Embed Size (px)
Citation preview

Från Hench till MainiBehandling av rheumatoid
artrit
Några kapitel ur farmakoterapins historia som jag upplevt
ellerNågra farmakas uppgång och fall i
kampen mot RA
Lund 12 Nov 2004

• Bromine containing hypnotics – RA pharmacotherapy in the 1950’ties
• NSAIDs: From ASA to Cox-2• Cortisone – an on-going saga• D-penicillamine – the box of Medusa• Anti-TNF –The first Crafoord Prize• Some remaining challenges
– DMARDS vs biologicals– How to use cortisone– Is there a risk of over-treatment?
From Hench to Maini (Sir Ravinder)
Lund 12 Nov 2004
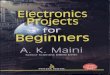
The beginning…
Question: Can the bromine containing hypnotics give rise to bromism?Method: Determine total urine Br after oxidizing and organic Br after precipitation with silver nitrate.Material: Patients from ”Reumaten” (and FAW)
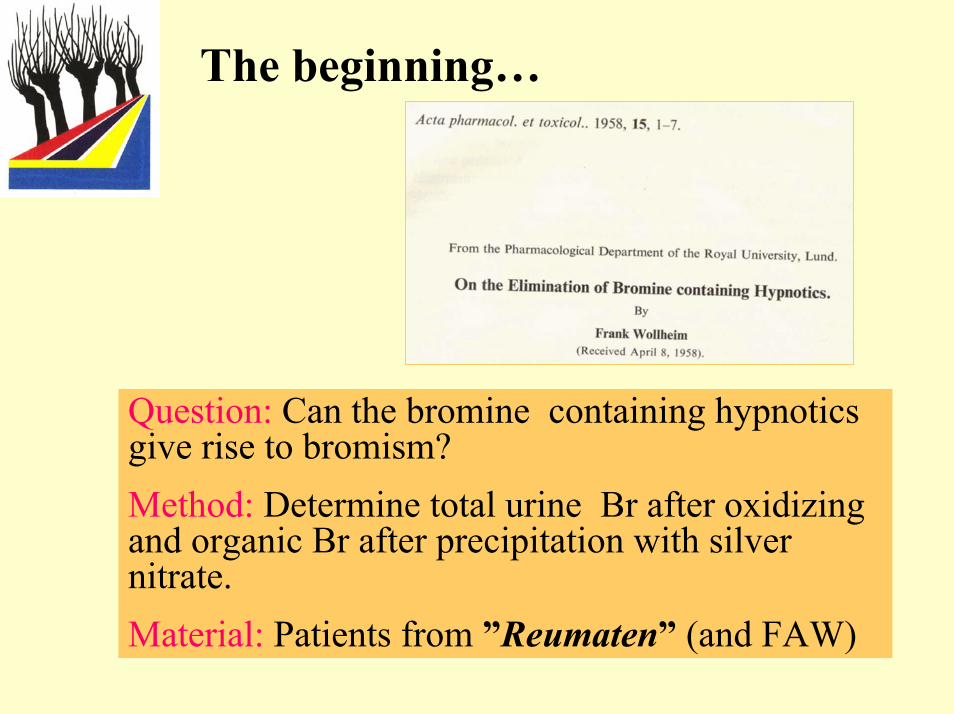
Brome excretion in urine
Lund 12 Nov 2004

Total and organic urinary bromine Department of Pharmacology in 1957
Lund 12 Nov 2004

