Embed Size (px)
Citation preview
GI diseases II. Tomas Koller, MD. PhD. Assoc. Prof.
Acute diarrhea
Acute diarrhea Definition
>3x/day, >300 g/day
<2 weeks, mostly<1 week
Abrupt onset
Mostly infectious origin
Does not relapse
Acute diarrhea
• Dysenteric syndrome
• Content of pus and blood separated from the stool
• Tenesms (pianful urgency)
• Balloning
• Distal colon
Acute diarrhea Causes
• Toxins from bacteria
• Incubation short (hours)
• Staphylococcus aureus
• Bacillus cereus
• Clostridium perfringens
• Infection
• Incubation <24h
• Viruses
• Salmonella
• Campylobacter
• E.Coli enterohemorhagic
• Yersinia enterocolitica
• Giardia intestinalis
Acute diarrhea Diagnosis
• Diagnosis is clinical
• Evaluate for hypovolemia
• BP<90 mmHg, pulse<120/min
• Oliguria
• Capullary refill tie >3s
• Cold and pale extremities
• Marble skin
• Hypokaliemia
• Abdominal palpation
• Sensibility diffuse due to air
Acute diarrhea Diagnostic workup
• Not indicated unless:
• Blood in the stool, dysenteric syndrome = organic origin
• Signs of sepsis (>39˚C), septic shock, hypothermia
• Severe dehydration
• Cardiac valve disease, elderly, comorbid
• Persisting diarrhea > 3 days
• Full blood count, CRP, stool culture focused on Salmonella, Shigella, Campylobacter, Yersinia, E.Coli 0157
• Dehydration , Na, K , Cl
• Blood in the stool > 4 days, sigmoidoscopy
• Sepsis - hemoculture
Acute diarrhea Therapy
• Symptomatic
• Rehydration
• Correction of electrolytes
• Spontaneous evolution is favorable
• < 5 days
• In patients with sepsis, or risk factors and severe condition
• Bacterial or parasitic agent is identified
• Antibiotics could be prescribed for Campylobacter, Yersinia
• Ciprofloxacin 2x500 mg 3-5 days
• Macrolides (Camppylbacter)
• Antiparasitic drug for Amoeba, Gardia
• Metronidazol
Nosocomial acute diarrhea
• Risk factors
• antibiotics,
• age,
• time in the hospital,
