-
8/6/2019 galeazzi #
1/11
The PDF of the article you requested follows this cover
page.
This is an enhanced PDF from The Journal of Bone and Joint
Surgery
1975;57:1071-1080.J Bone Joint Surg Am.ZD Mikic Galeazzi
fracture-dislocations
This information is current as of January 14, 2011
Reprints and Permissions
Permissions] link.and click on the [Reprints andjbjs.orgarticle,
or locate the article citation on
to use material from thisorder reprints or request
permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The
Journal of Bone and Joint Surgery
http://www.jbjs.org/http://www2.ejbjs.org/misc/reprints_perms.dtlhttp://www.jbjs.org/http://www2.ejbjs.org/misc/reprints_perms.dtlhttp://www.jbjs.org/http://www.jbjs.org/http://www.jbjs.org/http://www.jbjs.org/http://www.jbjs.org/http://www2.ejbjs.org/misc/reprints_perms.dtl
-
8/6/2019 galeazzi #
2/11
EAR LY M ANAG EM ENT OF OPEN JO IN T IN JUR IE S 1071
VOL . 57-A , NO . 8, DEC EM BER 1975
6. D oslisR ow ski, E . T . an d DuNN . A . W .: T rea tm ent o
fO steom yel itis by D#{233}bridem en t and C losed W ound
Irrigatio n-Suc tion . C Iin . O rthop . . 43 :215-231 . 1 965.
7. DR FFt , D . J.: SCHAF FNER . W iL .t.IAS I: H iL i.S IAN , J
. W .; an d KOENIG . M . G .: T he P enetr a tion o f P en icillin
an d O ther A n tim icroh ia ls in to Jo in tF lu id . Th ree C ase
R epo rts w ith a R eapp raisal o f th e L itera tu re . J. B one
and Jo in t S urg ..9 -A: 1415-1421 . O ct. 9 67 .
S. FR ANKE I.. C . J. : SPEAR . C . V .: HICKS . J . R .: and H
su. Y . T .: T he T reatm ent ofPenicillin R esis tan t S taphy
loco ccu s .A ureus Jo in t Infec tions w ithIn tra-a rtic u la r B
ro ad Spectrum A ntib io t ics. Su rg . Forum ,1: 453-4 56 . 19 60
.
9 . G ot i )MAN . V I. A .: JOHNSON , R . K .: an d GROSSBERG .
N . M .: A rtific ial C ircu la tion : Aew Appro ach to C hron ic O
steotiy eIttts . O rthop edics . 2 :63 -65 , 1960.
0 . HAM FION . 0 . P . . J R .: Editoria l. M an agem en t of
Open F racture s an d O pen W ounds o f Jo in ts . J . T raum a, 8
: 4 75-475 . 968 .I I . Ku iv . P . J .: MAR T IN . W . J .: and CO
SENTR Y , M . B .: C hronic O steoniyelitis . II . Treatm ent w ith
C lo sed Irriga tion and Suc tion . J . Am . M ed.
A ssn .. 2 13 : l84 3-l)48 , 1 970 .2. K i t v , P . J .: WI t .
KOWSKE . C . J .: an d WASH I NGTON , J . A .. II: M usculo ske
leta l Infec tion s D ue to Se rra tia m a rce scens . C lin . O
rthop . . 9 6 : 7 6-83 ,
1973.13 . Px i/A K ts. M . J.: H A R \EY . J. P .. JR. : and
Ivt.ER , D AN IEL : Th e R o le of An tib io tics in the M an agem
entofOpen F rac tures . J. B one and Join t
Su rg .. 56 -A : 5 32-541 . A pr il 1 97 4 .14. RA ii. G . F .
:RIFFITH . R . S . : an d HI uB i.1 W . M . : Th e Pe rm eab ility
of T raum atical ly In flam ed Synovia l M em brane to Comm on ly U
sed
Antib io tic s. J. B one and Jo in t Surg .. 4 8-A : 15 34-1539.
D ec. 19 66.IS . S s1 trIt-P ET IR st:N . M . N .: LAR SON , C . B
.: an d C OCHRAN . W ILL IASIs : Lo ca l C hem othe rapy w ith P
rim a ry C losure ofSep tic W ounds by M eans of
D ra inage and Irrig ation C annulae. J. B on e and Join t Surg
..7: 562-57 1, O ct. 194 5.
G alea zz i F rac tu re -D is lo ca tion sBY 2LELIM IR DJ . M IK
IC , M .D .* , N OV I SA D , Y UG OSLAV IA
F ron t the C lin iea l H ospita l . N on Sad
ABSTRACT : Am ong 125 patien ts w ith th e G a lea zz i-type
frac tu re -d is lo ca tio n o f the fo rearm , th ere w erefou
rteen ch ild ren and e igh ty-s ix adu lts w ith th e cla ssicG a
lea zzi les ion , and tw en ty-five pa tien ts w ith a spec ia
ltype - fra c tu re of both bones and d islo ca tion of th ed ista
l radio -u lna r jo in t. C on serva tiv e m anagem en tw as
successfu l on ly in ch ild ren . In adu lts th is m ethodresu lted
in fa ilu re in 80 per cen t ofca ses. T he resu lts o foperative
treatm en t w ere m uch better . T he frac tu refragm en ts of th e
rad iu s and the d islo ca tion of th erad io-u lna r jo in t in th
is com p lex in ju ry are very un -stab le, e sp ec ia lly in th e
lesion w ith frac tu res of th erad ius and u lna , and it appears
that rig id in terna l f ixa -tion is n ecessa ry fo r th e d
isloca tion a s w ell as th e frac -tu re. W ith com b ined fixa
tion over half o f the resu ltsw ere exce llen t.
