Embed Size (px)
Citation preview

DEFENSE HEALTH CARE Plans Needed to Ensure Implementation of Required Elements for TRICARE’s Managed Care Support Contracts Accessible Version
Report to Congressional Committees
February 2020
GAO-20-197
United States Government Accountability Office

______________________________________ United States Government Accountability Office
February 2020
DEFENSE HEALTH CARE Plans Needed to Ensure Implementation of Required Elements for TRICARE’s Managed Care Support Contracts
What GAO Found The Department of Defense (DOD) made selective changes to its TRICARE managed care support contracts and acquisition process from the third generation of contracts (T-3) to the fourth generation (T-2017) of contracts. According to DOD officials, the contracts are generally the same, and changes were made to clarify or streamline TRICARE requirements and administrative processes. Officials told GAO they prioritized the continuation of beneficiary services, rather than implement significant contract changes that could potentially be disruptive. Some of the T-2017 changes include a reduction from three to two contract regions and a different method for paying the contractors.
GAO found that DOD has partially implemented six of the 13 elements required by the National Defense Authorization Act for Fiscal Year 2017 (NDAA 2017), in its T-2017 contracts. DOD leadership explained that they decided to implement each of the 13 elements separately rather than by developing a single strategy that addressed all of the elements. DOD officials explained that some of the 13 elements will be implemented through modifications to the T-2017 contracts, while others will be addressed in the fifth generation of managed care support contracts (T-5), which are expected to be awarded in 2021. While DOD has taken steps to begin implementing some of the required elements, GAO found that DOD lacks plans with specific time frames and actions needed to fully implement all of the elements. As a result, it is unclear exactly how and when all 13 elements will be implemented.
The National Defense Authorization Act for Fiscal Year 2017 (NDAA 2017) Section 705(c) Elements Implemented in the T-2017 Contracts, as of January 2020
Why GAO Did This Study In fiscal year 2018, DOD provided health care services to more than 9 million eligible beneficiaries through TRICARE, its regionally structured health care program. In each of its two regions (East and West), DOD uses contractors to manage health care delivery through civilian providers. The NDAA 2017 required a number of changes to the TRICARE program through its contracts. Specifically, it required DOD to implement a strategy with 13 specific elements—related to provider networks, telehealth services, and referrals, among other areas—for its contracts.
The NDAA 2017 and the accompanying Senate Report 114-255 included provisions for GAO to examine DOD’s managed care support contract acquisition process and requirements. This report (1) describes changes DOD made to its TRICARE contracts and acquisition process between its T-3 and T-2017 contracts and (2) examines the extent to which DOD implemented the 13 elements as required by the NDAA 2017, among other things. GAO reviewed and analyzed relevant federal statutes, T-3 and T-2017 planning and contracting documents, and interviewed DOD officials and TRICARE contractors.
What GAO Recommends
GAO recommends that DOD develop and implement plans with time frames and specific actions needed for all 13 required elements in the TRICARE contracts. DOD concurred with GAO’s recommendation and noted its plans to address each of the required elements in the T-5 contracts.
View GAO-20-197. For more information, contact Sharon Silas at (202) 512-7114 or [email protected] or William T. Woods at (202) 512-4841 or [email protected].
Highlights of GAO-20-197, a report to congressional committees

Page i GAO-20-197 TRICARE Acquisitions
Contents Letter 1
Background 5 DHA Made Selective Changes between the T-3 and T-2017
Contracts; Some Changes Are Consistent with Provisions and Themes in Prior NDAA Legislation 12
DHA Has Implemented Two Value-Based Incentive Pilots; Other Pilots Are Planned 16
DHA Has Partially Implemented Six of 13 Required Elements, but It Is Unclear When Implementation of All Elements Will Be Complete 17
Conclusions 22 Recommendation for Executive Action 23 Agency Comments 23
Appendix I: Comments from the Department of Defense 26
Agency Comment Letter 31
Appendix II: GAO Contacts and Staff Acknowledgments 36
GAO Contacts 36 Staff Acknowledgments 36
Tables
Table 1: The National Defense Authorization Act for Fiscal Year 2017 (NDAA 2017), Section 705 (c)(5) and (c)(6) Elements 11
Table 2: Status of DHA’s Efforts to Address the Specific Elements Outlined in Section 705(c)(5) of NDAA 2017, as of January 2020 18
Table 3: Status of DHA’s Efforts to Address the Specific Elements Outlined in Section 705(c)(6) of NDAA 2017, as of January 2020 21

Page ii GAO-20-197 TRICARE Acquisitions
Figures
Figure 1: Timeline of Key Events Related to the Defense Health Agency’s (DHA) T-2017 Contracts 8
Figure 2: Consolidation of TRICARE Contract Regions from T-3 to T-2017 13
Abbreviations DHA Defense Health Agency DOD Department of Defense NDAA 2017 National Defense Authorization Act for Fiscal Year 2017 PCM primary care manager RFP Request for Proposals
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.

Page 1 GAO-20-197 TRICARE Acquisitions
441 G St. N.W.Washington, DC 20548
Letter
February 7, 2020
The Honorable James M. Inhofe Chairman The Honorable Jack Reed Ranking Member Committee on Armed Services United States Senate
The Honorable Adam Smith Chairman The Honorable Mac Thornberry Ranking Member Committee on Armed Services House of Representatives
In fiscal year 2018, the Department of Defense (DOD) offered health care services to more than 9 million eligible beneficiaries worldwide through TRICARE, its regionally structured health care program.1 Beneficiaries may obtain health care services through DOD’s direct care system of military hospitals and clinics—referred to as military treatment facilities—or from its purchased care system of civilian providers. In each of its TRICARE regions, DOD contracts with private sector companies—referred to as managed care support contractors—to develop and maintain networks of civilian providers and perform other customer service functions, such as processing claims, enrolling beneficiaries, and assisting beneficiaries with finding providers. In fiscal year 2018, purchased care accounted for about 54 percent of the total costs for health care services delivered to TRICARE beneficiaries.2
Within DOD, the Defense Health Agency (DHA) administers the TRICARE program, which includes awarding and overseeing the managed care support contracts (contracts) and setting policy for both the 1Eligible beneficiaries include active duty servicemembers and their dependents, medically eligible National Guard and Reserve members and their dependents, and retirees and their dependents and survivors, among others. Active duty personnel include Reserve component members on active duty for at least 30 days. 2Defense Health Agency, Evaluation of the TRICARE Program: Fiscal Year 2019 Report to Congress (February 28, 2019).

Letter
Page 2 GAO-20-197 TRICARE Acquisitions
direct and purchased care systems, among other responsibilities. In July 2016, DHA awarded its fourth generation of TRICARE contracts, referred to as the T-2017 contracts, to succeed its third generation of contracts, referred to as the T-3 contracts.
The National Defense Authorization Act for Fiscal Year 2017 (NDAA 2017), enacted in December 2016, required a number of changes to the TRICARE program through its contracts.3 Specifically, it required DOD to develop and implement value-based incentive programs that typically reward providers with additional payments for improved performance based on certain quality and efficiency metrics.4 In addition, the act directed DOD to develop and implement a strategy—by January 1, 2018—for its TRICARE contracts that includes 13 specific elements related to provider networks, telehealth services, and referrals, among other areas.5 These elements are intended to improve access to care, health outcomes, quality of care, beneficiaries’ experience, as well as lower costs to the department. The NDAA 2017 required DOD to modify its TRICARE contracts to ensure consistency with the required strategy providing for the 13 specific elements.6
The NDAA 2017 and the accompanying Senate Report 114-255 also included provisions for us to examine issues related to DHA’s managed care support contract acquisition process and requirements.7 In this report, we
1. describe changes DHA made to its TRICARE contracts and acquisition process between its T-3 and T-2017 contracts,
2. examine the extent to which DHA implemented value-based incentive programs as required by the NDAA 2017, and
3. examine the extent to which DHA implemented the 13 elements as required by the NDAA 2017.
3Pub. L. No. 114-328, 130 Stat. 2000 (2016). 4Pub. L. No. 114-328, § 705(a), 130 Stat. 2000, 2201-2202 (2016). 5Pub. L. No. 114-328, § 705(c)(1), (5), (6), 130 Stat. 2000, 2202-2204 (2016). 6Pub. L. No. 114-328, § 705(c)(2)(B), 130 Stat. 2000, 2202-2203 (2016). 7S. Rep. No. 114-255, at 199 (May 18, 2016).

