Embed Size (px)
Citation preview

Thorax (1955), 10, 157.
FOREIGN BODY GRANULOMATA OF THE LUNGS DUETO LIQUID PARAFFIN
BY
J. C. WAGNER, D. I. ADLER, AND D. N. FULLERFrom the Department of Pathology, South African Institute for Medical Research, and the Thoracic Surgery Unit,
General Hospital, Johannesburg
(RECEIVED FOR PUBLICATION SEPTEMBER 20, 1954)
This paper is based on the clinical, operative,and pathological findings of five cases of liquidparaffin granulomata of the lung.
HISTORICALThe recognition of oil granulomata of the lung
followed the use of oils as a vehicle for medicamentsand radio-opaque substances in diagnostic broncho-graphy.Rosenberg (1885) used menthol in olive oil for
the treatment of tuberculous laryngitis. Thistreatment was fairly widely adopted. Followingthe discovery of the efficacy of chaulmoogra oilas a treatment for leprosy this oil was substitutedfor the menthol by Lukens (1922). They believedthat medicated oils did not penetrate further thanthe larynx. This was disproved by Guieysse-Pellissier (1920), who showed, in rabbits, that oliveoil injected into the larynx could be demonstratedin the alveoli within six hours. Corper and Freed(1922) showed that oil placed in the nasal cavitywas also carried to the alveoli. Laughlen (1925)first described cases of lipoid pneumonia followingthe use of nose drops of which the base was liquidparaffin. Pinkerton (1927) described six cases inwhich he could trace the pathogenesis from asimple lipoid pneumonia to a discrete fibrotic oilgranuloma.Graef (1935) suggested that mineral oils gain
entrance to the lungs by (a) not irritating the surfaceof the pharyngeal mucosa and so not exciting acough reflex; (b) the presence of mild anaestheticsubstances in the mineral oil, such as menthol,enhancing the passage of the oil into the trachea;(c) a defect of the cilia in chronic respiratory infec-tions; and (d) loss of the cough reflex in weak- anddebilitated patients.
Ikeda (1937) distinguished between infantile andadult forms of lipoid pneumonia. The " infantile
form" can occur in infants and the aged. Thislesion, usually of a diffuse nature, is essentially aninterstitial proliferative inflammation not infre-quently combined with exudative pneumonia. The" adult type," usually localized, mostly occursamong older persons as a result of the habitualself-administration of oil in large amounts bymouth or intra-nasally over a long period, andoccasionally also as a result of direct intra-trachealinstillation. Ikeda pointed out the clinical andradiographical difficulty of distinguishing these"adult " lesions from other intrapulmonary lesions.
Stryker (1941) showed that liquid paraffin canbe absorbed from the gut and demonstrated in theregional lymph glands. Daniel, Frazer, French,and Sammons (1953) suggested that a portion ofthe liquid paraffin taken by mouth is absorbed fromthe gut as fatty acids. It is possible that liquidparaffin in an emulsified form may be carried inthe lymphatic ducts directly into the systemic venouscirculation and thence to the lungs. Some of thecases of " paraffinoma" that have been describedby previous authors may have had their origin inthis way.The intra-tracheal injection of radio-opaque
substances in oil was first carried out in animals byWaters, Bayne-Jones, and Rowntree (1917). Someof these animals died of a proliferative bronciio-pneumonia in which the alveolar and bronchialepithelium was stated to be considerably hyper-trophied. Sicard and Forestier (1922) used " lipio-dol," which is iodized poppyseed oil, to demonstratethe bronchial tree in human subjects. Pinkerton(1928) after extensive investigation came to theconclusion that (1) mineral oil is quickly emulsifiedin the lungs and taken up by the alveolar phagocyteswhich fill the alveoli, producing a consolidationwhich is followed by fibrosis; (2) most vegetableoils produce practically no reaction in the lung even
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

J. C. WAGNER, D. L ADLER, and D. N. FULLER
if retained for a long time; (3) animal oils produceoil granulomata; (4) the reaction of the lungs toan oil varies directly with the free fatty acid contentof the oil; (5) poppyseed oil and sesame oil beingalmost inert are suitable for bronchography. Thisview was generally held until Brody (1943) firstdescribed an oil granuloma due to iodized poppy-seed oil following bronchography. The granulomaoccurred distal to a bronchial obstruction causedby a carcinoma. A further case of " lipiodol "granuloma due to poppyseed oil was reported byFortner and Miles (1950). Cases of oil granulomataof the lung due to iodized poppyseed oil have beenreviewed and investigated by Felton (1952). Heexamined 37 lung specimens from 34 patients, allofwhom had had bronchograms with iodized poppy-seed oil 46 to 1,404 days before operation. In23 of the specimens residual poppyseed oil wasdemonstrated, and in six cases oil granulomatawere found.
