Embed Size (px)
Citation preview
Genetic Testing for Non-Cancerous Inheritable Diseases
Policy Number: Original Effective Date: MM.02.009 03/01/2010 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 04/01/2015 Section: Medicine Place(s) of Service: Outpatient I. Description
A genetic test is the analysis of human DNA, RNA, chromosomes, proteins, or certain metabolites in order to detect alterations related to an inheritable disorder. This can be accomplished by directly examining the DNA or RNA that makes up a gene (direct testing), looking at markers co-inherited with a disease-causing gene (linkage testing), assaying certain metabolites (biochemical testing), or examining the chromosomes (cytogenetic testing). Genetic tests are conducted for a number of purposes, including predicting disease risk, newborn screening, determining clinical management, identifying carriers, and establishing prenatal or clinical diagnoses or prognoses in individuals, families, or populations.
Expanded Carrier Screening
The American College of Medical Genetics (ACMG ) defines expanded panels as those that use next-generation sequencing to screen for mutations in many genes, as opposed to gene-by-gene screening (e.g., ethnic-specific screening or panethnic testing for cystic fibrosis). An ACMG position statement states that although commercial laboratories offer expanded carrier screening panels, there has been no professional guidance as to which disease genes and mutations to include.
For the purpose of this policy, first-degree relatives are defined as parents, full siblings, and offspring. Second-degree relatives are defined as grandparents, grandchildren, aunts, uncles, nephews, nieces, half-siblings and third-degree relatives are defined as great-grandparents, great-aunts, great-uncles, first cousins.
This policy does not address oncology-related genetic testing or pre-implantation genetic diagnosis (PGD).
II. Criteria/Guidelines
A. Genetic testing for all the inheritable diseases listed below must meet the following factors (in addition to any specific criteria) in order to be covered:
Genetic Testing for Non-Cancerous Inheritable Diseases 2
1. There must be a reasonable expectation based on family history, pedigree analysis, risk factors, and/or symptomatology that a genetically inherited condition exists.
2. The genotypes to be detected by a genetic test must be shown by scientifically valid methods to be associated with the occurrence of the disease.
3. The analytical and clinical utility validity of the test must be established (e.g., test results will influence decisions concerning disease treatment or prevention).
B. Genetic testing for the conditions listed below is covered (subject to Limitations/Exclusions and Administrative Guidelines) if after history, physical exam, pedigree analysis, and completion of conventional diagnostic studies, a definitive diagnosis remain uncertain. These include but are not limited to:
Achrondroplasia
Amino acid metabolic disturbances
Charcot-Marie Tooth disease
Classical lissencephaly
Congenital hydrocephalus
Cri-du-chat
Cystic kidney disease (including polycystic kidney, autosomal dominant)
Down's syndrome
Dwarfism
Fabry disease
Factor XIII deficiency, congenital (Factor XIII beta globulin)
Friedreich's ataxia
Gonadal dysgenesis (Turner's, XO syndrome)
Hereditary progressive muscular dystrophy (Duchene[dystrophin]-Becker's type(limb girdle muscular dystrophy Oculopharyngeal muscular dystrophy
Neurofibromatosis type 2
Osteogenesis imperfecta
Phenylketonuria
Prader-Willi-Angelman syndrome
Peutz-jeghers
Thanatophoric dysplasia
Tuberous sclerosis
Turners syndrome
Velo cardio facial syndrome
Von Hippel-Lindau syndrome
Von Willebrand's disease
C. Preconceptional or prenatal genetic testing is covered (subject to Limitations/Exclusions and of Administrative Guidelines) for a parent or prospective parent to determine carrier status of cystic fibrosis according to the ACMG recommendations. The ACMG recommends testing for specific mutations which will result in a carrier detection rate of ≥95%. Ethnicities with the highest risk for cystic fibrosis are in the Caucasian and Ashkenazi Jewish populations.
Genetic Testing for Non-Cancerous Inheritable Diseases 3
D. The following genetic tests are covered (subject to Limitations/Exclusions and Administrative Guidelines) with precertification
1. Complete analysis of the cystic fibrosis transmembrane conductance regulator (CFTR) gene is covered (subject to Limitations/Exclusions and Administrative Guidelines) in the following:
a. For patients with cystic fibrosis b. Patients with a family history of cystic fibrosis c. Males with congenital bilateral absence of the vas deferens d. Newborns with a positive newborn screening result when mutation testing, using the
standard 23-mutation panel, has a negative result
2. Chromosomal microarray analysis for diagnosing a genetic abnormality in children with apparent nonsyndromic cognitive developmental delay /intellectual disability (DD/ID) or autism spectrum disorder (ASD) when ordered by a geneticist or pediatric neurologist when all of the following conditions are met:
a. Any indicated biochemical tests for metabolic disease have been performed, and results are non-diagnostic.
b. FMR1 gene analysis (for fragile X), when clinically indicated, is negative c. In addition to a diagnosis of nonsyndromic DD/ID or ASD, the child has one or more of the
following: i. Two or more major malformations, or ii. A single major malformation or multiple minor malformations, in an infant or child who
is also small-for-dates, or iii. A single major malformation and multiple minor malformations, and
d. The results from the genetic test have the potential to impact the clinical management of the patient
3. Genetic testing for carrier status of spinal muscular atrophy (SMA) in high-risk individuals when ordered by a geneticist or pediatric neurologist meeting any of the following criteria:
a. Individuals with a positive family history of SMA, limited to first- or second-degree relatives b. Reproductive partner of an individual with SMA or is a known SMA carrier c. Individuals with a first-degree relative identified as a SMA carrier
4. Genetic testing for fragile X syndrome for individuals in any of the following risk categories where the results of the test will affect clinical management or reproductive decisions:
a. Individuals with an intellectual disability, DD, or ASD b. Prenatal testing of fetuses of known carrier mothers c. Individuals planning a pregnancy who have either of the following;
i. A first- or second- degree relative with fragile X syndrome, or ii. A first- or second- degree relative with MR, etiology unknown
5. Carrier screening for Ashkenazi Jewish individuals for:
a. Tay-Sachs disease b. Canavan disease c. Familial Dysautomia
Genetic Testing for Non-Cancerous Inheritable Diseases 4
d. Fanconi anemia e. Niemann-Pick (type A) f. Bloom syndrome g. Gaucher disease
6. Genetic testing for HFE gene mutations related to hereditary hemochromatosis:
a. For diagnostic testing when the individual with symptoms consistent with hemochromatosis and serum transferrin iron saturation is greater than or equal to 45%, but the diagnosis remain uncertain after completion of conventional testing.
b. In individuals with a family history of hemochromatosis in a first degree relative.
7. Genetic testing for predisposition to hypertrophic cardiomyopathy (HCM) for individuals having one first-degree relative with established HCM when there is a known pathogenic gene mutation present in that affective relative.
8. Genetic testing for suspected congenital Long QT Syndrome (LQTS) for individuals who do not meet the clinical criteria for LQTS but have one of the following:
a. A first- or second- degree relative with a known LQTS mutation b. A first- or second- degree relative diagnosed with LQTS by clinical means whose genetic
status is unavailable c. Signs and/or symptoms indicating a moderate to high pretest probability of LQTS, defined
as a Schwartz score of 2-3. (See Table I in the Appendix)
9. Genetic testing for Factor V Leiden and/or prothrombin G20210A mutations when any of the following criteria are met:
a. Age 50 or less , any venous thrombosis b. Age 50 or less , in patients who develop acute arterial thrombosis in the absence of other
risk factors for atherosclerotic arterial occlusive disease c. Venous thrombosis in unusual sites (such as portal hepatic, mesenteric and cerebral veins) d. Recurrent venous thrombosis e. Venous thrombosis and a first-or second- degree relative with thrombotic disease f. Venous thrombosis in pregnant women or women taking oral contraceptives g. Women with recurrent pregnancy loss or unexplained severe preeclampsia, placental
abruption, intrauterine fetal growth retardation or stillbirth h. Myocardial infarction in female smokers under age 50
10. One-time genotypic or phenotypic analysis of the enzyme Thiopurine Methyltransferase (TPMT) is covered in patients beginning therapy with azathioprine (AZA),mercaptopurine (6-MP) or thioguanine (6-TG) or in patients on thiopurine therapy with abnormal complete blood count results that do not respond to dose reduction.
11. Genetic testing for hemoglobinopathies (i.e., thalassemias and sickle cell disease) is covered when one of the following criteria is met:
a. For confirmation of a diagnosis in either of the following situations:
Genetic Testing for Non-Cancerous Inheritable Diseases 5
i. For individuals with clinical features suggestive of a hemoglobinopathy when test results from conventional studies (e.g., Iron deficiency test and serum electrophoresis) are inconclusive and have failed a trial of iron therapy
ii. Infants who are diagnosed on newborn screening as having a hemoglobinopathy
b. For carrier testing in either of the following situations:
i. When there is an affected first- or second- degree relative with thalassemia or sickle cell disease
ii. When the patient is the reproductive partner of a known carrier (disease-causing mutation of gene HBB, HBA1, or HBA2) and the couple has the capacity and intention to reproduce
12. Because of the rapidly evolving field of genetic testing, this policy does not address every genetic test available. All other genetic tests not mentioned in this policy will be reviewed based on medical necessity and the policy criteria (II.A. 1-3).
III. Limitations/Exclusions
A. The following genetic tests are not covered because they have not been shown to improve health outcomes:
1. Genetic testing to determine preterm labor 2. Genetic testing to determine warfarin sensitivity 3. Genetic testing for the diagnosis or risk assessment of Alzheimer's disease including but not
limited to testing for, apolipoprotein E epsilon 4 allele, presenilin genes or amyloid precursor gene
4. Genetic testing for helicobacter pylori treatment 5. MTHFR polymorphism testing
B. Genetic testing is not covered in the following circumstances:
1. Family members of subscribers, who themselves are not subscribers or dependents 2. Members if the results of the genetic testing are for the benefit of relatives who are not
subscribers or dependents
C. If a patient has been screened previously, CF screening results should be documented and the test should not be repeated.
D. Complete analysis of the CFTR gene by DNA sequencing is not appropriate for routine carrier screening.
E. Except as referenced in Criteria/Guidelines, genetic screening of individuals is not covered in the absence of associated signs, symptoms or complaints. General population screening for genetic disorders is not covered except where mandated by State and Federal law.
F. Laboratories that conduct genetic testing must be CLIA certified.
G. Genetic counseling is not a covered benefit.
H. Genetic tests for a specific inherited disease will be covered once per lifetime, unless new techniques that increase sensitivity are utilized.
I. Home genetic testing is not a covered benefit.
Genetic Testing for Non-Cancerous Inheritable Diseases 6
J. For a known deleterious mutation, HMSA will only cover a targeted single site analysis genetic test not a full analysis (i.e., testing for the mutation that has been identified in the family).
K. Chromosomal microarray analysis is not covered to confirm the diagnosis of a disorder or syndrome that is routinely diagnosed based on clinical evaluation alone.
