Embed Size (px)
Citation preview

Journal of Internal Medicine 1998; 243: 447–453
© 1998 Blackwell Science Ltd 447
Introduction
Multiple endocrine neoplasia type 1 (MEN-1) haslong been recognized as an interesting model forbenign and malignant growth disturbance inendocrine and other tissues [1, 2]. Until recently the
roles of the MEN1 gene could only be predicted fromindirect indices. These indirect indices have includedsigns and symptoms, biochemical markers (such ashormone radioimmunoassays), and linked geneticmarkers. Prior predictions about the MEN1 geneinclude: (i) the MEN1 gene is probably a tumour sup-pressor gene [3]; (ii) all or most familial MEN-1 casesare probably caused by germline mutation in thesame gene [4]; and (iii) the MEN1 gene frequentlyseems implicated in sporadic tumours arising in tis-sues affected by MEN-1 [5].
Germline and somatic mutation of the gene for multipleendocrine neoplasia type 1 (MEN1)
S. J. MARX a , S. K. AGARWAL a , M. B. KESTER a , C. HEPPNER a , Y. S. KIM a , M. R. EMMERT-BUCK b et a l .*From aMetabolic Diseases Branch, NIDDK, bLaboratory of Pathology, NCI, cLaboratory of Gene Transfer, NHGRI, dDiagnostic Radiology Department,CC, and eSurgery Branch, NCI; National Institutes of Health, Bethesda, MD, USA
MINISYMPOSIUM MEN & VHL
Abstract. Marx SJ, Agarwal SK, Kester MB, HeppnerC, Kim YS, Emmert-Buck MR, Debelenko LV,Lubensky IA, Zhuang Z, Guru SC, Manickam P,Olufemi SE, Skarulis MC, Doppman JL, AlexanderRH, Liotta LA, Collins FS, Chandrasekharappa SC,Spiegel AM, Burns AL (National Institutes of Health,Bethesda, USA). Germline and somatic mutation ofthe gene for multiple endocrine neoplasia type 1(MEN1) (Minisymposium: MEN & VHL). J Intern Med1998; 243: 447–53.
Dideoxyfingerprinting was used to screen for germlineand somatic MEN1 mutations. This method, appliedto a panel of germline DNA from 15 probands withmultiple endocrine neoplasia type 1 (MEN-1), allowedconfident discovery of the MEN1 gene. GermlineMEN1 mutation has been found in 47 out of 50
probands with familial MEN-1, in 7 out of 8 caseswith sporadic MEN-1, and in 1 out of 3 cases withatypical sporadic MEN-1. Germline MEN1 mutationwas not found in any of five probands with familialhyperparathyroidism. Somatic MEN1 mutations werefound in 7 out of 33 parathyroid tumours not associ-ated with MEN-1. Allowing for repeating mutations, atotal of 47 different germline or somatic MEN1 muta-tions have been identified. Most predict inactivation ofthe encoded ‘menin’ protein, supporting expectationsthat MEN1 is a tumour suppressor gene. The 16observed missense mutations were distributed acrossthe gene, suggesting that many domains are impor-tant to its as yet unknown functions.
Keywords: gastrinoma, oncogene, parathyroid ade-noma, tumour suppressor.
*L. V. Debelenkob, I. A. Lubenskyb, Z. Zhuangb, S. C. Guruc,P. Manickamc, S. E. Olufemic, M. C. Skarulisa, J. L. Doppmand,R. H. Alexandere, L. A. Liottab, F. S. Collinsc, S. C.Chandrasekharappac, A. M. Spiegela & A. L. Burnsa.

S. J. MARX et a l . : GERMLINE AND SOMATIC MUTATION OF THE MEN1 GENE448
© 1998 Blackwell Science Ltd Journal of Internal Medicine 243: 447–453
The complete spectrum of disorders arising fromgermline and somatic MEN1 mutations can only beestablished by measuring such mutations directly.The MEN1 gene has recently been cloned [6]. Directtesting of MEN1 mutation has led to general confir-mation of the prior expectations (see above) and tonew insights [6–9].
