Embed Size (px)
DESCRIPTION
general pediatric
Citation preview

1
General Pediatrics
Michael Davis, M.D.

2
General Pediatric Care
General pediatric care consists of the process of diagnosing the problems
which adversely impact the health of children--followed by providing care which
minimizes disease and optimizes the potential of each child.
General pediatrics involves assessment a the child, with or without a medical
complaint.
Children depend upon the general pediatrician to recognize their problems. In general pediatrics their problem often hasn’t yet even been recognized. As general pediatricians
we first we observe; we see a child for one thing but we observe them for other problems. Second, we anticipate problems; we know what to expect so we can give guidance
about anticipated problems. The third thing we do is screen for hidden problems.
General pediatrics involves detecting the problems that are going to hurt children. Sometimes children come to you for routine care but other problems are recognized by
the astute clinician.

3
Objectives of Presentation
# Discuss a variety of General Pediatric Topics
# Stress use of observational skills

4
Screening Test
# A screening test must be able to be used in a large population to detect
individuals with early, mild or asymptomatic disease.
< The disease must be relatively common
< Morbidity is substantial
< Test implementation is achievable
< Intervention is available
A screening test is a test that is use in a large population to detect individuals who have mild, early or asymptomatic disease. Before they normally would come to recognition.
There are four things you need for a good screening test. There has to be a disease that is relatively common, it has to be something that hurts children. The morbidity has to be
substantial. You have to have a test that is affordable. And then there has to be some intervention available, so that if you find a problem, you have something to offer.

5
Sensitivity of the Screening Test
# Sensitivity: Refers to the proportion of individuals with disease who are
detected by test. (ie, test is abnormal).
# Specificity: Refers to the proportion of individuals without disease who are
correctly identified by test (ie, test is normal).
Sensitivity means refers to the proportion of all the individuals who have the disease, how sensitive is this test to detect those who
have it. Where specificity means the proportion of those who don’t have the disease, who will come out negative. So we don’t want
a whole lot of false positives.

6
A four month old male is new to the area and is brought in for
immunizations. Birth hx is normal and birth weight was 7 lbs. 4 oz.
Today's growth parameters:
Wt- 4.3 kg
Ht - 56 cm
OFC - 40 cm
First one: four month old brought to your office, for baby shots. His birth rate, the birth history was normal, he weighed
7 lbs. 4 oz. And today at four months of age he weighs 4.4 kg, height 57 cm and his head size is 40 cm. What’s the
problem? He’s not growing.

7
Inadequate Growth
# Adequate growth depends on adequate calories
being provided, absorbed, and utilized.
# Inadequate growth is frequently linked to poor
development.
# The term "failure to thrive" is a descriptive term
rather than diagnosis.
The concern is that this child has had
inadequate growth. The point that adequate
growth does depend upon the child getting
adequate calories, absorbing adequate
calories and utilizing them. Inadequate
growth is frequently linked to poor
development. The child who isn’t growing,
whose muscles mass is inadequate, will
often be developmentally delayed. So you
have this term, “Failure to thrive”. It’s
usually used when a child is not growing
and is developmentally not doing quite what
they should be doing. The term is a
descriptive term and not a diagnosis. You
really shouldn’t diagnose failure to thrive.
You should be describing it and then finding
out what the diagnosis is.

8
Normal Weight Pattens
# Fetal weight triples during third trimester
# Birth weight average 7 lbs
# Birth weight regained by day 14
# Birth weight doubles at 4 too, triples at 12 mo,
quadruples at 24 mo.
# First year gain/day:
0-6 mo = 20 gm
7-12 mo = 15 gm
# Second year gain/month = 0.25 kg/month (1/2
lb/month)
# Memory Aids:
age 2-6: gain/year is 5 lbs.
Wt (lbs) = 17 + (5 x age)
age 7-12: gain/year is 7 lbs.
Wt (lbs) = 5 + (7 x age:)
Chart of normal growth patterns.
The fetus in the last trimester is in the most
rapid period of growth of it’s entire life.
The fetus will triple it’s weight in the third
trimester. The average birth weight is 7 lbs.
Most babies lose a little weight after birth.
The average baby should be back at birth
weight no later than two weeks. He will
regain his birth weight in 14 days. The birth
weight doubles at four months, triples at 12
months and quadruples at 24 months.
In the first six months, the average child
gains 20 grams a day. Then the weight
slows up a little bit and the average child in
the second half of his first year will gain 15
gms a day. And then by the second year of
life they are only gaining 250 grams per
month. Children the first year of life will
come in and everyone will stress weight
growth and then after the first birthday, the
weight slows up. And we don’t care so
much.
Between the ages of two and six the average
child will gain five pounds a year. And be-
tween the ages of seven and 12, they will
gain seven pounds a year.