F rac tu re o f the sha ft o f the rad iu s assoc iated w ith ad
islo ca tion o f th e d ista l rad io -u lna r jo in t is a ra re
in ju ry ,f irs t rep o rted in 1 822 by S ir A stley C oope r Ju
de t and S chn ek also w ro te abo u t the le sion , b u t th e epo
nymG aleazz is frac tu re -d islo ca tion is based on a se rie s o
f e igh -teen cases d e scr ibed in 1 934. i4. I5. t7J i.2i.21i.
:tu. :t2
A survey of th e litera tu re rev ea led o n ly a few artic leso
n th is sp ecif ic su b ject. m ost o f th em reporting sm allser
ies. T o m y know led ge , th e la rgest se rie s a re tho se o fH
ughston in 1957 (fo rty -o ne cases) W ong in 1967(fo rty -fou r
case s) R eck ling and C orde ll in 1968(tw en ty -th ree cases )
21 , and M au re l in 1 970 (tw en ty -sixcases) 17
* C lin ic al H o sp ita l . H ajd uk V eljko va 1 , 2 1 000 Nov
i S ad , Y ugosla v ia .
C lin ica l M ater ia lBy defin ition , the G a leazzi frac tu
re -d is locatio n is a
frac tu re o f the sh aft o f th e rad iu s w ith an assoc ia
ted d islo -catio n of the d ista l rad io -u ln ar a r ticu latio
n . T he sha ft isco nside red to be th at pa rt o f the rad ius be
tw een the b ic ip i-tal tu be ro sity p ro x im a lly and an area
fou r to f ive cen tim e te rsfrom the d ista l ar ticu la ting su
rface o f the rad ius d ista lly .A cco rd ing ly , fractu re s o f
the d is tal end o f th e rad iu s(C o lle s frac tu res) , w h ich
a re o ften accom pan ied b y a d is -loca tion o f the u lna r
head , and fractu re s o f th e rad ia l neckand h ead , w h ich a
re occasio na lly a sso cia ted w ith a d islo -ca tion of the d
ista l rad io -u ln ar jo in t (E ssex -L op resti frac-tu re s), a
re exc luded from th is se rie s . H ow eve r , in thepresen t ser
ies cases in w hich th e shafts o f bo th the rad iusan d the u lna
w ere frac tu red and th e d is tal rad io -u lna r jo in tw as d
isloca ted a re in clu ded . T h is k ind of in ju ry , desp iteits
dev ia tion from the c la ssic d efin itio n , sho u ld be con
si-de red a pa rticu lar type of G aleazz i le sion .
F rom 1964 th roug h 1974 , I treated 12 5 pa tien ts w ithin ju
r ies o f th e G a leazz i type . N ine ty - tw o of the pa tien
tsw ere m a le (73 .6 p er cen t) and th irty -th ree, fem ale (26
.4pe r cen t) . M ost w ere adu lts be tw een the ag es o f tw en
tyand fif ty (F ig . 1. T his frac tu re-d islo ca tio n rare ly o
ccu rs inch i ld ren 14 .21 . 22 , and w e h ad on ly on e pa tien
t in th e ag egroup o f b ir th to ten y ea rs . T he equ iva len t
le sio n in ch il-d ren is a frac tu re o f the rad iu s a ssoc ia
ted w ith sepa ratio nof the d is tal u ln ar ep iph ysis: h ow eve
r, th e pa tho logy andpro gno sis o f th is in ju ry in a ch ild a
re qu ite d iffe ren t, and itis the refo re exc lud ed from th is
rep ort. F ifty -e igh t (46 .4pe r cen t) o f th e fractu re s
occu rred on the righ t sid e andsix ty -seven (5 3 .6 pe r cen t)
on th e lef t. F o rty -n ine pa tien ts(3 9 .2 pe r cen t) w ere m
anu al lab o rers; tw en ty -fo u r (1 9 .2
-
8/6/2019 galeazzi #
3/11
3230
25 -
20 -
15
10
2220
7
1 0 7 2 ; D J. M IK IC
T H E JO U R N A L O F B O N E A N D JO IN T SU R G E R Y
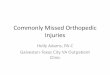
35 - n um be r o r c a s e s
o -5_ 3 -b ,t ;2 o a ;, ii , ; -so -- ,.bo bo sFIG . 1
A ge distribution in 125 cases of G aleazzi
fracture-dislocation.
pe r cen t) , fa rm ers; tw en ty -th ree (1 8 .4 pe r cen t), h
ouse-w iv es; n ine teen (1 5 .2 pe r cen t), s tuden ts ; s ix , o
fficew orke rs ; an d fo ur , re tired .
