Embed Size (px)
Citation preview

Genotypic and Phenotypic Characterization of Carriage and InvasiveDisease Isolates of Neisseria meningitidis in Finland
Ulla Jounio,a,b,c Annika Saukkoriipi,d Holly B. Bratcher,e Aini Bloigu,d Raija Juvonen,f Sylvi Silvennoinen-Kassinen,a Ari Peitso,c
Terttu Harju,g Olli Vainio,a,b Markku Kuusi,h Martin C. J. Maiden,e Maija Leinonen,d Helena Käyhty,h and Maija Toropainenh
Institute of Diagnostics, Department of Medical Microbiology, University of Oulu, Oulu, Finlanda; Clinical Microbiology Laboratory, Oulu University Hospital, Oulu, Finlandb;Finnish Defence Forces, Centre for Military Medicine, Lahti, Finlandc; National Institute for Health and Welfare, Oulu, Finlandd; University of Oxford, Oxford, UnitedKingdome; Kainuu Central Hospital, Department of Otorhinolaryngology, Kajaani, Finlandf; Oulu University Hospital, Department of Internal Medicine, Oulu, Finlandg; andNational Institute for Health and Welfare, Helsinki, Finlandh
The relationship between carriage and the development of invasive meningococcal disease is not fully understood. We investigated thechanges in meningococcal carriage in 892 military recruits in Finland during a nonepidemic period (July 2004 to January 2006) andcharacterized all of the oropharyngeal meningococcal isolates obtained (n � 215) by using phenotypic (serogrouping and serotyping)and genotypic (porA typing and multilocus sequence typing) methods. For comparison, 84 invasive meningococcal disease strains iso-lated in Finland between January 2004 and February 2006 were also analyzed. The rate of meningococcal carriage was significantlyhigher at the end of military service than on arrival (18% versus 2.2%; P < 0.001). Seventy-four percent of serogroupable carriage iso-lates belonged to serogroup B, and 24% belonged to serogroup Y. Most carriage isolates belonged to the carriage-associated ST-60clonal complex. However, 21.5% belonged to the hyperinvasive ST-41/44 clonal complex. Isolates belonging to the ST-23 clonal com-plex were cultured more often from oropharyngeal samples taken during the acute phase of respiratory infection than from samplestaken at health examinations at the beginning and end of military service (odds ratio [OR], 6.7; 95% confidence interval [95% CI], 2.7to 16.4). The ST-32 clonal complex was associated with meningococcal disease (OR, 17.8; 95% CI, 3.8 to 81.2), while the ST-60 clonalcomplex was associated with carriage (OR, 10.7; 95% CI, 3.3 to 35.2). These findings point to the importance of meningococcal vaccina-tion for military recruits and also to the need for an efficacious vaccine against serogroup B isolates.
Neisseria meningitidis causes both epidemic and endemic life-threatening diseases worldwide, most notably sepsis and bac-
terial meningitis. It is also part of the normal nasopharyngeal mi-crobiota of healthy persons (25, 34). The rate of asymptomaticcarriage varies greatly depending on the population and epidemi-ological situation in question, ranging between 10% and 35%among young adults in Europe and the United States (6, 10, 34).Carriage is more common in teenagers and young adults than inyoung children (3), and the highest transmission and carriagerates have been reported for populations of people living in closecontact with one another, such as university students or militaryrecruits sharing dormitories (7). The molecular epidemiology ofmeningococcal carriage and disease development is not fully un-derstood.
Previous phenotypic and genotypic studies have shown that N.meningitidis strains recovered from carriers are genetically morediverse than those isolated from patients with invasive meningo-coccal disease (IMD) (8, 9). Relatively few genotypes, the “hyper-invasive lineages,” have been responsible for most IMD, whileonly a small proportion of the strains isolated from carriers gen-erally belong to these hyperinvasive lineages (26). Since most pa-tients with life-threatening invasive disease have not been in con-tact with other IMD patients, it is assumed that carriers are themajor source of the virulent strains that are potential causes ofdisease. In order to introduce effective IMD prevention policies,including vaccination, more carriage studies are needed to im-prove our understanding of the spread of N. meningitidis in pop-ulations at heightened risk of meningococcal disease, includingmilitary recruits.
The incidence of invasive meningococcal disease in Finland(�0.7 case/100,000 inhabitants/year) is currently low. In contrast
to the case in many other European countries, with increases inserogroup C disease during the last few decades, there have beenno major meningococcal epidemics or outbreaks in Finland sincethe serogroup A meningococcal epidemic in the 1970s (27) and asmaller serogroup B epidemic involving military recruits in south-ern Finland in 1995 and 1996 (31). Thus, meningococcal vaccina-tion is currently recommended in Finland only for high-riskgroups, including military recruits, who receive a tetravalent sero-group ACYW135 polysaccharide vaccine as a part of their vacci-nation program when entering service.
The present study aimed to follow changes in meningococcalcarriage in military recruits in Finland during a nonepidemic pe-riod (July 2004 to January 2006). To investigate the diversity of thecarriage isolates, meningococci isolated from oropharyngealswabs taken at the beginning and end of military service or duringthe acute phase of respiratory tract infection were subjected tophenotyping (serogrouping and serotyping) and genotyping(porA typing and multilocus sequence typing [MLST]). For com-parison, 84 meningococcal strains isolated from IMD patients inFinland in January 2004 to February 2006 were also analyzed.
(Some of the data in this study were presented previously at the
Received 9 August 2011 Returned for modification 1 September 2011Accepted 18 November 2011
Published ahead of print 30 November 2011
Address correspondence to Ulla Jounio, [email protected].
Copyright © 2012, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.05385-11
The authors have paid a fee to allow immediate free access to this article.
264 jcm.asm.org 0095-1137/12/$12.00 Journal of Clinical Microbiology p. 264–273
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
Seventeenth International Pathogenic Conference 2010, Banff,Canada [21a].)
