Embed Size (px)
Citation preview

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 483
Review Articles
Gene Expression Profiling Data inLymphoma and Leukemia
Review of the Literature and Extrapolation of Pertinent Clinical Applications
Cherie H. Dunphy, MD
● Context.—Gene expression (GE) analyses using microar-rays have become an important part of biomedical andclinical research in hematolymphoid malignancies. How-ever, the methods are time-consuming and costly for rou-tine clinical practice.
Objectives.—To review the literature regarding GE datathat may provide important information regarding patho-genesis and that may be extrapolated for use in diagnosingand prognosticating lymphomas and leukemias; to presentGE findings in Hodgkin and non-Hodgkin lymphomas,acute leukemias, and chronic myeloid leukemia in detail;and to summarize the practical clinical applications in ta-bles that are referenced throughout the text.
Data Source.—PubMed was searched for pertinent lit-erature from 1993 to 2005.
Conclusions.—Gene expression profiling of lymphomasand leukemias aids in the diagnosis and prognostication ofthese diseases. The extrapolation of these findings to more
timely, efficient, and cost-effective methods, such as flowcytometry and immunohistochemistry, results in better di-agnostic tools to manage the diseases. Flow cytometric andimmunohistochemical applications of the informationgained from GE profiling assist in the management ofchronic lymphocytic leukemia, other low-grade B-cell non-Hodgkin lymphomas and leukemias, diffuse large B-celllymphoma, nodular lymphocyte–predominant Hodgkinlymphoma, and classic Hodgkin lymphoma. For practicalclinical use, GE profiling of precursor B acute lymphoblas-tic leukemia, precursor T acute lymphoblastic leukemia,and acute myeloid leukemia has supported most of the in-formation that has been obtained by cytogenetic and mo-lecular studies (except for the identification of FLT3 mu-tations for molecular analysis), but extrapolation of theanalyses leaves much to be gained based on the GE pro-filing data.
(Arch Pathol Lab Med. 2006;130:483–520)
Gene expression (GE) analyses by use of microarrays(MAs) have become an important part of biomedical
and clinical research, and the resulting data may provideimportant information regarding pathogenesis and maybe extrapolated for use in diagnosing and prognosticatinglymphomas and leukemias. This article will review thevarious techniques used in GE profiling (GEP) and thensystematically review the discoveries in various types oflymphomas (including Hodgkin lymphoma [HL] and non-HL [NHL]), acute leukemia, and chronic myeloid leuke-mia (CML). The findings in these various types of lym-phoid and hematologic malignancies are presented in de-tail, with the pertinent practical clinical applications sum-marized in tables that are referenced throughout the text.
TECHNIQUES OF GEPMicroarrays contain precisely positioned DNA probes
that are designed to specifically monitor the expressionlevels of genes in parallel. Data mining often utilizes
Accepted for publication December 14, 2005.From the Department of Pathology and Laboratory Medicine, The
University of North Carolina at Chapel Hill.The author has no relevant financial interest in the products or com-
panies described in this article.Reprints: Cherie H. Dunphy, MD, Department of Pathology and Lab-
oratory Medicine, The University of North Carolina at Chapel Hill, CB7525, Chapel Hill, NC 27599-7525 (e-mail: [email protected]).
mathematic techniques that are traditionally used to iden-tify patterns in complex data. Supervised and unsuper-vised approaches may be used.
Supervised GEP
To correlate array data directly to clinical, cytomor-phologic, or cytogenetic features, the application of a su-pervised analysis typically requires the grouping of pa-tients according to predefined characteristics. After de-tecting differential GE, it is often necessary to accuratelyclassify samples into known groups.1 In supervised ma-chine learning methods, the observer derives GEP on atraining set of cases and then tests the predictive powerof this GEP on a set of previously unanalyzed test cases.Many of these techniques, particularly when leave-one-outcross-validation is performed on large data sets, requireextensive parametric studies or the solution of large ma-trix problems that can only be done using parallel com-puters. Therefore, these methods require carefully de-signed cohorts, cross-validation, and statistical analyses. Itis best to confirm preliminary results on independent datasets. Willman2 developed and applied several differentlearning methods for class prediction in leukemia cohorts,including Bayesian networks and support vector ma-chines. A Bayesian network is a graph-based model forrepresenting probabilistic relationships between randomvariables. A Bayesian network asserts that each node is

484 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
statistically independent of all its nondescendants, oncethe values of its parents (immediate ancestors) in thegraph are known. This makes Bayesian networks an at-tractive framework for GE analysis, because they can me-thodically hypothesize and test gene regulatory models(and other relationships) using the rigorous methods ofclassic probability theory and statistics. Support vectormachines attempt to define the maximal hyperplane (orcorridor) between 2 parameters (such as long-term remis-sion vs failure) in a GE data set. This corridor (or hyper-plane) may be linear or nonlinear. Genes marking theboundaries of this hyperplane are the most discriminat-ing. A first step in most classification models is the appli-cation of feature selection techniques to identify uniqueand robust gene sets that best discriminate among theclasses of interest. Recursive feature elimination is a sup-port vector machine–based method for feature selection inbinary classification problems. Recursive feature elimina-tion searches through the given gene space of approxi-mately 12 000 genes to find the optimal hyperplane sepa-rating the 2 classes.
Unsupervised GEP
By contrast, clustering is an unsupervised method fororganizing expression data into groups with similar sig-natures. Unsupervised clustering can be used not only toreduce the complexity of the matrix-like data and to vi-sualize it in a more understandable way but also to predictthe categorization of unknown samples, as well as for classdiscovery, the discovery of intrinsic biologic groups of pa-tients based on shared patterns of GE.2 Patterns are dis-covered solely from the data, without assumptions of pre-vious knowledge or grouping of the data. Many mathe-matical algorithms can be used for class discovery, includ-ing hierarchic clustering (HC), K-means, self-organizingmaps, and principal component analysis. Two-dimension-al HC sorts patients and genes according to similaritiesand leads to a tree-structured dendrogram that can easilybe viewed and explored. This hierarchic structure pro-vides potentially useful information about the relationshipbetween adjacent clusters. Common crossing points rep-resent similar patient characteristics and similarities withregard to the coexpression of distinct genes. By use of adetailed gene annotation, functional groupings of genesbased on their similarity may be discovered in GEP. Suchinformation can offer insights into physiologic pathwaysand may also help to characterize genes of uncertain func-tion. However, except for principal component analysis,most unsupervised HC algorithms are not multidimen-sional enough or stable enough to resolve multiple clustersin large data sets. Willman2 developed higher-order mul-tidimensional clustering algorithms such as VxInsight(Sandia National Laboratories, Albuquerque, NM), whichhas the capacity to cluster patients or genes in a novel andintuitive way, using all of the GE data without having toselect smaller subsets of genes for actual clustering. Sim-ilar genes are clustered together spatially and are repre-sented in a 3-dimensional terrain map, on which largemountains represent large clusters of similar genes andsmaller hills represent clusters with fewer genes. Clustersthat are the most similar (genes or patients) are also sitednearer to each other and farther away from less similarclusters.
Comparison of Detection of Protein Expression Levelsand Messenger RNA by Flow Cytometry and MA Analysis
A study compared the methodologies of flow cytometry(FC) and MA in parallel and correlated the protein ex-pression levels and messenger RNA (mRNA) abundanceof 39 relevant genes in 113 patients with newly diagnosedacute myeloid leukemia (AML) and acute lymphoblasticleukemia (ALL) and in 4 normal bone marrow (BM) sam-ples.3 There was a significant correlation between proteinexpression and mRNA abundance for genes that are es-sential for diagnosing and subclassifying AML and ALLwith regard to positivity and expression.
Usefulness of Ready-Made Macroarrays
Dales et al4 determined the usefulness of ready-mademacroarrays as routine diagnostic tools by analyzinglymph node (LN) biopsies (4 follicular lymphomas [FLs],2 diffuse large B-cell lymphomas [DLBCLs], and 3 benignLNs). In the clustered array data, purified cells that weresorted from samples sharing common histologic lesionswere grouped together, whereas the array and histologycorrelation was less satisfactory for tissues. Gene expres-sion profiling of the array and the immunohistochemistry(IHC) methods correlated for most caspases and samples,suggesting that pathologists in the future might be able toanalyze, using IHC methods, potential markers of interestthat were previously identified using array technology.The reliability of the array analysis on tissues remainsquestionable, because even NHL samples of the same typeare intrinsically heterogeneous regarding their neoplasticand reactive cell contents. The correlation between HCand histologic features is better for purified cells than fortissues. This could possibly hamper the use of the methodfor routine diagnostic purposes because the preparation ofthe sorted cells is technically more complex.
Likewise, Staal et al5 reviewed the applications and in-frastructure for MA experiments. These were illustratedvia an MA-based comparison of GEP of paired diagnosis–relapse samples from patients with precursor B ALL (BALL). Initial experiments showed that several seeminglydifferentially expressed genes were actually derived fromcontaminating nonleukemic cells, particularly myeloidcells and T lymphocytes. In addition, extra RNA amplifi-cation led to skewing of particular gene transcripts. Thesetechnical aspects should be considered when applyingthese techniques to lymphoma and leukemia diagnosisand prognosis. The application of GEP to lymphoid ma-lignancies (chronic lymphocytic leukemia, NHLs, andHLs) will be discussed in the sections that follow.
CHRONIC LYMPHOCYTIC LEUKEMIA
Differentiation of Chronic Lymphocytic Leukemia CellsFrom Normal Lymphocytes
Using 3 different MA platforms (oligonucleotide arraysand complementary DNA [cDNA] arrays printed on glassslides and printed on nylon membranes), Wang et al6
found that several genes were consistently differentiallyexpressed between chronic lymphocytic leukemia (CLL)and normal B-cell (NBC) samples. The following 10 geneshave been shown to be differentially expressed in CLLcompared with tonsillar B lymphocytes and plasma cells:FCER2 (CD23), FGR, TNFRSF1B, CCR7, IL4R, PTPN12,FMOD, TMEM1, CHS1, and ZNF266.7

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 485
Table 1. Prognostic Factors in Chronic Lymphocytic Leukemia (CLL) and Correlation WithPractical Clinical Applicability*
Prognostic Factor Effect on Outcome Correlation With Practical Clinical Measurement
Mutational status of IGVH† Mutated IGVH, associated with better OSUnmutated IGVH, associated with worse OS
No detection of ZAP70 expressionUnmutated IGVH with up to 93% concordance
with ZAP70 expression; no detection of ZAP70expressed due to rare biologic occurrence
HTERT Increased expression associated with advancedstage and shorter OS
NA
ZAP70‡ ZAP70 expression, associated with worse OS andup to 93% concordance with unmutated IGVH
May be detected by IF, FC, IHC, and RT-PCR tech-niques
* Data are from Damle et al,10 Hamblin et al,11 Oscier et al,12 Tchirkov et al,13 Staudt,14 Orchard et al,15 Ferrer et al,16 Weistner et al,17 Weistnerand Staudt,18 and Crespo et al.19 IGVH indicates immunoglobulin heavy-chain variable region; OS, overall survival; HTERT, human telomerasereverse transcriptase; NA, not applicable; IF, immunofluorescence; FC, flow cytometry; IHC, immunohistochemistry; and RT-PCR, real-time poly-merase chain reaction.
† Considered the single most informative stage-independent prognostic factor.‡ Considered the CLL subtype distinction gene.
Diagnosis of CLLThe results of GEP of CLL cells appear to be closest to
those of resting blood, nonproliferating B cells, or memoryB cells rather than to those of naive, germinal center (GC),mitogenically activated blood cells or CD5-positive Bcells.8,9 Other genes have been termed CLL signature genesbecause they are selectively expressed in CLL and not innormal or other types of B-cell malignancies.9 The CLLsignature included genes that were known to be charac-teristic of CLL, such as CD5, IL2RA (CD25), and bcl-2, aswell as genes not previously known to be expressed inCLL, such as WNT3 and ROR1. A study comparing GEPof purified tumor cells from untreated patients with CLLand from patients who were newly diagnosed as havingmultiple myeloma (MM) by MA and HC analysis (6800genes) showed that CLL and MM have distinct GEP.7
Chronic lymphocytic leukemia differentially expressedhigher levels of the tumor necrosis factor (TNF)–TNF re-ceptor pathway genes LTB, TRAF5, TNFRSF9, TNFSF7,and LITAF. The IAP family gene (BIRC1) and the XIAPantagonist (HSXIAPAF1) were expressed at higher levelsonly in CLL. bcl-2 Expression was also higher in CLL thanin MM. However, investigators in this study concludedthat the relative mRNA expression was a reliable predictorof phenotype for only 4 of 10 diagnostically importantgenes in CLL and MM, suggesting an important limitationof the current clinical utility of GE analysis. Table 1 sum-marizes the prediction of prognosis.
IGVH Mutational StatusIn B-cell CLL (B-CLL), the immunoglobulin heavy-chain
variable region may be mutated or unmutated. It has beenrecognized that the presence or absence of somatic mu-tations in the immunoglobulin heavy-chain regions of CLLcells distinguishes 2 clinically distinct forms. Patientswhose CLL cells contained unmutated IGVH genes (im-munoglobulin-unmutated CLL) have a much worse over-all survival (OS), with a shorter median survival (79–119months), than patients whose CLL cells had mutatedIGVH genes (immunoglobulin-mutated CLL), who have amedian survival reaching 293 months and many of whomnever require treatment.10–12 IGVH mutational status hasbeen considered the single most informative stage-inde-pendent prognostic factor in CLL.12
Human telomerase reverse transcriptase has been as-sociated with disease aggressiveness in human cancers. A
study using real-time polymerase chain reaction (RT-PCR)to quantitate the amount of human telomerase reversetranscriptase and analyzing for somatic mutations inIGVH genes in mononuclear blood cells from 90 patientswith CLL revealed that the HTERT gene was detected in59% of patients.13 The level of expression increased withadvancing B-CLL stage (P 5 .006). Not surprisingly, thepatients expressing HTERT showed significantly shortersurvival than HTERT -negative patients (P , .001), irre-spective of the disease stage. On average, the level ofHTERT mRNA expression was 7-fold higher in the poorprognosis (immunoglobulin-unmutated) CLL group thanin the immunoglobulin-mutated group (P , .001), and thelevel of HTERT expression discriminated between the 2groups in 89% of cases.
The CLL subtypes (mutated vs unmutated IGVH)showed enhanced expression of genes that are related toB-cell activation through the B-cell receptor (BCR).14 Spe-cifically, genes that are up-regulated during BCR stimu-lation were more highly expressed in immunoglobulin-unmutated CLL, and genes that are down-regulated dur-ing BCR stimulation were expressed at lower levels in thisgroup. This finding suggests that stimulation through theBCR may play a role in the pathogenesis of CLL. It isfurther suggested that ongoing BCR stimulation in the im-munoglobulin-unmutated CLL subtype contributes to themore progressive clinical course of these patients.
However, 2 recent studies demonstrated that, regardlessof IGVH mutational status, all CLL cases share a broad-range common GE signature that is distinct from normaland other malignant cells.8,9 Although GEP data of a com-mon signature supports the concept that CLL is one dis-ease, the clinical differences between immunoglobulin-un-mutated and immunoglobulin-mutated CLL suggest thatthere are GEP differences between these 2 subgroups.
Indeed, Rosenwald et al9 found more than 100 genesthat were differentially expressed between the 2 CLL sub-types, with high statistical significance. The most differ-entially expressed gene was ZAP70, which encodes a ty-rosine kinase. It was expressed in all immunoglobulin-un-mutated CLL samples and in some B-cell lymphoma celllines but in none of the immunoglobulin-mutated CLLsamples. Another study demonstrated that samples of pu-rified B lymphocytes from healthy individuals all showedZAP70 values of less than 10% (NBCs do not expressZAP70).15

486 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
ZAP70
Subsequently, Ferrer et al16 analyzed GEP of 20 immu-noglobulin-unmutated and 11 immunoglobulin-mutatedCLL samples and investigated the VH gene mutation sta-tus by sequencing. The array data showed that the greatestvariances between the unmutated groups and the mutatedgroups were in expressions of ZAP70, RAF1, PAX5, TCF1,CD44, SF1, S100A12, NUP214, DAF, GLVR1, MKK6, AF4,CX3CR1, NAFTC1, and HEX. ZAP70 was significantlymore expressed in the immunoglobulin-unmutated CLLgroup, whereas expression of all the other genes was high-er in the immunoglobulin-mutated cases. This study con-firmed that ZAP70 expression could predict the VH mu-tation status and suggested that RAF1, PAX5, and otherdifferentially expressed genes may be good markers fordifferentiating between these 2 groups and can serve asprognostic markers.
Weistner et al17 further profiled an expanded cohort of107 patients with CLL and confirmed that ZAP70 was thesingle best gene distinguishing the unmutated and mu-tated subtypes. Immunoglobulin-unmutated CLL samplesexpressed ZAP70 5.54-fold more highly than immuno-globulin-mutated CLL samples (P , .001). ZAP70 expres-sion correctly predicted the IGVH mutational status in93% of patients. ZAP70 expression and IGVH mutationstatus were comparable in their ability to predict the timeto requirement of therapy following diagnosis.
Methods of Detection of ZAP70 Expression
ZAP70 expression may be detected at the mRNA leveland by various techniques, including immunofluorescence,FC, and IHC.15 The sensitivity and specificity of ZAP70 byimmunofluorescence detection have been reported as be-ing 91% and 100%, respectively.13 The detection of ZAP70expression by these various techniques has been comparedwith the IGVH mutational status and has revealed occa-sional discordant results between ZAP70 expression andmutational status.
Discordance Between IGVH Mutational Status andZAP70 Expression
In 7 of 107 patients, Weistner and Staudt18 showed dis-cordant results between ZAP70 expression and IGVH mu-tational status (4 immunoglobulin-mutated CLL sampleshad high ZAP70 expression and 3 immunoglobulin-un-mutated CLL samples had low ZAP70 expression).Among these ZAP70 outliers, the 4 patients with immu-noglobulin-mutated CLL had clinical features that are un-characteristic of this CLL subtype: 2 patients required ear-ly treatment, and 2 patients had a mutated VH321 gene(an IGVH gene that has been associated with progressivedisease). In addition, the investigators in this study de-veloped RT-PCR and IHC assays for ZAP70 expressionthat could be applied clinically and determined thatZAP70 was the best gene to distinguish between CLL sub-types. Based on their findings, these authors suggestedthat CLL should be considered a continuum of diseasesrather than 2 discrete subtypes and stressed that, whileIGVH mutational status and ZAP70 expression can defineprognostically distinct subtypes of CLL, some patientswith immunoglobulin-mutated CLL may have progressivedisease, and some patients with immunoglobulin-unmu-tated CLL may remain stable for long periods or showonly minimal disease progression.
Because of the detection of these discordant cases, asubsequent study by Orchard et al15 clarified whether themutational status of the IGVH gene best predicted the clin-ical outcome in CLL and assessed whether ZAP70 may beused as a prognostic marker in CLL. They developed anFC assay for ZAP70 protein expression and investigatedits concordance with ZAP70 mRNA expression, IGVHgene mutational status, and clinical outcome in 167 patientwith CLL. This study showed high concordance betweenZAP70 protein expression and IGVH gene mutations. Onehundred eight (65%) of 167 patients had mutated IGVHgenes and were ZAP70 negative; 46 (28%) of the 167 hadunmutated IGVH genes and were ZAP70 positive. Find-ings were discordant in 13 of the 167 patients: 6 had mu-tated IGVH genes but were ZAP70 positive and 7 had un-mutated genes and were ZAP70 negative. The expressionof mRNA showed 97% concordance with ZAP70 proteinexpression. The median survival was 24.4 years in ZAP70-negative patients and 9.3 years in ZAP70-positive patients.In regard to the discordant cases, 5 of 6 patients who ex-pressed ZAP70 but had mutated IGVH genes had 97%homology to the germline sequence, and 1 patient had96% homology. These patients would be judged as havinga poor outlook in investigations in which 95% or 97% ho-mology is used to define prognostic subgroups. All pa-tients with less than 95% homology failed to expressZAP70, emphasizing the correlation between ZAP70 ex-pression and a low mutational load rather an absence ofmutations. The 7 patients with 98% or greater homologyto the germline sequence who were ZAP70 negative areof even more biologic interest. Crespo et al19 identified 3similar patients and concluded that this finding representsa biologic occurrence rather than a technical difficulty inZAP70 measurement. Longer follow-up of many more dis-cordant cases will be needed to ascertain whether ZAP70expression or IGVH gene mutational status is the betterpredictor of patients’ clinical courses.
Correlation Between ZAP70 and Deletion of 13q14Genome-wide expression profiling of micro RNA
(miRNA) in human B-CLL, using an MA containing hun-dreds of human precursor and mature miRNA oligonu-cleotide probes, identified at least 2 clusters of CLL sam-ples that were associated with the presence or absence ofZAP70 expression.20 Two miRNA sequences were associ-ated with the presence or absence of mutations: expressedIGVH genes correlated with the presence of mutations,and deletions of 13q14 correlated with the absence of mu-tations. Because they had a single cytogenetic defect, thesepatients with CLL had a good prognosis, and samplesfrom these patients were associated with the presence ofmutated IGVH genes. The specific signature profile asso-ciated with the expression of mutated IGVH was com-posed of 5 differentially expressed genes (MIR186,MIR132, MIR161, MIR192, and MIR29C). The common el-ement between the 13q14 deletion–related and the IGVH-related signatures was MIR161.
Additional Prognostic Indicators in CLLThe presence of CD38 has previously been shown to
indicate the worst prognosis in CLL.15 However, in thatstudy by Orchard et al15 CD38 was measured by FC, hadweak prognostic value in univariate analysis, and did notimprove the predictive power of ZAP70 or IGVH gene mu-tational status in multivariate analysis.

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 487
Table 2. Immunohistochemical Stains of Practical Use in Non–Chronic Lymphocytic Leukemia Cases Based onGene Expression Profiling Data
Type of Small B-Cell Malignancy Immunohistochemical Marker Clinical Use or Indication
Mantle cell lymphomaHairy cell leukemiaFollicular lymphoma
Cyclin D1Annexin A1CD68
Diagnosis associated with worst prognosis29
Diagnosis specific to hairy cell leukemia45
Increased number associated with better prognosis39
Genomic aberrations and survival in CLL were the fo-cus of a study by Dohner et al.21 Unbalanced genomic ab-errations concerning 17p or 11q were shown to be impor-tant independent predictors of disease progression andsurvival.
Stratowa et al22 studied 54 peripheral blood (PB) lym-phocyte samples from patients with B-CLL to determinethe expression levels of 1024 selected genes on a cDNAMA, and expression levels correlated with patient surviv-al. The reduced expression of the genes coding for inter-leukin 1b (IL-1b), IL-8, and L-selectin in B-CLL cells cor-related with a significantly reduced OS compared withpatients showing higher rates of expression. In contrast,high expression of TCL1 correlated with diminished pa-tient survival. These findings suggest that B-CLL prog-nosis may be related to a defect in lymphocyte trafficking,causing accumulation of leukemic B cells in the PB.
Zent et al23 identified patterns that seemed to discrimi-nate between indolent and aggressive CLL in untreatedpatients. Gene expression profiling was determined for 7patients with untreated indolent CLL and for 5 patientswith untreated aggressive CLL. A set of 16 differentiallyexpressed genes was identified that could distinguish be-tween the indolent and aggressive groups. This referenceset of genes was then used to predict the clinical classifi-cation of 5 additional patients with CLL, all of whom werecorrectly classified, 4 in the indolent group and 1 in theaggressive group. Results of this study suggest that GEPcould be used to predict the rate of progression of CLL,although the authors recommended a larger study for con-firmation of their findings.
Studies of Resistant CLL SamplesA study comparing GEP of 4 sensitive CLL samples and
of 3 resistant CLL samples to in vitro radiation-inducedapoptosis using 2 series of MA analyses (before and afterthe apoptotic stimulus of radiation) detected 16 genes thatwere differentially expressed ($2-fold, specifically in re-sistant cells).24 The findings of these selected genes werethen validated by quantitative RT-PCR on 7 MA samples,and their altered expression level was confirmed on 15additional CLL samples that were not included in the MAanalysis. In 11 sensitive and 11 resistant CLL samples test-ed, the following 13 genes were specific for all resistantsamples: nuclear orphan receptor TR3, major histocom-patibility complex (MHC) class II glycoprotein HLA-DQA1, MTMR6, CMYC, CREL, CIAP1, and FMOD wereup-regulated, whereas MIP1A/GOS191 homologue,STAT1 , BLK, HSP27, and ECH1 were down-regulated. Thisstudy defined new molecular markers that are specific toresistant CLL subsets that could be of clinical relevance.
Gene expression profiling to investigate the molecularconsequences of fludarabine phosphate therapy amongpatients with CLL was further studied by Rosenwald etal.25 In 7 CLL samples, a consistent GE signature of in vivofludarabine exposure was identified. Many of the fludar-
abine signature genes were known p53 target genes andgenes involved in DNA repair. Because in vivo treatmentwith fludarabine induces a p53-dependent GE response,this treatment has the potential to select p53 mutant CLLcells, which are more drug resistant and are associatedwith an aggressive clinical course. Therefore, treatment ofpatients with CLL with fludarabine has the potential toselect for outgrowth of p53 mutant subclones that wouldbe cross-resistant to several other chemotherapeuticagents. It is also possible that p53 mutant CLL cells couldcause a more aggressive disease on the basis of recentevidence that deletion of the p53 locus is associated witha poor prognosis.
Future DirectionsA dual enzyme global methylation study showed that
CLL is characterized by widespread nonrandom CpG is-land methylation (an epigenetic alteration that contributesto tumorigenesis by transcription inactivation of genes).26
The authors of that study provide a panel of novel meth-ylation targets that may be used in larger studies that aredesigned to assess the effect on disease progression andsurvival.
MANTLE CELL LYMPHOMADifferentiation From Normal Lymphocytes
Similar to CLL, differential GE using high-density (HD)MA chips has identified 300 to 400 genes that are dereg-ulated in mantle cell lymphoma (MCL) samples comparedwith NBC populations.27 Genes that are involved in anti-proliferative signaling in NBCs were deregulated in MCLsamples. In addition, lymphoproliferative signal pathwayswere active, and genes encoding receptors for differentneurotransmitters mediating B-cell stimulation were up-regulated in MCLs compared with NBCs.
Diagnosis of MCLMantle cell lymphoma is known to be associated with
t(11;14)(q13;q32), resulting in deregulated cyclin D1 ex-pression.28 High levels of cyclin D1 are associated withgreater proliferation and with poorer survival (Table 2).29
A determination of these abnormalities is important for adiagnosis of MCL, and they have conventionally been de-tected by routine cytogenetics and fluorescence in situ hy-bridization (FISH) techniques for t(11;14) and by IHC forcyclin D1 protein overexpression.
More recently, a GEP study was performed among 101lymphoma cases that were morphologically consistentwith MCL.30 Of these, 92 cases showed high expression ofcyclin D1 mRNA by quantitative RT-PCR. More than 1000genes were differentially expressed between cyclin D1–positive MCLs and other lymphoma subtypes, with highstatistical significance. A GE-based predictor of MCL wasfashioned from 42 of the most discriminatory genes, yield-ing an MCL signature. Cyclin D1 was excluded to testwhether cyclin D1–negative MCL samples could be iden-