L. The following expanded prenatal panel tests are not covered because the clinical utility has not been established: (This is not an all inclusive list)
1. Counsyl 2. GoodStart Select 3. Inherigen 4. Inheritest 5. Natera One Disease Panel 6. Progenity CFnxt
IV. Administrative Guidelines
A. For the genetic tests requiring precertification. Complete HMSA's Precertification Request and fax or mail the form as indicated with the following information:
1. Specify the condition for which the genetic test is being performed and if there are any known first- or second- degree relatives with the condition
2. Other types of biochemical testing apart from molecular genetic testing (enzyme activity assays, hemoglobin electrophoresis, blood chemistries, etc.), phenotypic findings and relevant clinical history and exam details
3. Specify how the results of the genetic test will impact the clinical management of the patient in terms of improving health outcomes
B. If precertification is not sought, the member will not be held responsible for payment of denied services unless an Agreement of Financial Responsibility is completed and signed.
C. Applicable codes requiring precertification:
CPT Description
81200 ASPA (aspartoacylase) (e.g. Canavan disease) gene analysis, common variants (e.g. E285A, Y231X)
81221 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g. cystic fibrosis) gene analysis ;known familial variants
81222 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g. cystic fibrosis) gene analysis; duplication/deletion variants
81223 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g. cystic fibrosis) gene analysis; full gene sequence
81224 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g. cystic fibrosis) gene analysis;; intron 8 poly-T analysis
81228 Cytogenetic constitutional (genome-wide) microarray analysis; interrogation of genomic regions for copy number variants, (e.g.,
Genetic Testing for Non-Cancerous Inheritable Diseases 7
Bacterial Artificial Chromosome [BAC] or oligo-based comparative genomic hybridization [CGH] microarray analysis)
81229 Cytogenomic constitutional (genome-wide) microarray analysis; interrogation of genomic regions for copy number and single nucleotide polymorphism (SNP) variants for chromosomal abnormalities
81240 F2 (prothrombin, coagulation factor II) (e.g. hereditary hypercoagulability) gene analysis, 20210G>A variant
81241 F5 (coagulation factor V) (e.g. hereditary hypercoagulability) gene analysis, Leiden variant
81243 FMR1 (fragile X mental retardation 1) (e.g. fragile X mental retardation) gene analysis; evaluation to detect abnormal alleles
81244 FMR1 (fragile X mental retardation 1) (e.g. fragile X mental retardation) gene analysis; characterization of alleles
81251 GBA (glucosidase, beta, acid) (e.g., Gaucher disease) gene analysis, common variants (e.g., N370S, 84GG, l444P, IVS2+1G>A)
81255 HEXA (hexosaminidase A [alpha polypeptide]) (e.g., Tay-Sachs disease) gene analysis, common variants (e.g., 1278insTATC, 1421+1G>C, G269S)
81256 HFE (hemochromatosis) gene analysis, common variants (e.g., C282Y, H63D)
81257 HBA1/HBA2 (alpha globin 1 and alpha globin 2) (e.g., alpha thalassemia, Hb Bart hydrops fetalis syndrome, HbH disease), gene analysis, for common deletions or variant (e.g., Southeast Asian, Thai, Filipino, Mediterranean, alpha3.7, alpha4.2, alpha20.5, and constant spring)
81260 Ikbkap (inhibitor of kappa light polypeptide gene enhancer in b-cells, kinase complex-associated protein) (eg, familial dysautonomia) gene analysis, common variants (eg, 2507+6t>c, r696p)
81280 Long QT syndrome gene analyses (e.g., KCNQ1, KCNH2, SCN5A, KCNE1, KCNJ2, CACNA1C, CAV3, SCN4B, AKAP, SNTA1 and ANK2); full sequence analysis
81281 Long QT syndrome gene analyses (e.g., KCNQ1, KCNH2, SCN5A, KCNE1, KCNJ2, CACNA1C, CAV3, SCN4B, AKAP, SNTA1 and ANK2); known familial sequence variant
81282 Long QT syndrome gene analyses (e.g., KCNQ1, KCNH2, SCN5A, KCNE1, KCNJ2, CACNA1C, CAV3, SCN4B, AKAP, SNTA1 and ANK2); duplication/deletion variants
81470 X-linked intellectual disability (XLID) (eg, syndromic and non-syndromic XLID); genomic sequence analysis panel, must include sequencing of at
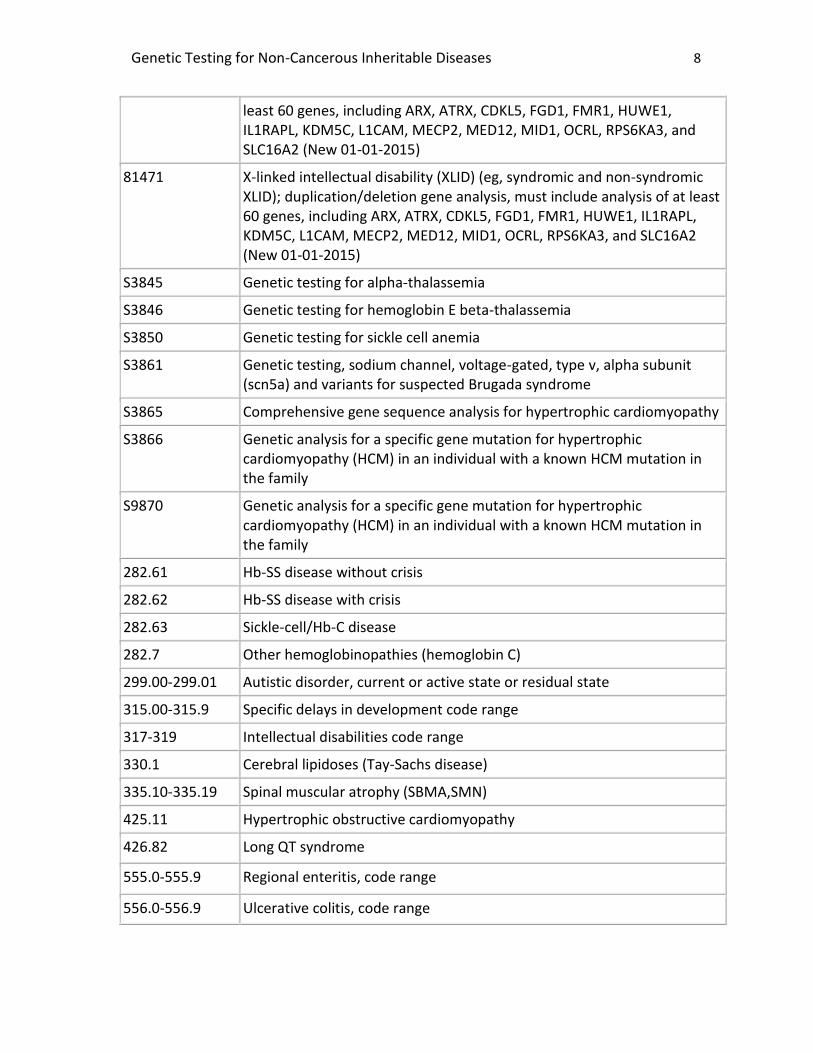
Genetic Testing for Non-Cancerous Inheritable Diseases 8
least 60 genes, including ARX, ATRX, CDKL5, FGD1, FMR1, HUWE1, IL1RAPL, KDM5C, L1CAM, MECP2, MED12, MID1, OCRL, RPS6KA3, and SLC16A2 (New 01-01-2015)
81471 X-linked intellectual disability (XLID) (eg, syndromic and non-syndromic XLID); duplication/deletion gene analysis, must include analysis of at least 60 genes, including ARX, ATRX, CDKL5, FGD1, FMR1, HUWE1, IL1RAPL, KDM5C, L1CAM, MECP2, MED12, MID1, OCRL, RPS6KA3, and SLC16A2 (New 01-01-2015)
S3845 Genetic testing for alpha-thalassemia
S3846 Genetic testing for hemoglobin E beta-thalassemia
S3850 Genetic testing for sickle cell anemia
S3861 Genetic testing, sodium channel, voltage-gated, type v, alpha subunit (scn5a) and variants for suspected Brugada syndrome
S3865 Comprehensive gene sequence analysis for hypertrophic cardiomyopathy