• source of infection in the proximity
• Clostriudium difficile
• Giardia
• Multiresistant microbes
• Klebsiella
• Enterococci
Travellers diarrhea
• During travel or after returning from a trip
• Dysbiosis (loose stools) is frequent, short and benign
• Higher probability of parasitic infection
• Amoeba
• Depending on the country
Acute diarrhea post-antibiotic
• 10% of patients receiving antibiotics have some transit modification
• Usually bening diarrhea after 3-5 days
• No fever, spontaneously terminates
• No therapy
• 10% of post antibiotic diarrhea
• Clostriudiumm difficile (pseudomembranous colitis)
• Klebsiella oxytoca (bloody diarrhea)
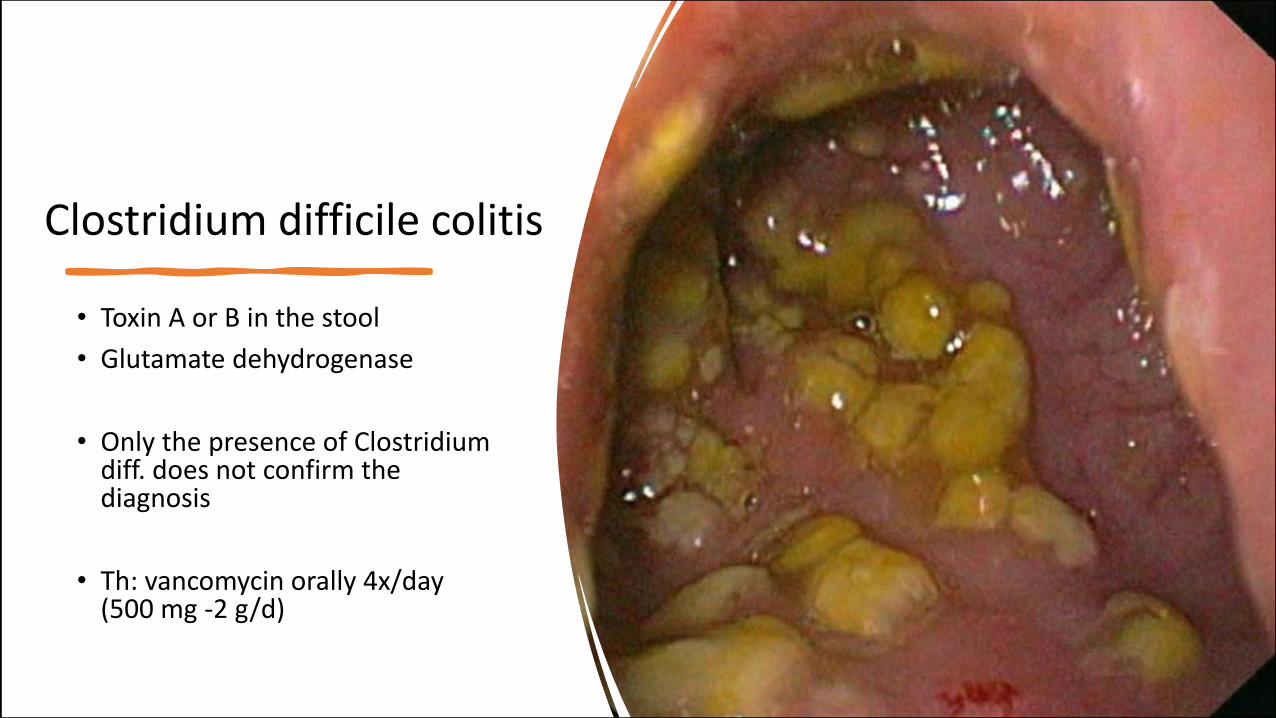
• Toxin A or B in the stool
• Glutamate dehydrogenase
• Only the presence of Clostridium diff. does not confirm the diagnosis
• Th: vancomycin orally 4x/day (500 mg -2 g/d)
Clostridium difficile colitis
Chronic diarrhea
Chronic diarrhoe
Definition • >3 stools / day
• > 4 weeks
• Rectal syndrome • Frequent urgency for passing stool
• Non-fecal content (bloody, mucus)
• Sign of organic rectal disease • Cancer
• Inflammation
To be differentiated from
• Fecal incontinence
• False diarrhea of constipation • Exsudation of the mucosa in contact with
hard stool, explosive evaluation, liquid with some small parts of hard stool
Mechanisms and causes of chronic diarrhea
Motoric
Osmotic
Malabsorbtion
Secretory
Exsudative and inflammatory
Mechanisms and causes of chronic diarrhea
Motoric d. • No gut anatomic lesion
• Morning and after meals
• In groups
• Accelerated transit time
• Irritable bowel (IBS-D)
• Autonomic neuropathy • Hyperthyroidism • Endocrine tumors
• VIP, medullary thyroid cancer
Mechanisms and causes of chronic diarrhea
Osmotic d. • No gut anatomic lesion
• Liquid stool • Lactose intolerance
• Magnesium
• Laxative use
• Ingestion of polyols
Malabsorption d.