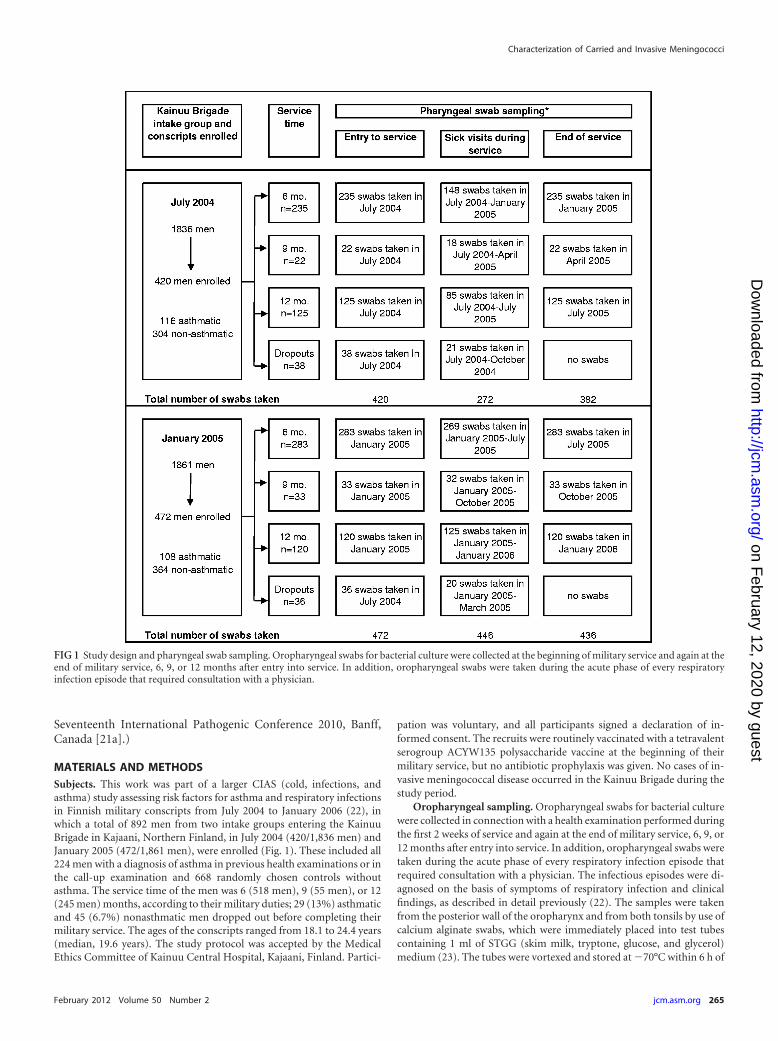
MATERIALS AND METHODSSubjects. This work was part of a larger CIAS (cold, infections, andasthma) study assessing risk factors for asthma and respiratory infectionsin Finnish military conscripts from July 2004 to January 2006 (22), inwhich a total of 892 men from two intake groups entering the KainuuBrigade in Kajaani, Northern Finland, in July 2004 (420/1,836 men) andJanuary 2005 (472/1,861 men), were enrolled (Fig. 1). These included all224 men with a diagnosis of asthma in previous health examinations or inthe call-up examination and 668 randomly chosen controls withoutasthma. The service time of the men was 6 (518 men), 9 (55 men), or 12(245 men) months, according to their military duties; 29 (13%) asthmaticand 45 (6.7%) nonasthmatic men dropped out before completing theirmilitary service. The ages of the conscripts ranged from 18.1 to 24.4 years(median, 19.6 years). The study protocol was accepted by the MedicalEthics Committee of Kainuu Central Hospital, Kajaani, Finland. Partici-
pation was voluntary, and all participants signed a declaration of in-formed consent. The recruits were routinely vaccinated with a tetravalentserogroup ACYW135 polysaccharide vaccine at the beginning of theirmilitary service, but no antibiotic prophylaxis was given. No cases of in-vasive meningococcal disease occurred in the Kainuu Brigade during thestudy period.
Oropharyngeal sampling. Oropharyngeal swabs for bacterial culturewere collected in connection with a health examination performed duringthe first 2 weeks of service and again at the end of military service, 6, 9, or12 months after entry into service. In addition, oropharyngeal swabs weretaken during the acute phase of every respiratory infection episode thatrequired consultation with a physician. The infectious episodes were di-agnosed on the basis of symptoms of respiratory infection and clinicalfindings, as described in detail previously (22). The samples were takenfrom the posterior wall of the oropharynx and from both tonsils by use ofcalcium alginate swabs, which were immediately placed into test tubescontaining 1 ml of STGG (skim milk, tryptone, glucose, and glycerol)medium (23). The tubes were vortexed and stored at �70°C within 6 h of
FIG 1 Study design and pharyngeal swab sampling. Oropharyngeal swabs for bacterial culture were collected at the beginning of military service and again at theend of military service, 6, 9, or 12 months after entry into service. In addition, oropharyngeal swabs were taken during the acute phase of every respiratoryinfection episode that required consultation with a physician.
Characterization of Carried and Invasive Meningococci
February 2012 Volume 50 Number 2 jcm.asm.org 265
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

collection for later analysis. The samples were cultured in batches after anaverage storage time of 6 months at �70°C.
Culture, isolation, and characterization of carriage isolates. Theoropharyngeal swabs stored in STGG medium were thawed at room tem-perature for 15 to 30 min, vortexed for about 10 s, and cultured on non-selective chocolate agar plates. The plates were incubated in 5% carbondioxide at 37°C and examined at 24 and 48 h for the growth ofmeningococcus-like colonies. A single colony was picked from each platewith suspected meningococcal growth for subculturing prior to speciesidentification by Gram staining, oxidase reaction, and carbohydrate uti-lization tests. All isolates identified as N. meningitidis were initially char-acterized with regard to serogroup and serotype by whole-cell enzyme-linked immunosorbent assay (ELISA) as described previously (37). Themonoclonal antibodies for phenotyping were purchased from the Na-tional Institute for Biological Standards and Control, United Kingdom,with the exception of the serogroup Y-specific monoclonal antibody 1938(39), a kind gift from Ulrich Vogel and Heike Claus (University of Wür-zburg, Germany), and the serogroup B-specific monoclonal antibodyNmB 735 (16), purchased from Dade Behring Marburg GmbH (Marburg,Germany). Isolates that did not react with any of the serogrouping re-agents (A, B, C, Y, and W135) or with the serotyping reagents (P2.2a,P2.2b, P3.1, P3.4, P3.14, P3.15, and P3.21) were defined as nongroupable(NG) or nontypeable (NT), respectively. The isolates were further ana-lyzed by MLST and porA typing (VR1 and VR2) as previously described(20, 26). A combination of serogroup, serotype, and porA type was used todefine each meningococcal isolate.
Characterization of invasive disease isolates. Out of the total of 91notifications of IMD cases that were referred to the National InfectiousDisease Registry (NIDR) at the National Institute for Health and Welfare(THL) between January 2004 and February 2006, 92% (84/91 cases) wereculture-confirmed cases for which corresponding isolates were submittedto the National Meningococcal Reference Laboratory at the THL for spe-cies confirmation, serogrouping by latex and/or slide agglutination, andserotyping by whole-cell ELISA. DNAs extracted from the culture-confirmed cases were sent to the University of Oxford for MLST, porAtyping, and ClonalFrame analysis.
Statistical analysis. Statistical analyses were performed using SPSSv.17.0 (SPSS Inc., Chicago, IL). The chi-square test or Fisher’s exact test, asappropriate, was used for categorical variables. A logistic regression anal-ysis was used to calculate odds ratios (OR), and the results for the carrierstrains were adjusted for smoking and intake group. A two-sided P valueof �0.05 was considered statistically significant.
ClonalFrame analysis. ClonalFrame, version 1.1 (12), a statisticaltree-building algorithm, was used to infer the clonal relationships of theisolate sets, taking into account homologous recombination that mayhave been present. ClonalFrame draws inferences by using a Monte CarloMarkov chain and requires an assessment of the convergence and mixingof its results (13); therefore, several independent runs of ClonalFrame(100,000 to 150,000 iterations) were run for each assessment. The resultswere compared for convergence by using the Gelman and Rubin statistic(17), and the runs were combined for maximum robustness. The conver-gence was judged satisfactory, and the samples from the runs were com-bined for maximum robustness. Statistical support for any grouping ofisolates was assessed by the proportion of clonal genealogies exhibitingthis grouping in the combined sample. This approach was applied inde-pendently to each of the carriage and disease isolate sets separately and ina combined isolate tree.
RESULTSSerogroups, MLST sequence types (STs), and antigen profiles ofmeningococcal carriage isolates from army recruits. A total of193 carriers were identified among the 892 conscripts, and 215meningococcal carriage isolates were obtained. Twenty of the 215oropharyngeal isolates (9.5%) were obtained from swabs collectedon entry to military service, 151 (70%) were from swabs collected
at the end of service, and 44 (20.5%) were from swabs collectedduring acute respiratory infections (Table 1). Twenty (10.4%) ofthe 193 carriers were culture positive for N. meningitidis morethan once during their military service, while the remaining car-riers (173/193 individuals [89.6%]) were culture positive onlyonce. The carriage of N. meningitidis did not differ between asth-matics and nonasthmatics (P � 0.05), and therefore these twogroups were analyzed together. Serogroups B, Y, and W135 ac-counted for 25.6% (55/215 isolates), 8.4% (18/215 isolates), and0.4% (1/215 isolates) of the isolates, respectively, and 65.6% (141/215 isolates) of the isolates were NG.