9
Normal Length and Height Pat-
terns
# In the first year, length increases by 50%
Normal Length and Height Patterns
Inches Cm.
Birth 20 50
Year 1 30 75
Year 2 34 87
# Birth length doubles by 4, triples by 13
# During year 2, gain/yr =12 cm (5-6 in)
Years > 2, gain/yr = 5.5 cm (2-2 1/2 in)
# Memory Aid:
After age 2, Ht (in) = 30 +(2.5 x age)
For lengths, the numbers are 20, 30 and 35
length. The most average child is 57 cm at
birth, and they grow 50% of that, 75 cm by a
year. Another 50% of that, 87½ when he’s
two. The birth length doubles by the time
he’s four. It depends on genetically and ado-
lescence, but roughly it triples by the time
he’s started puberty.
During the second year of life you gain five
or six inches and after that you only gain
two or 2 ½ inches a year.

10
Head Circumference Patterns
Average Head Circumference Growth
1-3 mo 5 cm
3-6 mo 4 cm
6-9 mo 2 cm
9-12 mo 1 cm
Average Head Circumference by Age
birth 34 cm
yr l 46 cm
adult 55 cm
The head circumference is very important.
In the first year the average baby is born
with a birth head circumference of 34. But
that is modified by molding. The first three
months they gain 5 cm. The next three
months, 4 cm. The next three months, 2 cm.
And the next three months 1 cm. The aver-
age child’s head will grow up 12 cm in its’
first year of life. When that brain growth in
that first year of life compares to the rest of
the brain, so the average adult head circum-
ference is 55.

11
Failure to Thrive
## Failure to thrive (FTT) can be caused by organic
factors (caused by medical diseases), or
nonorganic factors (caused by social/environmental
issues), or mixed.
# The cause of most FTT is nonorganic.
# Inadequate calories are often linked to ignorance,
dysfunctional parent/child interaction, poverty,
abuse or neglect, or poor feeding practices.
# Babies less than 6 months old usually improve
when calories are given.
“Failure to thrive”. It is important to deter-
mine whether it’s due to a medical disease,
or not a disease. It may be caused by social
or environmental diseases, or it may have a
mixed etiology. The cause in this country,
the most common cause of a child not grow-
ing, failure to thrive, is non-organic. It’s
environmental usually. Inadequate calories
provided to a baby is often linked to igno-
rance. Dysfunctional parent/child relation-
ship. Poverty and poor feeding practices.
For most children who are failing to thrive
under six months, the cause is psychosocial,
if the environment is changed, most of
those children will regain their growth
pretty easily. Sometimes if they are over
that age they don’t respond as well to the
simple practice of giving calories.

12
A six month old is seen for routine child
care. He is noted to have a normal
weight and height and an OFC of 38 cm.
The mother has noticed that the child
does not have as many
skills other infants his age.
Six month old, routine child care. His prob-
lem is his head. It’s 39 cm. And we already
talked about them, they are supposed to gain
that measurement in the first three months.
He’s six months old. The mother has re-
cently enrolled him and now that she is
comparing him with other children, she is
worried that he doesn’t have as many skills
as other infants.