Pharmacotherapy of RA in the 1950’ties
• Aspirin 1898• Gold salts 1927• Sulfasalazin 1942 (Stockholm) • Phenacetin-Paracetamol• Fenylbutazone 1952• Glucocorticoids 1949• Antimalarials - 1948• Intra-articular Osmium tetroxide 1959
Osmic acid in arthritis therapy.Acta Rheumatol Scand. 1959;5(1):70-4.
BERGLÖF FE.
Lund 12 Nov 2004
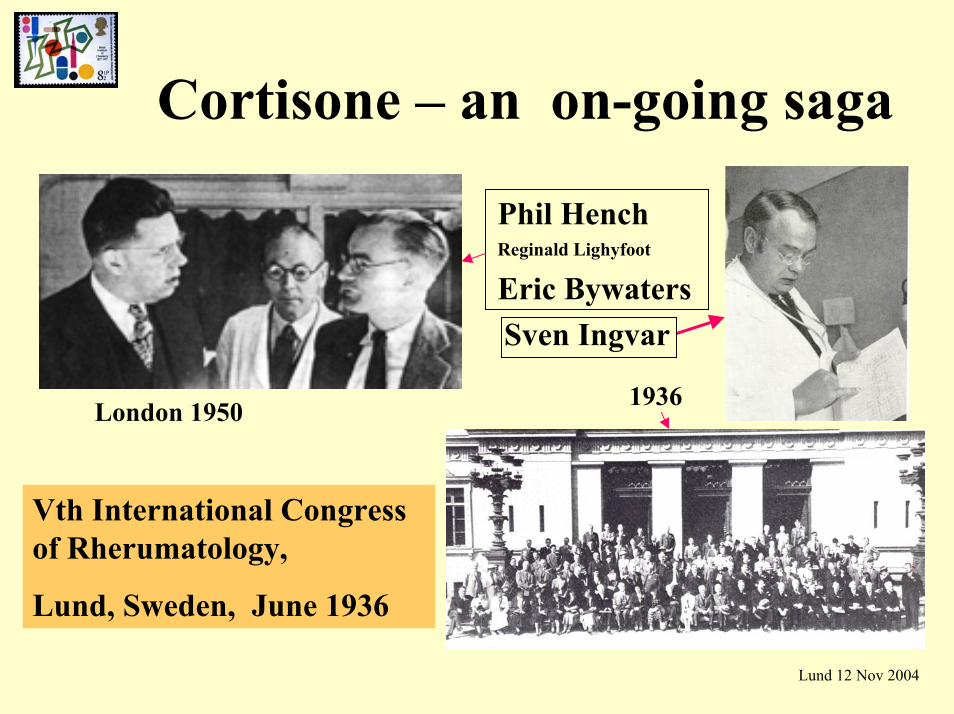
Cortisone – an on-going saga
Phil HenchReginald Lighyfoot
Eric BywatersSven Ingvar
1936London 1950
Vth International Congress of Rherumatology,
Lund, Sweden, June 1936
Lund 12 Nov 2004
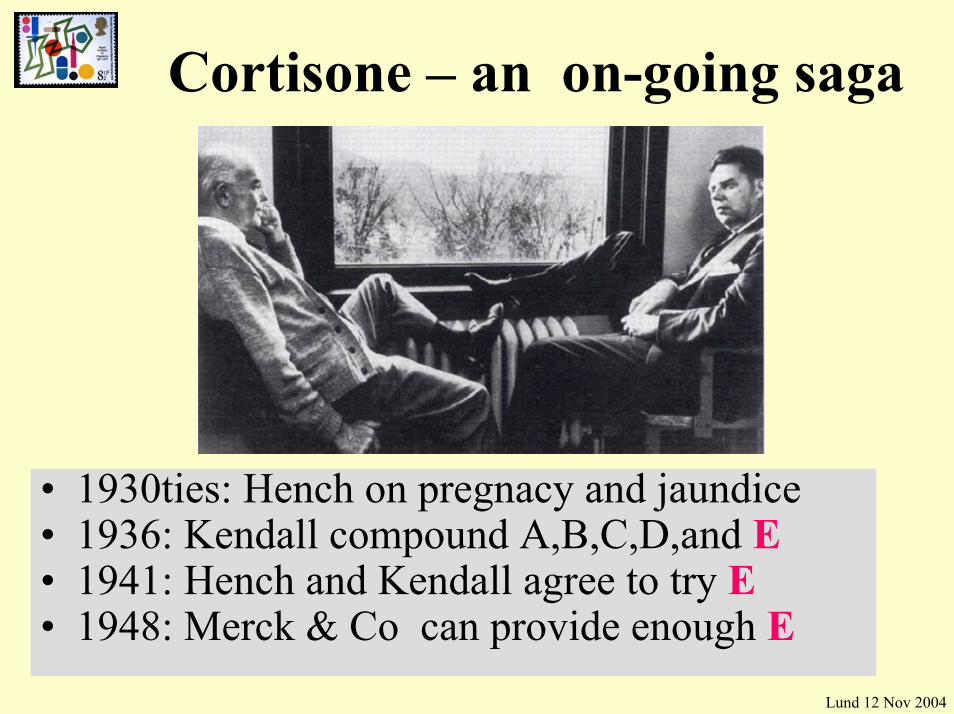
Cortisone – an on-going saga
• 1930ties: Hench on pregnacy and jaundice• 1936: Kendall compound A,B,C,D,and E• 1941: Hench and Kendall agree to try E• 1948: Merck & Co can provide enough E