Letter
Page 3 GAO-20-197 TRICARE Acquisitions
To describe changes DHA made to its TRICARE contracts and acquisition process between its T-3 and T-2017 contracts, we reviewed the T-3 and T-2017 contract documents as well as acquisition planning documents, such as the T-3 and T-2017 Acquisition Strategy and the Acquisition Plan.8 We interviewed TRICARE acquisition officials and representatives from the two T-2017 managed care support contractors—Humana Government Business and Health Net Federal Services—about the process to award the T-2017 contracts and any changes between the T-3 and T-2017 contracts. We compared relevant contract changes provided by DHA that may be consistent with certain provisions in section 705 of the NDAA 2017. These provisions are related to improving access to care, health outcomes, health care quality, experience of care for covered beneficiaries, and lowering health care costs. In addition, we identified statutory acquisition themes pursued by Congress over the last 5 years to improve the way federal agencies acquire goods and services. Specifically, we reviewed the NDAAs for fiscal years 2015 through 2019 and identified common themes aimed at improving DOD and federal contracting and acquisition practices.9 We determined that three of these acquisition themes were relevant to the TRICARE program, including (1) following commercial best practices, (2) promoting competition, and (3) focusing on value. We then identified T-2017 contract changes that incorporated or were consistent with these themes.10
To examine the extent to which DHA implemented value-based incentive programs as required by the NDAA 2017, we reviewed the provisions of section 705(a) of the NDAA 2017, DHA’s January 2018 report to Congress on its efforts to implement a value-based pilot program, and specific sections of the 2015 edition of the TRICARE Operations Manual 8The Acquisition Strategy and the Acquisition Plan are documents used to guide the TRICARE program’s acquisition process. The Acquisition Strategy documents the program’s programmatic goals and identifies the acquisition approach. The Acquisition Plan documents the specific actions necessary to execute the approach outlined in the approved acquisition strategy. Although we reviewed DHA’s acquisition process, we did not assess DHA’s evaluation of contract proposals. 9Pub. L. No. 113-291, tit. VIII, 128 Stat. 3292, 3424-3461 (2014); Pub. L. No. 114-92, tit. VIII, 129 Stat. 726, 876-956 (2015); Pub. L. No. 114-328, tit. VIII, 130 Stat. 2000, 2245-2338 (2016); Pub. L. No. 115-91, tit. VIII, 131 Stat. 1283, 1447-1510 (2017); Pub. L. No. 115-232, tit. VIII, 132 Stat. 1636, 1823-1919 (2018).
10Commercial best practices are established methods or processes already being used by leading commercial companies that can be adapted by the government to lower costs and maximize value. Competition can help the government achieve the best return on its investment.

Letter
Page 4 GAO-20-197 TRICARE Acquisitions
that describe DHA’s implementation of value-based pilots and demonstrations.11 We also reviewed DHA’s decision papers that summarized the value-based pilots and demonstrations as well as DHA’s modifications to the T-2017 contracts to implement them. We conducted interviews with DHA officials and representatives from the two managed care support contractors to discuss the status of the department’s value-based program efforts.
To examine the extent to which DHA implemented the 13 elements as required by the NDAA 2017, we reviewed the provisions in section 705(c) of the NDAA 2017 as well as specific sections of the 2015 edition of the TRICARE Operations Manual and the TRICARE Policy Manual that have information related to the 13 required elements.12 We also reviewed any modifications DHA made to the T-2017 contracts associated with the required elements. We interviewed officials from DHA, including DHA leadership, the Chief of the TRICARE Health Plan, and other DHA staff involved in the implementation of the required elements, as well as representatives from the two managed care support contractors, to obtain information on the status of the department’s efforts and any additional planned activities. We assessed this information against the 13 required elements to determine the extent to which DHA had implemented them. Based on our review, we established three categories to describe the extent of implementation: (1) not implemented, (2) partially implemented,
11Report to the Armed Services Committees on Pilot Program on Incorporation of Value-Based Health Care in Purchased Care Component of TRICARE Program, Section 701(h)(3) National Defense Authorization Act for Fiscal Year 2017 (Public Law 114-328), and Implementation Plan – Value-Based Incentives Under Section 705(d) National Defense Authorization Act for Fiscal Year 2017 (Public Law 114-328), January 31, 2018.
The TRICARE Operations Manual—one of four primary manuals applicable to the T-2017 contracts—is the primary vehicle for operational guidelines and instructions to the contractor. 12The TRICARE Policy Manual is the primary vehicle for policy and benefit guidelines and instructions.

Letter
Page 5 GAO-20-197 TRICARE Acquisitions
and (3) fully implemented.13 We also evaluated DHA’s efforts against sound practices for planning, as reported in our prior work.14
We conducted this performance audit from November 2018 to February 2020 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
Fourth Generation TRICARE Contracts (T-2017)
For the T-2017 contracts, DHA consolidated its TRICARE regions from three regions (North, South, and West) to two regions (East and West).15
Humana Government Business is the managed care support contractor for the East Region, and Health Net Federal Services is the managed care support contractor for the West Region. Health care delivery under the T-2017 contracts began on January 1, 2018.
13For the purposes of this report, we define the three categories as follows: (1) not implemented (DHA officials have not initiated activities to implement the element, although they did provide information about their plans); (2) partially implemented (DHA provided evidence showing that implementation was initiated, but additional work is planned for the element); or (3) fully implemented (DHA provided sufficient evidence showing that it implemented the entire element and no additional work remains). Two analysts independently reviewed DHA information and determined which of the three status categories the requirement fell under. The analysts subsequently reached consensus on the status of each of the 13 required elements. 14In past reports, we have identified sound practices in planning. For example, see GAO, Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism, GAO-04-408T (Washington, D.C.: Feb. 3, 2004) and GAO, Social Security Disability: Additional Performance Measures and Better Cost Estimates Could Help Improve SSA’s Efforts to Eliminate Its Hearings Backlog, GAO-09-398 (Washington, D.C.: Sept. 9, 2009). To identify these leading practices, we consulted numerous sources, including general literature on strategic planning and performance and guidance from the Office of Management and Budget.15As of November 2019, the East region covers approximately 6.1 million beneficiaries, and the West region covers approximately 2.9 million beneficiaries, according to representatives of Humana Government Business and Health Net Federal Services.