488 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
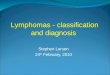
Figure 1. Expression of MCL signature genes in 7 cyclin D1–positiveand 7 cyclin D1–negative lymphoma cases. Cyclin D1–negative caseshad mantle cell lymphoma (MCL) morphology and immunophenotypeand were classified as being MCL based on their gene expression pro-file. Shown is the relative gene expression of cyclin D1 (as measuredby quantitative real-time polymerase chain reaction) and cyclins D2and D3 (as measured by DNA microarray analysis). Data are fromRosenwald et al30 and are reprinted with permission from Elsevier Inc,New York, NY.
tified by the predictor. The predictor correctly classified98% of cyclin D1–positive MCL samples. Of the 9 cyclinD1–negative MCL samples, 7 were classified as MCL bytheir expression of the MCL signature genes. Three ofthese tumors expressed high levels of cyclin D3 or cyclinD2, suggesting that these proteins may functionally sub-stitute for cyclin D1 in these MCL samples (Figure 1). Theexistence of cyclin D1–negative MCLs with MCL signatureGEP, some with overexpression of cyclin D2 or cyclin D3,has been confirmed in an additional study, indicating thatoverexpression of cyclin D1–related cyclins may have apathogenetic role in these cases.29
Prediction of PrognosisGene expression data have also been used to search for
molecular determinants of the length of survival of pa-
tients with MCL.30 A supervised analysis of 92 cyclin D1–positive MCL samples identified 48 genes whose expres-sion correlated with survival duration (P 5 .001); all ofthese genes were more robustly expressed in tumors thatwere associated with the worst clinical outcome.26 Hier-archic clustering analysis revealed 2 subpopulations ofMCLs, which indicated that, despite the homogeneousstrong expression of cyclin D1, further subtyping was pos-sible. A subset of 20 proliferation signature genes was themost predictive. Most of these genes were expressed athigher levels in dividing cells than in quiescent cells. De-letion of p16INK4a and increased cyclin D1 coding regionmRNA expression were found to be statistically indepen-dent predictors of a high proliferation rate and a shortsurvival in MCL.31,32 This is due to the fact that anothermolecular mechanism underlying the enhanced prolifer-ation of some MCLs is the deletion of the INK4a/ARF lo-cus, which encodes 2 tumor suppressor genes, includingp16INK4a and p14ARF.31,32 The expression of cyclin D1 washigher in MCL samples from patients with a poor prog-nosis; deletions of the INK4a/ARF locus (CDKN2A) weredetected in about 20% of MCL samples from patients witha poor prognosis. The INK4a/ARF deletion and cyclin D1overexpression independently contributed to reduced pa-tient survival. These findings suggest that inhibitors of cy-clin D1 function should prolong the lives of patients withMCL.
Blastoid Variant of MCL
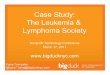
In the aggressive blastoid variant of MCL (MCL-BV),overexpression of genes that are involved in cell cycle con-trol at the G1/S and G2/M checkpoints and in apoptosisinhibition has been identified.33 Studies using gene arrayand comparing GEP of microdissected normal mantlecells, MCL cells, and MCL-BV cells using oligonucleotideMAs and quantitative RT-PCR have identified 118 genesthat show significant differential expression between MCLand MCL-BV, including tumor suppressors, transcriptionfactors, proto-oncogenes, and genes that are associatedwith cell cycle regulation, proliferation, chromatin assem-bly, mitosis, and spindle assembly.33 The highly expressedcyclin-dependent kinase (CDK) 4 is a cell cycle kinase thatassociates with cyclin D1 for the progression through theG1/S checkpoint, whereas the overexpression of CDC28protein kinase 1 blocks the inhibition of the cyclin D1/CDK4 complex by the CDK inhibitor p27/Kip1. Otherhighly expressed genes in MCL-BV that promote passageof cells through the G1/S checkpoint include the onco-genes BMYB, PIM1, and PIM2, and passage through theG2/M checkpoint is enhanced by high levels of CDC25B.In addition, 2 highly expressed genes that inhibit apopto-sis are defenders against cell death (DAD1) and RSK1. Fur-thermore, the transcription factor YY1, which is involvedin cyclin D1 overexpression, has been shown to be in-creased in MCL-BV (Figure 2).33,34 These findings suggesta potential pathogenetic role of these genes in the evolu-tion of MCL-BV.
FOLLICULAR LYMPHOMA
Comparison With Normal GC B Cells
Gene expression profiling of normal GC B (GCB) cellshas been shown to be unchanged in FL, supporting theview that this lymphoma arises from this stage of B-celldifferentiation.35 However, using a cDNA MA with 588

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 489
Figure 2. Hierarchic clustering of differentially expressed genes in mantle cell lymphoma (MCL) and blastoid variant of MCL (MCL-BV). Thegenes displayed were identified by 2 independent search strategies. Five samples of MCL and 4 samples of MCL-BV are shown. Red indicatesincreased expression; blue, decreased expression, and yellow, unchanged. Data are from de Vos et al33 and are reprinted with permission.
cDNAs, Husson et al36 identified 28 genes that were down-regulated and 37 genes that were up-regulated in FL cellscompared with normal GCB cells. The expression level ofeach differentially expressed gene was verified by quan-titative PCR, resulting in 24 up-regulated genes and 8down-regulated genes (P , .10). Up-regulated genes inFL included 2 cell cycle regulator proteins that are in-volved in G1 arrest, p21CIP1 and p16INK4a, which is consis-tent with the low proliferative nature of FL cells. Up-reg-ulated genes included cell cycle regulator proteins(CDK10, p120, p21CIP1, and p16INK4a), genes that are involved
in cell-cell interactions (TNF, IL2RG, and IL4RA), and thetranscription factors PAX5 and Id-2 that are involved inNBC development. Down-regulated genes in FL includedMRP8 and MRP14, which are involved in adhesion.
Grade of Disease and Disease AggressivenessSupervised classification of paired FLs with indolent
and aggressive disease courses has established GEP of 81genes that accurately classified 93% of FL samples in anindependent validation set.37 Most important, in a thirdseries of FLs with ambiguous histologic grading, this 81-

490 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
member GEP set showed a classification accuracy of 94%.37
Genes that are significantly up-regulated in the aggressivephase of the disease include those involved in cell cyclecontrol (CCNE2, CCNA2, CDK2, CHEK1, and MCM7) andDNA synthesis (TOP2A, POLD3A, HMGA1, POLE2,GMPS, and CTPS), as well as those reflecting increasedmetabolism (FRSB, RARS, HK2, and LDHA) and activationof several signaling pathways (FRZB, HCFCR1, PIK4CA,and MAPK1). Genes that are derived from the reactiveinfiltrate of T cells and macrophages (CD3D, CXCL12, andTM4SF2) were up-regulated in the indolent phase of thedisease.
Dave et al38 determined the prognostic significance ofthe ‘‘nonmalignant’’ components of the tumor microen-vironment in FL. Using whole-genome MA analysis of 191untreated FL samples, they further defined 2 GE signa-tures of tumor-infiltrating immune cells that by multivar-iate analysis predicted survival in FL. Genes that wereassociated with a favorable prognosis had an ‘‘immuneresponse 1 signature,’’ and genes that were associatedwith an unfavorable prognosis had an ‘‘immune response2 signature.’’ The immune response 1 signature includedgenes encoding T-cell markers (CD7, CD8B1, ITK, LEF1,and STAT4 ) and genes that are highly expressed in mac-rophages (ACTN1 and TNFSF13B). The immune response2 signature included genes known to be preferentially ex-pressed in macrophages, dendritic cells, or both (TLR5,FCGR1A, SEPT10, LGMN, and C3AR1). A more recentstudy by Farinha et al39 demonstrated that the lymphoma-associated macrophage content, detected by CD68 IHC,within FLs is an independent predictor of OS. The studycomprised 99 FLs. Patients with FLs with 15 or moreCD68-positive macrophages per high-power field had abetter OS than those with FLs with less than 15 CD68-positive macrophages per high-power field, independentof the International Prognostic Index (IPI) score.
Prediction of Disease Response to RituximabBy analyzing the expression of more than 20 000 genes
in FL samples from patients who received rituximab ther-apy, Bohen et al40 identified differentially regulated genesin responding and nonresponding patients. There were 2groups of tumors, one that clustered with normal lym-phoid tissues from spleen and tonsil and the other thatclustered with more malignant cells. Rituximab nonre-sponders comprised the normal lymphoid tissue group,whereas rituximab responders mainly comprised the oth-er group. An analysis of the statistically significant differ-entially expressed genes between the 2 groups suggeststhat the major differences lie in the antilymphoma im-mune response profiles between nonresponders and re-sponders. Another study analyzing GEP of FL samplesfrom 24 patients before rituximab therapy showed thatGEP in the nonresponders, again, appeared to be moresimilar to GEP of normal lymphoid tissues than to GEPof responders.41
MARGINAL ZONE LYMPHOMATranslocations involving the MALT1 gene have been
identified in a subset of extranodal marginal zone lym-phomas (MZLs).42 The presence of this translocation instomach tumors indicated that the tumor is no longer re-sponsive to antibiotic therapy that is directed against Hel-icobacter pylori. Marginal zone lymphomas also may rarelyprogress to a large cell lymphoma.43
In addition, deregulated MALT1 expression may occurin other histologic subtypes of B-cell NHL (B-NHL)through translocation to the IGH locus or by genomic am-plification.27 This study also examined the structure andGEP of genomic amplifications involving 18q21 in a panelof 40 B-NHL cell lines using comparative genomic hybrid-ization to MAs and GEP techniques. Using array compar-ative genomic hybridization, 2 peaks of genomic amplifi-cation were observed (one centered around bcl-2 and theother around MALT1). The translocation t(14;18) may in-volve MALT1 rather than bcl-2 in MZLs and lymphomasof mucosa-associated tissues. Molecular cloning of variant14;18 break points identified MALT1 as the targeted gene.MALT1 is a target for amplification and overexpression inthe 18q21 amplicon of B-NHL. Of the 3 cell lines withMALT1 amplification, 2 showed MALT1 overexpression asassessed by GEP, quantitative RT-PCR, and Western blotanalysis.
HAIRY CELL LEUKEMIA
Differentiation From Normal B Lymphocytes
Compared with GEP of purified NBC subpopulations,hairy cell leukemia (HCL) cells are more related to mem-ory cells.44 However, compared with memory cells, HCLcells display a remarkable conservation in proliferation,apoptosis, and DNA metabolism programs, whereas theyappear to be significantly altered in the expression ofgenes controlling cell adhesion and response to chemo-kines. Within the proliferation program, the exceptions ofcyclin D1 and CHC1L are notable, which were clearly up-regulated in HCL. In addition, several genes encoding ad-hesion molecules that are absent in memory B cells areexpressed in HCL cells (GARP, CD9, CD103, and PCDH9),while RNA species that are expressed in memory B cellsare not expressed in HCL (CD1C and ICAM3), suggestingthe acquisition of peculiar adhesion properties by HCL.Gene expression profiling of HCL showed a homogeneouspattern of GE that is distinct from that of the other B-NHLs.
Diagnosis of HCL
Several genes have been specifically identified in HCLby GEP, and their expression has been confirmed at theprotein level by IHC analysis.44 Some of these genes werealready known to be expressed in HCL (cyclin D1, FGF2,and IL3RA). The expression of only 7 genes was found tobe decreased in HCL cells compared with all other sam-ples; these included the chemokine receptor CXCR5, whichis involved in B-cell homing, and the TNF receptor–asso-ciated factor 5, which is involved in the signal transduc-tion of TNF-type receptors, including CD40 and CD27.44
Among the recently identified genes that are overex-pressed in HCL are GAS7, a growth arrest–specific genethat is essential for neurite outgrowth in cultured cere-bellar neurons (overexpression of GAS7 in HCL may ex-plain the characteristic projections of the hairy cells); theFGFR1 receptor, which with overexpression of its ligandsuggests the presence in HCL of an autocrine loop; thereceptor tyrosine kinase FLT3, which functions as agrowth factor receptor for hematopoietic stem cell or pro-genitor cells; and 3 different inhibitors of matrix metallo-proteinases (TIMP1 and TIMP4, 2 secreted tissue inhibi-tors of metalloproteinases, and RECK, a membrane-an-chored glycoprotein that represses synthesis and secretion

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 491
of metalloproteinases). The up-regulated mRNA expres-sion in HCL cells was confirmed for the following proteinsby IHC analysis: FGF2, annexin 1, CD135 (FLT3), sodium-positive CP type I (SCN1B), CD63, syndecan-3, TIMP1,IL-3Ra, cyclin D1, FGFR1, GAS7, EPB4.1L2, b-actin,CPVL, b-arrestin 2, insulin-like growth factor bindingprotein, MYF6, protein tyrosine phosphatase receptor m,synaptotagmin 1, plexin-C1, TIMP4, and b2-microglobu-lin. Investigators in a subsequent study stained 500 B-celltumors with antiannexin A1 and showed that antiannexinA1 protein expression was specific to HCL (Table 2).45 Itwas especially useful in differentiating HCL from spleniclymphoma with villous lymphocytes and from HCL var-iant (2 entities that are sometimes in the differential di-agnosis of HCL). The findings of the studies about theseproteins have biologic implications that are relevant to thepathogenesis of HCL and clinical implications for its di-agnosis and therapy.44,45
DIFFERENTIATION OF REACTIVE LNs FROM FL, MCL,AND SMALL LYMPHOCYTIC LYMPHOMA OR CLL
By GEP analysis, 120 genes were identified as being sig-nificantly differentially expressed between reactive LN tis-sue and the following 3 types of small B-cell lymphomas:FL, MCL, and small lymphocytic lymphoma (SLL) orCLL.46 A subset of 39 genes was selected based on theirhigh differential expression by array analysis, and 23 werevalidated by quantitative RT-PCR. Among these 23 vali-dated genes were cyclin D1 (CCND1) and B-CLL/lym-phoma 2 (bcl-2) (Table 2); the remaining 21 genes have noestablished role in lymphoma development. The expres-sion of CCND1 and 7 additional genes was studied byquantitative RT-PCR in a panel of individual specimens.CCND1 was significantly overexpressed in MCL. bcl-2 Wassignificantly overexpressed in SLL relative to reactivenodes (RNs), was 2.3-fold increased in FL relative to RN(P 5 .002), was 1.9-fold overexpressed in FL relative toMCL (P 5 .001), and was 2.3-fold overexpressed in SLLrelative to MCL (P 5 .01). CJUN was significantly over-expressed in MCL relative to FL, RN, and SLL. DNAmethyltransferase 3A (DNMT3A) was significantly over-expressed in MCL relative to FL and CLL. CD69 was over-expressed in MCL relative to RN. CMYB was significantlyunderexpressed in MCL versus SLL. ESTMGC40441 (orHGAL and GCET2) was overexpressed in RN and FL rel-ative to MCL and CLL, which was consistent with theoverexpression of this gene product in FL, purified GCBcells, and GCB-like DLBCLs, relative to SLL and MCLspecimens.
DIFFERENTIATION OF SLL OR CLL FROM FLThe most prominent distinction between CLL and FL
came from genes that are characteristic of GCB cells (clus-ter 10).35,46 These were distinguishable from resting bloodB cells and from in vitro–activated blood B cells.
DIFFERENTIATION OF NON-FLsThieblemont et al47 identified for the first time 7 genes
(of 588) that allowed distinction of the 3 major subtypesof nonfollicular small B-cell lymphomas (SLL, splenicMZL, and MCL) through specific GEP, using cDNA ma-croarray analysis. Although 93% of the transcripted geneson the macroarray had similar levels of expression in the3 lymphoma subtypes, 7 of the transcripted genes (bcl-2,bcl-1, MMP17, a3 type IV collagen, NOTCH2, UPAR, and
TIMP1) were expressed at significantly different levels ineach subtype. Validation by quantitative RT-PCR showedthat all selected genes, except for a3 type IV collagen,were differentially expressed as observed in the macro-analysis, supporting the following 4 conclusions. (1) Rel-ative amounts of bcl-2 and MMP17 mRNA were signifi-cantly increased in SLL compared with splenic MZL andMCL. (2) NOTCH2 mRNA was significantly increased insplenic MZL compared with the other 2 subtypes. (3) bcl-1, UPAR, and TIMP1 were increased in MCL comparedwith the other 2 subtypes. (4) a3 Type IV collagen showedheterogeneity between the 3 subtypes. Three of these dif-ferentially expressed genes (MMP17, UPAR, and TIMP1)are related to the interaction of lymphoma cells with theextracellular matrix.
Investigators in a subsequent study, aimed at the iden-tification of specific genomic signatures for these same 3lymphoma subtypes, analyzed 128 primary tumors usingHD MAs.48 Using 44 genes selected within the gene clus-ters that were discriminant for the 3 lymphoma subtypes,investigators in this study generated a class predictionscore that allowed classification of the 3 entities in 96% ofcases, including borderline cases. Whereas specific tran-scription profiles easily distinguished MZLs, SLLs, andmost of the MCLs, a few MCLs exhibited MZL-type tran-scription profiles. Survival among 5 patients with ‘‘mis-classified’’ MCL was not significantly different from thatof other patients with MCL. In addition, 5 CD5-positivesplenic MZL samples and 3 CD5-negative MCL samplesexpressed the expected signatures corresponding to theirsubtype.
Several clusters of genes significantly discriminated the3 subtypes as follows.48 (1) Genes associated with cell ad-hesion, angiogenesis, and inhibition of apoptosis (bcl-2,survivin, and TNFR10) were identified as being up-regu-lated in SLL. The common CLL signatures included L-selectin and P-selectin, titin, IL4R, CCR, adenylate kinase,diacylglycerol kinase, cyclin D2, and bcl-2 overexpression.(2) Genes associated with intracellular signaling, via theAKT1 pathway, were up-regulated in splenic MZL. SplenicMZLs were specifically characterized by the overexpres-sion of a gene cluster containing AKT1. In the same genecluster, the analysis showed S100A proteins and AGERgrouped together with the same overexpression amongthe MZL samples. The expression of several other genesthat are related to transcription were significantly corre-lated in this AKT1 cluster, including ZFP36, which codesfor a zinc finger protein that is related to the TNF-a–in-duced inflammatory process; MXI1, a maximum interact-ing protein; and TFCP2, a transcription factor for CP2 in-teracting with the a-globin gene promoter. (3) Genes as-sociated with cell cycle control and multidrug resistancewere up-regulated in MCL. A comparison of the MCL-specific signature with the SLL and MZL signaturesshowed high levels of expression of cell cycle progressiongenes that function in the G1 phase (such as cyclin D1 andCDK4), in the G2/M phase (such as cyclin F), or in both(such as PCNA, which is responsible for controlling thetransition from the G1 phase to the S phase and from theG2 phase to the M phase). Moreover, when consideringMCL analysis, clustering resulted in the delineation of 2signatures, the cyclin D1 signature and a signature thatincluded all the other MCL genes. This suggests that, ifcyclin D1 overexpression is important and is consideredto be characteristic of MCL, cyclin D1 overexpression

492 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
alone is not sufficient to provide an MCL phenotype andthat the control of cyclin D1 expression is independent ofthat of other MCL-specific genes. In this case, entry intothe S phase may depend on the overexpression of othercyclins (such as cyclin D2 or cyclin D3), which supportsthe previous discussion regarding GEP data in MCL. Geneexpression–increased cell cycle activity was correlated toan overexpression of (1) genes encoding for protein ma-chinery (actin b and g genes; TUBB2, a b-tubulin type IIgene; DDBN1 or debrin 1, actin-binding proteins that areinvolved in the regulation of the growth process; BMP4,or bone morphogenetic protein 4; and SMARCA4, an ac-tin-dependent regulator of chromatin) and (2) genes en-coding for cell proliferation (FYN, ABL, PTK, and KIT en-coding for tyrosine kinase proteins). Several genes that en-code for membrane transporters and that are implicatedin drug resistance were also overexpressed, including 2GSTP and 2 multidrug resistance/ATP-binding cassettemembrane proteins (ABCG2 and ABCC5). This overex-pression of several genes related to multidrug resistanceis consistent with the known MCL clinical evolution thatis marked by treatment failure, leading to fatal recurrence,with a median survival of about 3 years.
DIFFUSE LARGE B-CELL LYMPHOMA
Distinction of De Novo DLBCL From DLBCL ofFollicular Origin
Follicular lymphomas may progress or transform toDLBCL, and most DLBCLs are of follicle center cell origin,but DLBCLs may also arise de novo. In a study by Lossoset al,49 DLBCLs derived from FLs were distinguishablefrom de novo DLBCLs by GEP. The most prominent dif-ferences were in proliferation and cell cycle genes, c-Myctarget genes, MHC genes, and a miscellaneous group ofother genes, including CD20, CD52W, WAS, LYN, andSYK. Compared with de novo FL, GEP of transformedDLBCL was closer to GEP of FL than to GEP of de novoDLBCL. In the transformed group, genes that were relatedto proliferation, basic metabolism, and invasion were up-regulated, while antiapoptotic genes, accessory genes, andT-cell–related genes were down-regulated.50 In a study byHuang et al,51 all DLBCLs carrying a translocation (14;18)belonged to the GCB-like group. As will be discussed, thedistinction between these entities is important because ofprognostic implications.
Prediction of Prognosis
A study by Alizadeh et al35 revealed that GEP ofDLBCLs was largely distinct from GEP of CLL and GEPof FL and showed additional biologic complexity. Thegenes that defined GCB-like DLBCL were highly ex-pressed in normal GCB cells. In contrast, most of thegenes that defined activated B-cell–like (ABC) DLBCLwere not expressed in normal GCB cells. Known markersof GC differentiation included CD10, CD38, nuclear factor(NF) A-myb, the DNA repair protein 8-oxoguanine DNAglycosylase (OGG1), bcl-6, and other new genes (bcl-7Aand LMO2). The ABC DLBCL signature also included agene that is translocated in lymphoid malignancies, IRF4(MUM1/LSIRF). Another notable feature of GEP of ABCDLBCLs was the expression of 2 genes whose productsinhibit programmed cell death, FLIP (FLICE-like inhibi-tory protein, which can block apoptosis) and the key an-tiapoptotic gene bcl-2 (which is 4-fold higher than in GCB
cells). This overexpression did not correlate with the bcl-2translocation.
Germinal center B–like and ABC DLBCLs were associ-ated with statistically significant differences in OS (P ,.01) and event-free survival.35 Seventy-six percent of pa-tients with GCB-like DLBCL were alive after 5 years, com-pared with only 16% of patients with ABC DLBCL. Thisdifference remained after consideration of the IPI score.Therefore, GEP of DLBCL and the IPI apparently identifydifferent features of these patients that affect survival.
Based on the MA data by Alizadeh et al,35 Ando et al52
created a method for the precise and simple prediction ofsurvival of patients with DLBCL by developing a fuzzyneural network (FNN) model. The FNN is an advancedartificial neural network model in which causality be-tween input and output variables can be accurately de-scribed as linguistic ‘‘if-then’’ rules from the acquiredmodel. In this study, a type I FNN was used to establishthe relationship between GE and clinical outcome. Fromdata on 5857 genes, this model identified 4 genes (CD10,AA807551, AA805611, and IRF4) that could be used to pre-dict the prognosis (4-year survival rate) with 93% accu-racy among 40 patients with DLBCL. CD10 was the firstgene selected and was more strongly expressed in DLBCLsurvivors than in those who died. The next 2 genes(AA807551—stronger expression in those who died andAA805611—lower expression in those who died) were un-identified genes. The fourth gene selected was IRF4 (orMUM1), which is associated with a poorer prognosis. Pa-tients with low expression of CD10 were predicted to havea poorer prognosis in the FNN model, particularly whencombined with high IRF4 expression. The FNN modelalso identified patients with a poor prognosis, despite ahigh expression ratio of CD10. The correct identificationof these cases was obtained by adding the expression in-formation of the other 2 unidentified genes; the outcomesof patients were poor even with high CD10 expression ifAA807551 expression was high and AA805611 expressionwas low. There was independence of the predictive valueof the FNN model and the IPI; however, the FNN wasmore informative in combination with clinical presenta-tion.
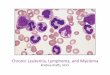
Rosenwald et al53 later used DNA MAs and identifiedthe following 3 GE subgroups of DLBCL based on HC:GCB-like, ABC, and type 3 DLBCL (which did not expresseither set of genes at a high level and was associated withan intermediate outcome) (Figure 3). There were 4 GE sig-natures that correlated with survival: GCB cells, prolifer-ating cells (proliferation signature), reactive stromal andimmune cells in the LN (LN signature), and MHC classII. Seventeen genes, including genes from these 4 signa-tures and BMP6 (which is associated with a poor out-come), were used to construct a predictor of OS after che-motherapy. The GCB-like subgroup had the highest 5-yearsurvival rate (60%), compared with 35% for the ABCgroup and 39% for the type 3 DLBCL group. This gene-based predictor and the IPI were independent prognosticindicators. Two common oncogenic events in DLBCL (bcl-2 translocation and CREL amplification) were detectedonly in the GCB-like subgroup; the ABC subgroup hadthe highest level of expression of the proliferation signa-ture and BMP6 and had the lowest level of expression ofthe LN signature. Wright et al54 further described that theABC subgroup expressed a subset of genes that are char-acteristic of plasma cells, particularly those encoding en-

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 493
Figure 3. A, Subgroups of diffuse large B-cell lymphoma (DLBCL) according to geneexpression profiling. Hierarchic clustering,according to the level of expression of 100genes, is shown of DLBCLs from 240 patientswith untreated disease and from 34 patientswho had previously been treated or who hada preexisting low-grade lymphoma. Red in-dicates increased expression; and green, de-creased expression. Each column representsa single DLBCL, and each row represents asingle gene. Genes that are characteristicallyexpressed in germinal center B-cell–likeDLBCL or activated B-cell–like DLBCL are in-dicated. The dendrogram at the top shows thedegree to which each diffuse large B-cell lym-phoma is related to the others with respect togene expression. B, The number of sampleswith amplification of the CREL locus and bcl-2 translocations in subgroups of DLBCL. Theratio of genomic copy number for the CRELand b2-microglobulin loci was determinedusing a quantitative polymerase chain reac-tion (PCR) assay, and ratios greater than 2were considered to indicate CREL amplifica-tion. The bcl-2 translocations were detectedwith the use of a PCR assay for the mainbreakpoint cluster region that is frequently in-volved in the t(14;18) translocation. Data arefrom patients who had untreated DLBCL,without preexisting cancer. C, Kaplan-Meierestimates of overall survival after chemother-apy among the 240 previously untreated pa-tients, according to the gene expression sub-group. Data are from Rosenwald et al53 andare reprinted with permission. Copyright2002, Massachusetts Medical Society, Bos-ton.
doplasmic reticulum, and golgi proteins that are involvedin secretion; they also confirmed that the GC and ABCsubgroups had significantly different 5-year survival ratesafter multiagent chemotherapy (62% vs 26%; P 5 .005).
Wang et al55 used the first self-organizing map withsubsequent HC and K-means clustering and identified 4prominent GEP patterns in DBLCL, distinguished by geneclusters 10, 11, and 1 and the large group of clusters 7 and9. Cluster 10 contained genes that are expressed in GCBcells (FAK, WIP, CD10, CD27, CD38, FMR2, bcl-6, and bcl-7A). Cluster 11 contained genes that are expressed by Tcells (CD3, CD2, and TCR), natural killer (NK) cells (NK4),macrophages (CD14, CD63, CD64, and CD115), LN den-dritic cells (S100), and genes coding for chemokines andchemokine receptors (RANTES, BLC, IP10, SLC, FPR,STRL331, and MIP1), which play a role in the chemoat-traction of inflammatory cells. Diffuse large B-cell lym-phoma variably expressed genes in the adjacent clusters1, 7, and 9. Cluster 1 included genes that are associatedwith proliferation (KI67, cyclin A, BUB1, cyclin B1, andthymidine kinase), whereas clusters 7 and 9 includedgenes that are associated with cell survival (bcl-XL, de-fender against cell death 1 [BFL1], BAK, BAG1, and MCL1)and with plasma cell differentiation (XBP1, STAT3 , IRF4,and ribosomal proteins). Similar to the previous results ofRosenwald et al,53 Wang et al confirmed the better survivalfor patients expressing GC-related genes (gene cluster 10).In addition, they showed a significantly improved survivalof patients expressing inflammation-related genes (gene
cluster 11) and a significantly reduced survival of patientsexpressing genes related to cell proliferation, antiapopto-sis, and plasma cell differentiation (clusters 1, 7, and 9).
In contrast to results of the study by Alizadeh et al,35
Shipp et al56 subsequently reported successful outcomeprediction in a series of 58 patients with DLBCL using GEdata from oligonucleotide MAs with supervised learningmethods, and they identified molecular correlates of out-come that were independent of the ‘‘cell of origin’’ dis-tinction that was previously described by Alizadeh et alsuggesting that additional factors may be important in de-termining the therapeutic response of DLBCL. Genes thatwere implicated in DLBCL outcome included genes thatregulate responses to BCR signaling (PKCB), critical ser-ine/threonine phosphorylation pathways (PDE4B), andapoptosis (NOR1).56 All 3 of these outcome genes regulateapoptotic responses to antigen receptor engagement and,potentially, cytotoxic chemotherapy. PKCB was overex-pressed in fatal/refractory DLBCL. The consequences ofBCR signaling were dependent on associated activation ofPKCB. In the presence of an intact PKCB pathway, BCRengagement resulted in B-cell proliferation. These findingssuggest that PKCB activity enhances B-cell proliferationand survival. The cyclic adenosine monophosphate–spe-cific phosphodiesterase (PDE4B) was also overexpressedin fatal/refractory DLBCL and may be an attractive ther-apeutic target. The mitogen-inducible nuclear orphan re-ceptor, or NOR1, was overexpressed in patients with cured