Lund 12 Nov 2004
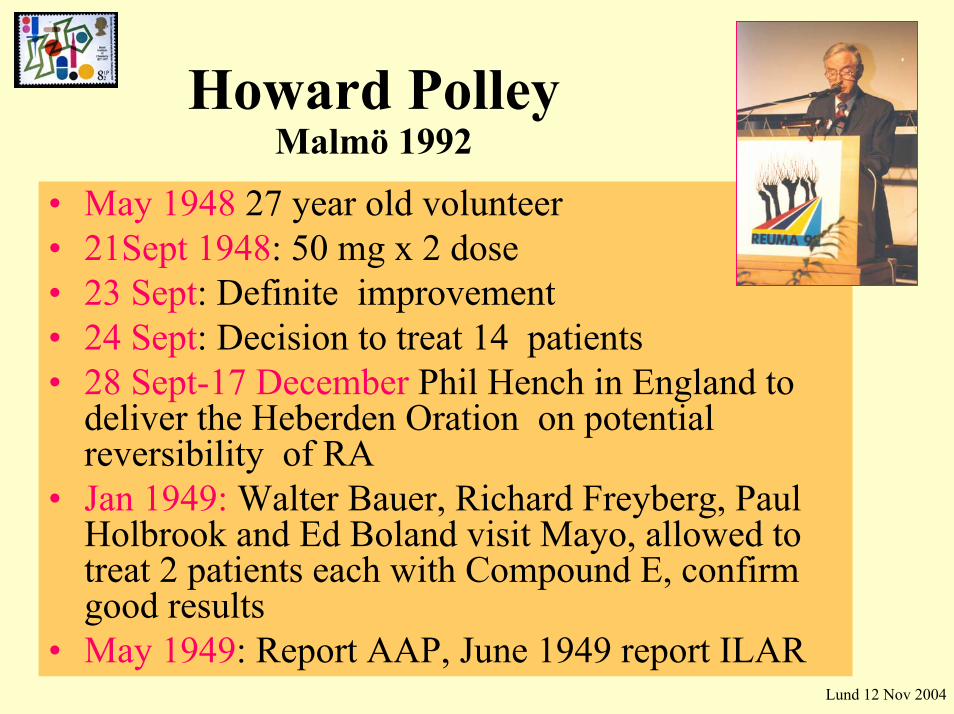
Howard Polley Malmö 1992
• May 1948 27 year old volunteer• 21Sept 1948: 50 mg x 2 dose• 23 Sept: Definite improvement• 24 Sept: Decision to treat 14 patients• 28 Sept-17 December Phil Hench in England to
deliver the Heberden Oration on potentialreversibility of RA
• Jan 1949: Walter Bauer, Richard Freyberg, Paul Holbrook and Ed Boland visit Mayo, allowed to treat 2 patients each with Compound E, confirm good results
• May 1949: Report AAP, June 1949 report ILARLund 12 Nov 2004
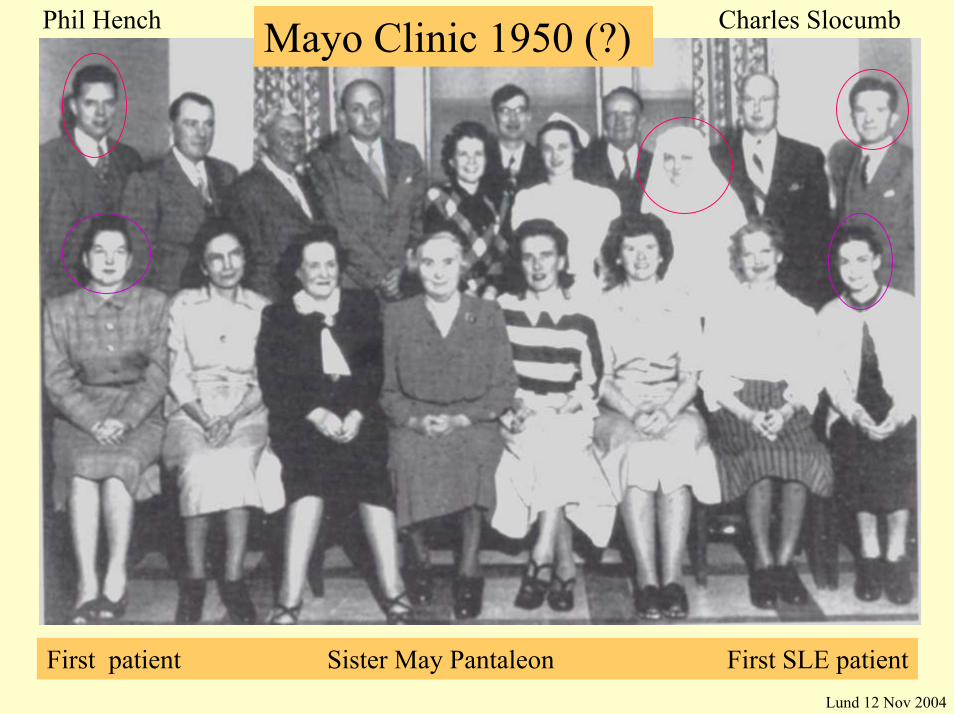
Mayo Clinic 1950 (?)Phil Hench Charles Slocumb
First patient Sister May Pantaleon First SLE patientLund 12 Nov 2004