Letter
Page 6 GAO-20-197 TRICARE Acquisitions
DHA expects the costs of the two contracts to total approximately $58 billion over a 5-year performance period, which is scheduled to end on December 31, 2022. The primary responsibilities of the managed care support contractors include the following:
· developing civilian provider networks, which include hospitals and clinicians;
· processing referrals and authorizations for beneficiaries to receive health care;
· enrolling beneficiaries; · processing health care claims; · providing comprehensive, readily accessible customer services for
beneficiaries and providers; and · establishing and maintaining a medical management program that
includes requirements in the TRICARE Operations Manual.16
In addition, DHA officials told us that they have begun their planning activities for the fifth generation of TRICARE contracts, referred to as the T-5 contracts. If DHA exercises all option years for the T-2017 contracts, health care delivery under the T-5 contracts is expected to begin in 2023.17
16As part of medical management, the contractor shall ensure that care provided, including mental health care, is medically necessary and appropriate and complies with the TRICARE benefits. 17After making the determination that the option is the most advantageous method of fulfilling the government’s need, price and other factors considered, contracting officers are generally authorized to exercise options without additional competition. FAR § 17.207(c). DHA expects to award its T-5 contracts in 2021.

Letter
Page 7 GAO-20-197 TRICARE Acquisitions
Overview of the Acquisition Process for the T-2017 Contracts
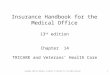
DHA’s acquisition process for the T-2017 contracts consisted of four steps: (1) planning the acquisition, (2) issuing the Request for Proposals (RFP) and soliciting responses, (3) awarding the contracts, and (4) post award activities (see figure 1).18
18There are federal- and department-level requirements that govern the process for each phase of the acquisition process. The regulatory policies and procedures for DOD acquisitions are outlined in the Federal Acquisition Regulation and the Defense Federal Acquisition Regulation Supplement. The Federal Acquisition Regulation defines uniform policies and procedures for the acquisition of supplies and services for executive agencies. The Federal Acquisition Regulation is codified in title 48 of the Code of Federal Regulations. The Defense Federal Acquisition Regulation Supplement defines uniform policies and procedures for the acquisition of supplies and services for DOD that supplement the Federal Acquisition Regulation, and delegates authorities for deviations from the Federal Acquisitions Regulation requirements. In general, agencies may grant deviations from the Federal Acquisition Regulation when necessary to meet the specific needs and requirements of each agency, unless precluded by law, executive order, or regulation. For a full definition of “deviation,” see FAR § 1.402. In addition, DOD issues other guidance documents, such as the DOD Instruction (DODI) 5000.74, Defense Acquisition of Services (Incorporating Change 2, Aug. 31, 2018), to assist in the acquisition process.

Letter
Page 8 GAO-20-197 TRICARE Acquisitions
Figure 1: Timeline of Key Events Related to the Defense Health Agency’s (DHA) T-2017 Contracts

Letter
Page 9 GAO-20-197 TRICARE Acquisitions
1. Acquisition planning. DHA defined the contract requirements—the work to be performed by the contractor—and developed an acquisition plan to meet those requirements.19 The T-2017 program manager and contracting officer developed key acquisition documents—including the T-2017 Acquisition Strategy and the Acquisition Plan—and conducted market research.20 The T-2017 Acquisition Strategy provides a high-level description of the milestones in the acquisition process and how those milestones will be achieved. The T-2017 Acquisition Plan outlines the specific actions necessary to execute the approach outlined in the approved acquisition strategy.
2. Request for proposals. DHA issued an RFP that documented the requirements for T-2017—including the contract type, significant contract dates, pricing arrangements, and the criteria to be used to assess offerors’ proposals.21
3. Award. DHA established a source selection team to evaluate the proposals received in response to the RFP.22 The source selection authority selects the winning proposals using a best value tradeoff
19Acquisition planning is the process by which the efforts of all personnel responsible for an acquisition are coordinated and integrated through a comprehensive plan for fulfilling the agency’s needs in a timely manner and at a reasonable cost. It includes developing the overall strategy for managing the acquisition. FAR § 2.101. Federal regulations generally require agencies to perform acquisition planning for all acquisitions. FAR § 7.102(a). 20Market research is the collection and analysis of information about capabilities within the market to satisfy the agency’s need. FAR § 2.101. Market research can be accomplished by publishing requests for information, which are publicly released documents that allow the government to obtain feedback from industry on items such as price, delivery, or capabilities for planning purposes. 21The RFP is used to communicate government requirements to prospective contractors and to solicit proposals. FAR § 15.203. 22A source selection team consists of key individuals participating in the evaluation and source selection process, which can include an evaluation board, advisory council, source selection authority, and the contracting officer.

Letter
Page 10 GAO-20-197 TRICARE Acquisitions
process after considering reports written by other members of the source selection team.23
4. Post-Award Activities. DHA provides a 12-month transition period between its outgoing and incoming contractors to ensure that its incoming contractors are prepared for their new responsibilities.24 The transition period for the T-2017 contracts began on January 1, 2017, and ended on December 31, 2017. The incoming contractors assumed full responsibility for health care delivery on January 1, 2018.
NDAA 2017 Section 705 Requirements
The NDAA 2017 required a number of changes to the TRICARE program through its contracts.25 Specifically, section 705(a) of the NDAA 2017 required DOD to develop and implement value-based incentive programs in its contracts to help improve the quality of health care services provided to eligible TRICARE beneficiaries by rewarding civilian providers with additional payments for improved performance based on certain metrics. In addition, section 705(c) of the NDAA 2017 directed the department to develop and implement a strategy—by January 1, 2018—for its TRICARE contracts that includes 13 specific elements, such as telehealth services and beneficiary referrals, among others (see table 1).26 The act required DOD to modify its TRICARE contracts to ensure consistency with the required strategy providing for the 13 elements.
23The source selection authority also produces the source selection decision document, which is the single summary document supporting selection of the winning proposal consistent with the stated evaluation criteria. A tradeoff process is appropriate when it may be in the best interest of the government to consider award to other than the lowest priced offeror or other than the highest technically rated offeror. This process permits tradeoffs among cost or price and non-cost factors and allows the government to accept other than the lowest priced proposal. The perceived benefits of the higher priced proposal shall merit the additional cost, and the rationale for tradeoffs must be documented in the file in accordance with FAR § 15.406. See FAR § 15.101-1.
24According to 10 U.S.C. § 1095c(b), DOD is generally required to allow non-incumbents a 9- to 12-month transition-in period. 25Pub. L. No. 114-328, 130 Stat. 2000 (2016). 26Pub. L. No. 114-328, § 705(c)(1), (5), (6), 130 Stat. 2000, 2202-2204 (2016).

Letter
Page 11 GAO-20-197 TRICARE Acquisitions
Table 1: The National Defense Authorization Act for Fiscal Year 2017 (NDAA 2017), Section 705 (c)(5) and (c)(6) Elements
Statute Description of the Element Section 705 (c)(5)
(A) Provider Networks: Maximize flexibility in the design and configuration of networks of individual and institutional health care providers.
(B) Medical Management: Establish an integrated medical management system between military medical treatment facilities and health care providers in the private sector.
(C) Telehealth: Maximize the use of such services to provide real-time interactive communications between patients and health care providers and remote patient monitoring; and use of standardized payment methods to reimburse health care providers for the provision of such services.
(D) Value-Based Methodologies: Use value-based reimbursement methodologies that transfer financial risk to health care providers and managed care support contractors.
(E) Financial Incentives: Use financial incentives for contractors and health care providers to receive an equitable share in the cost savings to the Department resulting from improvement in health outcomes for covered beneficiaries and the experience of covered beneficiaries in receiving health care.
(F) Prevention and Wellness Incentives: Use incentives that emphasize prevention and wellness for covered beneficiaries receiving health care services from private sector entities to seek such services from high-value health care providers.
(G) Beneficiary Enrollment: Adopt a streamlined process for enrollment of covered beneficiaries to receive health care and timely assignment of primary care managers to covered beneficiaries.
(H) Referrals: Eliminate the requirement for a referral to be authorized prior to receiving specialty care services at a facility of the Department of Defense or through the TRICARE program.
(I) Medical and Lifestyle Incentives: Use incentives to encourage covered beneficiaries to participate in medical and lifestyle intervention programs.
Section 705 (c)(6)
(A) Rural, Remote, and Isolated Areas: Assess the unique characteristics of providing health care services in Alaska, Hawaii, and the territories and possessions of the United States, and in rural, remote, or isolated locations in the contiguous 48 states.
(B) Rural, Remote, and Isolated Areas: Consider the various challenges inherent in developing robust networks of health care providers in those locations
(C) Rural, Remote, and Isolated Areas: Develop a provider reimbursement rate structure in those locations that ensures: (i) timely access; (ii) high-quality primary and specialty care; (iii) improvement in beneficiaries’ health outcomes; and (iv) an enhanced experience for beneficiaries
(D) Rural, Remote, and Isolated Areas: Ensure that managed care support contracts under the TRICARE program in those locations will: (i) establish provider networks providing timely access to care for covered beneficiaries, and (ii) deliver high-quality care, better health outcomes, and a better experience of care for covered beneficiaries
Source: GAO summary of the NDAA 2017 section 705(c) provisions. | GAO-20-197

