Embed Size (px)
Citation preview

doi: 10.1111/joim.12448
Gene expression signatures, pathways and networksin carotid atherosclerosisL. Perisic1, S. Aldi1,*, Y. Sun2,*, L. Folkersen3,4, A. Razuvaev1, J. Roy1, M. Lengquist1, S.�Akesson1, C. E. Wheelock5,
L. Maegdefessel4, A. Gabrielsen4, J. Odeberg4,6, G. K. Hansson4, G. Paulsson-Berne4 & U. Hedin1
From the 1Department of Molecular Medicine and Surgery, Karolinska Institute; 2Translational Science Center, Personalized Healthcare andBiomarkers, R&D, Astra Zeneca, Stockholm, Sweden; 3Department of Molecular Genetics, Novo Nordisk, Copenhagen, Denmark;4Department of Medicine, Karolinska Institute; 5Division of Physiological Chemistry 2, Department of Medical Biochemistry and Biophysics,Karolinska Institute; and 6Science for Life Laboratory, Department of Proteomics, School of Biotechnology, Royal Institute of Technology,Stockholm, Sweden
Abstract. Perisic L, Aldi S, Sun Y, Folkersen L,Razuvaev A, Roy J, Lengquist M, �Akesson S,Wheelock CE, Maegdefessel L, Gabrielsen A,Odeberg J, Hansson GK, Paulsson-Berne G,Hedin U (Karolinska Institute, Stockholm; R&D,Astra Zeneca, Stockholm, Sweden; Novo Nordisk,Copenhagen, Denmark; Karolinska Institute,Stockholm; Karolinska Institute, Stockholm;Royal Institute of Technology, Stockholm,Sweden). Gene expression signatures, pathwaysand networks in carotid atherosclerosis. J InternMed 2015; doi: 10.1111/joim.12448.
Background. Embolism from unstable atheromas inthe carotid bifurcation is a major cause of stroke.Here, we analysed gene expression in endarterec-tomies from patients with symptomatic (S) andasymptomatic (AS) carotid stenosis to identifypathways linked to plaque instability.
Methods. Microarrays were prepared from plaques(n = 127) and peripheral blood samples (n = 96) ofS and AS patients. Gene set enrichment, pathwaymapping and network analyses of differentiallyexpressed genes were performed.
Results. These studies revealed upregulation ofhaemoglobin metabolism (P = 2.20E-05) and boneresorption (P = 9.63E-04) in S patients. Analysis ofsubgroups of patients indicated enrichment ofcalcification and osteoblast differentiation in S
patients on statins, as well as inflammation andapoptosis in plaques removed >1 month comparedto <2 weeks after symptom. By prediction profiling,a panel of 30 genes, mostly transcription factors,discriminated between plaques from S versus ASpatients with 78% accuracy. By meta-analysis,common gene networks associated withatherosclerosis mapped to hypoxia, chemokines,calcification, actin cytoskeleton and extracellularmatrix. A set of dysregulated genes (LMOD1,SYNPO2, PLIN2 and PPBP) previously not describedin atherosclerosis were identified from microarraysand validated by quantitative PCR and immuno-histochemistry.
Conclusions. Our findings confirmed a central rolefor inflammation and proteases in plaque insta-bility, and highlighted haemoglobin metabolismand bone resorption as important pathways.Subgroup analysis suggested prolonged inflam-mation following the symptoms of plaque insta-bility and calcification as a possible stabilizingmechanism by statins. In addition, transcrip-tional regulation may play an important role inthe determination of plaque phenotype. Theresults from this study will serve as a basis forfurther exploration of molecular signatures incarotid atherosclerosis.
Keywords: atherosclerosis, carotid plaques, geneexpression, microarrays.
Introduction
Atherosclerotic plaque rupture followed by myocar-dial infarction or stroke is the major cause ofmorbidity and mortality in patients with
cardiovascular disease. In order to improve identi-fication of individuals at risk and to facilitate thedevelopment of future preventive therapeuticstrategies, there is a need for better understandingof the pathophysiology underlying the transition ofatherosclerosis from clinically asymptomatic (AS)
*These authors contributed equally.
ª 2015 The Association for the Publication of the Journal of Internal Medicine 1
Original Article

and stable lesions to symptomatic (S) and unstabledisease [1].
The unstable atheroma has previously been char-acterized by enhanced activity of proinflammatoryT cells and macrophages, increased cytokinerelease and secretion of matrix metalloproteinases(MMPs), thinning of the fibrous cap due to impairedcollagen fibre formation, collagenolysis and cellapoptosis. Together with haemodynamic forces,these processes lead to fibrous cap rupture, expo-sure of tissue factor, atherothrombosis and clinicalmanifestations [1, 2].
Embolization of ruptured plaques in the carotidbifurcation to the cerebral circulation can occur,causing transient or permanent ischaemia.Patients with high-grade carotid stenosis aretreated with stroke preventive interventions, butneither laboratory tests nor imaging have beenclinically established for precise detection of unsta-ble individuals or lesions [3]. A number of clinicalparameters influence the risk of stroke in patientswith carotid stenosis. AS carotid disease is associ-ated with an annual stroke risk of 1–3%, whereas Spatients with either transient ischaemic attack(TIA) or minor stroke (MS) have a more than 10-fold increased risk [4]. In addition, it has beenshown that TIA and MS confer a higher risk thanocular symptoms [retinal TIA, amaurosis fugax;(AF)] [3]. Recurrent embolization and symptomsare most pronounced within the first 2 weeks afterthe index event [5, 6] and are thereafter graduallyreduced. Medical therapy with HMG CoA reductaseinhibitors (statins) significantly reduces strokerisk, probably by improving plaque stability [7, 8].
Large-scale transcriptomic analyses usingmicroarrays enable studies of expression patternsto be performed for thousands of genes simultane-ously [9]. Although alternative technologies suchas RNA sequencing are becoming available,microarrays remain powerful tools for investiga-tions of disease-related gene expression changes,particularly when combined with open-source soft-ware for high-throughput data exchange (e.g. GeneExpression Omnibus (GEO) data sets and ArrayEx-press) and a growing number of web-based pro-grams for functional analysis. Previous attempts toinvestigate global gene expression profiles inhuman atherosclerotic plaques [10–15] have beenrestricted by small sample sizes, the lack ofundiseased (nonatherosclerotic) vascular controltissues or the inability to classify patients based on
clinical categories. Hence, factors determiningplaque vulnerability and healing remain largelyunknown.
The Biobank of Karolinska Endarterectomy (BiKE)was established in 2002 for prospective collectionof atherosclerotic plaque tissue and blood frompatients undergoing carotid endarterectomy forhigh-grade carotid artery stenosis, with a databaseof clinical parameters including risk factors, med-ication, symptoms, time of surgery, preoperativeimaging and anthropometric and laboratory mea-surements. Transcriptomic and genomic profileshave been generated by microarray and genotypingchips, enabling multivariate analysis of geneexpression patterns in relation to clinical parame-ters and genotype. Data from this biobank havebeen utilized previously, both in hypothesis-drivenand hypothesis-independent studies [16–31]. Inthis study, we postulated that phenotypes ofpatients with carotid atherosclerosis would corre-late with specific gene expression patterns and weanalysed the global transcriptome in relationshipto clinical features stratifying stroke risk. We havebeen able to identify novel molecular signaturesand pathways of plaque instability, validateestablished processes featuring late-stageatherosclerosis as well as to highlight the temporaldynamics and modulation of atherosclerosis bystatin therapy.
Materials and methods
Human material
Patients undergoing surgery for S or AS, high-grade (>50% North American Symptomatic CarotidEndarterectomy Trial, NASCET) [32] carotid steno-sis at the Department of Vascular Surgery, Karolin-ska University Hospital, were consecutivelyenrolled in the study. Informed consent wasobtained, and clinical data were recorded onadmission. The following clinical parameters wereselected for investigation in this study: presenceand type of symptoms; statin treatment; and timebetween last symptom and surgery. Symptoms ofplaque instability were defined as TIA, MS and AF.TIA was defined as a transient episode of neuro-logical dysfunction, and MS as symptoms persist-ing >24 h with complete or nearly completerecovery.
Patients without qualifying symptoms within6 months prior to surgery were categorized as ASand indication for carotid endarterectomy based on
L. Perisic et al. Atherosclerosis transcriptome
2 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine

results from the Asymptomatic Carotid SurgeryTrial (ACST) [33]. Patients with atrial fibrillationand those who had suffered a major stroke wereexcluded from the study. Carotid endarterectomies(carotid plaques, CP) and peripheral blood sampleswere collected at surgery and retained within theBiKE. Plaques were divided transversally by thesurgeon at the most stenotic part, and the proximalhalf of the lesion used for RNA preparation and thedistal half fixed in 4% Zn-formaldehyde and pro-cessed for histology. RNA from tissues and periph-eral blood mononuclear cells (PBMCs) wasanalysed by gene expression microarrays, andgene expression in plaques was validated by quan-titative PCR (qPCR). A summary of the samplesused in the study is provided in Fig. 1a, anddemographics of the cohort are given in Table S1.Nonatherosclerotic, further referred to as normalartery (NA), control samples were obtained fromnine macroscopically disease-free iliac arteries andone aorta from organ donors without a history ofcardiovascular disease. The vessels were dissectedand the intima and media used for RNA isolationand arrays. NAs for immunohistochemistry (IHC)were radial arteries obtained at coronary bypasssurgery and one control internal carotid arteryfrom a 61-year-old man undergoing surgical exci-sion of a neck tumour. All samples were collectedwith informed consent from patients and organdonors or their guardians. The study was approvedby the regional ethics committee.
Antibodies
A summary of the primary antibodies kindly pro-vided by the Human Protein Atlas (HPA) project isshown in Table S2 with information about thecorresponding gene function and tissue expressionpattern obtained from www.proteinatlas.org. Forcolocalization, the following antibodies for celltype-specific markers were used as recommendedby the manufacturers: anti-alpha smooth muscleactin (aSMA; #M0851; DAKO, Glostrup, Denmark),CD61 (#M0753; DAKO) and CD68 (#NCL-L-CD68;Novocastra, Newcastle, UK).
RNA extraction
Plaques were frozen at �80 °C immediately aftersurgery, and peripheral blood was processedaccording to standard procedures for separationof the mononuclear cell fraction and RNA isolation.Briefly, whole blood was collected at surgery andsubjected to density gradient centrifugation
through Ficoll-Paque preparation tubes (Vacu-tainer CPT, Becton-Dickinson, Franklin Lakes,NJ, USA). PBMCs were resuspended using RLTbuffer (Qiagen, Hilden, Germany) before freezing at�80 °C. RNA was prepared using Qiazol Lysis
(a)
(b)
(c)
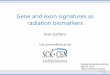
Fig. 1 The Biobank of Karolinska Endarterectomy (BiKE)data sets, workflow for microarray comparisons anddistribution of samples. (a) Outline of the subcohorts fromthe BiKE used for microarray profiling. (b) Schematicrepresentation of the comparisons performed from thediscovery data set within clinically defined groups. (c)Principal components analysis of discovery data set fromplaque tissues for symptomatic and asymptomaticpatients based on expression values shows randomscattering of the samples in groups and no clustering.The first two principal components (PC1 and PC2) explain23% and 22%, respectively, of variance amongst samplesin this comparison. PBMC, peripheral blood mononuclearcell; S, symptomatic; AS, asymptomatic; qPCR, quantita-tive PCR; TIA, transient ischaemic attack; MS, minorstroke; AF, amaurosis fugax.
L. Perisic et al. Atherosclerosis transcriptome
ª 2015 The Association for the Publication of the Journal of Internal Medicine 3
Journal of Internal Medicine

Reagent (Qiagen) and purified using the RNeasyMini kit (74106, Qiagen), including DNase diges-tion. The concentration of RNA was measuredusing Nanodrop ND-1000 (Thermo Scientific,Waltham, MA, USA) and quality estimated usinga Bioanalyser capillary electrophoresis system(Agilent Technologies, Santa Clara, CA, USA). Formicroarrays, only RNA of good integrity (RNAIntegrity Number >7), A260/A280 ratio 1.8–2.1,A260/230 ratio 0.7–1.5 and concentration about50–500 ng lL�1 was used, according to recom-mended standards for whole-transcript arrays.
Microarray analysis
Gene expression analyses of 127 endarterectomysamples were performed in two batches usingAffymetrix HG-U133 plus 2.0 Genechip arrays(Santa Clara, CA, USA). A separate analysis wasperformed on an additional 50 samples usingAffymetrix HG-U133a Genechip arrays. Robustmulti-array average normalization, filtering ofprobesets based on signal intensity and batcheffect correction were performed, and processedgene expression data were recorded on a log2 scaleas previously described [16, 23]. The full data set isavailable from Gene Expression Omnibus (acces-sion number GSE21545).
Data analyses
Data set analyses were performed with GraphPadPrism 6 and Bioconductor using a linear regressionmodel adjusted for age and gender and a two-sidedStudent’s t-test assuming nonequal deviation, withcorrection for multiple comparisons performedaccording to the method of Sidak–Bonferroni [34].Spearman correlations with Benjamini–Hoechbergcorrection were calculated to determine the asso-ciation between mRNA expression levels frommicroarrays. In all analyses, P-values <0.05 wereconsidered statistically significant, although raw P-values are also reported. The following publicallyavailable programs were used for functional anal-yses of the microarray data sets: ArrayMining [35],GOrilla and DAVID for gene set enrichment anal-yses (GSEAs) based on functional grouping ofgenes defined in gene ontology (GO) categories[raw P-values reported with false discovery rate(FDR) correction; categories with more than onegene and nonoverlapping gene sets considered];INMEX for meta-analysis using Fisher’s weight-freemethod for combined P-values [36]; GeneMania forfunctional network construction; PINA [37, 38] and
Cytoscape for protein–protein interactome networkanalyses; MSigDB (Broad Institute) for mapping oftranscription factors and microRNA motif bindingsites (FDR set to 1%). Information about individualgenes and proteins was extracted from www.-genecards.org, www.noncode.org and www.unipro-t.org. Prediction modelling was performed based onsparse partial least square-discriminant analysis(sPLS-DA) [39]. Statistical resampling was used tobalance the number of S and AS patients in theanalysis. In order to optimize the prediction per-formance, a nested cross-validation machinelearning method was applied: the samples wererandomly divided into one training set and one testset as an independent hold-out set for validation.Within the training set, the samples were randomlydivided into subtraining sets and subtest sets. ThesPLS-DA model was built on the training set. Theprediction error rate was estimated by classifying asubset of test samples. The prediction accuracywas determined by performing a 10-fold cross-validation. New sPLS-DA models were builtsequentially by including different numbers ofvariables in the model, and prediction error rateswere determined. Then, the final sPLS-DA modelwas constructed with the minimum number ofvariables selected for achieving the smallest pre-diction error rate. One dimension of sPLS-DA wasused in the model. The independent hold-out testset was predicted based on this final model.
qPCR
For qPCR, total RNA was reverse-transcribedusing the High-capacity RNA-to-cDNA Kit(4387406; Applied Biosystems, Life TechnologiesCorporation, Carlsbad, CA, USA). PCR amplifica-tion was performed in 96-well plates using the7900 HT real-time PCR system (Applied Biosys-tems), TaqMan Universal PCR Master Mix (AppliedBiosystems) and TaqMan Gene Expression Assays(LMOD1 Hs00201704_m1, SYNPO2 Hs00326493_m1, PPBP Hs00234077_m1, PLIN2 Hs00605340_m1; Applied Biosystems). All samples weremeasured in duplicate. Results were normalizedrelative to the equal mass of total RNA as well asthe Ct values of the RPLPO housekeeping controlgene (probe Hs99999902_m1). The relativeamount of target gene mRNA was calculated bythe 2 (�DDCt) method and presented as foldchange compared to the average baseline expres-sion in normal arteries. The qPCR results wereevaluated using the nonparametric Mann–WhitneyU-test.
L. Perisic et al. Atherosclerosis transcriptome
4 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine

IHC
All IHC reagents were purchased from BiocareMedical (Concord, CA, USA). Isotype rabbit andmouse IgG were used as negative controls. In brief,5-lm sections were deparaffinized in Tissue Clearand rehydrated in a graded series of ethanolconcentrations. For antigen retrieval, slides weresubjected to high-pressure boiling in DIVA buffer(pH 6.0). After blocking with Background Sniper,primary antibodies diluted in Da Vinci Greensolution were applied and incubated at roomtemperature for 1 h. A double-stain probe–polymersystem containing alkaline phosphatase andhorseradish peroxidase was applied, with subse-quent detection using Warp Red and Vina Green.Slides were counterstained with Haematoxylin QS(Vector Laboratories, Burlingame, CA, USA),dehydrated and mounted in Pertex (Histolab,Gothenburg, Sweden). Images were captured usinga Nikon OPTIPHOT-2 microscope equipped with adigital camera and processed with NIS-Elementssoftware.
Results
Characterization of gene expression differences in patient subgroups
Plaques from 127 consecutively enrolled patients(40 AS and 87 S) were analysed by gene expressionmicroarrays (discovery data set). An overlappingsubset of 96 PBMC preparations (30 AS and 66 Spatients) was separately analysed by microarrayprofiling. A nonoverlapping set of 50 plaques (10AS and 40 S patients) was analysed with a differentmicroarray platform and used as an independentvalidation cohort. In addition, RNA from 77nonoverlapping plaques (21 AS and 56 S patients)was used for qPCR validation of the microarrayresults. A summary of these cohorts and the studyworkflow is shown in Fig. 1a.
Pairwise comparisons of microarray profiles fromthe discovery data set were assessed as outlined inFig. 1b, by grouping the patients into clinicallydefined categories. The majority of the study cohortwas male (78%); S patients were generally olderthan AS patients (mean age 72.5 vs. 66.4,P = 0.0002) and had significantly lower meanhaemoglobin (Hb) levels (131.55 vs. 141.62 g L�1,P = 0.0077). The demographic characteristics areshown in detail in Table S1. Principal componentsanalysis, performed to give an overview of theexpression data distribution in S and AS tissuesamples (Fig. 1c), showed that these patient
groups roughly cluster together with 23.6% and22.2% variability explained by the first two princi-pal components. These results emphasize subtlebiological differences that reflect the overall geneexpression patterns in plaques from S and ASpatients.
Hb metabolism and bone resorption are enriched in plaques from Spatients
Analyses of plaques isolated from S and ASpatients revealed small differences in gene expres-sion levels (up to 2-fold change). The fraction ofdifferentially regulated probesets was <5%. In thisanalysis, many genes were identified that havepreviously not been reported in similar compar-isons, for example ADM, PPBP, MARCO and MREG(Table 1; for full list see Table S3), in addition tothose already established in atherosclerosis, suchas matrix metalloproteinases (MMPs), markers ofmacrophages, chemokines, cathepsins andapolipoproteins that were upregulated and mark-ers of differentiated smooth muscle cells (SMCs)that were downregulated [10, 14, 23, 40]. GSEA onGO categories for the differentially expressed genesin plaques from S patients showed enrichment oflow-density lipoprotein particle clearance, inflam-matory response, macrophage-derived foam celldifferentiation, cell proliferation, apoptosis, angio-genesis and extracellular matrix (ECM) disassem-bly. It is interesting that enrichment was alsoobserved for positive regulation of bone resorption(Tables 2 and S5). There were also small differ-ences in gene expression (up to 1.5-fold change;overall about 1% differentially regulated probesets;Tables 1 and S4) in PBMCs from S versus ASpatients. Here, we observed upregulation of anumber of genes including HBB, CA1, IFNG, F8,ALAS2, ARG2, ARSD and SELENBP1. Apart fromHBB, several genes implicated in erythropoiesiswere also upregulated, particularly GATA2, ERAFand KLF1. Even genes associated with Hb catabo-lism were upregulated, including iron-binding PIR,OGFOD1 and several members of the cytochromeP450 family such as CYP2B6 and CYP26A1. Themost enriched pathways were response to nitrosa-tive stress, positive regulation of nitric oxidebiosynthesis, IL1B secretion, lymphocyteactivation and Hb metabolism (Tables 2 and S5).
We also assessed gene expression differences insubgroups of clinical phenotypes of S patients,which consequently reduced sample size andstatistical power. Gene expression profiles in
L. Perisic et al. Atherosclerosis transcriptome
ª 2015 The Association for the Publication of the Journal of Internal Medicine 5
Journal of Internal Medicine

patients with TIA and MS were compared to thosein patients with AF because it has been shown thatpatients with TIA and MS have an increased strokerisk [41]. Small differences in expression levels (upto 1.5-fold change) and in the number of differen-tially regulated probesets (about 3%; Table S6)were observed. Here, several genes associated withplatelet activation, such as TUBB1, PTAFR,TREML1 and platelet-specific GP6, were stronglyupregulated in patients with TIA and MS. GSEAhighlighted angiogenesis, oxidoreductase activity,secretion, chemotaxis and inflammation as pro-cesses enriched in plaques of S patients with TIAand MS (Table S9). Categorization of patients withrespect to time from last qualifying symptom tosurgery surprisingly yielded marked differences ingene expression. A higher relative fold change (upto 10-fold) and more differentially expressed probe-sets (about 20%) were found in this than in other
comparisons (Table S7). Of note, prolongedimmune system activation and apoptosis wereongoing in plaques extracted 1 month or later aftersymptom as compared to those removed within thefirst 2 weeks (Table S9). We also investigateddifferences between S patients treated with statinscompared to those who did not receive this therapy.As expected, serum cholesterol and LDL choles-terol levels were significantly decreased in thetreated group (mean difference � SD �0.7204 �0.3310 mmol L�1, P = 0.03 and �0.8782 �0.3321 mmol L�1, P = 0.01, respectively). Compar-ison of gene expression in lesions from S patientswith and without statin treatment showed modestdifferences in fold change (up to 2.5-fold), but anabundance of differentially expressed probesets(about 15%; Table S8). Notably, regulation ofcalcium-mediated signalling, osteoblast differenti-ation and negative regulation of angiogenesis and
Table 1 Most significantly upregulated genes in microarray comparisons
Affymetrix ID Gene Gene product P- value Fold change
Plaques S vs. AS (n = 87 + 40)
210072_at CCL19 Chemokine (C-C motif) ligand 19 0.002 1.871
209396_s_at CHI3L1 Chitinase 3-like 1 (cartilage glycoprotein-39) 0.002 1.817
203980_at FABP4 Fatty acid binding protein 4, adipocyte 0.046 1.759
212657_s_at IL1RN Interleukin 1 receptor antagonist 0.021 1.712
202859_x_at IL8 Interleukin 8 0.006 1.705
223484_at C15ORF48 Chromosome 15 open reading frame 48 0.010 1.702
204580_at MMP12 Matrix metallopeptidase 12 (macrophage elastase) 0.026 1.694
203936_s_at MMP9 Matrix metallopeptidase 9 (gelatinase B, 92-kDa
gelatinase, 92-kDa type IV collagenase)
0.016 1.621
203665_at HMOX1 Haeme oxygenase (decycling) 1 0.013 1.620
205819_at MARCO Macrophage receptor with collagenous structure 0.006 1.602
PBMCs S vs. AS (n = 66 + 30)
1562981_at HBB Haemoglobin, beta 0.027 1.507
205949_at CA1 Carbonic anhydrase I 0.023 1.421
235867_at GSTM3 Glutathione S-transferase mu 3 (brain) 0.027 1.392
238813_at ALAS2 Aminolevulinate, delta-, synthase 2 0.043 1.380
221690_s_at NLRP2 NLR family, pyrin domain containing 2 0.021 1.333
219672_at ERAF Erythroid-associated factor 0.022 1.331
210354_at IFNG Interferon-gamma 0.030 1.310
229437_at MIR155HG MIR155 host gene (nonprotein coding) 0.034 1.296
222793_at DDX58 DEAD (Asp-Glu-Ala-Asp) box polypeptide 58 0.035 1.289
219385_at SLAMF8 SLAM family member 8 0.012 1.273
Top 10 genes sorted by P-value and fold change for each comparison are shown. P-values are adjusted for multiplecomparisons; expanded lists of genes are shown in the Tables S3 and S4. PBMC, peripheral blood mononuclear cell;S, symptomatic; AS, asymptomatic.
L. Perisic et al. Atherosclerosis transcriptome
6 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine

inflammatory response were enriched in S patientsreceiving statin treatment (Table S9).
For comparison, gene expression alterations inatherosclerotic CP tissue compared with NA tissuewere considerable (up to 274-fold change forMMP12) with a larger portion of dysregulatedprobesets (25%), reflecting the profound biologicaldifferences in these tissues. In plaques, pathwaysof cell proliferation, nitric oxide signalling, lipopro-tein and apoptotic particle clearance, activation ofimmune cells, chemokine secretion, blood coagu-lation and ECM disassembly were all enriched(Fig. S1a–c) and, as in PBMCs, the Hb–haptoglobin(Hp) complex was one of the most dominant GOcategories. In confirmation, generally similarresults were obtained when pathways were
analysed in a separate microarray data set ofn = 50 plaques (Fig. S1d).
MALAT1, MIR155HG and TP53TG are involved in the regulation of geneexpression in carotid atherosclerosis
Gene expression analyses in plaques and PBMCsfrom patients with carotid atherosclerosis alsorevealed dysregulation of many noncoding (nc)transcripts (selected ncRNAs are presented inFig. 2a; for full list see Table S10). MIR155HG,found in activated B and T cells and macrophages,was significantly upregulated in comparisonsbetween S and AS plaques and PBMCs. The longnoncoding (lnc) RNA MALAT1 associated with cellproliferation, apoptosis [42], neovascularization[43] and prostate cancer [44] was substantially
Table 2 Gene set enrichment analysis (GSEA) based on gene ontology (GO) processes enriched in microarray comparisons
GO term Description P-value Enrichment
Plaques S vs. AS (n = 87 + 40)
GO:0006935 Chemotaxis 9.68E-08 1.66
GO:0007155 Cell adhesion 8.30E-07 1.43
GO:0002523 Leucocyte migration involved in inflammatory response 3.22E-06 26.79
GO:0034383 Low-density lipoprotein particle clearance 9.66E-06 422.67
GO:0030593 Neutrophil chemotaxis 4.99E-05 2.23
GO:0008284 Positive regulation of cell proliferation 1.26E-04 1.39
GO:0002544 Chronic inflammatory response 1.34E-04 14.92
GO:0043277 Apoptotic cell clearance 2.65E-04 25.47
GO:0033005 Positive regulation of mast cell activation 3.01E-04 9.65
GO:0010743 Macrophage-derived foam cell differentiation 7.12E-04 8.89
GO:0048514 Blood vessel morphogenesis 7.61E-04 9.63
GO:0050708 Regulation of protein secretion 7.81E-04 1.85
GO:0045780 Positive regulation of bone resorption 9.63E-04 5.14
GO:0022617 Extracellular matrix disassembly 9.91E-04 5.97
PBMCs S vs. AS (n = 66 + 30)
GO:0051409 Response to nitrosative stress 1.44E-05 38.56
GO:0020027 Haemoglobin metabolic process 2.20E-05 47.46
GO:0045429 Positive regulation of nitric oxide biosynthetic process 2.95E-04 77.12
GO:0009636 Response to toxic substance 4.24E-04 23.14
GO:0050718 Positive regulation of interleukin-1 beta secretion 7.23E-04 51.42
GO:0046649 Lymphocyte activation 9.88E-04 3.3
LDL particle clearance was the most enriched category in comparisons between plaques from symptomatic (S) andasymptomatic (AS) patients. In peripheral blood mononuclear cells (PBMCs), nitric oxide biosynthesis, haemoglobinmetabolism, lymphocyte activation and IL1B secretion were dominant in cells from S versus AS patients. Adjusted P-values are shown; expanded pathway analyses are shown in the Table S5. Enrichment was calculated as (b/n)/(B/N),where N is the total number of genes, B is the total number of genes associated with a specific GO term, n is the number ofgenes in the target set and b is the number of genes in the intersection.
L. Perisic et al. Atherosclerosis transcriptome
ª 2015 The Association for the Publication of the Journal of Internal Medicine 7
Journal of Internal Medicine

downregulated in S compared with AS plaquetissue, and in comparison TIA+MS versus AFpatients. By contrast, MALAT1 was upregulatedin plaques extracted >1 month after the symptomscompared to those removed within 2 weeks.TP53TG lncRNA regulating p53 expression [45]was repressed in TIA+MS compared with AFpatients.
To investigate the regulation through transcriptionfactors and miRNAs, we performed reverse analysisby mapping for the corresponding binding motifs ingenes differentially expressed between S and AS
patients. This approach confirmed enrichment offactors involved in regulation of the immuneresponse, response to cytokines, expression byliver, angiogenesis and muscle expansion (Fig. 2b;for full list see Table S11).
A panel of 30 genes discriminates between plaques from S and ASpatients
Prediction modelling was performed to determinemolecular signatures for classification of plaquesfrom S versus AS patients. A panel of 30 genes wasfound to be capable of predicting S and AS lesions
(a)
(b)
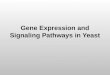
Fig. 2 Regulation of gene expression in carotid atherosclerosis. (a) MIR155HG was strongly upregulated in plaquescompared with normal arteries (mean difference � SD 1.627 � 0.2513; P < 0.0001), whilst MALAT1 was the mostupregulated gene in plaques extracted more than 1 month after symptom compared to those removed within <2 weeks(mean difference 1.018 � 0.3451; P = 0.0045). TP53TG1 was downregulated in the same comparison (mean difference�0.3072 � 0.1324; P = 0.0238). (b) Examples of transcription factors regulating genes associated with immune response,response to cytokines, angiogenesis and muscle expansion. Binding motifs are shown on the right-hand side.
L. Perisic et al. Atherosclerosis transcriptome
8 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine

with 78% accuracy, and 47% and 7% variabilityexplained by the first two principal componentsrespectively (Fig. 3). Of interest, many of thesegenes, such as HCG11, DNAJC19, ZNF41, ZNF493and RPL9, were involved in transcriptional regula-tion (Table S12). The panel also included genesassociated with lysosomes (PIK3C3 and CNO),cytokine signalling (ASB1), cholesterol distribution(TSPO2) and the ECM (CRTAC1).
Functional gene networks in carotid atherosclerosis
A meta-analysis was performed using a similarpublished data set [14] of CP samples from asmaller cohort of S and AS patients (12 S and 9 AS)with the same microarray platform and technicalrequirements as the BiKE. This analysis showedabout 20% overlap in significantly differentiallyexpressed probesets (Fig. 4a; for full list seeTable S13), such as CCL18, MMP12, CTSZ, CD36,CD163, IGFBP4, FABP5, GLUL, MYH11, SMTN,MYOCD and CNN1. From the full list of meta-genes, 85 of the most commonly reported and wellcharacterized in atherosclerosis [23, 40] wereselected for functional network construction(Fig. 4c), and GSEA showed that they were mainlyinvolved in ECM organization (FDR 1.53E-09),inflammation (FDR 3.71E-03), angiogenesis (FDR
3.46E-03) and response to hypoxia (FDR1.52E-02). Overall, 87% of these genes exhibitedstrong positive expression cross-correlations in theBiKE, many with Spearman r > 0.90 and P < 10E-30 (e.g. MMP12 and MMP9 with CD36 and CD163markers of macrophages; see representative heatplot in Fig. 4b and for full data see Table S14).When meta-genes were connected into an extendedprotein–protein interaction network, key interac-tion nodes were centred around Hif1a, Actn2,Cxcr4, S100A9, S100A10, Casp4, Hspg1, Ubc,Pdlim7, Nos1, Hspa6 and Egfr (Fig. 4d).
LMOD1, SYNPO2, PPBP and PLIN2 are dysregulated in carotidatherosclerosis
Many genes were identified in this study that hadpreviously not or only poorly been characterized inatherosclerosis. Several strongly dysregulatedgenes, representative of different cell types basedon publically available information (Table S2), werechosen for validation by IHC and qPCR. LMOD1and SYNPO2 were downregulated in CP versus NAmicroarrays (mean difference � SD �2.405 �0.2162, P < 0.0001 and �4.256 � 0.2827, P <0.0001, respectively) and in microarrays compar-ing S and AS patients (mean difference �1.431 �0.5172, P < 0.0001 and �1.709 � 0.3711,
(a) (b)
Fig. 3 Predictionmodelling for genes discriminating between plaques from symptomatic (S) and asymptomatic (AS) patients.Heat plot showing expressionprofile for a panel of 30 genes (a; patients presented on the x-axis) found to discriminate betweenplaques from S and AS patients with high accuracy as shown by the principal components analysis (b).
L. Perisic et al. Atherosclerosis transcriptome
ª 2015 The Association for the Publication of the Journal of Internal Medicine 9
Journal of Internal Medicine