Mechanisms and causes of chronic diarrhea
• Celiac disease • Crohn’s disease of small bowel • Postradiation enteritis
• Intestinal resection
• Exocrine pancreatic insufficiency
• Short bowel syndrome
• Lymphoma
• Chronic bowel ischemia • Posprandial pain
• Small intestinal bacterial overgrowth
• Whipple disease
Secretory d. • Liquid, hypovolemia, hypokaliemia
• Colitis • Microscopic colitis
• Lymphocytic, colagenous
• Infection in immunocompromised • Giardia intestinalis • Cryptosporidium • Isospora belli
• Neuroendocrine tumors (gastrinoma, VIPoma)
• Mastocytosis
Mechanisms and causes of chronic diarrhea
Exsudative d. • ulcers on the GI mucosa
• exsudation of blood, lymph, proteins
• IBD • Crohn’s disease • Ulcerative colitis
• Lymphoma
• Lymphangiectasia
• Malignant compression of lymph ducts
Mechanisms and causes of chronic diarrhea
Investigations for chronic diarrhea
Clinical and laboratory
• History • Timeline and trendline
• Physical examination • Herpetiform dermatitis • Goiter • Nails and hair abnormalities • Lymphadenoapthy • Hypotension • Flush
Laboratory exams • Blood
• Electrolytes • B12, folate • IgA anti-transglutaminase Ab • ASCA, pANCA antibodies • TSH • Chromogranin • Gastrin
• Stool • ova and parasites • elastase • calprotectin

Investigations for chronic diarrhea
Endoscopy
• Colonoscopy
• Enteroscopy
• Capsule enteroscopy
• EUS
• Upper GI endoscopy
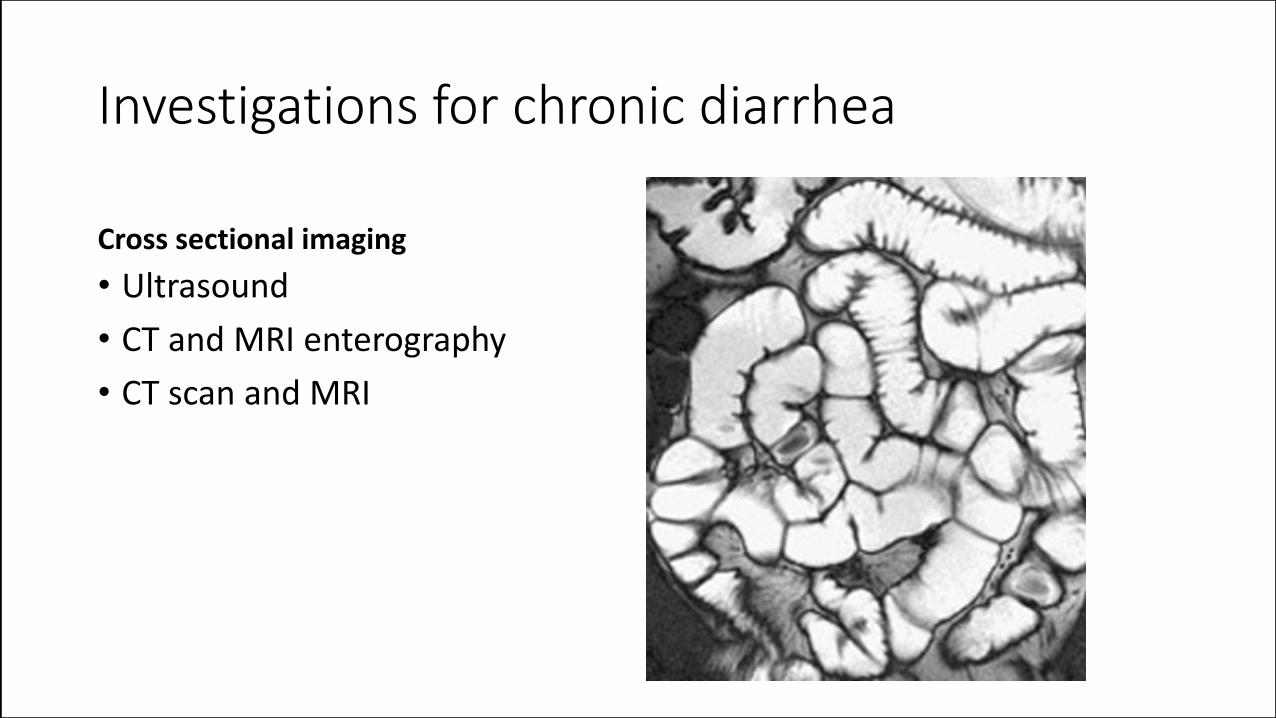
Investigations for chronic diarrhea
Cross sectional imaging
• Ultrasound
• CT and MRI enterography
• CT scan and MRI
Constipation
Constipation
• Definition 1. Less than 3 stools per week 2. Sensation of incomplete evacuation 3. Both 1. and 3.