S3866 Genetic analysis for a specific gene mutation for hypertrophic cardiomyopathy (HCM) in an individual with a known HCM mutation in the family
S9870 Genetic analysis for a specific gene mutation for hypertrophic cardiomyopathy (HCM) in an individual with a known HCM mutation in the family
282.61 Hb-SS disease without crisis
282.62 Hb-SS disease with crisis
282.63 Sickle-cell/Hb-C disease
282.7 Other hemoglobinopathies (hemoglobin C)
299.00-299.01 Autistic disorder, current or active state or residual state
315.00-315.9 Specific delays in development code range
317-319 Intellectual disabilities code range
330.1 Cerebral lipidoses (Tay-Sachs disease)
335.10-335.19 Spinal muscular atrophy (SBMA,SMN)
425.11 Hypertrophic obstructive cardiomyopathy
426.82 Long QT syndrome
555.0-555.9 Regional enteritis, code range
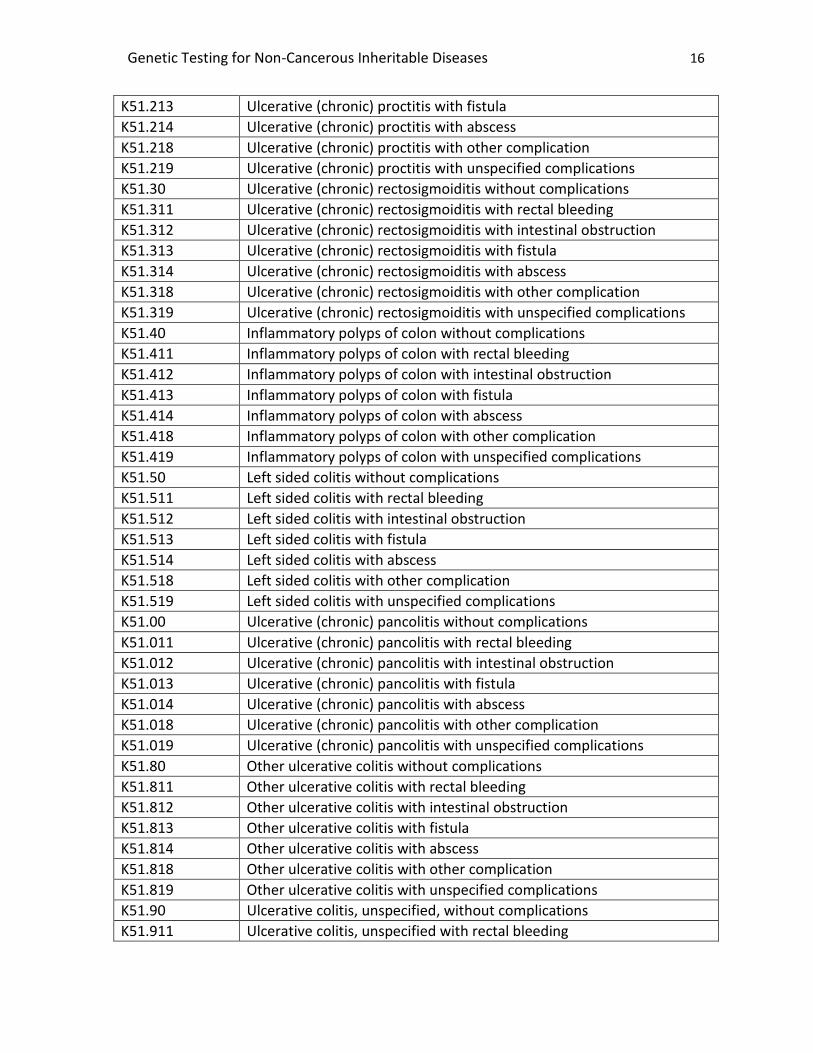
556.0-556.9 Ulcerative colitis, code range
Genetic Testing for Non-Cancerous Inheritable Diseases 9
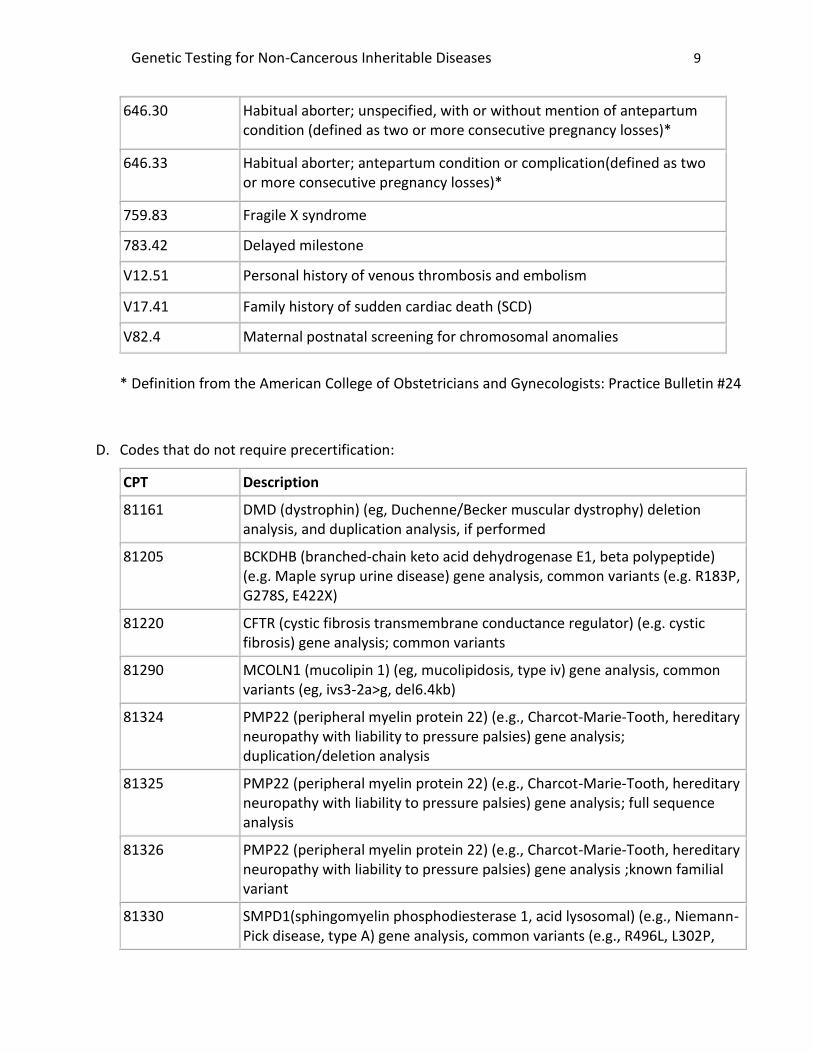
646.30 Habitual aborter; unspecified, with or without mention of antepartum condition (defined as two or more consecutive pregnancy losses)*
646.33 Habitual aborter; antepartum condition or complication(defined as two or more consecutive pregnancy losses)*
759.83 Fragile X syndrome
783.42 Delayed milestone
V12.51 Personal history of venous thrombosis and embolism
V17.41 Family history of sudden cardiac death (SCD)
V82.4 Maternal postnatal screening for chromosomal anomalies
* Definition from the American College of Obstetricians and Gynecologists: Practice Bulletin #24
D. Codes that do not require precertification:
CPT Description
81161 DMD (dystrophin) (eg, Duchenne/Becker muscular dystrophy) deletion analysis, and duplication analysis, if performed
81205 BCKDHB (branched-chain keto acid dehydrogenase E1, beta polypeptide) (e.g. Maple syrup urine disease) gene analysis, common variants (e.g. R183P, G278S, E422X)
81220 CFTR (cystic fibrosis transmembrane conductance regulator) (e.g. cystic fibrosis) gene analysis; common variants
81290 MCOLN1 (mucolipin 1) (eg, mucolipidosis, type iv) gene analysis, common variants (eg, ivs3-2a>g, del6.4kb)
81324 PMP22 (peripheral myelin protein 22) (e.g., Charcot-Marie-Tooth, hereditary neuropathy with liability to pressure palsies) gene analysis; duplication/deletion analysis
81325 PMP22 (peripheral myelin protein 22) (e.g., Charcot-Marie-Tooth, hereditary neuropathy with liability to pressure palsies) gene analysis; full sequence analysis
81326 PMP22 (peripheral myelin protein 22) (e.g., Charcot-Marie-Tooth, hereditary neuropathy with liability to pressure palsies) gene analysis ;known familial variant
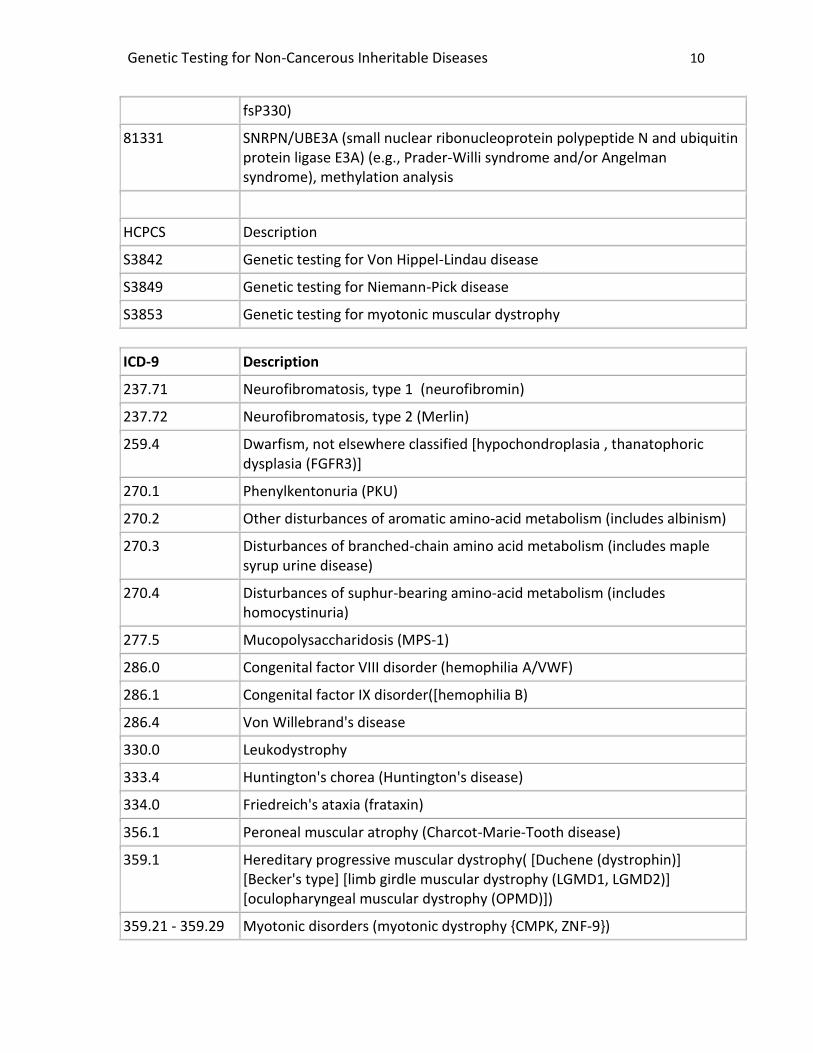
81330 SMPD1(sphingomyelin phosphodiesterase 1, acid lysosomal) (e.g., Niemann-Pick disease, type A) gene analysis, common variants (e.g., R496L, L302P,
Genetic Testing for Non-Cancerous Inheritable Diseases 10
fsP330)
81331 SNRPN/UBE3A (small nuclear ribonucleoprotein polypeptide N and ubiquitin protein ligase E3A) (e.g., Prader-Willi syndrome and/or Angelman syndrome), methylation analysis
HCPCS Description
S3842 Genetic testing for Von Hippel-Lindau disease
S3849 Genetic testing for Niemann-Pick disease
S3853 Genetic testing for myotonic muscular dystrophy
ICD-9 Description
237.71 Neurofibromatosis, type 1 (neurofibromin)
237.72 Neurofibromatosis, type 2 (Merlin)
259.4 Dwarfism, not elsewhere classified [hypochondroplasia , thanatophoric dysplasia (FGFR3)]
270.1 Phenylkentonuria (PKU)
270.2 Other disturbances of aromatic amino-acid metabolism (includes albinism)
270.3 Disturbances of branched-chain amino acid metabolism (includes maple syrup urine disease)
270.4 Disturbances of suphur-bearing amino-acid metabolism (includes homocystinuria)
277.5 Mucopolysaccharidosis (MPS-1)
286.0 Congenital factor VIII disorder (hemophilia A/VWF)
286.1 Congenital factor IX disorder([hemophilia B)
286.4 Von Willebrand's disease
330.0 Leukodystrophy
333.4 Huntington's chorea (Huntington's disease)
334.0 Friedreich's ataxia (frataxin)
356.1 Peroneal muscular atrophy (Charcot-Marie-Tooth disease)
359.1 Hereditary progressive muscular dystrophy( [Duchene (dystrophin)] [Becker's type] [limb girdle muscular dystrophy (LGMD1, LGMD2)] [oculopharyngeal muscular dystrophy (OPMD)])
359.21 - 359.29 Myotonic disorders (myotonic dystrophy {CMPK, ZNF-9})
Genetic Testing for Non-Cancerous Inheritable Diseases 11
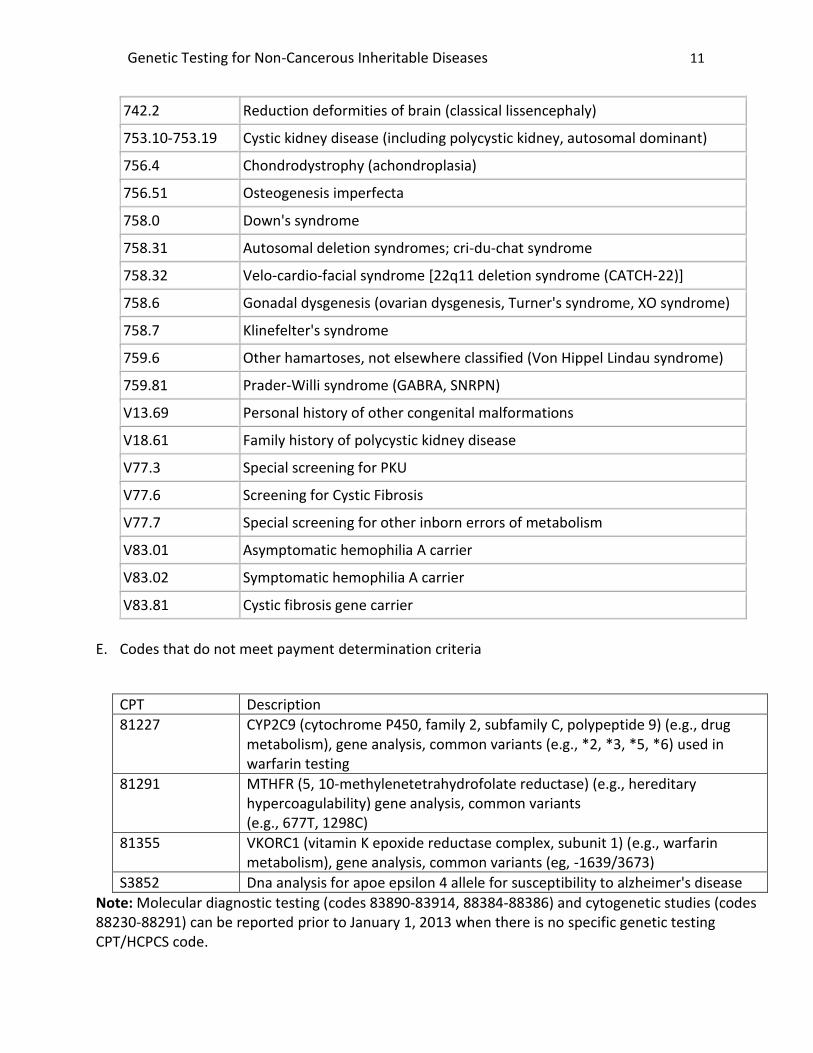
742.2 Reduction deformities of brain (classical lissencephaly)
753.10-753.19 Cystic kidney disease (including polycystic kidney, autosomal dominant)
756.4 Chondrodystrophy (achondroplasia)
756.51 Osteogenesis imperfecta
758.0 Down's syndrome
758.31 Autosomal deletion syndromes; cri-du-chat syndrome
758.32 Velo-cardio-facial syndrome [22q11 deletion syndrome (CATCH-22)]
758.6 Gonadal dysgenesis (ovarian dysgenesis, Turner's syndrome, XO syndrome)
758.7 Klinefelter's syndrome
759.6 Other hamartoses, not elsewhere classified (Von Hippel Lindau syndrome)