Those entering military service, in general, had a low rate of N.meningitidis carriage (Table 1), and this was significantly (P �0.001) lower for the summer intake group than for the winterintake group (0.5% [2/420 individuals] versus 3.8% [18/472 indi-viduals]). The rate of carriage was significantly (P � 0.001) higherat the end of military service than it had been at arrival, with 14.7%(56/382 individuals) of those in the summer intake group and21.8% (95/436 individuals) of those in the winter intake groupbeing culture positive for meningococci (P � 0.001 between thetwo groups). Only five conscripts (0.6%) were culture positive forN. meningitidis at both the beginning and end of their service.
By MLST, 111 different STs were identified among 214 carriageisolates with complete MLST profiles, of which 57.7% (64/111STs) were new STs. Overall, 93.5% (200/214 isolates) of the iso-lates fell into 14 previously known clonal complexes (Table 2). TheST-60 clonal complex was the most common, with 60 (28%) iso-lates and 20 different STs, followed by the ST-41/44 clonal com-plex, with 46 isolates (21.5%) and 25 STs, and the ST-23 clonalcomplex, with 25 isolates (12%) and 11 STs. The two most com-mon STs were ST-4146 (ST-60 clonal complex), with 29 isolates(13.6%), and ST-136 (ST-41/44 clonal complex), with 14 isolates(6.5%). Two-thirds of all carriage isolates were nongroupable by tra-ditional serogrouping methods. Of the clonal complexes representedby two or more isolates (this includes the isolates with unassignedSTs, grouped as “unassociated”), five (clonal complexes 254, 178,198, 53, and 32) could not be serogrouped, three (clonal complexes60, 35, and 213) were partially serogrouped but with limited results,and the remaining four (clonal complexes 41/44, 23, and 269 and the“unassociated” group) had moderate to high success for serogroup-ing (Table 2). The majority of serogroupable isolates belonged to
TABLE 1 Carriage of N. meningitidis by intake group, service time, andtime of sampling
Intake groupServicetime (mo)
Carriage rate (no. of carriers/no. ofindividuals [%])
Entry Sick visits End of service
July 2004 6 1/235 (0.4) 9/148 (6) 27/235 (11.5)9 0/22 1/18 (5.6) 5/22 (22.7)12 1/125 (0.8) 3/85 (3.2) 24/125 (19.2)Dropouts 0/38 2/21 (9.5) NAa
January 2005 6 9/283 (3.2) 18/269 (6.7) 68/283 (24)9 1/33 (3) 0/32 7/33 (21)12 8/120 (6.7) 9/125 (7.2) 20/120 (17)Dropouts 0/36 2/20 (10) NAa
Total 20/892 (2.2) 44/718 (6.1) 151/818 (18.5)a NA, not applicable.
Jounio et al.
266 jcm.asm.org Journal of Clinical Microbiology
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
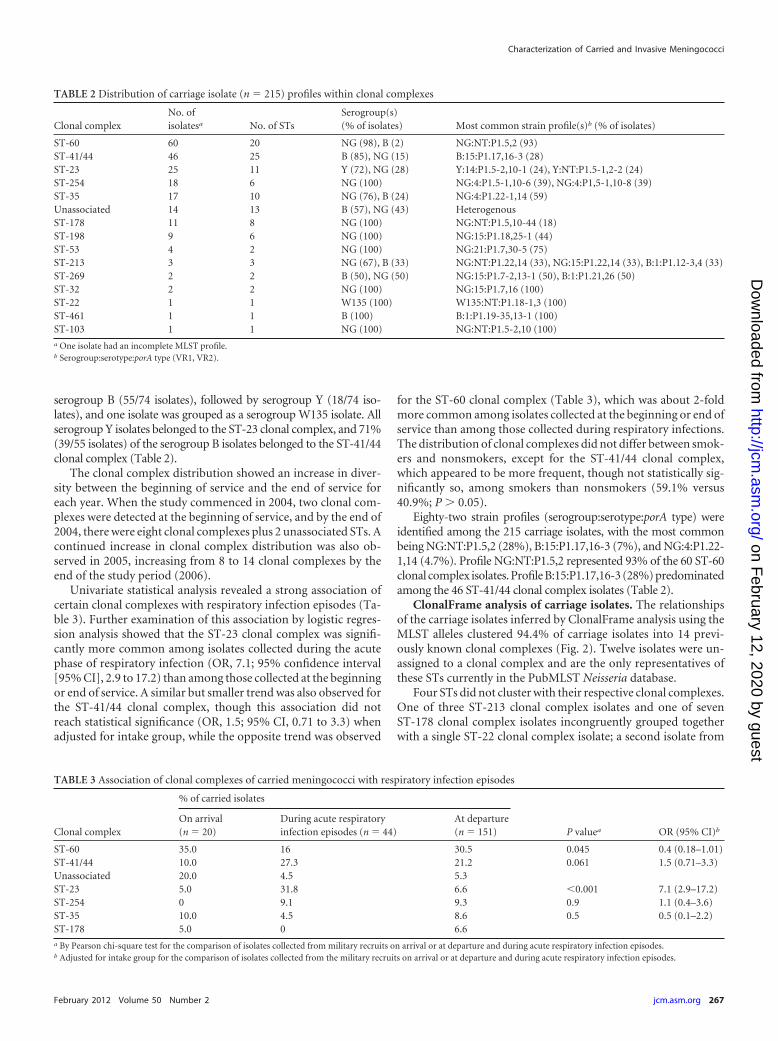
serogroup B (55/74 isolates), followed by serogroup Y (18/74 iso-lates), and one isolate was grouped as a serogroup W135 isolate. Allserogroup Y isolates belonged to the ST-23 clonal complex, and 71%(39/55 isolates) of the serogroup B isolates belonged to the ST-41/44clonal complex (Table 2).
The clonal complex distribution showed an increase in diver-sity between the beginning of service and the end of service foreach year. When the study commenced in 2004, two clonal com-plexes were detected at the beginning of service, and by the end of2004, there were eight clonal complexes plus 2 unassociated STs. Acontinued increase in clonal complex distribution was also ob-served in 2005, increasing from 8 to 14 clonal complexes by theend of the study period (2006).
Univariate statistical analysis revealed a strong association ofcertain clonal complexes with respiratory infection episodes (Ta-ble 3). Further examination of this association by logistic regres-sion analysis showed that the ST-23 clonal complex was signifi-cantly more common among isolates collected during the acutephase of respiratory infection (OR, 7.1; 95% confidence interval[95% CI], 2.9 to 17.2) than among those collected at the beginningor end of service. A similar but smaller trend was also observed forthe ST-41/44 clonal complex, though this association did notreach statistical significance (OR, 1.5; 95% CI, 0.71 to 3.3) whenadjusted for intake group, while the opposite trend was observed
for the ST-60 clonal complex (Table 3), which was about 2-foldmore common among isolates collected at the beginning or end ofservice than among those collected during respiratory infections.The distribution of clonal complexes did not differ between smok-ers and nonsmokers, except for the ST-41/44 clonal complex,which appeared to be more frequent, though not statistically sig-nificantly so, among smokers than nonsmokers (59.1% versus40.9%; P � 0.05).
Eighty-two strain profiles (serogroup:serotype:porA type) wereidentified among the 215 carriage isolates, with the most commonbeing NG:NT:P1.5,2 (28%), B:15:P1.17,16-3 (7%), and NG:4:P1.22-1,14 (4.7%). Profile NG:NT:P1.5,2 represented 93% of the 60 ST-60clonal complex isolates. Profile B:15:P1.17,16-3 (28%) predominatedamong the 46 ST-41/44 clonal complex isolates (Table 2).
