Embed Size (px)
Citation preview

From biomarkers for patient selection to
companion diagnostics in drug development
Gerard Sanderink, PhD
Sanofi R&D

DEFINITION OF BIOMARKER
• A biomarker is a defined characteristic that is measured as an indicator of normal biological processes, pathogenic processes, or responses to an exposure or intervention, including therapeutic interventions.
• Molecular, histologic, radiographic, or physiologic characteristics are considered to be types of biomarkers.
• A biomarker is not an assessment of how an individual feels, functions, or survives
| 2

Characteristics of an “Ideal Biomarker
modified from Bay-Jensen 2018 CO Rheumatology | 3
Characteristics Description
Specific • Not present in non-target tissue/organ
Sensitive • Low baseline level without disease or drug treatment
• Rapid change with disease state or after drug treatment
• High ratio between baseline and disease or treated state
Stable • Sufficient stability
• Correlation of biomarker level with extent of disease or drug response
• Low variability of biomarker levels between and within the same population of
subjects
Robust • Rapid, simple, accurate and inexpensive detection
Low patient burden • No biopsy needed
• Detection in urine, serum or plasma

Biomarkers in Early Development
| 4
• Predictive Biomarker
• Identifies patients more likely to benefit of a drug treatment
• Patient selection, enrichment
• Identify patients with better possible treatment outcomes to show proof-of-concept
• Potential future companion diagnostics
• Prognostic Biomarkers
• Identifies patients with a possible specific outcome, independent of treatment
• identify fast progressors
• To allow for shorter studies, less subjects for proof-of-concept trial
• Diagnostic Biomarker
• Defines patients with a disease or a subset thereof
Analytical Method needs
sufficient precision to
show between-subject
variability
0
2
4
6
8
10
12
14
Baseline EoT
BM
val
ue
Placebo /BM+
Drug / BM-
Placebo / BM-
Drug / BM+
posritive outcome
0
2
4
6
8
10
12
14
16
18
20
Baseline EoT
BM v
alue
BM+ / Placebo
BM+ / Drug
BM- / Placebo
BM- / Drug
progression

Serum protein as predictive biomarker
• Periostin as predictive biomarker of lebrikizumab treatment on FEV1 in asthma patients
• Corren et al, N Engl J Med 2011: 365: 1088-98
| 5

• Support to clinical Phase I program:
• Inclusion criteria: Diagnosis of Ag-positive solid tumors defined as moderate to intense membrane staining of ≥ than 15% of tumor cells in patients with measurable and/or non-measurable disease for which no standard therapy is available
precision : CV% < 10.4% on bladder tumor / CV%<5.4% on ovarian tumor, 3 XT
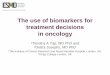
Predictive Biomarker; Immunohistochemistry assay for patient screening
STEP1: SAR used as primary Ab to detect Antigen
STEP4: DAB revelation
STEP2: biotinylated mouse anti DM4 secondary Ab
STEP3: Amplification with DABmap (streptavidin-Biotin-Peroxidase)
Brown precipitate
DAB
H2O2 H2O
Ag
Positive control used to validate batches Bladder – 7-384-T, score 3+ on membrane and 2+ in cytoplasm
Negative tissue control TUM3539 – Ramos xenograft

Prognostic biomarker; Imaging classification of ADPKD
Model helps to recruit a homogeneous patient population
| 7

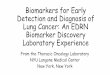
Diagnostic Biomarker; glucosylsphingosine (lyso-GL1) in type 1 Gaucher disease
Biomarkers & CDx - Club Phase I 5 April 2018 | 8
N Dekker et al. Blood 2011;118:e118-e127
Response of plasma glucosylsphingosine to therapy.
(A) Responders to enzyme replacement therapy ERT).
(B) Poor responders to ERT.
(C) Substrate reduction therapy (SRT)
Glucosylsphingosine and glucosylceramide levels in plasma of type 1 Gaucher
patients and controls
open circles ; homozygous mutation N370S

Response Biomarkers in Development
| 9
• Target Engagement
• Proof - of - Mechanism
• Level, duration of response; support dose selection
• Pharmacodynamic / early disease progression Biomarkers
• Rapid indication of clinical benefit – Proof-of-Concept
• Surrogate marker
• Allows for shorter, smaller studies with early read-out
• Safety Biomarkers
• Surrogate Endpoint
• Validated: approved marker that can substitute for a clinical endpoint • eg Hb1Ac – HIV RNA – LDL-cholesterol
• Likely surrogate endpoint • Tumor response rate, PFS
• Can allow for accelerated approval, followed by post-approval confirmation
Method needs to be able
to show within-subject
variability
- change from baseline