Materials and methods
Patients, tumours and DNA
Multiple endocrine neoplasia type 1 was defined astumour in two of the three principal tissues (parathy-roid, enteropancreatic endocrine and anterior pitu-itary). Familial MEN-1 (FMEN-1) was defined asMEN-1 plus at least one first-degree relative withtumour in one or more of the three principal tissues.Subjects were inpatients or outpatients at theNational Institutes of Health (NIH), Bethesda, MD.Their relatives were interviewed and were testedlocally or at the NIH. Whenever possible, outsiderecords including autopsy reports were reviewed.Tumours were obtained at NIH and portions wereeither frozen or fixed in buffered formalin. DNA waspurified from blood, Epstein–Barr virus transformedlymphocytes, or formalin-fixed tissue, includingmicrodissected tumour or normal tissue adjacent totumour. Studies were carried out with informed con-sent, approved by an NIDDK institutional reviewboard.
Mutation detection
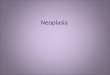
MEN1 exons from germline or tumour DNA wereamplified by PCR and analysed by dideoxyfinger-printing (ddF) (Fig. 1) [10]. Samples showing abnor-mally migrating ddF bands were sequenced, usingthe same PCR product and end-labelled primer as inthe ddF analysis. If a variant sequence could not bedetermined because of an insertion or deletion thatcaused overlap with normal sequence in the het-erozygous setting, the DNA products were segregatedby cloning and then sequenced [6]. The sequence ofsome mutations was confirmed independently byrestriction enzyme digestion, hybridization withallele-specific oligonucleotides, or oligonucleotide-engineered restriction digest.
Results
Germline mutations as an indicator for identifying theMEN1 gene
Dideoxyfingerprinting was the principal method usedto screen for mutations in candidate genes during thesearch for the MEN1 gene. In general, once a tran-script from a candidate gene was identified, its full-length cDNA sequence and its intron–exonboundaries were determined. Then, a panel ofgermline DNA from normal vs. FMEN-1 probandswas used to amplify exons from the intronicsequences, and ddF was then used to screen for vari-
Fig. 1 Mutation detection bydideoxyfingerprinting (ddF). MEN1exons 2–10 were amplifiedindividually or in groups bypolymerase chain reaction (PCR) withprimers derived from intron sequences.The amplified primary products wereused for ddF and cycle sequencing [6,10]. For ddF, the primary PCR productwas used as template in a chaintermination (cycle sequencing type)reaction with an end-labelled primerand only one dideoxynucleotide(dideoxyguanosine triphosphate), andthen separated on a nondenaturinggel. This allows recognition of anabnormal variant band from gain orloss of the terminal G nucleotide (gainis shown in this illustration) andmultiple additional abnormal bandsfrom single strand conformationpolymorphism (SSCP).

MINISYMPOSIUM: MEN & VHL 449
© 1998 Blackwell Science Ltd Journal of Internal Medicine 243: 447–453
ant bands [6]. Nine genes were excluded as not theMEN1 gene by this detailed testing. Benign polymor-phisms were recognized in several rejected candi-dates [11, 12]. The correct gene ‘mu’ or the MEN1gene revealed a broad spectrum of predicted truncat-ing mutations and likely inactivating missense muta-tions as well as several benign polymorphisms [6].
Germline MEN1 mutation analysed in several possiblyhereditary diseases
Familial MEN-1. DNA was tested from a proband of50 apparently unrelated MEN-1 kindreds. Thirty-twodifferent MEN1 mutations were distributed amongst47 kindreds [6, 7].
A correlation with phenotype was sought by inves-tigating three large kindreds with the prolactinomavariant of FMEN-1 [13]. Two of these kindreds haddifferent MEN1 germline mutations (Y312X, R460X[14]); the third had no mutation identified butshowed tight linkage to 11q13.