494 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
DLBCL. It is possible that NOR1 increases the apoptoticresponse to chemotherapy in curable DLBCL.
Oligonucleotide MAs were used to analyze the expres-sion of 6817 genes in pretreatment DLBCL biopsies from77 patients who were subsequently treated with cyclo-phosphamide, adriamycin, vincristine sulfate, and pred-nisone, and a supervised learning prediction method wasapplied to identify cured versus fatal/refractory disease.56
The genes were sorted by their degree of correlation withthe DLBCL versus FL distinction. Genes that were ex-pressed at higher levels in DLBCLs than in FLs includedknown DLBCL markers (lactate dehydrogenase and trans-ferring receptor), as well as genes that are associated withcellular proliferation (cyclin B1 and a CDC47 homologue)and with invasion and metastasis (cathepsins B and D).Diffuse large B-cell lymphomas also overexpressed thefollowing: (1) the high-mobility group protein isoforms Iand Y (HMGIY), known to be a Myc target and encodedby a potential oncogene; (2) the hematopoietic cell kinase(HCK), which has been linked with CD44 signaling; and(3) the inhibitors of apoptosis, such as the carbohydrate-binding protein galectin 3 and the Bcl-2–related proteinBFL1A1 (also known as Bcl-2A1). BFL1A1 overexpressionin DLBCL is of particular interest because this antiapop-totic molecule is induced by CD40 signaling and is re-quired for CD40-mediated B-cell survival. It is also a di-rect transcription target of NF-kB, which suppresses che-motherapeutic-associated and TNF-associated apoptosis.Therefore, BFL1A1 overexpression may represent an im-portant antiapoptotic mechanism for reducing the che-mosensitivity of DLBCLs.
Genes that were overexpressed in FLs compared withDLBCLs included additional regulators of apoptosis suchas human programmed death 1 (HPD1) and WSLLR (alsoknown as TNFRSF12).56 Follicular lymphomas also hadmore abundant expression of genes encoding cytoskeletalcomponents (ankyrin 2) and adhesion molecules (a4 inte-grin) and of genes expressed by follicular dendritic cells(clusterin), infiltrating cells (TCRB, CD3E, CD3D, CD40 li-gand, TXK, T-cell activation antigens, CD69, and V7), andthe T-cell chemoattractant SLC (also known as SCYA21).
To predict whether GEP that is associated with DLBCLand FL was sufficiently robust to predict the lymphomatype of an unknown sample, Shipp et al56 used the weight-ed voting algorithm, which calculates the weighted com-bination of informative marker genes to make a class dis-tinction (DLBLC vs FL). The algorithm classified 2 cate-gories of patients within specific IPI risk categories whowere likely to be cured or to die of their disease. A 30-gene predictor correctly distinguished 71 (92%) of 77 tu-mors with respect to DLBCL versus FL (P , .001 com-pared with random prediction).
The success in distinguishing DLBCL from FL prompt-ed a similar supervised learning classification approach todelineate clinically relevant DLBCL subsets.56 The genesthat most highly correlated with the cured versus fatal/refractory distinction included those previously associatedwith DLBCL outcome, such as VEGF, which is linked withan adverse outcome and is overexpressed in fatal/refrac-tory DLBCL, and E2F, which is associated with a favorableoutcome and is overexpressed in patients with curedDLBCLs. Predictors containing 8 to 16 genes yielded sta-tistically significant outcome predictions, with the highestaccuracy obtained using 13 genes.56 The predictor classi-fied 58 patients who had a 5-year OS of 54% into 2 groups,
those predicted to be cured (5-year OS of 70%) and thosepredicted to have fatal/refractory disease (5-year OS of12%) (P , .001). The study also investigated whether theGE-based outcome predictor contained additional infor-mation that was not captured by the IPI. Low- and low/intermediate–risk patients with the ‘‘cured’’ GE signaturehad significantly higher OS rates than low- and low/in-termediate–risk patients with the fatal/refractory signa-ture (5-year OS, 75% vs 32%; P 5 .02). Similarly, the out-come of high-risk patients could be further predicted bythe application of the GE model (5-year OS, 57% vs 0%;P 5 .02). These results indicated that the MA-based out-come predictor provided additional information that wasnot reflected in the clinical prognostic model and sug-gested a possible strategy for further individualization ofpatient treatment. However, the GE-based predictor didnot entirely eliminate outcome differences between low-and low/intermediate–risk patients and high-risk pa-tients, suggesting that the clinical and molecular modelscontain at least partially independent information.
Shipp et al56 then investigated whether there was a con-nection between this supervised model and the cell-of-or-igin classification by Alizadeh et al.35 Using 90 genes ofthe HU 6800 array (a subset of the cell-of-origin signaturegenes), the successful distinction between GCB-likeDLBCL and ABC DLBCL was confirmed in the 58 ana-lyzed patients; however, the distinction was not signifi-cantly correlated with patient outcome in this series.56
Therefore, although the signature genes reflected the cellof origin, they did not explain a significant portion of theclinical variability seen in this DLBCL data set.
Next, Shipp et al56 investigated whether the 13 genesused in their outcome predictor were of use in the dataset in the study by Alizadeh et al35 and identified 3 of the13 genes that were represented on the lymphochip (NOR1,PDE4B, and PKCB). When analyzed as single markers inthat data set, NOR1 (P 5 .05) and PDE4B (P 5 .07) cor-related with outcome.56 In addition, 2 clones that are spe-cific for the PKCB isoform correlated with outcome in thisdata set (P 5 .04). Therefore, these results from an inde-pendent data set supported the previous results and high-lighted the value of publicly accessible GE databases forrapid computational validation of hypotheses.
The potential extension of MA-based outcome predic-tion was further explored using IHC.56 A tissue array ofthe study DLBCLs was analyzed by IHC for PKCB. Itsprotein expression was highly correlated with MA-deter-mined transcript abundance in the DLBCLs and was as-sociated with a worse clinical outcome (P 5 .03).
As seen in the studies by Rosenwald, Wang, Glas, andDave and their colleagues,37,38,53,55 the presence of a prom-inent T-cell and follicular dendritic cell signature in theFLs demonstrated that MA GEP can be used to captureadditional nonmalignant components of the tumor micro-environment.56 This study also highlighted the importantdifference between the unsupervised (clustering) and thesupervised machine learning analytic approaches.56
Lossos et al57 subsequently applied significance analysisof MAs (a supervised method for the identification ofgenes with a statistically significant association with sur-vival) to the data set in the study by Alizadeh et al35 toidentify genes that may have been missed in the unsu-pervised analyses. The expression of 36 genes whose ex-pression had been reported to predict survival in DLBCLwas measured in 66 independent lymphoma samples by

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 495
Table 3. Immunohistochemical (IHC) Markers Associated With Prediction of Outcome in Diffuse Large B-CellLymphoma (DLBCL) Based on Gene Expression Profiling Data*
Expression Pattern of DLBCL IHC Markers Expressed Association With Prognosis
A. GCB pattern CD101 or Bcl-61 Best OSB. Activated GCB pattern At least 1 GCB marker (CD10, Bcl-6) and 1 activation marker
(MUM1, CD138)Worse OS than pattern A
C. Activated non-GCB pattern MUM1 or CD138 Worse OS than pattern A
* Data are from Chang et al.60 GCB indicates germinal center B cell; OS, overall survival.
quantitative RT-PCR analyses, and the results were relatedto OS.57 Then, in a univariate analysis, genes were rankedon the basis of their ability to predict survival, and a mul-tivariate model was developed (validated in 2 independentMA data sets) based on the expression of the 6 ‘‘strongestpredictor’’ genes (LMO2, bcl-6, FN1, CCND2, SCYA3, andbcl-2). These genes occur in the GCB-like signature (LMO2and bcl-6), the ABC signature (bcl-2, CCND2, and SCYA3),and the LN signature (FN1). bcl-6 Is known to down-reg-ulate the expression of CCND2 and SCYA3. The expres-sion of LMO2, bcl-6, and FN1 correlated with prolongedsurvival. The expression of bcl-2, CCND2, and SCYA3 cor-related with shorter survival. None of these genes aloneindependently predicted OS at a statistically significantlevel. The model was independent of the IPI and added toits predictive power. However, serum lactate dehydroge-nase was the only independent predictor of OS (P 5 .004),and it was not included in the model. This study conclud-ed that measurement of the expression of these 6 genes issufficient to predict OS in DLBCL.
Correlation of IHC Analyses With GEP Data in DLBCLA study analyzing the expression and prognostic sig-
nificance of CD44s (CD44v4, CD44v6, and CD44v9) inDLBCLs, including 22 GCB-like (bcl-6 positive, CD10 pos-itive, and bcl-2 negative), 25 ABC (bcl-6 negative, CD10negative, and bcl-2 positive), and 35 unclassifiableDLBCLs, found that CD44v6 was coexpressed with bcl-2,was predominantly associated with bcl-6–negative cases,and correlated with higher disease stage.58 CD44v6-nega-tive patients had an OS of 82% at 70 months, and CD44v6-positive patients had an OS of 58% at 70 months. Theexpression of CD44v6 correlated with higher disease stageand may contribute to lymphoma dissemination. CD44v6was expressed predominantly in ABC DLBCL and inCD44-negative cases. CD44v6 expression was associatedwith worse OS.
Linderoth et al59 analyzed the application of IHC mark-ers (Bcl-6, CD10, Bcl-2, bax, CD138, CD40, and CD23) to125 DLBCL samples to delineate histogenetic origin andprognosis, as in GEP. Bcl-6, CD10, and CD40 were consid-ered markers of GC phenotype, CD23 of pre/early-GC or-igin, and CD138 of post-GC origin. Bcl-2 and bax wereconsidered apoptotic regulators. There was no prognosticsignificance of CD10, Bcl-6, or CD138 IHC results. CD40was expressed in 76% of cases and was associated withsuperior time to treatment failure (failure-free survival) (P5 .03) and OS (P 5 .007), independent of IPI. CD23 wasexpressed in 16% of patients (all CD5 negative and CD40positive) and was associated with a strong tendency forbetter OS (P 5 .03). CD40 expression correlated with baxexpression but not with Bcl-2 expression.
However, an additional IHC study evaluated whetherusing a panel of GCB cell markers (CD10 and Bcl-6) andactivation makers (MUM1/IRF4 and CD138) defined the
prognosis in 42 patients with de novo DLBCL.60 Patientswere classified based on the following 3 expression pat-terns: (1) a GCB cell pattern expressing CD10 or Bcl-6 butnot expressing activation markers, (2) an activated GCBcell pattern expressing at least 1 of the GCB cell markersand at least 1 of the activation markers, and (3) an acti-vated non–GCB cell pattern expressing MUM1/IRF4 orCD138 but not expressing GCB cell markers. Patients withpattern 1 had much better OS than those with the other 2patterns (P , .008). The IPI scores and the expression pat-terns of these markers were independent prognostic mark-ers; thus, these IHC markers may be practically applied(Table 3).
Correlation of GEP Data and IHC Patterns WithCytogenetic Abnormalities in DLBCL
In a correlation study of GEP of de novo primaryDLBCL demonstrating cytogenetic abnormalities, partic-ularly the occurrence of t(14;18)(q32;q21) in the GCB-likeand ABC subgroups of DLBCL, t(14;18) was detected in7 (20%) of 35 cases, all with GCB-like GEP, representing35% of the cases in the GCB-like DLBCL subgroup.51 Sixof these 7 cases had similar GEP. The expression of Bcl-2(75% in the GCB-like DLBCL subgroup vs 67% in the ABCDLBCL subgroup) and Bcl-6 proteins was not significantlydifferent between t(14;18)-positive and t(14;18)-negativecases. However, CD10 was detected only in the GCB-likeGEP group (in 55%), and CD10 was most frequently ex-pressed in t(14;18)-positive cases. This study supports thevalidity of subdividing DLBCL into 2 major subgroups byGEP, with t(14;18) being an important event in the path-ogenesis of a subset of GCB-like DLBCL. This study alsosupports the use of CD10 protein expression in identify-ing cases of GCB-like DLBCL, as well as the frequent ex-pression of CD10 protein in cases with t(14;18).
Similarly, in a study evaluating t(14;18) using FISH in141 cases of DLBCL in which GEP had been previouslyperformed, this translocation was detected in 17% ofDLBCLs and in 34% of the GCB-like DLBCLs, which con-tained most of the positive cases.61 Twelve t(14;18)-posi-tive cases that were detected using PCR on additionalsamples were added to the FISH-positive cases. In con-trast to the findings of the previous study,51 IHC in thisstudy indicated that Bcl-2, Bcl-6, and CD10 proteins werepreferentially expressed in t(14;18)-positive cases com-pared with t(14;18)-negative cases.61 Within the GCB-likesubgroup, the expression of Bcl-2 and CD10, but not Bcl-6, differed significantly between cases with and withoutt(14;18) (88% vs 24% for Bcl-2 and 72% vs 32% for CD10,respectively). In the GCB-like subgroup, a heterogeneousgroup of genes was overexpressed in the t(14;18)-positivesubset, among which Bcl-2 was a significant discriminator.The t(14;18)-negative subset within the GCB-like sub-group was dominated by overexpression of cell cycle–as-sociated genes, indicating that these tumors are signifi-

496 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
cantly more proliferative and suggesting distinctive path-ogenetic mechanisms. However, despite this higher prolif-erative activity, there was no significant difference inpatient survival (OS or failure-free survival) between thet(14;18)-positive and the t(14;18)-negative subsets withinthe GCB-like subgroup.
Future DirectionsSeveral known downstream targets of the NF-kB tran-
scription factors are highly expressed in many cases ofABC DLBCL but not in GCB-like DLBCL.62 The NF-kBfamily is a group of homodimeric and heterodimeric tran-scription factors that play critical roles in the development,lymphocyte activation, and prevention of apoptosis.63 Nu-clear factor kB transcription factors are latent in the cy-toplasm of cells in a complex with a member of the inhib-itory kB family of proteins. These findings establish theNF-kB pathway as a new therapeutic target for patientswith DLBCL who are refractory to current therapies.14
TRANSFORMED FL VERSUS EPSTEIN-BARR VIRUS–POSITIVE AND EPSTEIN-BARR VIRUS–NEGATIVEBURKITT LYMPHOMA VERSUS DE NOVO DLBCL
A comparison of GEP of cell lines from transformed FL,Epstein-Barr virus (EBV)–negative Burkitt lymphoma(BL), EBV-positive BL, and de novo DLBCL, based on theHC levels of 43 genes, highlighted the characteristic ex-pression patterns of transformed FL, EBV-negative BL,and EBV-positive BL.64 Genes that were expressed at high-er levels in transformed FL than in BL included calcium/calmodulin-dependent protein kinase (CAMK1) and mi-togen-activated protein kinase 10 (MAPK10). Epstein-Barr–negative BL was characterized by high-level expres-sion of amyloid b precursor protein (APP), heat shock 27-kDa protein 1 (HSPB1), and mothers against decapenta-plegic homologue (MADH1). Gardner-Rasheed felinesarcoma viral oncogene homologue (FGR) was the mostsignificant gene to delineate EBV-positive BL. A subtypeprediction algorithm using 34 genes correctly classified92% of transformed FL, EBV-negative BL, and EBV-posi-tive BL samples. Compared with NBCs, the expressionpatterns of the selected genes were characteristic of lym-phomas. The study extended the HC analysis to cell linesfrom de novo DLBCL. The de novo DLBCL cell lines sep-arated from the transformed FL, EBV-negative BL, andEBV-positive BL or segregated with the EBV-positive BL,possibly reflecting variable genetic abnormalities. The as-sociations of CAMK1 with transformed FL, of APP andMADH1 with EBV-negative BL, of FGR with EBV-positiveBL, and of bcl-2 with transformed FL and DLBCL wereconfirmed by RT-PCR. This study provided new molecularmarkers whose expressions are closely associated withsmall B-cell lymphoma subtypes.
DIFFERENTIATION OF DE NOVO DLBCL, DE NOVOCD5-POSITIVE DLBCL, AND MCL
An analysis of GEP, using cDNA MA technology, in 9CD5-negative DLBCLs, 11 de novo CD5-positive DLBCLs,and 10 MCLs identified a series of genes distinguishingthese 3 lymphoma types.65 Integrin b1 (also confirmed byIHC) or CD36 adhesion molecules were overexpressed inmost cases of CD5-positive DLBCL. Integrin b1 overex-pression may account for the high extranodal involvementand the poor prognosis of CD5-positive DLBCLs. CD36was overexpressed on vascular endothelia in CD5-positive
DLBCLs, although there was no difference in the vascu-larity as detected by von Willebrand factor antibody be-tween CD5-positive and CD5-negative DLBCLs. These re-sults suggest that CD5-positive and CD5-negativeDLBCLs have different GE signatures in tumor cells andin their vascular systems.
AIDS-RELATED DLBCL
Patrone et al66 analyzed 18 candidate genes and founddistinct patterns of expression in AIDS-related DLBCLand DLBCL samples. However, none of these genes werepreferentially associated with AIDS-related DLBCL orwith DLBCL. The study data suggest that the increasedincidence and severity of AIDS-related DLBCL comparedwith DLBCL are likely due to crippled immune surveil-lance rather than markedly different GEP.
PRIMARY EFFUSION LYMPHOMA
Jenner et al67 showed that GEP of primary effusion lym-phoma (PEL) closely resembles that of malignant plasmacells, including the low expression of mature B-cell genes.Primary effusion lymphomas were defined by the over-expression of genes that are involved in inflammation, celladhesion, and invasion, which may be responsible for theirpresentation in body cavities. Similar to malignant plasmacells, all tested PEL samples expressed the vitamin D re-ceptor and were sensitive to the vitamin D analogue drugEB 1089 (seocalcitol).
Kleine et al68 used GEP (of 12 000 genes) to further de-fine the phenotype of AIDS-related PEL and to investigatethe relationship of lymphoma to NBCs and to other tumorsubtypes, including NHL of immunocompetent hosts andAIDS-associated NHL. Their results showed that PEL dis-played common GEP that was distinct from that of allNHLs of immunocompetent hosts and from that of AIDS-NHL subtypes. In contrast to those NHLs, AIDS-relatedPEL was not related to GC or memory B cells. Similar tothe findings in the previous study,67 GEP of PEL was de-fined in this study as being plasmablastic, showing fea-tures of immunoblasts (CD30, CD39, and MUM1/IRF4identified by EBV-transformed lymphoblastoid cell linesand AIDS immunoblastic lymphoma) and plasma cells(BLIMP1 and CD138 defined by MM cell lines).68 AIDS-related PEL was negative for the memory B-cell markerCD27 and for the B-cell transcription factor PAX5. Thisstudy also identified a set of genes (specifically expressedin PEL tumor cells) that were validated at the protein level,suggesting their potential pathogenetic and clinical sig-nificance. For example, the cell surface expression of theIL-2Rb chain may suggest that PEL tumor cells are sus-ceptible to IL-2 or to IL-15 or that such cytokines may benecessary for their survival.
Future studies of PEL may be directed at several mol-ecules that are expressed on the membranes of PEL tumorcells that could be targets for therapeutic intervention.First, cross-linking of the adhesion molecule PSGL-1 hasbeen noted to inhibit proliferation of hematopoietic stemcells, implying a potential functional role for this surfacereceptor that is also in the control of cell proliferation.68
Second, as suggested for other vitamin D3 receptor–posi-tive B-cell malignancies, activation through the vitamin D3
receptor exposed on PEL cells might induce differentiationof the tumor cells and potentially contribute to therapeuticoptions.68 Third, PEL cells express mucin-1, a tumor-as-

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 497
sociated antigen that might represent a suitable target forantibody-mediated therapy.68
CUTANEOUS LARGE B-CELL LYMPHOMAHoefnagel et al69 investigated GEP of 21 primary cuta-
neous large B-cell lymphomas (PCLBCLs) by oligonucle-otide MA analysis to establish a molecular basis for theirsubdivision into primary cutaneous follicle center celllymphoma and PCLBCL of the leg. Hierarchic clustering,based on a B-cell signature of 7450 genes, classifiedPCLBCL into 2 distinct groups consisting of 8 primarycutaneous follicle center cell lymphomas and 13 PCLBCLsof the leg. Primary cutaneous large B-cell lymphomas ofthe leg showed increased expression of the genes that areassociated with cell proliferation (the proto-oncogenesPIM1, PIM2, and CMYC) and of the transcription factorsMUM1/IRF4 and Oct-2. Pim kinases are known to co-operate with CMYC and with NMYC to generate T-cell andB-cell lymphomas. In the group of primary cutaneous fol-licle center cell lymphomas, high expression of SPINK2was observed. The SPINK2 gene encodes a Kazal-type ofserine threonine kinase with ill-defined functions in phys-iologic and pathologic cellular processes. Further analysissuggested that primary cutaneous follicle center cell lym-phoma and PCLBCL of the leg have expression profilesthat are similar to GEP of GCB-like DLBCL and to GEPof ABC DLBCL, respectively. These results suggest thatdifferent pathogenetic mechanisms are involved in the de-velopment of these lymphomas, and their GEP may pre-dict prognosis, as in the distinction of their noncutaneousDLBCL counterparts.
PRIMARY MEDIASTINAL LARGE B-CELL LYMPHOMAPrimary mediastinal large B-cell lymphoma (PMBL)
demonstrates GEP that bears similarity to that of HL-de-rived cell lines. In a study by Rosenwald et al,70 more thanone third of the genes that were more highly expressed inPMBL than in other DLBCLs were also characteristicallyexpressed in HL cells (Figure 4). In this study, PDL2,which encodes a regulator of T-cell activation, was thegene that best discriminated PMBL from other DLBCLsand was highly expressed in HL cells. Savage et al71 re-ported that PMBLs had low levels of expression of mul-tiple components of the BCR signaling cascade, a profileresembling that of classic HL (cHL) cells. Like cHL, PMBLhad high levels of expression of IL-13 receptor and down-stream effectors of IL-13 signaling (Janus kinase 2 andsignal transducer and the activator of transcription STAT1 ,also confirmed by IHC), TNF family members, and TNFreceptor–associated factor 1 (TRAF1), also confirmed byIHC. In addition, in almost all PMBLs, c-Rel was localizedto the nucleus, which is consistent with activation of theNF-KB pathway. These studies identified a molecular linkbetween PMBL and cHL and a shared survival pathway.The characteristics of low levels of expression of BCR sig-naling pathway components, a distinctive cytokine path-way signature, and activation of NF-KB are similar tothose of cHL. Patients with PMBL had a better 5-year sur-vival rate (64%) than all patients with DLBCL after ther-apy (46%).70
CLASSIC HODGKIN DISEASECell of Origin and Pathogenesis
Cossman72 described single-cell micromanipulation ofliving Reed-Sternberg (R-S) cells to determine their ge-
nome-wide GEP. Further analysis with HD GE MAs dem-onstrated the expression of approximately 12 000 genes byR-S cells with GEP of an ‘‘aberrant germinal center B-lym-phocyte that resists apoptosis through CD40 signalingand NFkB activation.’’ 72(p799)
A later study by Garcia et al73 analyzed the expressionof 29 genes regulating the cell cycle and apoptosis in 288cHL biopsies, by means of IHC and in situ hybridizationusing tissue MA, and reported multiple alterations in dif-ferent pathways and checkpoints, including G1/S andG2/M transitions and apoptosis. A multiparametric anal-ysis identified overexpression of proteins that are associ-ated with increased growth fraction (Hdm2, p53, p21, RB,cyclin A, cyclin B1, cyclin D3, cyclin E, CDK2, CDK6,SKP2, Bcl-XL, survivin, STAT1, and STAT3) and of pro-teins associated with apoptosis (NF-kB, STAT1, Bcl-2, andRB). The analysis also demonstrated that EBV-positive cas-es displayed a characteristic profile, confirming the path-ogenic role of EBV in cHL. Schwering et al74 comparedGEP generated by serial analysis of GE and DNA chipMAs of HL cell lines with that of NBC subsets and founddecreased mRNA levels for nearly all established B-line-age–specific genes, with histochemical confirmation of alack of protein expression for 9 of these genes. Down-reg-ulation of genes affected multiple components of signalingpathways that are active in B cells, including BCR signal-ing. Because several genes that are down-regulated in R-S cells are positively regulated by the transcription factorPAX5, which is expressed in most R-S cells, HL cell lineswere studied for mutations in the PAX5 gene; however, nomutations were found. The lost B-lineage identity in R-Scells is a possible explanation for their survival withoutBCR expression.
Using MAs, Kuppers et al75 compared GEP of 4 HL celllines with profiles of the main B-cell subsets and B-NHLs.The HL lines clustered as a distinct entity, and their GEwas most similar to that of EBV-transformed B cells andcells derived from DLBCLs showing features of in vitro–activated B cells. Twenty-seven genes (previously notknown to be expressed in R-S cells) were aberrantly ex-pressed (the transcription factors GATA-3, ABF1, EAR3,and Nrf3). These newly identified HL-specific genes mayplay important roles in the pathogenesis of HL, representnovel diagnostic markers, and be considered for therapeu-tic targeting.
Clinical Outcome
Devilard et al76 further used cDNA arrays to study pu-rified cells from 21 cases of cHL and, using HC, identified3 main molecular groups of cHLs that are relevant to thehistologic features and to clinical outcome (response totreatment and survival). Samples from all ‘‘bad outcome’’cHLs clustered in 1 group, whereas the other 2 groupscontained most ‘‘good outcome’’ cHLs. As might be ex-pected, the nodular sclerosing good outcome cHLs over-expressed genes that are involved in apoptotic inductionand cell signaling, including cytokines, while the bad out-come cHL samples were characterized by the up-regula-tion of genes that are involved in fibroblast activation, an-giogenesis, extracellular matrix remodeling, cell prolifer-ation, and down-regulation of tumor suppressor genes.Garcia et al73 later determined that shorter OS was signif-icantly related to multiple factors, including overexpres-sion of Bcl-2, p53, bax, Bcl-XL, MIB1, and apoptotic index.

498 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
Figure 4. Relationship of primary mediastinal large B-cell lymphoma (PMBL) to Hodgkin lymphoma (HL). Relative gene expression is shown inprimary PMBLs (mean of all biopsy samples), the PMBL cell line K1106, 3 HL cell lines, and 6 germinal center B (GCB) diffuse large B-celllymphoma (DLBCL) cell lines. A, Primary mediastinal large B-cell lymphoma signature genes that are also expressed at high levels in HL cell linescompared with GCB DLBCL cell lines. B, Primary mediastinal large B-cell lymphoma signature genes that are not expressed in HL cell lines. C,Mature B-cell markers that are expressed in PMBL and in GCB DLBCL but not in HL. D, Enrichment within the set of PMBL signature genes ofgenes that are highly expressed in HL cell lines or in the K1106 PMBL cell line relative to GCB DLBCL cell lines. Data are from Rosenwald etal53 and are reprinted with permission from The Rockefeller University Press, New York, NY.
Figure 5. Distinct leukemia subtypes can be defined based on their expression profiles. Expression profiles were obtained on leukemic blastsfrom 132 diagnostic bone marrow aspirates, and the data were analyzed using (A) an unsupervised 2-dimensional clustering algorithm and (B-D)principal component analysis (PCA). The cases in the training and test sets were combined, and the analysis was performed with 26 825 genes

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 499
Table 4. Immunohistochemical (IHC) Markers Useful in Differentiation of Classic Hodgkin Lymphoma (cHL), NodularLymphocyte-Predominant Hodgkin Lymphoma (NLPHL), and Diffuse Large B-Cell Lymphoma (DLBCL) Based on
Gene Expression Profiling Data*
Lymphoma Subtype IHC Pattern
cHL BSAP1 and OCT-22/BOB.12 was predictive of cHL (75% of cases)BSAP2/OCT-22/BOB.12 was seen only in cHLBSAP1/OCT-21/BOB.11 was seen in only 18% of cHLOCT-2 and BOB.1 staining was weak to moderate and focal in Reed-Sternberg cellsNo cHL cases expressed all 3 pan B-cell markers (CD20, CD22, and CD79a)
NLPHL and DLBCL BSAP1/OCT-21/BOB.11 was predictive of NLPHL and DLBCLOCT-2 and BOB.1 staining was uniform and strong in NLPHL and in 96% of DLBCL casesAll NLPHL cases and 91% of DLBCL cases expressed all 3 pan B-cell markers (CD20, CD22, and CD79a)
* Data are from Browne et al.78
←
from the Affymetrix U133A and B microarrays that varied in their expression across this data set. A, A 2-dimensional hierarchic clustering wasperformed by means of the Pearson product moment correlation coefficient and the unweighted pair group method using arithmetic means. B,Multidimensional scaling plot of all cases using PCA. C, Multidimensional scaling plot of 118 B-lineage acute lymphoblastic leukemia cases. D,The identical multidimensional scaling plot as shown in C, except that the plot was rotated 908. Each case is represented by a sphere and is colorcoded to indicate the genetic subgroup to which it belongs. Orange indicates BCR-ABL; aqua, E2A-PBX1; yellow, hyperdiploid with more than50 chromosomes; purple, MLL; red, TALL; green, TEL-AML1; blue, novel cases; and gray, unclassified cases. Data are from Ross et al101 and arereprinted with permission.
DIFFERENTIATION OF cHL FROM LYMPHOCYTE-PREDOMINANT HL AND FROM DLBCL
Marafioti et al77 investigated the expression of 5 intra-cellular signaling molecules in B cells in HL (45 cases and3 cell lines) and found that the Src family kinase Syk, theB-cell adaptor protein BLNK, and phospholipase C g 2were consistently absent from R-S cells, whereas 2 otherSrc kinases (Lyn and Fyn) were heterogeneously ex-pressed in some cases (in 12% and 42%, respectively). Incontrast, the tumor cells in all cases of lymphocyte-pre-dominant HL (LPHL) were positive for Syk, BLNK, phos-pholipase C g 2, and Fyn; Lyn was positive in a smallnumber of biopsy specimens. These results indicate thatin R-S cells the defect in B-cell–lineage marker expressionincludes a spectrum of molecules that are involved in in-tracellular signaling, as previously described, and the dif-ference in the expression of these signaling proteins be-tween the 2 major subtypes of HL may be of diagnosticvalue.
A study by Browne et al78 evaluated the expression ofB-cell–specific activator protein, octamer-binding tran-scription factor 2 (Oct-2), and B-cell Oct-binding protein1 (BOB.1) in 57 cases of cHL, 5 cases of nodular LPHL, 25cases of DLBCL (including T-cell–rich large B-cell lym-phoma), and 8 cases of T/‘‘null-cell’’ anaplastic large celllymphoma (ALCL). B-cell–specific activator protein posi-tivity and Oct-2 or BOB.1 negativity were predictive ofcHL (in 75% of cases). All BSAP-negative cHL cases werealso negative for Oct-2 and BOB.1. B-cell–specific activatorprotein positivity/Oct-2 positivity/BOB.1 positivity waspredictive of nodular LPHL or DLBCL; however, 18% ofcHLs were positive for all 3. The staining of cHL withOct-2 or BOB.1 tended to be weak to moderate and wasoften focal in the R-S cells, whereas these 2 stains werestrongly positive in the nodular LPHL cases and in 96%of the DLBCL cases. None of the cHL cases expressed all3 pan B-cell markers, whereas 91% of the DLBCL casesand all of the nodular LPHL cases had expression of all 3pan B-cell markers (Table 4).
Garcia-Cosio et al79 subsequently described the use of
the tissue microarray technique in performing an IHCstudy of Oct-1, Oct-2, and BOB.1 in 325 cHLs. The resultswere correlated with the expression of B-cell markers(CD20, CD79a, BSAP, and MUM.1), the presence of EBV,and the histologic subtype. The percentages of CD20-pos-itive and CD79a-positive cases were low (18% each),whereas MUM.1 and BSAP were positive in most cases.Among the positive cases with independence of the inten-sity of staining, 62% of them expressed Oct-2, 59% Oct-1,and 37% BOB.1. Among only the strongly positive cases,the results were similar to those of previous studies.77,78
No statistical association was found between the transcrip-tion factor expression, histologic subtype, and presence ofEBV.
T-CELL MALIGNANCIES
Fillmore et al80 used cDNA MA technology to compareGEP of T-cell malignancies (8 cell lines) with that of CD4-positive T cells. Unsupervised HC of 4364 genes demon-strated substantial heterogeneity, resulting in the follow-ing 4 distinct groups: precursor T ALLs (T ALLs), t(2;5)-positive ALCLs, cutaneous T-cell lymphomas (TCLs), andmiscellaneous TCLs. Although no genes were found to beuniformly up-regulated or down-regulated across all celllines, the study identified 111 overexpressed genes (.2-fold) and 1118 down-regulated genes (.2-fold) in the lym-phomas as a group compared with CD4-positive T cells.Many genes involved in cell cycle regulation, intracellularsignaling, cytoskeletal regulation, cellular metabolism,and apoptosis were identified as being commonly dereg-ulated genes. Additional differentially expressed genes in-cluded those involved in proliferation, signaling pathwaygenes, cell adhesion genes, nuclear transcription factors,and known oncogenes and tumor suppressor genes. Real-time polymerase chain reaction analysis demonstrated70% concordance with the MA results.
T-CELL LYMPHOMAS
Martinez-Delgado et al81 used cDNA MAs (containing6386 cancer-related genes) to establish GEP of TCLs (using

