Embed Size (px)
Citation preview

Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
1977GASTROINTESTINAL IMAGING
Andrei S. Purysko, MD • Erick M. Remer, MD • Christopher P. Coppa, MD • Hilton M. Leão Filho, MD • Chakradhar R. Thupili, MD • Joseph C. Veniero, MD, PhD
Hepatocellular carcinoma (HCC) is a global health problem, with the burden of disease expected to increase in the coming years. Patients who are at increased risk for developing HCC undergo routine imag-ing surveillance, and once a focal abnormality is detected, evaluation with multiphasic contrast material–enhanced computed tomography or magnetic resonance imaging is necessary for diagnosis and staging. Currently, findings at liver imaging are inconsistently interpreted and reported by most radiologists. The Liver Imaging–Reporting and Data System (LI-RADS) is an initiative supported by the American College of Radiology that aims to reduce variability in lesion interpretation by standardizing report content and structure; improving communication with clinicians; and facilitating decision making (eg, for transplanta-tion, ablative therapy, or chemotherapy), outcome monitoring, perfor-mance auditing, quality assurance, and research. Five categories that follow the diagnostic thought process are used to stratify individual observations according to the level of concern for HCC, with the most worrisome imaging features including a masslike configuration, arterial phase hyperenhancement, portal venous phase or later phase hypoenhancement, an increase of 10 mm or more in diameter within 1 year, and tumor within the lumen of a vein. LI-RADS continues to evolve and is expected to integrate a series of improvements in future versions that will positively affect the care of at-risk patients.
©RSNA, 2012 • radiographics.rsna.org
LI-RADS: A Case-based Review of the New Categorization of Liver Findings in Patients with End-Stage Liver Disease1
ONLINE-ONLY CME
See www.rsna .org/education
/search/RG
LEARNING OBJECTIVES
After completing this journal-based CME activity, participants
will be able to:
■ Discuss the con-cepts and impor-tance of LI-RADS.
■ Describe the de-fining criteria for each LI-RADS cat-egory and ancillary features that favor HCC or benignity.
■ Enumerate the terms used in LI-RADS.
Abbreviations: ACR = American College of Radiology, HASTE = half-Fourier acquisition single-shot turbo spin-echo, HCC = hepatocellular car-cinoma, LAVA = liver acquisition with volume acceleration, LI-RADS = Liver Imaging–Reporting and Data System, OPTN = Organ Procurement and Transplantation Network, UNOS = United Network for Organ Sharing, VIBE = volumetric interpolated breath-hold examination
RadioGraphics 2012; 32:1977–1995 • Published online 10.1148/rg.327125026 • Content Codes: 1From the Abdominal Imaging Section, Imaging Institute, HB6, Cleveland Clinic, 9500 Euclid Ave, Cleveland, OH 44195 (A.S.P., E.M.R., C.P.C., C.R.T., J.C.V.); and HCor, Hospital do Coração and Teleimagem, São Paulo, Brazil (H.M.L.F.). Recipient of a Certificate of Merit award for an education exhibit at the 2011 RSNA Annual Meeting. Received March 6, 2012; revision requested April 12 and received April 25; accepted May 8. For this journal-based CME activity, the authors, editor, and reviewers have no relevant relationships to disclose. Address correspondence to A.S.P. (e-mail: [email protected]).
©RSNA, 2012
INVITED COMMENTARY
See discussion on this article by Sirlin (pp 1995–1998).

1978 November-December 2012 radiographics.rsna.org
IntroductionLiver cancer is the fifth most common cancer in men and the seventh most common cancer in women, with a male-female ratio of 2.4:1. The very poor prognosis associated with this disease makes it the third leading cause of cancer-related mortality worldwide, with an estimated 694,000 deaths in 2008 (1). Hepatocellular carcinoma (HCC) is the predominant primary liver cancer in most countries; thus, variations in liver cancer rates are believed to reflect trends in HCC inci-dence (2). In the United States, approximately 90% of primary liver cancers are HCCs; most of the remaining 10% are intrahepatic cholangiocar-cinomas (3).
HCC is a global health problem, with the bur-den of disease expected to grow in the coming years (4,5). Past growth has been partially attrib-uted to an epidemic of hepatitis C virus infection during the 1960s and, in more recent decades, to the rising rates of obesity and diabetes, both of which are associated with nonalcoholic fatty liver disease (4).
The most important risk factor for the devel-opment of HCC is liver cirrhosis, regardless of its etiology (6). Among patients with cirrhosis, those with chronic viral infection (hepatitis B and C) and high alcohol intake have the highest risks of HCC development (7,8). In patients who are at increased risk, imaging surveillance is a widely accepted measure that increases the likelihood of early detection of HCC (8–10).
Technical advances in multidetector computed tomography (CT) and faster high-resolution mag-netic resonance (MR) imaging sequences have improved the ability of these imaging modalities to demonstrate the typical features of HCC (11–13), leading to an increased role for imaging in the di-agnosis of HCC. A recent study conducted by the National Cancer Institute demonstrated that from 1992 to 2008, the incidence of histologically un-confirmed HCC increased 2.5 times more rapidly than that of confirmed HCC. This trend reflects changing clinical practice guidelines, according to which pretreatment biopsy is no longer indicated when appropriately performed imaging tests show typical features of HCC (14).
Regardless of the imaging modality used, the imaging report is an essential part of the service provided to patients with cirrhosis. It is of para-mount importance, therefore, that the report be uniform, comprehensive, and easily managed
(15). The current free-text reporting model precludes the creation of referenceable report databases, which are essential to large-scale re-port data analysis (16). In addition, reporting and interpretation of imaging findings in patients with cirrhosis have been found to be inconsistent (17,18). Because there is no standard lexicon, ra-diologists use different terms to convey the same interpretation, and observations are interpreted inconsistently. These problems limit clinicians’ ability to compare findings and outcomes both within and between institutions (19,20).
Structured radiology reporting may improve patient care by increasing clarity and thorough-ness in the communication of imaging findings; such reporting allows information to be stan-dardized and presented in a clear and organized fashion, tracking the attributes of each obser-vation (eg, lesion location and size) (21). The Breast Imaging–Reporting and Data System (BI-RADS), the first practice management system developed for imaging by the American College of Radiology (ACR), has proved to be a very suc-cessful tool that has positively affected the care of patients with breast disease (16). The U.S. Food and Drug Administration, recognizing the advan-tages of structured reporting, mandated use of the BI-RADS for all mammography reports (21).
Following in the footsteps of its successful predecessor, the Liver Imaging–Reporting and Data System (LI-RADS) is an ACR-supported initiative to develop a standardized reporting and data collection system, along with minimum ac-ceptable technical parameters, for CT and MR imaging of the liver in patients undergoing HCC surveillance. The initial phase of the system was developed at the University of California–San Di-ego, and was later combined with an equivalent system being developed at Thomas Jefferson Uni-versity Hospital in Philadelphia, Pennsylvania. The LI-RADS Committee was then created, with representatives from institutions throughout the United States now actively engaged in developing the system further (19).
The goals of LI-RADS include reducing vari-ability in lesion interpretation; improving com-munication with clinicians; facilitating decision-making processes (eg, for transplantation, ablative therapy, or chemotherapy); reducing omissions of relevant information from CT and MR imaging reports by standardizing report content and struc-ture; and facilitating outcome monitoring, perfor-mance auditing, quality assurance, and research (22).

