Embed Size (px)
Citation preview
Functional Imaging with PET for Sarcoma
Rodney Hicks, MD, FRACP
Director, Centre for Molecular Imaging
Guy Toner, MD, FRACP
Director, Medical Oncology
The Peter MacCallum Cancer Centre, Melbourne, Australia
Functional Imaging with PET in Sarcoma
Potential Applications
• Benign versus malignant
• Grading
• Biopsy guidance
• Staging
• Therapeutic monitoring
• Restaging ( local recurrence)
Functional Imaging with PET in Sarcoma
Potential Applications
• Benign versus malignant
• Grading
• Biopsy guidance
• Staging
• Therapeutic monitoring
• Restaging ( local recurrence)
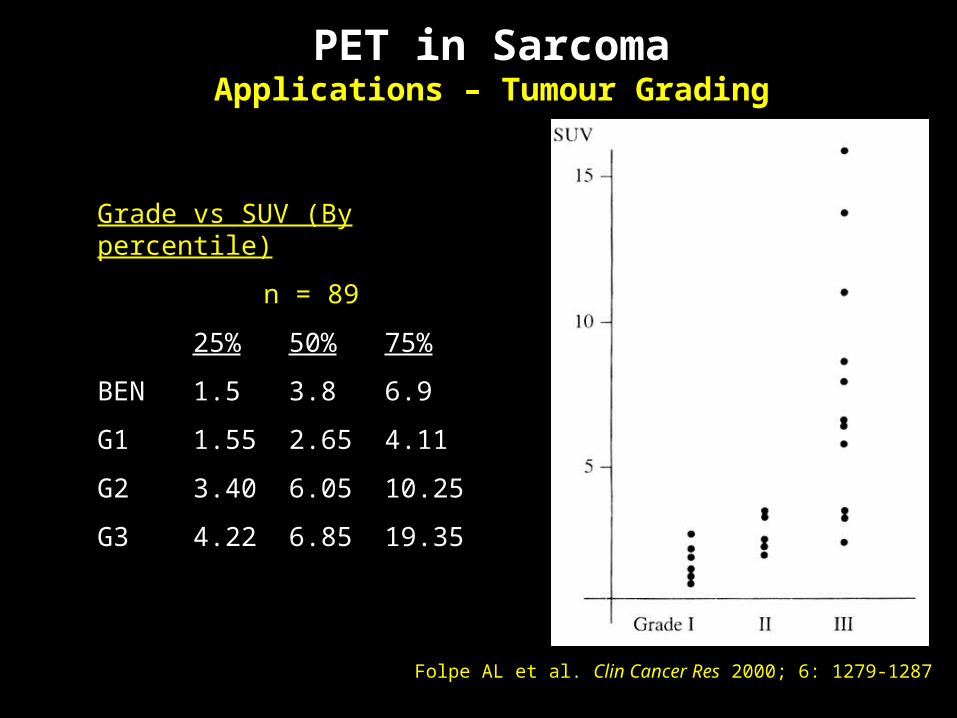
Folpe AL et al. Clin Cancer Res 2000; 6: 1279-1287
Grade vs SUV (By percentile)