500 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
42 tumor samples representing some of the most frequentsubtypes of these lymphomas in Spain) and comparedthem with those of normal T-cells and LNs. Clusteringanalysis of TCLs identified 2 major subgroups, lympho-blastic TCL and peripheral TCL (PTCL); NF-kB is not ac-tivated in lymphoblastic TCL but is hyperactivated inPTCL. A comparison of PTCLs with normal T cells andwith reactive LNs revealed subsets of 17 and 35 signifi-cantly differentially expressed genes, respectively. Someof these genes represented immune response proteins,and some could represent tumor markers characterizingTCL. The study also found that genes that are associatedwith response to treatment were highly correlated withgenes that are associated with patient survival. Genes thatare associated with therapeutic response included theEBV-induced gene EB13, the cytokine receptor CCRL2, thethyroid hormone receptor interactor 4, and insulin-likegrowth factor 1 receptor. Other genes that are associatedwith survival but not with response to treatment or todisease stage included HOXC5, PIG11, and STK15.
Another study further analyzed the following T-cellsubtypes in PTCL using DNA chips of chemokine, its re-ceptor, and cytokines: angioimmunoblastic lymphoma(AILD) (4 cases), ALCL (4 cases), adult T-cell leukemia/lymphoma (ATLL) (7 cases), NK cell lymphoma (NKL) (2cases), and unspecified PTCL (PTCL-U) (6 cases).82 An-gioimmunoblastic lymphoma, ALCL, ATLL, and NKLshowed a tendency for respective clusters, and PTCL-Uclustered with AILD, ALCL, and ATLL. Based on GEP,additional IHC was performing using CCR4, CCR3,CXCR3, BLC, and MIG. Adult T-cell leukemia/lymphoma(48 cases) expressed CCR4, ALCL (26 cases) expressedCCR3, AILD (29 cases) expressed CXCR3 or BLC, andNKL (20 cases) expressed MIG. From the expression pat-terns, 134 cases of PTCL-U were classified into the follow-ing 3 groups: (1) CCR4 positive (42 cases), (2) CCR3 pos-itive (31 cases), and (3) CXCR3 positive/BLC positive andnegative (54 cases); 6 cases were not represented. Theprognosis was poor for ATLL (CCR4 positive), favorablefor ALCL (CCR3 positive), and intermediate for AILD(CXCR3 positive or BLC positive) (P 5 .001). Not unex-pectedly, among the PTCL-U, the CCR4-positive, CCR3-positive, and CXCR3-positive prognoses were equivalentto those of ATLL, AILD, and ALCL, respectively (P ,.001); thus, the expression patterns were able to bettercharacterize these PTCL-U, which would not have beenpossible using other morphologic or immunophenotypicparameters.
CUTANEOUS TCLGene expression profiling using cDNA arrays of PB
mononuclear cells from patients with leukemia with highblood tumor burden of cutaneous TCL, primarily Sezarysyndrome (Sezary cells comprising .60% of the lympho-cytes), revealed 385 genes that were differentially ex-pressed compared with healthy control subjects (P ,.01).83 Using penalized discriminate analysis, 8 genes wereidentified that distinguished Sezary syndrome in patientswith as few as 5% circulating tumor cells. Highly over-expressed genes included the TH2 cell–specific transcrip-tion factors Fata-3 and Jun B, as well as integrin b1, pro-teoglycan 2, the RHOB oncogene, and dual-specificityphosphatase 1. Highly underexpressed genes includedCD26, STAT4 , and the IL-1 receptors.
The loss of expression of STAT4 is required for TH1 T-
cell differentiation, and this loss of expression is one of themost significant characteristics of cutaneous TCLs.83
STAT4 is 1 of 2 genes (the other one being RHOB) thatmay be used in penalized discriminate analysis to classifypatients with high percentages of Sezary cells from con-trols and is 1 of 8 genes that classify patients with lowpercentages of circulating Sezary cells, suggesting that theloss of STAT4 may be an early event in cutaneous TCLdevelopment. In addition, a message for plastin-T, not nor-mally expressed in lymphoid tissue, was detected only inpatient samples, possibly providing a new diagnosticmarker.
In addition, this study identified a class of poor-out-come patients (succumbing within 6 months of samplingregardless of their tumor burden).83 Identification wasbased on the differential expression of 10 genes (IL2RB,TGFBR3, bcl-2, TCN1, and SFTPD, which were overex-pressed in long-term survivors, and P4HB, LY64, HEHU,DAD1, and BATF, which were overexpressed in short-termsurvivors, representing a terminal signature).
ADULT T-CELL LEUKEMIA
An analysis of fresh PB mononuclear cells from patientswith acute and chronic ATLL isolated mRNAs that wereexpressed differentially between the acute and chronictypes of ATL.84 A T-cell differentiation antigen (MAL), alymphoid-specific member of the G protein–coupled re-ceptor family (EBI-1/CCR7), and a novel human homo-logue to a subunit (MNLL) of the bovine ubiquinone ox-idoreductase complex were up-regulated in acute ATL. Ahuman fibrinogen-like protein (hpT49) was down-regu-lated in acute and chronic ATL.
A subsequent comparison of GEP (using HD oligonu-cleotide DNA arrays of .6000 genes) of fresh ATL cellsin 4 pairs of samples (sequential samples of progressionof chronic to acute phase in 3 patients, as well as a typicalchronic-phase sample versus a typical acute-phase sample,all of which were PB, except for an ascitic fluid obtainedduring the acute phase from 1 of the first 3 patients) iden-tified 203 genes that were commonly differentially up-reg-ulated in acute versus chronic samples, including ribo-somal proteins, proteosome subunits, eukaryotic transla-tion factors, immunophilins, heat shock proteins, andgenes that are important for DNA replication.85 Also iden-tified were 91 genes that are commonly differentiallydown-regulated in acute versus chronic samples, includ-ing immune molecules related to MHC and a phosphatase(dual-specific phosphatase 1).
T-CELL LARGE GRANULAR LYMPHOCYTIC LEUKEMIA
An analysis of 2 cell lines (1 from the chronic phase ofCD56-positive T-cell large granular lymphocytic leukemiaand 1 from the aggressive phase of the same clone), usingan MA containing 406 cDNAs, revealed genes that weredifferentially expressed, including 13 genes with in-creased expression and 3 genes with reduced expressionin the aggressive-phase cell line compared with the chron-ic-phase cell line.86 Increased expression of the DEK, RAC,OP18, CD6, CD58, CD106, ID2, ATF4, IRF5, ELL2, and D6genes and reduced expression of the GXMA and GZMKgenes were confirmed by RT-PCR and paralleled the MAdata. These up-regulated genes encode oncoproteins, cellsurface antigens (including molecules related to T-cell pro-liferation), transcription factors, and a chemokine receptor.

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 501
The 2 down-regulated genes encode granzymes that playan important role in induction of cell death.
NK-CELL LYMPHOCYTOSIS/LEUKEMIAA comparison of GEP of more than 12 000 genes of
purified CD3-negative/CD5-positive fractions from 9healthy individuals, 9 patients with chronic NK lympho-cytosis, and 1 patient with aggressive NK cell leukemiaidentified 15 ‘‘lymphoproliferative disease of granularlymphocyte–associated genes.’’ 87 An analysis of thesegenes indicated that the lymphoproliferative disease ofgranular lymphocyte samples shared a molecular signa-ture that was distinct from that of normal NK cells.
ALCL VERSUS cHLAn analysis of GEP (using cDNA arrays covering 1176
cDNA sequences) of 11 lymphoma cell lines (5 ALCL, 4HL, 1 immunoblastic lymphoma, and 1 BL) identified 27genes that were deregulated in all cell lines or in a par-ticular entity, compared with GEP of B cells and T cells.88
For the establishment of GEP, the 27 genes were assignedto the following 4 groups in which genes were deregulat-ed: (1) all lymphoma cell lines (6 up-regulated and 5down-regulated genes compared with stimulated T cellsand B cells), (2) ALCL and HL (5 genes deregulated, 2 ofwhich were B-cell translocation gene 2 [BTG2] and basigin[BSG], overexpressed in 3 ALCL and 2 HL cell lines), (3)HL exclusively (3 genes highly expressed, including cal-modulin 1, and 1 gene significantly down-regulated), and(4) ALCL exclusively (7 genes differentially expressed, in-cluding TIMP-1 protein). The results indicated that ALCLand HL share the differential expression of at least 5genes. In addition, both entities were characterized by thedifferentially deregulated expression of 4 genes in HL andof 7 genes in ALCL.
A subsequent study comparing GEP of 4 ALCL and 3HL cell lines found that bcl-3, which encodes a nuclearprotein belonging to the IkB family of inhibitors of NF-kBtranscription factors, was expressed at higher levels inALCL than in HD.89 Northern and Western blot analysesconfirmed the high-level expression of bcl-3 in ALCL atthe mRNA and protein levels. The study established anRT-PCR assay to measure the bcl-3 mRNA level and founda predominant level of bcl-3 expression in t(2;5)-positiveALCL.
DIFFERENTIATION OF ALL VERSUS AML AND T ALLVERSUS B ALL AND IDENTIFICATION OF
MIXED-LINEAGE LEUKEMIASGolub et al90 analyzed 38 acute leukemia BM samples
(27 ALL and 11 AML). They described a class discoveryprocedure that categorizes samples as being AML or ALLand to categorize ALL samples as being T ALL or B ALL,without previous knowledge of the classes, based on classpredictors.
A total of 6817 genes were sorted by their degrees ofcorrelation.90 Neighborhood analysis (to see whether thereis an unusually HD of genes that is similar to this ideal-ized pattern, compared with equivalent random patterns)showed that about 1100 genes were more highly correlatedwith the AML-ALL class distinction than would be ex-pected by chance. A 50-gene molecular predictor (thosethat were most closely correlated with AML-ALL distinc-tion in the known samples), constructed to assess its ac-curacy in an independent set of 34 leukemia samples (24
BM samples and 10 PB samples), showed that the predic-tor made strong predictions for 29 of 34 samples and thatthe accuracy was 100%. Finer subclasses of the acute leu-kemias were then defined by a self-organizing map thatdivided the acute leukemias into 4 clusters (B1, B2, B3,and B4), largely corresponding to AML, T ALL, B ALL,and B ALL, respectively. The 4 classes could be distin-guished from one another, except for B3 and B4, confirm-ing the distinction corresponding to AML, B ALL, and TALL and suggesting a merging of classes B3 and B4, com-posed primarily of B ALL.
The list of informative genes that was used in the AMLversus ALL predictor was highly instructive.90 Somegenes, including CD11C, CD33, and MB1, encode cell sur-face proteins for which monoclonal antibodies have beendemonstrated to be useful in distinguishing lymphoid-lin-eage from myeloid-lineage cells, and other genes providednew markers of acute leukemia subtypes. For example, theleptin receptor, originally identified through its role inweight regulation, showed high relative expression inAML. Similarly, the zyxin gene has been shown to encodea LIM domain protein that is important in cell adhesionin fibroblasts, but a role in hematopoiesis has not beenreported. In addition, many of the genes were found toencode proteins that are critical for S-phase cell cycle pro-gression (cyclin D3, OP18, and MCM3), chromatin remod-eling (RBAP48 and SNF2), transcription (TFIIEB), and celladhesion (zyxin and CD11C) or were known oncogenes(CMYB, E2A, and HOXA9). Furthermore, one of the infor-mative genes encodes topoisomerase II, the principal tar-get of the antileukemic drug etoposide. Therefore, thesedata suggest that genes may also provide insight into can-cer pathogenesis and pharmacology. Moos et al91 furtherconfirmed the findings of Golub et al90 by discriminatingAML from ALL, as well as B-lineage from T-lineage ALL,in 51 pediatric leukemias using cDNA arrays representing4608 genes. Genes that were predictive of leukemia enti-ties were validated by RT-PCR in some cases.91 Similarly,Kees et al92 defined GEP of a panel of 13 pediatric ALLcell lines (6 T ALL, 3 pre–B ALL, and 4 infant B ALL 2)by the use of cDNA MAs and compared the data with theresults of immunophenotypic and cytogenetic analyses. TALLs and B ALLs were distinguished by 50 genes thatwere defined by HC.
FLT3 is the most differentially expressed gene that dis-tinguishes MLL from AML and ALL.93–95 Armstrong et al96
examined the distinctions between ALL, AML, and MLLby analyzing MAs (based on 12 200 genes) of 20 ALLs,20 AMLs, and 17 MLLs. An unsupervised analysis suc-cessfully segregated all 3 groups, and subsequent leave-one-out cross-validation resulted in a high accuracy (95%)of classification. A 100-gene predictor best correlated withthe 3-class distinction and had 90% accuracy in classifying10 test samples. The ALLs with MLL translocation hadcharacteristic highly distinct GEP that is consistent withan early hematopoietic progenitor (CD79B, CD19, CD44,SPN, PROML1, LMO2, and FLT3), expressing select mul-tilineage markers (including myeloid-specific genes) andindividual HOX genes (HOXA9 and HOXA5). (Gene ex-pression profiling and clinical implications of MLL will beevaluated in more detail in the discussion of MLL.)
Foa et al97 confirmed and extended the findings thatwere previously reported by Armstrong et al96 and by Ro-zovskaia et al98 by determining GEP of adult ALLs usingoligonucleotide MAs targeting 12 600 gene sequences. Hi-

502 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
Table 5. Class Assignment of Pediatric Precursor B Acute Lymphoblastic Leukemia (ALL) Based onGene Expression Profiling (GEP) (97% Accuracy)*
7 Classes Correlation With Known Markers Correlation With Prognosis
1. Rearrangement of MLL gene Lower undetectable expression of CD10 Unfavorable2. E2A-PBX [t(1;19)] Intermediate expression of CD10 Unfavorable3. Hyperdiploid (.50 chromosomes)† Favorable4. BCR-ABL [t(9;22)] Unfavorable5. TEL-AML1 [t(12;21)]‡ High expression of CD10 Favorable6. Cases with a distinct GEP (high expression of receptor
phosphatase, PTRM, and LHFPL2) with no consistent cy-togenetic abnormality (including normal, pseudodiploidy,or hyperdiploidy)
Unknown
7. Heterogeneous group lacking any defined genetic lesionsand not clustering with class 6
Unknown
* Data are from Yeoh et al100 and from Ross et al.101
† Precursor B ALL with more than 1 abnormality (ie, BCR-ABL and hyperdiploidy of .50 chromosomes) may only be assigned to 1 class (ie,hyperdiploidy by GEP)
‡ Fluorescence in situ hybridization analysis has been shown to be more sensitive than real-time polymerase chain reaction analysis for detectionof TEL-AML1.
erarchic clustering identified 2 well-defined groups thatcorrelated with the T-cell or B-cell immunophenotype ofALL.98 Further analysis identified GEP that was associatedwith the presence of MLL1-AF4 or BCR-ABL gene rear-rangements; MLL1-AF4 cases again had unique GEP thatwas distinguishable from the other subgroups of ALL.
Kern et al3 compared FC and MA methodology in par-allel and correlated the protein expression levels andmRNA abundance of 39 relevant genes in 113 samplesfrom patients with newly diagnosed AMLs/ALLs and in4 normal BM samples. Congruent results were obtainedin 69% with regard to positivity or negativity of expres-sion, and there was a significant correlation between theprotein expression and mRNA abundance for positivityand expression of genes that are essential for diagnosingand subclassifying AML and ALL.
Kohlmann et al99 subsequently analyzed the expressionprofiles of 12 000 genes and 22 000 genes using HD oli-gonucleotide MAs in adult ALL (25 cases) and in AML(65 cases). The GE signature of a small set of differentiallyexpressed genes was sufficient to accurately discriminatebetween 8 clinically relevant acute leukemia subgroupsbased on their distinct GEP (AML with 8;21, 15;17, 11q23/MLL, or inv(16); B ALL with 9;22, 8;14, or 11q23/MLL;and T ALL). For the 4 AML subtypes, the 24 most infor-mative genes were used, and the gene that was most valu-able for the prediction of M4Eo AML subtype with inv(16)was MYH11. Seventeen genes were used for B ALLs.Genes encoding for the T-cell receptor b subunit and thesurface CD3 d chain were identified as being highly in-dicative of T ALL. CD10 was highly expressed in ALLwith 9;22 only. The identification of connective tissuegrowth factor as being specific for ALL with 4;11 was alsoconfirmed.
SUBTYPES OF ALLThe GEP study of pediatric ALLs by Yeoh et al100 used
oligonucleotide MAs with HC to analyze GEP in leukemicblasts from 360 pediatric ALLs and identified 6 major leu-kemia subtypes, corresponding to T ALL, hyperdiploid(.50 chromosomes), BCR-ABL, E2A-PBX1, TEL-AML1,and MLL gene rearrangements. In addition, a seventh sub-group was identified with a distinct GEP that includedcases with normal, pseudodiploid, or hyperdiploid kar-yotypes and that lacked any consistent cytogenetic abnor-
mality. This subgroup was defined by the high expressionof a group of genes that included the receptor phosphatasePTPRM and LHFPL2, a gene that is a part of the LHFP-like gene family, the founding member of which was iden-tified as the target of a lipoma-associated chromosomaltranslocation.
Classification in this study was approached using a de-cision-tree format, in which the first decision was T ALLversus B lineage (non–T ALL); then within the B-lineagesubset, cases were sequentially classified into the knownrisk groups that are characterized by the presence of E2A-PBX1, TEL-AML1, BCR-ABL, and MLL chimeric genes andhyperdiploid (.50 chromosomes) (Table 5).100 Cases thatwere not assigned to one of these classes were left unas-signed. Application of this classification model to a blind-ed test set of the remaining 112 samples resulted in anoverall accuracy of 96% for class assignment. The numberof genes that was required for optimal case assignmentvaried between classes; a single gene was sufficient to give100% accuracy for T ALL (CD3D) and for E2A-PBX1(PBX1), whereas 7 to 20 genes were required for the pre-diction of the other classes.
Gene expression profiling that was specific for the im-munophenotypically defined differentiation stages of theB ALLs could not be defined; the top-ranked discriminat-ing genes primarily consisted of genes that were overex-pressed within the specific leukemia subtype.100 However,for T ALL, 2 gene clusters were identified, one expressedat high levels and one at low levels. T-lineage–restrictedRNA expression was observed for CD2, CD3, and CD8,whereas B-lineage–restricted expression was observed forCD19 and CD22. The level of CD10 RNA expression cor-related with protein levels, with high expression detectedin TEL-AML1 leukemias, intermediate expression in E2A-PBX1, and low to undetectable expression in cases withrearrangements of MLL.
The rare cases that were misclassified by GE analysiswere informative.100 For example, 4 leukemias that wereinitially misclassified (because they were lacking the clas-sic chimeric transcript by RT-PCR analysis) were correctlyassigned to the TEL-AML1 group. On further analysis, 1case was shown by FISH analysis to have a TEL-AML1fusion, presumably a variant rearrangement that could notbe detected with the amplification primers used for theTEL-AML1 RT-PCR assay. In the other 3 cases, reexami-

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 503
nation of the karyotypes revealed translocations that in-volved the p arm of chromosome 12 in each case. By FISHanalysis, 2 of these cases had deletion of 1 TEL allele,whereas the remaining case had a partial deletion of 1TEL allele. Therefore, the identified GEP appears to reflectan abnormality of the TEL transcription factor and mayprovide a more accurate means of identifying a specificleukemia subtype that is defined by its underlying biolo-gy.
Collectively, these data suggest that the single platformof GEP can accurately identify the known prognostic sub-types of ALL.100 The authors of the study assert that, oncea diagnostic algorithm using a defined set of genes is es-tablished, its routine use in a clinical setting will requireonly minimal expertise. They also predict that, as the costof GEP decreases, this type of analysis will likely becomecompetitive compared with the cumulative cost of the var-ious diagnostic studies that are presently used.
A subsequent study examined leukemic blasts from 132pediatric ALLs using HD oligonucleotide MAs represent-ing most of the identified genes in the human genome andidentified discriminator genes for the subgroups, achiev-ing an overall diagnostic accuracy of 97%.101 Almost 60%of the newly identified subtype discriminating genes werenovel markers that were not identified in the previousstudy100 and provided new insights into the altered biol-ogy underlying ALLs.101 Some of the newly selected geneswere highly ranked as class discriminators and, when in-corporated into class-predictor algorithms, resulted in anoverall diagnostic accuracy of 97%.
In agreement with the results of the previous study,100
these unbiased clustering algorithms demonstrated thatpediatric ALLs clustered primarily into the following 7major subgroups: T ALL and 6 subtypes of B ALL cor-responding to (1) rearrangement in the MLL gene, (2) t(1;19)(E2A-PBX1), (3) hyperdiploid (.50 chromosomes), (4)t(9;22)(BCR-ABL), (5) the previously described novelgroup,100 and (6) t(12;21)(TEL-AML1) (Table 5).101 In addi-tion, a heterogeneous group of B-lineage cases was iden-tified that lacked any of the defined genetic lesions andthat failed to cluster in the novel subgroup (Figure 5). Onehundred percent diagnostic accuracy was achieved foronly 2 of the leukemia subtypes (T ALL and TEL-AML1).The top 5 class-discriminating genes were used in a su-pervised learning algorithm and resulted in 97% accuracyof class assignment. Although the number of genes thatwas required for optimal class assignment varied betweenclasses, the overall diagnostic accuracy was the same us-ing the top 20 or the top 50 genes per class.
Of the rare misclassification errors, 2 were BCR-ABL–expressing ALLs that by GE analysis were classified ashyperdiploid (.50 chromosomes).101 Therefore, GEP cor-rectly identified the presence of the hyperdiploid (.50chromosomes) class; however, because each case is as-signed to only a single class, the algorithm failed to cor-rectly identify the presence of BCR-ABL. Nevertheless, thedata demonstrated the exceptional accuracy of this singleplatform for the diagnosis of the prognostically importantsubtypes of pediatric ALL.
COMPARISON OF GEP OF PEDIATRIC ANDADULT ALLs
Kohlmann et al102 showed that GE signatures that weredefined for pediatric ALLs also distinguished the sub-types of 34 adult ALLs. Previously reported GEP that was
identified by MA technology100 was validated and con-firmed on independent leukemic samples, including BALLs with MLL (10 cases) and with t(9;22) (15 cases) andT ALLs (9 cases).102 Kohlmann et al102 also analyzed 7 ge-netically more heterogeneous adult B ALLs that were neg-ative for t(9;22) and MLL chromosomal aberrations, whichwere projected into the space of the 510 relevant leukemiasubtype genes and were shown to intercalate with BCR-ABL–positive ALLs, sharing similar characteristics withBCR-ABL–positive ALLs. Furthermore, by HC, the moreheterogeneous B ALLs were exclusively distributed in thebranch containing all BCR-ABL–positive ALLs (Table 5).
In the study by Kohlmann et al,102 several subtrees in-dicated coexpression of genes for the distinct ALL sub-types. Subtree 1 contained the following genes that wereoverexpressed in T ALL that have also recently been re-ported in other MA studies90: TRB, CD1D, CD1E, CD2,CD6, MAL, LCK, ITM2A, and SH2D1A. A large numberof these genes and candidates, such as transmembraneadapters (LAT and TRIM), additional CD3 complex signaltransducing members (CD3G, CD3Z, and CD8A corecep-ter), and ZAP70 tyrosine kinase, could be correlated to afunctional role in the class I MHC-restricted T-cell recep-tor signalosome.102
Subtrees 4 and 5 grouped the genes with high expres-sion in MLL-positive ALLs, also recently reported by otherMA studies,93–96 including ADAM10, BLK, CD72, CD79A,CSPG4, HOXA9, HOXA10, IGHM, LGALS1, LM02, MBNL,MEF2A, PPP2R5C, PTPRC, and VLDLR.102 Candidategenes such as IGHM, BLK, and CD79A illustrated the B-lineage characteristics of these cases, and overexpressionof HOXA cluster members illustrated important compo-nents of leukemogenesis that are driven by MLL genetranslocations.
Subtree 3 mainly contained the genes with a functionalrole in immune response. BLNK, BRDG1, CD24, MHC2TA,CD74, HLA-DMA, HLA-DMB, HLA-DPA1, HLA-DRA,HLA-DPB1, HLA-DQB1, HLA-DRB1, HLA-DRB3, HLA-DRB4, and TNFRSF14 demonstrated similar patterns forBCR-ABL–positive cases, MLL-positive cases, and themore heterogeneous precursor B cases.102 Major compo-nents of the class II MHC-restricted antigen presentationmachinery were consistently overexpressed comparedwith T ALL samples: MHC2TA, interacting with MHCclass II and HLA-DM and CD74 promoters, is a highlyregulated transactivator governing all spatial, temporal,and quantitative aspects of MHC class II expression. Thechaperone CD74 (invariant chain) blocks the peptide-link-ing site or the newly synthesized MHC class II moleculesby its so-called CLIP fragment. HLA-DM molecules cata-lyze the exchange of CLIP for antigenic profiles that arederived from endosomal compartments. Twenty-six probesets demonstrated similar expression signatures for BCR-ABL–positive and the more heterogeneous B ALLs. Allcandidate genes were consistently overexpressed in thesecases compared with T ALL and MLL samples. LGMN(legumain), also called asparaginyl endopeptidase (AEP),has been reported to be critically involved in the process-ing of antigens for MHC class II presentation.102 Geneti-cally heterogeneous samples again clustered together withBCR-ABL cases; they did not manifest as an independentfourth distinct cluster that was separate from adult T ALL,MLL, and BCR-ABL–positive leukemias.102