RG • Volume 32 Number 7 Purysko et al 1979
In this article, we discuss the rationale of LI-RADS and the terminology used in the system, the major and ancillary features that are used to categorize imaging observations on CT and MR images of cirrhotic livers, and the implications of using imaging criteria to diagnose HCC prior to liver transplantation.
The information presented in this article is based on the first version of the system officially released on the ACR website (www.acr.org), where updates can be found.
LI-RADS OverviewLI-RADS assigns imaging findings to one of five categories (Table 1), allowing radiologists to stratify individual observations―not the entire
liver―according to the level of concern for HCC. The term observation is used instead of lesion be-cause some observations may actually correspond to areas that are not histologically distinct from the adjacent parenchyma, such as areas of perfu-sion alteration.
The LI-RADS categories are used to classify observations as either a “definite” HCC (LR-5) or definitely benign (LR-1) with a method that matches the diagnostic thought process (19,23,24). If some, but not all, imaging features of an HCC or benign observation are present, the categories LR-4 (probably HCC) and LR-2 (probably benign) can be used. The middle
Table 1 Imaging Features of Observations by LI-RADS Category
Category Description Imaging Features
LR-1 Definitely benign Features that are diagnostic for a benign entity, or definite disappear-ance in the absence of treatment
LR-2 Probably benign (a) Features suggestive of a benign entity; or (b) stable imaging fea-tures for ≥2 y, no increase in diameter for ≥2 y, and failure to meet criteria for LR-1, LR-4, or LR-5; or (c) probable disappearance in the absence of treatment
LR-3 Intermediate probability of being HCC
<20 mm: (a) masslike configuration with arterial phase hyperen-hancement and no additional major features,* or (b) masslike configuration with arterial phase hypoenhancement and no more than one additional major feature*
≥20 mm: masslike configuration with arterial phase hypoenhance-ment and no additional major features*
Any size: (a) nonmasslike configuration and neither definitely nor probably benign; or (b) cannot be categorized as LR-1, LR-2, LR-4, or LR-5 because of equivocal imaging features; or (c) meets criteria for LR-4 or LR-5, with stable imaging features and size for ≥2 y
LR-4 Probably HCC Category A (<20 mm): (a) masslike configuration with arterial phase hyperenhancement and one additional major feature,* or (b) masslike configuration with arterial phase iso- or hypoen-hancement and two additional major features,* or (c) probable tumor within lumen of vein
Category B (≥20 mm): (a) masslike configuration with arterial phase hyperenhancement and no additional major features,* or (b) mass-like configuration with arterial phase iso- or hypoenhancement and one or two additional major features,* or (c) probable tumor within lumen of vein
LR-5 Definitely HCC Category A (≥10 mm but <20 mm): (a) masslike configuration with arterial phase hyperenhancement and two additional major fea-tures,* or (b) definite tumor within lumen of vein
Category Β (≥20 mm): (a) masslike configuration with arterial phase hyperenhancement and one or two additional major features,* or (b) definite tumor within lumen of vein
Source.―Adapted, with permission, from reference 22.*Additional major features: portal venous phase or later phase hypoenhancement, increase in diameter of at least 10 mm within 1 year.

1980 November-December 2012 radiographics.rsna.org
category, LR-3, is used for indeterminate ob-servations that do not have specific features that allow them to be characterized as more probably benign or HCC (22).
The current version of LI-RADS applies to un-treated observations only and should be used only for patients at risk for HCC. The classification also applies only to CT and MR images obtained with extracellular contrast agents. Given the growing interest in and knowledge of hepatocyte-specific MR imaging contrast agents, particularly gadox-etic acid disodium (gadoxetate disodium, or Gd-EOB-DTPA) (Eovist or Primovist; Bayer Health-care, Leverkusen, Germany), we expect their inte-gration in future versions of the system (19).
Major Imaging Features That Favor HCC
Before we discuss the defining criteria used for each category, it is important to review the five major features used by the system that favor the diagnosis of HCC (Fig 1). Observations are char-acterized as LR-5 or LR-4 primarily on the basis of their size and the presence of these features.
Masslike ConfigurationAn observation that represents a space-occupying process is described as masslike. Features sug-gesting a mass as described by LI-RADS include ring enhancement during the portal venous phase or later (equivalent to a capsule or pseudocap-sule); visibility on images obtained prior to the administration of contrast material and on diffu-sion-, T2-, or T2*-weighted images; discrete mar-gins; rounded shape; focal deformity of the liver contour; and displacement of intraparenchymal structures (22).
Arterial Phase HyperenhancementAll or part of the observation must demonstrate greater enhancement than the surrounding liver parenchyma during the arterial phase.
Arterial phase hyperenhancement is the single most consistently seen feature in patients with HCC and is considered to be the most impor-
tant feature for imaging diagnosis of the disease (13,24,25). This feature reflects the development of anomalous arterial vascularization (neoangio-genesis), which is associated with the stepwise pro-cess of carcinogenesis and becomes the dominant blood supply in overt HCC lesions (26,27). Note that many factors, including portal hypertension, may cause a delay in organ enhancement dynam-ics; therefore, in some patients, hyperenhancement may be more evident on portal venous phase im-ages than on arterial phase images (22).
Portal Venous Phase or Later Phase HypoenhancementPortal venous phase or later phase hypoenhance-ment is also considered a strong predictor of HCC, particularly when combined with arterial phase hyperenhancement (28), and is popularly referred to as “washout,” although this term is not included in the LI-RADS lexicon. Hypoen-hancement seen during the portal venous phase or later is believed to be caused not only by early venous drainage, but also by the decreased portal venous supply to HCC that accompanies neo-angiogenesis, resulting in greater enhancement of the surrounding liver parenchyma than of the HCC in those phases (28,29).
In an observation that demonstrates arterial phase hypoenhancement, the attenuation or sig-nal intensity during the portal venous phase or later must be unequivocally less than during an earlier phase to be assigned this major imaging feature (ie, portal venous phase [or later phase] hypoenhancement). It is important to ensure that the observation demonstrates unequivocal enhancement compared with the precontrast phase, and that the determination of portal ve-nous phase or later phase hypoenhancement is compared with the same portion of the observa-tion for which the determination of arterial phase enhancement is made.
Fibrotic tissue in cirrhotic livers typically dem-onstrates delayed enhancement. This may cause a false appearance of hypoenhancement of a regen-erative nodule or hypertrophic pseudomass when these are surrounded by fibrosis. In some cases,
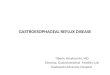
Figure 1. Drawings illustrate the five major features used by LI-RADS that favor the diagnosis of HCC: masslike configuration (A), arterial phase hyperenhancement (B), portal venous phase or later phase hypoenhancement (C), increase of 10 mm or more in diameter within 1 year (D), and tumor within the lumen of a vein (E).