Cortisone -The ups and downs
• Initial euphoria –1949 to early fifties• Immediate and long term adverse reactions• Disease modification?
– Empire Reumatism Council to present
• Management of adverse reactions– Dosing of the glucocorticoid– Route of administration– Preventive strategies– Improved glucocorticoid preparation???
Lund 12 Nov 2004

At what hour should prednisolon be administered?
• 26 pat:s randomly given 5 or 7.5 mg prednisolon at 7.30 am or 2.00 am
• The effect was better on symptoms and IL-6 in the 2 am group after 5 days
• Both groups had similar (modest) effects on ESR, CRP and SAAReference:Arvidson NG et. al ARD 1997;56:27-31
Lund 12 Nov 2004

Do glucocorticoids retard joint damage?
• 1959 2nd MRC-study(prednisolone) -yes• 1983 Ed Harris-study(18 patients) - yes ?• 1984 Million et al - (toxicity) - yes (?) • 1994 Mc Dougal - no• 1995 Kirwan-2 year study -yes• 1997 Boers 28 mo study - yes• 1998 Simera-18 month study -yes• 1998 Kirwan- 3 year follow up -yes
Lund 12 Nov 2004

CorticoateroidsCorticoateroids
Corticosteroids and radiologic progression
SIMERACyclosporin
vsGold
Brit J Rheumatol 1998;37:874-82

ARC low dose glucocorticosteroid study group
ARHickling et al. Brit J Rheumatol 1998;37:930-45
Lund 12 Nov 2004

Cortisone -Medical complications• Early unavoidable: Insomnia, boosted appetite• Patients at risk factors: Hypertension, diabetes,
peptic ulcer, acne• Dose related: Cushing, HPA suppression,
infections, osteonecrosis, sarcopenia• Insidious: Osteoporosis, skin atrophy, cataract,
atheroscleosis, growth inhibition.• Rare, unpredictible: Psychosis,glaucoma,
pancreatitis (Ann Int Med 1993;119:1198-1208)

Glucocorticoids: mechanism of action
• Glucocorticoids, cyclosporin A and gold function by modulating gene activation
• GC receptor activation inhibits NF-κB, AP-1, NFATp and C/EBP function
• Small molecule selective inhibitors of one or multiple transcription factors identified
• p38 MAPK inhibitors block synthesis of TNF-α and IL-1
Lund 12 Nov 2004

Glucocorticoids: mechanism of action
Macrophage
Science 1995;270:286 Lund 12 Nov 2004

Two ducks with one pillThe sulphasalazine story
Nanna Svartz MD h.c in HelsinkiSalazopyrin, a new sulfanilamide preparation
N Svartz Acta Med Scand 1942;60:577-98Sulphasalazin discontinuation in RA – no flares
R Gullberg et al 1977 ?Sulphasalazin in rheumatoid arthritis
B McConkey BMJ 1980;280:442-4”This is a popular first choice drug…
RS Amos BMJ 1995;310:652-654 Sulfasalazine resistance –induces ABCG2
Gerrit Jansen. Rheum Dis. 2004;63:138-43.

University College London1952 Charles Dent’s lab
Wilson´s Wilson´s diseasedisease
John M Walshe at his laboratory in the Department of Experimental Med Cambridge 1960

The penicillamine story• ”The story of penicillamine: a difficult birth.”
John Walshe Mov Disord. 2003 Aug;18(8):853-9.– Identified in urin as a –SH aa after penicillin intake
(London 1952)– First 3 patients with Wilson’s respond to 1 g of D-pen
Am J Med 1956;21:4587-95
• The effect of penicillamine on the laboratoryparameters in rheumatoid arthritis. Jaffe IA Arthritis Rheum 1965;8(6):1064-79
• Controlled trial of D-penicillamine in rheumatoid arthritis.Multicentre Trial Group: The Lancet 1973;1:275-285

Formation of mixed Di-sulphides and S-methyl-
D-pen in vivo
Inactive
Active

α1-antitrypsin-IgA complexes
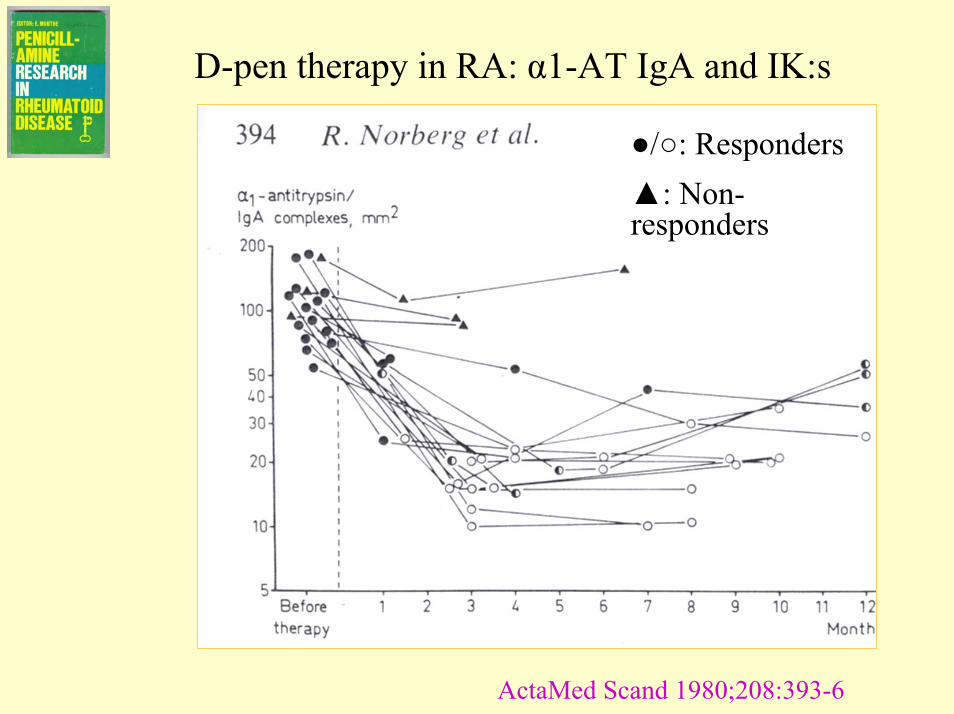
D-pen therapy in RA: α1-AT IgA and IK:s
●/○: Responders▲: Non-responders
ActaMed Scand 1980;208:393-6