759.81 Prader-Willi syndrome (GABRA, SNRPN)
V13.69 Personal history of other congenital malformations
V18.61 Family history of polycystic kidney disease
V77.3 Special screening for PKU
V77.6 Screening for Cystic Fibrosis
V77.7 Special screening for other inborn errors of metabolism
V83.01 Asymptomatic hemophilia A carrier
V83.02 Symptomatic hemophilia A carrier
V83.81 Cystic fibrosis gene carrier
E. Codes that do not meet payment determination criteria
CPT Description
81227 CYP2C9 (cytochrome P450, family 2, subfamily C, polypeptide 9) (e.g., drug metabolism), gene analysis, common variants (e.g., *2, *3, *5, *6) used in warfarin testing
81291 MTHFR (5, 10-methylenetetrahydrofolate reductase) (e.g., hereditary hypercoagulability) gene analysis, common variants (e.g., 677T, 1298C)
81355 VKORC1 (vitamin K epoxide reductase complex, subunit 1) (e.g., warfarin metabolism), gene analysis, common variants (eg, -1639/3673)
S3852 Dna analysis for apoe epsilon 4 allele for susceptibility to alzheimer's disease
Note: Molecular diagnostic testing (codes 83890-83914, 88384-88386) and cytogenetic studies (codes 88230-88291) can be reported prior to January 1, 2013 when there is no specific genetic testing CPT/HCPCS code.
Genetic Testing for Non-Cancerous Inheritable Diseases 12
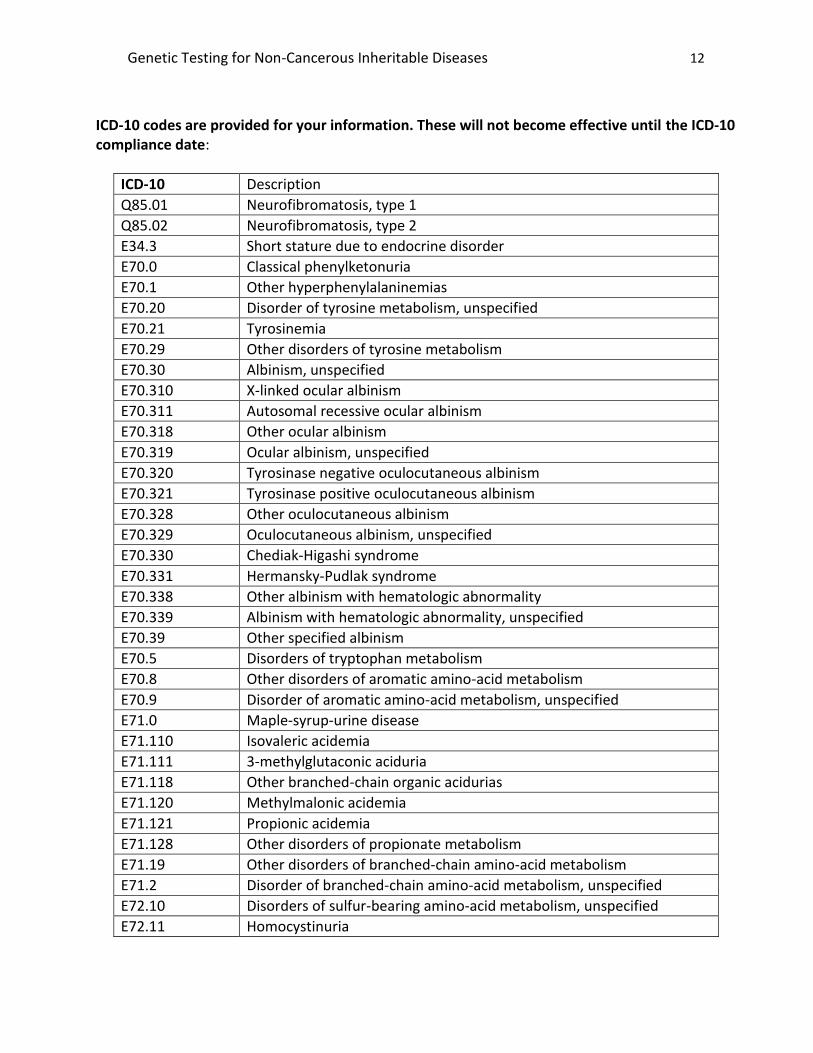
ICD-10 codes are provided for your information. These will not become effective until the ICD-10 compliance date:
ICD-10 Description
Q85.01 Neurofibromatosis, type 1
Q85.02 Neurofibromatosis, type 2
E34.3 Short stature due to endocrine disorder
E70.0 Classical phenylketonuria
E70.1 Other hyperphenylalaninemias
E70.20 Disorder of tyrosine metabolism, unspecified
E70.21 Tyrosinemia
E70.29 Other disorders of tyrosine metabolism
E70.30 Albinism, unspecified
E70.310 X-linked ocular albinism
E70.311 Autosomal recessive ocular albinism
E70.318 Other ocular albinism
E70.319 Ocular albinism, unspecified
E70.320 Tyrosinase negative oculocutaneous albinism
E70.321 Tyrosinase positive oculocutaneous albinism
E70.328 Other oculocutaneous albinism
E70.329 Oculocutaneous albinism, unspecified
E70.330 Chediak-Higashi syndrome
E70.331 Hermansky-Pudlak syndrome
E70.338 Other albinism with hematologic abnormality
E70.339 Albinism with hematologic abnormality, unspecified
E70.39 Other specified albinism
E70.5 Disorders of tryptophan metabolism
E70.8 Other disorders of aromatic amino-acid metabolism
E70.9 Disorder of aromatic amino-acid metabolism, unspecified
E71.0 Maple-syrup-urine disease
E71.110 Isovaleric acidemia
E71.111 3-methylglutaconic aciduria
E71.118 Other branched-chain organic acidurias
E71.120 Methylmalonic acidemia
E71.121 Propionic acidemia
E71.128 Other disorders of propionate metabolism
E71.19 Other disorders of branched-chain amino-acid metabolism
E71.2 Disorder of branched-chain amino-acid metabolism, unspecified
E72.10 Disorders of sulfur-bearing amino-acid metabolism, unspecified
E72.11 Homocystinuria
Genetic Testing for Non-Cancerous Inheritable Diseases 13
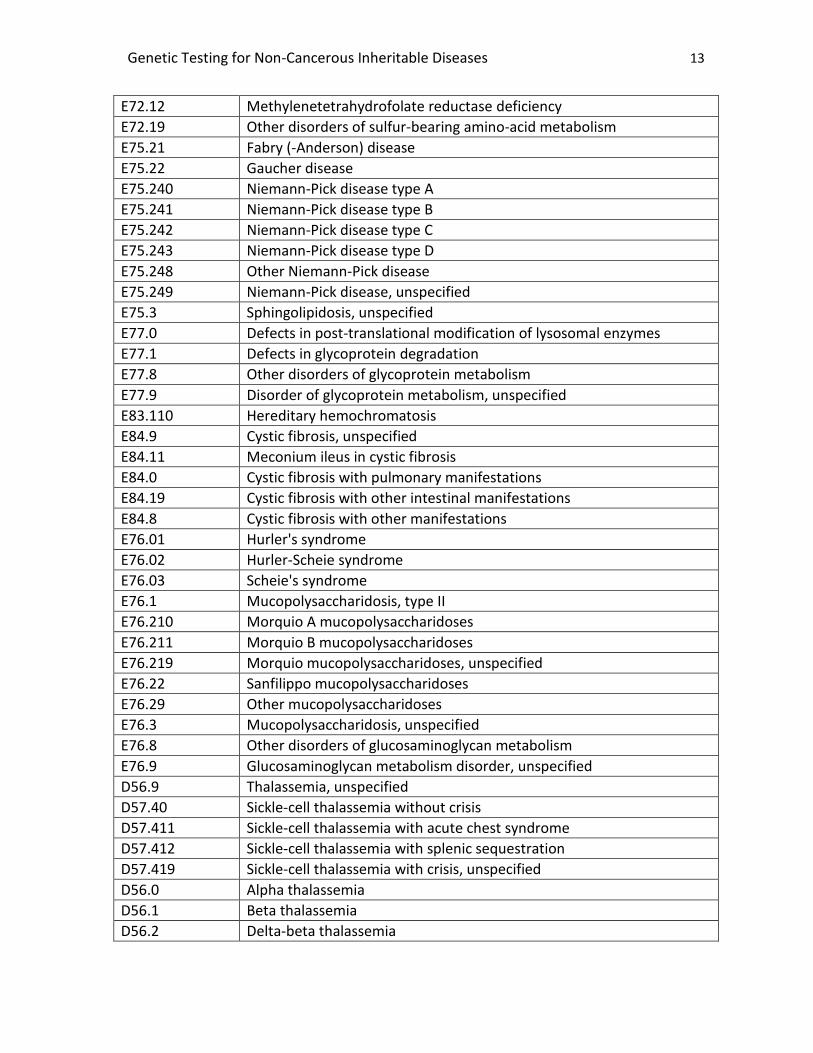
E72.12 Methylenetetrahydrofolate reductase deficiency
E72.19 Other disorders of sulfur-bearing amino-acid metabolism
E75.21 Fabry (-Anderson) disease
E75.22 Gaucher disease
E75.240 Niemann-Pick disease type A
E75.241 Niemann-Pick disease type B
E75.242 Niemann-Pick disease type C
E75.243 Niemann-Pick disease type D
E75.248 Other Niemann-Pick disease
E75.249 Niemann-Pick disease, unspecified
E75.3 Sphingolipidosis, unspecified
E77.0 Defects in post-translational modification of lysosomal enzymes
E77.1 Defects in glycoprotein degradation
E77.8 Other disorders of glycoprotein metabolism
E77.9 Disorder of glycoprotein metabolism, unspecified
E83.110 Hereditary hemochromatosis
E84.9 Cystic fibrosis, unspecified
E84.11 Meconium ileus in cystic fibrosis
E84.0 Cystic fibrosis with pulmonary manifestations
E84.19 Cystic fibrosis with other intestinal manifestations
E84.8 Cystic fibrosis with other manifestations
E76.01 Hurler's syndrome
E76.02 Hurler-Scheie syndrome
E76.03 Scheie's syndrome
E76.1 Mucopolysaccharidosis, type II
E76.210 Morquio A mucopolysaccharidoses
E76.211 Morquio B mucopolysaccharidoses
E76.219 Morquio mucopolysaccharidoses, unspecified
E76.22 Sanfilippo mucopolysaccharidoses
E76.29 Other mucopolysaccharidoses
E76.3 Mucopolysaccharidosis, unspecified
E76.8 Other disorders of glucosaminoglycan metabolism
E76.9 Glucosaminoglycan metabolism disorder, unspecified
D56.9 Thalassemia, unspecified
D57.40 Sickle-cell thalassemia without crisis
D57.411 Sickle-cell thalassemia with acute chest syndrome
D57.412 Sickle-cell thalassemia with splenic sequestration
D57.419 Sickle-cell thalassemia with crisis, unspecified
D56.0 Alpha thalassemia
D56.1 Beta thalassemia
D56.2 Delta-beta thalassemia
Genetic Testing for Non-Cancerous Inheritable Diseases 14
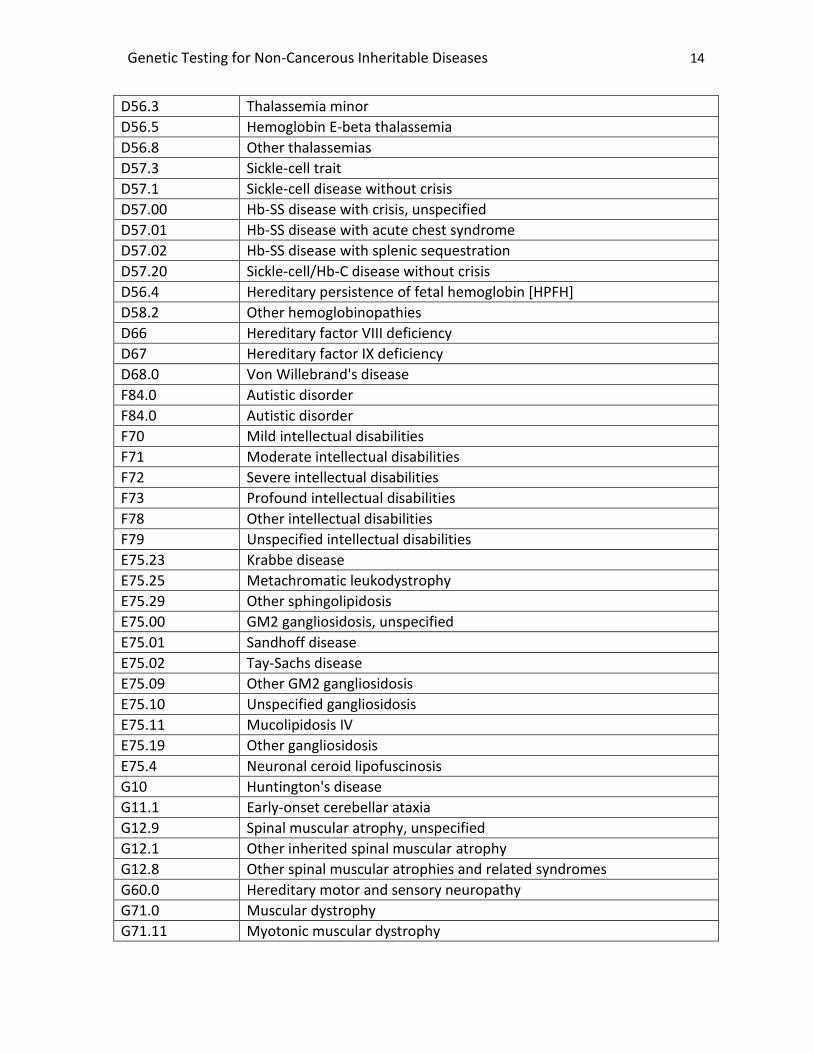
D56.3 Thalassemia minor
D56.5 Hemoglobin E-beta thalassemia
D56.8 Other thalassemias
D57.3 Sickle-cell trait
D57.1 Sickle-cell disease without crisis
D57.00 Hb-SS disease with crisis, unspecified