Similar granulomata have been found elsewherein the body following the use of "lipiodol." Rubin(1939) reviewed 27 cases inwhich "lipiodol" was usedfor uterosalpingorrhaphy in which radiographswere taken from one month to one year afterwards.In 18 cases residual " lipiodol" was observed andin one further case an oil granuloma was subse-quently removed at operation.
PATHOLOGY
Jacob and Faure-Fremiet (1917) described thehistological features of subcutaneous paraffinomata.By recognizing the similarity between these lesionsand those seen in the lung, Pinkerton (1927) wasthe first to describe a " paraffinoma of the lung."The case was that of a boy aged 6 who had beengiven medicated liquid paraffin nose drops over aperiod of several months. At post-mortem exam-ination, several firm, discrete nodules were foundin the lung. Macroscopically these were consideredto be neoplastic in origin, but section " showed thelung tissue to be virtually replaced by a looseconnective tissue framework interspersed by numer-ous small lipoid droplets, large mononuclear cells,lymphocytes, and occasional eosinophils and neutro-phils." In this case there were deposits of liquidparaffin in the bronchial lymph glands and thespleen. In several other cases he emphasized thepresence of liquid paraffin in the peribronchiallymphatics and in one case he noted lymphoidfollicles developing along the course of the oil-containing lymphatics. Ikeda (1937) discussed 18cases of the " adult type " recorded in the literature.These cases were due to the instillation of liquid
paraffin, mostly intra-nasally, but a few cases fol-lowed oral administration. He stated that
" Liquid paraffin acts purely as a foreign bodywhich is initially removed mainly by expectorationand partly by wandering phagocytes. The smallamount of residual lipoid leads to a low-grade inflam-mation of the foreign body type. The active agentsfor which the liquid paraffin is a vehicle (e.g., menthol,thymol, and ephedrine) may set up an acute chemicalreaction which, however, is of short duration. Thepathological nature of the adult type of lipoid pneu-monia therefore is essentially that of a paraffinomaof the lung. Its various stages of development extendfrom an early non-suppurative proliferative inter-stitial pneumonitis to a chronic granulomatous foreignbody reaction with widespread fibrosis and tume-faction of the involved area."He described the three cardinal features as (1) a
diffusely spreading fibroblastic proliferation whichobliterates the usual alveolar framework; (2) thewidespread infiltration by plasma cells and lympho-cytes; (3) a few large, foamy macrophages withinthe stroma and irregular masses within the distortedalveoli. In the more fibrous areas alveoli arerepresented by distended spaces surrounded by athick, densely fibrous collagenous connective tissueframework. These spaces are filled with oil whichtends to become adherent to the inner lining andoften forms a large crescent giant cell. Numerousforeign-body giant cells are present and there areareas of pseudo-tubercle formation. Lymphoidnodules form along the course of the draininglymphatic presumably due to the rupture of theseover-distended vessels.
Vascular changes in the lung containing liquidparaffin granulomata were first described byHastings (1950), who stated that there was pro-liferation of the elastic tissue in the walls of theblood vessels. Young, Applebaum, and Wasser-man (1939) discussed a case in which there wasa liquid paraffin granuloma of the lung with necro-tizing changes in the kidneys, adrenals, and ovaries.This case is remarkably similar to those publishedby Fienberg (1953) under the title of " Necrotisinggranulomatosis and angiitis of the lungs withmassive splenic necrosis and focal thromboticgranulomatous glomerulo-nephritis."
CASE HIsTORIEs
CASE I.-A. V. C. was a man aged 50 who wasasymptomatic until July 10, 1952, when he noticed hoarse-ness, a dry cough, and, a week later, pleuritic pain inthe left anterior chest. While under treatment withinjections and inhalations of penicillin, he developed a
constant pain in the left shoulder and on two occasionshad profuse night sweats. After a month his symptomsabated and he returned to work. Within a week the
158
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

GRANULOMATA OF LUNG DUE TO LIQUID PARAFFIN
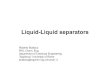
-Radiograph of August 14, 1952, showing a dense left apical
shadow with a suggestion of tissue breakdown and elevation of
the hilum.