ClonalFrame analysis of carriage isolates. The relationshipsof the carriage isolates inferred by ClonalFrame analysis using theMLST alleles clustered 94.4% of carriage isolates into 14 previ-ously known clonal complexes (Fig. 2). Twelve isolates were un-assigned to a clonal complex and are the only representatives ofthese STs currently in the PubMLST Neisseria database.
Four STs did not cluster with their respective clonal complexes.One of three ST-213 clonal complex isolates and one of sevenST-178 clonal complex isolates incongruently grouped togetherwith a single ST-22 clonal complex isolate; a second isolate from
TABLE 2 Distribution of carriage isolate (n � 215) profiles within clonal complexes
Clonal complexNo. ofisolatesa No. of STs
Serogroup(s)(% of isolates) Most common strain profile(s)b (% of isolates)
ST-60 60 20 NG (98), B (2) NG:NT:P1.5,2 (93)ST-41/44 46 25 B (85), NG (15) B:15:P1.17,16-3 (28)ST-23 25 11 Y (72), NG (28) Y:14:P1.5-2,10-1 (24), Y:NT:P1.5-1,2-2 (24)ST-254 18 6 NG (100) NG:4:P1.5-1,10-6 (39), NG:4:P1,5-1,10-8 (39)ST-35 17 10 NG (76), B (24) NG:4:P1.22-1,14 (59)Unassociated 14 13 B (57), NG (43) HeterogenousST-178 11 8 NG (100) NG:NT:P1.5,10-44 (18)ST-198 9 6 NG (100) NG:15:P1.18,25-1 (44)ST-53 4 2 NG (100) NG:21:P1.7,30-5 (75)ST-213 3 3 NG (67), B (33) NG:NT:P1.22,14 (33), NG:15:P1.22,14 (33), B:1:P1.12-3,4 (33)ST-269 2 2 B (50), NG (50) NG:15:P1.7-2,13-1 (50), B:1:P1.21,26 (50)ST-32 2 2 NG (100) NG:15:P1.7,16 (100)ST-22 1 1 W135 (100) W135:NT:P1.18-1,3 (100)ST-461 1 1 B (100) B:1:P1.19-35,13-1 (100)ST-103 1 1 NG (100) NG:NT:P1.5-2,10 (100)a One isolate had an incomplete MLST profile.b Serogroup:serotype:porA type (VR1, VR2).
TABLE 3 Association of clonal complexes of carried meningococci with respiratory infection episodes
Clonal complex
% of carried isolates
P valuea OR (95% CI)b
On arrival(n � 20)
During acute respiratoryinfection episodes (n � 44)
At departure(n � 151)
ST-60 35.0 16 30.5 0.045 0.4 (0.18–1.01)ST-41/44 10.0 27.3 21.2 0.061 1.5 (0.71–3.3)Unassociated 20.0 4.5 5.3ST-23 5.0 31.8 6.6 �0.001 7.1 (2.9–17.2)ST-254 0 9.1 9.3 0.9 1.1 (0.4–3.6)ST-35 10.0 4.5 8.6 0.5 0.5 (0.1–2.2)ST-178 5.0 0 6.6a By Pearson chi-square test for the comparison of isolates collected from military recruits on arrival or at departure and during acute respiratory infection episodes.b Adjusted for intake group for the comparison of isolates collected from the military recruits on arrival or at departure and during acute respiratory infection episodes.
Characterization of Carried and Invasive Meningococci
February 2012 Volume 50 Number 2 jcm.asm.org 267
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
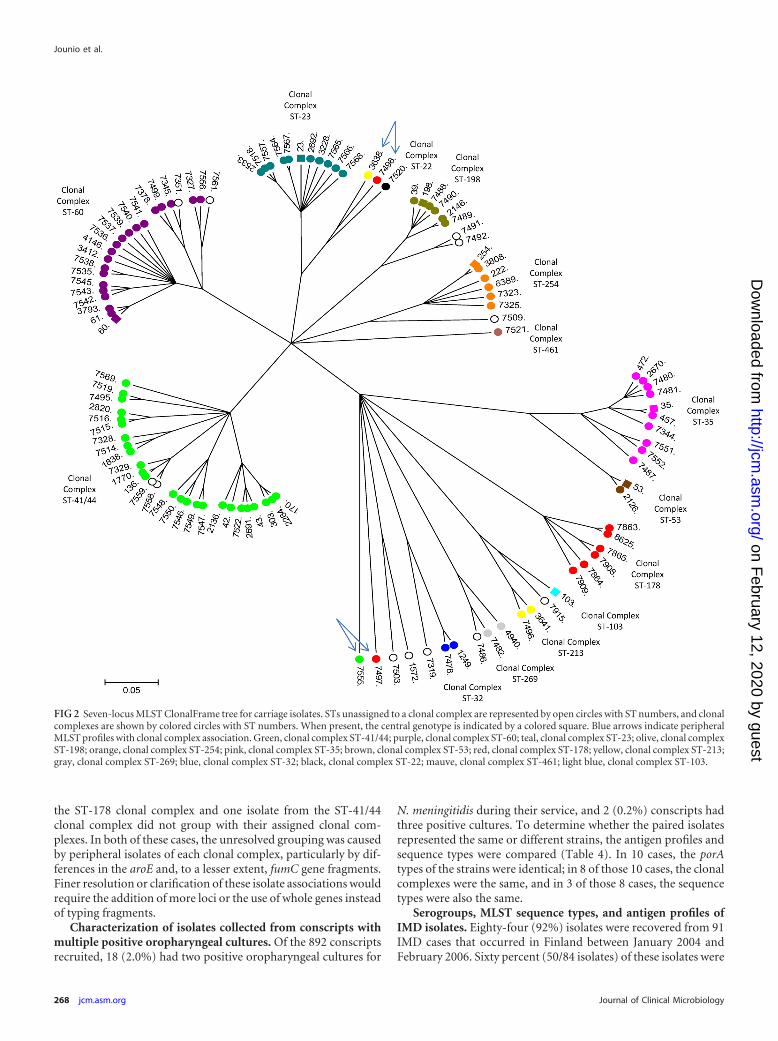
the ST-178 clonal complex and one isolate from the ST-41/44clonal complex did not group with their assigned clonal com-plexes. In both of these cases, the unresolved grouping was causedby peripheral isolates of each clonal complex, particularly by dif-ferences in the aroE and, to a lesser extent, fumC gene fragments.Finer resolution or clarification of these isolate associations wouldrequire the addition of more loci or the use of whole genes insteadof typing fragments.