D57.01 Hb-SS disease with acute chest syndrome
D57.02 Hb-SS disease with splenic sequestration
D57.20 Sickle-cell/Hb-C disease without crisis
D56.4 Hereditary persistence of fetal hemoglobin [HPFH]
D58.2 Other hemoglobinopathies
D66 Hereditary factor VIII deficiency
D67 Hereditary factor IX deficiency
D68.0 Von Willebrand's disease
F84.0 Autistic disorder
F84.0 Autistic disorder
F70 Mild intellectual disabilities
F71 Moderate intellectual disabilities
F72 Severe intellectual disabilities
F73 Profound intellectual disabilities
F78 Other intellectual disabilities
F79 Unspecified intellectual disabilities
E75.23 Krabbe disease
E75.25 Metachromatic leukodystrophy
E75.29 Other sphingolipidosis
E75.00 GM2 gangliosidosis, unspecified
E75.01 Sandhoff disease
E75.02 Tay-Sachs disease
E75.09 Other GM2 gangliosidosis
E75.10 Unspecified gangliosidosis
E75.11 Mucolipidosis IV
E75.19 Other gangliosidosis
E75.4 Neuronal ceroid lipofuscinosis
G10 Huntington's disease
G11.1 Early-onset cerebellar ataxia
G12.9 Spinal muscular atrophy, unspecified
G12.1 Other inherited spinal muscular atrophy
G12.8 Other spinal muscular atrophies and related syndromes
G60.0 Hereditary motor and sensory neuropathy
G71.0 Muscular dystrophy
G71.11 Myotonic muscular dystrophy
Genetic Testing for Non-Cancerous Inheritable Diseases 15
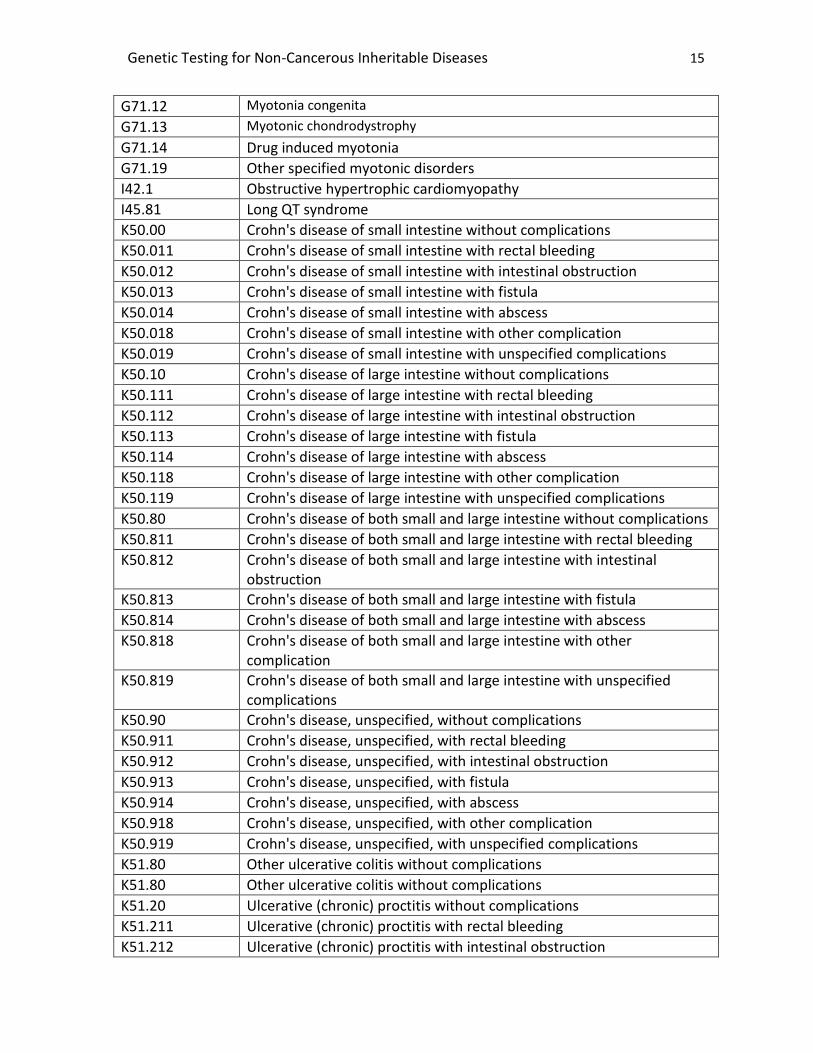
G71.12 Myotonia congenita
G71.13 Myotonic chondrodystrophy
G71.14 Drug induced myotonia
G71.19 Other specified myotonic disorders
I42.1 Obstructive hypertrophic cardiomyopathy
I45.81 Long QT syndrome
K50.00 Crohn's disease of small intestine without complications
K50.011 Crohn's disease of small intestine with rectal bleeding
K50.012 Crohn's disease of small intestine with intestinal obstruction
K50.013 Crohn's disease of small intestine with fistula
K50.014 Crohn's disease of small intestine with abscess
K50.018 Crohn's disease of small intestine with other complication
K50.019 Crohn's disease of small intestine with unspecified complications
K50.10 Crohn's disease of large intestine without complications
K50.111 Crohn's disease of large intestine with rectal bleeding
K50.112 Crohn's disease of large intestine with intestinal obstruction
K50.113 Crohn's disease of large intestine with fistula
K50.114 Crohn's disease of large intestine with abscess
K50.118 Crohn's disease of large intestine with other complication
K50.119 Crohn's disease of large intestine with unspecified complications
K50.80 Crohn's disease of both small and large intestine without complications
K50.811 Crohn's disease of both small and large intestine with rectal bleeding
K50.812 Crohn's disease of both small and large intestine with intestinal obstruction
K50.813 Crohn's disease of both small and large intestine with fistula
K50.814 Crohn's disease of both small and large intestine with abscess
K50.818 Crohn's disease of both small and large intestine with other complication
K50.819 Crohn's disease of both small and large intestine with unspecified complications
K50.90 Crohn's disease, unspecified, without complications
K50.911 Crohn's disease, unspecified, with rectal bleeding
K50.912 Crohn's disease, unspecified, with intestinal obstruction
K50.913 Crohn's disease, unspecified, with fistula
K50.914 Crohn's disease, unspecified, with abscess
K50.918 Crohn's disease, unspecified, with other complication
K50.919 Crohn's disease, unspecified, with unspecified complications
K51.80 Other ulcerative colitis without complications
K51.80 Other ulcerative colitis without complications
K51.20 Ulcerative (chronic) proctitis without complications
K51.211 Ulcerative (chronic) proctitis with rectal bleeding
K51.212 Ulcerative (chronic) proctitis with intestinal obstruction
Genetic Testing for Non-Cancerous Inheritable Diseases 16
K51.213 Ulcerative (chronic) proctitis with fistula
K51.214 Ulcerative (chronic) proctitis with abscess
K51.218 Ulcerative (chronic) proctitis with other complication
K51.219 Ulcerative (chronic) proctitis with unspecified complications
K51.30 Ulcerative (chronic) rectosigmoiditis without complications
K51.311 Ulcerative (chronic) rectosigmoiditis with rectal bleeding
K51.312 Ulcerative (chronic) rectosigmoiditis with intestinal obstruction
K51.313 Ulcerative (chronic) rectosigmoiditis with fistula
K51.314 Ulcerative (chronic) rectosigmoiditis with abscess
K51.318 Ulcerative (chronic) rectosigmoiditis with other complication
K51.319 Ulcerative (chronic) rectosigmoiditis with unspecified complications
K51.40 Inflammatory polyps of colon without complications
K51.411 Inflammatory polyps of colon with rectal bleeding
K51.412 Inflammatory polyps of colon with intestinal obstruction
K51.413 Inflammatory polyps of colon with fistula
K51.414 Inflammatory polyps of colon with abscess
K51.418 Inflammatory polyps of colon with other complication
K51.419 Inflammatory polyps of colon with unspecified complications
K51.50 Left sided colitis without complications
K51.511 Left sided colitis with rectal bleeding
K51.512 Left sided colitis with intestinal obstruction
