1990.
From 1990 to 2010, the annual number of maternal deaths dropped 47
percent from more than 543,000 to 287,000.2
A quarter of a million women die each year during pregnancy and
childbirth from preventable causes such as hemorrhages, infections
and high blood pressure. Ninety-nine percent of these deaths occur in
resource-limited settings where women lack access to basic nutrition
and health care. Care from a skilled health worker before, during andafter childbirth can save the lives of women and newborn babies. 3
Of all childhood deaths, approximately 40 percent occur within the first
month of life. Preterm birth is the leading cause of neonatal mortality
with over one million newborn babies dying each year because they
were born too early.4
For children under the age of 5, pneumonia and diarrheal diseases are
the leading killers, together claiming the lives of 2 million children each
year.5
By 2015, it is estimated that more than 2 million child deaths
could be averted if the utilization of key cost-effective interventions for
pneumonia and diarrhea are available to the poorest populations in
countries with the highest mortality rates.
Vaccines save 2.5 million young lives each year,6
and are among the
most cost-effective health interventions, with an economic return of 18-
30 percent.7
The interventions that prevent childhood diseases, such as
immunization, access to safe water, sanitation and adequate nutrition,
are best provided as a package of services in order to achieve optimal
outcomes.8
Continued U.S. support and leadership amongst bilateral and
multilateral stakeholders are critical to creating a cohesive approach to
maternal and child health.
Gabe Bienczycki, PATH
Global Health Briefing Book 2013 | 27
7/28/2019 GlobalHealthBriefingBook FINAL Web
30/66
Making Progress
The longstanding investments by the U.S. government in child and maternal health, though modest, have proven
highly successful. Roughly 6 million children each year are saved by U.S.-funded treatments, preventions
and nutrition programs.9
In the 19 countries where U.S. involvement has been the greatest, maternal mortality has declined by 30
percent in the last 20 years.10
In 2012, the United States, along with Ethiopia and India, led the way for a global pledge, the Child Survival Call to
Action, to end preventable child death within a generation and improve maternal health. Significant investments
are needed to meet this commitment.
U.S. Response and StrategyU.S. support for maternal and child health is provided through bilateral USAID assistance and partially through the
Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH). USAID supports
programs that care for women before, during and after labor; provide prevention and treatment of severe diseases and
infections for children and newborns and promote routine immunization. Additionally, USAID has a long history of
investing in training and support for the frontline health workers, including midwives and community health workers,
who can properly manage pregnancy, delivery and complications for women and newborns; and in research and the
development of products to address health challenges impacting women and children, such as vaccines, nutrition
strategies and oral rehydration therapy to treat diarrheal disease. The CDC provides scientific and technical assistance
to strengthen health systems, including the health workforce, and is involved in immunization programs, while the NIH
supports basic and applied research for maternal and child health.
The U.S. also partners with multilateral organizations, providing additional support for vaccines and immunizationsthrough funding to UNICEF and the Global Alliance for Vaccines and Immunizations (GAVI), a public-private global
health partnership focused on increasing access to new and underutilized vaccines and immunizations within poor
countries. GAVI enables countries to take ownership over their immunization programs by requiring that country
ministries and the private sector work together to fund, in part, and implement these programs. With GAVIs support,
over 370 million children have been immunized. In 2011, the U.S. government made a three-year, $450 million
commitment to support the GAVI Alliance and its programs. In the final year, $175 million is required to meet the
commitment in FY2014.
Global Health Briefing Book 2013 | 28
Source: Making Sense of the Alphabet Soup for Maternal and Child Health Programs at USAID.
http://www.slideshare.net/COREGroup1/usaids-mch-portfoliojohn-borrazzo101411
7/28/2019 GlobalHealthBriefingBook FINAL Web
31/66
Recommendations
The U.S. government must follow through on its commitment to end preventable child death in a
generation and improve maternal health with financial and technical assistance. In order to reach this
ambitious goal, developing countries that have joined the Child Survival Call to Action will need to build health
programs and systems, including a skilled, equipped and supported health workforce, that reach the poorest and
most vulnerable communities. Many developing countries, including India and Ethiopia, are committed to achieving
the goal, but they cannot get there without long-term technical and financial assistance from the U.S. and other
donor nations. As a leading donor for child and maternal health, the U.S. should encourage more financial and
political support from multi- and bilateral organizations, as well as the public and private sectors.
