Embed Size (px)
Citation preview

Generalizability of economic evaluations: Using results from other geographic areas or from multinational trials to help inform health care decision making in Canada
Ron GoereeProgram for Assessment of Technology in Health (PATH)Clinical Epidemiology & Biostatistics (CE&B), McMaster UniversityCenter for Evaluation of Medicines (CEM), St. Joseph’s Hospital Hamilton, Ontario
April 26, 2005.

Core Funding for this project was provided by a CCOHTA HTA Capacity Building Grant(2004/05 - Grant #67)

Acknowledgements
PATH (Ron Goeree, Natasha Burke, Gord Blackhouse, Daria O’Reily, Jean-Eric Tarride) is core funded by the Ontario Ministry of Health & Long-term Care (MOHLTC).
New program of research on the evaluation of new and existing health care technologies.
Other collaborators:Andrea Manca, Mark Sculpher (York, UK)
Andrew Willan (University of Toronto)

Background
Pressure on health care decision makers to make more efficient use of scarce health care resources
Increasing demand for ‘high quality’ effectiveness data (RCT or meta-analyses RCTs)
Also increasing demands to determine ‘value for money’ through high quality economic appraisals
Includes stochastic trials (concurrent clinical & economic) and decision analytic models

Background (2)
Clinical and economic evaluations are expensive and time consuming (sometimes taking years)
Ever growing list of technologies that need to be assessed or re-assessed over time
Often funding decisions need to be made today (or at least earlier than years needed to complete trials)
Fortunately, published evaluations from another jurisdiction or from multinational trials are available
Q. How can information from these evaluations be used for local reimbursement/funding decisions?

Generalizability
Many alternative meanings and definitions
Usually refers to extent data collected on a particular patient population, under unique study circumstances, at a particular point in time, treated in a particular way, can be applied to another group of patients, under different study circumstances, at another point in time or under different treatment conditions
Applies to both cost and clinical effectiveness data
Focus of report is not on clinical generalizability

Generalizability (2)
For purposes of this report, we refer to 2 separate but related applications of using results from an economic evaluation or HTA report
First, is where an evaluation is done in another geographic area (e.g. UK) - transferability
Portability, extrapolation, external generalizability
Second, is where the target country (e.g. Canada) participated in a multinational trial, and where country-specific cost-effectiveness is desired

Objectives
To gain a better understanding of the factors affecting, and approaches used for, transferability and analyses of multinational trials
10 inter-related systematic literature reviews
Factors affecting transferability or analyses of multinational trialsApproaches which have been proposed or usedSystems for determining transferability potential
Conceptual papers and empirical studies

Generalizability
Countries Studied Do Not Include Target Country
Countries Studied Include Target Country
Transferability Multinational Economic Evaluations
Factors Affecting Multinational Analyses
Traditional Approaches for Analyzing Multinational Trials
Conceptual Factors Affecting Transferability
Transferability Factors from Empirical Studies
Statistical Applications in Multinational Analyses
Criteria/Guidelines for Determining Transferability
Application of Multilevel Modeling Approaches
Literature Review
Approaches for Transferring Economic Evaluations
Generalizability

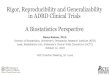
Initial Search of Electronic Databases n=4140
Title and Abstract Rejected n=3415 (82%)
Title and Abstract Accepted n=725 (18%)
Bibliography and Hand Search n=81
Full-Text Review n=808
Included in Systematic Review
n=248 (31%)
Not Included in Systematic Review
n=560 (69%)

Generalizability Papers
248248Total Papers62005**145Other Journals/Books (109 with < 5 papers/journal)
112004**5Respiratory Medicine
3320035New England Journal of Medicine
2220025Lancet
2520015Clinical Therapeutics
2220006European Journal of Cancer
3219996Circulation
2519987Health Policy
2119978European Heart Journal
12199610Health Economics
11199512International Journal of Technology Assessment in Health Care
281981-199434Pharmacoeconomics
# PapersYear of Publication
# PapersSource of ArticleNumber of Papers by Source and Year of Publication