504 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
PRECURSOR B ALL
Diagnosis and Differentiation From NormalCD19-Positive/CD10-Positive B-Cell Progenitors
An analytic comparison of GEP, using cDNA MAs, of17 pediatric B ALLs and of NBCs from adenoid tissuerevealed 25 genes that are most overexpressed comparedwith the reference, including 4 genes that are normallyexpressed only in myeloid hematopoietic cells (RNASE2,GCSFR, PRTN3, and CLC) and S100A12, which is nor-mally expressed in nerve cells and in myeloid cells.103 Inaddition to the myeloid-specific genes, other overex-pressed genes included AML1 (a transcription factor),LCP2 (an adaptor protein), and FGP6 (a fibroblast growthfactor).
Comparison of GEP of B ALL With Immunophenotypeand Cytogenetic Findings and Correlation of Cytogenetic
Findings and GEP With Prognosis
Hyperdiploidy. The previously described study byYeoh et al100 showed marked differences in GEP betweenthe subgroup of hyperdiploid ALL with more than 50chromosomes and the subgroup of hyperdiploid ALLwith 47 to 50 chromosomes. This marked difference inGEP is important because hyperdiploid ALL with morethan 50 chromosomes correlated with an excellent prog-nosis. Almost 70% of the genes that defined this subgroupwere localized to chromosome X or to chromosome 21.Moreover, the class-defining genes on chromosome X wereoverexpressed in the hyperdiploid ALL with more than50 chromosomes, irrespective of whether the leukemicblasts had a trisomy of this chromosome. Other studieshave shown that the presence of FLT3 mutations in hy-perdiploid ALL samples, which also frequently expresshigh levels of this receptor, extends the significance ofthese results to this genetic group and reinforces the valueof GE analysis as a powerful approach for the identifica-tion of novel therapeutic targets in ALL.104,105
t(1;19)(E2A-PBX1). Yeoh et al100 also offered insightsinto the underlying biology of the different leukemia sub-types. E2A-PBX1 leukemias were characterized by highexpression of the C-MER receptor tyrosine kinase(MERTK), a known transforming gene, suggesting that C-MER may be involved in the abnormal growth of thesecells. Therefore, they proposed that C-MER receptor ty-rosine kinase in E2A-PBX1 may prove to be a useful targetagainst which novel therapeutic agents could be devel-oped.
t(12;21)(TEL-AML1). High expression of MTG16, ahomologue of ETO, has been found in TEL-AML1 cases.100
Alteration of ETO family members in t(8;21) AML and inTEL-AML1 suggests that alteration in the biologic functionof ETO genes may be mechanistically involved in theseleukemias.
De novo purine synthesis is a target of widely used an-tileukemic agents (MTX and MCP). Therefore, Zaza et al106
determined the rate of de novo purine synthesis and theexpression of genes that are involved in purine metabo-lism in different ALL subtypes. Among 113 childhoodALLs, lymphoblasts with the TEL-AML1 translocation hadsignificantly lower de novo purine synthesis than all othergenetic subtypes of B ALL or T ALL. By assessing theexpression of 82 genes that are involved in purine metab-olism in ALL blasts from 38 patients with B ALL (14 withTEL-AML1 and 24 without), 16 genes were identified that
were differentially expressed in TEL-AML1–positive andTEL-AML–negative ALL (P , .001). The pattern of ex-pression of these 16 genes discriminated TEL-AML1–pos-itive ALL with a true accuracy of 84% (confidence interval,70%–94%) in an independent test (n 5 17; P , .001). Dif-ferentially expressed genes included HPRT, IMPDH,PAICS, and GART, all of which were expressed at a sig-nificantly lower level in TEL-AML1–positive ALL. Thesefindings established that TEL-AML1–positive ALL has sig-nificantly lower de novo purine synthesis and differentialexpression of genes that are involved in purine metabo-lism.
Kees et al92 defined GEP of a panel of 13 pediatric ALLcell lines (6 T ALL, 3 pre–B ALL, and 4 infant B ALL 2),using cDNA MAs, and compared the data with the resultsof immunophenotypic and cytogenetic analyses. Leuke-mia cells with translocations t(12;21)(TEL-AML1) and t(1;19)(E2A-PBX1) (already described) showed common GEP,and these subtypes were associated with a good treatmentoutcome, particularly with current treatment protocols. Incontrast, patients with the subtypes that are associatedwith t(4;11)(MLL-AF4) and with t(9;22)(BCR-ABL) (de-scribed in a subsequent section) will benefit from hema-topoietic stem cell transplantation.
t(11q23)(MLL-AF4). As discussed previously, MLL-positive ALLs display high expression of many myeloidand monocyte/macrophage-specific genes.100 This indi-cates derivation from an early-stage B-cell hematopoieticprogenitor that has initiated transdifferentiation to a my-elomonocytic cell.
The study by Rozovskaia et al107 of pediatric and adultALLs demonstrated that GEP distinguishing 4;11-positiveALLs from other ALLs includes overexpressed oncogenes(HOXA9, MEIS1, HOXA10, LMO2, MYC, LGALSI, andPDGFRB), overexpressed genes that are involved in drugresistance (CD44, DHFR, BMLH, and CAT), and overex-pressed genes that are involved in protection from apo-ptosis and in survival (CDC2, PPP2R5C, and MAP3K5).Gene expression profiling also distinguished underex-pressed proapoptotic genes (ITPR3, IGFBP3, and JUN),underexpressed tumor suppressors and growth inhibitors(FHIT, DAPK1, and MADH1), and overexpressed genesacting in cell cycle progression and in cell proliferation(CCNAI, BMYB, and CDKN3).
Yeoh et al100 further showed that HOXA9 and MEIS1were exclusively expressed in cases having MLL rear-rangements, indicating that these genes may be directlyinvolved in MLL-mediated alterations in the growth of theleukemic cells. HOX GE depends on the normal MLL pro-tein for appropriate expression108,109; therefore, HOX genesrepresent a set of targets that have been evaluated in MLL-positive leukemia. Select HOX genes are highly expressedin MLL-positive leukemias compared with other leuke-mias.96,97 This high-level expression of HOX genes in MLL-positive leukemias suggests that the presence of an MLLfusion protein leads to inappropriate expression of HOXgenes.110 As mentioned previously, FLT3 is the most dif-ferentially expressed gene that distinguishes MLL fromAML and ALL.94,95 As a tyrosine kinase receptor, FLT3represents an attractive valid therapeutic target for MLL-rearranged ALLs that are identified by MA GEP.50,111–113
Tsutsumi et al113 identified distinct GEP for 23 pediatricALLs with 11q23 translocations, including 4;11 (15 cases),11;19 (6 cases), and 5;11 (2 cases) compared with 9 ALLswith other translocations, including 12;21 (6 cases) and 1;

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 505
19 (3 cases) by analyzing Affymetrix (Santa Clara, Calif)oligonucleotide MAs (12 600 probe sets). Gene expressionscores of FLT3, MEISI, and CD44 for MLL-positive ALLswere particularly high compared with those for otherALLs. Also, there was lower expression of CD10, CD22,CD24, and CD79B in the MLL-positive ALLs comparedwith ALLs with other translocations. The authors of thisstudy also reported that a statistical analysis of GEP forthe 21 diagnostic MLL-positive ALLs revealed 2 sub-groups that correlated with prognosis. The transcriptionfactors CBF2 and CDP (a tumor suppressor) were highlyexpressed in the poor prognosis and the good prognosissubgroups, respectively. TRIP3 and CBF2 were the topdiscriminating genes in the poor prognosis subgroup, andCDP, NCOR1, USF2, ZFP36L2, and SMARCC2 were thetop discriminating genes in the good prognosis subgroup.Their downstream target genes were also differentially ex-pressed. This GEP study showed for the first time thatinfant MLL-positive ALL could be divided into 2 sub-groups that are predictive of outcome.
MLL Versus ALL Using No-DeterminantChromosomal Translocation
Qiu et al114 developed an integrated approach for GEPthat coupled suppression subtractive hybridization, con-catenated cDNA sequencing, and RT-PCR, and they iden-tified 600 genes that are differentially expressed between4;11 ALL and pre–B ALL using no-determinant chromo-somal translocation. The expression of 67 genes was ana-lyzed in different cytogenetic ALL subgroups and in Blymphocytes that were isolated from healthy donors.Three genes (BACH1, TP53BPL, and H2BS) were consis-tently expressed as a significant cluster that was associatedwith the low-risk ALL subgroups. Forty-two genes weredifferentially expressed in ALL versus normal B lympho-cytes, with no association with any particular ALL sub-groups. The remaining 22 genes were part of a specificGEP that was associated with the hyperdiploid, 12;21, and4;11 subgroups. The 12;21 subgroup was characterized byan increase in DKFZP566J091, p68, and UN18 GE and bya decrease in FLT3 expression. The hyperdiploid groupwas characterized by increased expression of RTVP1,IFITM2, and IFIT1 and by decreased expression of BAALCand UN197. The 4;11 subgroup was characterized by in-creased KIAA1576, DAD1, HOXA9, and MEIS1 and by de-creased ERG, CD10, and FBXW7. Only one gene charac-terized the no-determinant chromosomal translocationgroup, AC133, a marker of hematopoietic stem and pro-genitor cells. It was consistently expressed at a low levelin ALL and was differentially expressed using no-deter-minant chromosomal translocation. High levels of AC133expression were detected in the hyperdiploid and 4;11ALL.
Philadelphia Chromosome–Positive ALL and SignificantDifferences Between Childhood and Adult Philadelphia
Chromosome–Positive ALLScrideli et al115 dissected the heterogeneity in Philadel-
phia chromosome (Ph)–positive ALL by analyzing the GElevels at diagnosis of genes that had emerged as beingparticularly significant in Ph-positive ALL by GEP,100,116
and the authors found the genes to be limited to thoseinvolved in cell cycle control, apoptosis, or stress re-sponse.115 Among the 10 genes whose expression was spe-cific enough to discriminate childhood Ph-positive leuke-
mia from other genetic subclasses, Scrideli et al115 selectedthe following 4 related genes: mitogen-activated proteinkinase–activated protein kinase 3 (MAPKAPK3), cyclin D2,caspase 8, and caspase 10. In addition, the following 5genes were selected from those that presented the highestdifferential expression in adult Ph-positive ALL that wasresistant to imatinib mesylate (Gleevec, Novartis Phar-maceuticals Corporation, East Hanover, NJ) and was sen-sitive to imatinib: histone-deacetylase 2 (HDAC2), mini-chromosome maintenance Schizosaccharomyces pombe ho-mologue of 6 (MCM6), microtubule affinity–regulating ki-nase 3 (MARK3), beclin 1 (BECN1), and telomerase proteincomponent (TEP1).
Using this approach, 26 pediatric and 9 adult BM sam-ples of Ph-positive ALL were compared with 8 normal BMsamples and with 5 normal PB samples.115 Compared withnormal BM, the mean levels of GE in normal PB was low,except for BECN1, whose expression was higher in PB, andHDAC2 and MAPKAPK3, which had similar expressionlevels in BM and PB. Different GEP was observed in nor-mal BM compared with Ph-positive ALL blasts. For mostgenes (HDAC2, MAPKAPK3, CASP8, TEP1, and MCM6),the level of expression in normal BM was significantlyhigher than that in Ph-positive ALL blasts, although greatheterogeneity was observed. Only BECN1 and MARK3 GEwas significantly less in the normal BM compared withthe Ph-positive ALL blasts, while for CCND2 the valueswere similar. The level of expression of CASP10 in normalBM was more similar to that of pediatric Ph-positive ALLBM samples. This finding suggests participation of thesegenes in the Ph-positive leukemogenesis.
Multidimensional analysis has shown a statistically sig-nificant difference in GE levels of 9 genes between pedi-atric and adult Ph-positive ALLs (P 5 .001).116 In partic-ular, a significant difference in expression levels was ob-served for the HDAC2, MAPKAPK3, CASP10 (showing thehighest difference), MARK3, and TEP1 genes. Gene ex-pression profiling of the adult group was more similar tothat of the pediatric group with poor response to pred-nisone than to that of the pediatric group with good re-sponse. While the children with good response differen-tially expressed 4 genes (HDAC2, CASP10, TEP1, andMARK3) compared with adults (P , .05), these differenc-es were reduced to 2 genes (CASP10 and TEP1) whencomparing children with poor response with adults. Nomajor differences were observed in GEP for the geneswhen comparing pediatric patients with good and poorresponse (P 5 .40). However, the patients in the good re-sponse group who relapsed or died showed GE levels thatwere more similar to those of the patients in the poorresponse group and of the adults than to the children withgood response who were in clinical complete response(CCR). Therefore, investigators in this GEP study and ina subsequent study identified a set of genes whose ex-pression discriminated between resistance and sensitivityof Ph-positive ALL to imatinib.116,117 The application of thistechnique has generated several hypotheses regarding theability of these leukemic cells to bypass the BCR-ABL sig-nal transduction pathway and to proliferate even in thepresence of imatinib.
Comparison of Ph-Positive ALL With MLL-AF4 ALL andTEL-AML1 ALL
Fine et al118 obtained a global view of GE in cell linesand in pediatric ALLs that harbored 1 of several chro-

506 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
mosomal abnormalities (BCR-ABL, MLL-AF4, and TEL-AML1). Each chromosomal abnormality was associatedwith a characteristic GE signature in cell lines and in clin-ical samples. However, BCR-ABL was associated with amore heterogeneous pattern of expression than the TEL-AML1 and MLL abnormalities. Among the genes found tobe statistically significantly differentially expressed in 2groups with BCR-ABL abnormalities was CD20. The in-vestigators were unable to assess a difference in clinicaloutcome between these groups. The erythropoietin recep-tor (EPOR) was consistently highly expressed in TEL-AML1 ALL compared with BCR-ABL and MLL.
Prediction of Relapse, Minimal Residual Disease,Response to Therapy, and Development of Therapy-Related Malignancies in Unrelated Tissues in ALL
Prediction of Relapse. To determine whether GEPmight further enhance the ability to identify patients whoare likely to relapse, Yeoh et al100 compared GEP of thefollowing 4 groups of leukemic samples: (1) diagnosticsamples from patients who developed hematologic relaps-es, (2) diagnostic samples from patients who remained inCCR, (3) diagnostic samples from patients who developedtherapy-induced AML, and (4) leukemic samples collectedat the time of ALL relapse. Not surprisingly, because ofthe overwhelming differences in GEP of the different ALLsubtypes, a single GEP that was predictive of relapse, ir-respective of the genetic subtype, could not be identified.However, within individual leukemic subtypes, distinctGEP could be defined that predicted relapse. For the TALL and hyperdiploid (.50 chromosomes) subgroups,GEP identified patients who relapsed with accuracies of97% and 100%, respectively.
A key point is that no single gene could predict the riskof relapse; rather, patterns of expression for a combinationof genes were predictive.100 A provocative observation wasthe identification of a distinct GEP in the ALL blasts frompatients who developed therapy-induced AML. Becausesecondary AML is thought to originate from a hemato-poietic stem cell that is distinct from where the primaryleukemia originates, it is difficult to understand how thebiology of the original ALL blasts could predict the riskof developing a therapy-induced complication (AML).Nevertheless, Yeoh et al100 evaluated the accuracy of GEPin identifying such patients. Although no single GEP wasidentified across the different leukemia subgroups, withinthe TEL-AML1 subgroup a distinct GEP consisting of 20genes was identified, with 100% accuracy in cross-vali-dation, in all patients who developed secondary AML (P5 .03). Genes within this signature included RSU1, a sup-pressor of the ras signaling pathway, and MSH3, a mis-match repair enzyme. Whether the overexpression of thesegenes is mechanistically involved in the increased risk oftherapy-induced AML or is only a chance association re-mains to be determined.
Staal et al5 evaluated GEP of 7 paired diagnosis-relapsesamples of B ALL using Affymetrix U95A chips contain-ing 12 600 human genes. These diagnosis-relapse compar-isons revealed 6 genes that differed significantly in ex-pression. These were mostly signaling molecules (the Btk-associated SH3-domain–containing protein SH3 BH5 andthe ras guanyl-releasing protein RASGRP2) and transcrip-tion factors (the transforming growth factor b–responsivetranscription factor Smad3) that are involved in cell pro-liferation and in cell survival and were highly up-regu-
lated at relapse, but there was no increase in drug-resis-tance markers (MDR1). This finding fits with the obser-vation that tumors with a high proliferation index have apoor prognosis. The genes that changed in quantity be-tween diagnosis and relapse are not in use as diagnosticor disease progression markers but represent potentialnew markers for such applications.
Subsequently, GEP analysis (using Affymetrix FocusArray GeneChip) of 45 pediatric ALLs that accurately(100% accuracy) classified precursor B versus T lineageeven in samples with as few as 10% leukemic cells alsopredicted 5-year event-free survival or relapse after treat-ment, independent of immunophenotype.119 The sensitiv-ity and specificity for prediction of relapse were 87% and69%, respectively.
Detection of Minimal Residual Disease. Chen et al120
identified new markers of minimal residual disease(MRD) in B ALL by comparative cDNA MA analysis ofGEP of 4 newly diagnosed ALLs and of normal CD19-positive/CD10-positive B-cell progenitors from 2 healthydonors. Three hundred thirty-four of 4132 genes studiedwere overexpressed (1.5-fold to 5.8-fold higher) in leuke-mic cells relative to the normal samples. Nine genes wereselected from 274 genes that were overexpressed in at least2 leukemic samples, and expression of the encoded pro-teins was then measured by FC. Seven proteins (CD58,creatine kinase B, ninjurin 1, Ref1, calpastatin, HDJ-2, andannexin VI) were expressed in B ALLs at higher levelsthan those in normal CD19-positive/CD10-positive B-cellprogenitors (P , .05). CD58 was chosen for further anal-ysis, and anti-CD58 identified residual leukemic cells(0.01%–1.13%) in 9 of 104 BM samples from children withALL in CCR; the MRD that was estimated by CD58 stain-ing correlated well with the results of PCR analysis. Thesefindings indicate that studies of GE with cDNA arrays canaid in the discovery of markers for MRD in leukemia.
Subsequently, a comparison of the GE signatures ofALLs with high MRD load with those of ALLs withoutdetectable MRD during treatment identified 54 genes thatdistinguished resistant from sensitive ALLs.121 Genes withlow expression in resistant samples were predominantlyassociated with cell cycle progression and with apoptosis,suggesting that impaired cell proliferation and apoptosisare involved in therapeutic resistance. Prediction analysisusing randomly selected samples as a training set and theremaining samples as a test set revealed an accuracy of84%. The investigators concluded that resistance to che-motherapy seems at least in part to be an intrinsic featureof ALL cells. Because the therapeutic response could bepredicted with high accuracy, GEP may become a clini-cally relevant tool for therapeutic stratification in the earlycourse of pediatric ALL.
Response to Chemotherapy. Foa et al97 comparedGEP of adult ALL patients who achieved CCR with thatof patients who were refractory to induction chemother-apy and identified a small set of genes that were differ-entially expressed in 2 case series. They also identified aset of genes that were significantly associated with theduration of remission.
The genomics of cellular responses of 60 pediatric ALLsbefore and after treatment with methotrexate and mercap-topurine, alone or in combination, have also been eluci-dated by GEP.122 One hundred twenty-four differentiallyexpressed genes accurately discriminated the 4 possibletreatment groups. Genes included those that are involved

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 507
in apoptosis, mismatch repair, cell cycle control, and stressresponse. Leukemic cells in different patients appeared toreact in a similar manner after specific therapy andseemed to share common pathways of genomic responsesto a variety of drug schedules.
Holleman and coworkers123 subsequently used an in vi-tro assay to analyze leukemic cells from 173 pediatricALLs for sensitivity to prednisolone, vincristine, asparag-inase, and daunorubicin. Gene expression profiling usingHD oligonucleotide MAs identified genes that were dif-ferentially expressed in patients with drug-sensitive anddrug-resistant ALLs who were treated with prednisolone(33 genes), vincristine sulfate (40 genes), asparaginase (35genes), and daunorubicin hydrochloride (20 genes). On thebasis of the observation that in vitro resistance to thesedrugs is associated with prognosis, Holleman and co-workers123 tested the prognostic significance of GEP thatis associated with sensitivity or resistance to the 4drugs.124 A combined GE score that indicated resistanceto these 4 agents was significantly and independently re-lated to treatment outcome, in this series123 and in an in-dependent cohort of patients who were treated at anotherinstitution. 124 The results from this study demonstratedthat drug resistance was associated with the differentialexpression of a small number of genes and that this ge-netic signature could predict the treatment outcome inchildhood ALL.123
Development of Therapy-Related Malignancies in Un-related Tissues in ALL. A comparison of GEP of diag-nostic ALL blasts of 9 patients who developed radiother-apy-associated brain tumors with GEP of 33 patients whodid not identified 33 probe sets that were associated withthe time-dependent development of brain tumors, usingweighted rank regression analysis.125 K-means clusteringidentified 2 groups that differed significantly in the cu-mulative incidence of brain tumors (P 5 .01). Linear dis-criminant analysis (time-independent categorization ofoutcome) was used to identify 70 probe sets whose ex-pression differentiated between the 2 groups of patients.Five probe sets were in common between the time-inde-pendent and time-dependent methods. The distinguishinggenes included those involved in neural growth (FGFRI)and in nuclear trafficking (HNRPL and KPNBI). These datasuggest that GEP from accessible tissues may identify tar-gets that are involved in therapy-related malignancies inunrelated tissues.
PRECURSOR T ALLSeveral genes have been shown to play a role in T ALL,
including HOX11, SCL, LM01, LM02, and LYL1. Ferrandoet al126 studied 37 T ALLs and demonstrated that distinctGEP was strongly associated with specific oncogenic tran-scription factors. Using GE studies, they identified 5 T-celloncogenes (HOX11, TAL1, LYL1, LMO1, and LMO2) thatwere often aberrantly expressed in a much larger fractionof T ALLs than those actually harboring the activatingchromosomal translocations. Using oligonucleotide MAs,these investigators identified several GE signatures thatwere indicative of leukemic arrests at specific stages ofnormal thymocyte development, including the LYL1-posi-tive signature (pro-T), HOX11-positive signature (earlycortical thymocyte), and TAL1-positive signature (late cor-tical thymocyte) (Figure 6). These results suggest that T-cell oncogenes interfere with transcription programs thatcontrol thymocyte development, leading to stage-specific
developmental arrest. Hierarchic clustering analysis of GEsignatures grouped the samples according to their sharedoncogenic pathways and identified HOX11L2 activation asa novel event in T-cell leukemogenesis. Five multisteppathways leading to T ALL were subsequently identifiedthat involved activation of the following 5 T ALL onco-genes: HOX11, HOX11L2, TAL1-LMO1/2, LYL1-LMO2, andMLL-ENL (Table 6).127 HOX11 activation was significantlyassociated with a favorable prognosis when patients aretreated with modern combination therapy, while expres-sion of TAL1, LYL1, or, surprisingly, HOX11L2 confers amuch worse response to treatment and a high risk of earlyfailure.
HOX11, an orphan homeobox gene that is essential forsplenic development, is activated in a subset of T ALLcases bearing t(10;14)(q24;q11) or t(7;10)(q35;q24) trans-location; overexpression of the HOX11 orphan homeoboxgene occurs in 5% to 10% of pediatric T ALLs and in 30%of adult T ALLs.92 Using quantitative RT-PCR analysis ofthe HOX11 gene, Kees et al92 identified a substantial pro-portion of HOX11-positive cases that express high levelsof the oncogene and that lack cytogenetically detectablealterations of the 10q24 region. By subsequent nearestneighbor analysis, HOX11-positive cases showed in-creased expression of the CD1, LAR, and CD10 genes ina pattern that resembled that of normal cells undergoingthe early cortical stage of thymocyte differentiation. Manyof the genes that are associated with HOX11 expressionare involved in cell growth and in proliferation. HOX11can immortalize hematopoietic progenitors and can inter-act directly with cell cycle regulatory proteins. High levelsof HOX11 correlated with increased expression of MYCand of the proapoptotic glucocorticoid receptor gene. Be-cause drugs used to treat human leukemias are more ac-tive in proliferating cells, the better therapeutic respon-siveness in HOX11-positive T ALL may be explained bythe expression of genes that are associated with increasedproliferative activity and by the lack of expression of bcl-2 and related antiapoptotic genes in HOX11-positive lym-phoblasts.
Prominent among T-cell oncoproteins are the followingmembers of the basic helix-loop-helix family of transcrip-tion factors: TAL1, TAL2, LYL1, and the recently describedBHLHB1 protein.92 These transcription regulators are be-lieved to act through a common mechanism that involvesdominant negative interference with the activities of theE47 and E12 variants of E2A transcription factors, whosehomozygous inactivation leads to T-cell tumors in mice.Quantitative real-time polymerase chain reaction analysisrevealed increased levels of TAL1 mRNA in 29 (49%) ofthe 59 cases. None of these samples harbored any of therecurrent translocations of chromosome band 1p32 thatare known to cause aberrant expression of TAL1 in T ALL.However, 9 (31%) of the 29 cases with increased expres-sion of TAL1 had the TAL1D variant, which results froma small deletion next to the TAL1 locus. Therefore, mostcases with high levels of TAL1 oncogene expression lackedcytogenetic and molecular evidence of rearrangements af-fecting the TAL1 locus. In contrast to HOX11-positive cas-es, the GE pattern that is associated with TAL1 expressionappears to reflect the late cortical stage of thymocyte dif-ferentiation, as indicated by the upregulation of LCK,TCRA, TCRB, CD2, CD6, and CD3E. TAL1 overexpressionwas associated with the up-regulation of proto-oncogenessuch as CBFA2 (AML1) and the myb-related gene MYBL2,

508 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
Figure 6. HOX11-positive, TAL1-positive,and LYL1-positive nearest neighbor analysis.Each row of squares shows the expressionpattern of a particular gene that was selectedby nearest neighbor analysis,90 while eachcolumn represents 1 of the 27 samples thatwere positive for HOX11, TAL1, or LYL1 byreal-time polymerase chain reaction. Thegenes depicted were chosen from the top 200nearest neighbors of each major oncogene(boldface type) on the basis of their potentialfunctional relevance and then were groupedaccording to their involvement in T-cell dif-ferentiation, apoptosis, cell proliferation, orchemotherapy response. Expression levels foreach gene were normalized across the sam-ples; levels greater than and less than themean (by as much as 3 SDs) are shown inshades of red and blue, respectively. Num-bers at the bottom correspond to the casenumbers of the samples in the study. Data arefrom Ferrando et al126 and are reprinted withpermission from Elsevier Inc.
Table 6. Distinctive Gene Expression (GE) Signatures of Precursor T Acute Lymphoblastic Leukemia (ALL) andCorrelation With Stage of Differentiation, Markers, Cytogenetic Findings, and Prognosis*
T-Cell OncogenesExpressed Stage of Differentiation
Correlation WithKnown Markers
Correlation WithCytogenetic Findings Prognosis
LYL11
(LMO21 and LM012)†Undifferentiated or
prothymocyteCD341
bcl-21
Myeloid markers1
5q and 13q deletions Unfavorable
HOX111 Early cortical thymocyte CD11, CD101/2, CD41,CD81, CD32
t(10;14)/(q24;q11) ORt(7;10)(q35;q24)
Favorable
TAL11
(LMO11 or LMO21)‡Late cortical thymocyte CD21, CD3e1
bcl-2A11
Recurrent translocations ofchromosome band 1p32
Unfavorable
HOX11L2 NA Not described Chromosome 5q abnormal-ity
Unfavorable
MLL-ENL§ NA Not described t(11;19)(q23;p13.3) Not necessarilyunfavorable
* Data are from Ferrando et al126 and from Ferrando and Look.127
† The LYL11 GE signature was associated with high expression of LM02 but not LM01.‡ The TAL11 GE signature was associated with expression of LM01 or LM02.† Very rare cases of precursor T ALL reveal MLL-ENL by real-time polymerase chain reaction analysis; none of these rare patients have died.