Response Biomarkers – PD/TE
• CD38 receptor occyupancy by isatuximab in vitro and in vivo
Biomarkers & CDx - Club Phase I 5 April 2018 | 10
In vitro determination of CD38 occupancy by isatuximab on CD4+ T
lymphocytes (T4), CD8+ T lymphocytes (T8), B lymphocytes (B cells),
and monocytes from normal donors compared to theoretical calculated
RO (curve).
RO measured in bone marrow as a factor of isatuximab concentrations
measured in plasma after the second dose

Biomarker Analysis performance
Clinical Validation
Analytical Validation
Biomarker Discovery Phase I
Profiling / Multiplexing
Biomarker Application Phase I-II Studies
Proof-of-Concept / MOA Dose Escalation
Support Label Claim Patient stratification Differentiate Product
Companion Diagnostic
Phase II-III Studies Prolonged Clinical
Endpoint Proof-of-Concept / MOA
Dose Optimization
High
Low
Low
High
Exploratory BM Confirmatory BM
Adapted from R. Bowsher

Biomarker Assays: what performance criteria?
•Exploratory?
•Fit-for-purpose?
•Qualification?
•Full Validation?
16-May-18 12

Biomarker assays aren’t PK assays
PK
Assays But
• Many aspects of the
testing can be
performed
• Some additional work
must be done
However,
different
requirements and
criteria may
apply
• Endogenous compound – no pure “blank” matrix • Multiple isoforms • No exact reference – rhP may have different stability, affinity • Precision adapted to inter-individual and intra-individual variability,
expected response • Qualitative methods

If biomarker assays are not PK assays….. • What really matters for biomarker assays?
To understand what is being measured • The value of assessments with endogenous samples (LLOQ, selectivity, stability)
To understand the assay’s capabilities and limitations • Will dictate how the assay can be deployed and what decisions can be made
To detect changes in analyte levels that are meaningful • > biological + analytical variability
14
• Standard validation parameters • Precision (Inter and intra assay precision)
• Specificity
• Selectivity
• Parallelism (especially important to use endogenous samples)
• Relative accuracy
• Stability (especially important to use endogenous samples)
• Operator effect
• Be aware of critical reagent variability & supply, especially for long trials
• Cross-validation of different batches of kits may become necessary

Serum protein as predictive biomarker – periostin • Assay needs already good qualification and/or standardization to be reproducible over time
• eg test kit may not be interchangeable: two-fold difference in concentrations and different predicitivity
• KIT 1 periostin
Dose 1
Dose 2
• KIT 2 periostin
Dose 1
Dose 2

Predictive Biomarkers in Late Development (and beyond)
| 16
• A predictive biomarker can be used to select patients for Phase II / III trials
• To enrich study with patients at risk and to increase the PoS to demonstrate efficacy
• Targeted therapy
• Dose optimization
• In the US these regulations apply:
• Laboratory Developed Tests (LDT)
• CLIA – accredited labs
• In Vitro Device Exemption (IDE)
• For marketed drugs;
• Companion Diagnostic (CDx)
• Complementary Diagnostic
• In the EU:
• CE-marked tests (medical device subclass)
• In Vitro Diagnostics Directive 98/79/EC
• New regulations are being implemented;
• Medical Device Regulation (2020)
• In Vitro Diagnostic Regulation (2022)

Laboratory developed tests (LDTs)
| 17
• LDTs are a specific class of IVD laboratory
tests that hospitals, academic, and clinical
laboratories develop as testing services
according to their own procedures
• Often created in response to unmet
clinical needs, and are commonly used for
early diagnosis, monitoring, and guiding
patient treatment
Laboratory Developed Tests
http://www.acla.com/issues/laboratory-developed-tests/
Regulated by a comprehensive federal statutory
framework under the Clinical Laboratory
Improvement Amendments (CLIA)
Generally no FDA oversight; no 510(k)
premarket submission
Allows for efficient development and
implementation

Clinical Laboratory Improvement Amendments (CLIA)
• The CLIA law is administered by the US federal Centers for Medicare and Medicaid services (i.e., “CMS”) in conjunction with the FDA. CLIA is defined in 42CFR part 493 and was initially enacted due to high error rates in laboratory testing.
• The intent of CLIA is to ensure accuracy, reliability and timeliness of patient test results regardless of where the test is being performed.
• The CLIA federal law regulates clinical laboratory testing on specimens taken from human subjects undergoing some form of medical monitoring or response to treatment.
• In the US, it is required to perform clinical analysis under CLIA regulation if results will be used to diagnose or make treatment decisions.
| 18