PathologyT here is som e d isag reem en t o n th e ex ac t m
echan ism
th at p ro duces th e G aleazzi frac tu re -d islocatio n . T he
m ostp rob ab le m echan ism is a fa ll on the ou tstre tched h an
dcom bined w ith ex trem e prona tion of th e fo re-ar m
17JI.22.:to. :U T he fo rces are tho ugh t to c ros s therad io
carp a l a rticu la tion , p rodu cing the d isloca tion andfo re
shorten ing of the rad ia l sha ft. A s the d isp lacem en tcon tin
ues, d is loca tion of the u ln ar head o ccu rs w ith tear -in g o
f the triang u la r f ib roca rtilage , w h ich th en lo se s itss
tab iliz ing in fluence on the w rist. T h is o ccu rred in six ty
-e igh t o f o u r p atien ts (54 .4 pe r cen t) . H ugh ston
consid -ered the u sua l cause o f th is in ju ry to b e a d irect
b low toth e do rso rad ia l a spec t o f the fo rearm , bu t tha t
m ech an ismw as re spo nsib le fo r on ly e igh t (6 .4 pe r cen
t) o f the in ju rie sin th is ser ie s . In the re st o f o u r
case s th e m ode of in ju ryw as no t de term in ab le. Tw en ty
-five o f ou r p atien ts (2 0 pe rcen t) w ere in ju red in tra ff
ic acc iden ts , n ine teen (1 5 .2 p ercen t) w hile a t w o rk o
n m ach in es , an d five in m isce llane -ous o the r w ays : they
w ere no t ab le to ex p la in h ow the irfo rea rm s w ere in ju
red . In any case, ro ta tion al stres ses o nthe fo rea rm w ou ld
seem to be essen tia l fo r d is locatio n o fth e d ista l rad io
-u lna rjo in t. It h as been dem onstrated clin i-ca lly and ex pe
rim en ta lly tha t a tea r o r d etachm en t o f thed iscus articu
la ris is th e firs t s tep to d isloca tio n and occu rsa t the ex
trem e of p rona tion and ex ten sion of th ew r i s t
:i.2t.22.24.:4O
T he frac tu re o ccu rs m os t o ften at th e ju nc tion of
them id d le and d ista l th ird s o f th e rad ius (seven ty -o ne
cases,o r 5 6 .8 pe r cen t in ou r se rie s) , and les s o ften in
the m idd leth ird o f th e rad ia l sh aft (th irty -n in e case
s, o r 3 1 .2 pe rcen t) . T he jun ctio n of the p ro x im a l and
m id d le th irds(eig h t case s) , the d istal th ird (fiv e case
s) , and the p ro x im a lth ird o f th e rad iu s ( tw o cases ) a
re in freq uen t site s o f the
frac tu re . In tw o p atien ts a doub le frac tu re o f the rad
iu s oc -cu rred . Th e fractu re o f th e rad ius u sua lly is com
posed o fon ly tw o fragm en ts (eig h ty -th ree case s in o ur se
rie s) , bu tfo rty -tw o cases (33 .6 p er cen t) w ere m
ultifragm en ta ryfractu re s . T he tran sve rse- type frac tu re
w as m os t freq uen t(six ty -n ine case s). In tw en ty -on e
cases the frac tu re w asob lique an d in fou rteen , sp iral. In e
lev en cases the typ e off ractu re cou ld no t be c lass ified
because of comm inu tion .T he subp erios tea l fractu re w ith an
gu la r d isp lacem en t on lyw as no ted in ten p atien ts , a ll
le ss th an six teen yea rs o ld .Tw en ty -seven frac tu re s (2 1
.6 pe r cen t) w ere o pen , an d insom e o f them th e so ft
tissue w as seve re ly dam aged . A ll o fthe se frac tu re s had m
arked d isp lacem en t an d the rad iusa lw ays w as sh orten ed .
The u sua l d isp lacem en t o f the d is -ta l rad ia l fragm en t
w as to th e u lna r side (6 0 pe r cen t) , bu tit occu rred to th
e dorsa l, vo la r , and rad ia l s ide s, an d prox -im a lly as w
e ll. O n ly ra re ly w as the d isp lacem en t in oned irect ion
.
M os t o f th e tim e (n in ety -n ine case s, o r 7 9 .2 pe r
cen t)the d isloca tio n of the d istal rad io -u lna r jo in t w
as ev iden tc lin ically an d roen tgeno grap h ica lly . H ow eve
r, som e tim es(tw en ty -tw o cases, o r 2 0 .8 p er cen t) th e u
ln ar headi-tia lly w as on ly sub lu xa ted , and th is w as m ore
ev id en t d in -ica lly th an roen tgen ograph ica lly . B u t in
those case s, b e-cau se the tr iangu lar f ib ro ca rtilag e w as
ru p tu red the jo in tw as ve ry unstab le, an d if th e ea rly
trea tm en t w as im p ro pe rcom p lete d isloca tion of th e jo
in t occu rred la ter .
T he d is tal rad io -u lna r jo in t is s tab iliz ed by va rio
usstruc tu re s (th e u lna r co llate ral lig am en t, the an te
rio r andposte rio r rad io -u lna r lig am en ts , and th e p ro
na to r q uad-ratu s m uscle ) , b u t the m os t im portan t stab
iliz ing fo rce isth e triang u la r f ib rocartilage 0. 1 . 2,
4.iii There can be no d is-loca tion of th e d ista l rad io -u ln
ar jo in t w ith ou t rup tu re o fth is stro ng in tra -ar ticu la
r ligam en t. T he refo re, the q ues-tio n of w he th er th e
triang u la r f ib roca rtilage is rup tu red orno t is the c ru c
ial one in de te rm in ing the p resen ce o f aG a leazz i le sio n
. Th e sp ec if ic fun ctio n of the tr iangu la rf ib ro cartilag
e is to lim it the ro ta tion a l m ovem en ts o f therad ius and u
lna o n one ano the r ii.1. () There fo re , if thejo in t w as ex
posed to an exagg e ra ted ro ta tion al m ovem en t(h yperp ro na
tion or hyp ersup ina tion ) , rup tu re o r de tach -m ent o f the
triang u la r f ib ro cartilag e co u ld occur and a d is-loca tion
of the u lna r head w as then po ssib le .
In th is rega rd the avu lsion o f th e u lna r sty lo id p
rocessw as equ iv alen t to rup tu re o f th e tr ian gu la r f ib
rocartilage ; itw as no ted in 3 1 .2 pe r cen t (th irty -n in e )
o f ou r pa tien ts . Infou r cases in the p resen t se r ies the u
ln a r head w as frac -tu red and d isloca ted . D isloca tion of
th e u lna u sua lly o c-cu rred d istally , do rsa lly , and m ed
ially (d ia sta sis) ; vo la rd isloca tion w as le ss frequen
t.