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 509
receptor genes such as IL8R and CSFR1, and the antia-poptotic gene bcl-2A1.
Thirteen (22%) of the 59 cases were classified as beingLYL1 positive on the basis of LYL1 expression levels thatwere 5-fold greater than the LYL1 expression level in nor-mal thymocytes.92 Again, increased expression of this on-cogene was not associated with cytogenetic abnormalitiesaffecting the LYL1 locus. High levels of LYL1 expressionwere associated with an undifferentiated thymocyte phe-notype that was characterized by increased expression ofthe early hematopoietic marker gene CD34, the cell ad-hesion gene L-selectin (SELL), the antiapoptotic gene bcl-2, and LSP-1, which encodes the lymphocyte-specific pro-tein 1. LYL1 positivity was related to higher expressionlevels of the MYCN, LMO2, and PLZF proto-oncogenes, aswell as the antiapoptotic gene bcl-2. As mentioned previ-ously, less favorable outcomes were observed in subgroupsthat were defined by GEP that is characteristic of TAL1-positive and LYL1-positive samples, which resemble latecortical and early pro-T thymocytes, respectively. Drugresistance in LYL-positive cases may be explained by thefact that early double-negative pro–T cells express highlevels of bcl-2 and show increased resistance to apoptosis.TAL1-positive cells appear to up-regulate bcl-2A1 (alsoknown as BFL1) and other antiapoptotic molecules thatare normally induced by signaling through the TCT in latecortical thymocytes, suggesting different mechanisms oftreatment-resistance in TAL1-positive and LYL1-positivecases. Therefore, the up-regulation of bcl-2 and bcl-2A1 inLYL1-overexpressing and in TAL1-overexpressing casesmay explain their relative resistance to chemotherapy,while the responsiveness of HOX11-positive cases couldpartly reflect the down-regulation of survival factors inearly cortical-stage thymocytes, most of which are target-ed for ‘‘death by neglect.’’
An analysis of the LIM-only domain genes (LMO1 andLMO2) showed an absence of significant expression of ei-ther LMO gene in the HOX11-positive samples.92 However,overexpression of one of these genes was observed in mostsamples that overexpressed TAL1, and high levels ofLMO2, but not LMO1, were found in the LYL1-positivesamples. These results support the theory that LMO pro-teins form heterocomplexes and act in concert with TAL1and possibly other bHLH proteins in T ALL. The findingof the abnormal expression of 1 or more of these onco-genes as being biallelic implicates upstream regulatorymechanisms.
In addition, 10 of 59 cases did not express abnormallevels of any of the aforementioned transcription factorgenes, raising the possibility of thymocyte transformationvia alternative oncogenic mechanisms.92 Although helpingto identify the sets of genes that are coordinately ex-pressed with HOX11, TAL1, and LYL1, the nearest neigh-bor analysis provided little useful information about the10 cases that lacked discernible expression of these onco-genes. To gain insight into the molecular characteristics ofthese poorly understood cases, Kees et al92 generated HCbased on 72 genes whose expression patterns best distin-guished between each group of HOX11-positive, TAL1-positive, LYL1-positive, and other cases in pairwise com-parisons. The HOX11-positive, TAL1-positive, and LYL-positive samples that were detected by RT-PCR weregrouped together within major branches of the dendro-gram. The branch containing the HOX11 samples com-prised 2 subgroups, one containing most of the HOX11
RT-PCR–positive cases and the other consisting primarilyof HOX11-like samples that lacked HOX11 expression byRT-PCR. Surface immunophenotype showed that thesesubgroups had related but distinct immunophenotypes.True HOX11 samples were primarily CD1 positive, CD10positive and negative, CD4 positive, CD8 positive, andCD3 negative (early cortical thymocytes), while theHOX11-like samples were primarily CD1 positive andnegative, CD10 positive, CD4 positive, CD8 positive, andCD3 positive (early cortical thymocytes with acquiredCD3 surface expression).
Similarly, the central cluster of TAL1-positive samplescontained 2 subgroups, a larger one comprising most ofthe true TAL1-positive samples and another one consistingmainly of TAL1-like samples.92 A third smaller branchemerged from the HC analysis and was characterized bya global pattern of increased expression of many of thegenes that distinguished among the other 3 groups (ie,HOX11, LYL1, and LIM-only domain genes). Two of 3 cas-es in this smaller branch had t(11;19)(q23;p13.3), whichproduces the MLL-ENL fusion gene, while the third casehad a normal karyotype. A previous study also identifiedMLL-ENL fusion in a subset of T ALL.128 Subsequent MLL-ENL RT-PCR analysis by Ferrando et al26 that was per-formed in 59 samples revealed the MLL-ENL fusion tran-script in only 3 cases, all in the third smaller-branch clus-ter that was identified by Kees et al,92 including the casewith a normal karyotype. These results illustrate the pow-er of DNA MA analysis to group samples according tospecific mechanisms of leukemic transformation.
Finally, the LYL-positive cluster included 2 branches.92
One contained 3 of the true LYL-positive samples, includ-ing the only T-cell sample in this series with the FLT3internal tandem duplication, which is often identified inAMLs. These leukemias also expressed high levels ofCD34 and myeloid markers, which is consistent with dif-ferentiation arrest in the early stages of T-cell develop-ment, when T-progenitor cells are migrating from the BMto the thymus. A second branch contained a LYL-positivesample and 2 samples with simultaneous expression ofTAL1 and LYL1 by quantitative RT-PCR. The exclusivepresence of cytogenetic features such as the 5q and 13qdeletions within the second-branch subgroup further at-tests to the effectiveness of the HC approach in this studyto group samples with common mechanisms of transfor-mation and suggests that tumor suppressor genes in the5q and 13q regions are inactivated as part of a distinctoncogenic pathway from which these leukemias originate.
The observation that T ALLs with MLL-ENL rearrange-ment and recurrent cytogenetic abnormalities weregrouped together in the HC analysis illustrates the abilityof GEP to identify cases with common mechanisms oftransformation. Results of this analysis also suggested thatcases without defined oncogene activation that clusteredwith the HOX11, TAL1, or LYL1 samples likely harbor re-lated but as yet unidentified oncogenes.92
This study also used quantitative RT-PCR to analyze theexpression of HOX11L1 and HOX11L2, 2 homeobox genesthat are functionally and structurally related to HOX11.92
HOX11L1 was expressed at comparable low levels in nor-mal thymus and in T ALL samples, indicating that it wasnot overexpressed in this group of leukemias. HOX11L2,on the other hand, was expressed at high levels in 6 TALL samples, and 3 of the 6 HOX11L2-positive cases hadsufficient RNA for MA analysis. The location in the

510 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
HOX11-related cluster that consisted primarily of HOX11-like samples that lacked HOX11 expression by RT-PCR ofthe hierarchic dendrogram confirms this study’s hypoth-esis that specimens with GE signatures resemblingHOX11-positive cases might be transformed through theeffects of highly related oncogenes operating through sim-ilar oncogenic pathways. Statistical analysis to identify thegenes that were differentially expressed in HOX11-posi-tive versus HOX11L2-positive cases revealed increased ex-pression of HOX11 and of 8 additional genes in HOX11-positive cases. None of the genes on the MA were ex-pressed at significantly higher levels in HOX11L2-positivecases. Therefore, despite the marked similarities in GEPbetween HOX11-positive and HOX11L2-positive cases,HOX11-positive cases are distinguished by increased ex-pression of genes that are involved in signal transductionand in chromatin-mediated control of GE.
Constitutive expression of HOX11 was associated witha favorable prognosis, with a 100% probability of survivalat 5 years, compared with 30% for the HOX11L2 groupand 51% for the BHLH-positive group.92 Patients whoseleukemic cells lacked expression of HOX11, HOX11L2, orBHLH oncogenes had essentially the same probability of5-year survival as the HOX11L2 group and the BHLH-pos-itive group. Primary drug resistance, demonstrated by thefailure to achieve CCR, was noted only in patients withoverexpression of TAL1 or LYL1. Similar results were ob-tained when Kaplan-Meier analysis focused on the majorgroups of GE signatures that were defined by HC: prob-ability of survival at 5 years was 92% for the HOX11-pos-itive cluster versus 43% and 33% for the TAL1-positiveand LYL1-positive clusters, respectively (P 5 .03). None ofthe 3 patients in the small cluster containing the MLL-ENLcases have died, suggesting that MLL-ENL translocationsin T ALL may not carry the dire prognosis that is asso-ciated with related translocations in infants and in olderchildren with a precursor B immunophenotype. In anotherrelated study, Ferrando et al129 reported that T ALLs withMLL-ENL fusion were characterized by an early arrest inthymocyte differentiation. They also reported that multi-ple genes linked to cell proliferation (PCNA, MYC, CDK2,POLA, DHFR, and TYMS) were down-regulated and thatmajor HOX genes (HOXA9, HOXA10, and HOXC6) andMEISI were up-regulated in these cases. They concludedthat MLL-positive T ALLs have a lower proliferative ratethan MLL-negative T ALLs, based on GEP.
Ferrando et al130 subsequently investigated the prognos-tic effect of the expression levels of the following 8 onco-genic transcription factors in 52 adult T ALLS: HOX11(TLX1), HOX11L2 (TLX3), TAL1, TAL2, LYL1, BHLHB1(OLIG2), LMO1, and LMO2. The leukemia-specific survivalrate for the 16 HOX11-positive patients was 88%, com-pared with 56% for all other patients (P 5 .02). Only theHOX11 oncogene expression subgroup showed a differ-ence in leukemia-specific survival, with HOX11 overex-pression conferring a good outlook for adult T ALLs.
Ballerini et al131 analyzed 28 T ALLs and detected TAL1in 6, HOX11L2 in 6, and HOX11 in 3; subclassification of50% of cases was obtained. HOX11L2 expression was as-sociated with a chromosome 5q abnormality (the locationof the HOX11L2 locus) in each case tested. Finally, thesedata showed that HOX11L2 expression was a suitablemarker for MRD follow-up and was significantly associ-ated with relapse (P 5 .02).
Chiaretti et al132 subsequently analyzed GEP in 33 adult
T ALLs. Nonspecific filtering criteria identified 313 genesthat were differentially expressed in the leukemic cells.Hierarchic clustering of samples identified 2 groups thatreflected the degree of T-cell differentiation (an undiffer-entiated group and a group with further T-cell differen-tiation), but the grouping was not associated with clinicaloutcome. A comparison between refractory patients andthose who responded to induction chemotherapy identi-fied high expression of a single gene, interleukin 8, andreduced expression of the remaining genes in refractoryT ALLs, as well as a set of 30 genes that were highlyexpressed in leukemic cells from patients who achievedCCR. Genes that were expressed at lower levels in the re-fractory group included a set of genes belonging to thehistone family (HIF0 and H2AFL) and several genes thathave a role in cell adhesion (CR2 and SELL) and in cellcycle progression (GF11 and BCL6). This pattern suggestsimpaired cell proliferation in T ALLs that did not respondto treatment. Another low-expressed gene in this groupwas Max-interacting protein 1 (MX11), a transcription re-pressor of Myc, which is thought to be a tumor suppressor.CD10 (which is characteristic of cycling apoptosis–pronecells) was expressed at lower levels in the refractory group.
Investigators in this study next identified 19 genes thatare differentially expressed in relapsed versus CCR pa-tients with T ALLs.132 ITBUB1B, TTK , and CENPF, whichplay a role in mitotic assembly and mitotic checkpoint,and CC2 were selectively and highly expressed, respec-tively, in CCR patients with T ALLs. AHNAK was amongthe few genes demonstrating increased expression in therelapse group. A model based on the expression of 3 ofthese genes (AHANK, CD2, and TTK ) was predictive ofduration of remission. The 3-gene model was validated inan additional 18 of patients with T ALL who were on thesame treatment protocol, demonstrating that GEP couldidentify a limited number of genes that are predictive ofresponse to induction therapy and of CCR duration inadult patients with T ALL.
ACUTE MYELOID LEUKEMIA
Correlation of GEP With French-American-BritishSubtype
To address whether French-American-British (FAB) sub-types showed distinct GEP to allow classification solelybased on GEP of a limited set of genes, Haferlach et al133
analyzed 20 000 genes using MAs of 130 AMLs that werecharacterized by cytomorphology and by cytogenetics (8M0s, 23 M1s, 28 M2s, 10 M3s, 9 M3vs, 13 M4s, 11 M4Eos,10 M5as, 12 M5bs, and 6 M6s). Real-time polymerasechain reaction was performed in all cases with 8;21, acutepromyelocytic leukemia (APL), and M4eos, and immu-nophenotyping was performed in all M0s. Based on theexpression of only 1 to 3 genes, it was possible to delineateM3, M3v, M4eo, and M6 from all other subtypes with100% accuracy. The comparison between M2 and M4 pro-duced the lowest accuracy (85%). Twenty-eight M2s wereclassified into the following 3 cytogenetic subgroups: 12with 8;21, 9 with a normal karyotype, and 7 with a com-plex aberrant karyotype.
A subsequent GEP study of 54 pediatric AMLs revealedthat those with t(8;21), inv(16), M4/M5 subtype, and M7subtype were grouped into different clusters.134 Thisgrouping suggests the existence of GEP that is specific tothese various subtypes.

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 511
Table 7. Acute Myeloid Leukemias With Recurringand Complex Abnormalities Associated With Distinct
Gene Expression Profiling and Correlation WithCommercially Available Molecular Markers by
Polymerase Chain Reaction (PCR) Analysisand With Prognosis*
CytogeneticAbnormality
MolecularMarker (PCR) Prognosis
t(8;21)t(15;17)inv(16)11q23Complex
AML1/ETOPML-RARCBFB-MYH11MLLNone
FavorableFavorableFavorableUnfavorableUnfavorable
* Data are from Haferlach et al.137
Figure 7. Hierarchic clustering (HC) analysis of adult acute myeloidleukemia (AML) samples (columns) using a combination of 1130 genes(rows) that were identified to separate specific cytogenetic subgroups.The normalized expression value of each gene is color coded: red in-dicates high expression; and green, low expression. The adult AMLsamples comprise 44 t(11q23)/MLL, 38 t(8;21), 42 t(15;17), 44 inv(16),and 76 complex aberrant karyotypes. The HC was performed by meansof the Euclidean distance metric and the Ward clustering algorithm asimplemented in GeneMaths software, version 2.01 (Applied MathsBVBA, Sint-Martens-Latern, Belgium). Data are from Schoch et al138
and are reprinted with permission.
Correlation of GEP With Recurring CytogeneticAbnormalities
A GEP study by Schoch et al135 revealed a unique cor-relation between AML-specific cytogenetic aberrationsand GEP (Table 7). They performed MA analyses on BMsamples from 37 adults with newly diagnosed AML, allrepresenting one of the distinct subtypes that were estab-lished by cytomorphology, cytogenetics, FISH, and RT-PCR, including M2 AML with t(8;21), M3 or M3v AMLwith t(15;17), or M4eo AML with inv(16). Using 2 differentstrategies for MA data analyses, a minimum set of only13 genes was sufficient to accurately predict the karyotype.
In an extended cohort of this study, GEP of 35 genesdistinguished with 100% accuracy between normal BM,M2 with 8;21, APL with 15;17, and M4eo AML withinv(16).136 A further step consisted of the addition of sam-ples with AML carrying 11q23/MLL rearrangements, rep-resenting an analysis of AML subtypes with all of therecurring chromosomal aberrations, as defined by theWorld Health Organization classification. Based on GEP, aminimum set of 39 genes was sufficient to distinguish be-tween normal BM samples and AMLs with 1 of the ab-errations with 100% accuracy using leave-one-out cross-validation.136
The potential of GEP to predict AML subtypes and toassign AMLs to specific cytogenetic groups, including t(8;21), inv(16), t(15;17), MLL, complex karyotype, and nor-mal karyotype, was validated with high accuracy (86%–100%) (Table 7).137 In addition, the transcription factorCEBPA, which is highly expressed in AMLs with inv(16),has been associated with a good outcome.138,139 The lowestaccuracy (86%) was seen in the group with a normal kar-yotype, indicating a high degree of heterogeneity in thisAML subtype.
A comparison of AMLs with a complex aberrant kar-yotype (36 cases) with AMLs with 8;21 (13 cases), inv(16)(12 cases), rearrangement of the MLL gene (15 cases), soletrisomy 8 abnormality (10 cases), and those with a normalkaryotype (64 cases) revealed that only 1 to 7 genes werenecessary to discriminate AML with a complex aberrantkaryotype from every other subgroup with 100% accuracyas assessed by leave-one-out cross-validation (Figure 7).140
The expression of HOXA9 and HOXA7 was discriminativebetween AML with a complex aberrant karyotype andAMLs with 8;21, 15;17, and inv(16), as both HOX geneswere expressed in group with a complex aberrant karyo-type but showed no or low expression in the prognosti-cally favorable subgroups. Compared with all other AMLsubtypes, AML with a complex aberrant karyotype had a
significantly higher expression of RAD21 (1.7-fold), whichis involved in double-stranded break repair and is apo-ptotic (P , .001). In addition, the expression of the follow-ing genes, which are involved in DNA repair and in DNAdamage-induced checkpoint signaling, was also signifi-cantly elevated 1.5-fold to 3-fold in AML with a complexaberrant karyotype: RAD1, RAD9, RAD23B, PIR51(RAD51 interacting protein), NBS1, MSH6, UBL1, andADPRTL2). The high expression of these genes may playan important role in resistance to chemotherapeutic agentsthat cause DNA damage.
A comparison of GEP of 15 AMLs with rearrangementsof the MLL gene and different partner genes with AMLswith trisomy 8 (13 cases), AMLs with a complex aberrantkaryotype (36 cases), and normal BM samples (9 cases)revealed that all groups could be classified robustly with100% accuracy (using leave-one-out cross-validation)based on distinct patterns of differentially expressedgenes.140 As mentioned previously, within the MLL sam-ples, a cluster of HOXA family members that includedHOXA7, HOXA9, and HOXA10 and TALE family genes(including PBX3 and MEIS1) was highly expressed.
Similarly, an independent comparison of GEP usingMAs of 28 patients with AML with 8;21, 15;17, inv(16),and 11q23 aberrations with 10 patients with AML withnormal cytogenetics (NC-AML) revealed many discrimi-nating genes.141 The expression status of specific genes cor-related with 11q23 and with AML of normal karyotype.The group with AML of normal karyotype was character-ized by distinctive up-regulation of members of the classI homeobox A and B gene families, implying a commonunderlying genetic lesion for AML of normal karyotype.

512 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
Three more recent reports on large and more represen-tative groups of patients with AML revealed the possibil-ity for a comprehensive unsupervised clustering of thedisease.142–144 Bullinger et al143 undertook an unsupervised2-way HC analysis that considered 6283 differentially ex-pressed genes in PB or BM samples from 116 adult AMLs,including 45 AMLs with a normal karyotype. Their anal-ysis delineated tight separate clusterings of AML with 15;17, 8;21, and inv(16). In the study by Valk et al,142 a Pear-son product moment correlation coefficient analysis wasused, with 2856 differentially expressed probe sets, basedon the ability of optimal clustering of known cytogeneticsubsets of AML. In this study, in 285 cases it appeared tobe possible to classify the prognostically important sub-groups of AML, including 8;21, 15;17, and inv(16). More-over, AMLs with 11q23 abnormalities or with FLT3 orCEBPA mutations aggregated in other signature clusters.In the final study, 130 pediatric AMLs and 20 adult AMLswere analyzed.144 In this study, unsupervised 2-dimen-sional HC analyses of pediatric AMLs resulted in recog-nizable clusters that were characterized by the geneticAML subtypes with the 15;17, 8;21, and MLL chimericfusion genes and by cases classified as FAB M7.
Different numbers of genes (13, 35, or 25 genes) havebeen shown to be predictive of AML with 8;21, inv(16),and 15;17, and the differences in the numbers of discrim-inating genes in these studies may be related to the se-lected study population.11,35,144 Valk et al142 were able topredict these 3 cytogenetic classes within a large and di-verse cohort of patients with AML according to the ex-pression levels of only 5 genes that were linked to thefusion genes of the recurrent translocation, including ETOin AML with 8;21 and MYH11, as well as AML withinv(16). In APL, the expression of hepatocyte growth fac-tor has been identified as being a particularly prominentdiscriminating gene.142
Gene expression profiling identified cases that had es-caped standard cytogenetic detection. Among homoge-neous expression clusters linked to inv(16) or 15;17, Valket al142 observed cases that had not initially demonstratedthe corresponding cytogenetic abnormality; however, ad-ditional molecular analysis of these cases revealed thepresence of these molecular abnormalities. Moreover, inthis same study, within clusters of patients carrying mu-tations in the CEBPA gene, cases without mutations in thisgene were found, suggesting that these AMLs share acommon underlying molecular theme. In addition, AMLwith FLT3-ITD was precisely discriminated within the 15;17 cluster, demonstrating the power of GEP to disclose themolecular heterogeneity within preestablished subsets ofleukemia.
FLT3/MLLThe most common molecular abnormality in AML is
the internal tandem duplication in the fms-like tyrosinekinase-3 gene (FLT3), a hematopoietic growth factor re-ceptor, which occurs in 23% of all cases and in 40% ofAMLs with a normal karyotype.93,145,146 Comparisons ofGEP of AMLs with a normal karyotype and AMLs withFLT3 length mutation (FLT3-LM) (21 cases) with GEP ofnormal BM samples (9 cases), AMLs with 8;21 (13 cases),inv(16) (12 cases), 15;17 (19 cases), TMLL (15 cases), tri-somy 8 (10 cases), and a complex aberrant karyotype (31cases) revealed discrimination of the FLT3-LM group fromtrisomy 8 with 97% accuracy and from all karyotypically
aberrant AML groups with 100% accuracy; the confidencewas 0.85 for comparison with AML with a complex ab-errant karyotype and 1.0 for all other comparisons.147 Al-though the delineation of AMLs with a normal karyotypeand FLT3-LM (27 cases) and AMLs without FLT3-LM (21cases) was not possible, the same analysis within each FABsubgroup resulted in a clear distinction between FLT3-LM–positive and FLT3-LM–negative cases. The 20 topgenes that were found to be discriminatively expressed ineach analysis varied substantially between the FAB sub-types, although many were downstream target genes ofthe FLT3 pathway.
Acute myeloid leukemia with FLT3-ITD is generallyidentified as a disease with a poor prognosis. RecentlyLacayo et al148 demonstrated that GEP could distinguish asubset with a good outcome among the AML cases withFLT3 mutations. An analysis of DNA MAs identified GEPrelated to FLT3 status and to outcome in childhood AML.Among 81 diagnostic specimens, 42 were FLT3-MU–pos-itive, and predictive analysis of MAs of these FLT3-MU–positive cases identified 128 genes that correlated withclinical outcome. Event-free survival in patients withFLT3-MU with a ‘‘favorable’’ signature was 45% versus 5%in those with an ‘‘unfavorable’’ signature (P 5 .02).Among FLT3-MU specimens, high expression of theRUNX3 gene and low expression of the ATRX gene wereassociated with an inferior outcome. The ratios of RUNX3-ATRX expression classified FLT3-MU cases into the fol-lowing 3 event-free survival groups: low ratios (with 70%event-free survival), intermediate ratios (with 37% event-free survival), and high ratios (with 0% event-free surviv-al) (P , .001). Therefore, GEP identified FLT3-MU–posi-tive AMLs with divergent prognoses, and the RUNX3-ATRX expression ratio should be a useful prognostic in-dicator in these AMLs.
Approximately 6% of AMLs are associated with a par-tial tandem duplication within the MLL gene (MLL-PTD);these cases do not show chromosomal rearrangements bybanding analysis and have been associated with an un-favorable prognosis.149 Discrimination of MLL-PTD (10cases) from AMLs with a normal karyotype and withoutthis aberration (30 cases) by GEP using MAs was not pos-sible because a specific GEP differentiating the MLL-PTD–positive from the MLL-PTD–negative cases has not beendefined. However, a specific GEP was found for the caseswith TMLL compared with the MLL-PTD and normal kar-yotype groups. Similarities in HOX GE pattern were foundbetween MLL-PTD and TMLL cases (HOXA7, HOXA9,HOXA4, HOXA5, and HOXA10), although HOXB2,HOXB5, HOXB6, and HOXB7 were expressed at lower lev-els in TMLL cases. These data suggest that, in TMLL andMLL-PTD–positive cases, HOX gene regulation is alteredin a common way, but the overall GEP is markedly dif-ferent between the 2 groups. Because the multilineagedysplasia (MLD)–PTD pattern cannot be well differenti-ated from that of AML of normal karyotype, these 2groups may be more closely related to each other thanMLL-PTD cases are to TMLL cases. Ross et al144 similarlyshowed in a combined pediatric data set of 130 AMLs and137 ALLs that AMLs containing MLL-PTDs failed to clus-ter with MLL chimeric fusion gene cases, suggesting a sig-nificant difference in their underlying mechanism of trans-formation.

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 513
8;21 AML
The AML1 (RUNX1-MTG8 (ETO) fusion transcriptionfactor that is generated by the 8;21 translocation is believedto deregulate the expression of genes that are crucial fornormal differentiation and proliferation of hematopoieticprogenitors, resulting in AML. Microarray analysis of ap-proximately 6500 genes in a murine progenitor cell linewith ectopic expression of AML1-MTG8 identified 32 can-didate genes that were under the downstream control ofAML1-MTG8.150 There was enhanced expression of severalgenes that are usually induced during granulocytic differ-entiation, particularly those encoding azurophil granuleproteins, including cathepsin G, MPO, and lysozyme, in-dicating that AML1-MTG8 induces partial differentiationof myeloid progenitor cells into promyelocytes in the ab-sence of the usual differentiation signals, while it inhibitsterminal differentiation into mature granulocytes. There-fore, AML1-MTG8 may play a crucial role in defining aunique cytologic type with abnormal maturation that ischaracteristic of 8;21 AML.
M1 AML and APL
Gene expression profiling of 21 AMLs using cDNAMAs, focusing on M1 AML (without recurring cytogeneticabnormality) and APL identified 24 strong-feature genesthat distinguish M1 AML and 33 strong-feature genes thatdistinguish APL from other AMLs.151 A direct comparisonbetween M1 AML and APL led to the selection of 13strong-feature separating genes, including some that areknown to be related to leukemogenesis and cell differen-tiation. RIN1, a gene in the ras pathway, was up-regulatedin APL. Growth factor–binding protein 2 was down-reg-ulated in M1 AML, and Huntington gene was up-regu-lated in M1 AML. Other genes included syndecan 4 (over-expressed in APL), IL2RB (overexpressed in APL), folatereceptor b (down-regulated in APL), rearranged immu-noglobulin l light chain (overexpressed in M1 AML, likelyreflecting immaturity of the leukemic cells with bilinealgenotypes of myeloid and lymphoid blasts), Fc receptorIIC precursor or CD32 that is normally expressed inmonocytes and neutrophils (low expression in M1 AML),insulin-like growth factor binding protein 2 (overex-pressed in APL), and MPO (overexpressed in APL), whichare all involved in cell differentiation. Overexpression ofMPO in APL compared with M1 AML is consistent withthe cytochemical findings. In addition, HC and multidi-mensional scaling analysis revealed 3 main clusters wheresamples from patients with M1 AML, APL, and the othersare clustered together, except for 1 M2 that was clusteredwith APL and 1 M0 that was clustered with M1 AML(suggesting that these patients are in transition betweensubtypes).
Acute Promyelocytic Leukemia
Gene expression profiling of APL has identified severalgenes that are strongly increased in the hypogranular var-iant of APL (M3v) and are decreased in classic APL(M3).152 Most genes were involved in cytoskeleton orga-nization, cell adhesion, and migration, as well as in signaltransduction and cell cycle control, and were differentiallyexpressed during cell maturation.
Gene expression profiling using cDNA MAs (12 288genes) of the human APL cell line NB4 during all-transretinoic acid (ATRA)–induced differentiation (after 12, 24,
48, 72, and 96 hours of ATRA exposure) identified 168 up-regulated and more than 179 down-regulated genes.153
Many of the altered genes encode products that partici-pate in signaling pathways, cell differentiation, pro-grammed cell death, transcription regulation, and pro-duction of cytokines and chemokines. CD52 and proteinkinase A regulatory subunit a (PKAA) genes, whose prod-ucts are being used as therapeutic targets for certain hu-man neoplasias in ongoing clinical trials, were among thegenes that were observed to be markedly up-regulated af-ter ATRA treatment. The finding of up-regulation ofPKAA expression by ATRA supports the strategy that acombination of ATRA with cyclic adenosine monophos-phate analogues synergistically induces APL cell differ-entiation and possibly reduces the ATRA-induced adverseeffects and the development of resistance to ATRA ther-apy. The induced up-regulation of CD52 antigen expres-sion in APL cells could provide a new target for an effec-tive regimen of a combination of ATRA and anti-CD52antibodies for the treatment of this disease.
M5 AMLAn analysis of the cytogenetic and molecular genetics
in M5a and M5b AML (126 cases) revealed significant dif-ferences, which have been refined by GE analyses of 10M5a and 12 M5b AMLs.154,155 Irrespective of the presenceof 11q23 aberrations and of FLT3-LM status, both groupswere delineated with 100% accuracy based on the expres-sion status of only 2 genes (HLX1 and PPP1R14B) that aredifferentially expressed during monocytic differentiation.Additional genes that discriminated M5a and M5b AMLwere APOC2, which was markedly enhanced in the pro-cess of differentiation into macrophage-like cells, andRGS2, which may play a role in leukemogenesis. TheHOXB family members (HOXB2, HOXB5, and HOXB6)were expressed in M5/11q23-negative AML cases but notat all or at low levels in M5/11q23-positive AML cases.
M7 AML Versus Transient Myeloproliferative DisorderAn analysis of transient leukemia and acute megakar-
yoblastic leukemia samples from patients with Down syn-drome using cDNA MAs showed that these samples par-tition separately by cluster analysis.156 Acute megakaryo-blastic leukemias had substantial increases in apolipopro-tein C-I, transporter 1, myosin alkali light-chain 4, andspermidine/spermine N-acetyltransferase, compared withtransient leukemias. Transient leukemia and acute mega-karyoblastic leukemia have distinct GEP, which providesthe bases for studies of the different mechanisms under-lying the resolution of transient leukemia or its progres-sion to acute megakaryoblastic leukemia.
Therapy-Related AMLDistinct subtypes of therapy-related AML have been
identified by analysis of CD34-positive hematopoietic pro-genitor cells using MAs.157 Gene expression profiling thatis typical of arrested differentiation in early progenitorcells has been commonly detected. Cases with a 5/del 5qhad higher expression of genes that were involved in cellcycle control (CCNA2, CCNE2, and CDC2), checkpoints(BUB1), or growth (MYC) and a loss of expression of thegene that encodes interferon consensus sequence–bindingprotein. Another subgroup with a distinct GEP clusteredthe cases with heterogeneous karyotypes, including thosewith loss of chromosome 7, normal karyotypes, and 3;3 or

