Embed Size (px)
Citation preview

F
B
F
petaIsfdOttmesfpopsadi
MB
Operative Techniques in Otolaryngology (2010) 21, 175-180
1d
rontal sinus stenting techniques
arry T. Malin, MD, MPP, David A. Sherris, MD
rom the Department of Otolaryngology, State University of New York at Buffalo, Buffalo, New York.
Postoperative reocclusion or obstruction of the frontal sinus outflow tract are key factors in the failureof surgical efforts to treat frontal sinus disease. Stenting of the frontal sinus is a useful adjunctivemeasure for select patients, including those who have failed previous surgical treatment or who aredeemed to be at high risk of failure due to unfavorable anatomy or mucosal disease. Multipleapproaches to stenting of the frontal sinus are available, including purely endonasal techniques, acombined approach using both endonasal access to the frontal sinus and external trephination, and anexternal approach via modified Lynch (Neel-Lake) frontoethmoidectomy. Herein, we describe thesurgical techniques for frontal sinus stent placement, review the options for choice of stenting material,and discuss key factors in postoperative management and stent maintenance.© 2010 Elsevier Inc. All rights reserved.
KEYWORDSFrontal sinus;Frontal sinusitis;Frontal sinus surgery;Stents;Paranasal sinusdisease;Rhinosinusitis
sns
I
Dsscdmndhoisto
soFe
Restenosis of the frontal sinus outflow tract (FSOT)ostoperatively is a primary cause of failure of surgicalfforts to establish and maintain ventilation and drainage ofhe frontal sinuses. The use of surgically placed stents in anttempt to maintain patency of the FSOT has a long history.n 1905, Ingals described the use of gold tubes as frontalinus stents.1 The use of 1-cm rubber tubing for stenting therontal sinus was a key component in Lynch’s originalescription in 1921 of his frontoethmoidectomy technique.2
ver subsequent years, progress in both surgical instrumen-ation, most notably the widespread adoption of endoscopicechniques for accessing the frontal sinus, and the develop-ent of new stenting materials and designs has greatly
xpanded the options available to the sinus surgeon fortenting in cases with a high anticipated risk of surgicalailure due to reocclusion of the frontal sinus drainageathway. An array of techniques may be used for placementf frontal sinus stents, including intranasal endoscopiclacement, Above and Below techniques using both endo-copic frontal sinusotomy and frontal sinus trephination,nd external approaches employing elaborations on stan-ard frontoethmoidectomy methods. Recent developmentsnclude a trend toward long-term maintenance of frontal
Address reprint requests and correspondence: David A. Sherris,D, Department of Otolaryngology, State University of New York atuffalo, 1237 Delaware Avenue, Buffalo, NY 14209.
aE-mail address: [email protected].
043-1810/$ -see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.otot.2010.07.002
inus stents in patients deemed to be at high risk of reste-osis and experimentation with a variety of drug-elutingtent materials.
ndications for frontal sinus stenting
espite the long history of surgical experience with frontalinus stenting, there are no universally accepted criteria toerve as indications for stenting. Considered within theontext of surgical options for establishment of frontal sinusrainage ranging from minimally invasive intranasal eth-oidectomy to more aggressive approaches, such as exter-
al ethmoidectomy, osteoplastic flap, or obliterative proce-ures, frontal sinus stenting is an alternative in patients whoave failed standard ethmoidectomy or frontal sinusotomyr in whom a high likelihood of failure with minimallynvasive procedures is expected. In such cases, frontal sinustenting is a valuable alternative to more extensive resec-ions, such as the endoscopic-modified Lothrop procedurer Lynch ethmoidectomy.
