Embed Size (px)
Citation preview

Chondromyxoid Fibroma of the Frontal SinusA Case Report and Review of the Literature
Washington University in St Louis Dept of Neurosurgery Otolaryngology and Oculoplastics
Townsend Melanie MD Chicoine Michael MD Custer Phillip MD Murphy Rory MD Schneider John MD
INTRODUCTION DISCUSSION
RESULTS
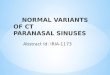
Figure 1 2 CT and MRI of the left frontoethmoid sinus lesion
ABSTRACT
METHODS AND MATERIALS
CONCLUSIONS
REFERENCES
Objective Chondromyxoid fibroma (CMF) is a rare cartilaginous tumor that is especially uncommon in the paranasal sinuses and skull base Only 3 cases of CMF with frontal sinus origin are reported including this case Proper diagnosis and management is essential for differentiating these tumors from their malignant counterparts
Methods We present a case of CMF arising in the frontal sinus and eroding intracranially in a healthy 45 year-old female An in depth discussion of the diagnosis and management of sinonasal and skull base CMF is presented along with a review of the literature
ResultsConclusion Twenty eight cases of sinonasal and skull base CMF were identified Complete excision is the treatment of choice for CMF with radiation therapy reserved for recurrences and difficult to reach locations as there have been reports of malignant transformation rate of 1-2 following radiation En bloc excision is not considered necessary at the expense of critical structures such as the eye The radiographic appearance of these tumors can be very similar to chondrosarcoma its malignant counterpart and proper diagnosis via histology is critical
A retrospective review of available literature was
conducted using PubMed Search terms included
ldquochondromyxoid fibromardquo ldquoparanasal sinusrdquo ldquoskull
baserdquo and ldquonasal cavityrdquo Publication dates from
1997 to 2016 were identified and included All
included articles were analyzed for radiologic and
histologic features demographic data symptoms
management and follow up
bull CMF tumors are extremely rare especially in
the paranasal sinuses
bull On imaging they often have malignant
appearing features and biopsy is required for
diagnosis
bull Complete surgical excision is the treatment
of choice but en block resection at the
expenses of critical structures such as the
eye is not recommended
bull Curettage excision is associated with
recurrence in this case series
bull Radiation is recommended only or difficult to
reach tumors or recurrences
Chondromyxoid fibroma (CMF) is a rare
cartilaginous tumor with benign pathologic
features and no metastatic potential About
5 of CMF lesions arise in the head and
neck and are even less common in the
paranasal sinuses1-3 Two cases of CMF
originating in the frontal sinus were identified
in the literature and we present a third It is
imperative that CMF be differentiated from
chondroblastoma and chondrosarcoma
which can have overlapping features but very
different treatment algorithms
CASE REPORT
A 45 year-old female presented with
progressive blurry vision in her left eye and
persistent headache in the left occipital and
frontorbital regions She also had drooping of
her left upper eyelid and edema of her left
eyebrow CT revealed complete opacification
of the left frontal and ethmoid sinuses with
hyperexpansion and erosion of bone Fig 1
3-D image reconstruction revealed complete
erosion of the medial third of the left superior
orbital rim MRI revealed a T1 hypointense
T2 hyperintense enhancing mass centered in
the left frontal sinus with extension into the
left anterior ethmoid air cells Fig 2
Destruction of the anterior and posterior
frontal tables was seen with erosion through
the superiormedial orbital wall and
impingement on the left medial rectus The
mass entered the anterior cranial fossa and
abutted the anteroinferior frontal lobe dura
Concern was for a malignant neoplasm but