_~~
~~~ ~ ~ ~ ~ ~ ~ ~ ~
4"
V
4t, te.., * ai s 1 b e
01tt>X
< s 1wS4'~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~
A
.S.irs># .,._~9*,r, .
ev~~~~~~~~~~i
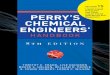
FIG. 3.-Photomicrograph showing accumulation of alveolar epithe-
lium, lymphocytes, plasma cells and occasional multinucleargiant cells in one corner of the alveolus. Note cuboidal appear-ance ofalveolar epithelium, x 140.
FIo. 2.-Specimen from Case 1 showing liquid paraffin granuloma.
V
containing liquid paraffin x 120
159
r
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

J. C. WAGNER, D. L. ADLER, and D. N. FULLER
.'w - t
* 4 7t ,
t,t X # b
J VR f >
:C @ a.:. *..o
. t
*.
s 4 ., . e #Xt . . *. * - * . .:v
&
Hs .6 e
*- ^ * *
e.**. S + y i.
.. ._ # {. s.
^ e s vi s_e b
.. f .. . :w . .X . ^.¢-s
_. ^ >
4
.: * w *
i s
{. b
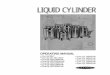
FIG. 5.-A fibrosed area in which a pedtunculated mass of fibroustissue projects into the alveolus, x 129.
.. ,£,
::1#
..A: P O iC
4 *r
A.^
A
4 4-
O1 r
*S
FIG. 6.-A general increase in reticulin in the necrotic area, 120.
a
4'
4.a,-S:
*le'.
)$-e ~ ~1,_ScwS ¢
. #.$I
FIG. 7.-An arteriole in which there is marked endarteritic change. Note the globules of oilin the lumen and the oil-containing vacuoles in the wall of the vessel,' x il40.
160
.I7
'r..4 .,
.A
. P,:p: Oll04 ... :..
1.
.f 1
A .- 14
.1 'i j.f 4
0
*.1I
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

GRANULOMATA OF LUNG DUE TO LIQUID PARAFFIN 161
0l~~~ ~ ~ ~ ~ ~ ~ +-18
4W~~~~~~~~~4
411
!--.."USo4meA;1
'Xs
W X v.A'+'-& to t s-'a}
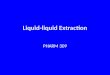
FIG. 8.-Sudan IV stain showing the lipoid in the lacunae in thewall of an arteriole, x 145.
FIG. 9.-The fragmentation of the elastic laminae in the wall of thesame vessel as shown in Fig. 6 is well demonstrated, x 230.
FIG. IO.-The needle-shaped crystals in the alveolar phagocytes in the granuloma, x 145.
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

J. C. WAGNER, D. I. ADLER, and D. N. FULLER
cough recurred and became productive of offensive,creamish-brown sputum which was occasionally blood-stained. The pain also became more severe and wasworse on lying down, so that he had to spend some nightssitting in a chair to obtain relief. On August 14 hischest was radiographed. The radiograph showed adense left apical opacity extending to the sixth ribposteriorly, slight mediastinal displacement to the leftand elevation, but no increase, in the left hilar shadows(Fig. 1). Two days later he was admitted to the medicalwards of the Johannesburg General Hospital under thecare of Professor Elliott. His previous history revealedthat for many years he had suffered from sinusitis forwhich he had been treated intermittently with nosedrops. It could not be ascertained subsequently whetherthese drops were oily. Apart from the fact that he hadlost a little weight and had smoked 30 to 40 cigarettesdaily for many years his history contributed nothing. Onadmission his pulse was 108 and his respirations were28 per minute. His temperature was 100.60 F.