RG • Volume 32 Number 7 Purysko et al 1981
fibrotic tissue may even mimic a delayed enhanc-ing capsule or pseudocapsule (22,30).
Increase of 10 mm or More in Diameter within 1 YearInterval growth is highly predictive of HCC and is particularly important at follow-up imaging for the characterization of initially small (<2-cm) lesions lacking the classic imaging features of HCC (31–33). If follow-up imaging is per-formed more than 1 year later, a similar rate of growth (ie, change in size per unit of time) should be applied (22).
Tumor within Lumen of VeinThe imaging criteria for definite and probable tu-mor within a vein are described in Table 2. Vascu-
lar invasion in HCC carries a poor prognosis (34) and occurs by means of direct tumor invasion into the adjacent portal vein or, less commonly, a hepatic vein (35,36).
Early enhancement of the portal veins mim-icking an enhancing tumor thrombus can occur when there is a late timing of the arterial phase or in the presence of arterioportal shunting or retrograde (hepatofugal) flow. Similarly, early enhancement of the hepatic veins can occur as a result of arteriovenous shunting or retrograde flow (reflux) into the hepatic veins from the right atrium and suprahepatic inferior vena cava (22). Tumor thrombus is in general heterogeneous, whereas shunted contrast material or retrograde flow tends to be more homogeneous.
Patients with cirrhosis can also develop benign portal vein thrombosis secondary to portal hyper-tension and venous stasis (36). A bland thrombus is usually not associated with significant expan-sion of the vessel, does not demonstrate contrast enhancement, and has low signal intensity at T2-weighted MR imaging due to the presence of hemosiderin content (25). Differentiating a bland thrombus from a tumor thrombus can be chal-lenging, especially when the latter is surrounded by cavernous transformation.
Ancillary Imaging Features That Favor HCC
In addition to these major features, there are ancillary features that favor the diagnosis of HCC (Table 3). With caution, ancillary features that favor HCC may be used to classify LR-4 or LR-5 observations that do not meet major feature criteria for those two categories (Fig 2) (22). Although some ancillary features such as
Table 2 Features of a Tumor within the Lumen of a Vein
Description Features
Definite tumor Unequivocal arterial phase hyperenhancement and venous phase hypoenhancement in lumenProbable tumor* Probable arterial phase hyperenhancement in lumen
Probable venous phase hypoenhancement in lumenOccluded vein with expanded lumenLuminal enhancement but late venous phase or delayed phase enhancement of the lumen
does not match that of patent veinsMarkedly restricted or impeded diffusion in lumenIll-defined hypoenhancing tubular structures in expected course and location of veinsPresence of arteries within lumen†
Source.―Adapted, with permission, from reference 22.*One or more of the features listed must be present.†Does not apply if the arteries represent cavernous transformation around a bland thrombus or occlusion.
Table 3 Ancillary Features That Favor HCC
Mild to moderate T2 hyperintensityCapsule or pseudocapsule*Mosaic architecture†
High signal intensity on diffusion-weighted images, restricted or impeded diffusion
Fat deposition disproportionate to that in the sur-rounding liver
Iron sparing in an iron-overloaded liver
Source.―Adapted, with permission, from refer-ence 22.*Discrete ring along the lesion margin that is thicker or of greater conspicuity than the ring along the margin of regenerative nodules in the surrounding liver.†Includes nodule-in-nodule and multinodule-in-nodule appearances and the presence of discrete internal compartments or elements within the observation.

1982 November-December 2012 radiographics.rsna.org
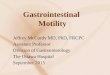
Figure 2. Ancillary features that favor the diagnosis of HCC. (a–c) Axial gadopentetate dimeglu-mine (Gd-DTPA)–enhanced fat-suppressed T1-weighted volumetric interpolated breath-hold ex-amination (VIBE) images obtained during the arterial (a), portal venous (b), and equilibrium (c) phases show a 1.5-cm observation that is hyperenhancing during the arterial phase (arrow in a) and hypoenhancing during the portal venous phase (black arrow in b) and later venous phases, with an enhancing capsule or pseudocapsule (white arrow in b). (d) On an axial T2-weighted half-Fourier ac-quisition single-shot turbo spin-echo (HASTE) (Siemens Medical Solutions, Malvern, Pa) image, the observation is mildly hyperintense (arrow). (e, f) Axial in-phase (e) and out-of-phase (f) T1-weighted gradient-echo images show signal loss with the out-of-phase sequence (arrow in f), a finding that is compatible with intratumoral fat. The observation is compatible with category LR-4 based on its size and major imaging features (masslike configuration, arterial phase hyperenhancement, and portal ve-nous phase hypoenhancement), but the presence of several ancillary features that favor the diagnosis of HCC requires categorization of this observation as LR-5A.