biopsy revealed a CMF The patient
underwent a combined endoscopic and open
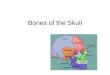
bicoronal approach for resection Fig 34
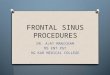
Figure 4 5 View of the posterior table after tumor excision Pericranial flap used for reconstruction
Figure 34 Bicoronal approach with osteplastic flap open Largest fragment of excised tumor
Author Age
(yr)gender
Symptoms at
presentation
Location Radiographic features Treatment approach Follow up
Azorin4 46M Supracilliary mass
otherwise
asymptomatic
Frontal sinus Destruction of the
posterior table with
dural involvement
Subfrontal approach
superior orbitotomy
en block resection
22mo DF
Baujat7 50F NAO HA Nasal bone extension into
ethmoids and frontal sinus
Invasion of skull base
dural involvement
Frontal osteoplastic
bone flap and dural
excision
18mo DF
Castle8 43F Sinus pressure Ethmoids invading through LP Bony erosion
displacement of
orbital contents
NR NR
Cruz9 10F Progressive
exophthalmos
Ethmoids invading through LP LP erosion and orbital
compression
Bicoronal approach
with en bloc tumor
resection
NR
Frank10 26M Diplopia Petroussphenoid bones
extending into clinoid sella
and cavernous sinus
Calcifications on CT Subtemporal approach
to excision
NR
Hashimoto11 32M Painless forehead
swelling
exophthalmos
Ethmoid sinus with extension
into frontal sinus and orbit
Lobulated mass on CT
with bony erosion
Excision 2yr DF
Isenburg12 34F NAO Ethmoids Calcifications on CT Endoscopic excision 8mo DF
Januszek13 51F NR Nasal septum extension into
sphenoid and maxillary sinus
Bony erosion on CT Excision Recurred at
12mo with re-
excision
Kadom6 14M Decline in school
performance HA
NAO
Frontal bone extension into
ethmoid and frontal sinus
with orbital infiltration
intradural extension
Calcifications on MRI
partially cystic and
inhomogeneous
Excision NR
Keel14 65F HA Clivus with sphenoid and
ethmoid extension
Bony erosion on CT Curettage 26mo DF
Keel14 66F NAO Sphenoid with extension into
ethmoids and hard palate
Bony erosion on CT Curettage recurred at
6mo radiation
given and DF
at 20mo
Keel14 34F Vision changes HA Clivus with nasopharynx
extension
Bony erosion on CT Incomplete excision
via curettage radiation
11mo DF after
radiation
Koay15 57F Painless swelling
over nasal dorsum
Nasal bone with extension
into frontal and ethmoid
sinuses
Erosive features on CT Incomplete excision
reported
NR
McClurg3 49F NAO Nasal septum with extension
into maxilla
Bony expansion and
destruction
Midface degloving 16mo DF
Mendoza16 1moM Respiratory
difficulty since birth
Ethmoid sinuses Homogenous
enhancement on MRI
En block resection 2yr DF
Morris17 52F Vertigo Sphenoid sinus locally destructive with
calcifications on CT
Endoscopic excision 2yr DF
Nazeer18 66F NAO Sphenoid sinus with sellar
and nasopharynx extension
Expansile and
enhancing on T1 MRI
heterogeneous on T2
Curettage Recurred at
1yr repeat
curettage and
DF at 6mo
Nazeer18 20daysM NAO Ethmoid sinuses Bony erosion on CT Excision 12mo DF
Perez-
Fernandez19
60M NAO epistaxis Maxillary sinus with ethmoid
extension
Bony expansion and
erosion
Combined endoscopic
and Caldwell-Luc
resection
5yr DF
Smith20 49F NAO Floor of nasal cavity
extending into hard palate
Bony erosion Excision 30mo DF
Shek37 6F NAO epistaxis
visual impairment
Ethmoids frontal bone maxilla nasal cavity
sella turcica
Heavily calcified Curettage x4 and
radiation following last
excision
Recurred until
radiation
Thomas21 NR Facial pain NAO Nasal cavity and palate NR En bloc excision 2yr DF
Townsend 45F HA visual changes Frontal sinus with extension
into orbit ethmoids and
dural abutment
Bony erosion
T1hypointense
contrast enhancing T2
heterogeneous
Osteoplastic frontal
sinus flap
6mo DF
Veras22 60F Incidental finding Nasal septum Sclerotic and scalloped
edges on CT lobulated
mass
Excision 12mo DF
Vernon23 44M Retroorbital pain Sphenoid sinus with
nasopharynx extension