Sporadic MEN-1. Eight cases with sporadic MEN-1were tested, revealing an MEN1 germline mutationin seven [7]. From a clinical standpoint, it wasnotable that the parathyroid neoplasia in all eightwas multiple parathyroid tumours, a feature that istypical of MEN-1. In addition three cases with atypi-cal variants of sporadic MEN-1 were tested, and agermline MEN1 mutation was found in one.
Parental DNA samples were tested in one case. Thisallowed confirmation of paternity and confirmationof a new MEN1 germline mutation [7]. Such a newmutation provides important further confirmationthat mutation of this gene is the cause of MEN-1.
Familial hyperparathyroidism. Primary hyperparathy-roidism is the commonest and usually the first fea-ture in MEN-1. Thus some small and even some largefamilies with apparently isolated hyperparathy-roidism have this as an expression of MEN-1 [15,16]. However, the term ‘familial hyperparathy-roidism’ includes the hyperparathyroidism–jawtumour syndrome [17, 18], familial hypocalciuric (orbenign) hypercalcaemia (FHH) [19], and probablyother disorders [20].
Probands were tested from five kindreds. The kin-dreds had 2–5 affected members. All probands hadmultiple parathyroid tumours and hypercalciuria,two features making FHH unlikely in each kindred.
None of the five probands showed a MEN1 germlinemutation [7].
Somatic MEN1 mutation analysed in parathyroidtumour without MEN-1
Loss of heterozygosity (LOH) at 11q13 has beenfound in 30–40% of sporadic parathyroid tumours[5]. Though Cyclin D1, Rb, P53, Ret and several otheranonymous tumour suppressor genes have also beenimplicated, the gene(s) at the 11q13 locus seems themost frequent contributor to these tumours [21].Testing was done with 33 parathyroid tumoursfrom 33 different patients without evidence ofMEN-1. No patient had an MEN1 germline mutation.There was 11q13 LOH in 13 (39%) tumours and aMEN1 somatic mutation was found in 7 (21%) [9].
Patterns amongst MEN1 mutations
There were 40 different germline mutations and 7different somatic mutations (Fig. 2). The somaticmutations were different from the germline muta-tions but without any distinguishing pattern foreither. Amongst the 47 mutations there were 12nonsense, 16 missense, 3 inframe deletion, 15frameshift (from small insertions or deletions), and 1splice junction change.
Nine of the germline mutations occurred morethan once, as often as six times (Fig. 2) [6–8].Analysis of core 11q13 haplotypes within andamongst families showed that at least two of therepeatedly observed mutations resulted from a com-mon ancestor [Emmert-Buck MR, unpublished]whilst one or more of the others apparently aroseindependently [7].
Discussion
Dideoxyfingerprinting is a robust screen for MEN1mutation
Dideoxyfingerprinting combines features of cyclesequencing and single strand conformation polymor-phism (SSCP). It was applied during the positionalcloning project to identify the MEN1 gene and subse-quently to identify other germline or somatic MEN1mutations [6, 7, 9].
In a cumulative series, 47 out of 50 FMEN-1probands and 8 out of 11 sporadic MEN-1 casesshowed a germline MEN1 mutation in the predicted

S. J. MARX et a l . : GERMLINE AND SOMATIC MUTATION OF THE MEN1 GENE450
© 1998 Blackwell Science Ltd Journal of Internal Medicine 243: 447–453
protein-coding sequence of the gene. Amongst sevenparathyroid tumours with somatic MEN1 mutation,one was a splice-site mutation at the intron–exonboundary. When MEN1 mutation was not found byddF, direct sequencing in the open reading framefailed to show an underlying mutation [6, 7]. ThusddF was robust. Its few, if any, ‘failures’ may be frommutations in MEN1 regions not tested or fromdeletion of entire exons.