Congress should maintain and increase support for overall maternal and child health programs by
appropriating $750 million in FY2014 to follow through on its commitments. This funding amount includes
$175 million to fulfill the U.S. pledge to the GAVI and provides critical complementary core services to women and
children.
The U.S. government should promote rapid scale-up of proven interventions and health services access
for rural, poor and underserved populations. Supporting programs that address disparities within countries as
well as among them will help achieve reductions in maternal and child mortality. Pregnant women should haveaccess to affordable medicines and skilled birth attendants that keep them safe during pregnancy and child birth,
no matter where they live.
Congress should support and provide flexible funding for disease-focused initiatives, to promote
intersections with maternal and child health. These programs include the Presidents Emergency Plan for AIDS
Relief (PEPFAR), the Presidents Malaria Initiative (PMI) and the Global Fund to Fight AIDS, Tuberculosis and
Malaria.
The U.S. government should invest in research and development of critical tools, such as vaccines, and
other essential health supplies for women and children. Many diseases that affect women and children will not
be completely eradicated with currently available tools. In addition to scaling up current interventions, additional
R&D is urgently needed to improve the health of women and children around the world.
Global Health Briefing Book 2013 | 29
Source: PATH
7/28/2019 GlobalHealthBriefingBook FINAL Web
32/66
Contributors
PATHHeather [email protected]
Save the ChildrenSmita [email protected]
U.S. Fund for UNICEFMark [email protected]
1Levels and Trends in Child Mortality, UNICEF, 2012.2 Trends in Maternal Mortality: 1990 2010, WHO, UNICEF, UNFPA, The World Bank, 2010.3 Factsheet on Maternal Mortality, WHO. http://www.who.int/mediacentre/factsheets/fs348/en/index.html.4 Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000, The Lancet. http://www.sciencedirect.com/science/article/pii/S0140673612605601.5Pneumonia and Diarrhea: Tackling the deadliest diseases for the worlds poorest children, UNICEF, 2012.6
State of the worlds vaccines and immunization, WHO, UNICEF, World Bank, 2009.7 Bloom, David E., Canning, David, and Weston, Mark. The Value of Vaccination, World Economics, July-September, 2005. Pg. 15-39.8Pneumonia and Diarrhea: Tackling the deadliest diseases for the worlds poorest children, UNICEF, 2012.9 Maternal and Child Health, USAID. http://www.usaid.gov/what-we-do/global-health/maternal-and-child-health.10USAID Contributions to Maternal and Child Health, USAID. http://transition.usaid.gov/press/factsheets/2011/fs110503.html.
Global Health Briefing Book 2013 | 30
7/28/2019 GlobalHealthBriefingBook FINAL Web
33/66
Summary
Undernutrition contributes to
the preventable deaths of
millions of mothers and
children under the age of 5
each year and results in lost
economic productivity and an
increased health burden.
The U.S. is committed to
improving nutrition for mothers
and children around the world
and scaling up proven, cost-effective solutions.
The linkages between nutrition;
health; agriculture; water,
sanitation and hygiene
(WASH); and other sectors of
development should be
leveraged in order to better
coordinate and integrate policy
and program implementation to
achieve significant reductions
in child deaths and stunting.
Nutrition
Overview
Undernutrition is one of the worlds most serious yet least addressed
development challenges, which contributes to the preventable deaths
of millions of mothers and children under the age of 5 each year. It
stunts the cognitive and physical development of millions more
children and results in lost economic productivity and an increased
health burden on already poor countries.