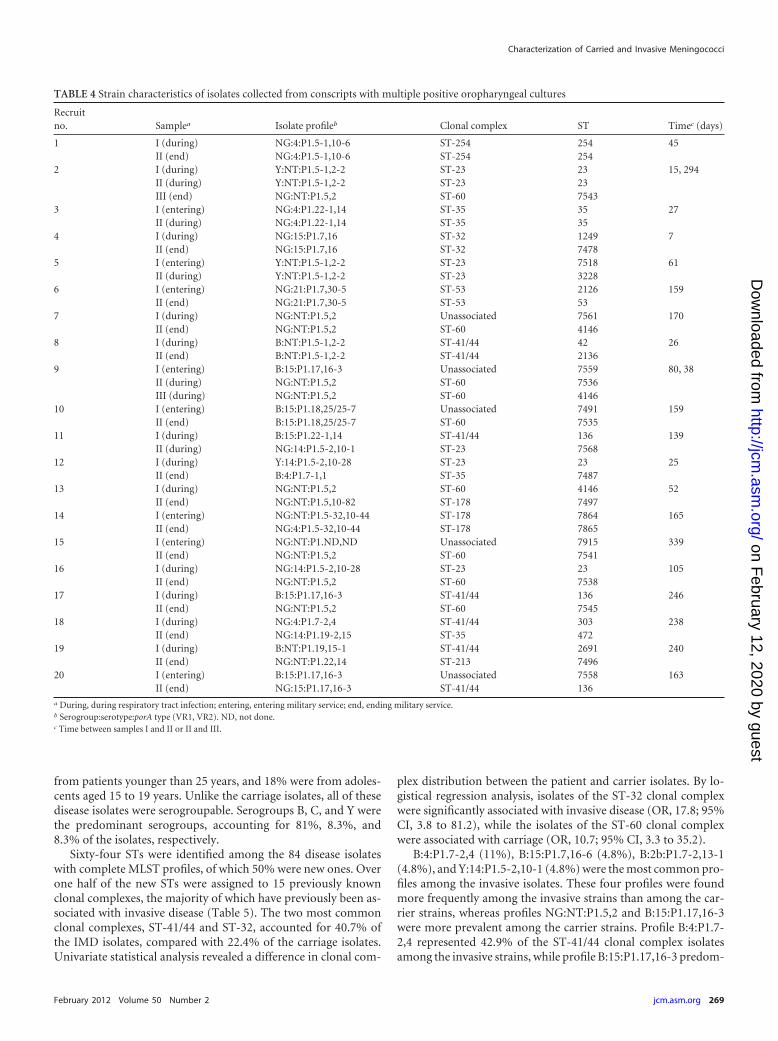
Characterization of isolates collected from conscripts withmultiple positive oropharyngeal cultures. Of the 892 conscriptsrecruited, 18 (2.0%) had two positive oropharyngeal cultures for
N. meningitidis during their service, and 2 (0.2%) conscripts hadthree positive cultures. To determine whether the paired isolatesrepresented the same or different strains, the antigen profiles andsequence types were compared (Table 4). In 10 cases, the porAtypes of the strains were identical; in 8 of those 10 cases, the clonalcomplexes were the same, and in 3 of those 8 cases, the sequencetypes were also the same.
Serogroups, MLST sequence types, and antigen profiles ofIMD isolates. Eighty-four (92%) isolates were recovered from 91IMD cases that occurred in Finland between January 2004 andFebruary 2006. Sixty percent (50/84 isolates) of these isolates were
FIG 2 Seven-locus MLST ClonalFrame tree for carriage isolates. STs unassigned to a clonal complex are represented by open circles with ST numbers, and clonalcomplexes are shown by colored circles with ST numbers. When present, the central genotype is indicated by a colored square. Blue arrows indicate peripheralMLST profiles with clonal complex association. Green, clonal complex ST-41/44; purple, clonal complex ST-60; teal, clonal complex ST-23; olive, clonal complexST-198; orange, clonal complex ST-254; pink, clonal complex ST-35; brown, clonal complex ST-53; red, clonal complex ST-178; yellow, clonal complex ST-213;gray, clonal complex ST-269; blue, clonal complex ST-32; black, clonal complex ST-22; mauve, clonal complex ST-461; light blue, clonal complex ST-103.
Jounio et al.
268 jcm.asm.org Journal of Clinical Microbiology
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
from patients younger than 25 years, and 18% were from adoles-cents aged 15 to 19 years. Unlike the carriage isolates, all of thesedisease isolates were serogroupable. Serogroups B, C, and Y werethe predominant serogroups, accounting for 81%, 8.3%, and8.3% of the isolates, respectively.
Sixty-four STs were identified among the 84 disease isolateswith complete MLST profiles, of which 50% were new ones. Overone half of the new STs were assigned to 15 previously knownclonal complexes, the majority of which have previously been as-sociated with invasive disease (Table 5). The two most commonclonal complexes, ST-41/44 and ST-32, accounted for 40.7% ofthe IMD isolates, compared with 22.4% of the carriage isolates.Univariate statistical analysis revealed a difference in clonal com-
plex distribution between the patient and carrier isolates. By lo-gistical regression analysis, isolates of the ST-32 clonal complexwere significantly associated with invasive disease (OR, 17.8; 95%CI, 3.8 to 81.2), while the isolates of the ST-60 clonal complexwere associated with carriage (OR, 10.7; 95% CI, 3.3 to 35.2).
B:4:P1.7-2,4 (11%), B:15:P1.7,16-6 (4.8%), B:2b:P1.7-2,13-1(4.8%), and Y:14:P1.5-2,10-1 (4.8%) were the most common pro-files among the invasive isolates. These four profiles were foundmore frequently among the invasive strains than among the car-rier strains, whereas profiles NG:NT:P1.5,2 and B:15:P1.17,16-3were more prevalent among the carrier strains. Profile B:4:P1.7-2,4 represented 42.9% of the ST-41/44 clonal complex isolatesamong the invasive strains, while profile B:15:P1.17,16-3 predom-
TABLE 4 Strain characteristics of isolates collected from conscripts with multiple positive oropharyngeal cultures
Recruitno. Samplea Isolate profileb Clonal complex ST Timec (days)
1 I (during) NG:4:P1.5-1,10-6 ST-254 254 45II (end) NG:4:P1.5-1,10-6 ST-254 254
2 I (during) Y:NT:P1.5-1,2-2 ST-23 23 15, 294II (during) Y:NT:P1.5-1,2-2 ST-23 23III (end) NG:NT:P1.5,2 ST-60 7543
3 I (entering) NG:4:P1.22-1,14 ST-35 35 27II (during) NG:4:P1.22-1,14 ST-35 35
4 I (during) NG:15:P1.7,16 ST-32 1249 7II (end) NG:15:P1.7,16 ST-32 7478
5 I (entering) Y:NT:P1.5-1,2-2 ST-23 7518 61II (during) Y:NT:P1.5-1,2-2 ST-23 3228
6 I (entering) NG:21:P1.7,30-5 ST-53 2126 159II (end) NG:21:P1.7,30-5 ST-53 53
7 I (during) NG:NT:P1.5,2 Unassociated 7561 170II (end) NG:NT:P1.5,2 ST-60 4146
8 I (during) B:NT:P1.5-1,2-2 ST-41/44 42 26II (end) B:NT:P1.5-1,2-2 ST-41/44 2136
9 I (entering) B:15:P1.17,16-3 Unassociated 7559 80, 38II (during) NG:NT:P1.5,2 ST-60 7536III (during) NG:NT:P1.5,2 ST-60 4146
10 I (entering) B:15:P1.18,25/25-7 Unassociated 7491 159II (end) B:15:P1.18,25/25-7 ST-60 7535
11 I (during) B:15:P1.22-1,14 ST-41/44 136 139II (during) NG:14:P1.5-2,10-1 ST-23 7568
12 I (during) Y:14:P1.5-2,10-28 ST-23 23 25II (end) B:4:P1.7-1,1 ST-35 7487
13 I (during) NG:NT:P1.5,2 ST-60 4146 52II (end) NG:NT:P1.5,10-82 ST-178 7497
14 I (entering) NG:NT:P1.5-32,10-44 ST-178 7864 165II (end) NG:4:P1.5-32,10-44 ST-178 7865
15 I (entering) NG:NT:P1.ND,ND Unassociated 7915 339II (end) NG:NT:P1.5,2 ST-60 7541
16 I (during) NG:14:P1.5-2,10-28 ST-23 23 105II (end) NG:NT:P1.5,2 ST-60 7538
17 I (during) B:15:P1.17,16-3 ST-41/44 136 246II (end) NG:NT:P1.5,2 ST-60 7545
18 I (during) NG:4:P1.7-2,4 ST-41/44 303 238II (end) NG:14:P1.19-2,15 ST-35 472
19 I (during) B:NT:P1.19,15-1 ST-41/44 2691 240II (end) NG:NT:P1.22,14 ST-213 7496
20 I (entering) B:15:P1.17,16-3 Unassociated 7558 163II (end) NG:15:P1.17,16-3 ST-41/44 136
a During, during respiratory tract infection; entering, entering military service; end, ending military service.b Serogroup:serotype:porA type (VR1, VR2). ND, not done.c Time between samples I and II or II and III.