n = 89
25% 50% 75%
BEN 1.5 3.8 6.9
G1 1.55 2.65 4.11
G2 3.40 6.05 10.25
G3 4.22 6.85 19.35
PET in SarcomaApplications – Tumour Grading
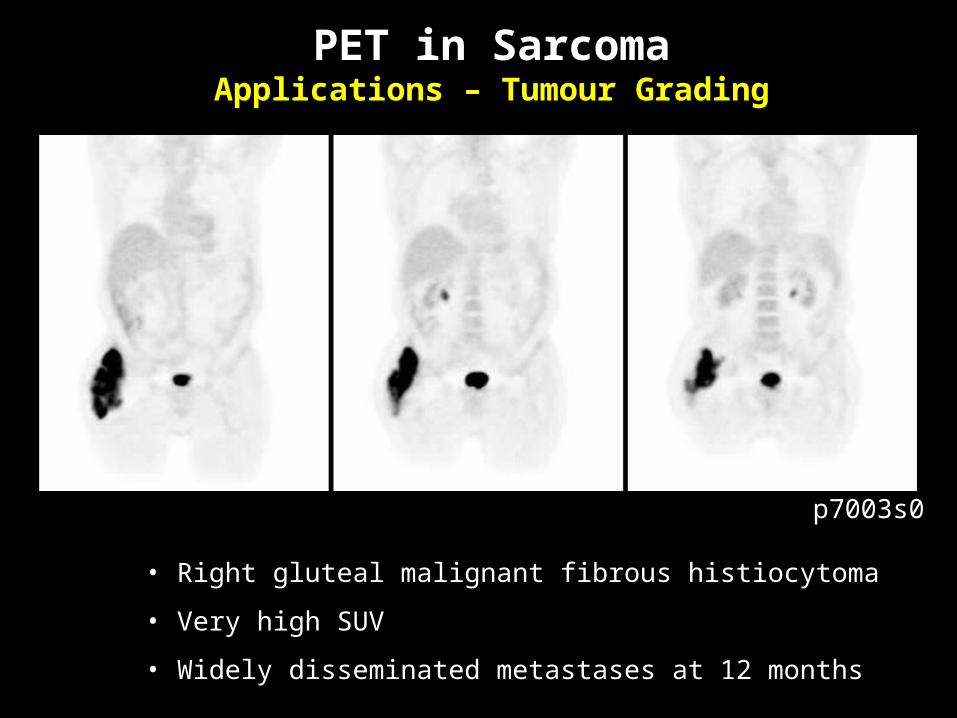
• Right gluteal malignant fibrous histiocytoma
• Very high SUV
• Widely disseminated metastases at 12 months
PET in SarcomaApplications – Tumour Grading
p7003s0
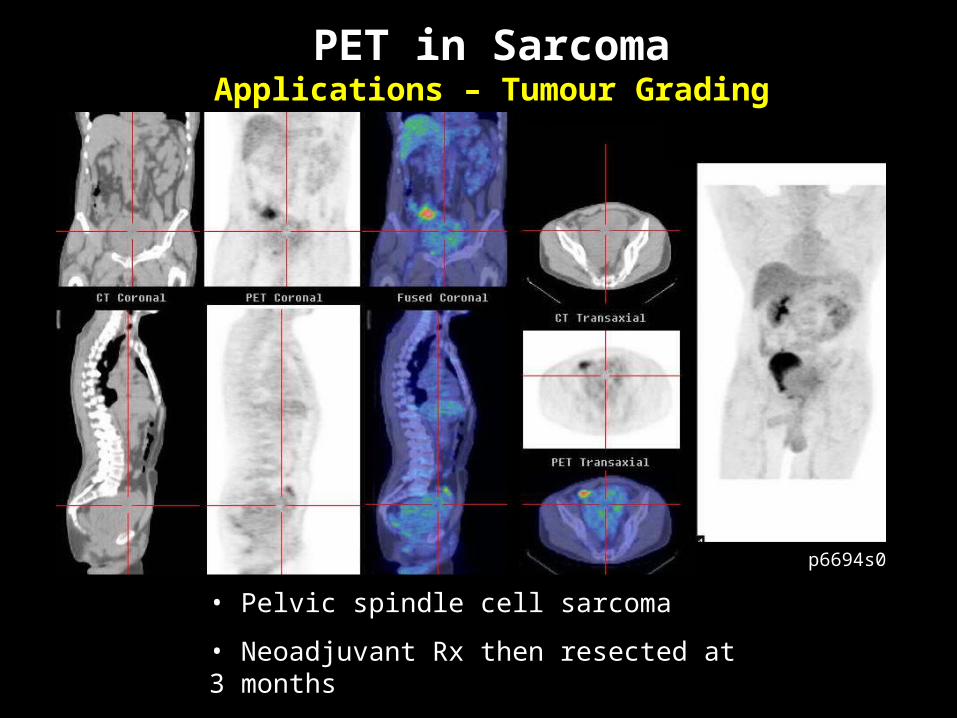
• Pelvic spindle cell sarcoma
• Neoadjuvant Rx then resected at 3 months
• No recurrence at 12 months
p6694s0
PET in SarcomaApplications – Tumour Grading

Functional Imaging with PET in Sarcoma
Potential Applications
• Benign versus malignant
• Grading
• Biopsy guidance
• Staging
• Therapeutic monitoring
• Restaging ( local recurrence)