514 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
3;21. Despite cytogenetic heterogeneity, this group of pa-tients had similar GEP, which was characterized by thedown-regulation of transcription factors that are involvedin early hematopoiesis (TAL1, GATA1, and EKLF) and theoverexpression of proteins that are involved in signaltransduction in myeloid cells (FLT3) and cell survival (bcl-2). These results suggest that GEP may define novel bio-logic groups of therapy-related AML that are not preciselyrelated to karyotype that may benefit from a commontherapeutic approach. In addition, markedly elevatedmRNA expression of the transcription factor EVI1, whichencodes a chimeric transcription factor that results fromt(3;21)(q26;q22) that is seen in therapy-related myelodys-plasia and AML, predicts poor survival.158
De Novo AML Versus AML Arising inMyelodysplastic Syndrome
Gene expression signatures have also been identifiedthat distinguish between de novo AML and AML arisingsecondarily from myelodysplastic syndrome (MDS).159 Pu-rified stem cells from a training set of 20 BM aspiratesfrom patients were used to identify the 57-gene classifiermodel based on 12 625 genes, which on leave-one-outcross-validation segregated the samples with 85% accu-racy.
A later study used HD oligonucleotide MAs (.12 000probe sets) to analyze the subcategories of de novo AML-MLD, MDS-related AML, and therapy-related AML bypurifying the AC133-positive hematopoietic stem cell–likefractions from the BM samples with de novo AML withoutdysplasia (15 cases), AML-MLD (11 cases), MDS-relatedAML (11 cases), and therapy-related AML (2 cases).160 Thestudy found 56 genes that significantly contrasted de novoAML-MLD and MDS-related AML. The study identifiedmany genes whose expression was specific to these vari-ous subcategories of AML. The gene for platelet factor 4was preferentially expressed in de novo AML-MLD. How-ever, although these 56 genes were able to identify a clus-ter containing only MDS-related AML, the other largecluster containing most of the de novo AML-MLD alsocontained some MDS-related AMLs.
Using the correspondence analysis and 3-dimensionalprojection strategy, the study visualized the independent,yet partially overlapping, nature of current AML subcat-egories on the basis of their transcriptones.160 De novoAML-MLD cases were more clearly delineated from MDS-related AMLs using this strategy. Also, de novo AMLwithout dysplasia was distinguished from MDS-relatedAML in most cases. The gene for lysosomal-associatedmultispanning membrane protein 5 (LAPTM5) was pref-erentially activated in MDS-related AML but was sup-pressed in AML without dysplasia and in AML-MLD.Nevertheless, even this strategy failed to accurately delin-eate AML without dysplasia from de novo AML-MLD.
Prediction of Prognosis in AMLPrediction of outcome is often associated with the cy-
togenetic and molecular findings that have already beendiscussed. However, the following additional prognosticinformation is provided by GEP.
Golub et al90 examined the most highly correlated genesfor potential biologic significance in AML and determinedfor the first time that the homeobox gene HOXA9 (over-expressed in patients with treatment failure) was the sin-gle most highly correlated gene among 6817 genes.
HOXA9 is rearranged by t(7;11)(p15;p15) in a rare subsetof AMLs. IHOXA9 expression was described as being up-regulated in AML with a complex aberrant karyotype andin AML with MLL.140,149 Furthermore, HOXA9 overexpres-sion was shown to transform myeloid cells in vitro and tocause leukemia in animal models.
Gene expression profiling using MAs was retrospec-tively performed to predict clinical outcome in 54 pedi-atric AMLs.134 By comparing 9 patients with a good prog-nosis with 9 patients with a bad prognosis, a prognosticset of 35 genes (including cell cycle control and apoptosis-related genes) was identified that were not correlated toknown cytogenetic abnormalities or to the morphologicFAB classification. When this set of genes was applied tothe analysis of the remaining patients with intermediaterisk, it allowed classification of the patients into 2 groups(good vs bad prognosis) that accurately reflected the pa-tients’ outcomes. This prognostic GE signature that wasfound in pediatric AML awaits validation in independentstudies.
Microarray technology has also been useful in deter-mining the chemosensitivity of AMLs. Okutsu and col-leagues161 analyzed 78 AMLs and derived 28 genes withdifferent expression levels in good responders to chemo-therapy versus poor responders to chemotherapy thatwere used to elaborate a ‘‘drug response score.’’ This setof genes predicted clinical response in 85% of the 20 casesanalyzed.
Prediction of clinical outcome from GEP using nonlin-ear system identification (‘‘black box’’ approach) has alsobeen described.162 This approach predicted the long-termtreatment response using the data of Golub et al.90 Geneexpression profiling that was taken at the time of AMLdiagnosis contained information that was predictive of theeventual response to chemotherapy. Gene expression pro-filing was predictive even when the genes did not havelarge differences in expression levels between the clas-ses.162
An abnormal expression profile of the bcl-X gene hasalso been associated with recurrence in AML.163 The bcl-X gene product exists in 2 forms (bcl-XL and bcl-XS). bcl-XL inhibits apoptosis, whereas bcl-XS counters the effectsof bcl-XL and bcl-2. Mononuclear BM cells from 50 AMLsat diagnosis and at relapse were obtained. The bcl-XL tran-script was detected in all patients at both stages, but thebcl-XS transcript was not detected in 6 cases at either stageand was not detected in 7 other cases at relapse. Relapse-free survival (P 5 .04) and OS (P 5 .02) of the bcl-XS–negative group were significantly shorter than those of thebcl-XS–positive group. A examination of the expressionprofile of the bcl-X gene could predict the chemotherapeu-tic resistance and the prognosis of patients with refractoryAML.
Using a cDNA MA, 12 differentially expressed genes(one of which was sorcin) were identified in a multidrug-resistant AML cell line.164 The expression of sorcin wasmeasured in leukemic blasts of 65 AMLs by RT-PCR. Sor-cin overexpression in AMLs was correlated with MDR1expression (P , .001) and was associated with a poor clin-ical outcome, with the CCR rate in sorcin-positive AMLsbeing significantly low (P , .001). The combination of ex-pression levels of sorcin and MDR1 was also related toclinical outcome; sorcin-negative and MDR1-negativeAMLs had the best response to induction chemotherapy.

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 515
Therefore, sorcin might be a factor that contributes to thedrug resistance of AMLs.
Gene expression profiling has also shown that NC-AMLs are a heterogeneous group.165 Using 9000-geneMAs, global HC, and supervised analysis of 55 AMLs (53were adult AMLs, including 36 NC-AMLs, trisomy 8, 15;17, 8;21, 11;19, and 7q deletion and 2 cell lines), the fol-lowing 2 subgroups of NC-AML were identified: one sub-group constituted a homogeneous normal cytogeneticscluster (‘‘pure NC-AML’’), and NC-AMLs in the othersubgroup were clustered close to the AMLs with trans-locations (‘‘translocation-like NC-AML’’). Gene expressionsignatures were also derived for patients with trisomy 8and for those with FLT3 and MLL gene duplications.Twenty-four NC-AML specimens that were evaluated forpatient outcome were analyzed, and 43 genes discrimi-nated between 2 significantly different prognostic classesof patients. Not surprisingly, the class with a poor prog-nosis contained most (8/11) of the pure NC-AMLs, where-as the translocation-like AMLs comprised the good prog-nosis class (11/13). Discriminator genes included genesthat are involved in drug resistance (TOP2B), proteintransport (MTX2 and SLC35A2), and cell signaling(MAPK1 and PRKAB2).
A comparison of AML BM samples and AML cell lineswith normal and non-AML samples revealed faulty ex-pression of genes that may contribute to the pathogenesisof AML and to therapeutic resistance.166 Five genes weresignificantly differentially expressed across the samplegroups. The migration inhibitory factor–related protein 8and 14 genes, the products of which inhibit cell migrationand induce differentiation, were the most highly ex-pressed in nonmalignant cells. The high mobility groupprotein gene (which may be associated with aggressivedisease) and genes encoding c-Myc and glutathione S-transferase p (with glutathione S-transferase p being im-plicated in chemotherapeutic resistance) were up-regulat-ed in leukemic samples and cell lines.
Gene expression profiling has also been useful in de-termining prognostic groups among NC-AMLs. Using un-supervised HC analyses of AMLs, Bullinger et al143 pos-tulated the existence of 2 novel molecular subtypes ofAML with predominantly normal karyotypes that wereassociated with significant differences in survival timesbased on a supervised constructed 133-gene predictor (P, .001). Group 1 was characterized by a high level of ex-pression of GATA2, DNMT3A, and DNMT3B and by ele-vated NOTCH1 expression and was associated with a pooroutcome. Group 2 was characterized in part by prominentGEP that was associated with granulocytic or monocyticdifferentiation and the immune response and was associ-ated with a good outcome. Genes that were associatedwith a favorable outcome included the forkhead box O1Agene (FOXO1A, also known as FKHR). Among the genesthat were associated with a poor outcome were MAP7,GUCY1A3, TCF4, and MSI2, as well as overexpression ofHOXB2, HOXB5, PBX3, HOXA4, HOXA10, and FLT3.There was no correlation between the levels of FLT3 ex-pression and the FLT3 mutational status. This finding sug-gests that increased expression of wild-type FLT3 mayfunctionally mimic mutational activation and contribute tothe pathogenesis of AML with a poor outcome.
Valk et al142 identified 16 clusters of homogeneous sig-natures in AML, some with multiple genetic or cytoge-netic abnormalities. One of the molecular signatures was
compatible with that of normal CD34-positive cells andcontained AMLs with no apparent cytogenetic markersand AMLs with a variety of known adverse cytogeneticmarkers, such as monosomies 7 and 5 and the 9;22 trans-location, and was associated with an unfavorable thera-peutic outcome.
Correlation of GEP With CD34 ExpressionGene expression profiling that was determined using
cDNA MAs and unsupervised HC of AML blasts from 25patients identified a cluster that was characterized by highGE and a high membrane-molecule level of CD34.167 Alarge proportion of patients with AML and high CD34expression showed similarities in GEP. In contrast, pa-tients with lower CD34 expression often had GEP that wassimilar to GEP of patients who were regarded as beingCD34-negative according to conventional criteria.
CHRONIC MYELOID LEUKEMIAPathogenesis and Differentiation From Normal
CounterpartsA comparison of GEP of 15 CMLs and of 7 normal do-
nors using cDNA MA analysis (5315 genes) revealed atleast a 4-fold difference in the mean expression of 263genes (148 up-regulated and 115 down-regulated) in theCMLs compared with the normal specimens.168 Differen-tially expressed genes include those that are associatedwith BCR-ABL–induced abnormalities in signal transduc-tion, gene transactivation, cell cycle control, apoptosis, ad-hesion, DNA repair, differentiation, metabolism, and ma-lignant progression.
In addition, CML blast crisis cells in PB differed fromthose in BM, indicating major changes in GEP on entranceinto the bloodstream.168 Genes exhibiting diminished ex-pression in CML blast crisis cells from PB included thoseaffecting cell cycle control (CDC25B), intracellular signal-ing (FZD2, RYK, ACVR1, and TC21), DNA metabolismand chromosome assembly (TREX1, GOLGA1, andKPNB3), adhesion (JUP), intracellular trafficking (RAB4and KPNB3), glucose metabolism (PVK2) and malignantprogression of the disease (DBY). Genes with enhancedexpression in CML blast crisis cells from PB includedthose involved in the regulation of adhesion or invasionand malignant progression of the disease (HMMG,LENG4, GSN, ELA2, CTSG, PRTN3, CEACAM8, IL8, andMMP9) and those affecting cell cycle control (CDKN3,CDKL1, and UBE2C), mitotic checkpoint and spindle as-sembly (KNSL1, BUB1, MAD2L1, and TTK ), DNA repairand synthesis (RAD54L, BRCA1, and TYMS), transcription(ZNF24 and ERG11), antimicrobial response (BPI, MPO,and AZU1), and metabolism (FAH and ALAD). Moreover,BCR-ABL modulates the expression of genes that are in-volved in the regulation of chromosome, chromatin, andDNA dynamics during S and M cell cycle phases. BCR-ABL induces protection from apoptosis in a growth factor–free environment, stimulates cell cycle control, modifiesadhesion and invasion, induces drug resistance, and con-tributes to malignant progression of the disease. The abil-ity of CML cells to recognize and respond to a pathogenicinfection may also be compromised. The treatment ofBCR-ABL–positive cells with the Abl-specific tyrosine ki-nase inhibitor STI571 (imatinib) has resulted in decreasedexpression at the mRNA and the protein levels of somebut not all of the gene products, suggesting that increasedGE is, in some cases, tyrosine kinase independent.169

516 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
In addition, a comparison of the expression profiles of3456 genes in the purified hematopoietic stem cell–likefractions that were isolated from 13 CMLs and fromhealthy volunteers by DNA MA analysis revealed thatdown-regulated expression of the gene for PIASY is as-sociated with stage progression in CML.169 PIASY is a po-tential inhibitor of STAT (signal transducer and activatorof transcription) proteins. PIAS protein activates a growthsuppressor and induces apoptosis; therefore, a decrease inits expression may allow a deregulated growth of leuke-mic blasts in the advanced stages of CML.
Pathogenesis of STI571 (Imatinib) ResistanceWhole-genome expression analysis of imatinib-sensitive
and imatinib-resistant cells that were derived from theoriginal KCL22 line, using Affymetrix MA, detected dif-ferential expression of 39 genes that correlated with theimatinib-resistant phenotype.170 The resistant cells over-expressed several genes that are associated with the sup-pression of apoptosis (ETS2, CRADD, TWIST , and angio-poietin 1) or are associated with conferral of a ‘‘malig-nant’’ transformed phenotype (PEA15 and ETS2). Severaldifferentially expressed genes that correlated with resis-tance suggest the activation of alternative pathways thatmaintain viability and growth independent of Bcr-Abl ki-nase activity.
In addition, molecular analysis of the imatinib-resistantBCR-ABL–positive cell line KCL22/SR showed no muta-tions in the BCR-ABL gene and no increase in the levelsof BCR-ABL protein and P-glycoprotein.171 Furthermore,the level of phosphorylated BCR-ABL protein was sup-pressed by imatinib treatment, providing further evidencethat mechanisms that are independent of BCR-ABL sig-naling are involved in imatinib resistance. DNA MA anal-yses demonstrated that the signal transduction–relatedmolecules ras p21 protein activator and RhoA, whichcould affect ras signaling, and the surface tumor antigenL6 were up-regulated, while c-myb (a transcription factorthat is important for the proliferation of early hematopoi-etic progenitors) and activin A receptor (also known aserythroid differentiation factor) were down-regulated inKCL22/SR cells. Furthermore, imatinib treatment signifi-cantly suppressed the level of phosphorylated p44/42(which would down-regulate ras-MAP kinase signaling)in KCL22 cells but not in KCL22/SR cells, even when BCR-ABL was inhibited by imatinib. These results support thenotion that various mechanisms, including disturbance ofras mitogen–activated protein kinase signaling, are in-volved in imatinib resistance. (ras-MAP kinase signalingis involved in cellular proliferation and differentiation).Activating such alternative pathways appears to correlatewith disease progression.170
Prediction of Prognosis in CMLA comparison of GEP by DNA MA technology between
CMLs with a major deletion of the region proximal to therearranged ABL gene on 9q (which is associated with theworst prognosis) and CMLs without this deletion revealedseveral genes that were differentially expressed, most ofwhich were involved in cell adhesion and migration.172 Inparticular, proteins such as matrix metalloproteinases andintercellular adhesion molecule 1 play an important rolein cell migration, whereas proteins such as migration in-hibitory factor–related protein, a-1 protease inhibitor, andneutrophil elastase inhibitor play important roles in the
inhibition of chemotaxis and in random migration. Thesefindings may identify a subgroup of patients with CMLthat is associated with different cell properties and a poorprognosis.
Prediction of Response to Imatinib TherapyGene expression profiling has been shown to predict the
clinical effectiveness of CML to imatinib and may lead tothe achievement of ‘‘personalized therapy’’ for this dis-ease.173 An analysis using cDNA arrays representing23 040 genes in 22 samples of PB mononuclear cells frompatients who had not received chemotherapy before re-ceiving imatinib therapy alone revealed differential ex-pression of genes in responders versus nonresponders toimatinib therapy. A training set of 18 patients (16 patientsin the chronic phase, to be treated with 400 mg/d of im-atinib mesylate, and 2 patients in blast crisis, to be treatedwith 600 mg/d of imatinib mesylate) were analyzed. After5 months of treatment, patients were considered to be cy-togenetically defined imatinib responders (12 patientswith ,35% t9;22-positive cells) or nonresponders (6 pa-tients with .65% t9;22-positive cells). Seventy-nine geneswith a significant difference between imatinib respondersand nonresponders became the ‘‘molecular predictor.’’ Aprediction score was then established using 15 or 30 ofthese genes that delineated imatinib responders from non-responders and that provided 100% accurate assignmentsof the 18-member training set and a test set of 4 patients(2 patients in the chronic phase and 2 patients in the ac-celerated phase), even by unsupervised HC analysis. Apexnuclease was overexpressed in the imatinib nonrespond-ers; it has a key function in the DNA repair system thatconfers resistance to ionizing radiation and to alkylatingagents in human cell lines. Kruppel-like factor 4 was sup-pressed in the imatinib nonresponders; it is known to sup-press cell proliferation.
SUMMARYGene expression profiling of lymphomas and leukemias
aids in the diagnosis and prognostication of these diseas-es. The extrapolation of these findings to more timely, ef-ficient, and cost-effective methods, such as FC and IHC,will continue to result in better diagnostic tools to managethese diseases. At this time, there are FC and IHC appli-cations of the information that is gained from GEP in CLL(IGVH status, HTERT , and ZAP70), in other low-grade B-cell lymphomas and leukemias (cyclin D1 in MCL, annex-in A1 in HCL, and CD68 in FL), in DLBCL (GCB, ‘‘acti-vated’’ GCB pattern, and activated non-GCB pattern), andin nodular lymphocyte-predominant Hodgkin diseaseand cHL (IHC reactivity patterns of BSAP, Oct-2, andBOB.1). For practical clinical applications, GEP of B ALLand T ALL has mainly supported the findings that havebeen obtained by cytogenetic and molecular studies, in-cluding ML, t(1;19), hyperdiploidy of more than 50 chro-mosomes, t(9;22), t(12;21) in B ALL, as well as undiffer-entiated and prothymocyte stage that is associated with5q and 13q, early cortical thymocyte stages that are as-sociated with t(10;14)(q24;q11) or with t(7;10)(q35q24), latecortical thymocyte stage that is associated with recurrenttranslocations of chromosome band 1p32, HOX11L2-posi-tive GEP that is associated with a chromosome 5q abnor-mality, and MLL-ENL–positive GEP that is associated witht(11;19)(q23;p13.3) in T ALL. Likewise, using cytogeneticand molecular techniques, GEP in AML has supported the

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 517
distinction of AMLs with recurring and complex cytoge-netic abnormalities, including t(8;21)AML1-ETO, t(15;17)PML-RARA, inv(16)CBFB-MYH11, and 11q23MLL.However, a distinct GEP was identified in AMLs withFLT3-LMs, which occur in 40% of AMLs with a normalkaryotype. This finding is important because FLT3 muta-tions may be detected by molecular analysis and havebeen associated with a poor prognosis. However, GEP hasalso identified a subset of AML with FLT3 mutations thatis associated with a good outcome. Therefore, continuedextrapolation of GEP data to more practical techniques isanticipated in the management of these diseases.
References1. Haferlach T, Kohlmann A, Kern W, Hiddemann W, Schnittger S, Schoch C.
Gene expression profiling as a tool for the diagnosis of acute leukemias. SeminHematol. 2003;40:281–295.
2. Willman CL. Discovery of novel molecular classification schemes and genespredictive of outcome in leukemia. Hematol J. 2004;5(suppl 3):S138–S143.
3. Kern W, Kohlmann A, Wuchter C, et al. Correlation of protein expressionand gene expression in acute leukemia. Cytometry B Clin Cytom. 2003;55:29–36.
4. Dales JP, Plumas J, Palmerini F, et al. Correlation between apoptosis ma-croarray gene expression profiling and histopathological lymph node lesions. MolPathol. 2001;54:17–23.
5. Staal FJT, van der Burg M, Wessels LFA, et al. DNA microarrays for com-parison of gene expression profiles between diagnosis and relapse in precursor-B acute lymphoblastic leukemia: choice of technique and purification influencethe identification of potential diagnostic markers. Leukemia. 2003;17:1324–1332.
6. Wang J, Coombes KR, Highsmith WE, Keating MJ, Abruzzo LV. Differencesin gene expression between B-cell chronic lymphocytic leukemia and normal Bcells: a meta-analysis of three microarray studies. Bioinformatics. 2004;20:3166–3178.
7. Zent CS, Zhan F, Schichman SA, et al. The distinct gene expression profilesof chronic lymphocytic leukemia and multiple myeloma suggest different anti-apoptotic mechanisms but predict only some differences in phenotype. Leuk Res.2003;27:765–774.
8. Klein U, Tu Y, Stolovitzky GA, et al. Gene expression profiling of B cellchronic lymphocytic leukemia reveals a homogeneous phenotype related tomemory B cells. J Exp Med. 2001;194:1625–1638.
9. Rosenwald A, Alizadeh AA, Widhopf G, et al. Relation of gene expressionphenotype to immunoglobulin mutation genotype in B cell chronic lymphocyticleukemia. J Exp Med. 2001;194:1639–1647.
10. Damle RN, Wasil T, Fais F, et al. Ig V gene mutation status and CD38expression as novel prognostic indicators in chronic lymphocytic leukemia.Blood. 1999;94:1840–1847.
11. Hamblin TJ, Davis Z, Gardiner A, Oscier DG, Stevenson FK. VHUnmutatedIg genes are associated with a more aggressive form of chronic lymphocytic leu-kemia. Blood. 1999;94:1848–1854.
12. Oscier DG, Gardiner AC, Mould SJ, et al. Multivariate analysis of prog-nostic factors in CLL: clinical stage, IGVH gene mutational status, and loss ormutation of the p53 gene are independent prognostic factors. Blood. 2002;100:1177–1184.
13. Tchirkov A, Chaleteix C, Magnac C, et al. hTERT expression and prognosisin B-chronic lymphocytic leukemia. Ann Oncol. 2004;15:1476–1480.
14. Staudt LM. Gene expression profiling. Ann Rev Med. 2002;53:303–318.15. Orchard JA, Ibbotson RE, Davis Z, et al. ZAP-70 expression and prognosis
in chronic lymphocytic leukaemia. Lancet. 2004;363:105–111.16. Ferrer A, Ollila J, Tobin G, et al. Different gene expression in immuoglob-
ulin-mutated and immunoglobulin-unmutated forms of chronic lymphocytic leu-kemia. Cancer Genet Cytogenet. 2004;153:69–72.
17. Weistner A, Rosenwald A, Barry TS, et al. ZAP-70 expression identifies achronic lymphocytic leukemia subtype with unmutated immunoglobulin genes,inferior clinical outcome, and distinct gene expression profiles. Blood. 2003;101:4944–4951.
18. Weistner A, Staudt LM. Towards molecular diagnosis and targeted therapyof lymphoid malignancies. Semin Hematol. 2003;40:296–307.
19. Crespo M, Bosch F, Villamor N, et al. ZAP-70 expression as a surrogatefor immunoglobulin-variable-region mutations in chronic lymphocytic leukemia.N Engl J Med. 2003;348:1764–1775.
20. Calin GA, Liu CG, Sevignani C, et al. MicroRNA profiling reveals distinctsignatures in B cell chronic lymphocytic leukemias. Proc Natl Acad Sci U S A.2004;101:11755–11760.
21. Dohner H, Stilgenbauer S, Benner A, et al. Genomic aberrations and sur-vival in chronic lymphocytic leukemia. N Engl J Med. 2000;343:1910–1916.
22. Stratowa C, Loffler G, Lichter P, et al. cDNA microarray gene expressionanalysis of B-cell chronic lymphocytic leukemia proposes potential new prog-nostic markers involved in lymphocyte trafficking. Int J Cancer. 2001;91:474–480.
23. Zent CS, Chen JB, Evans R, Zhan F, Shaughnessay JD, Schichman SA. Pre-dicting disease progression in chronic lymphocytic leukaemia from gene expres-
sion profiles. In: Program and abstracts of the 43rd Annual Meeting of the Amer-ican Society of Hematology; December 7-11, 2001; Orlando, Fla. Abstract 1970.
24. Vallat L, Magdelenat H, Merle-Beral H, et al. The resistance of B-CLL cellsto DNA damage–induced apoptosis defined by DNA microarrays. Blood. 2003;101:4598–4606.
25. Rosenwald A, Chuang EY, Davis RE, et al. Fludarabine treatment of patientswith chronic lymphocytic leukemia induces a p53-dependent gene expressionresponse. Blood. 2004;104:1428–1434.
26. Rush LJ, Raval A, Funchain P, et al. Epigenetic profiling in chronic lym-phocytic leukemia reveals novel methylation targets. Cancer Res. 2004;64:2424–2433.
27. Ek S, Hogerkorp CM, Dictor M, Ehinger M, Borrebaeck CA. Mantle celllymphomas express a distinct genetic signature affecting lymphocyte traffickingand growth regulation as compared with subpopulations of normal human Bcells. Cancer Res. 2002;62:4398–4405.
28. Rosenberg CL, Motokura T, Kronenberg HM, Arnold A. Coding sequenceof the overexpressed transcript of the putative oncogene PRAD1/cyclin D1 in 2primary human tumors. Oncogene. 1993;8:519–521.
29. Pan Z, Shen Y, Du C, et al. Two newly characterized germinal center B-cell–associated genes, GCET1 and GCET2, have differential expression in normaland neoplastic B cells. Am J Pathol. 2003;163:135–144.
30. Rosenwald A, Wright G, Wiestner A, et al. The proliferation gene expres-sion signature is a quantitative integrator of oncogenic events that predicts sur-vival in mantle cell lymphoma. Cancer Cell. 2003;3:185–197.
31. Pinyol M, Cobo F, Bea S, et al. p16INK4a gene inactivation by deletions,mutations, and hypermethylation is associated with transformed and aggressivevariants of non-Hodgkin’s lymphomas. Blood. 1998;91:2977–2984.
32. Sherr CJ, McCormick F. The RB and p53 pathways in cancer. Cancer Cell.2002;2:103–112.
33. de Vos S, Krug U, Hofmann WK, et al. Cell cycle alterations in the blastoidvariant of mantle cell lymphoma (MCL-BV) as detected by gene expression pro-filing of mantle cell lymphoma (MCL) and MCL-BV. Diagn Mol Pathol. 2003;12:35–43.
34. de Vos S, Hofmann WK, Grogan TM, et al. Gene expression profiling inserial samples of transformed follicular lymphoma. Lab Invest. 2003;83:271–285.
35. Alizadeh AA, Eisen MB, Davis RE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403:503–511.
36. Husson H, Carideo EG, Neuberg D, et al. Gene expression profiling offollicular lymphoma and normal germinal center B cells using cDNA arrays.Blood. 2002;99:282–289.
37. Glas AM, Kersten J, Delahaye LJMJ, et al. Gene expression profiling infollicular lymphoma to assess clinical aggressiveness and to guide the choice oftreatment. Blood. 2005;105:301–307.
38. Dave SS, Wright G, Tan B, et al. Prediction of survival in follicular lym-phoma based on molecular features of tumor-infiltrating immune cells. N Engl JMed. 2004;351:2159–2169.
39. Farinha P, Masoudi H, Skinnider BF, et al. Analysis of multiple biomarkersshows that lymphoma-associated macrophage (LAM) content is an independentpredictor of survival in follicular lymphoma (FL). Blood. 2005;106:2169–2174.
40. Bohen SP, Warnke R, Botstein D, Brown PO, Levy R. Predicting rituximabresponse of follicular lymphoma using cDNA microarray analysis. In: Programand abstracts of the 8th International Conference on Malignant Melanoma; June12–15, 2002; Lugano, Switzerland. Abstract 041.
41. Bohen SP, Troyanskaya OG, Alter O, et al. Variation in gene expressionpatterns in follicular lymphoma and the response to rituximab. Proc Natl AcadSci U S A. 2003;100:1926–1930.
42. Liu H, Ruskon-Fourmestraux A, Lavergne-Slove A, et al. Resistance of t(11;18) positive gastric mucosa-associated lymphoid tissue lymphoma to Helicobac-ter pylori eradication therapy. Lancet. 2001;357:39–40.
43. Starostik P, Patzner J, Greiner A. et al. Gastric marginal zone B-cell lym-phomas of MALT type develop along 2 distinct pathogenetic pathways. Blood.2002;99:3–9.
44. Basso K, Liso A, Tiacci E, et al. Gene expression profiling of hairy cellleukemia reveals a phenotype related to memory B cells with altered expressionof chemokine and adhesion receptors. J Exp Med. 2004;199:59–68.
45. Falini B, Tiacci E, Liso A, et al. Simple diagnostic assay for hairy cell leu-kaemia by immunocytochemical detection of annexin 1 (ANXA1) [published cor-rection appears in Lancet. 2004;363:2194]. Lancet. 2004;363:1869–1870.
46. Schmechel SC, LeVasseur RJ, Yang KH, Koehler KM, Kussick SJ, Sabath DE.Identification of genes whose expression patterns differ in benign lymphoid tissueand follicular, mantle cell, and small lymphocytic lymphoma. Leukemia. 2004;18:841–855.
47. Thieblemont C, Chettab K, Felman P, et al. Identification and validation of7 genes as potential markers for the differential diagnosis of indolent non-follic-ular B-cell lymphomas by cDNA arrays analysis. Leukemia. 2002;16:2326–2329.
48. Thieblemont C, Nasser V, Felman P, et al. Small lymphocytic lymphoma,marginal zone B-cell lymphoma, and mantle cell lymphoma exhibit distinct gene-expression profiles allowing molecular diagnosis. Blood. 2004;103:2727–2737.
49. Lossos IS, Alizadeh AA, Diehn M, et al. Transformation of follicular lym-phoma to diffuse large-cell lymphoma: alternative patterns with increased or de-creased expression of c-myc and its regulated genes. Proc Natl Acad Sci U S A.2002;99:8886–8891.
50. Levene AP, Morgan GJ, Davies FE. The use of genetic microarray analysis