A s m en tio ned , in tw en ty -fiv e case s (20 pe r cen t) th
eG aleazz i- type le sio n w as o ne in w hich th e sh a fts o f bo
thb on es w ere frac tu red an d the in fe rio r rad io -u lna rjo
in t w asd islo ca ted (F igs. 5 -A th rou gh 6 -D ). A lth ough d
islo ca tiono f the d istal rad io -u ln ar jo in t w ith fractu re
s o f bo th bon eso f th e fo rearm w as repo rted by som e au tho
rs3 J 6 J 9 , 2 8 . 2 9th e m ean ing and im portance o f th is pa
rticu la r le sion has no t
-
8/6/2019 galeazzi #
4/11
GA LEA ZZ I FRA CTU RE -D ISLOC ATIO NS 1073
VO L . 5 7-A . N O . 8 . D EC EM BER 1975
been understood or related to the usual G aleazzi lesion.From
the pathological and therapeutic point of view theselesions differ
from ordinary fractures of theorearm . Them ode of injury is the
sam e as in the classic type ofG aleazzi lesion - the distal fragm
ent of the radius is dis-placed and the bone shortened - but the m
ain and criti-cally differentiating characteristic is the
dislocation of thedistal radio-ulnarjoint. w hich alw ays is
present. T he frac-ture of the ulna w hich obviously occurs after
the disloca-tion of the radio-ulnar joint, as force continues to be
ap-plied, is the unique feature of the injury that m ight be
con-sidered a differentiating characteristic from typicalG aleazzi
fracture-dislocations. B ecause of the rupture ofthe triangular
fibrocartilage this special G aleazzifracture-dislocation is also
extrem ely unstable. C onse-quently the therapeutic problem and the
prognosis w iththis lesion are sim ilar to those of the classic G
aleazzi le-sion.
The G aleazzi fracture-dislocation can som etim es beassociated
w ith an injury to the ulnar nerve2, In the pres-ent series this
happened only once, in a tw enty-year-oldpatient w ith fractures of
both bones w hich w ere initiallyreduced and fixed w ith K irschner
w ires. T he distal radio-ulnar joint w as reduced closed but later
delayed union ofthe fracture and redislocation ofthe distal
radio-ulnar jointoccurred. A fter eight m onths, no recovery of the
ulnarnerve w as evident. Then the distal end of the ulna w as
re-sected and the nerve w as explored, but no obvious lesionof the
nerve w as found, and nerve function did not im -prove thereafter.
W arren st also reported a case of aninterosseous nerve palsy
follow ing a G aleazzi fracture.
DiagnosisA lthough the diagnosis of the G aleazzi fracture-
dislocation should not be difficult, it often seem s to bem
isdiagnosed :ti T he fracture, of course, is alw ays noted,but the
disruption of the distal radio-ulnar joint is oftenoverlooked. O ur
patients w ere treated by m any surgeonsand initial docum entation
in m any cases w as incom plete;therefore, the frequency of m
isdiagnosis, although high,could not be established. T he diagnosis
ofthis com plex in-jury is quite sim ple, providing a careful
clinical and roent-genographic exam ination of the distal
radio-ulnar joint ism ade w henever a fracture of the forearm , and
especiallyan isolated fracture of the radius, is encountered.
The clinical appearance is characteristic. T here isusually an
angular, concave deform ity on the radial side ofthe forearm , w
hich seem s shortened. T he distal radio-ulnar joint also is deform
ed, sw ollen, and painful. T heulnar head m ay seem to protrude and
to be slightly m orem obile than usual.
E very roentgenographic exam ination of an isolatedfracture of
the radius m ust include the inferior radio-ulnarjoint, but because
dislocation of the joint can also be as-sociated w ith a fracture
of both bones, it is advisable toexam ine the joint carefully in
every case of forearm frac-ture. R oentgenographic diagnosis
ofdislocation ofthe dis-
tal radio-ulnar joint, how ever, is not alw ays easy. W henthe
ulnar head is only subluxated (in about 20 per cent ofcases), the
roentgenographic appearance usually is norm alat first.
In these cases care m ust be taken w ith the physicalexam
ination, and roentgenographically attention shouldbe given to the
problem of plus and m inus variations of theulna 27, T hese norm al
variations can be m istaken roent-genographically for
dislocations.
In cases in w hich the diagnosis is uncertain, arthrog-raphy of
the w rist joint can be helpful in establishingw hether the
triangular fibrocartilage is rupturedt.tt W estarted to use this m
ethod of diagnosis three years ago andhave had experience w ith it
in eight cases of suspectedG aleazzi lesions. In five patients the
arthrogram s w erenorm al, show ing that no rupture of the
articular disc hadoccurred. O n the basis of that finding, a G
aleazzi injuryw as excluded. In three young patients, filling of
the w ristjoint w ith contrast m edium indicated a rupture of the
disc(Figs. 2-A through 2-D ), and in these cases the diagnosisof G
aleazzi fracture w as confirm ed. The positive arthro-graphic
finding (the passage of contrast m edium from thew rist into the
inferior radio-ulnarjoint) cannot be regardedas alw ays diagnostic
of a disc rupture, because there oftenis a perforation in the norm
al disc. This considerably re-duces the clinical value of w rist
arthrography, but accord-ing to m y ow n investigation of 100 fresh
cadavera (I 80w rist joints), perforation of the triangular
fibrocartilagedevelops from degenerative changes, and its
occurrencedepends on the age of the subject. In cadavera of
personsup to tw enty years old no perforation w as found, and in
thethird decade the perforation occurred only rarely (7.6 percent).
H ow ever, in cadavera of individuals over thirtyyears old the
incidence of perforation w as m uch higher,and in persons over
sixty the perforation occurred in 53.1per cent. Therefore, a
positive arthrographic finding ofdisc rupture m ay be considered
reliable only in persons upto thirty years old.
Treatm en t and R esu ltsW e w ill describe the treatm ent and
results in our
series w ith reference to three groups of patients: (1chil-dren
(up to sixteen years old); (2) adults w ith the classicG aleazzi
fracture-dislocation; and (3) adults w ith fractureof both bones
associated w ith dislocation of the distalradio-ulnar joint.