K51.513 Left sided colitis with fistula
K51.514 Left sided colitis with abscess
K51.518 Left sided colitis with other complication
K51.519 Left sided colitis with unspecified complications
K51.00 Ulcerative (chronic) pancolitis without complications
K51.011 Ulcerative (chronic) pancolitis with rectal bleeding
K51.012 Ulcerative (chronic) pancolitis with intestinal obstruction
K51.013 Ulcerative (chronic) pancolitis with fistula
K51.014 Ulcerative (chronic) pancolitis with abscess
K51.018 Ulcerative (chronic) pancolitis with other complication
K51.019 Ulcerative (chronic) pancolitis with unspecified complications
K51.80 Other ulcerative colitis without complications
K51.811 Other ulcerative colitis with rectal bleeding
K51.812 Other ulcerative colitis with intestinal obstruction
K51.813 Other ulcerative colitis with fistula
K51.814 Other ulcerative colitis with abscess
K51.818 Other ulcerative colitis with other complication
K51.819 Other ulcerative colitis with unspecified complications
K51.90 Ulcerative colitis, unspecified, without complications
K51.911 Ulcerative colitis, unspecified with rectal bleeding
Genetic Testing for Non-Cancerous Inheritable Diseases 17
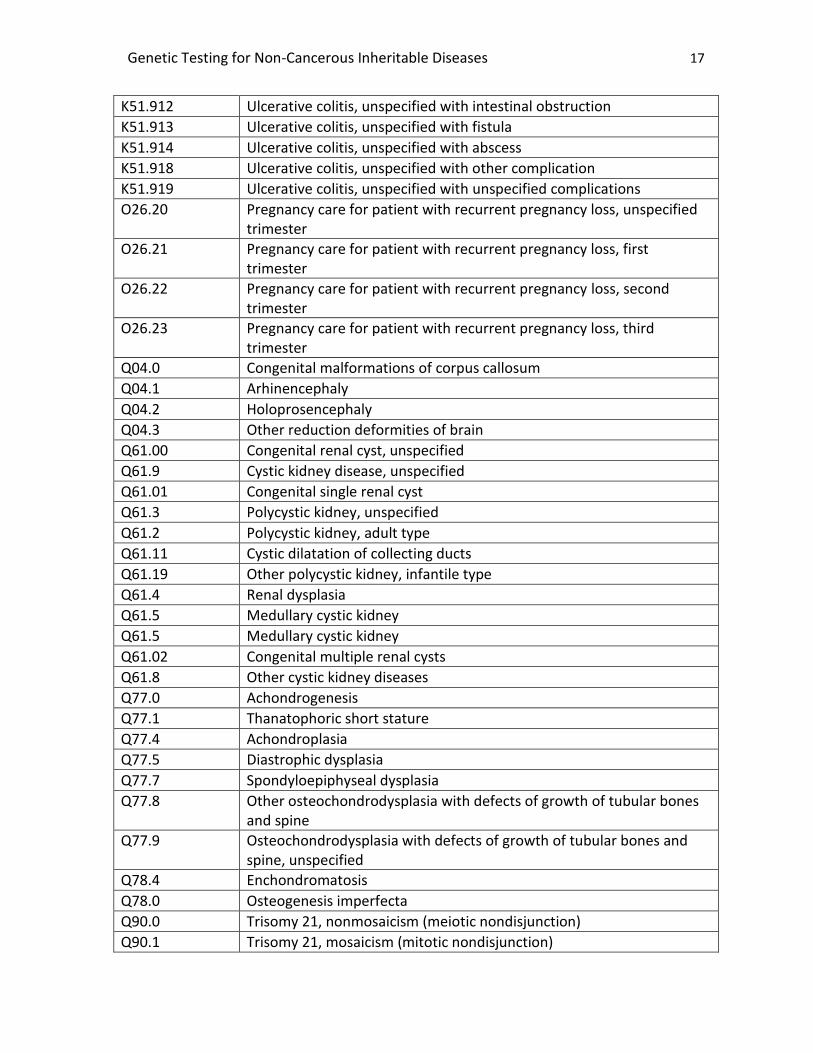
K51.912 Ulcerative colitis, unspecified with intestinal obstruction
K51.913 Ulcerative colitis, unspecified with fistula
K51.914 Ulcerative colitis, unspecified with abscess
K51.918 Ulcerative colitis, unspecified with other complication
K51.919 Ulcerative colitis, unspecified with unspecified complications
O26.20 Pregnancy care for patient with recurrent pregnancy loss, unspecified trimester
O26.21 Pregnancy care for patient with recurrent pregnancy loss, first trimester
O26.22 Pregnancy care for patient with recurrent pregnancy loss, second trimester
O26.23 Pregnancy care for patient with recurrent pregnancy loss, third trimester
Q04.0 Congenital malformations of corpus callosum
Q04.1 Arhinencephaly
Q04.2 Holoprosencephaly
Q04.3 Other reduction deformities of brain
Q61.00 Congenital renal cyst, unspecified
Q61.9 Cystic kidney disease, unspecified
Q61.01 Congenital single renal cyst
Q61.3 Polycystic kidney, unspecified
Q61.2 Polycystic kidney, adult type
Q61.11 Cystic dilatation of collecting ducts
Q61.19 Other polycystic kidney, infantile type
Q61.4 Renal dysplasia
Q61.5 Medullary cystic kidney
Q61.5 Medullary cystic kidney
Q61.02 Congenital multiple renal cysts
Q61.8 Other cystic kidney diseases
Q77.0 Achondrogenesis
Q77.1 Thanatophoric short stature
Q77.4 Achondroplasia
Q77.5 Diastrophic dysplasia
Q77.7 Spondyloepiphyseal dysplasia
Q77.8 Other osteochondrodysplasia with defects of growth of tubular bones and spine
Q77.9 Osteochondrodysplasia with defects of growth of tubular bones and spine, unspecified
Q78.4 Enchondromatosis
Q78.0 Osteogenesis imperfecta
Q90.0 Trisomy 21, nonmosaicism (meiotic nondisjunction)
Q90.1 Trisomy 21, mosaicism (mitotic nondisjunction)
Genetic Testing for Non-Cancerous Inheritable Diseases 18
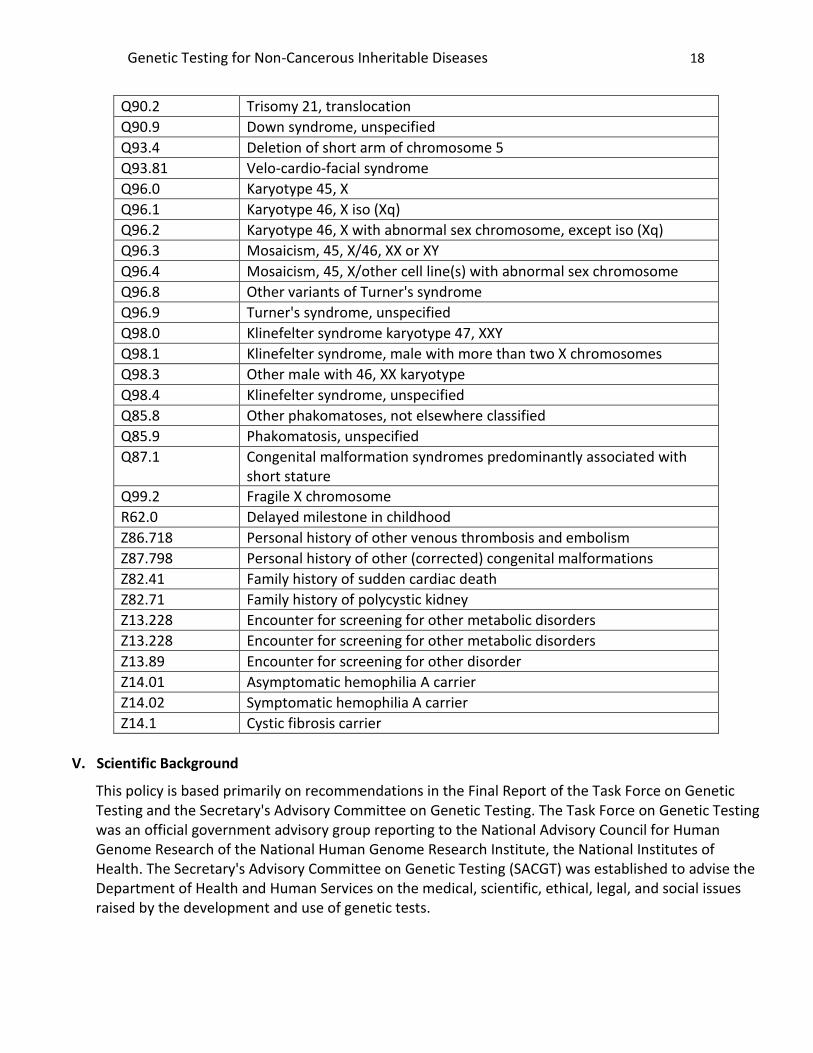
Q90.2 Trisomy 21, translocation
Q90.9 Down syndrome, unspecified
Q93.4 Deletion of short arm of chromosome 5
Q93.81 Velo-cardio-facial syndrome
Q96.0 Karyotype 45, X
Q96.1 Karyotype 46, X iso (Xq)
Q96.2 Karyotype 46, X with abnormal sex chromosome, except iso (Xq)
Q96.3 Mosaicism, 45, X/46, XX or XY
Q96.4 Mosaicism, 45, X/other cell line(s) with abnormal sex chromosome
Q96.8 Other variants of Turner's syndrome
Q96.9 Turner's syndrome, unspecified
Q98.0 Klinefelter syndrome karyotype 47, XXY
Q98.1 Klinefelter syndrome, male with more than two X chromosomes
Q98.3 Other male with 46, XX karyotype
Q98.4 Klinefelter syndrome, unspecified
Q85.8 Other phakomatoses, not elsewhere classified
Q85.9 Phakomatosis, unspecified
Q87.1 Congenital malformation syndromes predominantly associated with short stature
Q99.2 Fragile X chromosome
R62.0 Delayed milestone in childhood
Z86.718 Personal history of other venous thrombosis and embolism
Z87.798 Personal history of other (corrected) congenital malformations
Z82.41 Family history of sudden cardiac death
Z82.71 Family history of polycystic kidney
Z13.228 Encounter for screening for other metabolic disorders
Z13.228 Encounter for screening for other metabolic disorders
Z13.89 Encounter for screening for other disorder
Z14.01 Asymptomatic hemophilia A carrier
Z14.02 Symptomatic hemophilia A carrier
Z14.1 Cystic fibrosis carrier
V. Scientific Background
This policy is based primarily on recommendations in the Final Report of the Task Force on Genetic Testing and the Secretary's Advisory Committee on Genetic Testing. The Task Force on Genetic Testing was an official government advisory group reporting to the National Advisory Council for Human Genome Research of the National Human Genome Research Institute, the National Institutes of Health. The Secretary's Advisory Committee on Genetic Testing (SACGT) was established to advise the Department of Health and Human Services on the medical, scientific, ethical, legal, and social issues raised by the development and use of genetic tests.