• A. Habitual • Occasional • Pregnancy and lactation • Travel
• B. Secondary - organic
• C. Idiopathic - functional • Slow transit • Dyschesia
• difficulties in stool evacuation
False diarrhea of constipation
• Fecalome in rectum • False diarrhea
• Frequent passage of liquid stools or mucus
• Risk factors • Chronic constipation
• Elderly
• Use of opiates
• Immobilisation
• Diagnosis • Digital rectal examination
B. Secondary constipation
Causes of secondary constipation • Colonic or anal stenosis
• Colic or extra-colic cancer • Post-colitis stenosis
• IBD, NSAID, Radiation, Diverticulitis, Volvulus
• Pelvic floor abnormalities • Rectocele
• Systemic disease • Neurological (Parkinson, CVA, SM) • Metabolic (DM, low thyroid, SS, low Ca, Mg)
• Drugs • Antidepressants, opiates….
Causes of functional consipation
• Slow transit
• Idiopathic (IBS-C)
• Pelvic floor dysfunction • Static or dynamic
C. Idiopathic “functional” constipation
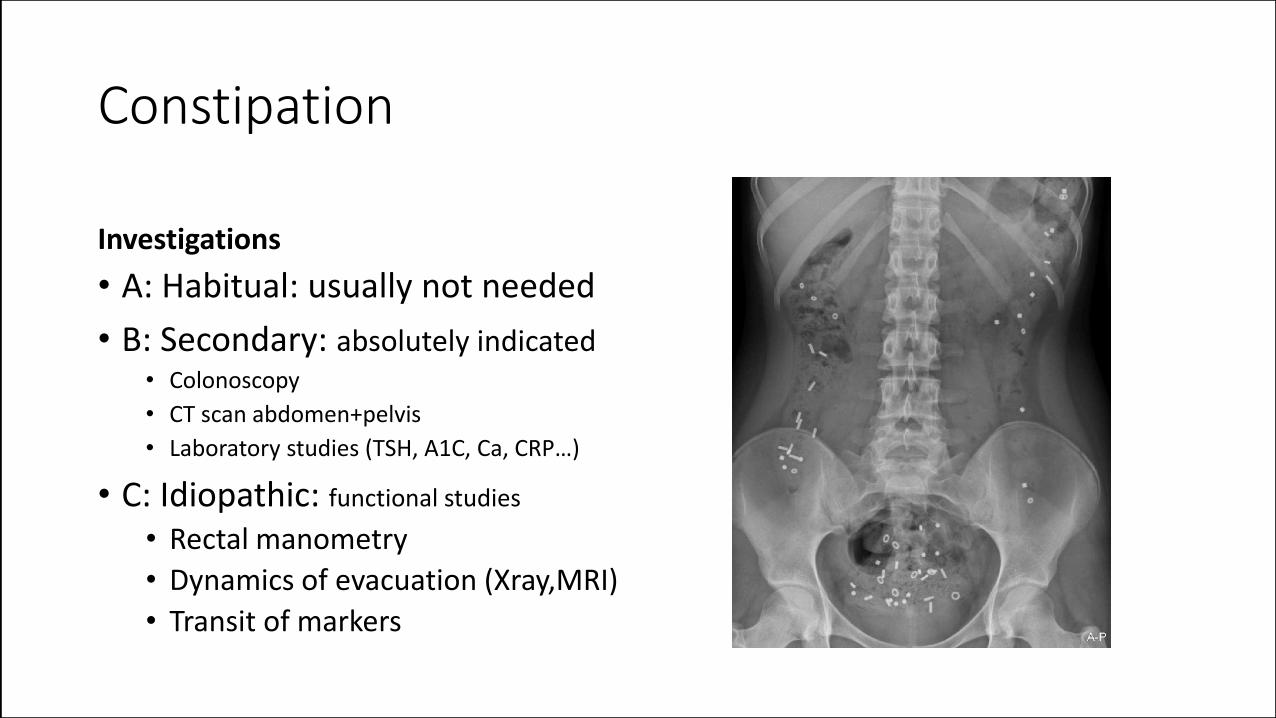
Constipation
Investigations
• A: Habitual: usually not needed
• B: Secondary: absolutely indicated • Colonoscopy
• CT scan abdomen+pelvis
• Laboratory studies (TSH, A1C, Ca, CRP…)
• C: Idiopathic: functional studies
• Rectal manometry
• Dynamics of evacuation (Xray,MRI)
• Transit of markers
Constipation Management
Osmotic laxatives
• Lactulose
• Macrogol
• Magnesium
Therapy
• A: Habitual • Fiber 15g/day • Physical activity • Hydration
• B: Secondary • Treatment of the cause
• C: Idiopathic • Laxatives (osmotic) • Behavioral therapy • Pelvic floor surgery

Diverticulosis
Diverticulosis
• Diverticuli of the colonic wall • Frequent
• Age related
• Mainly left colon
• Usually asymptomatic • Symptomatic diverticulosis ?