The results are classified as excellent, fair. and poor.A n
excellent result is one in w hich there is union, perfectalignm
ent, no loss of length, no subluxation of the distalradio-ulnar
joint, no lim itation of elbow and w rist func-tion, and no lim
itation of supination or pronation. A fairresult is one in w hich
there is one or m ore of the follow ing:delayed union, m inim um m
alalignm ent and shortening ofthe radius, subluxation of the ulnar
head, excessive scar,lim itation of pronation-supination up to 45
degrees, andsom e degree of restriction of m otion of the elbow
andw rist. A n im portant criterion for a fair result is that
subjec-
-
8/6/2019 galeazzi #
5/11
FIG . 2 -B F IG . 2 -C F IG . 2 -DFig. 2-B : The arthrography of
the w rist joint revealed the passage of contrast m edium into the
inferior radio-ulnarjoint,ndicating the rupture of
the triangular fibrocartilage. The extra-articular flow of the
contrast m edium (ef) show ed the seriousness of the injury to the
distal radio-ulnar joint.Fig. 2-C : C losed reduction and
percutaneous R ush pinning of the radius and radio-ulnar
transfixation w ere perform ed.Fig. 2-D : A fter seven m onths the
anatom ical and functional results w ere excellent.
TH E JO URNA L OF BO NE A N D JOIN T SU RGERY
I074
FIG . 2-AA tw enty-four-year-old patient w ith a dislocated
fracture of the radius
and suspected dislocation of the distal radio-ulnar joint.
tively the patient m ust be satisfied w ith the end result.
Theresult is rated poor ifthere is one or m ore ofthe follow
ing:pain. deform ity of the forearm . non-union, rem
arkableshortening or angulation of the radius, dislocation of
thedistal radio-ulnar joint. lim itation of pronation-supinationof
m ore than 45 degrees. and excessive restriction ofelbow and w rist
function.
T he follow -up period in our series w as from sixm onths to
eleven years. w ith an average of tw o years andseven m o nths.
In the group o fch i ld ren there w ere fourteen patients,of w
hom tw elve w ere treated conservatively. In all casesadequate.
stable reduction w as easily achieved by m a-nipulation. probably
because m ost of the fractures w eresubperiosteal. In nine patients
the results w ere excellent,and only in a fifteen-year-old boy did
redislocation of theradial fragm ents (volar angulation) occur.
The radius healed in an angulated position but func-tion w as
good and the result w as rated fair. C losed reduc-tion failed in
only one patient: open reduction w as thendone w ithout internal
fixation, and a fair result w as re-corded after six years of
follow -up. In one sixteen-year-old boy percutaneous R ush pinning
w as done w ith an ex-
z . D J. M IK IC
cellent result. The end result in tw o patients w as unknow
nbecause they w ere lost to follow -up. The average tim e
forfracture healing w as four to six w eeks.
There w ere eight-six adult patients w ith thelassicG aleazzi le
s io n . T hirty-four of them (39.5 per cent) w eretreated w ith
closed reduction and im m obilization only,and fourteen of these
could not be evaluated because therecords w ere incom plete. O f
the rem aining tw enty pa-tients, sixteen (80 per cent) had end
results that w ere poor.In m ost of these cases good position of
the fracture frag-m ents and good reduction of the ulnar head w ere
obtainedinitially by m eans of m anipulative reduction; but later,w
hile in a plaster cast, som e angulation and slipping of theradial
fragm ents and subluxation or dislocation of the dis-tal
radio-ulnar joint occurred, resulting in loss
ofsupination-pronation and loss of w rist and elbow m otion.The
slippage usually occurred seven to ten days after thereduction.
In tw o patients a second reduction w as tried, butw ithout
success. E xcellent results w ere obtained in onlytw o patients
treated conservatively, and in them the distalradio-ulnar joint w
as only subluxated. The healing periodof the conservatively treated
fractures w as usually tw o tothree m onths. D elayed union w as
noted in one patient andosteoarthritis of the distal radio-ulnar
joint w ith painfulforearm rotation occurred in five patients.
Fifty-tw o adult patients (60.5 per cent) w ere operatedon
early. They w ere treated by several surgeons over aneleven-year
period, and therefore the operative m ethodsw ere quite varied. In
m ost cases a closed reduction w as at-tem pted first, and w hen it
failed the operation w as donew ithin a few days. In forty-tw o
patients open reductionand internal fixation of the radius w as
perform ed. In tenpatients a closed reduction w as done w ith
percutaneousR ush pinning of the radius. T he distal radio-ulnar
jointw as alw ays reduced closed except in tw o cases in w
hich,because of fracture of the ulnar head, resection of the
dis-tal portion of the ulna w as perform ed. In fourteen
patientsthe radio-ulnar joint w as transfixed w ith K irschner w
ires
-
8/6/2019 galeazzi #
6/11
G ALEAZZ I FR AC TURE -D ISLOCAT IONS 1075
VO L . 57-A , NO . 8 , DECEM BER 19 75
FIG . 3 -A FIG . 3 -B F IG . 3-CFig. 3-A : M ultifragm entary
fracture in the m iddle third ofthe radius in a thirty-one-year-old
m an. T he dislocation ofthe distal radio-ulnarjoint is
show n.Fig. 3-B : B ecause the fracture w as m ultifragm entary,
a six-hole plate w as used. R adio-ulnar transfixation w ith K
irschner w ires w as applied to
stabilize the distal radio-ulnarjoint. O ne m onth
postoperatively the plaster cast and K irschner w ires w ere rem
oved and physical therapy w as initiated:although the fracture had
not healed, it w as stabilized sufficiently to begin
rehabilitation.
Fig 3-C : Four m onths after operation the fracture w as healed
and the patient had a full range of m otion.
(Figs. 3-A , 3-B , and3-C ). O f the patients operated
on,forty-three w ere follow ed up.