Letter
Page 12 GAO-20-197 TRICARE Acquisitions
DHA Made Selective Changes between the T-3 and T-2017 Contracts; Some Changes Are Consistent with Provisions and Themes in Prior NDAA Legislation DHA made selective changes between the T-3 and T-2017 contracts and acquisition strategy. According to DHA officials, the contracts are generally the same, and changes were made to clarify or streamline TRICARE requirements and administrative processes. The T-2017 Acquisition Strategy states that the T-2017 performance work statement, which identifies the TRICARE requirements to be implemented by the contractors, is essentially unchanged from the T-3 contracts. DHA officials explained that their leadership prioritized the continuation of beneficiary services during the T-2017 planning process over making significant changes to contract requirements that could potentially be disruptive. We found that some of the changes that were made to the T-2017 contracts are consistent with specific provisions and themes we identified in prior NDAA legislation.
Some Changes to the T-2017 Contracts Are Consistent with Specific NDAA 2017 Provisions
Although the NDAA 2017 was enacted after the T-2017 contracts had been awarded, some of the contract changes for T-2017 may be consistent with specific provisions outlined in section 705(c)(1), such as provisions related to improving access to care, health outcomes, health care quality, beneficiaries’ experience, as well as lowering health care costs. However, DHA officials stated that because health care delivery under the T-2017 contracts began in 2018, it is too early to measure any benefits from these changes. These contract changes include (1) the consolidation of contract regions, (2) the combining of administrative costs, and (3) the introduction of new contract incentives.
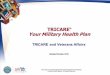
1. Consolidation of contract regions. While DHA awarded the T-3 contracts for three regions (West, South, and North), it consolidated two of the regions (North and South) for the T-2017 contracts (see figure 2).

Letter
Page 13 GAO-20-197 TRICARE Acquisitions
Figure 2: Consolidation of TRICARE Contract Regions from T-3 to T-2017
By eliminating the additional regional contract, DHA anticipates a savings of approximately $25 million a year in overhead and management costs. In addition, beneficiaries are less likely to have a disruption in care when moving. For example, beneficiaries who moved between the former North and South regions would now stay enrolled with the same contractor in the larger East region.
2. Combined administrative costs. For T-2017, DHA combined all administrative costs in one contract line item in order to lower total cost of care. For example, under the T-3 contracts, DHA reimbursed the contractors for processing individual claims with a higher rate for paper claims and a lower rate for electronic claims. Without a difference in costs for T-2017, contractors are incentivized to lower their costs and prioritize electronic claims, which DHA officials say are more efficient.
3. Contract incentives. DHA incorporated incentives into the T-2017 contracts to encourage contractors to negotiate reimbursement rate discounts with network providers in order to reduce health care costs. The T-2017 contracts state that the contractor must meet a required

Letter
Page 14 GAO-20-197 TRICARE Acquisitions
discount rate on care provided by network providers. If this discount rate is not met, DOD will offset the discount deficit amount from the next payment due to the contractor. DHA expects that negative incentive will reduce health care costs and result in government savings.
Several Contract Changes Are Consistent with Acquisition Themes in Prior NDAA Legislation
We also found examples of changes to the contract or acquisition process for T-2017 that are consistent with selected acquisition themes we identified in prior NDAA legislation. These acquisition themes are 1) leveraging commercial best practices, 2) promoting competition, and 3) focusing on value. We previously reported that the identified acquisition themes can reduce costs and increase value for the government.27
1. Leveraging commercial best practices: T-2017 required contractors to increase utilization of commercial best practices, including the use of automation technology to process referrals and authorizations, episodes of care, and procedure diagnosis coding. As we have previously reported, federal agencies can leverage commercial best practices to lower costs and maximize the value of the services they buy.28 According to DHA officials, adapting automation technology already in use in the health care industry should improve the quality of services, beneficiary satisfaction, and result in cost savings to the government. In addition, officials from one of the current TRICARE contractors stated that the T-2017 RFP was structured to incentivize contractors to innovate and bring best practices from their industry experience in both the commercial sector and other government programs, such as Medicare. For example, the T-2017 contract included a new requirement for contractors to use industry best practices when collecting health care data, in order to identify and reduce gaps in care and enhance quality of care for beneficiaries.
27GAO, Strategic Sourcing: Leading Commercial Practices Can Help Federal Agencies Increase Savings When Acquiring Services, GAO-13-417 (Washington, D.C: April 2013); GAO, Defense Contracting: DOD’s Use of Lowest Price Technically Acceptable Source Selection Procedures to Acquire Selected Services, GAO-18-139 (Washington, D.C: November 2017).28GAO-13-417.

Letter
Page 15 GAO-20-197 TRICARE Acquisitions
2. Promoting competition: We found that DHA made an effort to promote competition for the T-2017 RFP. Competitive contracts can result in cost savings for the federal government and promote accountability for results.29 In the acquisition planning phase, DHA identified an increased number of interested contractors through market research, from eight for T-3 to 22 for T-2017. In addition, DHA officials stated that they took steps during the acquisition planning process to ensure that the incumbent contractors did not have a significant advantage over prospective contractors. For example, the T-2017 contracting officer was assigned early in the planning process and did not participate in management of the T-3 contracts or in interactions with the incumbent contractors. DHA officials stated that they expected greater contractor interest in the East region because the larger beneficiary population of that region would result in a more valuable contract. However, DHA received a total of seven proposals each for T-3 and T-2017, including one new company that participated in T-2017 but had not previously submitted a proposal for T-3.30
3. Focusing on value: We found that DHA’s approach for T-2017 emphasizes value and quality, not just lower costs. Specifically, DHA focused on the value of improving health care by considering the total cost of care over time, rather than the cost of individual health care. This is reflected in the T-2017 Acquisition Strategy, which prioritizes quality and delivery of health care above lowest cost. For example, the T-2017 contracts required additional preventive screenings and diseases covered under a chronic care program to achieve improved quality of care despite the cost of screenings. We have previously reported that these preventive health services are determined to be cost-effective when they improve the benefit (e.g., health outcomes) in a less costly way than a given alternative care option.31 Some preventive services may also result in cost savings, where the cost of implementing the service is less than the expected future costs to treat a disease or condition.
29Office of Management and Budget, Enhancing Competition in Federal Acquisition (May 31, 2007). 30Offerors can submit proposals for more than one region; however, they will only be awarded the contract for one region. For T-3, six offerors submitted seven proposals in three regions. For T-2017, four offerors submitted seven proposals in two regions. 31GAO, Health Prevention: Cost-effective Services in Recent Peer-Reviewed Health Care Literature, GAO-14-789R (Washington, D.C: April 2014).