The most common causes of failure of standard endo-copic treatment of frontal sinus disease involve reocclusionf the frontal sinus drainage pathway or restenosis of theSOT due to postoperative scarring and adhesions, prolif-ration of obstructive polyposis, or middle turbinate later-
lization. Frontal sinus stents are intended to forestall such
cracibtdniootaIstmitpbwtftm
S
OtbssrdLciustlctcsrsabLsTsd
fm(Rpwivesmscstrfcpoo
E
TpstetcSitblsfomistitatnrs
At
I
176 Operative Techniques in Otolaryngology, Vol 21, No 3, September 2010
omplications by maintaining patency and structural integ-ity of the FSOT while the process of healing and regener-tion of the mucosal lining of the frontal neoostium areompleted. Despite the lack of universal agreement regard-ng the precise indications for stenting, several factors haveeen commonly cited as key considerations in the decisiono place frontal sinus stents: the presence of extensivelyenuded or circumferentially exposed bone around theeoostium perimeter; severe inflammatory disease of thenvolved mucosa; extensive polyposis which threatens tobstruct the frontal sinus drainage pathway; destabilizationf the middle turbinate predisposing to lateralization; andhe presence of osteitic bone within the FSOT. Particularttention has been paid to the size of the frontal neoostium.n an influential study, Hosemann and colleagues demon-trated that the likelihood of restenosis increased precipi-ously in cases where the frontal neoostium was less than 5m in diameter.3 This finding has led some authors to
dentify the presence of an intraoperatively fashioned fron-al sinus neoostium smaller than 5 mm in diameter as therimary indication for frontal sinus stenting.4 Exposure ofone at the frontal neoostium stimulates osteoneogenesis,hereas mucosal injury leads to granulation and scarring of
he FSOT. Mucosal factors predisposing to restenosis of therontal sinus postoperatively include extensive inflamma-ion, polyposis, allergic disease, vasculitides, and granulo-atous disease, such as Wegener’s or sarcoidosis.
tenting materials
ver nearly a century of experimentation with stenting ofhe frontal sinus, a large range of materials and designs haveeen used to stent or pack the frontal sinus. The mostignificant insight regarding the optimal nature of frontalinus stenting design is the importance of using soft mate-ials as stents. The importance of using soft stents wasemonstrated in a landmark study by Neel, Whicker, andake, in which the investigators demonstrated superior out-omes in stenting the FSOT using soft, rolled silicone sheet-ng compared with firm, rubber tubes in a dog model. These of firm tubes hampered effective epithelialization andtimulated extensive fibroplasia and granulation.5 The au-hors concluded that the use of firm tubes caused increasedocal ischemia, hampered effective drainage, caused an in-reased level of osteoblastic reaction, and enhanced infec-ion rates.6 Various soft stenting materials have been advo-ated by different surgeons, including rolled silicone sheeting,ilicone tubing, soft catheter devices, Merocel spacers, softubber T-tubes, and specially designed proprietary devices,uch as Rains self-retaining stents, Freeman silicone stents,nd Parrell frontal sinus T-stents. U- or H-shaped stents maye used for bilateral FSOT stenting in Draf III or endoscopicothrop procedures. In cases where the frontal intersinuseptum is taken down, a biliary-type or specially designed-tube may be employed with arms spread into both frontalinuses. Variations on stent design include the use of ra-
ioopaque markers, expandable elements, or winged flanges tor self-retention and suture tails to facilitate precise place-ent and easy removal in the office setting. Acclarent
Menlo Park, CA) now offers a frontal sinus stent, theelieva Stratus MicroFlow spacer, which features a micro-ore reservoir system for fluid delivery and is designed toork with its proprietary balloon sinuplasty system. Recent
nnovations in stent design include experimentation witharious types of drug-eluting stents. Herrmann and cowork-rs have reported experimentation in a sheep model withtents impregnated with Paclitaxel, which may decreaseucosal scarring.7 A dexamethasone-releasing frontal sinus
tent design was tested in a rabbit model by Beul andolleagues, who reported decreased granulation, thinnertroma, and more favorable mucosal regeneration on his-opathologic analysis.8 Huvenne and colleagues recentlyeported promising results using doxycycline-releasingrontal sinus stents in humans, with decreased MMP-9 con-entrations, decreased bacterial colonization rates, and im-roved surgical outcomes as demonstrated by patient ratingsn a visual analog symptom scale and observed rates ofstial restenosis.9