Examination revealed a flushed individual with noabnormal physical signs apart from diminished move-ment and air entry with increased vocal resonance atthe left apex. A blood examination showed no anaemiabut a leucocytosis of 12,000 per c.mm. with a normaldifferential count. Pending further investigation peni-cillin, 500,000 units, was given twice daily and theinitial fever ranging between 990 and 1030 F. graduallydropped to normal by lysis at the end of the fifth week.On August 21 tomography demonstrated the lesion inall films from 6 to 13 cm. in depth. Marked peri-bronchial thickening of the apical segmental bronchuswas shown on the 12 cm. cut and the 8 cm. film showedsimilar involvement of the subapical bronchus.On August 28 bronchoscopy showed no abnormality
apart from broadening of the left upper lobe carina:suitably fixed bronchial slides and sputa did not revealmalignant cells. A further radiograph on September 16showed the left apical lesion to be smaller, but tomo-graphy confirmed the previous findings and failed todemonstrate hilar glandular enlargement. A diagnosisof bronchogenic carcinoma was therefore made andleft thoracotomy was performed on September 18.The lung was firmly adherent over the upper lobe,especially over three fairly well circumscribed areaswhere it had to be separated extrapleurally. The lungunderlying these three areas was firmer than elsewhere.From the origin of the left upper lobe bronchus densecords of peribronchial tissue could be felt radiating outto the three above-mentioned areas. A left pneumonec-tomy was performed and the paucity of hilar glands,mainly sub-aortic and the size of millet seeds, noted.Recovery from operation was uneventful.
Pathological Examination.-Macroscopically the leftupper lobe showed a yellowish white tumour massmainly in the subapical segment with extension intothe apical segment. The pleura over the subapicalsegment was thickened and there was a small cavity1 cm. below the thickened pleura. The cavity had afairly smooth wall and contained yellowish whiteinspissated material. These macroscopic appearances
were very suggestive of a tuberculous cavity with infiltra-tion by tuberculous granulation tissue around thecavity (Fig. 2).
Sections taken from the subapical segment showed ageneralized obliteration of the normal lung tissue byloosely woven collagen fibres and fibroblasts, in whichthere were foci of lymphocytes and plasma cell infiltra-tion, with occasional multinucleate giant cells. In thisfibrous tissue there were numerous irregular spaces,which on frozen section could be shown to contain oil.In the regions where the alveoli were still distinguishable,they were grossly distorted and were either lined by acuboidal epithelium and contained foamy alveolarphagocytes in which sudanophilic material could bedemonstrated (Fig. 3), lymphocytes, plasma cells, andmultinucleate cells, or the epithelium was desquamatedand the fibrous-walled alveoli were packed with foamyalveolar phagocytes (Fig. 4). In the more denselyfibrosed areas groups of lymphocytes, plasma cells, andgiant cells were surrounded by fibrous tissue whichseparated them from the alveolar lumina resulting in apedunculated mass of fibrous tissue projecting into thealveolus (Fig. 5). In one region there was dense fibroustissue with hyalinization of many of the collagen fibres,surrounding a necrotic focus in which there was a densereticular network (Fig. 6). The most striking featureof these sections was the generalized endarteritis, whichwas most marked in the arterioles. In some vesselsthe lumina were obliterated. This endarteritis was mostmarked in the vessels surrounding the necrotic area.Oil globules were observed in the lumina of somearterioles and small lacunae containing sudanophilicmaterial were seen in their walls (Figs. 7 and 8). Inoccasional obliterated vessels there was evidence ofrecanalization.The elastic tissue in the vessel walls appeared to
have undergone a series of degenerative changes. Inthose arterioles in which there was early endarteriticchange, the elastic laminae were contorted, with somefragmentation of the intervening elastic fibrils. Thevessels in the walls of which the oil lacunae occurredshowed fragmentation of the elastic laminae at the siteof the vacuoles (Fig. 9). In the fibrosed vessels theelastic tissue had completely disappeared or remainedas small fragments. Under a polarizing microscopenumerous needle-shaped negatively birefringent crystalswere seen in the oil-containing alveolar phagocytes, inthe vacuoles between the collagen fibres, and in thelacunae in the arteriolar walls (Fig. 10). These crystalshad a melting point of between 41 and 430 C. Inaddition the globules of oil in the lumina of the arteriolesgave a " Maltese cross" effect on polarization (Fig. 11).On differential lipoid staining all the oil in this specimenstained rose-red with Sudan IV (Fig. 12), deep blue withNile blue sulphate, did not reduce osmic acid, and no"lipiodol" was detected in the tissue using the techniquedescribed by Felton (1953). These histological andhistochemical features were consistent with those of aliquid paraffin granuloma of the lung.