Genetic Testing for Non-Cancerous Inheritable Diseases 19
Many genetic tests are imperfect predictors of either existing disease or disease susceptibility, particularly when used in the context of population screening, where individuals without family histories of disease, risk factors or symptoms are tested. For example, the probability exists that a disease may still occur, even when a negative test result is obtained. Conversely, a specific disease may not occur when there is a positive test result. While these concepts hold true for at-risk individuals as well, the probability of both these occurrences is greater in population screening, so test results are more difficult to interpret in a manner that will meaningfully impact health outcomes. With a few limited exceptions (e.g., PKU testing), general screening of populations for diseases that can be attributed to genetic mutations is not advocated in the published scientific literature.
Ideally, peer-reviewed literature on the performance and indications for the test should be available. The evaluation of a genetic test focuses on these main principles: Analytic validity (technical accuracy of the test in detecting a mutation that is present or in excluding a mutation that is absent); Clinical validity (diagnostic performance of the test [sensitivity, specificity, positive and negative predictive values] in detecting clinical disease); and clinical utility (how results of the diagnostic test will be used to change management of the patient and whether these changes in management lead to clinically important improvements in health outcomes).
Analytical validity
Analytical validity is an indicator of how well a test measures the property or characteristic it is intended to measure, and it is made up of three components Analytical sensitivity: the test is positive when the relevant gene mutation is present. Analytical specificity: the test is negative when the gene mutation is absent and reliability: the test obtains the same result each time.
Clinical Validity
Clinical validity in genetic testing is a measurement of the accuracy with which a test identifies or predicts a clinical condition and involves the following:
1. Clinical sensitivity: the probability that the test is positive if the individual being tested actually has the disease or a predisposition to the disease.
2. Clinical specificity: the probability that the test is negative if the individual does not have the disease or a predisposition to the disease.
3. Positive predictive value: the probability that an individual with positive test results will get the disease.
4. Negative predictive value: the probability that an individual with negative test results will not get the disease.
5. Heterogeneity: different mutations within the same gene may cause the same disease and can result in different degrees of disease severity; a failure to detect all disease-related mutations reduces a test's clinical sensitivity.
6. Penetrance: the probability that the disease will appear when a disease-related genotype is present. Penetrance is incomplete when other genetic or environmental factors must be present for a disease to develop.
The clinical utility of the test must be established.
Genetic Testing for Non-Cancerous Inheritable Diseases 20
The development of genetic tests that can diagnose or predict disease occurrence has far outpaced the development of interventions to treat, ameliorate or prevent those same diseases. Clinical utility refers to the ability of genetic test results, either positive or negative, to provide information that is of value in the clinical setting. Specifically for positive test results, this could involve instituting treatments or surveillance measures, making decisions concerning future conception, or avoiding harmful treatments. Negative test results can have clinical utility in that unnecessary treatments or surveillance can be avoided. In the absence of such interventions, the benefits of testing are limited, and in fact, can cause psychological harm.
Genetic testing of children to confirm current symptomatology or predict adult onset diseases is not considered medically necessary unless direct medical benefit will accrue to the child and in the case of adult onset disease, this benefit would be lost by waiting until the child has reached adulthood.
It is generally accepted in the published literature that unless useful medical intervention can be offered to children as a result of testing, formal testing should wait until the child is old enough to understand the consequences of testing and request it for him or herself. Ethical concerns related to the testing of children include the breach of confidentiality that is required by revealing test results to parents, the lack of ability to counsel the child in a meaningful way regarding the risks and benefits of testing, the impact a positive test could have in terms of discrimination, and the potential psychological damage that could occur from distorting a family’s perception of the child.
Expanded Carrier Screening Panels
A 2011 study by Bell et al described the development of an ECS panel for 448 severe recessive diseases of childhood, using next generation sequencing (NGS). The authors tested 104 unrelated DNA samples. They noted that although technical standards and guidelines for laboratory-developed genetic testing for rare disorders in accredited laboratories have been established, there are several challenges in their adoption for NGS and for bioinformatic-based testing of many conditions. Specific national standards for quality assurance, quality control, test accessioning and reporting, and proficiency evaluation do not currently exist. Also, issues of specificity and false positives are complex when hundreds of genes are being sequenced simultaneously and need to be addressed. Lazarin et al (2013) reported on carrier status from an ethnically diverse clinical sample of 23,452 individuals. Using the Counsyl test screening platform, they assayed 417 disease-causing mutations associated with 108 recessive diseases. Of the individuals tested, 5633 (24%) were heterozygous for at least 1 condition, and 5.2% were identified as carriers for multiple disorders. Of 127 carrier couples identified (ie, pairs of individuals identified as partners by self-report who were both found to share heterozygosity for at least 1 disease), 47 (37%) were for alpha-1 antitrypsin deficiency, a condition which has reduced penetrance, variable severity, and uncertain clinical presentation in the newborn period and into adulthood. The American Thoracic Society discourages genetic testing for alpha-1 antitrypsin deficiency in asymptomatic adults with no increased risk for this disease.
In March 2011, six U.S. academic centers convened focus groups to examine genetics professionals’ views on ECS. Forty genetics professionals, including those specializing in medical genetics, pediatric genetics, genetic counseling, public health genetics, primary care, laboratory medicine, and law and bioethics, aimed to clarify how genetics professionals view potential benefits and challenges of ECS. Overall, participants agreed that there was financial value in ECS panels compared with conventional
Genetic Testing for Non-Cancerous Inheritable Diseases 21
carrier screening. However, their findings highlighted major limitations of ECS. Concerns included the following:
Use of ECS panels would be a significant departure from clinical practice guidelines in genetic and reproductive healthcare in the U.S., and carrier screening guidelines currently exist for only a few of the genetic disorders evaluated by ECS panels.
Technical limitations of ECS include the inability to fully rule out the possibility of severe recessive diseases due to rare mutations that could be identified by alternative methods such as DNA sequencing, and, there are gaps in coverage of both specific genes and individual mutations included in the ECS panels.
Current ECS panels typically examine only a fraction of the many genes associated with genetic disorders and limit their evaluation to common genetic mutations within those genes.
Reproductive healthcare providers might fail to recommend more conventional forms of targeted genetic evaluation, such as screening tests indicated by a couple’s ethnicity, based on erroneous perceptions about the coverage of ECS products being marketed as universal in scope. Less common mutations in specific ethnic populations may not be included, and couples may be falsely reassured by “negative” results.
As the number of individual assays on a multiplexed genetic test increases, the likelihood of erroneous results (eg, false positives) and clinically ambiguous findings (eg, variants of unknown significance) increases significantly.
As carrier screening panels expand to include less common genetic diseases, interpretation of mutation results is hindered by lack of data on clinical phenotypes associated with rare variants.
In 2013, Wienke et al issued a commentary on the limitations of using ECS panels. The authors stated that:
Patients may not understand the nature of every disease on the panel, confounding the process of informed consent.
In practice, it is infeasible to inform patients of the nature of each condition tested, and many healthcare providers are unfamiliar with some of the conditions tested, making it difficult to communicate residual risk and actionability of information obtained.
It is possible that a test primarily designed to assess reproductive risk will inadvertently identify an asymptomatic individual with the disease, which poses many challenges. These include unanticipated psychosocial burden to patients, and a burden to the healthcare system in general as a person identified through this method may undergo additional baseline testing for the disease and receive follow-up for the disease that may otherwise have been unnecessary.
VI. Important Reminder
The purpose of this Medical Policy is to provide a guide to coverage. This Medical Policy is not intended to dictate to providers how to practice medicine. Nothing in this Medical Policy is intended to discourage or prohibit providing other medical advice or treatment deemed appropriate by the treating physician.
Genetic Testing for Non-Cancerous Inheritable Diseases 22
Benefit determinations are subject to applicable member contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control.
This Medical Policy has been developed through consideration of the medical necessity criteria under Hawaii’s Patients’ Bill of Rights and Responsibilities Act (Hawaii Revised Statutes §432E-1.4), generally accepted standards of medical practice and review of medical literature and government approval status. HMSA has determined that services not covered under this Medical Policy will not be medically necessary under Hawaii law in most cases. If a treating physician disagrees with HMSA’s determination as to medical necessity in a given case, the physician may request that HMSA consider the application of this Medical Policy to the case at issue.
VII. References
1. Secretary's Advisory Committee on Genetic Testing. A public consultation on oversight of genetic tests. December 1, 1999 - January 31, 2000. National Institute of Health. Verified 10/25/2010
2. U.S. Preventive Services Task Force. Screening for hemochromatosis: Recommendation statement. Ann Intern Med. 2006 Aug 1;145(3):204-208
3. ACMG Policy Statement: Cystic fibrosis Population Carrier Screening: 2004 Revision of ACMG mutation panel. Reaffirmed 2013.