Germline MEN1 mutation is implicated in certaindisorders and excluded in others
These findings begin to define the spectrum of disor-ders arising from MEN1 germline mutation (Table
1). Familial MEN-1 always or almost always arisesfrom germline mutation in the same gene. In 3 out of50 MEN-1 families MEN1 germline mutation wasnot found. Since only the open reading frame of theMEN1 gene was tested for mutation, it seems possiblethat all three of the remaining kindreds have MEN1mutation. At present there is only one reported kin-dred with features of MEN-1 and with apparentexclusion of linkage to 11q13 [23].
No specific genotype correlated with the prolactin-oma MEN-1 phenotype. Further analysis of geno-type–phenotype correlations must await biologicalfunction assays of menin’s domains or testing forother causes of variant phenotypes.
Most cases of sporadic MEN-1 and some cases of
Table 1 Settings with proved [6–9], likely (based on 11q13 LOH data [2]), and speculative role for MEN1 mutation – either germline MEN1mutation in patient or somatic MEN1 mutation in neoplasm. Estimated frequency of MEN1 mutation in parentheses
MEN1mutation type Proved Likely Speculative
Germline Familial MEN-1 (95%) Sporadic gastrinoma (10%) Familial isolated insulinomaSporadic MEN-1 (85%) Sporadic parathyroid hyperplasia Familial isolated somatotropinoma
(10%) or prolactinomaAtypical sporadic MEN-1 (33%) Skin disorders
Somatic Sporadic parathyroid (20%) Uraemic parathyroid (10%) Common cancerParathyroid in familial hyperpara not Gastrinoma (20%) Thyroid tumour
FMEN-1 (20%) Pancr islet (10%) LeiomyomaAnt pituitary (5%) AngiofibromasLipoma (10%)
Collagenoma Aldosteronoma (10%)
Fig. 2 Germline and somatic MEN1mutations. Exons of the MEN1gene are shown with untranslatedportions hatched. Mutations abovethe MEN1 exons are nonsensemutations, frameshift mutations,and a splice junction mutation thatalso causes a frameshift(‘Truncation’); below the exons aremissense mutations and inframedeletions (‘Codon change’). Themajority of mutations are familialMEN1 germline mutation; asterisk(*) is for sporadic MEN1 germlinemutation; long tether and box arefor somatic MEN1 mutation inparathyroid adenoma withoutMEN-1. Parentheses alongside amutation indicate the number ofindependent families where thesame mutation was observed.Mutation numbering followsstandard nomenclature [22].

MINISYMPOSIUM: MEN & VHL 451
© 1998 Blackwell Science Ltd Journal of Internal Medicine 243: 447–453
sporadic MEN-1 variants have MEN1 germlinemutation. There are additional disorders in whichMEN1 germline mutation seems likely to contribute;these include sporadic Zollinger–Ellison syndromeand sporadic primary parathyroid hyperplasia(Table 1).
MEN1 germline mutations were excluded as thecause of disease in many kindreds with familialhyperparathyroidism. It seems unlikely that thesefamilies suffer from an unusual MEN1 mutation thathas escaped detection. However, since a linkageanalysis was not done, this remains a formal possi-bility. These families probably have different dis-orders. The first candidate disorder is thehyperparathyroidism–jaw tumour syndrome. Thishas been linked to an interval at 1q21–1q32 so link-age analysis could be informative in some of thesesmall kindreds [17, 18].
Other ‘variant’ MEN-1 families should be similarlytested. This includes families with multiple membersshowing tumour of only one endocrine system, suchas prolactinoma [24], somatotropinoma [25, 26],insulinoma [27] or carcinoid [28].
Somatic MEN1 mutation is a contributor to certaintumours
These findings prove the involvement of the MEN1gene in certain sporadic tumours. Prior studies of11q13 LOH have led to the prediction that MEN1mutations would contribute to sporadic tumours ofthe parathyroid, anterior pituitary, enteropancreaticendocrine tissue, carcinoid, thyroid and adrenal fas-ciculata [2]. This was proved for primary parathyroidtumours [9]. Proof of MEN1 somatic mutation insporadic primary parathyroid tumours makes it likelythat similar mutations will be found in uraemicparathyroid tumour [29, 30] and in sporadictumours of other endocrine tissues with 11q13 LOH[31–33]. Studies of MEN1 mutation in sporadictumours might lead to new prognostic indices oreven some day to new therapies.