ndonasal stent placement
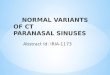
he least invasive approach for frontal sinus stenting em-loys endonasal stent placement using standard FESS in-trumentation. In this approach, conventional endoscopicechniques are used to complete an uncinectomy, anteriorthmoidectomy, and frontal sinusotomy. The frontal sinus ishen cannulated from below using a curved suction, curvedurette, guidewire, or specially designed stent introducer.tents are then slid over the cannulating instrument, which
s angled at approximately 45°, and advanced upwards intohe frontal sinus (Figure 1). Before stent insertion, care muste taken to ensure that the surgically fashioned ostium isarge enough to accommodate the stents with minimal pres-ure on the surrounding mucosa or bone. Agger nasi cells orrontal sinus cells should be resected as needed and anybstructing soft tissue or osteitic bone removed. Enlarge-ent of the FSOT via curetting or, in rare instances, drilling
n anterior and medial vectors may be necessary to ensure aufficiently large frontal neoostium.10 Care is necessary inrimming stents to the appropriate length. Stents that are ofnsufficient length are prone to obstruction by granulationissue, whereas excessively long stents are associated withirflow obstruction and crusting. Intranasally, stents may berimmed at roughly the inferior border of the middle turbi-ate or at the midlevel of the vertical septal height. Hoyteports the average length of appropriately trimmed frontalinus stents to be 5.5 cm.11
bove and Below approach with frontal sinusrephination
n cases with more difficult anatomic challenges or in pa-
ients with refractory frontal sinus disease, an Above and
BtefIsfasasdt
tctit
onsscmntifattiof3otfoetioei
dc
177Malin and Sherris Frontal Sinus Stenting Techniques
elow technique combining external frontal sinus trephina-ion and intranasal endoscopy may be useful. The combinedndoscopic and external mini-trephination approach to therontal sinuses features several advantages in selected cases.t provides enhanced access to the entirety of the frontalinus, facilitating treatment of disease within regions of therontal sinuses, particularly the most lateral and superiorspects, which may be inaccessible with standard endo-copic techniques alone. Enhanced access via trephinationllows for the ability to visualize completely the frontalinus mucosa and take down frontal sinus cells that areifficult to treat via standard FESS, especially type III and
Figure 1 Endonasal placement of frontal sinus stents.
ype IV cells. Creation of the external trephination facili-
ates ongoing postoperative care with external irrigation andulture collection as needed. Endoscopic visualization ofhe frontal recess and FSOT anatomy from above via treph-nation may also assist in identification and dissection of theract and facilitate precise stent placement.
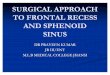
The frontal sinus trephination is begun with infiltrationf the medial aspect of the brow with lidocaine and epi-ephrine and a 1- to 2-cm incision performed along theupraorbital rim to allow access to the frontal sinus. Thekin incision may be placed within the brow or a browrease. In patients with thinner brows, optimal placementay be just above or below the brow in an arc parallel to the
atural curvature of the brow (Figure 2). The access incisionends to heal very well with favorable cosmesis. If thencision is performed within the brow, injury to the hairollicles should be minimized by beveling the incision par-llel to the follicles and avoiding the use of electrocautery athe level of the follicles. Dissection is then performed downo the level of the periostium. Care is exercised to avoidnjury to the supraorbital nerve, which may result in post-perative numbness or paresthesia. Trephination of therontal sinus is performed with a 4-mm cutting burr (Figure). The standard location for entry into the frontal sinus isver its mediolateral aspect. However, caution must be usedo avoid injury to the nasofrontal recess when opening therontal sinus in this area. If necessary due to patient anatomyr the specific location of pathology within the sinus, thentry point may be placed over any portion of the anteriorable. Preoperative CT scans should be carefully reviewedn planning the sinus entry site. Stereotactic image guidancer Caldwell templates may also be helpful in guiding sinusntry. Intracranial injury is possible if the entry site is placednappropriately.