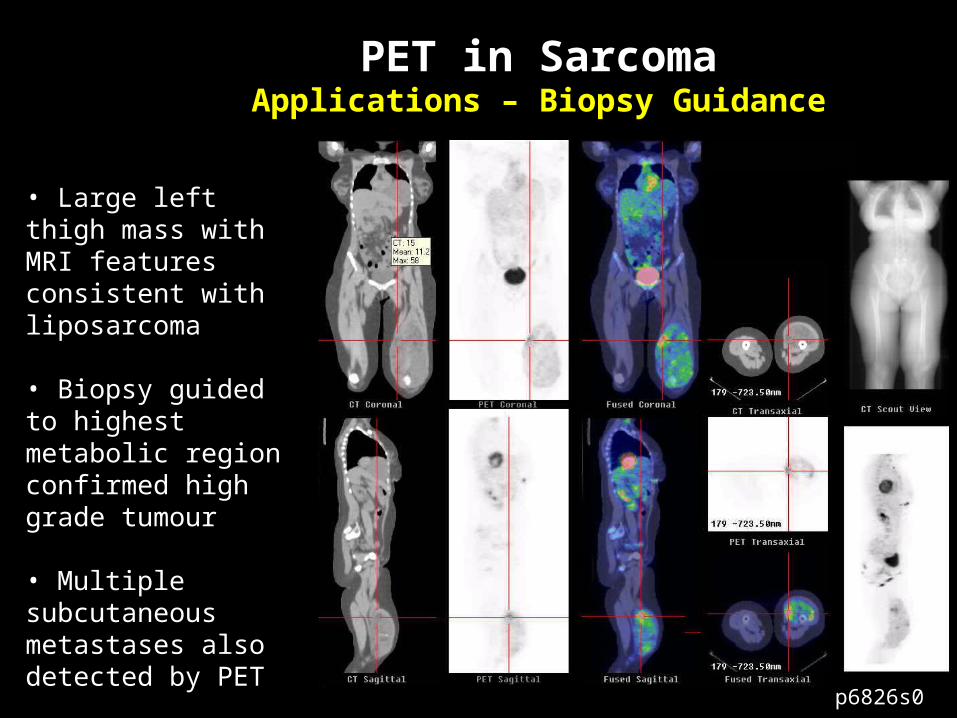
• Large left thigh mass with MRI features consistent with liposarcoma
• Biopsy guided to highest metabolic region confirmed high grade tumour
• Multiple subcutaneous metastases also detected by PET
PET in SarcomaApplications – Biopsy Guidance
p6826s0
Functional Imaging with PET in Sarcoma
Potential Applications
• Benign versus malignant
• Grading
• Biopsy guidance
• Staging
• Therapeutic monitoring
• Restaging ( local recurrence)
1. Franzius C et al Ann Oncol 2001; 12:479-486
2. Lucas JD et al J Bone Joint Surg Br 1998; 80:441-447
3. Franzius C et al Eur J Nucl Med 2000; 27:1305-1311
PET in SarcomaApplications - Staging