RG • Volume 32 Number 7 Purysko et al 1983
a capsule or pseudocapsule and mosaic archi-tecture (Fig 3) can be identified on both CT and MR images, several of these features are either MR imaging specific (eg, T2 signal and restricted diffusion) or are better seen at MR imaging (eg, intratumoral fat) (18).
Gadolinium-enhanced MR imaging has proved to be more sensitive and specific than ultrasonography (US) or CT for the diagnosis of HCC owing to better detection of the typical en-hancement pattern (11,37–39). In addition, MR imaging allows simultaneous evaluation of the
background liver parenchyma and liver lesions when a combination of sequences is used (eg, T2-weighted sequences, T1-weighted sequences [including in-phase and out-of-phase imaging], diffusion-weighted sequences, and dynamic gad-olinium-enhanced three-dimensional multiphase imaging). The use of such sequences in combina-tion frequently elucidates the nature of both focal and diffuse liver abnormalities, thereby improving the ability to diagnose HCC (Fig 4) (40).
Figure 3. HCC with mosaic architecture in a 50-year-old man with cirrhosis. Axial contrast mate-rial–enhanced arterial phase (a) and portal venous phase (b) CT scans show a 6-cm mass in the right hepatic lobe (arrow) that has discrete compartments with different enhancement patterns, including areas of arterial phase hyperenhancement that become hypoattenuating during the portal venous phase, interspersed with areas of hypoenhancement in both the arterial and portal venous phases. The term mosaic architecture can also be applied to observations with a nodule-in-nodule or multinodule-in-nodule appearance. Delayed venous phase CT revealed an enhancing capsule or pseudocapsule.
Figure 4. HCC in a 60-year-old man with an iron-overloaded cirrhotic liver. (a) Axial T2-weighted fast spin-echo MR image demonstrates diffuse nodular low signal intensity of the liver parenchyma, a finding that is compatible with iron overload, except for a masslike area of sparing in the posterior right hepatic lobe that is mildly hyperintense (*). (b) Axial gadolinium-enhanced fat-suppressed T1-weighted liver acquisition with volume acceleration (LAVA) image obtained during the delayed venous phase shows an encapsulated mass (arrow) in the area of iron sparing.

1984 November-December 2012 radiographics.rsna.org
Figure 5. Multiple observations with ancillary features that suggest benignity in a 40-year-old man with a history of Budd-Chiari syndrome. (a) Axial T2-weighted HASTE image shows a markedly hyperintense observation (black arrow), as well as a 4-cm mass in the right hepatic lobe with a hyperintense central scar (white arrow). (b–d) On axial Gd-EOB-DTPA–enhanced fat-suppressed T1-weighted VIBE images obtained during the arterial (b), portal venous (c), and 20-minute-delayed hepatocyte-specific (d) phases, the markedly hyperintense observation seen in a has nodular discontinuous centripetal enhancement during the arterial and portal venous phases (black arrow in b and c) and becomes completely hypointense in the hepatocyte phase (black arrow in d). These features are typical for hemangioma. The mass in the right hepatic lobe (arrowhead in b, white arrow in c and d) demonstrates persistent hyperenhancement, except for the central scar (white arrow in b), which has no enhancement during any of the three phases. Multiple additional smaller observations with similar features are scattered throughout the liver. Benign hyperenhancing hyperplastic nodules (some indis-tinguishable from focal nodular hyperplasia) are relatively common in certain clinical settings (eg, Budd-Chiari syndrome). Gd-EOB-DTPA–enhanced MR imaging findings have not been included in LI-RADS but will likely be incorporated in future versions of the system.
Table 4 Ancillary Features That Favor Benignity
Uniform marked T2 hyperintensityUniform marked T2 hypointensityPresence of normal undistorted vessels coursing through the observationEnhancement that follows blood pool characteristics on dynamic imagesProgressive enhancement of the observation (excluding septa and scars)Decrease in diameter of at least 10 mm in the absence of treatmentClinical setting*
Source.―Adapted, with permission, from reference 22.*In some clinical settings, hyperenhancing benign nodules are common (eg, hyperplastic nodules in Budd-Chiari syndrome).

RG • Volume 32 Number 7 Purysko et al 1985
Ancillary Imaging Features That Favor Benignity
LI-RADS also provides a list of ancillary features that favor benignity (Table 4). With caution, these features may be applied to downgrade the cat-egory of observations that otherwise meet major criteria for LR-4 or LR-5 (Fig 5) (22).
LI-RADS Categories
Category LR-5An LR-5 observation is a definite HCC (Fig 6). This category should be applied only when the radiologist is 100% certain that the observation is HCC. The imaging criteria used to categorize an observation as LR-5 are considered specific enough to render the diagnosis of HCC without the need for biopsy (22). These include arterial
phase hyperenhancing masses 10 mm or larger with one or two additional major features (hy-poenhancement during the portal venous phase or later, growth of 10 mm or more in 1 year, or both) (Table 1).
LR-5 observations are subdivided on the basis of size into categories A (≥10 mm but <20 mm) and B (≥20 mm). To increase its specificity, this criterion is more strict for observations at least 10 mm in size but smaller than 20 mm, since obser-vations of this size have been responsible for the misdiagnosis of HCC in a significant proportion of patients prior to their undergoing liver trans-plantation, in whom no corresponding HCC was
Figure 6. HCC in a 48-year-old man with alcoholic cirrhosis. (a–c) Axial contrast-enhanced CT scans obtained during the arterial (a), portal venous (b), and equilibrium (c) phases show a 3-cm hepatic mass that demonstrates arterial phase hyperenhancement (arrow in a) and equilibrium phase hypoenhancement (arrow in c). (d) On an axial arterial phase CT scan obtained 9 months earlier, the mass (arrow) measures only 2 cm. These features are consistent with category LR-5B.

1986 November-December 2012 radiographics.rsna.org
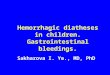
Figure 7. Tumor within the portal vein lumen in a 56-year-old man with chronic hepatitis C infec-tion. (a–c) Axial fat-suppressed T1-weighted VIBE images obtained without contrast material (a) and after the intravenous administration of Gd-DTPA during the arterial (b) and portal venous (c) phases show a tumor thrombus that expands the lumina of the right and left portal veins and demonstrates ar-terial phase hyperenhancement (arrow in b) and portal venous phase hypoenhancement. (d) Axial T2-weighted HASTE image shows the tumor thrombus with mild hyperintensity (arrow). (e) On an axial diffusion-weighted image, the tumor thrombus is hyperintense (arrow), a finding that is compatible with restricted diffusion. The spleen (arrowhead), an organ with normally restricted diffusion, can be used as a reference. (f) Corresponding apparent diffusion coefficient map shows the tumor thrombus with hypointense signal (arrow), a finding that confirms the presence of restricted diffusion. Arrowhead = spleen. Both mild T2 hyperintensity and restricted diffusion are considered ancillary features that favor the diagnosis of malignant thrombus.