Papers by Year of Publication
0
5
10
15
20
25
30
35
1981-1991
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Year of Publication
# of
Pap
ers
Incl
uded
in R
evie
ws
(N=2
48)

Variability Factors (70+)
Methodological CharacteristicsHealth Care System CharacteristicsProvider CharacteristicsDisease CharacteristicsPatient Characteristics
Proposed Classification System

Variability Factors (1)
24767
101082123
Demographics (age, gender, race), education, socio-economic statusRisk factors, medical history, genetic factorsLifestyle, environmental factorsMortality rates, life expectancyAttitudes toward treatment, culture, religion, hygiene, nutritionCompliance and adherence rates, ethical standardsPopulation values (utilities)Population density, immigration, emigration, travelling patternsIncome, employment rates, productivity, work loss time, friction timeType of insurance coverage, user fees, co-payments, deductiblesIncentives for patients
# CitationsPatient Characteristics

Variability Factors (2)
1767
Epidemiology (incidence/prevalence, disease progression/spread)Disease severity, case mixDisease interaction, co-morbidity, concurrent medications
# CitationsDisease Characteristics

Variability Factors (3)
39172212
11
Clinical practice, conventions, guidelines, norms Experience, education, training, skills, learning curve positionQuality of care providedMethod of remuneration (supplier-induced demand)Patient identificationCultural attitudesIncentives for providers, liability
# CitationsProvider Characteristics

Variability Factors (4)
352120512962133110
Absolute or relative pricesAvailable resources (staff, facilities, equipment), programs, servicesOrganization of delivery system, structure, level of competitionLevel of technological advancement, innovation and availabilityAvailable treatment options (comparators)Capacity utilization, economies of scale, technical efficiencyInput mix (personnel, equip.), specialization of labor, joint productionAccess to programs and services, gatekeepers, historical differencesWaiting lists, referral patternsRegulatory and organizational infrastructure, licensing of productsAvailability of generics or substitutesMarket form of suppliers, payment of suppliers, supplier incentivesIncentives for institutions
# CitationsHealth Care System Characteristics

Variability Factors (5)
89
18436562
Costing methodology, estimation procedures (e.g. productivity cost)Study perspectiveStudy factors (artificial trial conditions, industry-related bias)Timing of the economic evaluationClinical endpoints/outcome measuresDiscount ratesExchange rates, purchasing power paritiesOpportunity cost (foregone benefits)Affordability (CE thresholds)
# CitationsMethodological Characteristics

Systems for Transferability
Review identified 3 criteria, guidelines, decision rule systems for transferability
One focused on a head-to-head comparison of 10 key variability factors – yes/no (Heyland, 1996)
One focused on determining transferability potential – sufficient quality and detail (Spath, 1999)
One focused on determining transferability potential, followed by a sequence of steps for transferability act itself - Decision Chart (Welte, 2004)

Source: Welte, 2004

Transferability Approaches
Target Country Only
Target Country Only
Target Country Only
5
Target Country Only
Target Country Only
Studied Country Only
4
Target Country Only
Mixture of Studied and
Target Country
Studied Country Only
3
Target Country Only
Studied Country Only
Studied Country Only
2
Mixture of Studied and
Target Country
Studied Country Only
Studied Country Only
1
Least to Most Country-Specific Analysis
Unit Cost Data
Resource Utilization Data
Relative Clinical Efficacy Data
Source of Data by Transferability FactorModeling Approach

Transferability Approaches(2)
220#5 - Target country relative clinical efficacy, resource utilization and unit costs
15114#4 - Studied country relative clinical efficacy, target country resource utilization and unit costs
945#3 - Studied country relative clinical efficacy, mixture of studied and target country resource utilization, target country unit costs
11011#2 - Studied country relative clinical efficacy and resource utilization, target country unit costs
101#1 - Studied country relative clinical efficacy and resource utilization, mixture of studied and target country unit costs
Modeling Approaches000PPPs
101Exchange Rates
Non-modeling Approaches
Total
Decision Analytic ModelsTrials
Number of Empirical Studies
Transferability Approach