Letter
Page 16 GAO-20-197 TRICARE Acquisitions
DHA Has Implemented Two Value-Based Incentive Pilots; Other Pilots Are Planned As of October 2019, DHA had implemented two of the three value-based pilots described in its January 2018 report to Congress, which outlines the department’s plans for addressing the NDAA 2017’s requirement for developing value-based incentive programs. Specifically, in this report, DHA described its intent to implement three value-based pilots in response to section 705(a) of the NDAA 2017—(1) the Performance-Based Maternity Payments Pilot, (2) the Medication Adherence Pilot, and (3) the High-Value Primary Care Provider Pilot—through modifications to its TRICARE contracts over the next 6 to 18 months.32
1. Performance-Based Maternity Payments Pilot. DHA modified its T-2017 contracts to begin implementing the Performance-Based Maternity Payments Pilot in April 2018. This pilot was designed to provide both non-financial and financial incentives to hospitals that achieve and maintain excellence in maternity care quality. The first phase of this pilot focused on non-financial incentives by promoting greater transparency about the quality of maternity care delivered by hospitals in the TRICARE network. Specifically, DHA implemented a “steerage model” that identifies higher-performing hospitals in the managed care support contractors’ provider directories using specific visual prompts in order to encourage beneficiaries to seek care from those institutions. The second phase of the pilot began in October 2018 and incorporated performance-based payments, or financial incentives, for network hospitals that achieve a certain level of performance on specified maternity care quality measures. The anticipated end date for the pilot is March 2021.
2. Medication Adherence Pilot. DHA modified its TRICARE pharmacy contracts to begin implementing the Medication Adherence Pilot in February 2018.33 This pilot is designed to incentivize beneficiaries’
32DHA’s January 2018 report also highlights three other value-based efforts; however, these efforts specifically address a different statutory requirement in the NDAA 2017. While DHA’s January 2018 report noted the Medication Adherence pilot was intended to address statutory requirements from NDAA 2017 sections 701(h) and 705(a), the TRICARE Operations Manual only states that the purpose of the pilot is to meet the requirements set forth in the NDAA 2017 section 701(h). 33Although the Medication Adherence pilot falls within the scope of TRICARE’s pharmacy contracts, the two managed care support contractors told us they may share clinical data or inform beneficiaries about the program.

Letter
Page 17 GAO-20-197 TRICARE Acquisitions
adherence to medication regimens by reducing or eliminating copayments for two medications (one for diabetes and another for cardiovascular-related illnesses).
3. High-Value Primary Care Provider Pilot. As of October 2019, DHA officials told us they were still assessing the feasibility of implementing the High-Value Primary Care Provider Pilot, which would provide financial incentives (such as additional payments or reduced network discounts) to primary care providers who exceed certain quality thresholds, as well as financial incentives (such as reduced co-shares and copayments) for beneficiaries who use these providers.
DHA officials said other value-based efforts are being planned to address section 705(a) of the NDAA 2017, such as value-based pilots and demonstrations that aim to incentivize providers to provide quality care—including hospital, home health, and episode-based bundled payments pilots, among others. DHA has reported that these projects will offer DHA the opportunity to test value-based payment models and incorporate innovative ideas and solutions into its TRICARE contracts.34
DHA Has Partially Implemented Six of 13 Required Elements, but It Is Unclear When Implementation of All Elements Will Be Complete As of January 2020, we found that DOD had partially implemented six of the 13 elements required by sections 705(c)(5) and (c)(6) in the NDAA 2017, in its T-2017 contracts. DHA leadership explained that they had decided that the department would separately address each of the 13 elements through modifications to the TRICARE contracts rather than developing a single strategy that would address all of the elements. According to DHA officials, some of the 13 elements would be implemented through modifications to the T-2017 contracts while other elements would be addressed in the T-5 contracts as certain elements would require more time to develop.
· Section 705(c)(5): This section includes nine elements that focus on various aspects of health care delivery. We found that DHA had
34See Defense Health Agency, Evaluation of the TRICARE Program: Fiscal Year 2019 Report to Congress (February 28, 2019).

Letter
Page 18 GAO-20-197 TRICARE Acquisitions
partially implemented six of the nine elements—including provider networks, medical management, telehealth services, beneficiary enrollment, value-based methodologies, and prevention and wellness incentives (see table 2). Although DHA officials generally described their approach for addressing the three other elements, they were not able to provide documentation, such as implementation plans, with specific time frames or actions needed to fully implement each of them. Specifically, when asked about time frames for complete implementation, DHA officials told us that many of the elements should be addressed through the T-5 contracts. DHA officials also told us the department’s approach to addressing these elements—such as provider networks—will be informed by ongoing and future value-based pilots and demonstrations; however, data from these pilots and demonstrations are not expected to be available until they have concluded.
Table 2: Status of DHA’s Efforts to Address the Specific Elements Outlined in Section 705(c)(5) of NDAA 2017, as of January 2020
Statute Description of the Element Status Summary of Progress and Plans Section 705(c)(5)
(A) Provider Networks: Maximize flexibility in the design and configuration of networks of individual and institutional health care providers.
Partial Implemented
Defense Health Agency (DHA) officials told us that changes are planned to address this element in the fifth generation of TRICARE contracts (T-5), and some of these changes will be informed by the Accountable Care Organization demonstration, which began delivering care to beneficiaries on January 1, 2020. Specifically, DHA implemented an Accountable Care Organization demonstration in Atlanta, Georgia, that allows beneficiaries to enroll with and obtain care through Kaiser Permanente as their health provider. According to DHA, 1,757 beneficiaries have enrolled in this demonstration.
(B) Medical Management: Establish an integrated medical management system between military medical treatment facilities and health care providers in the private sector.
Partial Implemented
On December 27, 2019, DHA awarded a contract for the TRICARE Select Patient Navigator program. This pilot will assist beneficiaries enrolled in TRICARE Select to understand their benefits, including how to navigate the direct and purchased care systems, among other services.a The contractor started work on January 1, 2020, and is expected to begin recruiting beneficiaries to participate in the program starting in April 2020, according to officials. DHA officials also explained that integrated medical management between military treatment facilities and civilian providers is already being conducted through the coordination of care for beneficiaries enrolled in the TRICARE Prime.b These officials added that the department expects to make additional enhancements to improve integration between the direct care and purchased care systems in the T-5 contracts.