W ith the m ethod of R ush pinning, w e had satisfactoryresults
(thirteen excellent, five fair, and one poor). In tenpatients w ith
sim ple transverse fractures the closed reduc-tion and percutaneous
R ush pinning of the radius w as suc-cessfully perform ed. W e w
ere especially pleased w ith theresults of R ush pinning (open or
percutaneous) and radio-ulnar transfixation (five excellent and tw
o fair results)(Figs. 2-A through 2-D ). The healing period after R
ushpinning in m ost cases w as tw o to three m onths. O nly once,in
a tw enty-four-year-old m an w ith an open fracture, didw e
encounter non-union, after four m onths. T his patientinitially had
a poor result; onlay bone-grafting w as per-form ed and a fair
result w as achieved.
Plating of the radius w as used in thirteen patients,w ith
generally satisfactory results (six excellent, four fair,and tw o
poor). O nce again results w ere better w henradio-ulnar
transfixation had been done (Figs. 3-A , 3-B ,and 3-C ). In one
patient w ith a poor result (Figs. 4-Athrough 4-E), although the
osteosynthesis seem ed stable,m alunion of the radius and
redislocation of the distalradio-ulnar joint occurred. In the other
poor result, inw hich the fractured ulnar head w as also resected,
the fail-ure probably occurred because of technical error.
Slightredislocation and non-union w ere evident after sevenm onths;
onlay bone-grafting w as done and a fair result w asobtained. In m
ost instances the healing period w as tw o tothree m onths.
The m ost unsatisfactory results (none excellent, fivefair, and
three poor) occurred in the patients treated w ith
K irschner intram edullary pinning of the radius. The heal-ing
period for these fractures w as four m onths, and in tw opatients
non-union w as evident after six m onths.
W e used K #{252}ntscher nails only tw ice, w ith a poor re-suit
in one patient and an unknow n result in the other, inw hom
resection of the distal ulna w as also perform ed.
Tw o spiral fractures w ere fixed w ith w ire loops andthe final
result w as excellent in one; in the other the resultw as
originally poor, as the w ire cut through the bone.Later, onlay
bone-grafting w as perform ed w ith a satisfac-tory end result.
Prim ary bone-grafting (onlay bone graft fixed w ithfour screw
s) w as used only once, w ith a fair result.
A s m entioned earlier, in all except tw o patients
thedislocation of the distal radio-ulnar joint w as treated
con-servatively. O nly tw ice, because of ulnar-head fracture,w as
resection of the distal part of the ulna perform ed. Inone patient,
because of com plications w ith radial fracture,the result w as
poor, and in the other it w as unknow n. Inm ost patients w ith
fair and poor results, ulnar-head sub-luxation or dislocation
recurred. B ecause of this, a fewyears ago w e began to stabilize
the joint by percutaneoustem porary radio-ulnar transfixation. A
fter rigid osteosyn-thesis ofthe radius the distal radio-ulnarjoint
w as reducedand one or tw o K irschner w ires w ere placed
percutane-ously through the ulna into the radius slightly above
thehead of the ulna (Figs. 2-A through 3-C ), as visualizedw ith
the im age intensifier. A fter four w eeks the w ires w ererem
oved. This technique w as used inourteen patientsw ith a classic G
aleazzi fracture, w ith an excellent result innine patients and a
fair result in four. In one patient the
-
8/6/2019 galeazzi #
7/11
F IG . 4 -A FIG . 4 -B F IG . 4-C
Fi#{236}.4-D FIG . 4-E
I 0 7 6 z. D J. M IK IC
TH E JO U R N A L O F B O N E A N D JO IN T SU R G ER Y
Fig. 4-A : T he classic G aleazzi fracture-dislocation in a
forty-eight-year-old m an.Fig. 4-B : Plating of the radius and
closed reduction of the distal radio-ulnarjointw ere carried out. N
ote the good position ofthe radial fragm ents
and the distal radio-ulnar joint.Fig. 4-C : A m onth later the
redislocation of the radius and the distal radio-ulnar joint w as
discovered, but nothing w as done to correct it.
result w as unknow n. C om plications w ere recorded in tw
opatients w ith fair results: in one a slight infection de-veloped
and in the other, in w hom the radius w as plated,the K irschner w
ire w hich had not been rem oved after sixw eeks broke as the
patient started physical therapy.
A serious infection occurred in tw o patients treatedoperatively
(one closed and one open fracture). O steoar-thritis of the distal
radio-ulnar joint occurred in three pa-tients (tw o poor and one
fair result).
In the third group there w ere tw enty-four patientsw ith fr a c
tu r e of bo th bon es a nd a sso c ia ted d isloca t ion ofthe d
ista l r a th o-u lna r jo in t. Four patients w ere
treatedconservatively w ith unsatisfactory results. T he othersw
ere operated on early in various w ays. w ith unsatisfac-tory
results in 45 per cent. E xcellent results w ere obtainedin only
three patients, in w hom radio-ulnar transfixationw as done in
addition to rigid osteosynthesis of both bones(Figs. 5-A through
5-D ). In m ost cases of fair and poorresults there w as
redislocation of the distal radio-ulnarjoint (Figs. 6-A through 6-D
), and this resulted in restric-tion of pronation-supination. In tw
o patients painful os-teoarthritis of the joint w as also noted. D
elayed union oc-curred in six patients and non-union, in four. Six
patientshad infection (one closed and five open fractures).
D iscussion
H ughston in reporting the results of forty-oneG aleazzi
fractures, noted that thirty-eight had been treatedby closed m eans
and three by open reduction. O f histhirty-eight patients treated
conservatively, thirty-five(92 per cent) had an unsatisfactory
result and only three (8per cent) w ere satisfactory. O f the three
treated initiallyby open reduction, tw o attained a satisfactory
result andthe third resulted in failure.
In R eckling and C ordells series eigh t patien tsw ere treated
initially by closed reduction and plaster-castim m obilization
only. and there w as not a single good re-sult (five fair and three
poor). O pen reduction w as per-
form ed in tw elve patients and eight of them had a good re-suit
(three poor and one fair).