• Complications • Bleeding
• Diverticulitis
• Bowel perforation

Diverticulosis Complications
Acute diverticulitis • Acute inflammation of the bowel wall –
sigmoiditis
• Clinical • Left lower quadrant or epigastric pain • Constipation • Bowel stenosis • Fever
• Investiation • Ultrasound, CT scan, blood tests (Leu, CRP)
• Treatment • Rehydration • +/- antibiotics
Diverticulosis Complications
Acute diverticular bleeding • Severe arterial lower GI bleeding
• Risk factors • Anticoagulants and antiaggregants • Comorbidity
• Chronic renal or cardiac disease
• Clinical • Enterorhagia • Hypotension, tachycardia
• Investigations • Blood count
• Treatment • Correction of volume • Preparation for colonoscopy – macrogol orally
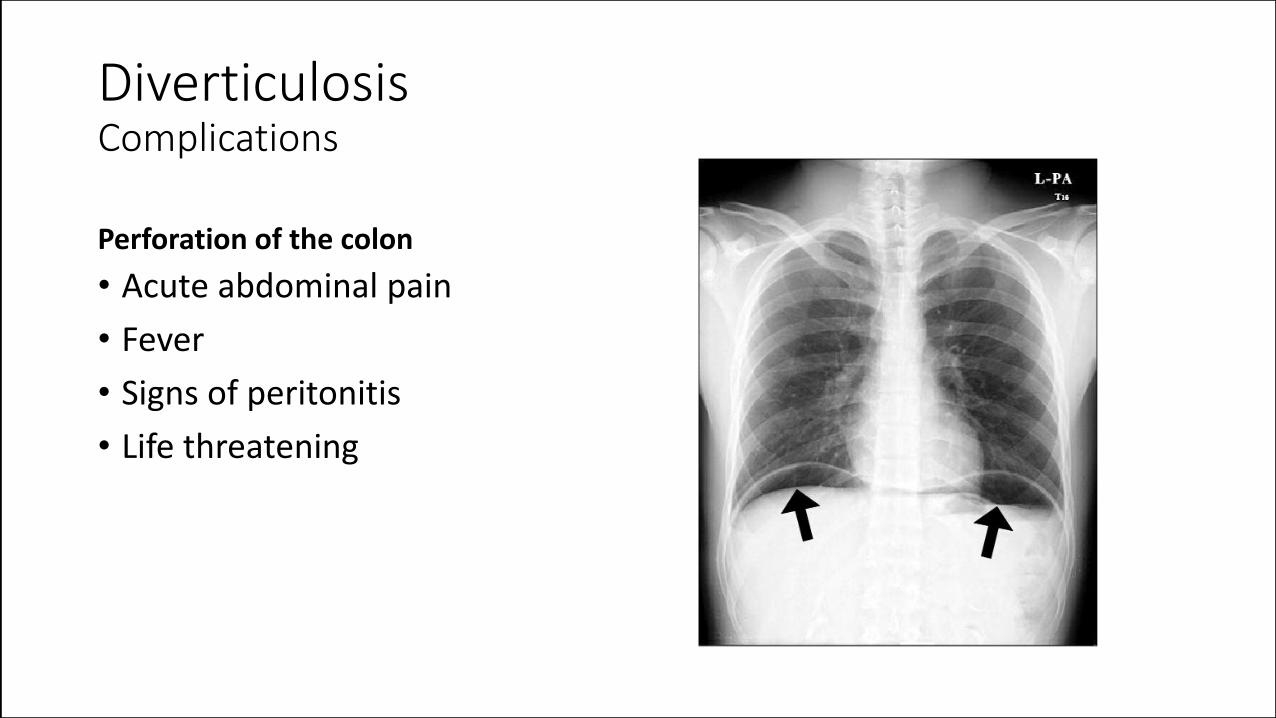
Diverticulosis Complications
Perforation of the colon
• Acute abdominal pain
• Fever
• Signs of peritonitis
• Life threatening
FUNCTIONAL GI DISORDERS
Dyspepsia
DISCOMFORT OR PAIN FOLLOWING A MEAL OR DURING DIGESTION