Plasma cystine in RA patients on D-pen
Scand J Rheumatol 1979 Suppl 28:21-23
Penicillamine –the promises• Wilson´s disease• Lead poisoning• Cystinuria• Rheumatoid arthritis• Scleroderma• Primary biliary cirrosis• Macroglobulinemia

Managing D-penicillamine in RA
Responder, thrombopenia, proteinuria Responder, SLE syndrome

• Myastenic syndrome• Lupus• Proteinuria• Goodpasture´s syndrome• Thrombocytopenia• Agranulocytosis• Aguesia• Pemfigoid• Proteinuria• Polymyositis• An so on….
Penicillamine – the toxicity

Changing DMARD practicesThe Malmö clinic
48%
34%
Bergström U et al. Scand J Rheumatol 1999;28:160-5

NSAIDs: many ups and downs
• Indometacin in Minneapolis 1964• Diclofenac in Malmö 1973• ASA –slow release issue
– Micro-incapsulated Premaspin• The benoxaprofen (Opren) story and closure• The piroxicam (Felden) experience• The indosmos disaster• The Cox-2 drama
– Cox in paradise– One pill a day does not put the the doctor away
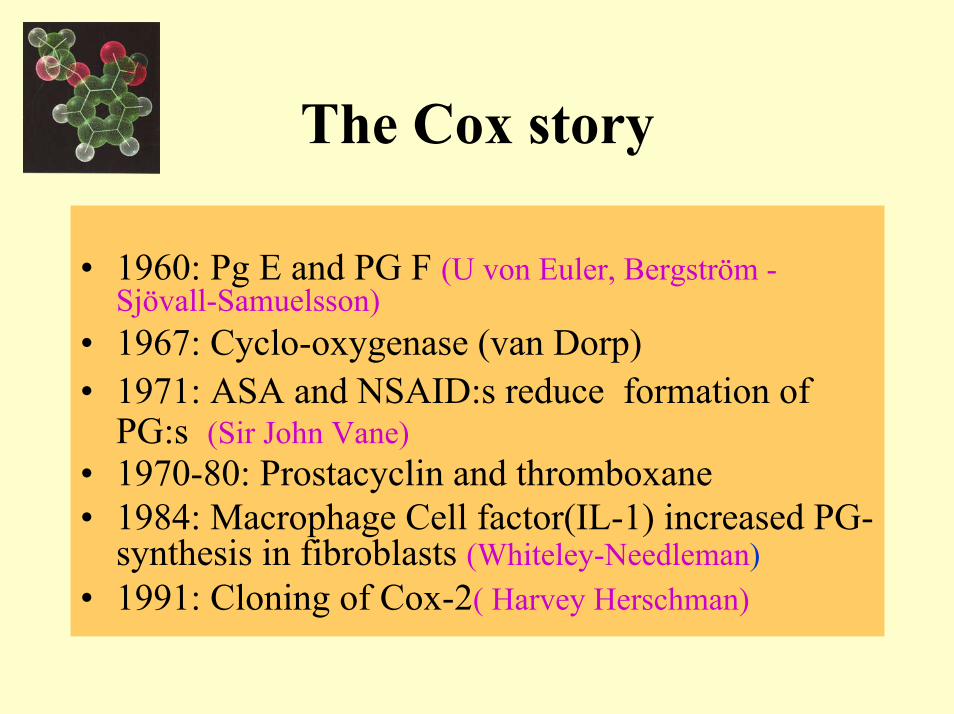
The Cox story
• 1960: Pg E and PG F (U von Euler, Bergström -Sjövall-Samuelsson)
• 1967: Cyclo-oxygenase (van Dorp)• 1971: ASA and NSAID:s reduce formation of
PG:s (Sir John Vane)• 1970-80: Prostacyclin and thromboxane• 1984: Macrophage Cell factor(IL-1) increased PG-
synthesis in fibroblasts (Whiteley-Needleman)• 1991: Cloning of Cox-2( Harvey Herschman)