13
Microcephaly
C Microcephaly is defined as a head circumference
<3 standard deviations below the mean.
Microcephaly is classified as primary (genetic) or
secondary (acquired).
" Causes of Primary Microcephaly
- Familial/autosomal dominant
- Chromosomal
" Causes of Secondary Microcephaly
- In utero exposures (radiation, alcohol)
- Maternal disorders [metabolic (diabetes),
hypothermia]
- Congenital infection
- Anoxia vascular event
- Perinatal insult
- Meningitis
The issue? His head is small. So we’ll talk
a little bit about microcephaly. It’s usually
defined as 3 standard deviations below the
mean. It’s broken down in two parts called
primary and secondary. Primary
microcephaly are those for which there is
sort of a genetic, familial or chromosomal
cause. And secondary is there is an event
that causes it. The most common causes of
acquired microcephaly are things that hap-
pen in utero. Possibly fetal alcohol syn-
drome, possibly a maternal disorder. Nature
is pretty good about keeping a pregnant
woman from hurting her baby, but congeni-
tal infections, anoxia, vascular events,
perinatal insults and meningitis may cause
microcephaly.
This is one we’ve all seen. A child whose
head is growing normal, there’s a hostile
event, following that microcephaly occurs.
Shaken baby syndrome may cause
microcephaly. Some shaken babies get hy-
drocephalus, but this baby had a lot of brain
tissue trauma.
This is another child. This is the pattern of
primary or congenital microcephaly. A child
whose head size just never grows. And this
child has a very high chance, more than
50%, of having a developmental delay. And
although the small head could possibly be
attributable to a small child, microcephaly
may occur in a child who is not going to be
neurologically normal.

14
Developmental Disability
! Risk factors for developmental disability may be
suggested by the history:
" Prenatal: in utero exposures or events
" Perinatal: birth and neonatal course
" Postnatal: meningitis
! The physical exam may reveal risk factors for
developmental disability, such as chromosomal
abnormalities or microcephaly.
! Parental concerns are often accurate predictors of
disabilities.
Prevalence of Disabilities (per 1000)
Cerebral palsy 2-3
Visual impairment 0.3 - 0.6
Hearing impairment 0.8-2
Mental retardation 20-30
Severe mental retarda- 3-4
tion
! The Denver Developmental Screen II is a com-
monly used screening tool for developmental
disability.
! Parent survey tools may be underutilized
! Measurements attempted in categories
Some populations are at risk for develop-
mental disability simply by their history.
They’ll have prenatal injury. Something
happened when they were born. Something
happened after they were born that puts
them at risk for developmental delay. Some
populations are at risk. The babies they
have, have become so large, not only do
they have hydrocephalies. They are at risk
just by exam. Then there are those children
who just aren’t doing well. We see it, the
parents see it. And parents who come in
have told me their children are not normal.
Because most parents tend to sort of exag-
gerate their children’s ability and tend to
sort of see the bright side. However, when
parents are worried about their children,
that’s a pretty good red flag that there is a
problem.
As far as developmental issues, an approxi-
mate prevalence of disability in 1000 chil-
dren is something like this: cerebral palsy
2-3 per thousand, visual impairment/hearing
impairment 2 per thousand. Mental retarda-
tion depends on how you define it obvi-
ously, but for severe mental retardation
about 3-4. All children need periodic assess-
ment of overall development. We do need
screening tools.
The most common screening tool is the
Denver Developmental II, which is the one
everyone accepts. But these are pretty time-
consuming. There’s a lot of concerns about
their usefulness. So parent surveys could be
underutilized.

15
" Gross Motor skills - large body muscles
" Fine Motor skills - small hand muscles
" Cognition- thinking, memory, learning
" Language - comprehension communication
" Social/emotional - interactions, reactions with
other persons

16
Developmental Assessments
28 week cognitive skills:
# Approach and grasp rattle with one hand
# Hold object and grasp for another
# Hold two cubes more than momentarily
# Bang bell on table
# Shake rattle, hold bell
# Transfer from one hand to another
24 month language skills:
# Uses 3 word sentences
# Uses “I,” “me,” and “you”
# Names three picture cards
# Names two test objects
# Knows four directional commands
The development and behavioral assess-
ments are linked to the very young child.
You usually break down your measurements
to the gross motor, fine motor, language and
social/emotional. And then some of the
scales include another, cognition. Particu-
larly if your child is a little bit older. And
these are the important things. And it’s sort
of independent. You all know the child who
has gross motor problems that have fine
motor skills that are normal. Okay. You all
know the children. It’s kind of comic that
babies are almost totally uncoordinated at
birth. That their bodies are totally controlled
by this primitive brain stem reflexes and
that you have to make the cortex to grow to
inhibit those reflexes and then take over.
This is just a normal baby of about two
months, this is sort of a normal prone posi-
tioning. And yet any pediatrician knows
that some of the skills we are looking for
are: sitting, three months, six months, seven
months.