The MEN1 gene could potentially be inactivated bymechanisms other than mutation. 11q13 LOH is anindex of loss of one presumably normal copy of theMEN1 gene. Another indicator of MEN1 in-activation is 11q13 LOH without evidence for muta-tion in the other copy of the MEN1 gene. This wasseen in sporadic parathyroid tumours as often as11q13 LOH with MEN1 somatic mutation. Thus it
appears that other gene inactivation mechanisms,such as promoter methylation, may contribute tosporadic tumorigenesis in the parathyroid gland [34,35].
It is also possible that the MEN1 gene contributesto yet other tumours either by a primary disturbancesuch as mutation or epigenetic silencing or as asecondary participant in the neoplastic process. Twolesions of particular interest are angiofibromas andleiomyomas. Multiple facial angiofibromas are com-mon in MEN-1 (88% of cases) [36], but 11q13 LOHwas not found in three MEN-1 angiofibromas [31].Muscle tumours have been seen in several MEN-1cases [7]; in two MEN-1 muscle tumours 11q13 LOHwas not found [31]. Last but not least, MEN1 muta-tion may contribute to certain common nonen-docrine cancers with 11q13 LOH [37, 38] or evenwithout known 11q13 LOH.
MEN1 mutation provides initial insights about MEN1gene function
The MEN1 gene was analysed for computer-assistedmatches to known sequences in databases for anyspecies [6]. The analysis showed evidence for a nearlyidentical gene in the mouse. Otherwise there were noother homologous genes. The gene predicts a 610-amino acid protein (menin) without domains thatwould predict known roles such as nuclear localiza-tion, transmembrane anchoring or secretion. The 47MEN1 mutations were mostly nonsense andframeshift mutations that could inactivate the pre-dicted protein (Fig. 2). This supported its predictedrole as a tumour suppressor gene that could con-tribute to tumours through sequential inactivation ofboth copies.
The mutation data include 16 missense mutations.Since missense mutations do not predict truncationof the protein, they can provide insight intomechanisms whereby subtle changes (switch of oneamino acid) cause an important change of function(probably near full inactivation). In this case, the 16missense mutations are spread across the predictedmenin molecule (Fig. 2). Whilst the lack of clusteringdoes not highlight any critical domain such as anenzymatic active site, the dispersion of mutationsitself suggests that the entire molecule is functionallyimportant. Of course, a missense ‘mutation’ could, infact, be a rare benign polymorphism. Whilst each ofthese missense ‘mutations’ was absent from a large

S. J. MARX et a l . : GERMLINE AND SOMATIC MUTATION OF THE MEN1 GENE452
© 1998 Blackwell Science Ltd Journal of Internal Medicine 243: 447–453
panel of normal samples [6], proof of theirdeleterious properties awaits assays of biologicalfunction.
MEN1 mutation testing will be used for geneticcounselling
Robust ascertainment of MEN1 mutation is now possi-ble. Highly informative testing for MEN1 germlinemutations is clearly possible with dideoxyfingerprint-ing (ddF). It seems that similar methods will be asinformative when applied to somatic mutation.Dideoxyfingerprinting is not widely available at pre-sent, so it will be important to determine whetherother methods will give a similar yield [8]. SSCP maybe as efficient as ddF, and high throughput sequenc-ing should give a similar yield to ddF. Protein trunca-tion-type assays alone are likely to be unsatisfactorybecause of the 33% frequency of missense mutationsthat would not be detected.
These data show many different MEN1 mutationsin germline and somatic DNA. Though the full spec-trum of recurrent mutations will only be clarified bytesting patients from multiple geographic regions, itis already clear that mutation detection shortcutsdirected to one or a few specific mutations will not bepromising except within a kindred or in a geographi-cally or otherwise reproductively restricted popula-tion [6, 14].