Cox-2 physiology
• Role in ovulation and nidation• Role in renal development• Role in salt excretion• Role in GI ulcer healing• Expressed in eye• Expressed in pancreatic islet beta cells• Produces ~ 75% of PGE2 and PGI
FW Turku 2000
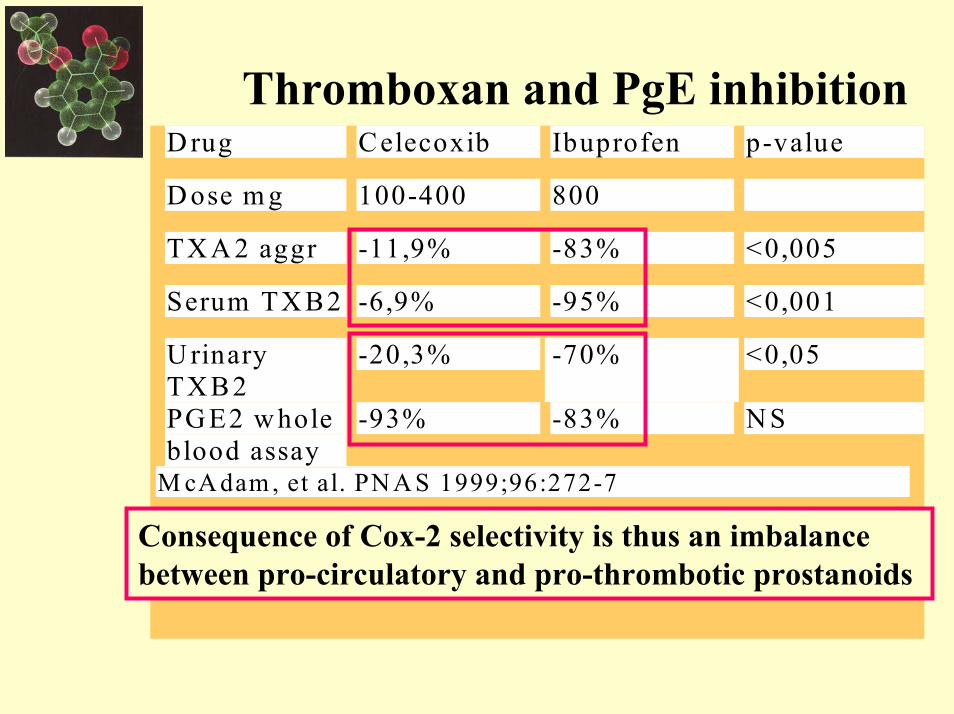
D rug Celecoxib Ibuprofen p-value
D ose m g 100-400 800
TX A 2 aggr -11,9% -83% <0,005
Serum TX B2 -6,9% -95% <0,001
U rinaryTX B2
-20,3% -70% <0,05
PG E2 w holeblood assay
-93% -83% N S
M cA dam , et al. PN A S 1999;96:272-7
Consequence of Cox-2 selectivity is thus an imbalance between pro-circulatory and pro-thrombotic prostanoids
Thromboxan and PgE inhibition
InhibitionInhibition of Cox2 of Cox2 aggravates aggravates doxorubicindoxorubicin--mediated cardiac mediated cardiac
injury in injury in vivovivo
• Doxorubicin induces Cox2 in rat neonatalcardiomyocytes
• Doxorubicin causes cardiac injury• Selective Cox2 inhibitor SC236 aggravates
this• Selective Cox 1 inhibitor SC 560 inert• Iloprost reverses SC236 aggravation
NP Dowd. JCI 2001;108:585-90
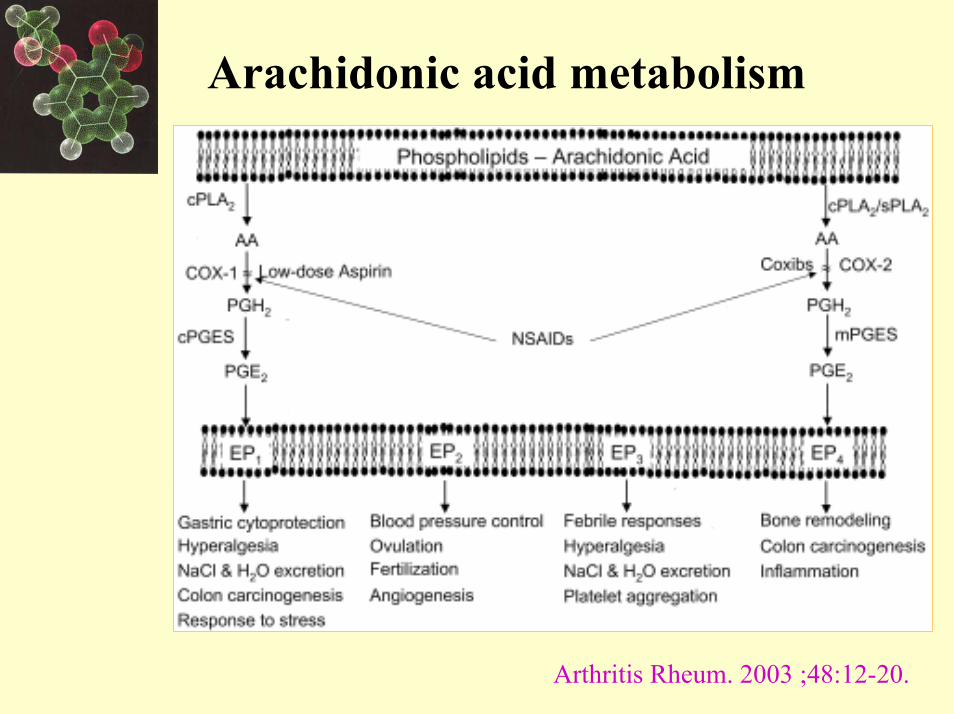
Arachidonic acid metabolism
Arthritis Rheum. 2003 ;48:12-20.