In W ongs series :i thirty-four patients w ere treatedinitially
by m anipulative reduction follow ed by im m obili-zation in
plaster. Im m obilization in plaster w ithout any at-tem pt at
reduction w as done in four patients. and operationw as perform ed
initially in six. A successful result w asachieved in only three of
the thirty-four patients (9 percent) treated conservatively. O f
the ten patients treated byopen reduction and internal fixation,
either initially or sub-sequently. a successful result w as
achieved in three (30 percent).
O ur experience w ith the treatm ent of the G
aleazzifracture-dislocation in adults has been sim ilar. W e agreew
ith H ughston, w ho said: W e believe that the high per-centage of
unsatisfactory end results in the treatm ent ofthis fracture is due
to m ost physicians lack ofknow ledge ofthe forces active w hen the
custom ary reduction and irn-m obilization is applied in the treatm
ent of these fractures.The rareness of this fracture and,
therefore, our unfam il-iarity w ith it, accounts for our lack of
know ledge of itscom p lex aspects
Figs. 4-D and 4-E : R oentgenogram s m ade a year later. The
radiushealed in a dislocated position. The distal radio-ulnarjoint
rem ained dis-located and osteoarthritic changes developed. w ith
pseudarthrosis ofthe ulnar styloid process. The patient had painful
and restricted rotationof the forearm . The result w as rated
poor.
-
8/6/2019 galeazzi #
8/11
L25
FI G . 5-AA th irty -seven -ye ar-o ld w om an fell from a
bicycle on to he r ou t-
s tre tch ed le ft h and . In itia l roen tgeno gram s sh ow the
fra ctu re of the sha ftsofb o th b one s, th e fra ctu re ofth e
sty lo id p roc ess ofthe u lna, a nd dislo ca-l ion o f the d ista
l rad io-u ln ar jo in t.
,1..
1F I G . 5- C
A f t e r tw o m onth s the K irschn er w ire w as rem ov ed and
phy sic altherapy w as beg un . a ltho ugh th e f rac tu re s w ere
no t he ale d . T he sta b lefix ation of the frac tu res al low ed
th is.
F I G . 5- BO p en r ed u ct ion an d p la t in g o f t h e r ad
iu s a n d R u sh p in n in g o f th e u ln a
w er e p er fo r m ed . A s t h e d is t a l r a d io -u ln ar j
o in t w as u n st ab le , r ad io -u ln a rtransfixation w ith a K
irschn er w ire w a s do ne.
G AL EA ZZ I F R A C T UR E-D I S L OC AT IO NS 1077
VOL . 5 7-A , N O . S . D ECEM B ER 1975
W hen the les ion occu rs in a ch ild , the situ atio n is d
if-feren t. T h is in ju ry is qu ite rare in ch ild hood , an d
the frac -tu re then is u sua lly su bpe rio steal w ith an gu la r
d isp lace-m en t. I t c an b e red uced , an d the d isloca tio n
o f the d is talrad io -u lna r jo in t can a lso be red uced w ith
ou t d ifficu lty .T he reduc tion of bo th th e frac tu re and the
d islo ca tion usu -a lly is stab le , and the re fo re the re su
lts o f trea tm en t a requ ite favorab le . Obviously . th is
fractu re -d isloca tion inch ild ren sho u ld b e m anaged con se
rv ativ ely O f cou rse ,
F I G . 5-DAn excelle n t a natom ical a nd fun ctio na l resu
lt af ter th ree yea rs.
the redu ctio n m ust b e ad eq ua te and m ust be checkedth
roug hou t th e p eriod of im m ob iliza tion . Th e im m ob iliza
-tion sh ou ld consis t o f an above -th e-e lbow p la ster ca st w
iththe fo rearm in su p ina tion , becau se o f th e m u scle fo
rce sw h ich ac t in the d istal rad io -u lna rjo in t
T he G a leazz i sy ndrom e in adu lts has been reco gn izedand
desc ribed as a ve ry u nstab le frac tu re-d islo ca -
-
8/6/2019 galeazzi #
9/11
F iG . 6 -B
I078 1 . D J. M IK IC
THE JOURNA L OF BON E AND JO INT SURGERY
F IG . 6-AA fo rty - tou r-y ear-o ld m an . in ju red in a traf
tic acc iden t. B oth bo nes
w ere f ractu red and th e d is ta l rad io-u lna r jo in t w a
si s loca ted .
Open redu ction and R ush pin n in g of bo th h one s w as p
erfo rm ed: th ep in in the u lna is ob vious ly to o short.
tion 8 , 21 , 30 , There a re m any fac to rs re spo nsib le fo
r th einstab i l i ty K, H ow ever, rup tu re o f the triangu la r
fib ro -ca rtilage seem s to b e the m ain cause o f th e freq uen
t re-d is locatio ns o f th e jo in t an d the p oor resu lts w h
ich
Roen tgenog ram s m ade sev en m onths after op era tion show th
e frac-tu re s h ealed in satisfac to ry po sition , b u t red
isloca tion of th e d ista lrad io-u lna r jo in t oc cur red . T
he resu lt w as rate d po or.
FIG . 6 -DT he p in s w ere rem oved an d th e d ista l end o f
th e u lnaas resect ed.
The fun ctio n o f th e fore arm im p rov ed subsequ ently . a
nd the end resu ltw as rate d fa ir.