Who should be tested? The candidates for germlineMEN1 mutation testing are mostly self-evident. Theyare new cases of MEN-1 and affected and unaffectedrelatives of MEN-1 cases (whether or not in a settingof FMEN-1). Most testing should be restricted to first-degree relatives [39, 40], except where the connect-ing first-degree relative is not available. In the USA,the genetics community has a consensus that minorsshould not be tested when testing results do not havea major impact on management [41]. With furtherresearch, it is possible that additional cases will beconsidered appropriate for MEN1 germline mutationtesting (Table 1).
Acknowledgements
We acknowledge the cooperation of the patients andtheir families. We thank many participants in theNIDDK/NICHD interinstitute endocrinology trainingprogram.
C.H. is supported by a grant from the Fritz ThyssenStiftung (Germany).
References1 Metz DC, Jensen RT, Bale AE, Skarulis MC, Eastman RC,
Nieman L et al. Multiple endocrine neoplasia type 1: clinicalfeatures and management. In: Bilezekian JP, Levine MA &Marcus R, eds. The Parathyroids. New York: Raven Press, 1994;591–646.
2 Friedman E, Larsson C, Amorosi A, Brandi ML, Bale AE, MetzD et al. Multiple endocrine neoplasia type 1: pathology, patho-physiology, and differential diagnosis. In: Bilezekian JP, LevineMA & Marcus R, eds. The Parathyroids. New York: Raven Press,1994; 647–80.
3 Larsson C, Skogseid B, Oberg K, Nakamura Y, Nordenskjold M.Multiple endocrine neoplasia type 1 gene maps to chromosome11 and is lost in insulinoma. Nature 1988; 332: 85–7.
4 Courseaux A, Grosgeorge J, Gaudray P, Pannett AAJ, ForbesSA, Williamson C et al. Definition of the minimal MEN1 candi-date area based on a 5-Mb integrated map of proximal 11q13.Genomics 1996; 37: 354–65.
5 Friedman E, Sakaguchi K, Bale AE, Falchetti A, Streeten E,Zimering MB et al. Clonality of parathyroid tumors in familialmultiple endocrine neoplasia type 1. N Engl J Med 1989; 321:213–18.
6 Chandrasekharappa SC, Guru SC, Manickam P, Olufemi S-E,Collins FS, Emmert-Buck MR et al. Positional cloning of thegene for multiple endocrine neoplasia type 1. Science 1997;276: 404–7.
7 Agarwal SK, Kester MB, Debelenko LV, Heppner C, Emmert-Buck MR, Skarulis MC et al. Germline mutations of the MEN1gene in familial multiple endocrine neoplasia type 1 and relat-ed states. Hum Mol Genet 1997; 7: 1169–75.
8 Lemmens I, Van de Ven WJM, Kas K, Zhang CX, Giraud S,Wautot V et al. Identification of the multiple endocrine neopla-sia type 1 (MEN1). gene. Hum Mol Genet 1997; 7: 1177–83.
9 Heppner C, Kester MB, Agarwal SK, Debelenko LV, Emmert-Buck MR, Guru SC et al. Somatic mutation of the MEN1 genein parathyroid tumors. Nat Genet 1997; 16: 375–8.
10 Sarkar G, Yoon HS, Sommer SS. Dideoxy fingerprinting (ddF):a rapid and efficient screen for the presence of mutations.Genomics 1992; 13: 441–3.
11 Manickam P, Guru SC, Debelenko LV, Agarwal SK, Olufemi SE,Weisemann JM et al. Eighteen new polymorphic markers inthe multiple endocrine neoplasia type 1 (MEN1) region. HumGenet 1997; 101: 102–8.
12 Guru SC, Agarwal SK, Manickam P, Olufemi SE, Crabtree JS,Weisemann JM et al. A transcript map of the 2.8 Mb regioncontaining the multiple endocrine neoplasia type 1 (MEN1)locus. Genome Res 1997; 7: 725–35.