Quality Standard Regulations
• Personnel Standards and Competency Assessment
• Board certified lab director, clinical consultant, supervisors, and testing personnel.
• Continuing Medical Education & Annual Competency Evaluation
• Patient Test Management
• Proper sample prep/collection, identification, and accurate reporting of results
• Quality Events
• Quality Plan
• Proficiency Testing Program:
• participate in three testing events of CAP per year
• External/Internal PT programs
• State Regulation (e.g., MA, NY..)
19

CLIA Lab vs. CLIA-grade Test
20
Labs approved by accreditation organizations with deeming authority under the CLIA
CLIA certification in specialty/sub-specialty areas Pre-analytical, analytical and post-analytical
compliance. CLIA and CAP require that laboratories validate
the performance of tests. This requirement applies when the lab Replaces a test system or instrument; Adds a new test or Changes the manufacture of a test kit.
Labs are subject to Dept. of Health and Human Services to conduct unannounced inspection at any time during its hours of operation
Labs are inspected by CLIA/State DPH every 2 years.
CLIA-grade Test CLIA Lab
Assay Performance Specification (similar to GCLP validated assays)
Reference ranges fit the patient population(s)
Require external and/or internal Proficiency Testing to monitor assay performance (not required for GCLP)
Data interpretation and test results sign-offs by
board certified director(s) Tests performed by qualified lab personnel
Crystal Sung, BCB-Clinical Diagnostics

Investigational IVDs; Investigational Device Exemption (IDE)
| 21
IDE for Dx =~IND for Rx
• Investigational IVD • IVD used in decisions on how to enroll, assign or manage subjects in a
therapeutic product clinical trial • That has not already received marketing authorization for that specific intended
use (e.g., to select patients for treatment with a therapeutic product) • Non-exempt IVD; “significant risk”
• if incorrect results would have potential consequences for subjects (diagnosis, curing, mitigating, treating disease)
• Need to apply for IDE (Investigational Device Exemption) • Exempt IVD
• Not used for diagnosis (eg exploratory), or with confirmation by other method or only retrospective
• Non-invasive (surplus of samples for other purpose allowed) • Need to justify to IRB or FDA

Companion Diagnostics (CDx)
| 22
• Companion Diagnostic (CDx)
• A medical device, often an in vitro device (IVD), which provides information that is essential for the safe and effective use of a corresponding drug or biological product
• Generally approved along with a NME
• Intended use/Indications for use: • Clinical purpose (diagnosis, prognosis, monitoring)
• Target population for whom the test is intended
• May need to validate threshold and show absence of therapeutic benefit for negative test result
• Complementary Diagnostic
• A test that aids in the benefit–risk decision–making about the use of the therapeutic product, where the difference in benefit–risk is clinically meaningful
• Complementary IVD information is included in the therapeutic product labeling

Characteristics and Potential Uses
| 23
Potential Uses for CDx
Patient Identification 1
Risk Stratification 2
Efficacy monitoring 3
Used to support safe and effective use
of paired product
Analytical validation and clinically
validation required
Regulated as in vitro diagnostic device
(IVD); subject to pre and post market
controls; risk based classification
High analytical quality required
General Characteristics
Optimal Dosing 4
Companion Diagnostics are paired with a product There are FDA cleared IVDs not paired with specific products

Late development – Companion Diagnostics
• About 30 tests approved so far in the US
• 29 are in Oncology, for 15 drugs and their combinations
• 10 for herceptin-based therapy alone
• Methodologies
• PCR – 10 + 1 NGS
• IHC – 10
• In Situ Hybridization - 8
• 1 in Thalassemia (MRI)
• Complementary Diagnostics
• Two approved in 2015 and 2017
• Both IHC for PD-L1 checkpoint inhibitors
| 24

US FDA guidance for CDx
• Guidance for Industry and FDA staff:
In vitro companion diagnostic devices
(finalized in Aug 2014) • Defines CDx and describes various scenarios for use
• Contemporaneous regulatory approvals of the device and drug
• Principles for Co-development of an In Vitro Companion Diagnostic Device with a Therapeutic Product (draft issued in July 2016)
• Co-development process
• Regulation of Investigational IVDs and Therapeutic Products
• Clinical Trial Design Consideration
• Marketing Authorizations and labeling considerations
| 25