RG • Volume 32 Number 7 Purysko et al 1987
identified in the explant (28,41). For category A observations, two additional major features are required for a definitive diagnosis of HCC; for category B observations, one or two additional major features are required (Table 1).
Observations with features of definite tumor within the lumen of a vein are also considered LR-5, regardless of whether other major imaging fea-tures suggestive of HCC are present (Figs 7, 8).
Figure 8. Tumor within the lumen of a hepatic vein in a 65-year-old man with alcoholic cirrhosis. (a, b) Axial Gd-DTPA–enhanced fat-suppressed T1-weighted VIBE images obtained during the arterial (a) and equi-librium (b) phases show a tumor thrombus (arrow) with hyperenhancement and hypoenhancement, re-spectively. (c, d) On axial (c) and coronal (d) T2-weighted HASTE images, the tumor thrombus is mildly hyperintense (arrow) and extends into the right atrium (arrowhead in d).

1988 November-December 2012 radiographics.rsna.org
Figures 9,10. (9) Probable HCC in a 49-year-old woman with chronic hepatitis B infection. (a) Axial precontrast fat-suppressed T1-weighted VIBE image shows a vague hypointense observation (arrow). (b, c) Axial Gd-DTPA–enhanced fat-suppressed T1-weighted VIBE images obtained during the arterial (b) and portal venous (c) phases reveal a 1.2-cm masslike lesion (arrow) with hyperenhance-ment and hypoenhancement, respectively, findings that are compatible with category LR-4A. (10) Prob-able HCC in a 50-year-old man with chronic hepatitis B infection. (a, b) Precontrast (a) and postcon-trast (b) arterial phase CT scans show a 3-cm masslike lesion (arrow) that is slightly hypoattenuating and isoenhancing, respectively, relative to the surrounding liver parenchyma. (c) On a portal venous phase CT scan, the lesion demonstrates hypoenhancement (arrow). All of these findings are compat-ible with category LR-4B.

RG • Volume 32 Number 7 Purysko et al 1989
Category LR-4An LR-4 observation is probably but not defi-nitely an HCC (ie, it has some but not all of the features required for LR-5 categorization) (Figs 9, 10). LR-4 observations are also subdivided on the basis of size, into categories A (<20 mm) and B (≥20 mm) (Table 1). As with LR-5 obser-vations, category B observations require fewer imaging features to be considered probable HCCs than do category A observations. Obser-vations with features of probable tumor within the lumen of a vein are considered LR-4 (22).
Category LR-3An LR-3 observation has intermediate prob-ability of being an HCC (Fig 11). This category includes all indeterminate observations that lack both (a) unequivocal features that would allow them to be categorized as LR-4 or LR-5, and
(b) the unequivocal benign features of LR-1 or LR-2. In addition, observations that have imag-ing features of LR-4 or LR-5 are placed in the LR-3 category if their size and features remain stable for 2 years (22).
The current version of LI-RADS does not make specific recommendations for follow-up imaging or further work-up with biopsy for LR-3 and LR-4 observations. The recently updated guidelines of the American Association for the Study of Liver Disease, which recognize imaging surveillance for HCC with US, recommend that lesions measuring less than 10 mm be reassessed with imaging in 3 months, whereas those measur-ing more than 10 mm and without the typical imaging features of HCC on multiphase contrast-enhanced CT or MR images (ie, arterial phase hyperenhancement and portal venous phase or later phase hypoenhancement) should be further evaluated with imaging-guided biopsy (42).
Figure 11. Observation of indeterminate prob-ability for HCC (LR-3) in a 52-year-old man with alcoholic cirrhosis. (a) Axial T2-weighted HASTE image shows a rounded hypointense observation (arrow). (b, c) On axial gadolinium-enhanced MR images obtained during the arterial (b) and delayed venous (c) phases, the observation shows hyperenhancement (arrow in b) followed by isointensity. The presence of T2 signal abnormality suggests that this observation represents a space-occupying process rather than a focal perfusion alteration.

1990 November-December 2012 radiographics.rsna.org
Category LR-2An LR-2 observation is probably benign (Fig 12). This category should be used when the ra-diologist has a high degree of confidence (but not 100% certainty) that the observation is be-nign. It should not be used if there is more than minimal doubt that the observation is benign or if the observation has features that are sugges-tive of HCC (22). Because of the large number of possible benign entities that may affect the liver, LI-RADS does not specifically delineate criteria for this category. Observations described
in the system that fit in this category are rela-tively common benign processes but with an atypical appearance.
Special attention must be given to a common condition in cirrhotic livers that may be a source of false-positive diagnosis of HCC: focal perfu-sion alterations. These are areas of arterial phase hyperenhancement most frequently caused by nontumorous arterioportal shunts or focal ob-struction of a parenchymal portal vein branch (43,44). These alterations are usually peripheral, wedge shaped, and isointense relative to the sur-rounding parenchyma on T1- and T2-weighted MR images, and can be confidently characterized
Figure 12. Probable benign observation in a 50-year-old man with cirrhosis. (a) Axial Gd-DTPA–enhanced arterial phase fat-suppressed T1-weighted LAVA image shows a 2.3-cm rounded obser-vation (arrow) with predominantly peripheral hyperenhancement. (b) On an axial Gd-DTPA–en-hanced portal venous phase fat-suppressed T1-weighted LAVA image, the observation is isointense or slightly hyperintense (black arrow) and, except for its persistently hypointense center, has a signal intensity similar to that of the portal vein (white arrow). (c) On an axial T2-weighted fast spin-echo MR image, the observation demonstrates marked hyperintensity (arrow). These findings are sugges-tive of an atypical hemangioma.