Characterization of Carried and Invasive Meningococci
February 2012 Volume 50 Number 2 jcm.asm.org 269
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

inated in the carriage isolates, representing 28% of the isolates ofthis clonal complex (Tables 2 and 5).
ClonalFrame analysis of disease isolates. ClonalFrame analy-sis clustered 66 of the 84 disease isolates into 15 previously knownclonal complexes (Fig. 3). Twenty-two isolates are currently un-assigned to a clonal complex, and 20 are the only representatives ofSTs currently in the PubMLST Neisseria database. The two re-maining STs have been observed once (each) before: ST-1470 wasobserved in Canada in 1999 (single isolate), and ST-2003 was ob-served in the United Kingdom in 2000 (single isolate). The diseaseisolates split into 2 groups forming 2 centralized tree nodes, andwhere a clonal complex is represented by more than one ST, amore defined branch occurs, with two exceptions: the clonal com-plex ST-23 has two branches from a shared node, and one ST-41/44 isolate does not group with the other ST-41/44 clonal com-plex isolates. The differences are confined primarily to the abcZ,fumC, and gdh alleles and, to a lesser extent, the gdh allele. Aspointed out for the carriage data set, these are also peripheralclonal complex STs, and their allele assignment places themwithin the assigned ST-32 and ST-41/44 clonal complexes, respec-tively.
The clonal complex assignments of these peripheral STs, com-pared against the known ST cohort for each respective clonal com-plex in the database, show overlapping MLST profiles, such thatthe STs do not cluster with their assigned clonal complexes as seenin each tree. As in most bacterial identification, there is a gray areawhere overlapping characteristics exist, making strict confine-ment of some isolates to a predefined group complicated and, atthe very least, occasionally inconsistent. As in the carriage MLSTanalysis, finer resolution of the disease isolates would require theaddition of more typing loci or the use of whole genes.
DISCUSSION
In the present study, the carriage of N. meningitidis increased froman average of 2.2% at the beginning of military service to 18.5% atthe end of military service. The carriage rates reported here aresomewhat lower than those in previous studies, in which ratesvarying from �16% to over 70% have been reported among mil-
itary recruits (1, 15, 28, 30). These previous studies were per-formed mainly on unvaccinated populations, however. In ourstudy, a tetravalent serogroup ACYW135 polysaccharide vaccinewas given to the recruits as a part of the routine vaccination pro-gram at the beginning of their military service. This may haveexplained the low or absent level of carriage of serogroup C, Y, andW135 meningococci during the period studied, although previousstudies suggested that the effect of polysaccharide vaccination oncarriage is probably short-term (11).
During the present study (2004 to 2006), the annual incidenceof IMD in Finland (�0.9 case/100,000 inhabitants) was relativelylow compared with that in other European countries (14), and nocases of IMD occurred in the Kainuu Brigade. It is known that thecapsule plays a major role in the pathogenesis of meningococcaldisease (24), and all of our patient isolates expressed a polysaccha-ride capsule. In contrast, 65.6% of the carrier isolates were non-groupable by serological means, suggesting that at least some ofthem may have been nonencapsulated. Both the disease and sero-groupable carrier isolates were predominantly serogroup B. Whileoutbreaks and increases in the incidence of serogroup C diseasehave occurred in other parts of Europe since the late 1990s (40),this serogroup was relatively uncommon among our disease iso-lates, and none of the recruits carried meningococci expressing theserogroup C capsule in their oropharynx. Serogroup Y, which hasincreased in the United States (33) and United Kingdom (36) aswell as in Scandinavian countries, including Finland (35, 36), dur-ing the past decade, accounted for about 8% of the disease isolatesand also for about 8% of the carriage isolates, despite vaccinationof the recruits against this serogroup at the time of entering mili-tary service. This suggests that the tetravalent ACYW135 polysac-charide vaccine does not prevent the carriage of serogroup Y me-ningococci completely, although it probably provides protectionagainst the development of invasive disease.
Molecular epidemiological studies have demonstrated that in2000 to 2002, most of the meningococcal disease in Europe wascaused by strains belonging to the ST-41/44, ST-11, ST-32, ST-8,and ST-269 clonal complexes (2, 4). In the present study, executedin July 2004 to January 2006, the ST-41/44 clonal complex caused
TABLE 5 Distribution of invasive meningococcal disease isolate (n � 84) profiles within clonal complexes
Clonal complexNo. ofisolatesa
No. ofSTs
Serogroup(s)(% of isolates) Most common strain profile(s)b (% of isolates)
Unassociated 27 23 B (89), C (11) HeterogenousST-41/44 21 12 B (100) B:4:P1.7-2,4 (42.9)ST-32 12 9 B (84), C (8), Y (8) B:15:P1.7,16-6 (25)ST-23 5 4 Y (100) Y:14:P1.5-2,10-1 (60)ST-22 2 2 B (50), W135 (50) B:NT:P1.18-1,3 (50), W13:NT:P1.18-1,3 (50)ST-269 2 2 B (50), C (50) B:4:P1.18,25/25-7 (50), C:21:P1.12-1,13-1 (50)ST-60 2 2 B (50), W135 (50) B:15:P1.7,16-6 (50), W135:NT:P1.22-1,14 (50)ST-865 2 1 B (100) B:14:P1.7-2,13-2 (100)ST-162 1 1 B (100) B:NT:P1.7-2,4 (100)ST-167 1 1 Y (100) Y:1:P1.5-1,10-1 (100)ST-174 1 1 B (100) B:14:P1.5-1,10-4 (100)ST-334 1 1 B (100) B:2b:P1.7-2,13-1 (100)ST-364 1 1 B (100) B:NT:P1.12-1,13-1 (100)ST-53 1 1 B (100) B:4:P1.22-1,14 (100)ST-549 1 1 B (100) B:4:P1.5-2,10-2 (100)ST-18 1 1 B (100) B:NT:P1.5-1,10-4 (100)a Three isolates had incomplete MLST profiles.b Serogroup:serotype:porA type (VR1, VR2).
Jounio et al.