13 Hershon KS, Kelly WA, Shaw CM, Schwartz R, Bierman EL.Prolactinomas as part of the multiple endocrine neoplasticsyndrome type 1. Am J Med 1983; 74: 713–20.
14 Olufemi SE, Green JS, Manickam P, Guru SC, Agarwal SK,Kester MB et al. A common ancestral mutation in the MEN1gene is likely responsible for the prolactinoma variant(MEN1Burin) in four kindreds from Newfoundland. Hum Mut1998; 11: 264–9.
15 Marx SJ, Spiegel AM, Levine MA, Rizzoli RE, Lasker RD,Santora AC II et al. Familial hypocalciuric hypercalcemia: the

MINISYMPOSIUM: MEN & VHL 453
© 1998 Blackwell Science Ltd Journal of Internal Medicine 243: 447–453
relation to primary parathyroid hyperplasia. N Engl J Med1982; 307: 416–26.
16 Kassem M, Zhang X, Brask S, Eriksen EF, Mosekilde L, Kruse T.Familial isolated primary hyperparathyroidism. Clin Endocrinol1994; 41: 415–20.
17 Szabo J, Heath B, Hill VM, Jackson CE, Zarbo RJ, Mallette LE etal. Hereditary hyperparathyroidism–jaw tumor syndrome: theendocrine tumor gene HRPT2 maps to chromosome 1q21-q31. Am J Hum Genet 1995; 56: 944–50.
18 Teh BT, Farnebo F, Kristoffersson U, Sundelin B, Cardinal J,Axelson R et al. Autosomal dominant primary hyperparathy-roidism and jaw tumor syndrome associated with renalhamartomas and cystic kidney disease: linkage to 1q21-q32and loss of the wild type allele in renal hamartomas. J ClinEndocrinol Metab 1996; 81: 4204–11.
19 Brown EM, Pollak M, Seidman CE, Seidman JG, Chou YHW,Riccardi D, Herbert SC. Calcium-ion-sensing cell-surfacereceptors. N Engl J Med 1995; 333: 234–40.
20 Law WM Jr, Hodgson S, Heath H III. Autosomal recessiveinheritance of familial hyperparathyroidism. N Engl J Med1983; 309: 650–3.
21 Tahara H, Smith AP, Gaz RD, Cryns VL, Arnold A. Genomiclocalization of novel candidate tumor suppressor gene loci inhuman parathyroid adenomas. Canc Res 1996; 56: 599–605.
22 Beaudet AL, Tsui L. A suggested nomenclature for designatingmutations. Hum Mutat 1993; 2: 245–8.
23 Stock JL, Warth MR, Teh BT, Coderre JA, Overdorf JH,Baumann G et al. A kindred with a variant of multipleendocrine neoplasia type 1 demonstrating frequent expressionof pituitary tumors but not linked to the multiple endocrineneoplasia type 1 locus at chromosome region 11q13. J ClinEndocrinol Metab 1997; 82: 486–92.
24 Berezin M, Karasik A. Familial prolactinoma. Clin Endocrinol1995; 42: 483–6.
25 Pestell RG, Alford FP, Best JD. Familial acromegaly. ActaEndocrinol (Copenh) 1989; 121: 286–9.
26 Yamada S, Yoshimoto K, Sano T, Takada K, Itakura M, Usui M.Teramoto A Inactivation of the tumor suppressor gene on11q13 in brothers with familial acrogigantism without multi-ple endocrine neoplasia type 1. Clin Endocrinol Metab 1997;82: 239–42.
27 Maioli M, Ciccarese M, Pacifico A, Tonolo G, Ganau A, Cossu Set al. Familial insulinoma: description of two cases. ActaDiabetol 1992; 29: 38–40.
28 Yeatman TJ, Sharp JV, Kimura AK. Can susceptibility to carci-noid tumors be inherited? Cancer 1989; 63: 390–3.
29 Falchetti A, Bale AE, Amorosi A, Bordi C, Cicci P, Bandini S etal. Progression of uremic hyperparathyroidism involves allelicloss on chromosome 11. J Clin Endocrinol Metab 1993; 76:139–44.