Letter
Page 19 GAO-20-197 TRICARE Acquisitions
Statute Description of the Element Status Summary of Progress and Plans (C) Telehealth: Maximize the use of
such services to provide real-time interactive communications between patients and health care providers and remote patient monitoring; and use of standardized payment methods to reimburse health care providers for the provision of such services.
Partial Implemented
DHA developed new telehealth requirements for its T-2017 contracts and, in July 2017, revised its TRICARE policy, in response to section 718 of the National Defense Authorization Act for Fiscal Year 2017 (NDAA 2017). These modifications expanded and standardized the range of health care services that can be provided via telehealth, as well as locations where these services may be received. Telehealth providers are also reimbursed at the same rate and in the same manner as when services are provided in person. The department expects to make additional enhancements that will further maximize the use of telehealth services in T-5—including leveraging new technologies and incentivizing and encouraging providers’ and beneficiaries’ appropriate use of these services.
(D) Value-Based Methodologies: Use value-based reimbursement methodologies that transfer financial risk to health care providers and managed care support contractors.
Partial Implemented
DHA modified its T-2017 contracts to begin implementing the Performance-Based Maternity Payments Pilot, in April 2018; the pilot partially addresses this element, by transferring some financial risk to health care providers. DHA is also planning additional value-based pilots. However, officials said they are trying to determine how they could use value-based reimbursement methodologies to transfer financial risk to the managed care support contractors. According to DHA officials, value-based methodologies will be incorporated in the T-5 contracts.
(E) Financial Incentives: Use financial incentives for contractors and health care providers to receive an equitable share in the cost savings to the department resulting from improvement in health outcomes for covered beneficiaries and the experience of covered beneficiaries in receiving health care.
Not Implemented
DHA officials told us the department expects to address this element in T-5, which will be informed by DHA’s Accountable Care Organization demonstration in Atlanta, Georgia, with Kaiser Permanente as a health care provider. Specifically, the demonstration is expected to include financial incentives for Kaiser Permanente providers based on improvements in health outcomes and experience for enrolled beneficiaries. These incentives will be paid on an annual basis starting in 2021. There are no incentives for the managed care support contractor for this demonstration, according to officials.
(F) Prevention and Wellness Incentives: Use incentives that emphasize prevention and wellness for covered beneficiaries receiving health care services from private sector entities to seek such services from high-value health care providers.
Partial Implemented
According to DHA officials, this element is partially addressed through the Performance-Based Maternity Payments Pilot. Specifically, under this pilot, high-performing network hospitals are identified in the managed care support contractors’ provider directories using specific visual prompts to encourage beneficiaries to seek care from those institutions. DHA officials told us the department will continue to address this requirement in T-5 and that other value-based incentive pilots will help inform related changes.

Letter
Page 20 GAO-20-197 TRICARE Acquisitions
Statute Description of the Element Status Summary of Progress and Plans (G) Beneficiary Enrollment: Adopt a
streamlined process for enrollment of covered beneficiaries to receive health care and timely assignment of primary care managers to covered beneficiaries.
Partial Implemented
DHA officials said that the Beneficiary Web Enrollment system, a pre-existing online portal that allows beneficiaries to perform several self-service functions—including enrolling in eligible TRICARE plans and making changes to primary care manager (PCM) assignments—has been modified.c Specifically, the system was updated to reflect the number of TRICARE health plans available for online enrollment, as well as a defined open enrollment period.d However, both contractors reported several administrative challenges related to this system—including the need to often revise beneficiaries’ PCM selections to conform to their PCM assignment rules, among other issues. In addition, during the 2019 Open Season, the Beneficiary Web Enrollment system also experienced technical issues that limited beneficiaries’ ability to enroll in or change plans online.e
(H) Referrals: Eliminate the requirement for a referral to be authorized prior to receiving specialty care services at a Department of Defense (DOD) facility, or through the TRICARE program.
Not Implemented
DHA officials told us that they are considering a pilot that is intended to reduce pre-authorization processing time and that the department is deliberating options for eliminating the requirement for a referral to be authorized in T-5.
(I) Medical and Lifestyle Incentives: Use incentives to encourage covered beneficiaries to participate in medical and lifestyle intervention programs.
Not Implemented
DHA officials told us that they intend to address this element in T-5. This element will also be informed by DHA’s Accountable Care Organization demonstration in Atlanta, Georgia, with Kaiser Permanente as a health care provider that began on January 1, 2020. The demonstration is expected to include incentives that encourage beneficiaries to participate in medical and lifestyle intervention programs. As planned, these incentives may be provided by Kaiser Permanente on an annual basis, at no cost to the government. For example, Kaiser Permanente could provide eligible beneficiaries a rewards card (up to $400 per household) to cover qualifying medical expenses for completing certain wellness activities. DHA officials told us they were still unsure how such incentives may be more broadly applied to the TRICARE program.
Source: GAO analysis of the NDAA 2017 section 705(c)(5) provisions and DHA information. | GAO-20-197
Note: For the purposes of our report, we define DHA’s efforts to address the specific elements required by the NDAA 2017 as follows: (1) “not implemented” - DHA officials have not initiated activities to implement the element, although they did provide information about their plans; (2) “partially implemented” - DHA provided evidence showing that implementation was initiated, but additional work is planned for the element; and (3) “fully implemented” - DHA provided complete evidence that showed it implemented the entire element and no additional work remains. aEligible beneficiaries must be aged 0-64 and have (1) complex medical conditions—two or more medical conditions requiring the coordination of multiple specialties for at least 12 months—or (2) high cost claimant status—costs equal to or exceeding $100K per year. bBeginning on January 1, 2018, TRICARE’s non-Medicare eligible beneficiary population could be enrolled in one of two basic health plan options—TRICARE Prime (a managed care option) or TRICARE Select (a self-managed, preferred provider option), which replaced TRICARE Standard and Extra. Pub. L. No. 114-328, § 701, 130 Stat. 2000, 2180-2193 (2016); 32 C.F.R. § 199.17. The

Letter
Page 21 GAO-20-197 TRICARE Acquisitions
Patient Navigator Pilot is expected to address requirements set forth in section 731 of NDAA 2018. Pub. L. No. 115-91, § 731, 131 Stat. 1283, 1441-1442 (2017). cAll Prime enrollees select or are assigned a PCM—who is responsible for providing all routine, non-emergency, and urgent health care. PCMs can be military or civilian providers. dThe Beneficiary Web Enrollment Application was updated to allow for TRICARE Retired Reserve and TRICARE Reserve Select enrollments, and enforce the annual open enrollment period and requirement for qualifying life event (such as marriage, birth of a child, or loss of eligibility) for TRICARE Prime and Select enrollments, among other updates. Prior to these changes, TRICARE Retired Reserve and TRICARE Reserve Select beneficiaries were required to log into a separate system, print an application, and mail or fax it to the contractors to establish coverage and set-up recurring payments, according to officials. eAs a result of these technical issues, beneficiaries were advised to call or mail in their form to enroll in or change health plans during the 2019 Open Season.
· Section 705(c)(6): This section included four required elements that focus on the delivery of health care in rural, remote, and isolated areas. DHA has not implemented any of these requirements. DHA officials told us they are considering requirements for T-5 that will address the four elements, but did not provide documentation with specific time frames and actions needed to fully implement each of them (see table 3).
Table 3: Status of DHA’s Efforts to Address the Specific Elements Outlined in Section 705(c)(6) of NDAA 2017, as of January 2020
Statute Description of the Element Status Summary of Progress and Plans Section 705(c)(6)
(A) Rural, Remote, and Isolated Areas: Assess the unique characteristics of providing health care services in Alaska, Hawaii, and the territories and possessions of the United States, and in rural, remote, or isolated locations in the contiguous 48 States
Not Implemented
DHA officials told us that they are considering requirements for T-5 that will address this element. They explained that under T-2017, the requirements for developing provider networks in rural, remote, and isolated areas are generally the same as those for more populated areas.
(B) Rural, Remote, and Isolated Areas: Consider the various challenges inherent in developing robust networks of health care providers in those locations
Not Implemented
DHA officials told us that they are considering requirements for T-5 that will address this element as well as recommendations made by a September 2010 interagency task force that reviewed how federal agencies are meeting the health care needs of Alaskans.a
(C) Rural, Remote, and Isolated Areas: Develop a provider reimbursement rate structure in those locations that ensures: (i) timely access; (ii) high-quality primary and specialty care; (iii) improvement in beneficiaries’ health outcomes; and (iv) an enhanced experience for beneficiaries
Not Implemented
DHA officials told us they are considering requirements for T-5 that will address this element. DHA already has the authority to increase reimbursement rates through the use of waivers in locations where it determines that the rates have had a negative impact on TRICARE beneficiaries’ access to civilian providers. Under T-2017, the civilian provider baseline reimbursement rate for outpatient care in Alaska is currently higher than the standard TRICARE maximum allowable charge. DHA has also established 14 additional locality based waivers in Alaska for certain specialty providers as well as two waivers for certain specialty providers in Hawaii.