• CT is superior to stand-alone FDG PET for detecting lung mets (1,2)
• PET can identify false positive CT masses
• NPV is proportional to uptake in primary tumor
• FDG PET has higher sensitivity than CT for soft tissue metastases (2)
• Whole-body FDG PET may be superior to bone scan for bone metastases (3)
Franzius C et al Ann Oncol 2002;13:157-160
Garcia R et al J Nucl Med 1996; 37:1476-1479
el Zeftawy H et al Cancer Biother Radiopharm 2001; 16:37-46
Bredella M et al AJR 2002; 179:1145-1150
Johnson GR et al Clin Nucl Med 2003; 28:815-820
• FDG-PET is not disabled by metal susceptibility or metal beam hardening artefacts
• Multiple studies indicating good accuracy of FDG PET for detecting late local recurrence
PET in SarcomaApplications – Suspected Local Recurrence
Functional Imaging with PET in Sarcoma
Potential Applications
• Benign versus malignant
• Grading
• Biopsy guidance
• Staging
• Therapeutic monitoring
• Restaging ( local recurrence)
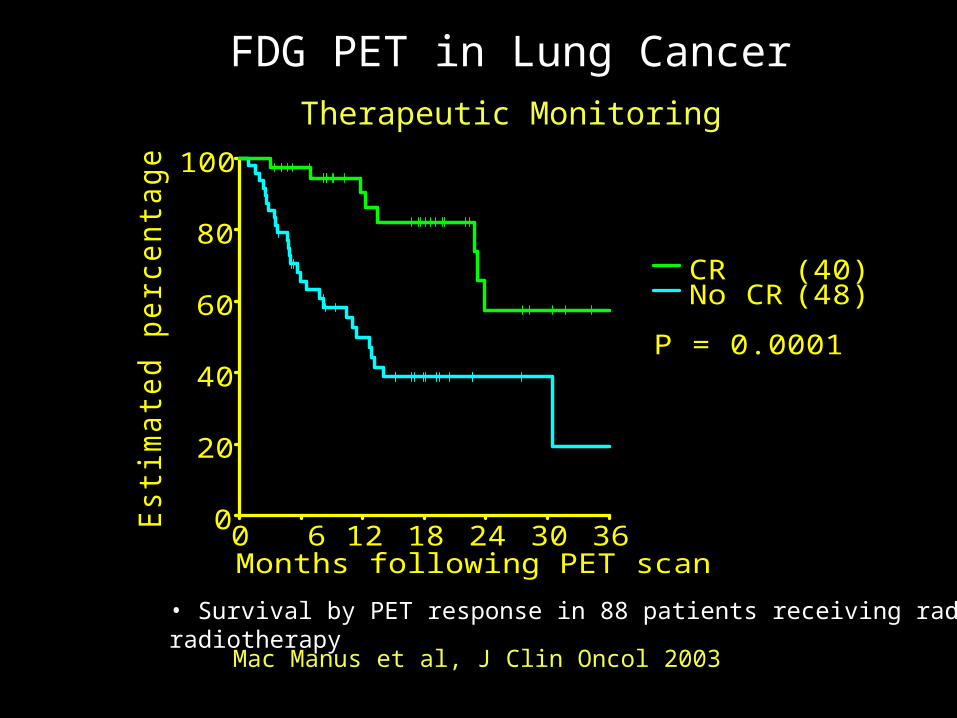
• Survival by PET response in 88 patients receiving radical radiotherapy
Mac Manus et al, J Clin Oncol 2003
FDG PET in Lung CancerTherapeutic Monitoring
0
20
40
60
80
100E
stim
ate
d p
erc
en
tag
e s
urv
ivin
g
0 6 12 18 24 30 36Months following PET scan
CRNo CR
(40)(48)
P = 0.0001
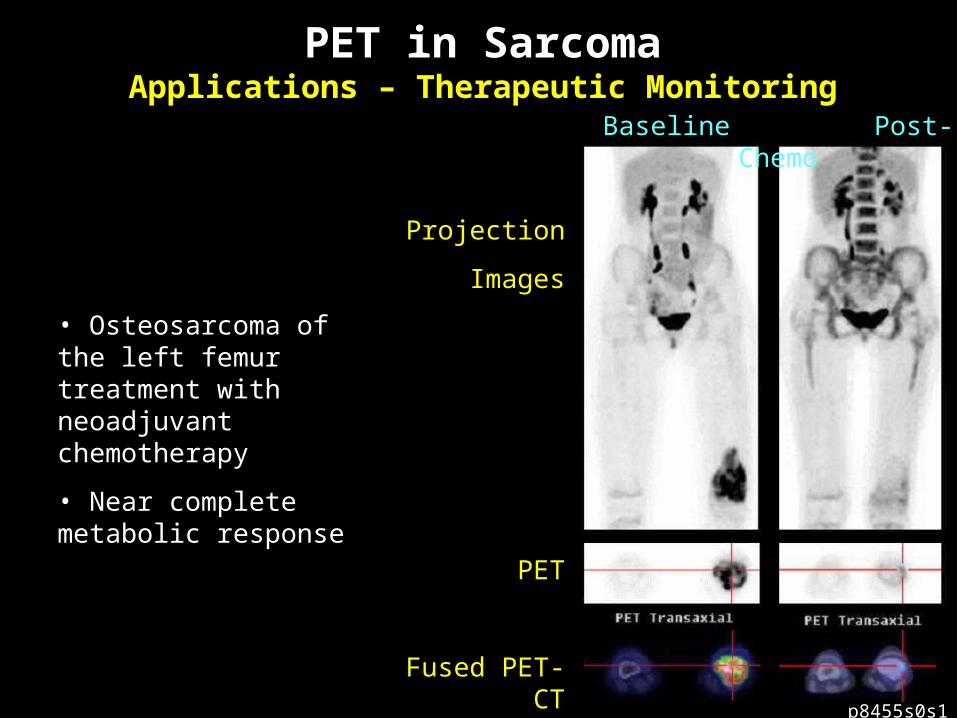
• Osteosarcoma of the left femur treatment with neoadjuvant chemotherapy
• Near complete metabolic response
PET in SarcomaApplications – Therapeutic Monitoring