RG • Volume 32 Number 7 Purysko et al 1991
Figure 13. Definite benign perfusion alterations (LR-1) in the liver of a 62-year-old woman with cirrhosis from hemochromatosis. (a) Axial Gd-DTPA–enhanced fat-suppressed T1-weighted VIBE image obtained during the arterial phase shows a large geographic area of hy-perenhancement in the posterior right hepatic lobe (black arrow) and a smaller wedge-shaped area of hyperenhancement in the periphery of the left hepatic lobe (white arrow). (b) On an axial Gd-DTPA–enhanced fat-suppressed T1-weighted VIBE image obtained during the portal venous phase, the hyperenhancing areas seen in a are isointense. (c) Axial T2-weighted HASTE image shows no corresponding signal abnormality.
as LR-1 (Fig 13); however, perfusion alterations can occasionally be nodular in contour and dif-ficult to distinguish from a true enhancing lesion (44). Areas of nodular arterial phase hyperen-hancement seen exclusively during the arterial phase are more appropriately categorized as LR-2 (33,45), but if corresponding abnormalities (eg, increased T2 signal) can be seen on unenhanced images or with other sequences, perfusion al-terations are considered unlikely (31), and the observation should be categorized as either LR-3 or LR-4 depending on its size and nonvascular
features. In addition, some areas of perfusion al-teration can occur secondary to focal liver lesions, including HCC (46).
Note that hepatocellular adenoma and focal nodular hyperplasia, both of which are benign and are usually hyperenhancing during the arte-rial phase, are purposely omitted from the pro-vided list of differential diagnoses for LR-1 and LR-2, since these conditions rarely occur in cir-rhotic livers (25,40).

1992 November-December 2012 radiographics.rsna.org
Category LR-1An LR-1 observation is definitely benign (Fig 14). This category should be applied exclusively to observations that the radiologist is 100% cer-tain are benign and that have no features sugges-tive of HCC (22). As with LR-2, no specific cri-teria are defined for the LR-1 category. Instead, a list of benign conditions that may be encountered is provided (Table 5).
LI-RADS and Liver TransplantationAmong the currently available treatment options with curative intent for patients with cirrhosis and HCC, liver transplantation is the most vali-dated intervention, with a reported 5-year sur-vival rate of 84%, compared with rates of 46%
among patients who undergo resection and 34% among those who undergo ablation therapy (14).
The Organ Procurement and Transplantation Network (OPTN), which is affiliated with the U.S. Department of Health and Human Services, maintains the only national patient waiting list in the United States. This list is governed by the United Network for Organ Sharing (UNOS). The OPTN/UNOS policy (47) uses the model for end-stage liver disease, which is predictive of mortality risk, to assess recipient priority scores (43). Patients with a diagnosis of stage T2 HCC may be given higher priority on the waiting list, since delays in transplantation could lead to HCC progression and preclude further consid-eration for transplantation because of poor out-comes (48). Stage T2 HCC is defined as either (a) a single lesion measuring 2–5 cm, or (b) two
Figure 14. Definite benign hypertrophic pseudomass and regenerative nodules in a 52-year-old woman with cirrhosis. Axial fat-suppressed T1-weighted VIBE images obtained before (a) and after (b–d) the ad-ministration of Gd-DTPA during the arterial (b), portal venous (c), and later venous (d) phases show a large mass (*) exophytic off the left hepatic lobe that is isoenhancing relative to normal liver parenchyma. Adjacent to the pseudomass is a band of focal fibrosis with progressive enhancement (arrow in d) that becomes hyperintense relative to the pseudomass, which creates a false appearance of hypoenhancement by the pseudomass. Multiple regenerative nodules surrounded by fibrosis with similar signal characteristics (arrowhead in d) are also present.

RG • Volume 32 Number 7 Purysko et al 1993
Table 6 Imaging Features of OPTN Class 5 Observations
Size Description
≥10 mm but <20 mm
Arterial phase hypervascularity, portal venous phase–delayed phase washout, and late capsule/pseudocapsule enhancement*
≥20 mm but <50 mm
Arterial phase hypervascularity, portal venous phase–delayed phase washout or late capsule/pseudocapsule enhancement, or interval growth on serial images
Source.―Reference 47.*If neither washout nor pseudocapsule enhancement is present, an increase of ≥50% in the maximum diameter of the observation must be demonstrated on serial CT or MR images obtained less than 6 months apart, using as reference the same contrast phase and preferably the same imaging modality.
Table 5 Examples of Definitely and Probably Benign Observations
Clinical Indication Examples
Definitely benign Cyst, hemangioma, focal fat deposition or sparing, hypertrophic pseudomass interpreted as definitely benign, wedge-shaped perfusional alterations, con-fluent fibrosis, focal scars, some arterial phase nonhyperenhancing atypical nodules, homogeneous siderotic nodules
Probably benign Atypical cyst, hemangioma, focal fat deposition or sparing, hypertrophic pseudomass interpreted as probably benign, rounded and patchy perfu-sional alterations, atypical confluent fibrosis or focal scars, some arterial phase nonhyperenhancing atypical nodules*(small ([<2-cm] heterogeneous siderotic, T1 hyperintense, or steatotic nodules; large [≥2-cm], otherwise unremarkable nodules; progressively enhancing observations)
Source.―Adapted, with permission, from reference 22.*Arterial phase nonhyperenhancing atypical nodules may be categorized as LR-2 at the discretion of the radiolo-gist. In general, such nodules should not have major or ancillary features of HCC. Arterial phase nonhyperen-hancing atypical nodules with one or more major or ancillary features of HCC should usually be categorized as LR-3 or LR-4.
or three lesions measuring 1–3 cm each, provided that extrahepatic involvement (ie, lymph node metastases) and macrovascular invasion (tumor thrombus) are absent (47).
The OPTN/UNOS policy does not require biopsy confirmation of HCC and accepts a mul-tiphasic contrast-enhanced CT or MR image as a foundation for staging disease in patients who are candidates for liver transplantation (47). Re-cently, the policy has been updated to include minimum technical parameters for hepatic CT and MR imaging, along with specific imaging criteria for HCC lesions, designated as OPTN class 5 lesions, for patients to become eligible for automatic exception points (47). Patients with OPTN class 5 lesions and stage T2 disease are eligible for higher priority and higher ranking on the transplant list. Patients with a larger number of lesions or with lesions of larger size (without extrahepatic spread or vascular invasion) may still be considered for transplantation but are not given higher priority.
The LI-RADS criteria are tailored for diagnos-ing HCC, whereas the updated OPTN/UNOS policy criteria are tailored for identifying candi-dates with HCC who are eligible for automatic exception points for liver transplantation (49). Although the imaging features of LR-5 (Table 1) and OPTN class 5 (Table 6) observations share similarities, they also have subtle differences. The new OPTN/UNOS policy has instituted the use of categories LR-1 through LR-4 for observa-tions that do not meet the criteria for OPTN class 5 (49).
ConclusionsHCC is a global health problem, with the bur-den of disease expected to increase in the com-ing years. Imaging plays a pivotal role in the detection, diagnosis, staging, and management of HCC. LI-RADS has been developed to stan-dardize the interpretation and reporting of liver