518 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
to classify and predict prognosis in haematological malignancies. Clin Lab Hae-matol. 2003;25:209–220.
51. Huang JZ, Sanger WG, Greiner TC, et al. The t(14;18) defines a uniquesubset of diffuse large B-cell lymphoma with a germinal center B-cell gene ex-pression profile. Blood. 2002;99:2285–2290.
52. Ando T, Suguro M, Hanai T, Kobayashi T, Honda H, Seto M. Fuzzy neuralnetwork applied to gene expression profiling for predicting the prognosis of dif-fuse large B-cell lymphoma. Jpn J Cancer Res. 2002;93:1207–1212.
53. Rosenwald A, Wright G, Chan WC, et al; Lymphoma/Leukemia MolecularProfiling Project. The use of molecular profiling to predict survival after chemo-therapy for diffuse large-B-cell lymphoma. N Engl J Med. 2002;346:1937–1947.
54. Wright G, Tan B, Rosenwald A, Hurt EH, Wiestner A, Staudt LM. A geneexpression–based method to diagnose clinically distinct subgroups of diffuselarge B cell lymphoma. Proc Natl Acad Sci U S A. 2003;100:9991–9996.
55. Wang J, Delabie J, Aasheim HC, Smeland E, Myklebost O. Clustering ofthe SOM easily reveals distinct gene expression patterns: results of a reanalysisof lymphoma study. BMC Bioinformatics. 2002;3:36–44.
56. Shipp MA, Ross KN, Tamayo P, et al. Diffuse large B-cell lymphoma out-come prediction by gene-expression profiling and supervised machine learning.Nat Med. 2002;8:68–74.
57. Lossos IS, Czerwinki DK, Alizadeh AA, et al. Prediction of survival in dif-fuse large-B-cell lymphoma based on the expression of 6 genes. N Engl J Med.2004;350:1828–1837.
58. Tzankov A, Pehrs AC, Zimpfer A, et al. Prognostic significance of CD44expression in diffuse large B cell lymphoma of activated and germinal centre Bcell–like types: a tissue microarray analysis of 90 cases. J Clin Pathol. 2003;56:747–752.
59. Linderoth J, Jerkeman M, Cavallin-Stahl E, Kvaloy S, Torlakovic E. Immu-nohistochemical expression of CD23 and CD40 may identify prognostically fa-vorable subgroups of diffuse large B-cell lymphoma: a Nordic Lymphoma GroupStudy. Clin Cancer Res. 2003;9:722–728.
60. Chang CC, McClintock S, Cleveland RP, et al. Immunohistochemical ex-pression patterns of germinal center and activation B-cell markers correlate withprognosis in diffuse large B-cell lymphoma. Am J Surg Pathol. 2004;28:464–470.
61. Iqbal J, Sanger WG, Horsman DE, et al. BCL2 translocation defines aunique tumor subset within the germinal center B-cell-like diffuse large B-celllymphoma. Am J Pathol. 2004;165(1):159–166.
62. Lam LT, Davis RE, Pierce J, et al. Small molecule inhibitors of IkB kinaseare selectively toxic for subgroups of diffuse large B-cell lymphoma defined geneexpression profiling. Clin Cancer Res. 2005;11:28–40.
63. Ghosh S, May MJ, Kopp EB. NF-kB and Rel proteins: evolutionarily con-served mediators of immune responses. Annu Rev Immunol. 1998;16:225–260.
64. Maesako Y, Uchiyama T, Ohno H. Comparison of gene expression profilesof lymphoma cell lines from transformed follicular lymphoma, Burkitt’s lympho-ma and de novo diffuse large B-cell lymphoma. Cancer Sci. 2003;94:774–781.
65. Kobayashi T, Yamaguchi M, Kim S, et al. Microarray reveals differences inboth tumors and vascular specific gene expression in de novo CD51 and CD52
diffuse large B-cell lymphomas. Cancer Res. 2003;63:60–66.66. Patrone L, Hesnon SE, Teodorovic J, et al. Gene expression patterns in AIDS
versus non–AIDS-related diffuse large B-cell lymphoma. Exp Mol Pathol. 2003;74:129–139.
67. Jenner RG, Maillard K, Cattini N, et al. Kaposi’s sarcoma–associated her-pesvirus-infected primary effusion lymphoma has a plasma cell gene expressionprofile. Proc Natl Acad Sci U S A. 2003;100:10399–10404.
68. Klein U, Gloghini A, Gaidano G, et al. Gene expression profile analysisof AIDS-related primary effusion lymphoma (PEL) suggests a plasmablastic deri-vation and identifies PEL-specific transcripts. Blood. 2003;101:4115–4121.
69. Hoefnagel JJ, Dijkman R, Basso K, et al. Distinct types of primary cuta-neous large B-cell lymphoma identified by gene expression profiling. Blood.2005;105:3671–3678.
70. Rosenwald A, Wright G, Leroy K, et al. Molecular diagnosis of primarymediastinal B cell lymphoma identifies a clinically favorable subgroup of diffuselarge B cell lymphoma related to Hodgkin lymphoma. J Exp Med. 2003;198:851–862.
71. Savage KJ, Monti S, Kutok JL, et al. The molecular signature of mediastinallarge B-cell lymphoma differs from that of other diffuse large B-cell lymphomasand shares features with classical Hodgkin lymphoma. Blood. 2003;102:3871–3879.
72. Cossman J. Gene expression analysis of single neoplastic cells and thepathogenesis of Hodgkin’s lymphoma. J Histochem Cytochem. 2001;49:799–800.
73. Garcia JF, Camacho FI, Marente M, et al. Hodgkin and Reed-Sternbergcells harbor alterations in the major tumor suppressor pathways and cell-cyclecheckpoints: analyses using tissue microarrays. Blood. 2003;101:681–689.
74. Schwering I, Brauninger A, Klein U, et al; Spanish Hodgkin LymphomaStudy Group. Loss of the B-lineage–specific gene expression program in Hodgkinand Reed-Sternberg cells of Hodgkin lymphoma. Blood. 2003;101:1505–1512.
75. Kuppers R, Klein U, Schwering I, et al. Identification of Hodgkin and Reed-Sternberg cell-specific genes by gene expression profiling. J Clin Invest. 2003;111:529–537.
76. Devilard E, Bertucci F, Trempat P, et al. Gene expression profiling definesmolecular subtypes of classical Hodgkin’s disease. Oncogene. 2002;21:3095–3102.
77. Marafioti T, Pozzobon M, Hansmann ML, et al. Expression of intracellularsignaling molecules in classical and lymphocyte predominance Hodgkin disease.Blood. 2004;103:188–193.
78. Browne P, Petrosyan K, Hernandez A, Chan JA. The B-cell transcriptionfactors BSAP, Oct-2, and BOB.1 and the pan-B-cell markers CD20, CD22, andCD79a are useful in the differential diagnosis of classic Hodgkin lymphoma. AmJ Clin Pathol. 2003;120:767–777.
79. Garcia-Cosio M, Santon A, Martin P, et al. Analysis of transcription factorOct-1, Oct-2 and BOB.1 expression using tissue arrays in classical Hodgkin’slymphoma. Mod Pathol. 2004;17:1531–1538.
80. Fillmore GC, Lin Z, Bohling SD, et al. Gene expression profiling of celllines derived from T-cell malignancies. FEBS Lett. 2002;522:183–188.
81. Martinez-Delgado B, Melendez B, Cuadros M, et al. Expression profilingof T-cell lymphomas differentiates peripheral and lymphoblastic lymphomas anddefines survival related genes. Clin Cancer Res. 2004;10:4971–4982.
82. Ohshima K, Karube K, Kawano R, et al. Classification of distinct subtypesof peripheral T-cell lymphoma unspecified, identified by chemokine and che-mokine receptor expression: analysis of prognosis. Int J Oncol. 2004;25:605–613.
83. Kari L, Loboda A, Nebozhyn, et al. Classification and prediction of survivalin patients with the leukemic phase of cutaneous T cell lymphoma. J Exp Med.2003;197:1477–1488.
84. Kohno T, Moriuchi R, Katamine S, Yamada Y, Tomonaga M, Matsuyama T.Identification of genes associated with the progression of adult T cell leukemia(ATL). Jpn J Cancer Res. 2000;91:1103–1110.
85. Tsukasaki K, Tanosaki S, DeVos S, et al. Identifying progression-associatedgenes in adult T-cell leukemia/lymphoma by using oligonucleotide microarrays.Int J Cancer. 2004;109:875–881.
86. Daibata M, Matsuo Y, Machida H, Taguchi T, Ohtsuki Y, Taguchi H. Dif-ferential gene-expression profiling in the leukemia cell lines derived from indolentand aggressive phases of CD561 T-cell large granular lymphocyte leukemia. Int JCancer. 2004;108:845–851.
87. Choi YL, Makishima H, Ohashi J, et al. DNA microarray analysis of naturalkiller cell–type lymphoproliferative disease of granular lymphocytes with purifiedCD32 CD561 fractions. Leukemia. 2004;18:556–565.
88. Thorns C, Gaiser T, Lange K, Merz H, Feller AC. cDNA arrays: gene ex-pression profiles of Hodgkin’s disease and anaplastic large cell lymphoma celllines. Pathol Int. 2002;52:578–585.
89. Nishikori M, Maesako Y, Ueda C, Kurata M, Uchiyama T, Ohno H. High-level expression of BCL3 differentiates t(2;5)(p23;q35)-positive anaplastic largecell lymphoma from Hodgkin disease. Blood. 2003;101:2789–2796.
90. Golub TR, Slonim DK, Tamayo P, et al. Molecular classification of cancer:class discovery and class prediction by gene expression monitoring. Science.1999;286:531–537.
91. Moos PJ, Raetz EA, Carlson MA, et al. Identification of gene expressionprofiles that segregate patients with childhood leukemia. Clin Cancer Res. 2002;8:3118–3130.
92. Kees UR, Ford J, Watson M, Murch A, Ringner M, Walker RL, Meltzer P.Gene expression profiles in a panel of childhood leukemia cell lines mirror crit-ical features of the disease. Mol Cancer Ther. 2003;2:671–677.
93. Nakao M, Yokota S, Iwai T, et al. Internal tandem duplication of the FLT3gene found in acute myeloid leukemia. Leukemia. 1996;10:1911–1918.
94. Tse KF, Mukherjee G, Small D. Constitutive activation of FLT3 stimulatesmultiple intracellular signal transducers and results in transformation. Leukemia.2000;14:1766–1776.
95. Zhao M, Kiyoi H, Yamamoto Y, et al. In vivo treatment of mutant FLT3-transformed murine leukemia with a tyrosine kinase inhibitor. Leukemia. 2000;14:374–378.
96. Armstrong SA, Staunton JE, Silverman LB, et al. MLL translocations specifya distinct gene expression profile that distinguishes a unique leukemia. Nat Gen-et. 2002;30:41–47.
97. Foa R, Vitale A. Towards an integrated classification of adult acute lym-phoblastic leukemia. Rev Clin Exp Hematol. 2002;6:181–202.
98. Rozovskaia T, Feinstein E, Mor O, et al. Upregulation of Meis1 and HoxA9in acute lymphocytic leukemias with the t(4 : 11) abnormality. Oncogene. 2001;20874–20878.
99. Kohlmann A, Schoch C, Schnittger S, et al. Molecular characterization ofacute leukemias by use of microarray technology. Genes Chromosomes Cancer.2003;37:396–405.
100. Yeoh EJ, Ross ME, Shurtleff SA, et al. Classification, subtype discovery,and prediction of outcome in pediatric acute lymphoblastic leukemia by geneexpression profiling. Cancer Cell. 2002;1:133–143.
101. Ross ME, Zhou X, Song G, et al. Classification of pediatric acute lym-phoblastic leukemia by gene expression profiling. Blood. 2003;102:2951–2959.
102. Kohlmann A, Schoch C, Schnittger S, et al. Pediatric acute lymphoblasticleukemia (ALL) gene expression signatures classify an independent cohort of adultALL patients. Leukemia. 2004;18:63–71.
103. Niini T, Vettenranta K, Hollmen J, et al. Expression of myeloid-specificgenes in childhood acute lymphoblastic leukemia: a cDNA array study. Leuke-mia. 2002;16:2213–2221.
104. Armstrong SA, Mabon ME, Silverman LB, et al. FLT3 mutations in child-hood acute lymphoblastic leukemia. Blood. 2004;103:3544–3546.
105. Taketani T, Taki T, Sugita K, et al. FLT3 mutations in the activation loopof tyrosine kinase domain are frequently found in infant ALL with MLL rearrange-ments and pediatric ALL with hyperdiploidy. Blood. 2004;103:1085–1088.
106. Zaza G, Yang W, Kager L, et al. Acute lymphoblastic leukemia with TEL-AML1 fusion has lower expression of genes involved in purine metabolism andlower de novo purine synthesis. Blood. 2004;104:1435–1441.
107. Rozovskaia T, Ravid-Amir O, Tillib S, et al. Expression profiles of acute

Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy 519
lymphoblastic and myeloblastic leukemias with ALL-1 rearrangements. Proc NatlAcad Sci U S A. 2003;100:7853–7858.
108. Yu BD, Hess JL, Homing SE, Brown GA, Korsmeyer SJ. Altered Hox ex-pression and segmental identity in Mll-mutant mice. Nature. 1995;378:505–508.
109. Hanson RD, Hess JL, Yu BD, et al. Mammalian Trithorax and Polycomb-group homologues are antagonistic regulators of homeotic development. ProcNatl Acad Sci U S A. 1999;96:14372–14377.
110. Armstrong SA, Hsieh JJ, Korsmeyer SJ. Genomic approaches to the path-ogenesis and treatment of acute lymphoblastic leukemias. Curr Opin Hematol.2002;9:339–344.
111. Ferrando AA, Thomas Look A. Gene expression profiling: will it comple-ment or replace immunophenotyping? Best Pract Res Clin Haematol. 2003;16:645–652.
112. Armstrong SA, Kung AL, Mabon ME, et al. Inhibition of FLT3 in MLL:validation of a therapeutic target identified by gene expression based classifica-tion. Cancer Cell. 2003;3:173–183.
113. Tsutsumi S, Taketani T, Nishimura K, et al. Two distinct gene expressionsignatures in pediatric acute lymphoblastic leukemia. Blood. 1995;85:2546–2552.
114. Qiu J, Gunaratne P, Peterson LE, et al. Novel potential ALL low-risk mark-ers revealed by gene expression profiling with new high-throughput SSH-CCS-PCR. Leukemia. 2003;17:1891–1900.
115. Scrideli CA, Cazzaniga G, Fazio G, et al. Gene expression profile unrav-els significant differences between childhood and adult Ph1 acute lymphoblasticleukemia. Leukemia. 2003;17:2234–2237.
116. Hofmann WK, de Vos S, Elashoff D, et al. Relation between resistance ofPhiladelphia-chromosome–positive acute lymphoblastic leukaemia to the tyro-sine kinase inhibitor STI571 and gene-expression profiles: a gene-expressionstudy. Lancet. 2002;359:481–486.
117. Hofmann WK, Komor M, Hoelzer D, Ottmann OG. Mechanisms of re-sistance to STI571 (Imatinib) in Philadelphia-chromosome positive acute lympho-blastic leukemia. Leuk Lymphoma. 2004;45:655–660.
118. Fine BM, Stanulla M, Schrappe M, et al. Gene expression patterns as-sociated with recurrent chromosomal translocations in acute lymphoblastic leu-kemia. Blood. 2004;103:1043–1049.
119. Willenbrock H, Juncker AS, Schmiegelow K, Knudsen S, Ryder LP. Pre-diction of immunophenotype, treatment response, and relapse in childhood acutelymphoblastic leukemia using DNA microarrays. Leukemia. 2004;18:1270–1277.
120. Chen JS, Coustan-Smith E, Suzuki T, et al. Identification of novel markersfor monitoring minimal residual disease in acute lymphoblastic leukemia. Blood.2001;97:2115–2120.
121. Cario G, Stanulla M, Fine BM, et al. Distinct gene expression profilesdetermine molecular treatment response in childhood acute lymphoblastic leu-kemia. Blood. 2005;105:821–826.
122. Cheok MH, Yang W, Pui CH, et al. Treatment-specific changes in geneexpression discriminate in vivo drug response in human leukemia cells. Nat Gen-et. 2003;34:85–90.
123. Holleman A, Cheok MH, den Boer ML, et al. Gene-expression patternsin drug-resistant acute lymphoblastic leukemia cells and response to treatment.N Engl J Med. 2004;351:533–542.
124. Den Boer ML, Harms DO, Pieters R, et al. Patient stratification based onprednisolone-vincristine-asparaginase resistance profiles in children with acutelymphoblastic leukemia. J Clin Oncol. 2003;21:3262–3268.
125. Edick MJ, Cheng C, Yang W, et al. Lymphoid gene expression as a pre-dictor of risk of secondary brain tumors. Genes Chromosomes Cancer. 2005;42:107–116.
126. Ferrando AA, Neuberg DS, Staunton JE, et al. Gene expression signaturesdefine novel oncogenic pathways in T cell acute lymphoblastic leukemia. CancerCell. 2002;1:75–87.
127. Ferrando AA, Look AT. Gene expression profiling in T-cell acute lympho-blastic leukemia. Semin Hematol. 2003;40:274–280.
128. Rubnitz JE, Camitta BM, Mahmoud H, et al. Childhood acute lympho-blastic leukemia with the MLL-ENL fusion and t(11;19)(q23;p13.3) translocation.J Clin Oncol. 1999;17:191–196.
129. Ferrando AA, Armstrong SA, Neuberg DS, et al. Gene expression signa-tures in MLL-rearranged T-lineage and B-precursor acute leukemias: dominanceof HOX dysregulation. Blood. 2003;102:262–268.
130. Ferrando AA, Neuberg DS, Dodge RK, et al. Prognostic importance ofTLX1 (HOX11) oncogene expression in adults with T-cell acute lymphoblasticleukaemia. Lancet. 2004;363:535–536.
131. Ballerini P, Blaise A, Brusson-Le Coniat M, et al. HOX11L2 expressiondefines a clinical subtype of pediatric T-ALL associated with poor prognosis.Blood. 2002;100(3):991–997.
132. Chiaretti S, Li X, Gentleman R, et al. Gene expression profile of adult T-cell acute lymphocytic leukemia identifies distinct subsets of patients with differ-ent response to therapy and survival. Blood. 2004;103:2771–2778.
133. Haferlach T, Kohlmann A, Dugas M, et al. Gene expression profiling isable to reproduce different phenotypes in AML as defined by the FAB classifi-cation [abstract]. Blood. 2002;100(suppl 1):195a.
134. Yagi T, Morimoto A, Eguchi M, et al. Identification of a gene expressionsignature associated with prognosis of pediatric AML. Blood. 2003;102:1849–1856.
135. Schoch C, Kohlmann A, Schnittger S, et al. Acute myeloid leukemias withreciprocal rearrangements can be distinguished by specific gene expression pro-files. Proc Natl Acad Sci U S A. 2002;99:10008–10013.
136. Kohlmann A, Dugas M, Shoch C, et al. Gene expression profiles of dis-tinct AML subtypes in comparison to normal bone marrow [abstract]. Blood.2001;98(suppl 1):91a.
137. Haferlach T, Kohlmann A, Dugas M, et al. The diagnosis of 14 specificsubtypes of leukemia is possible based on gene expression profiles: a study on263 patients with AML, CML, or CLL. In: Program and abstracts of the 44thAnnual Meeting of the American Society of Hematology; December 6–10, 2002;Philadelphia, Pa. Abstract 523.
138. van Waalwijk van Doom-Khosrovani SB, Erpelinck C, Meijer J, et al. Bial-lelic mutations in the CEBPA gene and low CEBPA expression levels as prognosticmarkers in intermediate-risk AML. Hematol J. 2003;4:31–40.
139. Preudhomme C, Sagot C, Boissel N, et al. Favorable prognostic signifi-cance of CEBPA mutations in patients with de novo acute myeloid leukemia: astudy from the Acute Leukemia French Association (ALFA). Blood. 2002;100:2717–2723.
140. Schoch C, Kern W, Kohlmann A, et al. Acute myeloid leukemia with acomplex aberrant karyotype is a distinct biological entity characterized by ge-nomic imbalances and a specific gene expression profile. Genes ChromosomesCancer. 2005;43:227–238.
141. Debernardi S, Lillington DM, Chaplin T, et al. Genome-wide analysis ofacute myeloid leukemia with normal karyotype reveals a unique pattern of ho-meobox gene expression distinct from those with translocation-mediated fusionevents. Genes Chromosomes Cancer. 2003;37:149–158.
142. Valk PJ, Verhaak RG, Beijen MA, et al. Prognostically useful gene-ex-pression profiles in acute myeloid leukemia. N Engl J Med. 2004;350:1617–1628.
143. Bullinger L, Dohner K, Bair E, et al. Use of gene-expression profiling toidentify prognostic subclasses in adult acute myeloid leukemia. N Engl J Med.2004;350:1605–1616.
144. Ross ME, Mahfouz R, Onciu M, et al. Gene expression profiling of pe-diatric acute myelogenous leukemia. Blood. 2004;104:3679–3687.
145. Gilliland DG, Griffin JD. The roles of FLT3 in hematopoiesis and leuke-mia. Blood. 2002;100:1532–1542.
146. Levis M, Small D. FLT3: ITDoes matter in leukemia. Leukemia. 2003;17:1738–1752.
147. Schnittger S, Schoch C, Dugas M, et al. Analysis of FLT3 length mutationsin 1003 patients with acute myeloid leukemia: correlation to cytogenetics, FABsubtype, and prognosis in the AMLCG study and usefulness as a marker for thedetection of minimal residual disease. Blood. 2002;100:59–66.
148. Lacayo NJ, Meshinchi S, Kinnunen P, et al. Gene expression profiles atdiagnosis in de novo childhood AML patients identify FLT3 mutations with goodclinical outcomes. Blood. 2004;104:2646–2654.
149. Schnittger S, Kohlmann A, Haferlach T, et al. Acute myeloid leukemia(AML) with partial tandem duplication of the MLL-gene (MLL-PTD) can be dis-criminated from MLL-translocations based on specific gene expression profiles[abstract]. Blood. 2002;100(suppl 1):312a.
150. Shimada H, Ichikawa H, Ohki M. Potential involvement of the AML1-MTG8 fusion protein in the granulocytic maturation characteristic of the t(8;21)acute myelogenous leukemia revealed by microarray analysis. Leukemia. 2002;16:874–885.
151. Morikawa J, Li H, Kim S, et al. Identification of signature genes by mi-croarray for acute myeloid leukemia without maturation and acute promyelocyticleukemia with t(15;17)(q22;q12)(PML/RARa). Int J Oncol. 2003;23:617–625.
152. Schmitz N, Kohlmann A, Schoch C, et al. Gene expression profiling inacute promyelocytic leukemia (APL) with t(15;17): microarray analyses and val-idation of important genes using real time PCR [abstract]. Blood. 2002;100(suppl1):312a.
153. Yang L, Zhao H, Li SW, et al. Gene expression profiling during all-transretinoic acid–induced cell differentiation of acute promyelocytic leukemia cells.J Mol Diagn. 2003;5:212–221.
154. Haferlach T, Schoch C, Schnittger S, Kern W, Loffler H, Hiddemann W.Distinct genetic patterns can be identified in acute monoblastic and acute mono-cytic leukaemia (FAB AML M5a and M5b): a study of 124 patients. Br J Haematol.2002;118:426–431.
155. Haferlach T, Schnittger S, Kohlmann A, et al. Genetic profiling in acutemonoblastic versus acute monocytic leukemia: a gene expression study on 22patients [abstract]. Blood. 2002;100(suppl 1):139a.
156. Lightfoot J, Hitzler JK, Zipursky A, Albert M, Macgregor PF. Distinct genesignatures of transient and acute megakaryoblastic leukemia in Down syndrome.Leukemia. 2004;18:1617–1623.
157. Qian Z, Fernald AA, Godley LA, et al. Expression profiling of CD341
hematopoietic stem/progenitor cells reveals distinct subtypes of therapy-relatedacute myeloid leukemia. Proc Natl Acad Sci U S A. 2002;99:14925–14930.
158. van Waalvijk van Doom-Khosrovani SB, Erpelinck C, van Putten WL, etal. High EVI1 expression predicts poor survival in acute myeloid leukemia: astudy of 319 de novo AML patients. Blood. 2003;101:837–845.
159. Oshima Y, Ueda M, Yamashita Y, et al. DNA microarray analysis of he-matopoietic stem cell-like fractions from individuals with the M2 subtype of acutemyeloid leukemia. Leukemia. 2003;17:1990–1997.
160. Tsutsumi C, Ueda M, Miyazaki Y, et al. DNA microarray analysis of dys-plastic morphology associated with acute myeloid leukemia. Exp Hematol. 2004;32:828–835.
161. Okutsu J, Tsunoda T, Kaneta Y, et al. Prediction of chemosensitivity forpatients with acute myeloid leukemia, according to expression levels of 28 genesselected by genome-wide complementary DNA microarray analysis. Mol CancerTher. 2002;1:1035–1042.

520 Arch Pathol Lab Med—Vol 130, April 2006 Gene Expression Profiling in Lymphoma and Leukemia—Dunphy
Cherie Hilborn Dunphy, MD
Cherie Hilborn Dunphy, MD, is associate professor of pathologyand laboratory medicine at The University of North Carolina atChapel Hill. She has been immersed in the field of diagnostic he-matopathology for the past 15 years of her career. She joined SaintLouis University, St Louis, Mo, in 1991, as an assistant professor andspent a decade there, establishing and developing the division ofhematopathology and the hematopathology fellowship at that insti-tution. She was recruited to The University of North Carolina atChapel Hill approximately 5 years ago as director of hematopathol-ogy and the hematopathology fellowship. The main goals and areasof interest of her research involve the applications of techniques (flowcytometry, immunohistochemistry, and molecular and cytogeneticprobes) to diagnostic hematopathology, and she has published exten-sively in these areas. She also codirects an annual American Societyfor Clinical Pathology long course entitled ‘‘Contemporary Hemato-lymphoid Diagnostic Pathways: State-of-the-Art Parameters, Powersand Pitfalls.’’ She is an associate editor and section editor for Archivesof Pathology & Laboratory Medicine.
162. Korenberg MJ. Prediction of treatment response using gene expressionprofiles. J Proteome Res. 2002;1:55–61.
163. Yamaguchi H, Inokuchi K, Dan K. The study for loss of bcl-xs expressionas a prognostic factor in acute myeloid leukemia. Leuk Res. 2002;26:1119–1123.
164. Tan Y, Li G, Zhao C, et al. Expression of sorcin predicts poor outcome inacute myeloid leukemia. Leuk Res. 2003;27:125–131.
165. Vey N, Mozziconacci MJ, Groulet-Martinec A, et al. Identification of newclasses among acute myelogenous leukaemias with normal karyotype using geneexpression profiling. Oncogene. 2004;23:9381–9391.
166. Court EL, Smith MA, Avent ND, et al. DNA microarray screening of dif-ferential gene expression in bone marrow samples from AML, non-AML patientsand AML cell lines. Leuk Res. 2004;28:743–753.
167. Oyan AM, Bo TH, Jonassen I, et al. CD34 expression in native humanacute myelogenous leukemia blasts: differences in CD34 membrane moleculeexpression are associated with different gene expression profiles. Cytometry BClin Cytom. 2005;64(1):18–27.
168. Nowicki MO, Pawlowski P, Fischer T, Hess G, Pawlowski T, Skorski T.
Chronic myelogenous leukemia molecular signature. Oncogene. 2003;22:3952–3963.
169. Ohmine K, Ota J, Ueda M, et al. Characterization of stage progressionin chronic myeloid leukemia by DNA microarray with purified hematopoieticstem cells. Oncogene. 2001;20:8249–8257.
170. Ohmine K, Nagai T, Tarumoto T, et al. Analysis of gene expression profilesin an imatinib-resistant cell line, KCL22/SR. Stem Cells. 2003;21:315–321.
171. Ohno R, Nakamura Y. Prediction of response to imatinib by cDNA mi-croarray analysis. Semin Hematol. 2003;40:42–49.
172. Cohen N, Rozenfeld-Granot G, Hardan I, et al. Subgroup of patients withPhiladelphia-positive chronic myelogenous leukemia characterized by a deletionof 9q proximal to ABL gene: expression profiling, resistance to interferon therapy,and poor prognosis. Cancer Genet Cytogenet. 2001;128:114–119.
173. Kaneta Y, Kagami Y, Katagiri T, et al. Prediction of sensitivity to ST1571among chronic myeloid leukemia patients by genome-wide cDNA microarrayanalysis. Jpn J Cancer Res. 2002;93:849–856.