17
A one month old baby is seen for a
routine checkup. The left eye appears watery
and has a slight amount of yellowish drain-
age.

18
Nasolacrimal Duct Obstruction
# Caused by incomplete lacrimal duct canalization
# Occurs in 5% of newborns
# Usually self-limited, resolves age 6-12 months
# Sx: tearing, mucoid material, crusting
# May predispose to bacterial conjunctivitis
# Treatment:
- Massage is applied upward over the lacrimal duct.
- Topical antibiotics are used if the eye is infected.
Blocked nasolacrimal duct. It’s caused by
an incomplete canalization, which almost
always improves on it’s own. It occurs in
5% of newborns, and it is usually self-lim-
ited. They get tearing, mucoid material,
crusting. It can predispose to bacterial con-
junctivitis. But the treatment is really reas-
surance and time. Massaging upwards
should be recommended to drain the
blocked duct. Topical antibiotics are pre-
scribed if the discharge gets purulent.

19
Strabismus
# Defined as abnormal eye alignment
# Occurs 4% of children <age 6
# Causes:
- Ocular pathology
- Cranial nerve abnormalities
- Muscle weakness
# Morbidity: vision in one eye suppressed, resulting in
amblyopia ("lazy eye")
# Terms:
- Tropia - deviation always present
- Phoria - latent deviation (tendency)
# Two test techniques:
- For tropia - corneal light reflex test
- For phoria - cover test (2 components)
# Cover-uncover
# Alternating cover
Strabismus. When the eyes are not aligned
right, 4% of children up to age 6 have ab-
normal eye alignment. It is caused by either
the eyes don’t work, or the nerves don’t
work, or their muscles don’t work. The
problem is that if their eyes don’t focus to-
gether, vision in one eye is suppressed. The
result is amblyopia or lazy eye. Tropia
means that the deviation is always present.

20
Corneal Light Reflex Test
"Hirschberg test"
Esophoria, exophoria, means that most of
the time the child will overcome it by con-
centrating and using muscles. These kids
tend to get headaches and when they are
tired their eyes will start crossing. For tropia
is diagnosed with the corneal light reflex
test, and phoria is diagnosed with the cover
test. If you work the eyes are aligned to-
gether and shined the distance of light and
look at its placement in the pupil. And
sometimes you have to look. It can be sub-
tle.

21
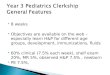
Eye Cover Test
A. Cover/Uncover
B. Alternate cover
Esophophoria
When eye covered, eye deviates
When uncovered, eye returns to center
Where it’s misplaced in one eye and you
see that there is a permanent slight
exotropia or esotropia, based upon the light
test. As far as the diagnosis, you typically
will cover one eye and the child who has a
lesser weakness, if it’s covered for a long
time, the eyelid also deviates some way.
And as soon as you take the cover off, it will
correct itself. So you are looking for a subtle
little correction. And you can even do a
cover/uncover test of one eye or you can
alternate covering the two eyes. And again,
what you are looking for is that the pupil has
a slight flick of the eye pupil of the child
corrects once both eyes are open.

22
A mother in your practice has just had a baby
with a unilateral cleft lip and cleft palate.
One of your mothers has just had a baby
with a cleft lip and palate. The parents are
obviously anxious and upset.

23
Cleft Lip and Palate
# Incidence: Cleft lip (+/- palate) 1:600
Cleft palate 1:1000
# Genetics play a role
# Thirty percent have associated anomalies
# Need referral as soon as possible
- Obturator for palate to control fluids
- Early efforts are made to align arch segments
- Feeding difficulties should be treated
# Future Complications
- Recurrent otitis media
- Hearing loss
- Dental. Malposition of teeth and excessive dental
decay
- Speech defects
- Cosmetic concerns
One of the issues with a cleft lip and palate,
typical number is 1:730. Cleft palate, genet-
ics play a role in about half of the cases.
Thirty percent will have other associated
anomalies. You do need to refer these chil-
dren as soon as possible to a specialized
team. Because they work on fixing the pal-
ate so the child can eat.
The children who have cleft lips and palates
still have complications. They all are predis-
posed to otitis media. Most places do put in
bilateral tubing prophylactically. They are
still at risk for hearing loss, although less so.
If they are watched properly to make sure
they don’t have too many problems with
fusion. They are still going to have risk of
dental problems with the malocclusion,
malpositioning of their teeth. Some of them
will still have speech defects and cosmetic
concerns.