1994 November-December 2012 radiographics.rsna.org
observations in patients who are at risk for devel-oping HCC. The five categories established by this system follow the diagnostic thought process and allow imaging observations to be categorized according to the risk of HCC. LI-RADS provides a comprehensive list of imaging features that favor HCC or benignity, along with appropriate terminology. The system is still evolving and is expected to promote a series of improvements that will ultimately positively affect the care of at-risk patients. Areas likely to be covered by LI-RADS in the future include findings at US and hepatocyte-specific contrast-enhanced MR imag-ing; recommendations for follow-up or biopsy of LR-4 and LR-3 observations; and assessment of response to treatment with local ablative thera-pies (including radiofrequency ablation, chemo-embolization, and radioembolization) or systemic chemotherapy with antiangiogenic agents.
References 1. International Agency for Research on Cancer,
World Health Organization (WHO). GLOBO-CAN 2008: cancer incidence, mortality and preva-lence worldwide in 2008. Available at: http://globo can.iarc.fr. Accessed April 19, 2012.
2. Parkin DM, Bray F, Ferlay J, Pisani P. Global can-cer statistics, 2002. CA Cancer J Clin 2005;55(2): 74–108.
3. London WT, McGlynn KA. Liver cancer. In: Schottenfeld D, Fraumeni JF Jr, eds. Cancer epi-demiology and prevention. 3rd ed. New York, NY: Oxford University Press, 2006; 763–786.
4. Venook AP, Papandreou C, Furuse J, de Guevara LL. The incidence and epidemiology of hepatocel-lular carcinoma: a global and regional perspective. Oncologist 2010;15(suppl 4):5–13.
5. Center MM, Jemal A. International trends in liver cancer incidence rates. Cancer Epidemiol Bio-markers Prev 2011;20(11):2362–2368.
6. Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet 2003;362(9399):1907–1917.
7. Altekruse SF, McGlynn KA, Reichman ME. He-patocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol 2009;27(9):1485–1491.
8. Bruix J, Sherman M, Llovet JM, et al. Clinical management of hepatocellular carcinoma: conclu-sions of the Barcelona-2000 EASL conference— European Association for the Study of the Liver. J Hepatol 2001;35(3):421–430.
9. Sharma P, Saini SD, Kuhn LB, et al. Knowledge of hepatocellular carcinoma screening guidelines and clinical practices among gastroenterologists. Dig Dis Sci 2011;56(2):569–577.
10. Thompson Coon J, Rogers G, Hewson P, et al. Surveillance of cirrhosis for hepatocellular carci-noma: systematic review and economic analysis. Health Technol Assess 2007;11(34):1–206.
11. Becker-Weidman DJ, Kalb B, Sharma P, et al. He-patocellular carcinoma lesion characterization: sin-gle-institution clinical performance review of multi-phase gadolinium-enhanced MR imaging—compar-
ison to prior same-center results after MR systems improvements. Radiology 2011;261(3):824–833.
12. Lee KH, O’Malley ME, Haider MA, Hanbidge A. Triple-phase MDCT of hepatocellular carcinoma. AJR Am J Roentgenol 2004;182(3):643–649.
13. Sharma P, Kalb B, Kitajima HD, et al. Optimization of single injection liver arterial phase gadolinium enhanced MRI using bolus track real-time imaging. J Magn Reson Imaging 2011;33(1):110–118.
14. Altekruse SF, McGlynn KA, Dickie LA, Kleiner DE. Hepatocellular carcinoma confirmation, treat-ment, and survival in surveillance, epidemiology, and end results registries, 1992–2008. Hepatology 2012;55(2):476–482.
15. Radiological Society of North America Infor-matics. Radiology report initiative. Available at: http://www.rsna.org/Reporting_Initiative.aspx. Accessed April 19, 2012.
16. Reiner BI. Medical imaging data reconciliation. 4. Reconciliation of radiology reports and clinical out-comes data. J Am Coll Radiol 2011;8(12):858–862.
17. Krinsky G. Terminology of hepatocellular nodules in cirrhosis: plea for consistency. Radiology 2002; 224(3):638.
18. Lee JM, Trevisani F, Vilgrain V, Wald C. Imaging diagnosis and staging of hepatocellular carcinoma. Liver Transpl 2011;17(suppl 2):S34–S43.
19. Radiological Society of North America. LI-RADS enables standardized interpretation, reporting of HCC. RSNA News 2012;22(2):13–14.
20. Napel SA, Beaulieu CF, Rodriguez C, et al. Auto-mated retrieval of CT images of liver lesions on the basis of image similarity: method and preliminary results. Radiology 2010;256(1):243–252.
21. Schwartz LH, Panicek DM, Berk AR, Li Y, Hricak H. Improving communication of diagnostic radiol-ogy findings through structured reporting. Radiol-ogy 2011;260(1):174–181.
22. American College of Radiology. Quality and safety resources: Liver Imaging–Reporting and Data System. Available at: http://www.acr.org/Quality-Safety/Resources/LIRADS. Accessed April 22, 2012.
23. Dixon AK. The impact of medical imaging on the physician’s diagnostic and therapeutic thinking. Eur Radiol 1998;8(3):488–490.
24. Hecht EM, Holland AE, Israel GM, et al. Hepa-tocellular carcinoma in the cirrhotic liver: gado-linium-enhanced 3D T1-weighted MR imaging as a stand-alone sequence for diagnosis. Radiology 2006;239(2):438–447.
25. Willatt JM, Hussain HK, Adusumilli S, Marrero JA. MR imaging of hepatocellular carcinoma in the cirrhotic liver: challenges and controversies. Radi-ology 2008;247(2):311–330.
26. Ayuso C, Rimola J, García-Criado A. Imaging of HCC. Abdom Imaging 2012;37(2):215–230.
27. Efremidis SC, Hytiroglou P. The multistep process of hepatocarcinogenesis in cirrhosis with imaging correlation. Eur Radiol 2002;12(4):753–764.
28. Marrero JA, Hussain HK, Nghiem HV, Umar R, Fontana RJ, Lok AS. Improving the prediction of hepatocellular carcinoma in cirrhotic patients with an arterially-enhancing liver mass. Liver Transpl 2005;11(3):281–289.
29. Sherman M. The radiological diagnosis of hepato-cellular carcinoma. Am J Gastroenterol 2010;105 (3):610–612.
30. Fowler KJ, Brown JJ, Narra VR. Magnetic resonance imaging of focal liver lesions: approach to imaging diagnosis. Hepatology 2011;54(6):2227–2237.