p8455s0s1
Baseline Post-Chemo
Projection
Images
PET
Fused PET-CT
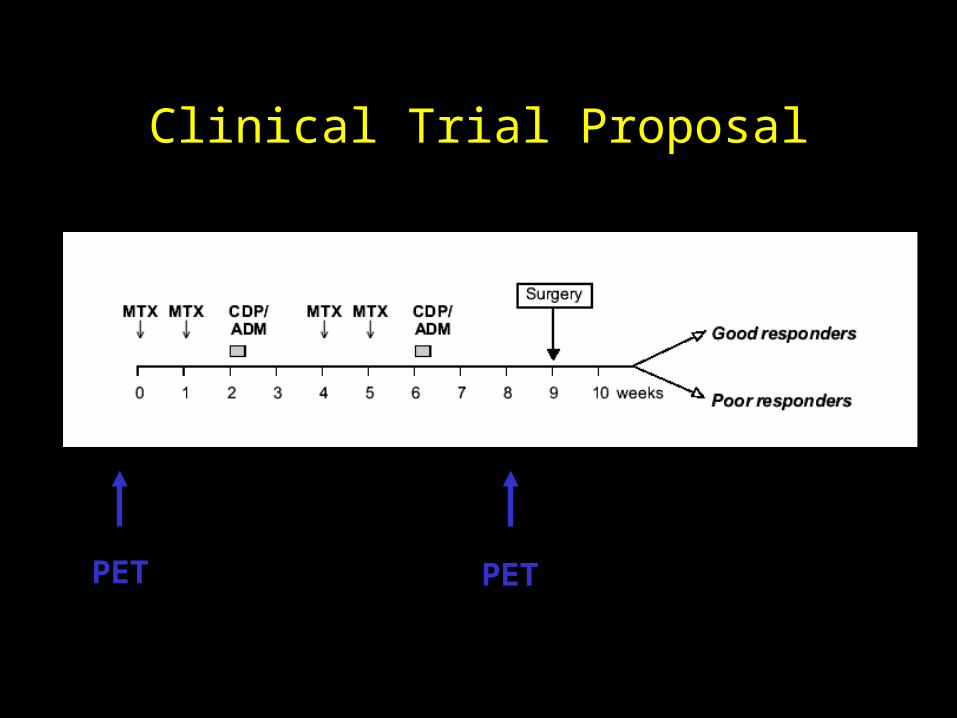
Clinical Trial Proposal
PET PET
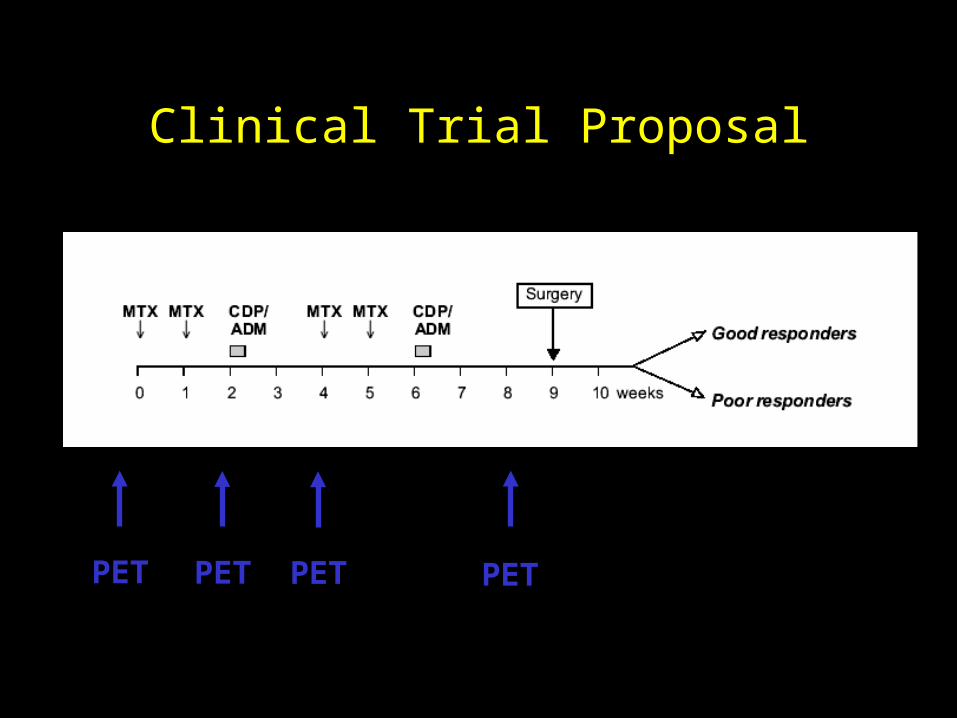
Clinical Trial Proposal
PET PETPET PET
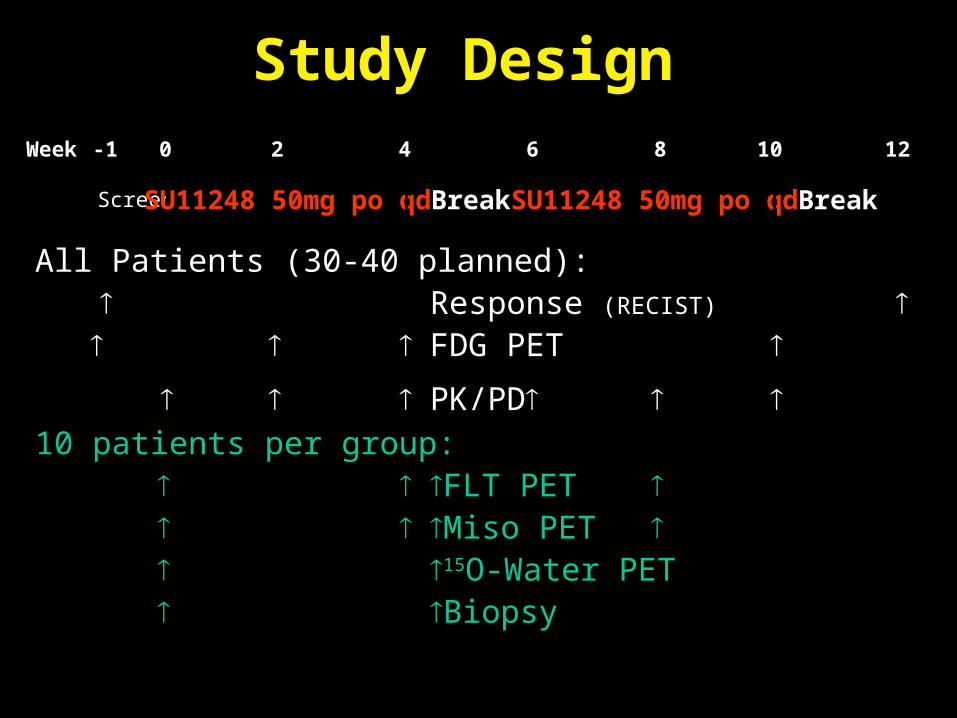
Study Design
-1
Screen SU11248 50mg po qd Break SU11248 50mg po qd Break
0 4 6 10 12Week 2 8
All Patients (30-40 planned): Response (RECIST) FDG PET
PK/PD 10 patients per group:
FLT PET Miso PET 15O-Water PET Biopsy
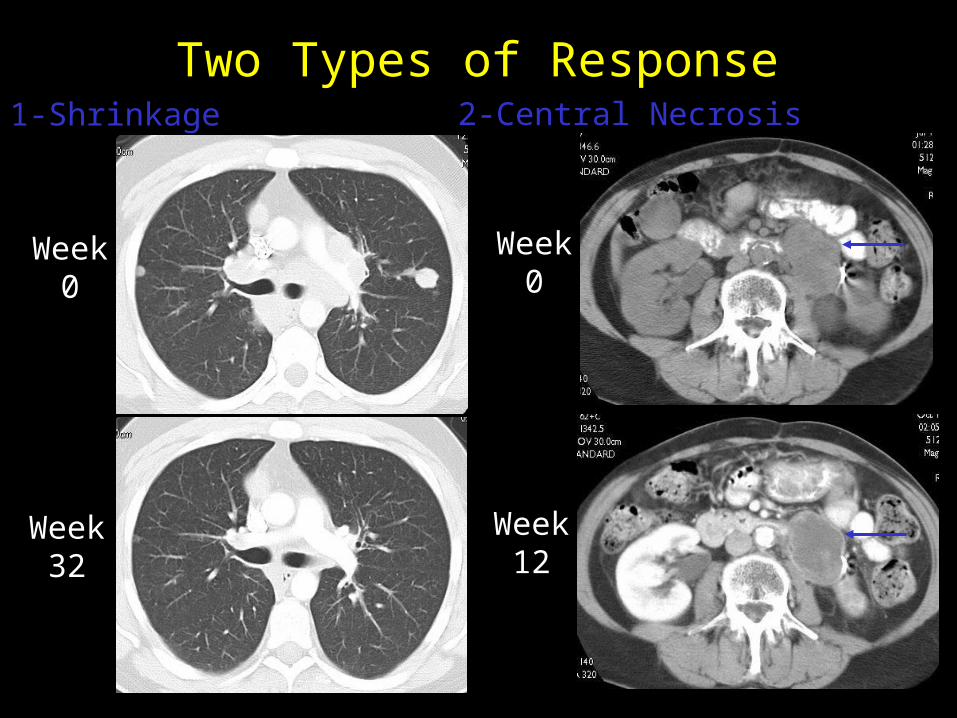
Two Types of Response
Week0
Week32
Week0
Week12
1-Shrinkage 2-Central Necrosis
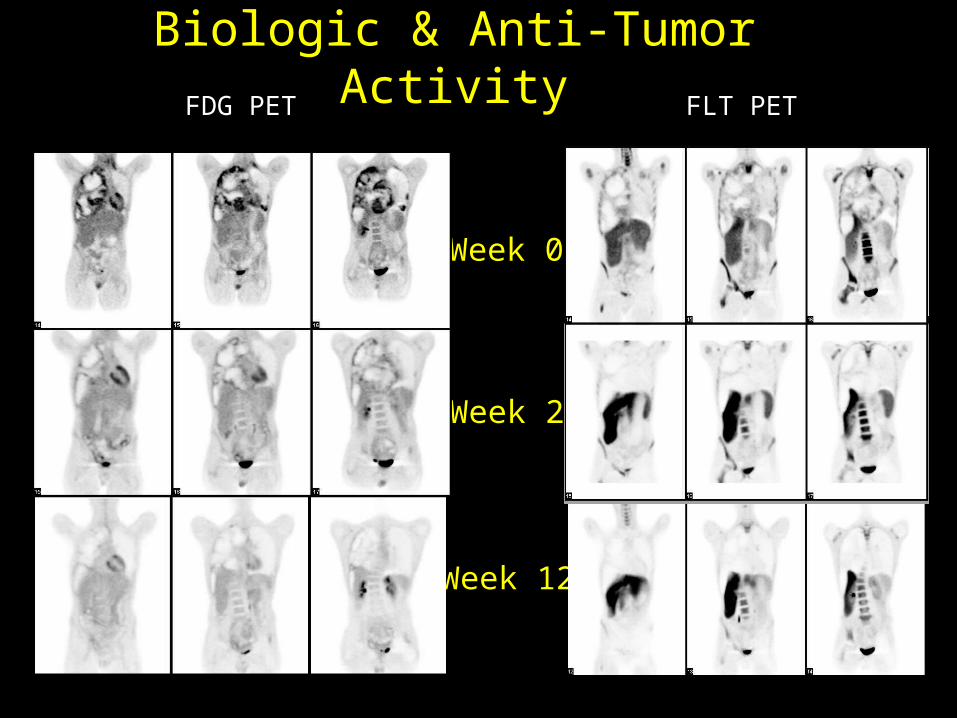
Biologic & Anti-Tumor ActivityFDG PET FLT PET
Week 2