P < 0.0001, respectively). PPBP and PLIN2 wereupregulated in CP versus NA tissues (mean differ-ence 3.560 � 0.3138, P < 0.0001 and2.640 � 0.2852, P < 0.0001, respectively) as wellas in S versus AS patients (mean difference1.439 � 0.5253, P < 0.0001 and 1.564 � 0.6460,P < 0.0001, respectively; Fig. 5a). The same trendsfor these genes were replicated in the microarrayvalidation data set (n = 50 patients; data notshown) and qPCR analysis in a separate subcohortof patients (n = 77, Fig. 5b): LMOD1 and SYNPO2were significantly downregulated in CP comparedwith NA tissues (mean difference�0.5654 � 0.2078 and �0.9424 � 0.1668,
respectively) and PPBP and PLIN2 were upregu-lated (mean difference 32.25 � 12.40 and8.701 � 1.156, respectively). The correspondingproteins were localized in plaques and normalinternal carotid artery by IHC (Fig. 5c; for addi-tional images and higher magnifications seeFig. S2). Ppbp (CXCL7) co-localized with the plate-let marker CD61 in areas of intraplaque haemor-rhage (IPH). Plin2 (perilipin 2) was co-localized withthe macrophage receptor CD68 mainly in foamcells. Lmod1 (leiomodin 1) and Synpo2 (synap-topodin 2) were expressed strictly by aSMA-positiveSMCs in the NA media, and no staining for thesetwo proteins was observed in CPs. Expression
(a) (b)
(c) (d)
Fig. 4 Network analyses of plaques from symptomatic (S) and asymptomatic (AS) patients. (a) Meta-analyses with anothersimilar publically available data set confirmed an overlap in significantly differentially expressed (DE) probesets comparingplaques from S and AS patients. (b) Many of the meta-genes showed strong positive expression correlations as depicted bythe heat plot representation of the large correlation Supplementary Table (white, correlation not significant; green,Spearman r ≤ 0.3; red, Spearman r > 0.3). (c) In the functional coupling network generated from meta-genes, response tohypoxia, regulation of immune response, angiogenesis, chemokine production and extracellular matrix organization werethe most significant functional categories. (d) When meta-genes were connected in a protein–protein interaction network,several nodes were distinctly populated with interactions.
L. Perisic et al. Atherosclerosis transcriptome
10 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine

correlations for LMOD1 and SYNPO2 in plaquearrays were positive solely with markers of differ-entiated SMCs whereas negative correlations wereobserved with cytokines, ECM degrading enzymesand inflammation markers (Table S15).
Discussion
Here, we present a comprehensive transcriptomicanalysis of human end-stage carotid atherosclero-sis in relationship to clinical parameters of plaqueinstability. We confirm established features ofvulnerable plaques and patients, but also revealnovel pathways and gene signatures determiningdisease phenotype. Data suggesting enhancedcalcification in patients on statin therapy and
rapid tissue repair followed by prolonged inflam-mation after plaque rupture were new observationsthat may be related to plaque stabilization, whilst,that is, processes associated with intraplaquehaemorrhage persisted in connection with vulner-able lesions. Coordination of gene expression andtranscription-regulating elements was shown to beessential in controlling the subtle overall differ-ences between S and AS disease. Importantly,many genes and candidate transcriptomicbiomarkers previously not characterized in unsta-ble atheroma were identified in our study.
Modest alterations in gene expression levels werefound in plaques and PBMCs from S and ASpatients, probably because these two groups
(a) (b) (c)
Fig. 5 Validation of novel genes from microarrays. LMOD1, SYNPO2, PPBP and PLIN2were some of the most dysregulatedgenes in microarrays (a) as confirmed by quantitative PCR (qPCR) (b). Data are presented in graphs as fold change � SD. (c)Immunohistochemistry (IHC) showed that Lmod1 and Synpo2 localized to alpha smooth muscle actin (aSMA)-positivesmooth muscle cells in normal carotid artery (left) whereas no staining was detected in the fibrous cap of plaques (right,arrowheads). Insets show the peripheral area of a plaque (with remains of the media) where Lmod1 and Synpo2 are notdetected either. Ppbp was detected in CD61-positive platelets at sites of intraplaque haemorrhage, whereas Plin2colocalized with CD68-positive foam cells in plaques (right, arrowheads). Ppbp and Plin2 were also expressed in normalartery adventitia and media, respectively (left, arrowheads).
L. Perisic et al. Atherosclerosis transcriptome
ª 2015 The Association for the Publication of the Journal of Internal Medicine 11
Journal of Internal Medicine

represent entities of the same underlying disease[14, 46]. Despite a reduction in sample size andstatistical power, we also compared gene expres-sion between different subgroups of patientphenotypes. It is interesting that more significantgene expression differences were observed whencomparisons were based on either the timebetween index symptoms and surgery or whetheror not patients received statin therapy. In Spatients treated with statins, pathways previouslyassociated with plaque stability such as suppres-sion of angiogenesis and MMPs were enriched.Notably, dysregulation of genes associated with theHMG CoA reductase pathway, such as AMFR [47],indicated direct effects of statins on plaques. Withrespect to the pleiotropic influence of statins, thedocumented decrease in cholesterol and LDL levelsalso indicates effects related to lipid lowering inthese patients [48]. Enrichment of pathwaysassociated with plaque calcification, such asregulation of calcium-mediated signalling andosteoblast differentiation, is a novel finding withthis methodological approach. This finding sug-gests that statins promote plaque stability ascalcified plaques have been associated with AScarotid disease [49] and statins have also beenshown to increase vascular calcification [50, 51].Interestingly, in the entire group of plaques from Spatients, bone resorption emerged as one of theenriched pathways. Taken together, these resultssuggest that statins mediate plaque stabilizationthrough calcification and by counteracting resorp-tion of calcified tissue. Mechanistically, theseeffects may be related to the lipid-lowering effectsof the treatment as hyperlipidaemia has beenshown to enhance osteoclast activity [52].
Because the risk of stroke in S patients with carotidstenosis decreases over time [4], plaques removedat different intervals after symptoms may representtime-dependent changes in plaque phenotype.Comparison of gene expression in plaques from Spatients who underwent surgery >1 month versus<2 weeks after symptom indicated altered plaquebiology following plaque rupture [23, 24, 53], withrecurrent upregulation of inflammatory processesin the later phases of the healing response anddownregulation of pathways associated with tissueregeneration. One of the most repressed genes wasMSTN, encoding a protein that regulates musclegrowth [54]. These findings are in contrast to thoseof some earlier studies [24, 53], but supportprevious conclusions from this cohort, and suggestthat the initial period after plaque rupture involves
a rapid initiation of tissue repair and SMCproliferation followed by a prolonged immuneresponse in the resolution phase towards restoredplaque stability [23].
Intraplaque haemorrhage, involving release fromred blood cells of Hb that is subsequently bound byHp to prevent oxidation [55], has previously beenrecognized in association with plaque instability. Inline with this, we found significantly lower Hblevels in S patients in our cohort. Furthermore, theHb–Hp complex was one of the most enriched GOcategories in plaques and Hb metabolism wasenriched in PBMCs. A common genetic variant ofHp has recently been associated with cardiovascu-lar disease risk in multiple independent cohorts,both in plaques and in peripheral blood [56–58],and Hp genotyping has been recommended for riskidentification and treatment optimization [56].
IL-1B secretion appeared as a major pathway inPBMCs and in CP tissue. In support of thisobservation, activation of IL-1B by cholesterol hasbeen reported in coronary atherosclerosis, andneutralization of IL-1B by a human monoclonalantibody canakinumab has been shown to reduceinflammation; this antibody is being investigatedas an attractive therapy for atherosclerosis [59].
In patients with increased stroke risk (TIA/MS),compared with those with AF [60], processes pre-viously associated with unstable lesions such asangiogenesis [61] were enriched and the mostupregulated gene was TUBB1, a platelet-specifictubulin variant linked to cardiovascular diseaserisk [62]. PTAFR (platelet-activating factor recep-tor), GP6 (platelet-specific glycoprotein VI) andgenes from the TREML family involved in plateletaggregation, inflammation and activation were alsoupregulated. These findings support the notionthat plaque rupture with platelet activation is moreprevalent in patients with TIA/MS than in thosewith ocular symptoms [63].
Here, we have shown that the profile of transcrip-tion factors in S compared with AS plaques reflectsthe same main pathways as in the gene expressionanalysis, and prediction modelling further empha-sized a central role for transcriptional regulation indetermination of patient phenotype. Previously, wehave reported that the predictive value of plaquesfor risk profiling is superior to that of bloodsamples [16]. The common gene expression pat-terns in S and AS plaques, especially those related
L. Perisic et al. Atherosclerosis transcriptome
12 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine

to chemokine signalling, apoptosis andcalcification, were highlighted in meta-analysesusing another publicly available data set. Together,these results suggest that the fine determination ofatherosclerosis state requires coordinatedregulation by multiple factors and plaque-specificnetworks. It is conceivable that end-stageatherosclerosis consists of an array of processeswhere minor alterations in plaque biology shift thebalance from a stable AS lesion to atherothrombo-sis and clinical symptoms. Similar observationshave recently been reported in cancers [44].
Many studies of novel target genes in atherosclero-sis using data from the BiKE have already beenreported [21, 23, 24, 29]. Here, the analysis revealedadditional genes that had not previously beenassociated with atherosclerosis, of which severalwere selected for replication in a nonoverlapping setof patients. LMOD1 (Leiomodin 1) has been pre-dicted to be an SMC-specific gene [64] and an SRF/MYOCD-dependent transcript [65] and SYNPO2(Synaptopodin 2) was predicted to be associatedwith SMC cytoskeletal organization [66]. BecauseLMOD1 and SYNPO2 were strongly downregulatedin plaques and correlated with all markers of differ-entiated SMCs, theymay represent novelmarkers ofSMC phenotype and should be explored in thecontext of SMC function in atherosclerosis. Themegakaryocyte PPBP gene product CXCL7 is aplatelet chemokine involved in vessel repair aftervascular injury [67] and was found in the presentstudy in plaques with IPH. Plin2 was detected infoam cells and cholesterol clefts within the necroticcore of plaques. Perilipin has previously beendescribed as an adipocyte protein that coats intra-cellular lipid droplets. It was proposed to contributeto inhibition of lipolysis [68, 69] and thus couldpromote plaque vulnerability through increasedlipid accumulation. Because of their associationwith IPH and lipid content, PPBP and Plin2 may beinteresting new candidate transcriptomic biomark-ers of unstable atheroma.
A limitation of this study is that the BiKE cohortcomprises only advanced lesions (American HeartAssociation grades IV and V), and therefore cannotprovide information about disease progression.This restricts the generalization of the presentresults to high-risk populations with end-stagedisease. It is most likely that the phenotyping ofpatients based on the presence or absence ofcerebral symptoms was insufficient to completelyexclude overlap between the groups, as lesions
from AS patients may vary with regard to morpho-logical features of plaque instability [46]. Unfortu-nately, histological plaque classification [70] wasincompatible with the sampling protocol used here.In analyses of time-dependent gene expressionchanges in plaques, two separate time-points weredefined, as too few patients underwent surgery inthe period between 2 weeks and 1 month aftersymptoms. In addition, comparisons based onstatin medication, time from symptom to surgeryand type of symptoms may be underpoweredregarding limited group sizes, but neverthelessmay provide novel insights into processes relatedto these clinical categories. Of note, even thesmallest subgroups of patients compared in thepresent study were larger than in most publishedhuman atherosclerosis microarray studies.
Consensus is lacking regarding the selection ofappropriate control tissues, and arteries of variousembryonic origins have been used for this purposeas well as adjacent macroscopically intact parts oflesions [40, 71]. In this study, control vesselscontained outer media that is not included in theendarterectomy intimal samples. From a technicalviewpoint, it is noteworthy that the gene arrayplatform used here does not provide a completeanalysis of ncRNAs. From a conceptual viewpoint,it should be noted that, even if the complexity oflarge-scale gene expression analyses is reduced byconstruction of functional networks, this method islimited in its ability to identify novel pathways as itis based on existing literature and databases. Weobtained similar overall results in our analyses ofindependent S versus AS array data sets of differ-ent sizes, suggesting that increasing the number ofpatients does not necessarily improve the discoveryof new pathways.
In conclusion, extensive analysis of the transcrip-tomic landscape in human atherosclerosis, incombination with patient phenotyping, facilitatednovel discoveries related to overall plaque insta-bility, time-dependent gene expression changesand medication. Although expression analysesfrom clinical samples cannot prove a causalrelationship between increased gene expressionand disease state, our findings provide a powerfulplatform for further functional and mechanisticexploration of novel molecular signatures incarotid atherosclerosis, which may aid in thedevelopment of clinical biomarkers and targetedmolecular imaging for identification of vulnerablepatients and lesions.
L. Perisic et al. Atherosclerosis transcriptome
ª 2015 The Association for the Publication of the Journal of Internal Medicine 13
Journal of Internal Medicine