CASE 2.-C. C., a man aged 23, stated that in January,1952, he had 10 teeth extracted under general anaesthesia
162
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

GRANULOMATA OF LUNG DUE TO LIQUID PARAFFIN
FIG. 11.-The spherite cross in one ofthe oil globulesin Fig. 6. Some ofthecrvstals in the walls of vesselsare also demonstrated (polarized light, x 2,400).
and remained well despite the fact that a routine chestradiograph in February showed a lesion in the rightlung. Subsequently he noticed some exertional dys-pnoea which persisted till the onset of a severe pain inthe right chest and fever in November. With this hedeveloped a cough productive of thick white sputumand went to bed. After a few days he was given asulphonamide and remained at home for three weeks.When he retumed to work he felt tired and weak anddeveloped an extremely severe pleuritic pain in the rightchest anteriorly. This pain was worse on lying flatand on the right side, and because of it he was admittedon November 24 to the General Hospital underDr. Sluis-Cremer.Of note was a previous history ofmalaria and dysentery
and the fact that for some months in 1949 he had usednose drops and a throat spray for hay fever. He hadsmoked 50 cigarettes and had drunk three-quarters ofa bottle of brandy daily for the preceding 18 months.He had also come into contact with a brother who hadpulmonary tuberculosis.Examination revealed a well-developed patient with
breathlessness and grunting respiration. He was notcyanosed nor was there any fever, but his pulse was
108 per minute. The only other abnormal clinicalfindings were a few crepitations and impaired air entryin the right axilla.On the day of admission a chest radiograph showed
emphysema at the right apex with a dense area ofpneumonitis at the right mid-zone (Figs. 13 and 14).A tentative diagnosis of unresolved pneumonia was
made and he was given 250,000 units of penicillin every
six hours and symptomatic treatment. With this themid-zone lesion regressed radiologically. Sputa were
consistently negative both for tubercle and malignantcells. Bronchoscopy on January 6, 1953, revealed no
FIG. 12.-Sudan IV stain showing the oil-laden phagocytes, x 120.
abnormality and smears were taken from the rightupper lobe and were negative for acid-fast bacilli andmalignant cells.On January 14 screening by Dr. H. Jackson demon-
strated an obstructive emphysema of the right upperlobe. This was confirmed the following day by abronchogram which showed the apical segment of theright upper lobe to be markedly emphysematous. Theremaining segments were atelectatic and depressed.The rest of the bronchial tree was normal.On February 24 right thoracotomy was performed.
The apex of the right upper lobe was very distendedand emphysematous and could not readily be deflated.The anterior segment was atelectatic. The axillarysub-segments of the right upper lobe were denselyadherent to the chest wall. The underlying lung wasfirm and felt as though it contained a lung abscess. Aprominent feature, however, was the peribronchialthickening extending to the origin of the right upperlobe bronchus and this suggested the possibility of anoil granuloma. Hilar glands were not noticeablyenlarged. Right upper lobectomy was performed.Convalescence was uneventful with good re-expansionof the residual lobes.
Patholoaical Examination.-Macroscopically this rightupper lobe showed an intact pleura and a partial fissurebetween the posterior and apical segments. The pleuraofthe posterior segment showed a yellowish discoloration.The apical segment was markedly emphysematous.The upper lobe bronchus was patent, and the posteriorsegmental bronchus was occluded by firm yellow tissue.On section the lung showed a diffuse, firm, yellowtumour mass in the posterior segment, extending toboth the anterior and the apical segments.The histological features were essentially similar to
those described in the previous case, but were less
163
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

J. C. WAGNER, D. 1. ADLER, and D. N. FULLER
FJG. 13.-Radiograph of Case 2 on November 24, 1952, showing ashadow in the right lung field at the level of the right eighth ribposteriorly with gross emphysema of the right upper lobe.