Letter
Page 22 GAO-20-197 TRICARE Acquisitions
Statute Description of the Element Status Summary of Progress and Plans (D) Rural, Remote, and Isolated Areas:
Ensure that managed care support contracts under the TRICARE program in those locations will: (i) establish provider networks providing timely access to care for covered beneficiaries, and (ii) deliver high-quality care, better health outcomes, and a better experience of care for covered beneficiaries.
Not Implemented
DHA officials told us that they are considering requirements for T-5 that will address this element.
Source: GAO analysis of the NDAA 2017 section 705(c)(6) provisions and DHA information. | GAO-20-197
Note: For the purposes of our report, we define DHA’s efforts to address the specific elements required by the NDAA 2017 as follows: (1) “not implemented” - DHA officials have not initiated activities to implement the element, although they did provide information about their plans; (2) “partially implemented” - DHA provided evidence showing that implementation was initiated, but additional work is planned for the element; and (3) “fully implemented” - DHA provided complete evidence that showed it implemented the entire element and no additional work remains.aThe Patient Protection and Affordable Care Act established the Interagency Access to Health Care in Alaska Task Force to review how federal agencies with responsibility for health care services in Alaska are meeting the needs of Alaskans. The task force, which terminated upon submission of a report to Congress, consisted of representatives from nine federal entities, including DOD. The task force found that Alaska benefits from a number of special payment policies targeted at rural communities, and provided several recommendations. Pub. L. No. 111-148, § 5104, 124 Stat. 119, 994-95 (2010).
Without plans that include specific time frames and actions needed, it is unclear exactly how and when DHA will fully implement all 13 elements into its TRICARE contracts. As we have previously reported, sound planning calls for results-oriented organizations to develop plans that (1) provide tools to ensure accountability, such as time frames, and (2) identify specific activities to obtain desired results, among other things.35
Developing and implementing plans with time frames and actions needed can help to ensure that DHA fully implements all 13 required elements, which is particularly important since it is in the process of developing its T-5 contracts.
Conclusions The NDAA 2017 required DHA to make numerous changes to its TRICARE program—some of which impact its T-2017 managed care 35The remaining components of sound plans include (1) define the goals the organization is seeking to accomplish, (2) purpose, scope, and methodology; (3) problem definition, causes, and operating environment; (4) roles, responsibilities, and coordination; and (5) integration among and with other entities. For example, see GAO-04-408T and GAO-09-398.

Letter
Page 23 GAO-20-197 TRICARE Acquisitions
support contracts. In particular, the act required DHA to modify these contracts to ensure consistency with 13 specific elements related to improving health care delivery, such as with provider network flexibility, increased use of telehealth services, and prevention and wellness incentives, among others. While DHA has taken steps to begin implementing some of these elements in its current T-2017 contracts, it has not developed implementation plans with time frames and specific actions needed to guide its efforts, which could help ensure that DHA successfully implements all of the required elements. Until these elements are fully implemented, the department may not achieve the TRICARE program improvements Congress intended related to access to care, health outcomes, quality of care, beneficiaries’ experience, and cost efficiency.
Recommendation for Executive Action We are making the following recommendation to DHA:
The Director of DHA should develop and implement plans with timeframes and specific actions needed for all 13 required elements to be reflected in the TRICARE contracts. (Recommendation 1)
Agency Comments We provided a draft of this report to DOD for comment. In its written comments, reproduced in appendix I, DOD generally agreed with our findings and concurred with our recommendation. The department reiterated its plans to address each of the elements required by sections 705(c)(5) and (c)(6) in the NDAA 2017 as part of its T-5 contracts. DOD also provided technical comments, which we incorporated as appropriate.
In addition, DOD provided updated information on the status of its efforts to address certain elements required by section 705(c)(5). As a result of this information, we updated the status of the following two elements from “not implemented” to “partially implemented” in our overall assessment for the following reasons:
1) Provider Networks: The department provided evidence that the Accountable Care Organization demonstration was implemented on January 1, 2020, and that beneficiaries were enrolled in the program.

Letter
Page 24 GAO-20-197 TRICARE Acquisitions
2) Medical Management: The department provided evidence that it awarded a contract for the TRICARE Select Patient Navigator Pilot on December 27, 2019, and that the contractor began work on January 1, 2020.
The department also provided updates on the status of two additional elements—Financial Incentives and Medical and Lifestyle Incentives. However, while we updated the department’s plans for these elements in the report, we determined that their status should remain “not implemented” in our overall assessment for the following reasons:
1) Financial Incentives: The department provided evidence that it plans to provide financial incentives to Kaiser Permanente providers on an annual basis under the Accountable Care Organization demonstration. These incentives are expected to begin in 2021.
2) Medical and Lifestyle Incentives: According to department officials, these incentives for beneficiaries may be provided by Kaiser Permanente on an annual basis under the Accountable Care Organization demonstration, at no cost to the government. These officials told us they were unsure whether and how such incentives may be more broadly applied to the TRICARE program.
We are sending copies of this report to the Department of Defense, appropriate congressional committees, and other interested parties. In addition, the report will be available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact Sharon Silas, Director, Health Care at (202) 512-7114 or [email protected] or William T. Woods, Director, Contracting and National Security Acquisitions at (202) 512-4841 or [email protected]. Contact points for our Office of Congressional Relations and Office of Public Affairs can be found on the last page of this report. Other major contributors to this report are listed in appendix II.
Sharon Silas Director, Health Care

Letter
Page 25 GAO-20-197 TRICARE Acquisitions
William T. Woods Director, Contracting and National Security Acquisitions

Appendix I: Comments from the Department of Defense
Page 26 GAO-20-197 TRICARE Acquisitions
Appendix I: Comments from the Department of Defense

Appendix I: Comments from the Department of Defense
Page 27 GAO-20-197 TRICARE Acquisitions

Appendix I: Comments from the Department of Defense
Page 28 GAO-20-197 TRICARE Acquisitions

Appendix I: Comments from the Department of Defense
Page 29 GAO-20-197 TRICARE Acquisitions

Appendix I: Comments from the Department of Defense
Page 30 GAO-20-197 TRICARE Acquisitions

Appendix I: Comments from the Department of Defense
Page 31 GAO-20-197 TRICARE Acquisitions
Agency Comment Letter
Text of Appendix I: Comments from the Department of Defense
Page 1
January 30, 2020
Sharon Silas Director, Health Care U.S. Government Accountability Office 441 G. Street, N.W. Washington, DC 20548
Dear Ms. Silas:
Thank you for the opportunity for the Department of Defense (DoD) to review and respond to the recommendationscon1ained in the Government Accountability Office (GAO) Draft Report GAO-20-197, " DEFENSE HEALTH CARE: Plans Needed to Ensure Implementation of Required Elements for TRICARE's Managed Care Support Contracts", dated December 12, 2019 (GAO code 103168).
The Department concurs with comment to the sole recommendation contained in the report. Technical comments on the report are enclosed per your request.
Again, thank you for the opportunity to review and respond to the recommendations. My point of contact for this issue is our GAO/DoD Inspector General Liaison, Mr. Richard LeggBenavides. Mr. Legg-Benavides can be reached at (703) 681-5922 or via email at [email protected].
Thomas P. McCaffery
Enclosure: As stated
cc: Mr. William T. Woods Director, Contracting and National Security Acquisitions