Acknowledgements
The authors would like to thank Malin Kronquist,Ingrid T€ornberg, Anneli Olsson and Linda Haglund(Karolinska Institute, Stockholm, Sweden) forskilful technical assistance and Siw Frebelius(Karolinska Institute) for long-standing adminis-trative support.
Funding sources
This study was supported by the Swedish Heartand Lung Foundation, the Swedish ResearchCouncil (K2009-65X-2233-01-3, K2013-65X-06816-30-4 and 349-2007-8703), UppdragBesegra Stroke (P581/2011-123), the StrategicCardiovascular Programs of Karolinska Institutetand Stockholm County Council, the StockholmCounty Council (ALF-2011-0260 and ALF-2011-0279), the Foundation for Strategic Research andthe European Commission (CarTarDis, AtheroR-emo, VIA and AtheroFlux projects).
Conflict of interest statement
No conflicts of interest to declare.
References
1 Libby P, Ridker PM, Hansson GK. Progress and challenges in
translating the biology of atherosclerosis. Nature 2011; 473:
317–25.
2 Hansson GK. Inflammation, atherosclerosis, and coronary
artery disease. N Engl J Med 2005; 352: 1685–95.
3 Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP, Barnett
HJ; Carotid Endarterectomy Trialists C. Endarterectomy for
symptomatic carotid stenosis in relation to clinical subgroups
and timing of surgery. Lancet 2004; 363: 915–24.
4 Giles MF, Rothwell PM. Risk of stroke early after transient
ischaemic attack: a systematic review and meta-analysis.
Lancet Neurol 2007; 6: 1063–72.
5 Rothwell PM. Prediction and prevention of stroke in patients
with symptomatic carotid stenosis: the high-risk period and
the high-risk patient. Eur J Vasc Endovasc Surg 2008; 35:
255–63.
6 Redgrave JN, Lovett JK, Gallagher PJ, Rothwell PM.
Histological assessment of 526 symptomatic carotid plaques
in relation to the nature and timing of ischemic symp-
toms: the Oxford plaque study. Circulation 2006; 113:
2320–8.
7 Crisby M, Nordin-Fredriksson G, Shah PK, Yano J, Zhu J,
Nilsson J. Pravastatin treatment increases collagen content
and decreases lipid content, inflammation,
metalloproteinases, and cell death in human carotid
plaques: implications for plaque stabilization. Circulation
2001; 103: 926–33.
8 Kunte H, Amberger N, Busch MA, Ruckert RI, Meiners S,
Harms L. Markers of instability in high-risk carotid plaques
are reduced by statins. J Vasc Surg 2008; 47: 513–22.
9 Lockhart DJ, Winzeler EA. Genomics, gene expression and
DNA arrays. Nature 2000; 405: 827–36.
10 Hiltunen MO, Tuomisto TT, Niemi M et al. Changes in gene
expression in atherosclerotic plaques analyzed using DNA
array. Atherosclerosis 2002; 165: 23–32.
11 Ijas P, Nuotio K, Saksi J et al. Microarray analysis reveals
overexpression of CD163 and HO-1 in symptomatic carotid
plaques. Arterioscler Thromb Vasc Biol 2007; 27: 154–60.
12 Randi AM, Biguzzi E, Falciani F et al. Identification of
differentially expressed genes in coronary atherosclerotic
plaques from patients with stable or unstable angina by
cDNA array analysis. J Thromb Haemost 2003; 1: 829–35.
13 Woodside KJ, Hernandez A, Smith FW et al. Differential gene
expression in primary and recurrent carotid stenosis.
Biochem Biophys Res Commun 2003; 302: 509–14.
14 Saksi J, Ijas P, Nuotio K et al. Gene expression differences
between stroke-associated and asymptomatic carotid pla-
ques. J Mol Med 2011; 89: 1015–26.
15 Sluimer JC, Kisters N, Cleutjens KB et al. Dead or alive: gene
expression profiles of advanced atherosclerotic plaques from
autopsy and surgery. Physiol Genomics 2007; 30: 335–41.
16 Folkersen L, Persson J, Ekstrand J et al. Prediction of
ischemic events on the basis of transcriptomic and genomic
profiling in patients undergoing carotid endarterectomy. Mol
Med 2012; 18: 669–75.
17 Miller CL, Haas U, Diaz R et al. Coronary heart disease-
associated variation in TCF21 disrupts a miR-224 binding
site and miRNA-mediated regulation. PLoS Genet 2014; 10:
e1004263.
18 Kojima Y, Downing K, Kundu R et al. Cyclin-dependent
kinase inhibitor 2B regulates efferocytosis and atherosclero-
sis. J Clin Investig 2014; 124: 1083–97.
19 Smedbakken LM, Halvorsen B, Daissormont I et al. Increased
levels of the homeostatic chemokine CXCL13 in human
atherosclerosis - Potential role in plaque stabilization.
Atherosclerosis 2012; 224: 266–73.
20 Salagianni M, Galani IE, Lundberg AM et al. Toll-like receptor
7 protects from atherosclerosis by constraining “inflamma-
tory” macrophage activation. Circulation 2012; 126: 952–62.
21 Perisic L, Hedin E, Razuvaev A et al. Profiling of atheroscle-
rotic lesions by gene and tissue microarrays reveals PCSK6 as
a novel protease in unstable carotid atherosclerosis. Arte-
rioscler Thromb Vasc Biol 2013; 33: 2432–43.
22 Wang J, Razuvaev A, Folkersen L et al. The expression of IGFs
and IGF binding proteins in human carotid atherosclerosis,
and the possible role of IGF binding protein-1 in the regula-
tion of smooth muscle cell proliferation. Atherosclerosis 2012;
220: 102–9.
23 Razuvaev A, Ekstrand J, Folkersen L et al. Correlations
between clinical variables and gene-expression profiles in
carotid plaque instability. Eur J Vasc Endovasc Surg 2011;
42: 722–30.
24 Agardh HE, Folkersen L, Ekstrand J et al. Expression of fatty
acid-binding protein 4/aP2 is correlated with plaque
instability in carotid atherosclerosis. J Intern Med 2011;
269: 200–10.
25 Gertow K, Nobili E, Folkersen L et al. 12- and 15-lipoxy-
genases in human carotid atherosclerotic lesions:
L. Perisic et al. Atherosclerosis transcriptome
14 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine

associations with cerebrovascular symptoms. Atherosclerosis
2011; 215: 411–6.
26 Gistera A, Robertson AK, Andersson J et al. Transforming
growth factor-beta signaling in T cells promotes stabilization
of atherosclerotic plaques through an interleukin-17-depen-
dent pathway. Sci Transl Med 2013; 5: 196ra00.
27 Gabrielsen A, Qiu H, Back M et al. Thromboxane synthase
expression and thromboxane A2 production in the
atherosclerotic lesion. J Mol Med 2010; 88: 795–806.
28 Olofsson PS, Soderstrom LA, Jern C et al. Genetic variants of
TNFSF4 and risk for carotid artery disease and stroke. J Mol
Med 2009; 87: 337–46.
29 Osterholm C, Folkersen L, Lengquist M et al. Increased
expression of heparanase in symptomatic carotid atheroscle-
rosis. Atherosclerosis 2013; 226: 67–73.
30 Ovchinnikova OA, Folkersen L, Persson J et al. The collagen
cross-linking enzyme lysyl oxidase is associated with the
healing of human atherosclerotic lesions. J Intern Med 2014;
276: 525–36.
31 Persson J, Folkersen L, Ekstrand J et al. High plasma
adiponectin concentration is associated with all-cause mor-
tality in patients with carotid atherosclerosis. Atherosclerosis
2012; 225: 491–6.
32 Rothwell PM, Pendlebury ST, Wardlaw J, Warlow CP. Critical
appraisal of the design and reporting of studies of imaging and
measurement of carotid stenosis. Stroke 2000; 31: 1444–50.
33 Halliday A, Harrison M, Hayter E et al. 10-year stroke
prevention after successful carotid endarterectomy for
asymptomatic stenosis (ACST-1): a multicentre randomised
trial. Lancet 2010; 376: 1074–84.
34 Lesack K, Naugler C. An open-source software program for
performing Bonferroni and related corrections for multiple
comparisons. J Pathol Inform 2011; 2: 52.
35 Glaab E, Garibaldi JM, Krasnogor N. ArrayMining: a modular
web-application for microarray analysis combining ensemble
and consensus methods with cross-study normalization.
BMC Bioinformatics 2009; 10: 358.
36 Xia J, Fjell CD, Mayer ML, Pena OM, Wishart DS, Hancock
RE. INMEX–a web-based tool for integrative meta-analysis of
expression data. Nucleic Acids Res 2013; 41: W63–70.
37 Wu J, Vallenius T, Ovaska K, Westermarck J, Makela TP,
Hautaniemi S. Integrated network analysis platform for
protein-protein interactions. Nat Methods 2009; 6: 75–7.
38 Cowley MJ, Pinese M, Kassahn KS et al. PINA v2.0: mining
interactome modules. Nucleic Acids Res 2012; 40: D862–5.
39 Le Cao KA, Boitard S, Besse P. Sparse PLS discriminant
analysis: biologically relevant feature selection and graphical
displays for multiclass problems. BMC Bioinformatics 2011;
12: 253.
40 Papaspyridonos M, Smith A, Burnand KG et al. Novel candi-
date genes in unstable areas of human atherosclerotic
plaques. Arterioscler Thromb Vasc Biol 2006; 26: 1837–44.
41 Rothwell PM. ACST: which subgroups will benefit most from
carotid endarterectomy? Lancet 2004; 364: 1122–3; author
reply 5-6.
42 Tripathi V, Ellis JD, Shen Z et al. The nuclear-retained
noncoding RNA MALAT1 regulates alternative splicing by
modulating SR splicing factor phosphorylation. Mol Cell
2010; 39: 925–38.
43 Michalik KM, You X, Manavski Y et al. Long noncoding RNA
MALAT1 regulates endothelial cell function and vessel
growth. Circ Res 2014; 114: 1389–97.
44 Ren S, Peng Z, Mao JH et al. RNA-seq analysis of prostate
cancer in the Chinese population identifies recurrent gene
fusions, cancer-associated long noncoding RNAs and aber-
rant alternative splicings. Cell Res 2012; 22: 806–21.
45 Takei Y, Ishikawa S, Tokino T, Muto T, Nakamura Y. Isolation
of a novel TP53 target gene from a colon cancer cell line
carrying a highly regulated wild-type TP53 expression sys-
tem. Genes Chromosom Cancer 1998; 23: 1–9.
46 Salem MK, Vijaynagar B, Sayers RD et al. Histologically
unstable asymptomatic carotid plaques have altered expres-
sion of genes involved in chemokine signalling leading to
localised plaque inflammation and rupture. Eur J Vasc
Endovasc Surg 2013; 45: 121–7.
47 Song BL, Sever N, DeBose-Boyd RA. Gp78, a membrane-
anchored ubiquitin ligase, associates with Insig-1 and cou-
ples sterol-regulated ubiquitination to degradation of HMG
CoA reductase. Mol Cell 2005; 19: 829–40.
48 Farmer JA. Pleiotropic effects of statins. Curr Atheroscler Rep
2000; 2: 208–17.
49 Kwee RM. Systematic review on the association between
calcification in carotid plaques and clinical ischemic symp-
toms. J Vasc Surg 2010; 51: 1015–25.
50 Saremi A, Bahn G, Reaven PD, Investigators V. Progression of
vascular calcification is increased with statin use in the
Veterans Affairs Diabetes Trial (VADT). Diabetes Care 2012;
35: 2390–2.
51 Grasser WA, Baumann AP, Petras SF et al. Regulation of
osteoclast differentiation by statins. J Musculoskelet Neuronal
Interact 2003; 3: 53–62.
52 Tintut Y, Morony S, Demer LL. Hyperlipidemia promotes
osteoclastic potential of bone marrow cells ex vivo. Arte-
rioscler Thromb Vasc Biol 2004; 24: e6–10.
53 Peeters W, Hellings WE, de Kleijn DP et al. Carotid atheroscle-
rotic plaques stabilize after stroke: insights into the natural
process of atherosclerotic plaque stabilization. Arterioscler
Thromb Vasc Biol 2009; 29: 128–33.
54 Kostek MA, Angelopoulos TJ, Clarkson PM et al. Myostatin
and follistatin polymorphisms interact with muscle pheno-
types and ethnicity. Med Sci Sports Exerc 2009; 41: 1063–71.
55 Levy AP, Moreno PR. Intraplaque hemorrhage. Curr Mol Med
2006; 6: 479–88.
56 Ijas P, Saksi J, Soinne L et al. Haptoglobin 2 allele associates
with unstable carotid plaque and major cardiovascular
events. Atherosclerosis 2013; 230: 228–34.
57 Degraba TJ, Hoehn GT, Nyquist PA et al. Biomarker discovery
in serum from patients with carotid atherosclerosis. Cere-
brovasc Dis Extra 2011; 1: 115–29.
58 Wingrove JA, Daniels SE, Sehnert AJ et al. Correlation of
peripheral-blood gene expression with the extent of coronary
artery stenosis. Circ Cardiovasc Genet 2008; 1: 31–8.
59 Ridker PM, Howard CP, Walter V et al. Effects of interleukin-
1beta inhibition with canakinumab on hemoglobin A1c,
lipids, C-reactive protein, interleukin-6, and fibrinogen: a
phase IIb randomized, placebo-controlled trial. Circulation
2012; 126: 2739–48.
60 Benavente O, Eliasziw M, Streifler JY, Fox AJ, Barnett HJ,
Meldrum H; North American Symptomatic Carotid
Endarterectomy Trial C. Prognosis after transient monocular
blindness associated with carotid-artery stenosis. N Engl J
Med 2001; 345: 1084–90.
61 McCarthy MJ, Loftus IM, Thompson MM et al. Angiogenesis
and the atherosclerotic carotid plaque: an association
L. Perisic et al. Atherosclerosis transcriptome
ª 2015 The Association for the Publication of the Journal of Internal Medicine 15
Journal of Internal Medicine