Subsequent review of the sections showed that almostidentical elastic tissue degeneration was taking place inthe bronchi and bronchioles as was occurring in theblood vessels. This resulted in distorted irregularbronchi and bronchioles which had a bronchiectaticappearance and contained acute inflammatory exudates.In addition, along the course of the distended peri-bronchiolar lymphatics, which contained foamy alveolarphagocytes and free globules of oil, numerous aggre-gations of lymphocytes occurred around globules of oil.Sections from the peripheral region of this specimenshowed the histological features of chronic emphysema.In the hilar area and in the regions distal to the granu-loma, alveolar phagocytes containing iodized vegetableoil were seen and the ciliated columnar epithelial cellslining the bronchi and bronchioles were distended andcontained small globules of iodized vegetable oil.The tumour itself contained only mineral oil and
there was no evidence of iodized vegetable oil in thealveolar phagocytes within the tumour area, althoughbronchial epithelium and alveolar phagocytes lying freein the adjacent portions of the lobe contained iodizedvegetable oil.CASE 3.-C. R., a man aged 22, was admitted to the
Thoracic Surgical Unit on September 17, 1951, forinvestigation and treatment. In 1947 he had a ribresection for a left-sided " empyema" which drainedfor three months. Following that he experiencedfrequent attacks of fever and of malaise. These occurredalmost monthly at first, but gradually the intervalshad increased and he had attacks three or four times ayear. Before admission he had a slight constant achebelow the left nipple and through to the back. He hadnoticed dyspnoea when playing football, but at no timedid he suffer from any cough. A radiograph (Fig. 15)on admission showed a large spherical homogeneous
FIG. 14.-Lateral view of November 24 showing the lesion in thepostero-lateral segment of the right upper lobe.
marked. Other prominent features of this case werethe changes in the bronchioles and peribronchiolarregions.
This case was initially reported as a liquid paraffingranuloma in a lung in which there was a " follicularbronchiectasis."
FIG. 15.-Radiograph of Case 3 on September 17, 1951, showing a
spherical shadow at the left base extending up to the lowerborder of the sixth rib with a small fluid level.
164
IPI]P..,-.,.":,
i..'.
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

GRANULOMATA OF LUNG DUE TO LIQUID PARAFFIN
FIG. 16.-Specimen showing tumour situated in the middle of lungcysts.
opacity in the left posterior costophrenic sulcus butextending well up into the chest. At the summit ofthis level was a small fluid level. On September 19400 ml. of thick, green mucus was aspirated. A diag-nosis of a congenital sequestrated cyst was made.On September 26 a left thoracotomy was performed.
The cyst, inseparable from the left lower lobe, was onlyadherent to the site of the previous rib resection. Itwas inadvertently opened and 600 ml. of mucoid materialwas aspirated. A left lower lobectomy was performedwith division of an aberrant artery arising from theaorta just above the diaphragm. Convalescence was
marred by atelectasis of the left upper lobe and persistenteffusion necessitating decortication, after which heremained well and asymptomatic.
Pathological Examination.-In the left lower lobethere was a large multiloculated cyst surrounding a
diffuse golden-yellow tumour (Fig. 16). The micro-scopical features of this tumour were similar to thosedescribed in the first case with the oil showing thehistochemical features of liquid paraffin. Sections fromthe cyst showed it to be lined by a pseudo-stratifiedcolumnar respiratory epithelium. In the lumen bloodclot and amorphous eosinophilic material containingnumerous cholesterol crystals were demonstrated.CASE 4.-H. C. B., a male clerk aged 46, was referred
for opinion on October 8, 1953. He stated that hehad been well until September, 1951, when he developedfever, pain, and cough with some blood streakingdiagnosed as pleurisy. From that time he had been
M
FIG. 17.-Section from a liquid paraffin granuloma showing a pseudo-tubercular appearance, x 210.
prone to chest colds, and had two further attacks ofpleurisy, and had been subject to repeated small haemo-ptyses but was otherwise well. He had smoked 40 to50 cigarettes daily for about 20 years, and for manyyears had used oily nose drops nightly.
Clinical examination showed dullness, absent airentry, and resonance below the right clavicle. Radio-logical examination showed a dense opacity (Fig. 17) inthe antero-lateral segment of the right upper lobe withan extension to the upper pole of the right hilum. Atentative diagnosis of bronchogenic carcinoma was made.Bronchoscopy revealed no abnormality, but a dionosilbronchogram showed a block of the apical and antero-lateral segmental bronchi. Examination elsewhereshowed no malignant cells in the bronchial smears.