270 jcm.asm.org Journal of Clinical Microbiology
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
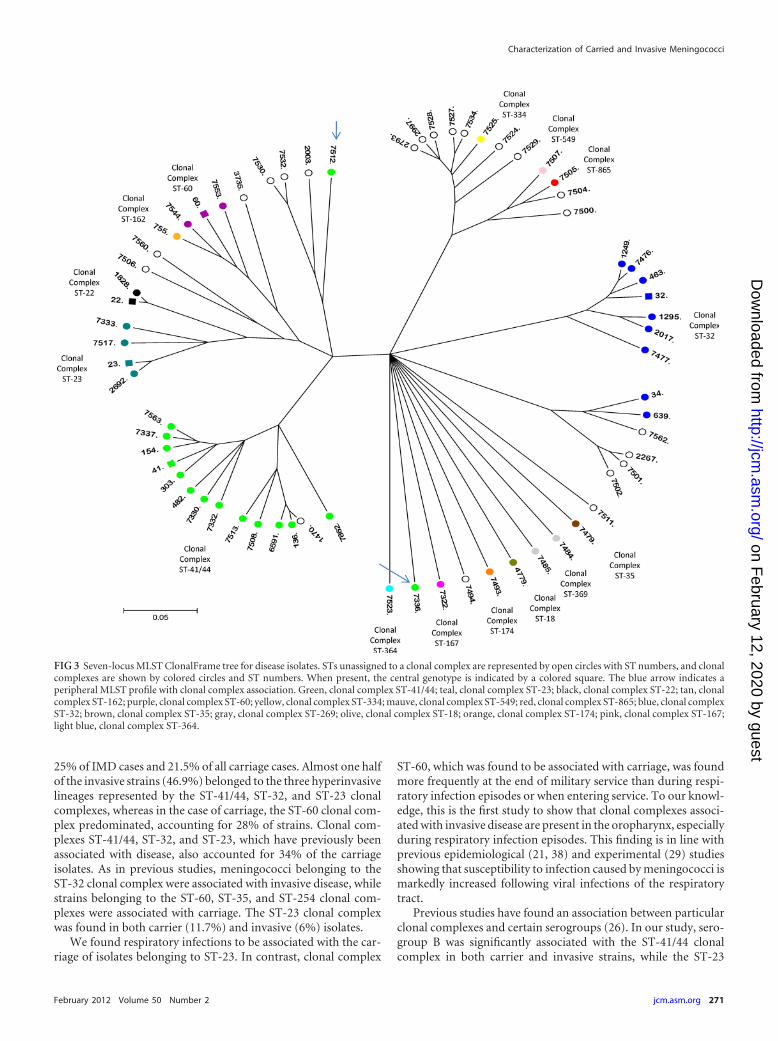
25% of IMD cases and 21.5% of all carriage cases. Almost one halfof the invasive strains (46.9%) belonged to the three hyperinvasivelineages represented by the ST-41/44, ST-32, and ST-23 clonalcomplexes, whereas in the case of carriage, the ST-60 clonal com-plex predominated, accounting for 28% of strains. Clonal com-plexes ST-41/44, ST-32, and ST-23, which have previously beenassociated with disease, also accounted for 34% of the carriageisolates. As in previous studies, meningococci belonging to theST-32 clonal complex were associated with invasive disease, whilestrains belonging to the ST-60, ST-35, and ST-254 clonal com-plexes were associated with carriage. The ST-23 clonal complexwas found in both carrier (11.7%) and invasive (6%) isolates.
We found respiratory infections to be associated with the car-riage of isolates belonging to ST-23. In contrast, clonal complex
ST-60, which was found to be associated with carriage, was foundmore frequently at the end of military service than during respi-ratory infection episodes or when entering service. To our knowl-edge, this is the first study to show that clonal complexes associ-ated with invasive disease are present in the oropharynx, especiallyduring respiratory infection episodes. This finding is in line withprevious epidemiological (21, 38) and experimental (29) studiesshowing that susceptibility to infection caused by meningococci ismarkedly increased following viral infections of the respiratorytract.
Previous studies have found an association between particularclonal complexes and certain serogroups (26). In our study, sero-group B was significantly associated with the ST-41/44 clonalcomplex in both carrier and invasive strains, while the ST-23
FIG 3 Seven-locus MLST ClonalFrame tree for disease isolates. STs unassigned to a clonal complex are represented by open circles with ST numbers, and clonalcomplexes are shown by colored circles and ST numbers. When present, the central genotype is indicated by a colored square. The blue arrow indicates aperipheral MLST profile with clonal complex association. Green, clonal complex ST-41/44; teal, clonal complex ST-23; black, clonal complex ST-22; tan, clonalcomplex ST-162; purple, clonal complex ST-60; yellow, clonal complex ST-334; mauve, clonal complex ST-549; red, clonal complex ST-865; blue, clonal complexST-32; brown, clonal complex ST-35; gray, clonal complex ST-269; olive, clonal complex ST-18; orange, clonal complex ST-174; pink, clonal complex ST-167;light blue, clonal complex ST-364.
Characterization of Carried and Invasive Meningococci
February 2012 Volume 50 Number 2 jcm.asm.org 271
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

clonal complex showed a strong association with serogroup Y ininvasive case and carriage isolates. Isolates belonging to the ST-23clonal complex are also frequently reported for patients with se-rogroup Y meningococcal disease in the United States (19). It isalso worth mentioning that serogroup C meningococci belongingto the ST-11 clonal complex, which has been responsible for mostserogroup C invasive disease cases in Europe during the last de-cade (41), were absent from both our invasive disease and carriageisolates.
We performed oropharyngeal cultures by using calcium alg-inate swabs which had been placed immediately into test tubescontaining STGG medium, which might have led to a lower yieldof positive meningococcal cultures than that for direct plating. Arecent literature review by Roberts et al. states that meningococcalcarriage should be assessed by swabbing the posterior wall of theoropharynx followed by direct plating or storage of the swab in atransport medium for less than 5 h before culturing (32). To ourknowledge, however, there are no reports on the use of an STGGtransport medium for the storage of meningococcal isolates at�70°C. STGG medium has previously been found to be suitablefor the storage of Streptococcus pneumoniae, Haemophilus influen-zae, and Moraxella catarrhalis and for nasopharyngeal swabs usedfor the detection of the same bacteria (23). In order to determineif STGG medium is also suitable for the storage of N. meningitidis,we stored the isolates in STGG medium and found over a 12-month period that the isolates survived at �70°C without changesin bacterial densities (in 12 repeated cultures) (our unpublishedobservations), suggesting that STGG medium is suitable for thestorage of N. meningitidis.
Great variation in the duration of meningococcal carriage hasbeen found previously, and sometimes a persistent carriage statemay exist for several months (5, 18). Of the 20 conscripts withmore than one positive oropharyngeal culture, 8 carried a strainwith the same clonal complex and porA type at two different timepoints. In seven of these eight cases, the period between the twosamples was less than 62 days, and in one case, it was over 5months (159 days).
To conclude, the results reported here show a significant in-crease in meningococcal carriage during military service. Our re-sults also show a clear difference in the phenotypic and genotypicdistribution of meningococci between patient and carrier strains.Furthermore, a significant association between acute upper respi-ratory tract infection and the oropharyngeal carriage of certainvirulent meningococcal clones is indicated. These findings high-light the importance of meningococcal vaccination of military re-cruits and also the need for an efficacious vaccine against sero-group B isolates.
ACKNOWLEDGMENTS
We thank Eeva Liisa Heikkinen, Elsi Saarenpää, and Leena Saarinen fortheir technical assistance. We also thank Heike Claus and Ulrich Vogelfrom the University of Würzburg for providing the serogroup Y-specificmonoclonal antibody.
This study was partly funded by the Finnish Defense Forces and theScientific Advisory Board for Defense.
REFERENCES1. Block C, et al. 1999. Factors associated with pharyngeal carriage of Neis-
seria meningitidis among Israel Defense Force personnel at the end of theircompulsory service. Epidemiol. Infect. 122:51–57.
2. Brehony C, Jolley KA, Maiden MC. 2007. Multilocus sequence typing for
global surveillance of meningococcal disease. FEMS Microbiol. Rev. 31:15–26.
3. Cartwright KA, Stuart JM, Jones DM, Noah ND. 1987. The Stonehousesurvey: nasopharyngeal carriage of meningococci and Neisseria lactamica.Epidemiol. Infect. 99:591– 601.
4. Caugant DA. 2008. Genetics and evolution of Neisseria meningitidis: im-portance for the epidemiology of meningococcal disease. Infect. Genet.Evol. 8:558 –565.
5. Caugant DA, et al. 2006. Pharyngeal carriage of Neisseria meningitidis in2-19-year-old individuals in Uganda. Trans. R. Soc. Trop. Med. Hyg. 100:1159 –1163.