Appendix I: Comments from the Department of Defense
Page 32 GAO-20-197 TRICARE Acquisitions
Page 2
Thank you for the opportunity for the Department of Defense (DoD) to review and respond to the recommendations contained in the Government Accountability Office (GAO) Draft Report GAO-20-197, "DEFENSE HEALTH CARE: Plans Needed to Ensure Implementation of Required Elements for TRlCARE's Managed Care Support Contracts", dated December 12, 2019 (GAO code 103168).
The Department concurs with comment to the sole recommendation contained in the report. Technical comments on the report are enclosed per your request.
Again, thank you for the opportunity to review and respond 10 the recommendations. My point of contact for this issue is our GAO/DoD Inspector General Liaison, Mr. Richard Legg-Benavides. Mr. Legg-Benavides can be reached at (703) 681-5922 or via email at [email protected].
Thomas P. McCaffery
Enclosure: As stated
cc: Ms. Sharon Silas Director, Health Care
Page 3
Department of Defense Response to Government Accountability Office Recommendation
DEFENSE HEALTH CARE: Plans Needed to Ensure Implementation of Required Elements for TRICARE's Managed Care Support Contracts
(GAO-20-197)
Government Accountability Office's (GAO's) recommendation to the Department of Defense (DoD):
RECOMMENDATION J: The Director, Defense Health Agency (DHA), should develop and implement plans with 1imeframes and specific actions needed for all 13 required elements 10 be reflected in the TRICARE contracts.
DoD RESPONSE: Concur with comment. The Department agrees that plans are needed to fully implement the required elements. DHA will fulfill this recommendation

Appendix I: Comments from the Department of Defense
Page 33 GAO-20-197 TRICARE Acquisitions
by addressing each of the elements required by Section 705 of the National Defense Authorization Act
(NDAA) for Fiscal Year 2017 in the acquisition strategy document and the resultant request for proposals (RFP) for the fifth generation of TRICARE contracts (T-5). DHA projects issuing draft and final RFPs in calendar year 2020. However, the Department does not agree with GAO's assessment regarding status of DHA"s efforts to address certain elements required by Section 705. Specifically:
Section 705(c)(5)(A) - Provider Networks: With the following additional information provided, DHA requested GAO reconsider its initial assessment of "incomplete" for this element and. rather, indicate as "partially implemented." During the period of the report, 65 members of the DHA team not only initiated activities to complete the Accountable Care Organization demonstration but also implemented in Atlanta. Georgia, resulting in beneficiary choice for 68,000 beneficiaries in the 2020 open enrollment season. As an update to the information DHA already provided about this project, as of December 9, 2019 (the closing date for open enrollment), 1,758 beneficiaries had enrolled under this demonstration and enrollees began receiving care on January 1, 2020.
Section 705(c)(5)(B) - Medical Management: With the following additional information provided, DHA requested GAO reconsider its initial assessment of "incomplete'' for this element and, rather, indicate as "partially implemented.” During the period of the report, DHA developed requirements, released an RFP, and awarded a separate contract on December 27, 2019, for the TRICARE Select Patient Navigator Pilot Program. This pilot program will provide TRICARE Select beneficiaries ages 0-64 who have complex medical conditions assistance in: understanding and using the health benefits under the TRICARE program; accessing and navigating the purchased care health care delivery system; providing/obtaining information to allow them to make informed decisions regarding the quality, safely, and cost of available healthcare services; and improving the health outcomes for such beneficiaries.
Section 705(c)(S)(C) - Telehealth: DHA agrees with status of partially implemented.
Section 705(c)(S)(D) - Value-Based Methodologies: DHA agrees with status of partially implemented.
Page 4
Section 705(c)(5)(E) - Financial Incentives: With the following additional information provided, DHA requested GAO reconsider its initial assessment of "incomplete" for this element and, rather, indicate as "partially implemented." During the period of the report, DHA created and awarded an innovative financial incentive package as part

Appendix I: Comments from the Department of Defense
Page 34 GAO-20-197 TRICARE Acquisitions
of the aforementioned Accountable Care Organization Demonstration that is directly linked to health outcomes and beneficiary experience.
Section 705(c)(5)(F) - Prevention and Wellness: DHA agrees with status of partially implemented.
Section 705(c)(5)(G) - Beneficiary Enrollment: DHA agrees with status of partially implemented.
Section 705(c)(5)(f) - Medical and Lifestyle Incentives: With the following additional information provided, DHA requested GAO reconsider its initial assessment of "incomplete for this element and, rather indicate as "partially implemented." During the period of the report, DHA developed and initiated a lifestyle intervention program with incentives as pan of the Accountable Care Organization demonstration. The intervention program includes a reward for beneficiaries to participate in healthy choices at a cost to the Agency.
DoD ACTIONS ALREADY TAKEN: The Department has prepared higher-level requirements mapped to each element to ensure they are accomplished during the development and execution ofT-5.
The Director, DHA, has approved high-level requirements linked to each element of the strategy with proposed implementation dates.

Appendix I: Comments from the Department of Defense
Page 35 GAO-20-197 TRICARE Acquisitions
Page 5
Higher-Level Requirements for TRICARE
NDAA 705 Subsection
Planned Implementation
1 Enhance Readiness by Managing the TRICARE Prime Benefit
(c)(5)(B), (c)(5)(G)
T-5 Award
2 Private Sector Integrated Care: Co-located Direct and Purchased Care
(c)(5)(B) Demonstration CY2020
3 MHS GENESIS Utilization and Enhance Data Transparency
(c)(5)(B) T-5 Award
4 Referrals (c)(S)(H) T-5 Award 5 Market and/or MTF On-Site Support (c)(S)(B) T-5 Award 6 Beneficiary Choice (c)(S)(A),
(c)(5)(G), (c)(6)(A), (c)(6)(B)
T-5 Award
7 Beneficiary Incentives (c)(5)(E), (c)(5)(F), (c)(5)(I)
Demonstration CY2021
8 High and Low Value Care (c)(5)(D) T-5 Award 9 Alternative Payment Methodologies (c)(5)(D),
(c)(5)(F) (c)(5)(I) (c)(6)(D)
T-2017
10 Expanded Use of Telehealth (c)(S)(C), (c)(6)(D)
T-5 Award
11 Centers of Excellence (c)(S)(A), (6)(5)(B)
Demonstration CY2020

Appendix II: GAO Contacts and Staff Acknowledgments
Page 36 GAO-20-197 TRICARE Acquisitions
Appendix II: GAO Contacts and Staff Acknowledgments GAO Contacts Sharon Silas, (202) 512-7114 or [email protected] William T. Woods, (202) 512-4841 or [email protected]
Staff Acknowledgments In addition to the contact named above, Bonnie Anderson, Assistant Director; La Sherri Bush, Analyst-in-Charge; LaKendra Beard, Jacquelyn Hamilton, Jessica Karnis, Miranda Riemer, and Lauren Wright made contributions to this report. Also contributing were Sam Amrhein and Vikki Porter.
(103168)

GAO’s Mission The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077, or TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO Connect with GAO on Facebook, Flickr, Twitter, and YouTube. Subscribe to our RSS Feeds or Email Updates. Listen to our Podcasts. Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs Contact FraudNet:
Website: https://www.gao.gov/fraudnet/fraudnet.htm
Automated answering system: (800) 424-5454 or (202) 512-7700

Congressional Relations Orice Williams Brown, Managing Director, [email protected], (202) 512-4400, U.S. Government Accountability Office, 441 G Street NW, Room 7125, Washington, DC 20548
Public Affairs Chuck Young, Managing Director, [email protected], (202) 512-4800 U.S. Government Accountability Office, 441 G Street NW, Room 7149 Washington, DC 20548
Strategic Planning and External Liaison James-Christian Blockwood, Managing Director, [email protected], (202) 512-4707 U.S. Government Accountability Office, 441 G Street NW, Room 7814, Washington, DC 20548