Bony erosion on CT T2
heterogeneity
Endoscopic removal
with ethmoidectomy
NR
Wang24 60F Incidental finding Nasal septum with ethmoid
extension
Bony erosion on CT Excision 6mo DF
Wolf25 35F Frontal HA Frontal-sphenoid junction
with orbital infiltration
Expansion into orbital
cavity
Craniotomy with
piecemeal removal
NR
Yoo26 2moM Dyspnea nasal
cavity mass
Nasal cavity inferior
turbinate
T1 enhancing T2
heterogeneous
Combination of
debridement and bloc
resection
2yr DF
Yahgi35 38F NAO serous
rhinorrhea
Clivus with extension into the
sphenoid
Expansile lesion on CT Transmaxillary
excision incomplete
excision
Persistent
tumor re-
excised and DF
at 45yr
Twenty eight cases were identified including 6
in patients less than 18 years old Table 1 A
review by McClurg et al identified 20 of these
cases There were several reports of dural
involvement orbital infiltration and erosion of
bone into the cavernous sinus The nasal
septum and ethmoid sinuses were the most
frequently reported origin Presentation
commonly included nasal airway obstruction
visual disturbances and headache On CT
CMF appear as a soft tissue density with
frequent expansion of or frank erosion of bone
Gross calcifications are seen roughly 15 of the
time MRI features include low signal intensity
on T1 images contrast enhancement and
heterogeneous enhancement on T2 sequences
similar to other cartilaginous tumors Histologic
features include well circumscribed lobulated
tumors with both myxoid and chrondroid
elements Mitosis are rare and areas of necrosis
are infrequently seen but occasional mild to
moderate nuclear atypia is seen and can
contribute to the difficulty in correct diagnosis
Treatment is primarily surgical Tumor
recurrence was most common after curettage
resection and re-excision or external beam
radiation were subsequently used for control A
small 1-2 rate of malignant transformation of
CMF after radiation was reported
Table 1
HL Jaffe L Lichtenstein Chondromyxoid fibroma of bone distinctive benign tumor likely to be mistaken especially for cho1 ndrosarcoma Arch Pathol 45 (1948) 541ndash551
Hammad HM Hammond HL Kurago ZB Frank JA Chondromyxoid fibroma of the jaws Case report and review of the literature Ora2 l Surg Oral Med Oral Pathol Oral Radiol
Endod 1998 Mar85(3)293-300
McClurg S Leon M Teknos T Iwenofu H Chondromyxoid fibroma of the nasal septum Case report and review of literature 3 Head Neck 2013 Jan35(1)E1-5
Azor4 ın A Gil G Saacutenchez-Aniceto C Ballestın F-J Martınez-Tello Chondromyxoid fibroma of the frontal sinus British Journal of Oral and Maxillofacial Surgery Volume 41 Issue
6 December 2003 418-420
Ostrowski ML Spjut HJ Bridge JA 5 2002Chondromyxoid fibromas In Fletcher CDM Unni KK Mertens F editors World Health Organization Classification of Tumors Pathology
and genetics of tumours of soft tissue and bone Lyon IARC Press 2002 p 243ndash245
Kadom N Rushin EJ Yuan A Santi M Chondromyxoid fibroma of the frontal bone in a teenager 6 Pediatr Radiol 2009 Jan39(1)53-6
Baujat B Attal P Racy E et al Chondromyxoid fibroma of the nasal bone with extension into the frontal and ethmoidal sinus7 es report of one case and a review of the literature
Am J Otol 200122150ndash153
Castle J Kernig M Chondromyxoid fibroma of the ethmoid sinus Head Neck Pathol 8 2011 2011 Sep5(3)261-4
Cruz AA Mesquita IM Becker AN Chahud F Orbital invasion by chondromyxoid fibroma of the ethmoid sinus Ophthal Plast Reco9 nstr Surg 200723427ndash428
Frank E Deruaz JP de Tribolet N Chondromyxoid fibroma of the petrous10 -sphenoid junction Surg Neurol 198727182ndash186
Hashimoto M Izumi J Sakuma I Iwama T Watarai J Chondromyxoid fibroma of the ethmoid sinus Neuroradiology 11 1998 40577ndash579
Isenberg SF Endoscopic removal of chondromyxoid fibroma of the ethmoid sinus Am J Otolaryngol 12 199516205ndash208
Januszek G Niemczyk K Gornicka B Gotlib T Chondromyxoid fibroma of the nasal septum Otolaryngol Pol 13 2010 6488ndash92