-
8/6/2019 galeazzi #
10/11
G ALEAZZI FRA CTU RE -D ISLO CA TIO NS 1079
VOL . 57-A , N O . 8 , DECEM BER 197 5
ensue. T he radius and ulna are nearly parallel and theyhave com
plex m echanical relationships to one another.A ny disproportion in
length results in a disturbance of oneof the radio-ulnar joints t
,:to, A ccordingly, any displacedand foreshortened fracture of the
radius or ulna m ust beassociated w ith a dislocation of the distal
or proxim alradio-ulnar joint or w ith a fracture of the other
boneFrom the standpoint of the restoration of norm al radio-ulnar
joint function and norm al pronation-supination, re-establishm ent
of the equal lengths of the bones is essen-tial. T herefore, if the
fracture is displaced, the fragm entsm ust be anatom ically reduced
and m ust be m aintainedthroughout the healing period. M oreover,
an unstable dis-tal radio-ulnarjoint should also be reduced and
fixed in op-tim um position. O bviously G aleazzi injuries in
adults arevery difficult to treat successfully by conservative m
eans,and it is quite understandable that the results of the
closedreduction and im m obilization are uniform lyunsatisfactory
5. 17 . 21 . 30 . 32 ,
T he results in patients treated operatively are obvi-ously
better than in those treated conservatively, but theyare still not
alw ays satisfactory, and there are too few ex-cellent results. It
is true that som e of the fractures in ourseries w ere com plicated
(open fractures w ith severe soft-tissue dam age and com m inuted
fractures) and difficult totreat, but the m ain reason for bad
results seem s to havebeen the inadequate surgical procedures that
w ere per-form ed in m any cases.
T he radius is a curved bone. Its concavity faces theulna. T he
m edullary canal of the radius is funnel-shaped inthe distal third,
and curved and narrow in the m iddlethird B ecause of this anatom
ical configuration, theradius is som ew hat unsuitable for intram
edullary fixation.W hen a radial fracture is reduced the arc on the
ulnar sidem ust be m aintained, because any deviation changes
thelength of the bone, involves the interosseous m em brane,affects
the distal radio-ulnarjoint, and produces som e re-striction of
pronation-supination. Therefore, the pin for anintram edullary
fixation of a radial fracture m ust be strongenough, and at the sam
e tim e m ust follow the arc so thatanatom ical reduction of the
radial fragm ents w ill obtainw ith optim um alignm ent. In m y
opinion, the best devicefor such a purpose is the R ush pin, w hich
is sufficientlyflexible to follow and m aintain the radial curve,
and at thesam e tim e strong enough to secure good fixation of
thefragm ents. In m ost cases, this also w ill allow stable
reduc-tion of the distal radio-ulnar joint. A ccording to m y
re-suits, R ush pinning (open or percutaneous) w as a satisfac-tory
m ethod for treating the sim ple tw o-fragm ent fractureand
especially the double fracture of the radius.K irschner w ires are
too w eak to stabilize the radial frag-m ents against the deform
ing forces w hich operate during
plaster im m obilization. Som e displacem ent of the frag-m ents
ordinarily leads to delayed union and subluxation ofthe distal
radio-ulnar joint, w ith consequent unfavorableresults. A lthough
the K #{252}ntscher nail is strong enough, it isstraight and too
rigid. and hence unsuitable for use in acurved bone like the
radius. Plating of the fracture of theradius is m ost suitable in
cases of m ultifragm entary frac-tures, and if correctly done w ill
provide rigid internalfixation of the bone and stable reduction of
the distalradio-ulnar joint in m ost cases. In addition, the firm
os-teosynthesis m akes early rehabilitation possible w ithoutw
aiting for the fracture to heal (Figs. 3-B and 3-C ). In am
ultifragm entary fracture a six-hole plate (Fig. 3-B )
ispreferable, in m y opinion, because it stabilizes the frag-m ents
better and prevents angulation (Fig. 4-B ).
T he stability ofthe distal radio-ulnarjoint is a specialproblem
. In m any cases in the present series. subluxationor dislocation
recurred. T his is understandable in cases inw hich the reduction
and fixation of the radial fracture w asnot adequate, but it w as
also encountered in several casesin w hich the osteosynthesis seem
ed solid (Figs. 4-B and4-C ). B ecause of m any factors (strong m
uscle action, thew eight of the hand, absorption at the fracture
site) therealw ays seem s to be a tendency tow ard redislocation of
thedistal radio-ulnar joint. Even rigid osteosynthesis of theradius
does not guarantee stable reduction of the ulnarhead in all cases.
O ne m ust keep this in m ind if this com -plex injury is to be
treated properly. B ecause of these fac-tors, w hen open reduction
and internal fixation of theradius have been perform ed the distal
radio-ulnar jointshould alw ays be tested for stability and in
cases w here itis unstable obviously som ething m ust be done. H
ughston suggested im m ediate resection of the distal portion of
theulna, but there are too few cases in his series to evaluatethe
value ofthis procedure as initial treatm ent. In m y opin-ion, this
is too aggressive, and it m ay be better in suchcases (and perhaps
in all cases) to tem porarily fix theradio-ulnar joint w ith one or
tw o K irschner w ires. W iththis m aneuver the ends of the
ruptured triangularfibrocartilage are approxim ated and can heal in
optim umposition.
Fractures of both bones of the forearm , w ith an as-sociated
dislocation of the distal radio-ulnar joint, is am uch m ore
difficult injury to m anage than the classicG aleazzi lesion. C
onclusions should not be firm ly draw non the basis of a relatively
sm all num ber of cases treated indifferent w ays, but it does seem
that open reduction andrigid internal fixation of both bones is the
first absolutenecessity. A s redislocation of the distal
radio-ulnarjoint isvery likely to occur - it w as present in all of
m y patientsw ith unsatisfactory results - I believe that
additionaltem porary radio-ulnar fixation also is necessary.
ReferencesI. ALBERT . S . M .: WOHL . M . A .: and R E C H TM A
N . A . M .: Treatm ent of the D isrupted R adio-U lnar Joint. J. B
one and Joint Surg.. 45-A :
1373-1381. O ct. 1963.2. BOHLER . J .: G elenknahe F rak tu r en
de s U n tera rm es. D er C h iru rg . 4 0 : 1 98 -20 3 , 19 69 .3.
CO L EMAN . H . M .: Injuries ofthe A rticular D isc atthe W rist.
J. B one and Joint Surg..2-B: 522-529. A ug. 1960.
-
8/6/2019 galeazzi #
11/11