RG • Volume 32 Number 7 Purysko et al 1995
31. Jeong YY, Mitchell DG, Kamishima T. Small (<20 mm) enhancing hepatic nodules seen on arterial phase MR imaging of the cirrhotic liver: clinical implications. AJR Am J Roentgenol 2002;178(6): 1327–1334.
32. Khalili K, Kim TK, Jang HJ, Yazdi LK, Guindi M, Sherman M. Indeterminate 1-2-cm nodules found on hepatocellular carcinoma surveillance: biopsy for all, some, or none? Hepatology 2011;54 (6):2048–2054.
33. Hwang SH, Yu JS, Kim KW, Kim JH, Chung JJ. Small hypervascular enhancing lesions on arterial phase images of multiphase dynamic computed tomography in cirrhotic liver: fate and implications. J Comput Assist Tomogr 2008;32(1):39–45.
34. Sakata J, Shirai Y, Wakai T, Kaneko K, Nagahashi M, Hatakeyama K. Preoperative predictors of vas-cular invasion in hepatocellular carcinoma. Eur J Surg Oncol 2008;34(8):900–905.
35. Ueda K, Matsui O, Kawamori Y, et al. Hyper-vascular hepatocellular carcinoma: evaluation of hemodynamics with dynamic CT during hepatic arteriography. Radiology 1998;206(1):161–166.
36. Dodd GD 3rd, Memel DS, Baron RL, Eichner L, Santiguida LA. Portal vein thrombosis in patients with cirrhosis: does sonographic detection of in-trathrombus flow allow differentiation of benign and malignant thrombus? AJR Am J Roentgenol 1995;165(3):573–577.
37. Leoni S, Piscaglia F, Golfieri R, et al. The impact of vascular and nonvascular findings on the nonin-vasive diagnosis of small hepatocellular carcinoma based on the EASL and AASLD criteria. Am J Gastroenterol 2010;105(3):599–609.
38. Burrel M, Llovet JM, Ayuso C, et al. MRI angi-ography is superior to helical CT for detection of HCC prior to liver transplantation: an explant cor-relation. Hepatology 2003;38(4):1034–1042.
39. Khalili K, Kim TK, Jang HJ, et al. Optimization of imaging diagnosis of 1-2 cm hepatocellular carci-noma: an analysis of diagnostic performance and resource utilization. J Hepatol 2011;54(4):723–728.
40. Hussain SM, Reinhold C, Mitchell DG. Cirrhosis and lesion characterization at MR imaging. Radio-Graphics 2009;29(6):1637–1652.
41. Varela M, Sanchez W, Bruix J, Gores GJ. Hepato-cellular carcinoma in the setting of liver transplan-tation. Liver Transpl 2006;12(7):1028–1036.
42. Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepato-cellular carcinoma: an update. Hepatology 2011;53 (3):1020–1022.
43. Brancatelli G, Baron RL, Peterson MS, Marsh W. Helical CT screening for hepatocellular carcinoma in patients with cirrhosis: frequency and causes of false-positive interpretation. AJR Am J Roentgenol 2003;180(4):1007–1014.
44. Yu JS, Kim KW, Jeong MG, Lee JT, Yoo HS. Non-tumorous hepatic arterial-portal venous shunts: MR imaging findings. Radiology 2000;217(3):750–756.
45. Holland AE, Hecht EM, Hahn WY, et al. Impor-tance of small (< or = 20-mm) enhancing lesions seen only during the hepatic arterial phase at MR imaging of the cirrhotic liver: evaluation and comparison with whole explanted liver. Radiology 2005;237(3):938–944.
46. Colagrande S, Centi N, Galdiero R, Ragozzino A. Transient hepatic intensity differences. 1. Those associated with focal lesions. AJR Am J Roentgenol 2007;188(1):154–159.
47. OPTN policy management. Available at: http://op tn.transplant.hrsa.gov/policiesAndBylaws/poli-cies.asp. Accessed April 22, 2012.
48. Mazzaferro V, Regalia E, Doci R, et al. Liver trans-plantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996;334(11):693–699.
49. OPTN/UNOS Liver and Intestinal Organ Trans-plantation Committee. Report to the Board of Di-rectors. Available at: http://optn.transplant.hrsa.gov/CommitteeReports/board_main_Liver&IntestinalOrganTransplantationCommittee_11_17_2011_17_35.pdf. Accessed April 22, 2012.
This journal-based CME activity has been approved for AMA PRA Category 1 CreditTM. See www.rsna.org/education/search/RG.

Teaching Points November-December Issue 2012
LI-RADS: A Case-based Review of the New Categorization of Liver Findings in Patients with End-Stage Liver DiseaseAndrei S. Purysko, MD • Erick M. Remer, MD • Christopher P. Coppa, MD • Hilton M. Leão Filho, MD • Chakradhar R. Thupili, MD • Joseph C. Veniero, MD, PhD
RadioGraphics 2012; 32:1977–1995 • Published online 10.1148/rg.327125026 • Content Codes:
Page 1978The goals of LI-RADS include reducing variability in lesion interpretation; improving communication with clinicians; facilitating decision-making processes (eg, for transplantation, ablative therapy, or chemothera-py); reducing omissions of relevant information from CT and MR imaging reports by standardizing report content and structure; and facilitating outcome monitoring, performance auditing, quality assurance, and research (22).
Page 1981With caution, ancillary features that favor HCC may be used to classify LR-4 or LR-5 observations that do not meet major feature criteria for those two categories (Fig 2) (22).
Page 1985The imaging criteria used to categorize an observation as LR-5 are considered specific enough to render the diagnosis of HCC without the need for biopsy (22).
Page 1991Note that hepatocellular adenoma and focal nodular hyperplasia, both of which are benign and are usu-ally hyperenhancing during the arterial phase, are purposely omitted from the provided list of differential diagnoses for LR-1 and LR-2, since these conditions rarely occur in cirrhotic livers (25,40).
Page 1992Patients with a diagnosis of stage T2 HCC may be given higher priority on the waiting list, since delays in transplantation could lead to HCC progression and preclude further consideration for transplantation because of poor outcomes (48).