6. Caugant DA, et al. 1994. Asymptomatic carriage of Neisseria meningitidisin a randomly sampled population. J. Clin. Microbiol. 32:323–330.
7. Caugant DA, Hoiby EA, Rosenqvist E, Froholm LO, Selander RK. 1992.Transmission of Neisseria meningitidis among asymptomatic military re-cruits and antibody analysis. Epidemiol. Infect. 109:241–253.
8. Caugant DA, Kristiansen BE, Froholm LO, Bovre K, Selander RK. 1988.Clonal diversity of Neisseria meningitidis from a population of asymptom-atic carriers. Infect. Immun. 56:2060 –2068.
9. Caugant DA, et al. 1987. Genetic structure of Neisseria meningitidis pop-ulations in relation to serogroup, serotype, and outer membrane proteinpattern. J. Bacteriol. 169:2781–2792.
10. Claus H, et al. 2005. Genetic analysis of meningococci carried by childrenand young adults. J. Infect. Dis. 191:1263–1271.
11. Dellicour S, Greenwood B. 2007. Systematic review: impact of meningo-coccal vaccination on pharyngeal carriage of meningococci. Trop. Med.Int. Health 12:1409 –1421.
12. Didelot X, Falush D. 2007. Inference of bacterial microevolution usingmultilocus sequence data. Genetics 175:1251–1266.
13. Didelot X, Urwin R, Maiden MC, Falush D. 2009. Genealogical typing ofNeisseria meningitidis. Microbiology 155:3176 –3186.
14. EU-IBIS Network. 2007. Invasive Neisseria meningitidis and invasive Hae-mophilus influenzae in Europe 2005. Health Protection Agency, London,United Kingdom.
15. Fraser PK, Bailey GK, Abbott JD, Gill JB, Walker DJ. 1973. Themeningococcal carrier-rate. Lancet i:1235–1237.
16. Frosch M, Gorgen I, Boulnois GJ, Timmis KN, Bitter-Suermann D.1985. NZB mouse system for production of monoclonal antibodies toweak bacterial antigens: isolation of an IgG antibody to the polysaccharidecapsules of Escherichia coli K1 and group B meningococci. Proc. Natl.Acad. Sci. U. S. A. 82:1194 –1198.
17. Gelman A, Rubin D. 1992. Inference from iterative simulation usingmultiple sequences. Stat. Sci. 7:457– 472.
18. Glitza IC, et al. 2008. Longitudinal study of meningococcal carrier rates inteenagers. Int. J. Hyg. Environ. Health 211:263–272.
19. Harrison LH, et al. 2006. Antigenic shift and increased incidence ofmeningococcal disease. J. Infect. Dis. 193:1266 –1274.
20. Holmes EC, Urwin R, Maiden MC. 1999. The influence of recombina-tion on the population structure and evolution of the human pathogenNeisseria meningitidis. Mol. Biol. Evol. 16:741–749.
21. Jansen AG, et al. 2008. Invasive pneumococcal and meningococcal dis-ease: association with influenza virus and respiratory syncytial virus activ-ity? Epidemiol. Infect. 136:1448 –1454.
21a.Jounio U, et al. 2010. Meningococcal carriage in army recruits inFinland, 2004 –2005, abstr. P049. Abstr. 17th Int. Pathog. Conf. 2010,Banff, Canada.
22. Juvonen R, et al. 2008. Risk factors for acute respiratory tract illness inmilitary conscripts. Respirology 13:575–580.
23. Kaijalainen T, Ruokokoski E, Ukkonen P, Herva E. 2004. Survival ofStreptococcus pneumoniae, Haemophilus influenzae, and Moraxella ca-tarrhalis frozen in skim milk-tryptone-glucose-glycerol medium. J. Clin.Microbiol. 42:412– 414.
24. Mackinnon FG, et al. 1993. Demonstration of lipooligosaccharideimmunotype and capsule as virulence factors for Neisseria meningitidisusing an infant mouse intranasal infection model. Microb. Pathog.15:359 –366.
25. Maiden MC. 2004. Dynamics of bacterial carriage and disease: lessonsfrom the meningococcus. Adv. Exp. Med. Biol. 549:23–29.
26. Maiden MC, et al. 1998. Multilocus sequence typing: a portable approachto the identification of clones within populations of pathogenic microor-ganisms. Proc. Natl. Acad. Sci. U. S. A. 95:3140 –3145.
Jounio et al.
272 jcm.asm.org Journal of Clinical Microbiology
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

27. Peltola H, Makela P, Pettay O, Renkonen OV, Sivonen A. 1976. Vac-cination against meningococcal group A disease in Finland 1974 –75.Scand. J. Infect. Dis. 8:169 –174.
28. Pether JV, et al. 1988. Carriage of Neisseria meningitidis: investigations ina military establishment. Epidemiol. Infect. 101:21– 42.
29. Raza MW, et al. 1999. Infection with respiratory syncytial virus enhancesexpression of native receptors for non-pilate Neisseria meningitidis onHEp-2 cells. FEMS Immunol. Med. Microbiol. 23:115–124.
30. Renkonen OV, Sivonen A, Visakorpi R. 1987. Effect of ciprofloxacin oncarrier rate of Neisseria meningitidis in army recruits in Finland. Antimi-crob. Agents Chemother. 31:962–963.
31. Ristola M, et al. 1995. Meningococcal outbreak in southern Finland.Eurosurveillance June: 2–3.
32. Roberts J, Greenwood B, Stuart J. 2009. Sampling methods to detectcarriage of Neisseria meningitidis; literature review. J. Infect. 58:103–107.
33. Rosenstein NE, et al. 1999. The changing epidemiology of meningococcaldisease in the United States, 1992–1996. J. Infect. Dis. 180:1894 –1901.
34. Stephens DS. 1999. Uncloaking the meningococcus: dynamics of carriageand disease. Lancet 353:941–942.
35. Thulin Hedberg S, Toros B, Fredlund H, Olcen P, Molling P. 2011.
Genetic characterisation of the emerging invasive Neisseria meningitidisserogroup Y in Sweden, 2000 to 2010. Euro Surveill. 16:19885.
36. Toropainen M, et al. 2011. Increase of invasive meningococcal diseasecaused by serogroup Y in Finland, 2010, poster P1078. Abstr. 21st Eur.Cong. Clin. Microbiol. Infect. Dis., Milan, Italy, 7 to 10 May 2011.
37. Toropainen M, Saarinen L, van der Ley P, Kuipers B, Kayhty H. 2001.Murine monoclonal antibodies to PorA of Neisseria meningitidis showreduced protective activity in vivo against B:15:P1.7,16 subtype variants inan infant rat infection model. Microb. Pathog. 30:139 –148.
38. Tuite AR, et al. 2010. Respiratory virus infection and risk of invasivemeningococcal disease in central Ontario, Canada. PLoS One 5:e15493.
39. Vogel U, et al. 1998. Necessity of molecular techniques to distinguishbetween Neisseria meningitidis strains isolated from patients with menin-gococcal disease and from their healthy contacts. J. Clin. Microbiol. 36:2465–2470.
40. Yazdankhah SP, Caugant DA. 2004. Neisseria meningitidis: an overviewof the carriage state. J. Med. Microbiol. 53:821– 832.
41. Yazdankhah SP, et al. 2004. Distribution of serogroups and genotypesamong disease-associated and carried isolates of Neisseria meningitidisfrom the Czech Republic, Greece, and Norway. J. Clin. Microbiol. 42:5146 –5153.
Characterization of Carried and Invasive Meningococci
February 2012 Volume 50 Number 2 jcm.asm.org 273
on February 12, 2020 by guest
http://jcm.asm
.org/D
ownloaded from





