Once the burr hole has been created, use of the poweredrill should be ceased before progression through the mu-osal lining of the sinus. The sinus mucosa should be dis-
Figure 2 Incision for frontal sinus trephination.

sFudoaifwocovdSftntaIfsiaBr
M
Afme
KodTidpomrefnfMcSi5am
P
Famsvcwcsrp
178 Operative Techniques in Otolaryngology, Vol 21, No 3, September 2010
ected sharply to minimize the degree of mucosal injury.ollowing completion of the frontal sinus trephination,ncinectomy and ethmoidectomy are performed using stan-ard endonasal techniques. Performance of frontal sinusot-my with adequate opening of the FSOT can be aided frombove using endoscopic visualization via the frontal treph-nation (Figure 4). Transillumination into the nasal cavityrom the frontal sinus or infusion through the trephinationith Methylene blue-stained irrigation are alternative meth-ds in which the presence of the frontal sinus trephinationan be used to aid in endonasal identification and dissectionf the FSOT. In opening of the frontal sinus neoostium,igilance should be used in attempting to minimize theegree of mucosal injury and exposure of denuded bone.tents fashioned from soft silicone sheeting rolled in aunnel shape or soft silicone tubing are then introduced viahe frontal sinus trephination and advanced through theasofrontal recess. Placement of a suture tail, which can behreaded through the nasofrontal recess into the nasal cavitynd grasped from below, may assist with proper placement.f difficulty is encountered introducing the stent into the naso-rontal recess, the stent may be advanced over a guidewire ormall-caliber catheter. Postoperatively, the frontal sinus treph-nation may be left open to facilitate continued irrigation. Theperture tends to heal well with no surgical closure required.ony defects greater than 3 cm in diameter may benefit from
epair with titanium mesh or hydroxyapatite.12
odified Lynch frontoethmoidectomy
n alternative combined external and intranasal approach torontal sinus stenting employs a modified Lynch frontoeth-oidectomy (Neel-Lake) procedure. An intranasal ethmoid-
Figure 3 Creation of the frontal sinus trephination.
ctomy and frontal sinusotomy are performed. A modified
illian incision is executed extending from the medial brownto the nasal sidewall terminating at a point lying half theistance between the nasofacial angle and the nasal dorsum.he portion of the incision lying medial to the inner canthus
s performed in a curved “gull wing” or “lazy S” fashion toecrease the risk of development of a webbed scar. Theeriosteum is elevated and retracted along with the trochleaf the superior oblique muscle and the orbit, while theedial canthus is cut. A portion of the lacrimal bone is
emoved at the superomedial angle of the orbit, allowing forxposure and removal of a segment of the floor of therontal sinus. A Kerrison rongeur is used to enlarge theasofrontal tract with establishment of an expanded naso-rontal communication approximately 1.5 cm in diameter.
ucosa is preserved to the greatest extent possible duringreation of the expanded nasofrontal communication. Ailastic stent is then introduced from above and advanced
ntranasally through the enlarged nasofrontal tract (Figuresand 6).13,14 The stent is then trimmed intranasally to the
ppropriate length and may be anchored with a suture to theucosa of the nasal septum or lateral nasal wall (Figure 7).
ostoperative management
ollowing placement of frontal sinus stents using any of thepproaches described, patients should be started on a regi-en of frequent nasal saline irrigation and topical nasal
teroids. Postoperative follow-up may require surveillanceisits with intranasal examination, debridement, and stentleaning to maintain patency. Although stents are generallyell tolerated by patients even over long periods, potential
omplications include stent displacement and the need fortent removal due to patient discomfort. Most authors alsoecommend that patients be maintained on a course ofostoperative antibiotics following frontal sinus stent place-
Figure 4 Above and Below approach to the frontal sinus.