24
A five month old develops white plaques
cover the palate and
buccal surfaces after taking antibiotics for an
ear infection.
A five month old goes to the ER. Has fever.
Given antibiotics. When he comes to you he
has white plaques covering his mouth.

25
Oral Candidiasis
# Thrush is diagnosed in 2-5% of newborns
# It is common until age 6 months, occasional until age 12
months.
# Predisposing factors include use of antibiotics, maternal
breast colonization, contaminated objects (vitamin
dropper)
# Candidiasis is a indicator of immunodeficiency if it is
severe or late appearing (eg, HIV)
This is obviously thrush. He’s got thrush.
Thrush is Candida or Candidiasis. It’s diag-
nosed in 2% - 5% of newborns. It’s com-
mon until six months of age. Occasionally
you will see it until 12 months of age, par-
ticularly if they are on antibiotics. Some-
times there are other predisposing factors.
Maternal breast colonization of breast-feed-
ing babies. Thrush is a flag for immunode-
ficiency. If severe or if it appears late.

26
The mother of a newborn asks what
she can do to prevent tooth decay
in this child.

27
Fluoride Supplementation
# Supplementation is important in prevention of dental
caries
# Supplements are rarely needed if the community water
supply is optimal (0.7-1.0 ppm)
# Supplements are not necessary infants less than 6
months of age or for breast-fed infants
# Dosage of supplement (.25, 0.5,1.0 mEq.) depend on
age and water concentration
# Excess fluoride causes dental staining, such as with
overuse of toothpaste
The issue is fluoride. Supplements are
rarely needed if your community water sup-
ply is optimal. We usually give supplements
to breast-feeding babies, but they probably
don’t need it. The dosage depends on their
age and the water concentration, and then of
course, excessive fluoride is bad.

28
Nursing Bottle Carries
# Nursing bottle carries are a common, severe form of
dental decay which may require expensive restorative
care.
# Prevention:
- Milk in bottle should never used as a pacifier at nap
or bedtime.
- Milk bottle feeding should be discontinued after
first birthday.
- Juice should always be offered from cup.
Nursing-bottle caries is the other concern
where there is a three-month-old that needs
all this dental work. It’s a severe form of
dental decay. The prevention is: you don’t
let them sleep with bottles. Milk in a bottle
should never be used as a pacifier at nap or
bedtime. We try to discontinue it by the first
birthday. You should always offer juice
from a cup and not from a bottle.

29
A 15 month old child makes sounds but
speaks no real words and points to objects
that he wants.

30
Delayed Speech
## Differential Diagnosis of Delayed Speech
- Hearing deficit
- Mental retardation
- Autism
- Neurologic disorders of articulation
- Abnormal environment
- Developmental language disorder
# Expressive
# Receptive
Delayed speech. This is a different diagno-
sis when a child isn’t speaking.
If hearing loss is greater than 30 decibels,
the hearing frequency will interfere with
speech and language development. The
degree of communicative disorder is associ-
ated with how deaf they are and the time of
onset. And unequivocally, early intervention
helps. There’s lots of problems with chil-
dren who don’t hear that aren’t recognized.
The types of hearing loss are: conductive,
obviously that means the structure, and
neurosensory. That’s the nerves and brains.
And often they are mixed. The average age
at this time is still greater than 12 months.
It’s when children are supposed to be speak-
ing, people realize they are not speaking and
then we do testing.

31
Hearing Loss
## Hearing loss of >30 dB, in the frequency region for
speech (500-4000 Hz), will interfere with speech and
language development.
# The degree of communicative disorder is associated
with degree of hearing impairment and time of onset.
# Early intervention reduces the degree of impairment.
# Types of Hearing Loss:
- Conductive. Caused by a structural abnormality
- Sensorineural. Caused by abnormal cochlea, nerves,
or brain
- Mixed
- Average age of diagnosis of hearing impairment is
>12 months.
Estimated Number of Infants Heating Impaired
Number Prevalence Total
born
No risk 3,600,000 3:1000 10,800
High risk 400,000 30:1000 12,000
Total 4 million 5.7:1000 22,800
Ref: Northern Audiology Today, v6n2,1994
Hearing loss. The prevalence is 3 per 1000,
but in high risk groups it is 10 times that.
But still, half of all children who are deaf
have no risk. So you can take a high risk
population and test them and follow them,
but you are going to miss half of all children
with hearing impairment. Now we can test
hearing at any age. There is no child that
you can’t do a hearing test on, even new-
borns.