30 Arnold A, Brown MF, Urena P, Gaz RD, Sarfati E, Drueke TB.Monoclonality of parathyroid tumors in chronic renal failureand in primary parathyroid hyperplasia. J Clin Invest 1995;95: 2047–53.
31 Dong Q, Debelenko L, Chandrasekharappa S, Emmert-BuckMR, Zhuang Z, Guru SC et al. Loss of heterozygosity at 11q13:analysis of pituitary tumors, lung carcinoids, lipomas, andother uncommon tumors in familial multiple endocrineneoplasia type 1. J Clin Endocrinol Metab 1997; 82:1416–20.
32 Bates AS, Farrell WE, Bicknell EJ, McNicol AM, Talbots AJ,Broome JC et al. Allelic deletion in pituitary adenomas reflectsaggressive biological activity and has potential value as aprognostic marker. J Clin Endocrinol Metab 1997; 82:818–24.
33 Debelenko LV, Zhuang Z, Emmert-Buck MR,Chandrasekharappa SC, Manickam P, Guru SC et al. Allelicdeletions on chromosome 11q13 in MEN1-associated and spo-radic duodenal gastrinomas and pancreatic endocrine tumors.Canc Res 1997; 157: 2238–43.
34 Herman JG, Latif F, Weng Y, Lerman MI, Zbar B, Liu S et al.Silencing of the VHL tumor suppressor gene by DNA methyla-tion in renal carcinoma. Proc Natl Acad Sci USA 1994; 91:9700–4.
35 Merlo A, Herman JG, Mao L, Lee DJ, Gabrielson E, Burger PC etal. 59 CpG island methylation is associated with transcriptionalsilencing of the tumor suppressor p16/CDKN2/MTS1 inhuman cancers. Nat Med 1995; 1: 686–92.
36 Darling TN, Skarulis MC, Steinberg SM, Marx SJ, Spiegel AM,Turner M. Multiple facial angiofibromas and collagenomas inpatients with multiple endocrine neoplasia type 1. ArchDermatol 1997; 133: 853–7.
37 Chuaqui RF, Zhuang Z, Emmert-Buck MR, Liotta LA, MerinoMJ. Analysis of loss of heterozygosity on chromosome 11q13in atypical ductal hyperplasia and in situ carcinoma of thebreast. Am J Pathol 1997; 150: 297–303.
38 Jesudasan RA, Rahman MR, Evans GA, Srivatsan ES. Reply toPopescu and Zimonjic. Am J Hum Genet 1996; 58: 424–5.
39 Marx SJ, Vinik AI, Santen RJ, Floyd JC Jr, Mills JL, Green J III.Multiple endocrine neoplasia type I. Assessment of laboratorytests to screen for the gene in a large kindred. Medicine 1986;65: 226–41.
40 Trump D, Farren B, Wooding C, Pang JT, Besser GM,Buchanan KD et al. Clinical studies of multiple endocrine neo-plasia type 1 (MEN1). Quart J Med 1996; 89: 653–69.
41 American Society of Human Genetics Board of Directors andAmerican College of Medical Genetics Board of Directors.Ethical, legal and psychosocial implications of genetic testingin children and adolescents. Am J Hum Genet 1995; 57:1233–41.
Received 25 November 1997; accepted 22 January 1998.
Correspondence: Stephen Marx MD, Genetics & EndocrinologySection, Bldg 10, Room 9C-101, National Institutes of Health,Bethesda, MD 20892-1802, USA (tel: 301 496 5051; fax: 301496 0200; e-mail: [email protected]).

![ENETS Consensus Guidelines for the Management of Patients ... · drome of Multiple Endocrine Neoplasia type 1 (MEN1) (25% of cases) will also be mentioned [11, 12] . I nsulinomas](https://img.pdfslide.us/doc/110x75/5ec39d2e59d16726d441c901/enets-consensus-guidelines-for-the-management-of-patients-drome-of-multiple.jpg)