Cox inhibition and PGI
Arthritis Rheum. 2003 ;48:12-20.
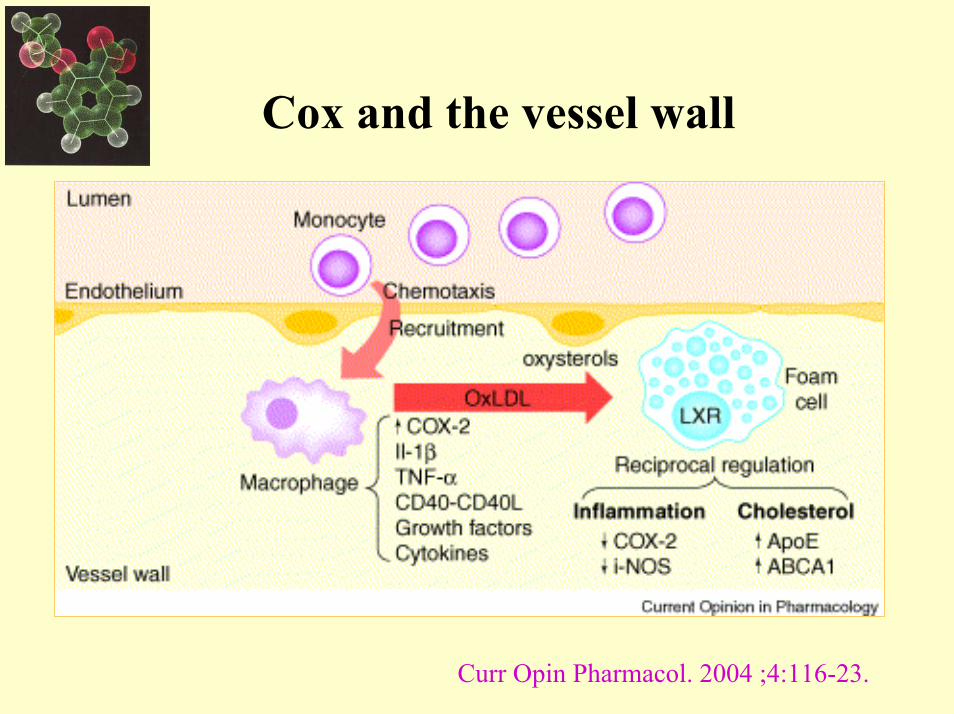
Cox and the vessel wall
Curr Opin Pharmacol. 2004 ;4:116-23.
Crafoord Prize Lund 2000
Tiny Maini, Margareta Nilsson, Marc Feldmann
EULAR Berlin 2004
Herman Mielants, Mrs and George Kollias, Sir Ravinder Maini
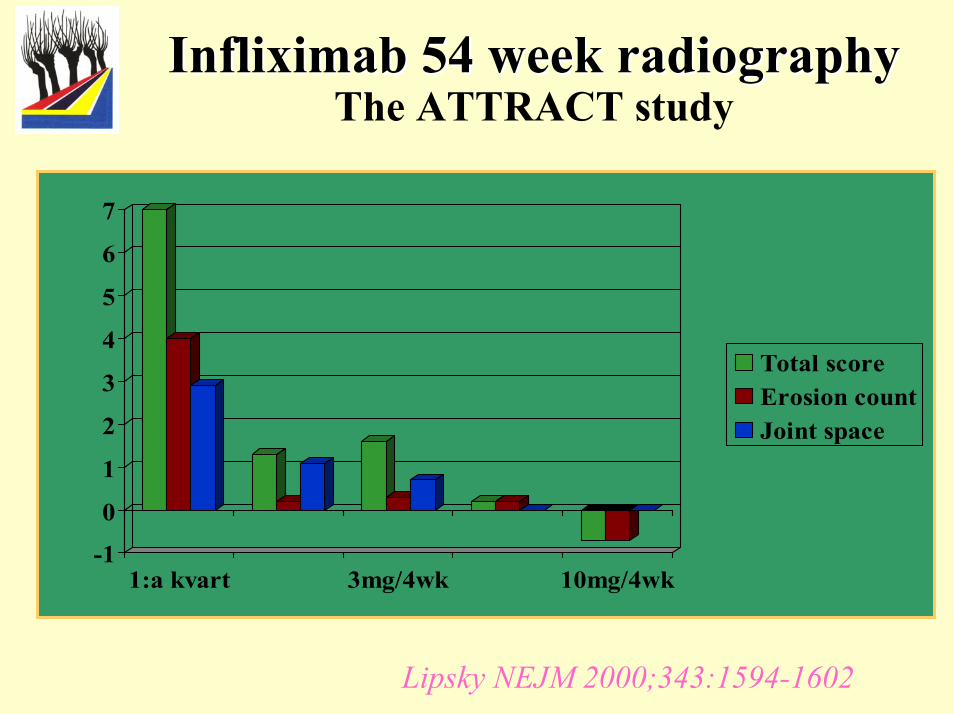
Infliximab Infliximab 54 54 week radiographyweek radiographyThe ATTRACT study
-1
0
1
2
3
4
5
6
7
1:a kvart 3mg/4wk 10mg/4wk
Total scoreErosion countJoint space
Lipsky NEJM 2000;343:1594-1602