md
srffdb
wiislwsThto
appro
179Malin and Sherris Frontal Sinus Stenting Techniques
ent; however, there is no consensus regarding the optimaluration of therapy.
One area of concern with maintenance of frontal sinustenting is the potential for stents to serve as a nidus forecurrent infection. Perloff and Palmer examined Silasticrontal sinus stents removed from six patients at 1-4 weeksollowing FESS using scanning electron microscopy andiscovered multicellular syncytia consistent with bacterialiofilm formation on all samples studied.15 The degree to
Figure 5 Modified Lynch
Figure 6 Stent placement via modified Lynch approach.
hich frontal sinus stents are likely to function as clinicallymportant reservoirs of bacteria predisposing to reinfections unknown, however. An additional risk in frontal sinustenting is toxic shock syndrome (TSS). Chadwell and col-eagues reported a case of life-threatening TSS associatedith frontal sinus stenting. Although TSS is a rare event, the
urgeon must recognize possible presenting symptoms ofSS following frontal sinus stenting, such as high fever,ypotension, macular rash, mucosal hyperemia, mental sta-us changes, and desquamation. It is important to note that thenset of TSS may occur remotely. In the case report by Chad-
ach to the frontal sinuses.
Figure 7 Intranasal anchoring of frontal sinus stent.

wfllo
S
TssilseopcgsorslrrppeoeMm
C
TlaowrmmwnesLtmd
fsdmt
R
1
1
1
1
1
1
1
1
1
1
2
2
180 Operative Techniques in Otolaryngology, Vol 21, No 3, September 2010
ell, onset of symptoms developed on postoperative day 18ollowing completion of a full course of postoperative prophy-actic antibiotic therapy with cephalexin. Case reports of de-ayed-onset TSS associated with nasal packing have describednset of symptoms at up to 5 weeks postoperatively.16
tenting duration
he question regarding the optimal duration of frontal sinustent maintenance remains controversial. To date, there iscant empiric evidence available to guide surgeons on thisssue, and no definitive clinical standards have been estab-ished.17 Traditionally, most authors have recommendedtent maintenance for varying durations ranging from sev-ral days to 8 weeks. It was assumed that significant post-perative reepithelialization and remodeling of the FSOTredisposing to restenosis of the frontal neoostium wereompleted within weeks. However, some studies have sug-ested that postoperative remodeling may persist over aignificantly longer period and that prolonged maintenancef stents may improve clinical outcomes.18,19 Recent reportsegarding clinical experience with long-term frontal sinustenting indicate that stenting for periods of 6 months oronger is well tolerated by most patients. Lin and Witterickeported low rates of spontaneous dislodgement (14%), ir-eversible obstruction (5%), and stent failure (9%) amongatients in whom frontal sinus stents were maintained for aeriod greater than 3 months.20 In a review of the experi-nce with long-term frontal sinus stenting at the Universityf Utah, Orlandi and Knight reported long-term stents (av-rage duration 33.8 months) were very well tolerated.21
ore investigation is needed, however, to determine opti-al strategies regarding duration of stent maintenance.
onclusions
reatment of chronic frontal sinus disease remains a chal-enging clinical problem, with high rates of surgical failuressociated with restenosis of the frontal neoostium or post-perative obstruction of the FSOT. When treating patientsho have failed conservative surgical therapy or are at high
isk for surgical failure due to unfavorable anatomy orucosal disease, postoperative stenting of the frontal sinusay be a useful adjunctive measure. Stents may be placedithin the frontal sinus using either purely endonasal tech-iques, a combined Above and Below approach using bothndonasal access to the frontal sinus and external frontalinus trephination, or an external approach via modifiedynch (Neel-Lake) frontoethmoidectomy. A variety of stent
ypes are available, but it is critically important that softaterials be used to minimize local ischemia and mucosal
isruption. Rolled silicone sheeting is our preferred choice
or stenting. Although the optimal duration of postoperativetenting has not been definitively established, recent evi-ence suggests that longer periods of postoperative stentaintenance, such as 6 months, may yield improved long-
erm outcomes and is generally well tolerated.