ABNORMAL SENSATION FROM THE DIGESTIVE TRACT (MAŘATKA)
😕
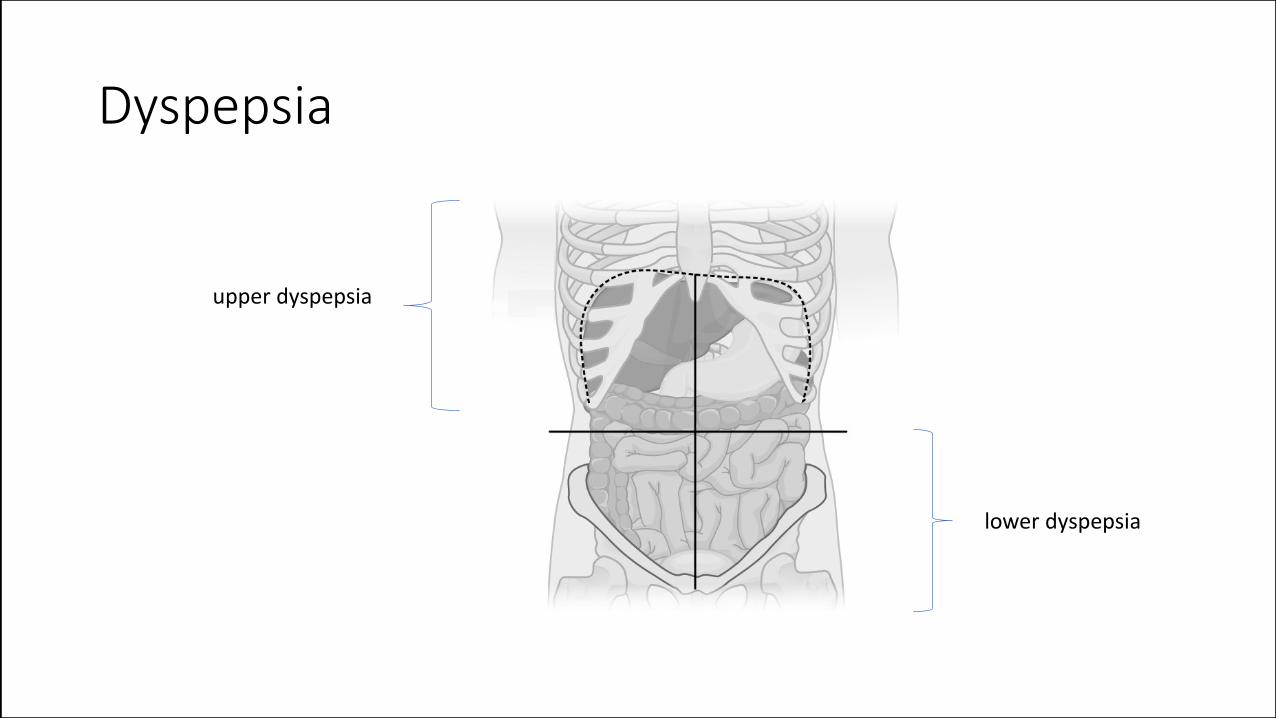
Dyspepsia
upper dyspepsia
lower dyspepsia
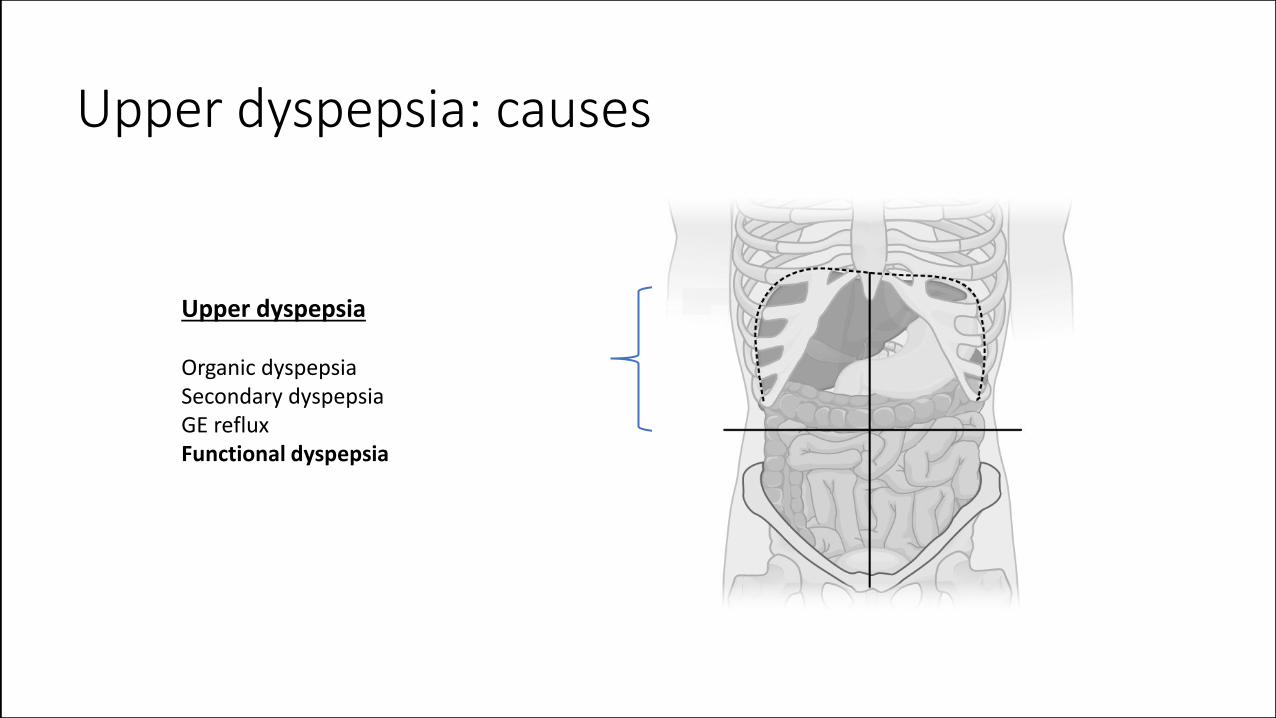
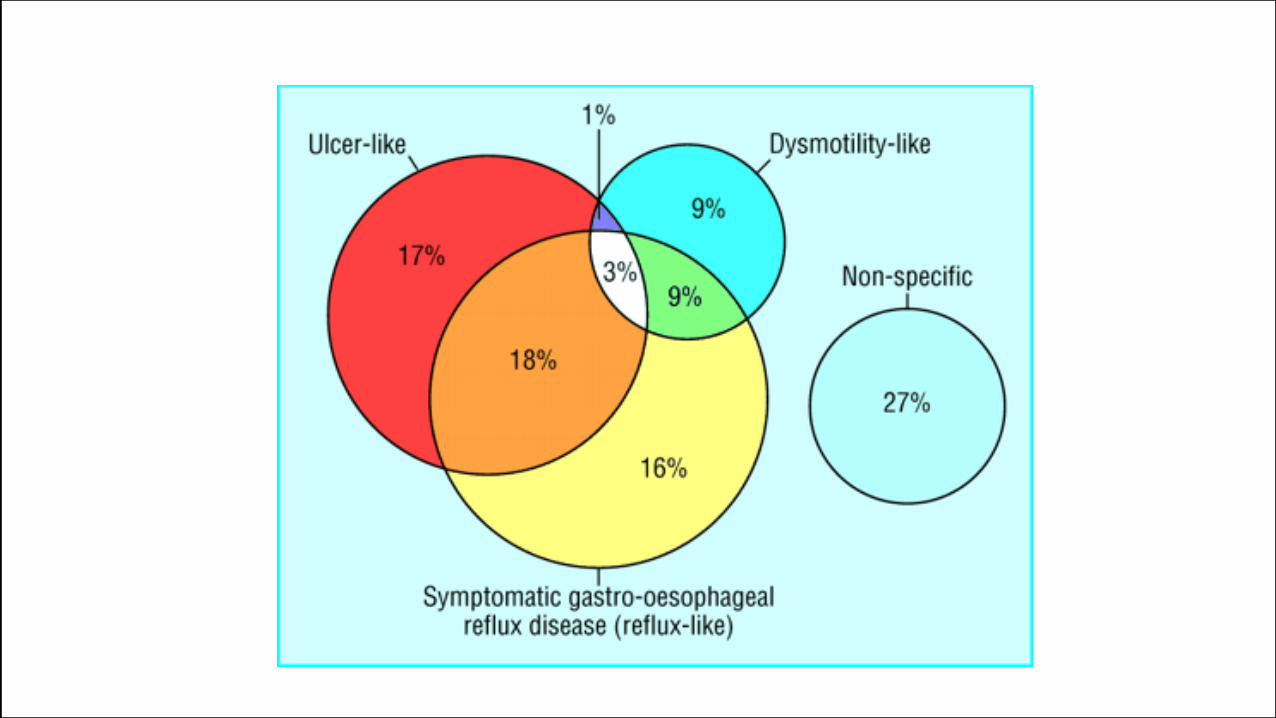
Upper dyspepsia: causes
Upper dyspepsia Organic dyspepsia Secondary dyspepsia GE reflux Functional dyspepsia
Functional dyspepsia Rome IV criteria
1. Epigastric pain syndrome Ulcer-like dyspepsia
Pain or epigastric burn
2. Postprandial distress syndrome Dysmotility-like dyspepsia
Postprandial fullness
Early satiety
Dyspepsia Investigations
Necessary Alarm symptoms
• Age above 55, new onset dyspepsia
• Family history of upper gi cancer
• Weight loss – unwanted
• GE bleeding
• Dysphagia
• Odynophagia
• Unexplained iron def. anemia
• Vomiting
• Palpable mass
• Lymphadenopathy
• Jaundice
Not necessary
• No alarm symptoms
Management
Epigastric pain syndrome
H.Pylori test (stool) and H.Pylori • eradication if positive