History of TNF in RA
• TNFα but not LT in SF and S, correlation toactive disease Saxne et al A&R 1988;31:1041-5
• Tumour necrosis factor in synovial exudates.Di Giovine et al, Ann Rheum Dis. 1988 Sep;47(9):768-72.
• Synovial presence of TNF in RA but not in OAHusby and Williams J Autoimun 1988;1:363-71
• TNF and IL-1 mRNA in synovial cell inRA Buchanet al Clin Exp Immunol 1988;73:449-55
• TNF antibodies inhibit IL-1 synthesis in RA Brennan et al Lancet 1989 Jul28;2:244-7

Discovery of natural TNF inhibition
• ”A tumor necrosis factor binding protein is present in human biological fluids” Peetre, Thysell, Grubb and Olsson Eur J Haematol 1988;41:414
• Purification and biologic characterization of a tumor necrosis factor alpha inhibitor Seckinger, Isaaz and Dayer J Biol Chem 1989;264:11966-73
• Two tumor necrosis factor-binding proteins purified from human urine. Evidence for immunologic cross-reactivity with cell surface tumor necrosis factor receptors Engelman, Novick and Wallach J Biol Chem 1990;265:1531-5

Biologicals in RA
• Anti CD4 – safe but not effective• Campath-1 – effective (?) but not safe• IL-1Ra – safe but mainly good at retarding
destruction• TNF-inhibitors – the break-through drugs !!• But they do not cure, there are risks and not
all patients respond

Artritis Rheum 2003;48:3308-19

New targets ?
Artritis Rheum 2003;48:3308-19
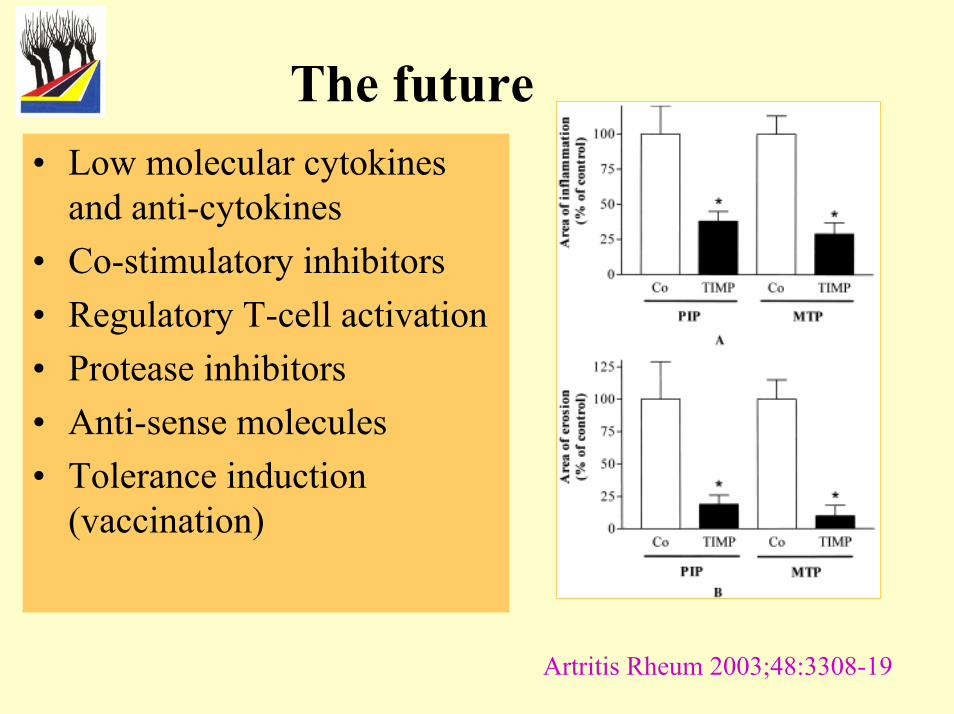
The future• Low molecular cytokines
and anti-cytokines• Co-stimulatory inhibitors• Regulatory T-cell activation• Protease inhibitors• Anti-sense molecules• Tolerance induction
(vaccination)
Artritis Rheum 2003;48:3308-19
• Bromine containing hypnotics – RA pharmacotherapy in the 1950’ties
• NSAIDs: From ASA to Cox-2• Cortisone – an on-going saga• D-penicillamine – the box of Medusa• Anti-TNF – The first Crafoord Prize• Some remaining challenges
– DMARDS vs biologicals– How to use cortisone– Is there a risk of over-treatment?
Summing up
Lund 12 Nov 2004
The end

![MAINI PRECISION PRODUCTS LIMITED - Capital …SUDARSHAN KUMAR MAINI, SANDEEP KUMAR MAINI, GAUTAM MAINI AND CHETAN KUMAR MAINI PUBLIC OFFER OF UP TO [ ] EQUITY SHARES OF FACE VALUE](https://img.pdfslide.us/doc/110x75/5f2b395e885ffb34c179bf00/maini-precision-products-limited-capital-sudarshan-kumar-maini-sandeep-kumar.jpg)