eferences
1. Ingals EE: New operations and instruments for draining the frontal sinus.Tr Am Laryng Rhin Otol Soc 11:183-189, 1905 [as cited in Kanowitz S,Jacobs J, Lebowitz R: Frontal sinus stenting, in Stilianos EK, Senior BA,Draf W (eds): The Frontal Sinus. Berlin, Springer, 2005]
2. Lynch RC: The technique of radical frontal sinus surgery that hasgiven me the best results. Laryngoscope 31:1-5, 1921
3. Hosemann W, Kuhnel TH, Held P, et al: Endonasal frontal sinusotomyin surgical management of chronic sinusitis: a critical evaluation. Am JRhinol 11:1-19, 1997
4. Rains B: Frontal sinus stenting. Otolaryngol Clin North Am 34:101-110, 2001
5. Neel HB III, Whitaker JH, Lake CF: Thin rubber sheeting in frontal sinussurgery: animal and clinical studies. Laryngoscope 86:524-536, 1976
6. Neel HB III, McDonald TJ, Facer GW: Modified Lynch procedure forchronic frontal sinus diseases: rationale, technique and long-term re-sults. Laryngoscope 97:1274-1279, 1987
7. Hermann BW, Citardi MJ, Volger G, et al: A preliminary report on theeffects of paclitaxel-impregnated stents on nasal sheep mucosa. Am JRhinol 18:119-124, 2004
8. Beaule A, Scharf C, Biebler K: Effect of topically-applied dexameth-asone on mucosal wound healing using a drug-releasing stent. Laryn-goscope 118:2073-2077, 2008
9. Huvenne W, Zhang N, Tijsma E, et al: Pilot study using doxycycline-releasing stents to ameliorate post-operative healing quality after sinussurgery. Wound Repair Regen 16:757-767, 2008
0. Freeman S, Blom E: Frontal sinus stents. Laryngoscope 110:1179-1182, 2000
1. Hoyt WH: Endoscopic stenting of nasofrontal communication in fron-tal sinus disease. ENT J 72:596-597, 1993
2. Han J, Hwang P: Image-guided trephination of the frontal sinus: anadjunct to endoscopic technique. Op Tech Otolaryngol Head NeckSurg 15:57-61, 2004
3. Neel HB, McDonald TJ, Facer GW: Modified Lynch procedure forchronic frontal sinus disease: rationale, technique, and long-term re-sults. Laryngoscope 97:1274-1279, 1987
4. Amble FR, Kern EB, Neel HB: Nasofrontal duct reconstruction withsilicone rubber sheeting for inflammatory frontal sinus disese: analysisof 164 cases. Laryngoscope 106:809-815, 1996
5. Perloff J, Palmer J: Evidence of bacterial biofilms on frontal recess stentsin patients with chronic rhinosinusitis. Am J Rhinol 18:377-380, 2004
6. Chadwell JS, Gustafson LM, Tami TA: Toxic shock syndrome asso-ciated with frontal sinus stents. Otolaryngol Head Neck Surg 124:573-574, 2001
7. Kanowitz SJ, Jacobs JB, Lebowitz RA: Frontal sinus stenting, inStilianos EK, Senior BA, Draf W (eds): The Frontal Sinus. Berlin,Springer, 2005
8. Weber R, Mai R, Housemann W, et al: The success of 6-monthstenting in endonasal frontal sinus surgery. ENT J 79:930-941, 2000
9. Yamasoba T, Kikuchi S, Higo R: Transient positioning of a siliconeT-tube in frontal sinus surgery. Otolaryngol Head Neck Surg 3:776-780, 1994
0. Lin D, Witterick I: Frontal sinus stents: how long can they be kept in?J Otolaryngol Head Neck Surg 37:119-123, 2008
1. Orlandi R, Knight J: Prolonged stenting of the frontal sinus. Laryn-
goscope 119:190-192, 2009