Multinational Economic Evaluations (MEE)
Factors affecting analyses of multinational trial data similar as with transferability
• clinical practice• unit prices• health care system
Two general approaches for MEE:Analyses that do not recognize the multilevel (hierarchical) nature in the data (patients nested within countries) - traditional approachesAnalyses that do recognize multilevel nature in the data - more recent statistical applications

Classifying Traditional Approaches Analysis of MEE
We developed a classification system based on the source for 2 data inputs (relative clinical efficacy and resource utilization)Three sources of data for each data input
Pooled trial-wideCountry-specific from within the trial (sub-group analysis)Country-specific from data collected outside the trial (separate sub-study)

Early/Traditional Approaches
2Target country-specific from data collected outside trial
Target country-specific from trial data (sub-group)
5
9Target country-specific from trial data (sub-group)
Target country-specific from trial data (sub-group)
4
16Target country-specific from data collected outside trial
Trial-wide pooled data3
15Target country-specific from trial data (sub-group)
Trial-wide pooled data2
80Trial-wide pooled dataTrial-wide pooled data1
# of Studies
Source for Resource Utilization Data
Source for Relative Clinical Efficacy Data
Approach
* With all approaches, country-specific unit costs are used

Problems with Standard Cost-Effectiveness Approach
The standard CE model assumes no between jurisdiction variability by ignoring natural clustering in the data (i.e. by country)This will produce inaccurate cost-effectiveness estimates and underestimate the measure of sampling variation (standard errors)Error will depend on degree of clustering in the data which in a nested dataset (patient within countries) is measured by the intraclass correlation coefficient

Analyses That Recognize Hierarchical Structures
Instead of separating MEE data for purposes of conducting country-specific analyses, an alternative is to analyze the pooled data, but recognize that there are potential country interactions (cost, effects, cost-effectiveness)In other words, the data can be recognized as having ‘levels’ or being hierarchical in nature
Patient levelCountry levelCan even include centre or provider levels

Standard Cost-Effectiveness Analysis (one level)
is cost for patient i
is treatment arm (0, 1)
is mean cost in control arm
is mean cost in treatment arm
random error term
i i iY tα β ε= + +
iY
it
αα β+
iε

Simple Hierarchical Model Multilevel Modeling (MLM)
ij ij j j ij ijY t v u tα β ε= + + + +
fixed effect random effectsIn addition to patients being seen as a random effect, country is also considered a random effect2 sources of error, one for each level in the dataThis model can be extended to include additional levels (e.g. centers) and other ‘cluster-level’ (country) explanatory variables (covariates)Successfully applied, work has just begun with MLM

Conclusions (Transferability)
Our variability review identified over 70 factors which are of potential concern when conducting transferability studies or analyzing multinational economic evaluationsThe most frequently cited factors are: absolute or relative prices, clinical practice, treatment efficacy and demographicsAlmost all (95%) of the empirical transferability studies have used studied country efficacy dataMost (75%) have substituted in target country resource utilization data into the analysis

Conclusions (MEE)
Factors affecting MEE are similar as those for transferability (prices, clinical practice, HC system)Most common approach (66%) for analyzing MEE has been to use trial-wide pooled efficacy and trial-wide pooled resource utilization dataIncreasing concerns that approaches that do not recognize the multilevel nature of MEE will result in biased cost-effectiveness estimates and underestimated standard errorsMLM is a promising new approach to address these concerns

Recommendations
Continue to update/develop guidelines and impose high quality standards of good practiceEncourage detailed and transparent reporting of methods (use of technical reports, web pages)Further development of criteria, guidelines or decision rules for transferability (potential, conduct)Development of guidelines for analyses of MEEFurther development of multilevel approaches (MLM) – model structure, which covariates, number of centers/patients per country,…