Companion Diagnostic and clinical trial phases
| 26
Image from: Luo, Dee et al. "A Quantitative Assessment of Factors Affecting the Technological Development and Adoption of Companion Diagnostics."
Front. Genet. Frontiers in Genetics 6 (2016): n. pag. Web.
510k, PMA
for CDx
NDA for
therapeutic
Crystal Sung 24Apr17

Marker based clinical trial designs
| 27
● Design A, interaction or biomarker-stratified design
● Evaluates treatment and marker effects, and their interaction
● Predictive & prognostic value ● Allows to confirm (and adjust) cut-off
● Design B, targeted or selection design ● evaluates treatment effects in a
targeted population by selecting only those who are test-positive.
● Trt A = experimental arm Trt B = standard-of-care or placebo.
FDA Draft Guidance- principles for codevelopment of an in vitro companion
diagnostic device with a therapeutic product - July 2016)

Scientific Review on Device Performance
• Analytical Performance characteristics
• Reliability
• Accuracy of analyte measurement
• Clinical Performance characteristics
• Clinical sensitivity
• Clinical specificity
• Need to assess lack of benefit in negative test population
• Labeling
• Intended use, device design, directions for use, warnings, result interpretation and etc
| 28

• New regulation IVDMDR (EU) 2017/46
• Official Publication May 2017
• 3 or 5 year transition period:
• Medical Device Regulation 2020
• In Vitro Diagnostic Regulation 2022
• New IVD classification
• 4 risk classes A, B, C, D - Companion Diagnostics are class C
• 7 rules
• B, C, D to be validated by Notified Bodies (80% devices)
• Demonstrate Clinical Evidence (Scientific, Analytical, Clinical performance)
• Post-marketing follow-up; performance evaluation, updated annually for class C, D
• One registration in EU, traceability through Unique Device Identifier (UDI), European Data Base
European IVD regulations
• CE-marked tests (medical device subclass)
• so far regulated by In Vitro Diagnostics Directive 98/79/EC
• Four classes (general, self-testing, B & A)
• Mainly self-certified (80%)
• Multiple registration procedures
Biomarkers & CDx - Club Phase I 5 April 2018 | 29

Conclusion
• Every Program/Project is unique in the biomarker need.
• Understanding the intended use of biomarkers during drug development is important.
• Since biomarkers (assays) need to be qualified in the context of their intended use, using them as part of the clinical trial process will provide evidence of the marker’s clinical utility.
• Prepare, plan and ensure that the quality of biomarker assays used for patient selection/companion diagnostics can support FDA, CLIA and EU requirements as they evolve.
30

Acknowledgements
• Special thanks to : Crystal Sung , Ph.D., D(ABMLI) Head Clinical Diagnostics, BCB Framingham
• With support from:
• Marie-Hélène Pascual
• Nathalie Mace
• Anne-Laure Bauchet
Biomarkers & CDx - Club Phase I 5 April 2018 | 31

THANK YOU!

FDA-approved Companion / Complementary Dx tests
• Oncology
• ERBITUX (cetuximab)/VECTIBIX (panitumumab) – 3 tests colorectal cancer – 2 PCR, 1IHC
• GILOTRIF (afatinib) therascreen Non-small cell lung cancer - PCR
• GLEEVEC (imatinib mesylate)- 3 tests – 3 cancer types – 1 IHC, 1PCR, 1FISH
• HERCEPTIN (trastuzumab) + combo’s - 10 tests – breast cancer – 5 IHC, 5 xISH
• IRESSA (gefitinib) - Non-small cell lung cancer - PCR
• KEYTRUDA (pembrolizumab) PD-L1 - Non-small cell lung cancer - IHC
• LYNPARZA (olaparib) - Ovarian cancer - PCR
• MEKINIST (trametinib)/ TAFINLAR (dabrafenib) - Melanoma - PCR
• RUBRACA (rucaparib) - Ovarian cancer - NGS
• TAGRISSO (osimertinib) - Non-small cell lung cancer - PCR
• TARCEVA (erlotinib) - Non-small cell lung cancer - PCR
• VENCLEXTA (venetoclax) - Chronic lymphocytic leukemia FISH
• XALKORI (crizotinib) - Non-small cell lung cancer - 2 IHC, 1 FISH
• ZELBORAF (vemurafenib) - Melanoma - PCR
•
Biomarkers & CDx - Club Phase I 5 April 2018 | 33
• Thalassemia
• EXJADE (deferasirox) - Thalassemia - MRI
• Complementary Diagnostics
• OPDIVO (nivolumab) PD-L1 Melanoma, Non-small cell lung cancer - IHC
• TECENTRIQ (atezolizumab) PD-L1 - Bladder cancer, Non-small cell lung Cancer - IHC