32
Evaluation for Hearing Loss
# Testing is available at all ages, even newborns.
# Types of Tests
- Auditory brainstem response
- Behavioral Techniques: Behavior observation,
visual reinforcement, play audiometry.
- Acoustic Immittance: Tympanometry, acoustic
reflex, static compliance.
# Limitations of Tests
- Mental age, neurologic status, cooperation, testor
environment

33
Risk Indicators for Hearing Loss
# Risk Indicators for Hearing Loss in Newborns thru
Age 28 Days
- Family history of hereditary sensorineural loss
- Congenital infections
- Craniofacial anomalies
- Birth weight < 1500 gm
- Hyperbilirubinemia
- Ototoxic drugs
- Low APGAR scores (#4 at one minute or #6 at five
minute testing)
- Mechanical ventilation > 5 days
- Stigmata of syndrome with hearing loss
# Risk Indicators for Hearing Loss Age 1 Month to 2
Years
- Parent concern over developmental delay
- History of bacterial meningitis
- History of head trauma with LOC or fractures
- Stigmata of syndrome with hearing loss
- Ototoxic medication use
- Recurrent acute otitis media or persistent otitis
media with effusion > 3 moths
Risk factors for hearing impairment include
family history of neurosensory loss, congen-
ital infections, craniofacial anomalies, low
birth weight, hyperbilirubinemia, ototoxic
drugs, meningitis, low Apgar, and treatment
with a ventilator. Hearing should be evalu-
ated anytime parents are concerned about
lack of language or that developmental de-
lay. Did they have meningitis? Major head
trauma? Stigmata of syndrome of hearing
loss that was present at birth? Ototoxic
drugs and of course your recurrent otitis
media or chronic otitis media with effusion.

34
Hearing Loss: Risk Indicators
# Serial audiology is required for patients with the fol-
lowing high risk indicators (repeat testing even if early
tests are normal):
- Family history of hearing loss
- Congenital infection
- Neurodegenerative diseases
- Recurrent or persistent otitis media
After two years of life you still need to
check some children, even if the early test is
normal. Some children should be serially
assessed. Those who have a family history
of deafness, those who have known congen-
ital infections, particularly CMV, the
neurodegenerative diseases and then of
course those children with bad ear infec-
tions.

35
Should all infants be screened for
hearing loss?
# Universal screening for infant hearing is not beneficial
and not presently justified. Bess, Paradise. Peals
98,2,1994
The trend has been testing infants and there
is a controversy. Only 50% of children with
hearing impairment can be identified by
those risk factors. So in 1993 there was a
NIH consensus statement that said we
should have universal hearing screening.
And they suggested it in two stages of oto-
acoustic emission, which is a behavioral
thing and then those who fail that should
have a brain stem. There are two states that
have done universal hearing testing for a
year now, Hawaii and Rhode Island. It is
probably worthwhile to test and detect these
children’s hearing impairments early and
make a difference in their lives.

36
References and Resources
Developmental Issues:
Atlas of Pediatric Physical Diagnosis, 2 edition. Zitellind
and David, ed., Mosby-Woffe Publishers, 1994.
Glascoe, Martin, Humphrey. Consumer Reports: A Com-
parative Review of Developmental Screening Tests.
Pediatrics, v.86, n.4, pp.547-54, 1990
Frankenburg WK, Dodcls J, Archer P, et al. The Denver
II: A Major Revision and Restandardization of the
Denver Developmental Screening Test. Pediatrics,
v.89, n. 1, pp.91-7, 1992
Speech/Hearing Loss
Coplan J. Normal Speech and Language Development:
An Overview. Feds in Review, V. 16, N3, March
1995
NIH consensus statement (V. 11, N. 1, March 1-3, 1993)
"Early Identification of Hearing Impairment in Infants
and Young Children". Office of Medical Applications
of Research, NIH, Bethesda Md.