Therapeutic trial • acid supressing therapy • sucralphate – may help • anti-spasmodics – may help
When ineffective • Endoscopy, • USG abdomen
Postprandial distress syndrome
Lifestyle changes
• Weight correction, small meal portions, less fatty meals, no NSA, no gas containing beverages, low coffein,
• Reducing some types of food: garlic, onion, black pepper, spices
• No smoking and alcohol
High placebo effect using any type of therapy Pharmacologic therapy
• Prokinetics – itopride, domperidone, metoclopramide
Dyspepsia lower: causes
Lower dyspepsia Organic cause (IBD, cancer....) Chronic diarrhea (malabs, coeliac.) Secondary causes (gynec, urol, other) Irritable bowel dyndrome (IBS)
Irritable bowel syndrome - IBS
Definition
Abdominal pain
Relief after defecation of loose stool
Provoked in the morning or after a meal
Variants
IBD-D, diarrhea
IBS-C, constipation
IBS-M, mixed type
Irritable bowel syndrome Mechanisms
Associated with microbiome
• Dysbiosis from the “western food”
Associated with gut neurons
• Post infectious IBS • Destruction of some myenteric
plexus neurons by toxins
Lowered pain theshold from the GI tract
Irritable bowel syndrome Investigations
Needed when • Unintentional or unwanted weight-loss
• Rectal syndrome – frequent, false need to pass stool
• Blood in the stool
• Change in stool consistency > 6 weeks in >60 years
• Anemia
• Palpable abdominal mass
• Family history of colorectal cancer
• Typical history and no alarm symtoms
Not needed
Management
Management • Empathy, education, understanding
• Life-style chages • weight loss
• physical exercise • reduction in coffeine, alcohol and fat
• increased consumption of fiber in constipation
• low FODMAP diet in diarrhea
• Drugs • Antispasmodics • Anti-motility agents
• Anti-bloating agents
• Antidepressant



























![Gi Diseases Pedia Auto Saved]](https://img.pdfslide.us/doc/110x75/577d20c21a28ab4e1e93b105/gi-diseases-pedia-auto-saved.jpg)