The 1,000 day window between a womans pregnancy and her childs
second birthday are critical to long-term human development and
economic growth. The right nutrition during this time produces a
lifetime of benefits: healthy growth and brain development, a strong
immune system, higher IQ, better educational performance and
greater lifetime earning potential.
While significant progress has been made in reducing deaths in
children under the age of 5, 6.9 million children annually about
19,000 each day still die from largely preventable deaths.
Undernutrition is the underlying cause of more than one-third, or 2.5
million, of these deaths.1
Around the world, some 165 million children are stunted due to chronic
undernutrition.2 Chronic undernutrition also leads to increased
susceptibility to infections and illnesses, such as diarrhea and
pneumonia; magnifies the impact of diseases such as HIV/AIDS and
malaria, and compromises the absorption and effectiveness of life-saving medicines. Better nutrition during the 1,000 day window can
result in a savings of about $20-30 billion annually in health costs. 3
The lack of key micronutrients and stunting in girls contributes to
complications later in life, such as obstructed labor, obstetric fistula
a preventable childbirth injury4 and even maternal death.
Undernutrition and stunting are serious drains on economic
productivity, costing countries as much as 11 percent of their GDP. 5
The right nutrition during childhood can increase individual earnings
over a lifetime by up to 46 percent.6
In the 2012 Copenhagen Consensus report, an expert panel ofeconomists concluded that fighting undernutrition in young children
should be a priority investment for policymakers. Every $1 invested in
nutrition generates as much as $138 in better health and increased
productivity.7
Without urgent action to improve nutrition, progress on disease
prevention and treatment and hunger and poverty alleviation will be
harder and costlier to achieve.
John Isaac, UN Photo
Global Health Briefing Book 2013 | 31
7/28/2019 GlobalHealthBriefingBook FINAL Web
34/66
Making Progress
In 2008, the medical journal TheLancetpublished a series on maternal and child undernutrition, highlighting the
impact on the critical 1,000 day window and recommending a set of evidence-based interventions.8
During the last two decades, collaborative efforts at all levels and across sectors have resulted in reducing the
deaths of children under age 5 from around 12 million in 1990 to about 6.9 million in 2011.9
U.S. leadershipon the inclusion of nutrition as a solution to ending child mortality has been vital.
The number of stunted children dropped by 35 percent, from 253 million in 1990 to 165 million children in
2011.10 However, overall progress is still insufficient and millions of children remain at risk.
U.S. Response and Strategy
In 2010, U.S. leadership led to the launch of the 1,000 Days Call to Action 11 and the Scaling Up Nutrition (SUN)12
movement to highlight the critical window of opportunity on nutrition and to support national leadership and collective
action to scale up nutrition. With the 1,000 Days Call to Action, the U.S. has highlighted the period between a womans
pregnancy and her childs second birthday as a critical window of opportunity to maximize investments and address
fundamental health and development challenges. SUN is a country-led movement with support and engagement by
donors, national governments, foundations, civil society and the private sector to increase the effectiveness of existingprograms, align resources and foster long-term commitment to nutrition. It now includes 33 countries committed to
advancing health and development through improved nutrition.
Current U.S. food security and global health initiatives include nutrition as a cross-cutting issue and efforts are
underway within USAIDs Feed the Future initiative to align metrics and indicators to measure nutritional outcomes and
impact across various U.S.-funded programs.
Dominic Sansoni, World Bank
Global Health Briefing Book 2013 | 32
7/28/2019 GlobalHealthBriefingBook FINAL Web
35/66
Recommendations
Continued U.S. leadership at all levels, including through SUN, is vital in harnessing the power of collaborative action
to combat maternal and child undernutrition. Increased and targeted investments are essential to scaling up evidence-
based, cost-effective nutrition interventions and leveraging investments in other areas to achieve significant and
sustainable reductions in maternal and child undernutrition rates. Bipartisan support is needed to reverse decades of
underinvestment in nutrition and enshrine it as a core development priority.