In view of the two-year history, the normal upperlobe bronchus on bronchoscopy, and negative smearsthe alternative diagnosis of an oil granuloma wassuggested. Right thoracotomy on October 15 showeddense adherent apical and antero-lateral segments withenlarged rubbery hilar and paratracheal glands. Theorigin of the right upper lobe bronchus was normal, butdistally there was complete obstruction from a hardmass. Frozen section on a paratracheal lymph glandwas reported upon as being consistent with the histologi-cal features of a lymph gland associated with oil granu-loma. Aright upper lobectomy was therefore performed.The lobe was immediately sectioned, fat could besqueezed out of its substance, and frozen sectionsconfirmed the diagnosis of an oil granuloma.
165
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

J. C. WAGNER, D. I. ADLER, and D. N. FULLER
Pathological Examination.-Macroscopic examinationshowed a large white necrotic hilar tumour, involvementof the lymph nodes, and obstruction of the antero-lateral and apical segmental bronchi. These segmentswere atelectatic, yellowish, and oily to the touch.
Histological examination showed a large-celled car-cinoma arising from the upper lobe bronchus. Beyondthis the obstructed segments showed the features of anoil granuloma similar to those described above. Para-ffin sections of the lymph node previously submittedfor frozen section showed infiltration with metastaticcarcinoma as well as the oil granuloma.
CASE 5.-Miss L. E. aged 57 was first seen in consulta-tion on February 21, 1954. She stated that she hadalways been well apart from a mild chronic sinusitis forwhich she had used a proprietary oily nasal medicament.In October, 1953, she developed a fever, myalgic pains,and a sore throat. From this she rapidly recovered, butthen developed a cough productive of a little muco-
purulent sputum which had persisted despite intensiveantibiotic therapy. Sputa were negative for tuberclebacilli and radiological investigation showed a well-circumscribed spherical opacity in the left upper lobe.With this history she was admitted to the Thoracic
Surgical Unit of the Florence Nightingale NursingHome. Bronchoscopy revealed no abnormality, butbronchial smears showed occasional cells with hyper-chromatic nuclei. No other site for a primary tumourcould be established. A tentative diagnosis of broncho-genic carcinoma was made.On March 3 a left thoracotomy was performed. A
small mobile mass was felt and a node removed. Thisnode, on frozen section, was reported upon as beinginfiltrated with carcinoma. Left upper lobectomy was,
however, performed and from this she recovereduneventfully.
Pathological Examination.-Macroscopic examinationof the lobe showed a well-circumscribed spherical whitishmass, 2 cm. in diameter, in the antero-lateral segmentof the left upper lobe. The appearances of this masswere compatible with a degenerating carcinoma (eitherprimary or secondary), a tuberculoma, or an oilgranuloma.
Histological examination of paraffin sections of this*mass and of the glands submitted for frozen sectionshowed the typical features of an oil granuloma.
THE BIOCHEMICAL IDENTIFICATION OF THE OILDERIVED FROM LUNG GRANULOMATA
Biochemical analysis was undertaken on speci-mens from the first three cases which were of theadult type of granuloma. As Graef (1939) hasshown, the total amount of fat recovered fromthese granulomata is slightly more than that whichis found in healthy lung tissue, i.e., IOV of the dryweight. Using the method described by Graef(1939) our results on the five cases presented inthis paper are:
Weight of Freeze-Case Wet dried Total %No. Specimen Residue Fat (g.)
(g.) (g.)
1 5-5 1-047 0 155 152 4-3 0-635 0-132 203 5-0 0-854 0-141 16-6
Using a minor modification of the methoddescribed by Donnelly and Hecht (1952), we were
able to extract a small amount of oily fluid fromthe granulomas. We are not satisfied that thesubstance extracted either by this method or bythe method described by Jampolis, McDonald, andClagett (1953) is liquid paraffin.
HISTOCHEMISTRY
The histochemistry of lipoids in the lung was
initially investigated by Pinkerton (1928). Follow-ing this it was accepted that liquid paraffin couldbe distinguished from animal and vegetable oils bybeing stained salmon pink with Sudan lV and darkblue with Nile blue sulphate and did not reduceosmic acid.