between symptomatology and plaque morphology. J Vasc
Surg 1999; 30: 261–8.
62 Freson K, De Vos R, Wittevrongel C et al. The TUBB1 Q43P
functional polymorphism reduces the risk of cardiovascular
disease in men by modulating platelet function and structure.
Blood 2005; 106: 2356–62.
63 Howard DP, van Lammeren GW, Redgrave JN et al.
Histological features of carotid plaque in patients with
ocular ischemia versus cerebral events. Stroke 2013; 44:
734–9.
64 Nelander S, Mostad P, Lindahl P. Prediction of cell type-
specific gene modules: identification and initial characteriza-
tion of a core set of smooth muscle-specific genes. Genome
Res 2003; 13: 1838–54.
65 Nanda V, Miano JM. Leiomodin 1, a new serum response
factor-dependent target gene expressed preferentially in dif-
ferentiated smooth muscle cells. J Biol Chem 2012; 287:
2459–67.
66 Schroeter MM, Beall B, Heid HW, Chalovich JM. In vitro
characterization of native mammalian smooth-muscle protein
synaptopodin 2. Biosci Rep 2008; 28: 195–203.
67 Gleissner CA, von Hundelshausen P, Ley K. Platelet chemoki-
nes in vascular disease. Arterioscler Thromb Vasc Biol 2008;
28: 1920–7.
68 Martinez-Botas J, Anderson JB, Tessier D et al. Absence of
perilipin results in leanness and reverses obesity in Lepr(db/
db) mice. Nat Genet 2000; 26: 474–9.
69 Tansey JT, Sztalryd C, Gruia-Gray J et al. Perilipin ablation
results in a lean mouse with aberrant adipocyte lipolysis,
enhanced leptin production, and resistance to diet-induced
obesity. Proc Natl Acad Sci USA 2001; 98: 6494–9.
70 Lovett JK, Redgrave JN, Rothwell PM. A critical appraisal of
the performance, reporting, and interpretation of studies
comparing carotid plaque imaging with histology. Stroke
2005; 36: 1091–7.
71 Turpeinen H, Raitoharju E, Oksanen A et al. Proprotein
convertases in human atherosclerotic plaques: the overex-
pression of FURIN and its substrate cytokines BAFF and
APRIL. Atherosclerosis 2011; 219: 799–806.
Correspondence: Ljubica Perisic, PhD, Department of Molecular
Medicine and Surgery, Division of Vascular Surgery, L8:03,
Karolinska Institute, SE-171 76 Stockholm, Sweden.
(fax: +468339309; e-mail: [email protected]).
and
Prof Ulf Hedin, MD, PhD, Department of Vascular Surgery,
Karolinska University Hospital A2:01 SE-171 76 Stockholm,
Sweden. (fax: +468339309; e-mail: [email protected]).
Supporting Information
Additional Supporting Information may be found inthe online version of this article:
Figure S1. Pathway analysis of genes differentiallyexpressed in plaques vs. normal arteries.
Figure S2. Additional photomicrographs showingcellular localizationofnovelgenes frommicroarrays.
Table S1. Demographics of the patient cohorts(*P < 0.05, ns-nonsignificant).
Table S2 Summary of antibodies used in valdationof microarray results.
Table S3. Most highly significantly dysregulatedprobes in microarray comparison plaque tissuesymptomatic vs. asymptomatic.
Table S4. Most highly significantly upregulatedprobes in microarray comparison PBMCs symp-tomatic vs. asymptomatic.
Table S5. GO terms enriched in comparisonsbetween symptomatic and asymptomatic patients.
Table S6. Most significantly upregulated probes inmicroarray comparison symptomatic plaqueTIA+MS vs AF.
Table S7. Most significantly upregulated probes inmicroarray comparison symptomatic plaque >1month vs <2 weeks.
Table S8. Most highly significantly upregulatedprobes in microarray comparison symptomaticplaque statins yes vs no.
Table S9. GOtermsenriched in comparisons sortedaccording to clinical parameters of instability.
Table S10. ncRNAsdifferentially regulated in different atherosclerosisprofiles.
Table S11. Transcription factors and miRs regu-lating the genes differentially expressed in symp-tomatic vs. asymptomatic plaques.
Table S12. Panel of genes obtained by predictivemodelling in S vs. As patient’s plaques.
Table S13. Genes with significant combined p-values from meta-analysis.
Table S14. Expression correlation matrix for genesfrom meta-analyses (Spearman r values given,p < 0.05 after correction for multiple testing).
Table S15. Expression correlations for LMOD1and SYNPO2 with markers from plaque arrays.
L. Perisic et al. Atherosclerosis transcriptome
16 ª 2015 The Association for the Publication of the Journal of Internal Medicine
Journal of Internal Medicine