Keel SB14 Bhan AK Liebsch NJ Rosenberg AE Chondromyxoid fibroma of the skull base a tumor which may be confused with chordoma and chondrosarcoma A report of three
cases and review of the literature The American Journal of Surgical Pathology Volume 21(5) May 1997 pp 577-582
Koay CB Freeland AP Athanasou NA Chondromyxoid fibroma of the nasal bone with extension in the frontal and ethmoid sinuses15 J Laryngol Otol 1995109258ndash261
Mendoza M Gonzalez I Aperribay M Hermosa JR Nogues A Congenital chondromyxoid fibroma of the ethmoid case report Pedia16 tr Radiol 199828339ndash341
Morris LG Rihani J Lebowitz RA Wang BY Chondromyxoid fibroma of sphenoid sinus with unusual calcifications case report w17 ith literature review Head Neck Pathol
20093169ndash173
Nazeer T Ro JY Varma DG de la Hermosa JR Ayala AG 18 Chondromyxoid fibroma of paranasal sinuses report of two cases presenting with nasal obstruction Skeletal Radiol
1996 25 (8) 779-782
Perez19 -Fernandez CA Armengot-Carceller M Lozano de Arnilla CG Valles AP Basterra-Alegria J Chondromyxoid fibroma of left maxillary and ethmoid sinuses Acta
Otorrinolaringol Esp 20096070ndash72
Smith CA20 Magenis RE Himoe E Smith C Mansoor A Chondromyxoid fibroma of the nasal cavity with an interstitial insertion between chromosomes 6 and 19 Cancer Genet
Cytogenet 2006 Dec171(2)97-100
Thomas B21 Black C Maddox T Venkatraman G Chondromyxoid fibroma of the nasal cavity and palate Ear Nose Throat J 2011 Oct90(10)E17-9
Veras EFT Santamaria IB Luna MA Sinonasal chondromyxoid fibroma Ann Diagn Pathol 22 20091341ndash46
Vernon SE Casiano RR Sphenoid sinus chondromyxoid fibroma mimicking a mucocele Am J Otolaryngol 23 200627406ndash408
Wang C Morrow T Friedman P Lara JF Chondromyxoid fibroma of the nasal septum a case report emphasizing clinical correlat24 ion Am J Rhinol 20001445ndash49
Wolf DA Chaljub G Maggio W Gelman BB Intracranial chondromyxoid fibroma Report of a case and review of the literature A25 rch Pathol Lab Med 1997121626ndash630
Yoo YT26 1 Park JH Sunwoo WS Rhee CS A huge chondromyxoid fibroma of the nasal cavity in a newborn baby Auris Nasus Larynx 2012 Aug39(4)422-4
Wu CT Inwards CY O27 rsquoLaughlin S Rock MG Beabout JW Unni KK Chondromyxoid fibroma of bone A clinicopathologic review of 278 cases Hum Pathol 199829438ndash446
Sreedharanunni S Rajwanshi A Vaiphei K Gupta N Bansal S Fine needle aspiration cytology in two cases of chondromyxoid f28 ibroma of bone and review of the literature
Diagnostic Cytopathology Vol 41 No 10 904-908
De Las Casas LE29 Singh HK Halliday BE Xu F Strausbauch PH Silverman JF Myxoid chondrosarcoma of the sphenoid sinus and chondromyxoid fibroma of the iliac bone
cytomorphologic findings of two distinct and uncommon myxoid lesions Diagn Cytopathol 2000 Jun22(6)383-9
Nasir30 -Ud-Din Ahmed A Pervez S Ahmed R Kayani N Chondroblastoma a clinico-pathological analysis J Coll Physicians Surg Pak 2014 Dec24(12)898-901
Shek TW Peh WC Leung G Chondromyxoid fibroma of skull base a tumour prone to local recurrence J Laryngol Otol 31 1999 113380ndash385
Zillmer DA Dortman HD Chondromyxoid fibroma of the bone 32 36 cases with clinicopathologic correlation Hum Pathol 1989 20 932ndash964
Haroon S33 Nasir-Uddin Pervez S Kayani N Ahmed R Hafeez K Umer M Chondromyxoid fibroma experience of 36 cases of an intriguing entity J Pak Med Assoc 2014
Dec64(12 Suppl 2)S175-9
Hersh DS Firempong AO Chesler D Castellani RJ Woodworth GF Chondromyxoid fibroma invasion of the transverse34 -sigmoid sinus junction causing posterior fossa hemorrhage
Journal of Clinical Neuroscience Volume 24 February 2016 Pages 149-150
Yaghi N DeMonte F Chondromyxoid Fibroma of the Skull Base and Calvarium Surgical Management and Literature Review J N35 eurol Surg Rep 2016 Mar 77(1) 023ndash034
Shek TW Peh WC Leung G 36 Chondromyxoid fibroma of skull base a tumour prone to local recurrence J Laryngol Otol 1999 113 (4) 380-385