The U.S. government should continue and strengthen its leadership at the global level to increase
nutrition investments within overall health, food security, agriculture, education and WASH assistance. This
includes supporting country-owned strategies and plans to scale up nutrition investments through SUN.
Congress should maintain and increase U.S. government support for nutritionprograms and initiatives.
The Administration should establish nutrition as a core component of U.S. development priorities and
launch a whole of government nutrition strategy that outlines how the U.S. will address and implement maternal
and child nutrition programs, with a particular focus on the critical 1,000 day window.
The Administration should utilize linkages between nutrition, agriculture, health, WASH and other sectors
of development in order to better coordinate and integrate policy and program implementation to achieve
significant reductions in child deaths and stunting.
TheAdministration should publish a more detailed U.S. nutrition budget across relevant initiatives and
accounts to ensure that investments across sectors are leveraged to improve nutritional outcomes.
Global Health Briefing Book 2013 | 33
7/28/2019 GlobalHealthBriefingBook FINAL Web
36/66
Contributors
1,000 Days Partnership
Mannik Sakayan
Save the Children USA
Smita Baruah
Bread for the World Institute
Asma Lateef
1 Committing to Child Survival: A Promise Renewed-Progress Report 2012, UNICEF. http://www.apromiserenewed.org/files/APR_Progress_Report_2012_final_web.pdf.2 Ibid.3 State of Food Insecurity in the World, FAO. 2004.4 Facts and Frequently Asked Questions about Fistula, Fistula Foundation. http://www.fistulafoundation.org/whatisfistula/faqs.html.5 Black, R.E., L.H. Allen et al., Maternal and Child undernutrition - global and regional exposures and health consequences, The Lancet, 2008, vol.371.6Hoddinott, J. et al., Effect of a nutrition intervention during early childhood on economic productivity in Guatemalan adults, The Lancet, 2008, vol.371.7 Hoddinott, Rosegrant and Torero, Copenhagen Consensus Challenge Paper, Copenhagen Consensus 2012.8 Maternal and Child undernutrition - global and regional exposures and health consequences, supra.9 Committing to Child Survival, supra.10 UNICEF-WHO World Bank Joint Child Malnutrition Estimates, United Nations Childrens Fund, World Health Organization, The WorldBank. 2012.11 1,000 Days. http://www.thousanddays.org/.12 Scaling Up Nutrition. http://scalingupnutrition.org/.
Global Health Briefing Book 2013 | 34
7/28/2019 GlobalHealthBriefingBook FINAL Web
37/66
Summary
Since 1965, the U.S. has been a
global leader in improving
access to voluntary family
planning services and
information in the poorest
countries. There has been
bipartisan support for the
international family planning
and reproductive health
programs lifesaving and cost-
effective efforts. Providing
women with access to
reproductive health services,
including a wide range of
voluntary contraceptive
options to determine the
number, timing and spacing of
their pregnancies, will reduce
the incidence of unsafe
abortion; improve maternal and
child health; reduce unintended
pregnancies and maternal
deaths; lower HIV infectionrates; promote womens
empowerment; enhance
womens and girls education;
and raise standards of living.
Family Planning and Reproductive Health
Overview
An estimated 222 million women in developing countries want to delay
or avoid pregnancy, but face barriers or lack access to effective family
planning information and services.1
In 2012, an estimated 291,000 women in developing countries died
from pregnancy-related causes, including unsafe abortions.2 In fact,
pregnancy related complications are the leading cause of death in the
developing world for young women 15-19 years old.
Investments in family planning and reproductive health (FP/RH) are
integral to the future progress of U.S. global health programs, as well
as important initiatives to combat HIV/AIDS and improve maternal,
newborn and child health.
For example, robust dual investment in maternal, newborn and
child health and family planning is one of the most cost-effective
strategies and saves more lives than either intervention alone.
Providing both sets of services to women would lead to a 70
percent decline in maternal deaths, compared to a 57 percent
decline if countries only invested in maternal and newborn care;
newborn deaths would decline by 44 percent, compared to a 39
percent decrease with investments in maternal