4. American College of Medical Genetic (ACMG) Practice Guidelines; Carrier screening for Spinal Muscular Atrophy. Genetics in Medicine 2008:10( 11) Reaffirmed 2013.
5. ACMG Practice Guidelines: Carrier screening in individuals of Ashkenazi descent. Genet Med 2008:10(1):54 –56. Reaffirmed 2013.
6. ACMG Practice Guidelines; Clinical genetics evaluation in identifying the etiology of autism spectrum disorders. 2013 Guideline Revisions
7. ACMG Practice Guidelines; Fragile X Syndrome: Diagnostic and carrier testing. October 2005 8. ACMG Consensus Statement on Factor V Leiden Mutation testing. Reaffirmed 05/14/2007 9. BCBSA Medical Policy Reference Manual. Pharmacogenetic and Metabolite Markers for Patients
Treated with Thiopurines #2.04.19. Last reviewed May 2014 10. ACMG Standards and Guidelines for Clinical Genetics Laboratories. Technical Standards and
Guidelines: Venous Thromboembolism (Factor V Leiden and Prothrombin 20210G>A Testing): A Disease-Specific Supplement to the Standards and Guidelines for Clinical Genetics Laboratories. 2006.
11. Bell CJ, Dinwiddie DL, Miller NA et al. Carrier testing for severe childhood recessive diseases by next generation sequencing. Sci Transl Med 2011; 3(65):65ra4.
12. BCBSA Medical Advisory Panel. Special Report: Evaluating evidence supporting a role for genetic markers assessing disease predisposition and prognosis, or predicting response to therapy. June 10, 2008
13. BCBSA Technology Evaluation Center Genetic testing for long QT syndrome. TEC Assessment 2007; volume 22 tab 9
14. American College of Obstetricians and Gynecologists (ACOG) and the American College of Medical Genetics (ACMG). Preconception and Prenatal Carrier Screening for Cystic Fibrosis: Clinical and Laboratory Provider Guidelines. ACOG/ACMG Position Statement. ACOG; 2001
15. Genetic testing for HFE gene mutations related to hereditary hemochromatosis. BCBSA Technology Evaluation Center. Chicago, IL: April 2002; 16(22)
Genetic Testing for Non-Cancerous Inheritable Diseases 23
16. Special Report: Molecular karyotyping by array comparative genomic hybridization (aCGH) for the genetic evaluation of patients with developmental delay/mental retardation and autism spectrum disorder. BCBSA Medical Advisory Panel. December 2008
17. ACOG. Practice Bulletin #24. Testing guidelines for early recurrent pregnancy loss. 18. Wienke S, Brown K, Farmer M et al. Expanded carrier screening panels-does bigger mean better? J
Community Genet 2013. 19. BCBSA Medical Policy Reference Manual. Genetic Testing for Helicobacter pylori Treatment-
Archived. #2.04.50. Reviewed July 2012 Archived 20. Lazarin GA, Haque IS, Nazareth S et al. An empirical estimate of carrier frequencies for 400+ causal
Mendelian variants: results from an ethnically diverse clinical sample of 23,453 individuals. Genet Med 2013; 15(3):178-86
21. BCBSA Medical Policy Reference Manual. Genetic Testing for Hereditary Hemochromatosis. #2.04.80. Reviewed April 2014
22. BCBSA Medical Policy Reference Manual. Chromosomal Microarray (CMA) Analysis for the Genetic Evaluation of Patients with Developmental Delay/Intellectual Disability or Autism Spectrum Disorder. #2.04.59. Reviewed March 2014
23. BCBSA Tec Assessment. Genetic Testing for Predisposition to Inherited Hypertrophic Cardiomyopathy. Vol. 34, No.11. August 2010
24. National Institute of Health. Genetics Home Reference. Sickle cell disease. Reviewed February 2007
25. BCBSA Medical Policy Reference Manual. Genetic Testing for FMR1 Mutations (Including Fragile X Syndrome). #2.04.83. Reviewed June 2014
26. BCBSA Medical Policy Reference Manual. Genetic Testing for Predisposition to Inherited Hypertrophic Cardiomyopathy. #2.02.28. Reviewed December 2013
27. Genetic Testing for Cystic Fibrosis. NIH Consensus Statement 1997 Apr 14-16; 15(4): 1-37. 28. ACMG Practice Guideline: Lack of Evidence for MTHFR Polymorphism Testing. Genet Med
2013:15(2):153–156 29. ACOG. Practice Bulletin #124. Inherited Thrombophilia in Pregnancy. September 11, 2011. 30. BCBSA Medical Policy Reference Manual. Carrier Testing for Genetic Diseases. #2.04.107. Last
reviewed: October 2014. 31. Grody WW, Thompson BH, Gregg AR et al. ACMG position statement on prenatal/preconception
expanded carrier screening. Genet Med 2013; 15(6):482-3.
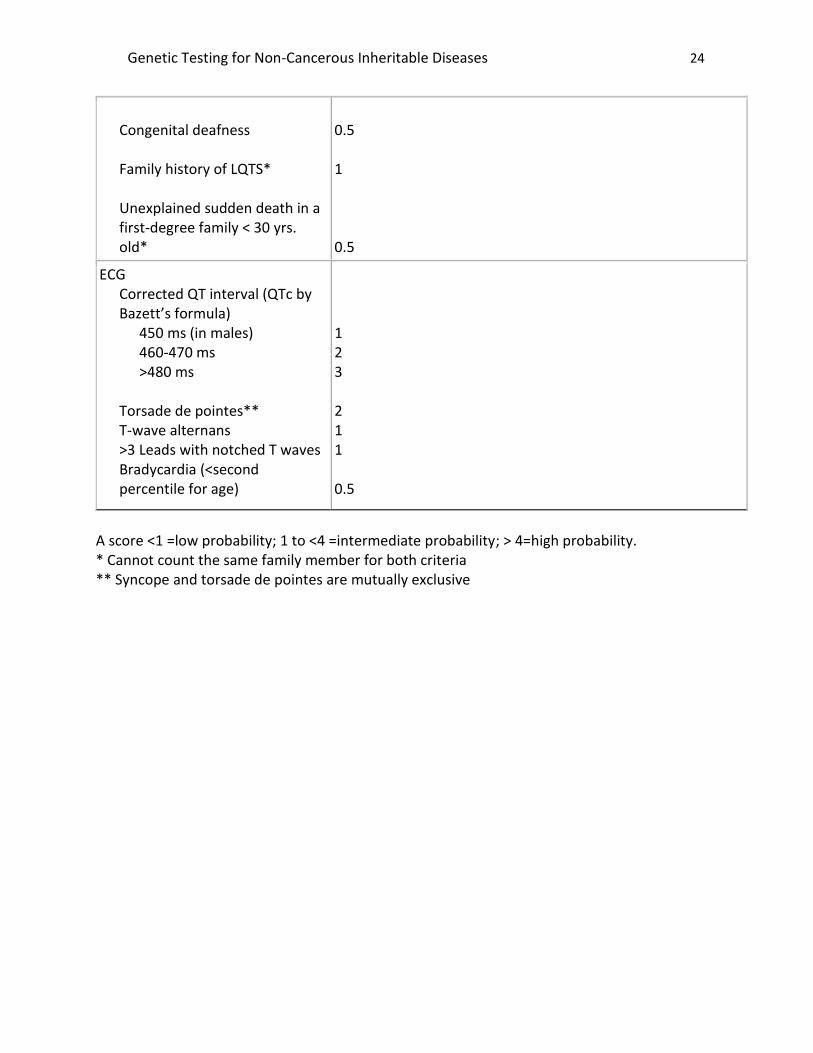
VIII. Appendix
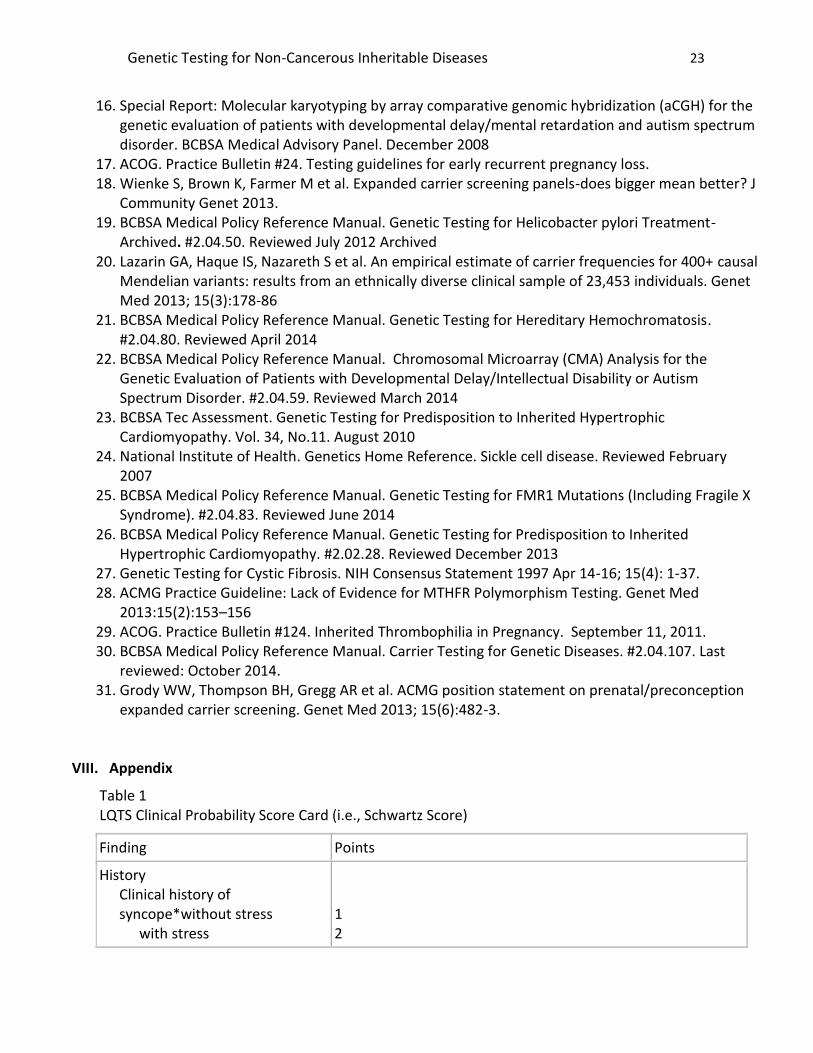
Table 1 LQTS Clinical Probability Score Card (i.e., Schwartz Score)
Finding Points
History Clinical history of syncope*without stress
with stress
1 2
Genetic Testing for Non-Cancerous Inheritable Diseases 24
Congenital deafness Family history of LQTS* Unexplained sudden death in a first-degree family < 30 yrs. old*
0.5 1 0.5
ECG Corrected QT interval (QTc by Bazett’s formula)
450 ms (in males) 460-470 ms >480 ms
Torsade de pointes** T-wave alternans >3 Leads with notched T waves Bradycardia (<second percentile for age)
1 2 3 2 1 1 0.5
A score <1 =low probability; 1 to <4 =intermediate probability; > 4=high probability. * Cannot count the same family member for both criteria ** Syncope and torsade de pointes are mutually exclusive