Week 12
Week 0
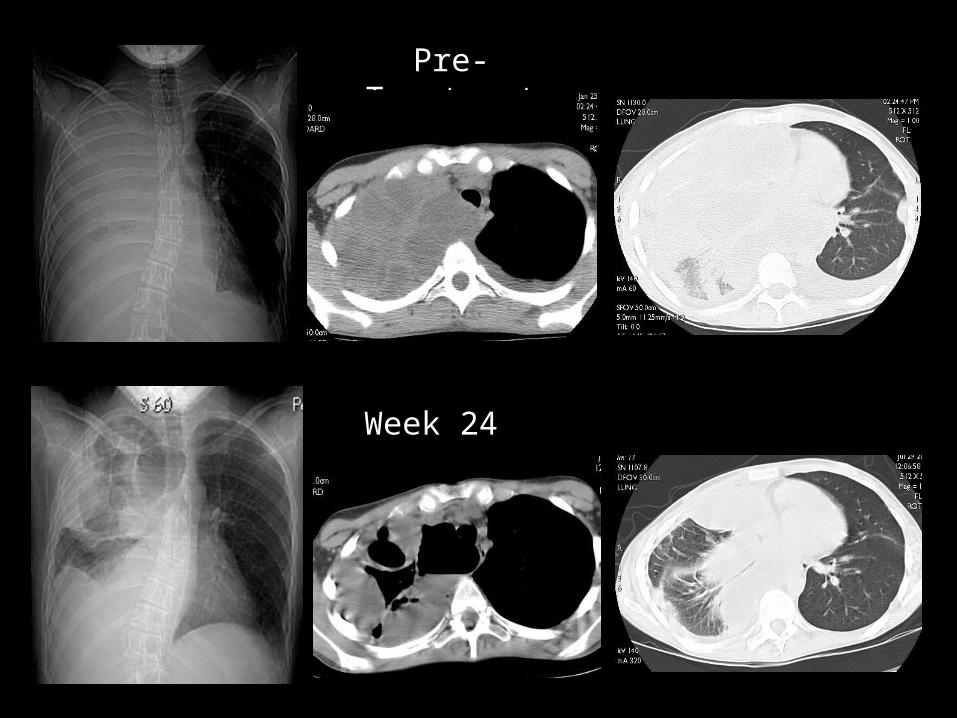
Pre- Treatment
Week 24
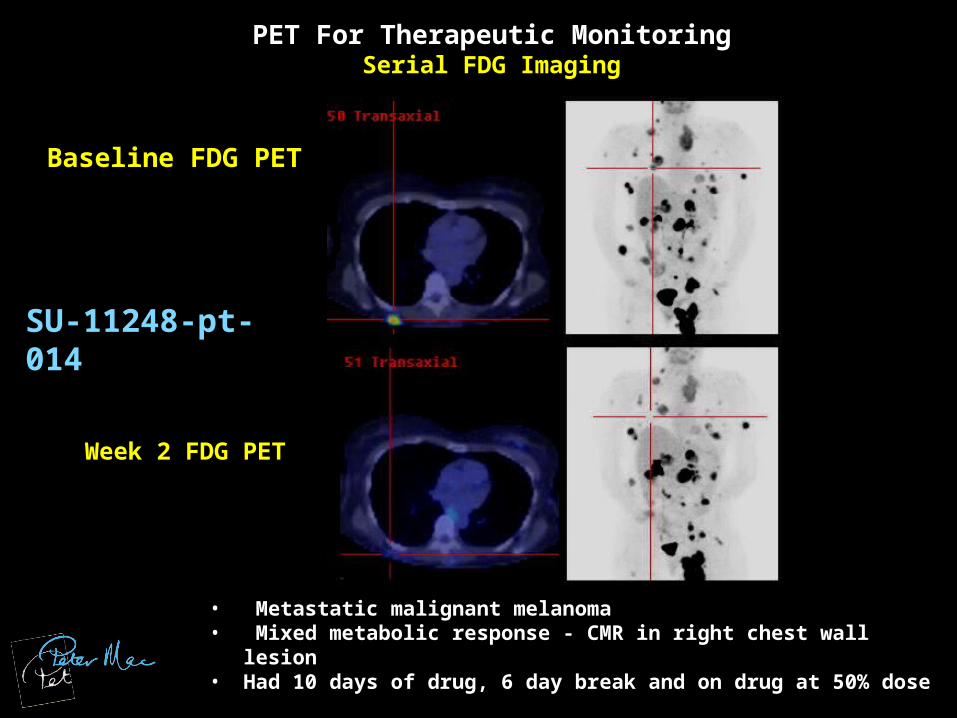
PET For Therapeutic MonitoringSerial FDG Imaging
• Metastatic malignant melanoma• Mixed metabolic response - CMR in right chest wall lesion• Had 10 days of drug, 6 day break and on drug at 50% dose
Baseline FDG PET
Week 2 FDG PET
SU-11248-pt-014
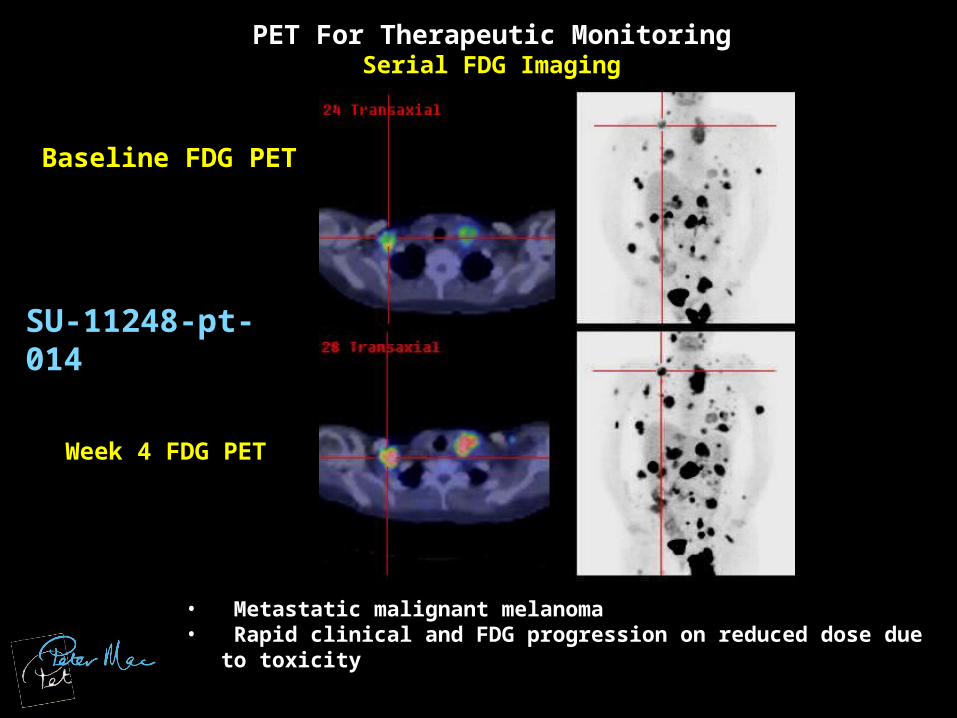
PET For Therapeutic MonitoringSerial FDG Imaging
• Metastatic malignant melanoma• Rapid clinical and FDG progression on reduced dose due to toxicity
Baseline FDG PET
Week 4 FDG PET
SU-11248-pt-014
Functional Imaging with PET in Sarcoma
Potential Applications - Conclusions
• Grading & Benign versus Malignant
provides useful complementary information
must be considered in context of clinical picture
chondroid matrix and sclerosing liposarcoma may produce false negative result
further studies required to determine if independently prognostic
• Biopsy guidance
very valuable, particularly PET/CT
Functional Imaging with PET in Sarcoma
Potential Applications - Conclusions
• Staging & re-staging
useful whole-body screen
NPV proportional to uptake in primary tumor
helpful in assessing possible local recurrence
• Therapeutic monitoring
potentially of enormous clinical value
changes evident rapidly (weeks)
further studies required to improve quantification of response
potential advantages for alternative tracers e.g. FLT