TABLE IREACTIONS OF " LIPOIDS " IN VITRO
Sudan IV Nile Blue Osmic Acid Fluorescence in PolarizedReagents (Sharlach R) Sulphate (Osmium Tetroxide) Ultra-violet Light Light
Cod liver oil Scarlet Purple Black (immediate) Golden No crystalsPeanut oil .iNilMilk fst ,, GoldenChaulmoogra oil Deep purple GoNilCastor oil Purple Black (in 30 min.) Silver-whiteOlive oil .. Black (immediate) NilPoppyseed oil ,, Nil Black beginning in
30 min., completein 4-12 hours
Liquid paraffin .. .. Red but paler , Nil ,.than above
White petroleum jelly .. ,, ,, Negatively birefringent needle-shaped crystals with meltingpoint about 400 C.
Yellow petroleum jelly .. ,, Golden , . ..
166
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

GRANULOMATA OF LUNG DUE TO LIQUID PARAFFIN
In in vitro experiments one of us (J. C. W.) obtainedthe results shown in Table I.At first we accepted the above criteria, but on
reviewing the literature on lipoid histochemistry(Pearse, 1953; Gomori, 1952; Cain, 1950; Thann-hauser, 1950) it became apparent that these criteriawere not acceptable, as the same reactions couldbe obtained with cholesterol, the other steroids,the phosphatides, and the cerebrosides. Anotherassumption which was found to be incorrect wasthat all negatively birefringent crystals were chol-esterol. The crystals in this series of oil granulo-mata are negatively birefringent and have a meltingpoint of 4143o C. A false clue to their origin wasthe discovery that in petroleum jelly there areneedle-shaped birefringent crystals with a meltingpoint of approximately 400 C., but these crystalsgive a negative reaction to Schultz's modification ofthe Liebermann-Burchardt reaction (Gomori, 1952),whereas the crystals in the oil granulomata gave apositive reaction. Cholesterol and its esters havea melting point of above 1400 C. Cain (1950) statesthat as far as is known the Liebermann-Burchardtreaction is a specific test for cholesterol in animaltissues.To confirm the origin of the crystals a study was
made of the reaction of crystals in sections from thegall bladder in a case of hypercholesterolosis. Inthese sections two forms of negatively birefringentcrystals were observed, viz., the true cholesterolcrystals and small, needle-shaped crystals similarto those seen in the lung granulomas. Both theseforms of crystals gave a positive Schultz reaction.The needle-shaped crystals melted at approximately420 C. and the large crystals showed no evidence ofdisintegration at a far higher temperature. AsCain (1950) states, " A particularly importantcharacteristic of lipoids is their ability to dissolvein each other, sometimes to a considerable extent."In view of this it seemed probable that in the gallbladder we were dealing with a combination ofcholesterol and a neutral fat.As a result of this, the possibility of the lipoid
in the granulomata consisting of a combination ofliquid paraffin, cholesterol, and a "neutral fat"or " neutral fats " was considered. To demonstratethis a modification of Keilig's extraction method(Pearse, 1953) was used. It was found that liquidparaffin is insoluble in cold acetone but soluble incold ether and cold chloroform.
Frozen sections were cut at 15 i and agitatedin cold acetone for five minutes. Then as a controlsome of these sections were removed from theacetone, stained with Sudan IV and Sudan black" B'" and unstained sections were mounted for
examination with a polarizing microscope. Addi-tional sections were prepared for the Schultzreaction. It was found that on Sudan staining theSudanophilic material was present in exactly thesame distribution as in the untreated sections butthe Schultz reaction was now negative, the crystalshad disappeared but the spherite crosses persisted.The remaining sections were then washed in dis-tilled water and placed in cold ether for 10 minutes.These sections were then stained with Sudan IVand Sudan black "B " and examined under apolarizing microscope. Small deposits of Sudano-philic material were observed in alveolar phagocytesand in the interstitial tissue and the spherite crosseswere still present.From Keilig's conclusions (Pearse, 1953) it was
assumed that the remaining small foci of lipoidwere either cerebrosides, phospholipids, or sphingo-myelins. In the one specimen of this series thatwas not in formalin Baker's acid haematin test(Baker, 1946) was negative for phospholipids.These crystals were present in unfixed sections ofthis specimen, suggesting that they are not the resultof formalin fixation.The obvious control of this experiment would
be to extract the liquid paraffin from the ether andidentify it chemically. This is being done, but weare informed by organic chemists that it will beextremely difficult because of the inert chemicalnature of the substance and the fact that it consistsof a series of hydrocarbons. The exact nature ofthe crystals is being investigated. The fact thatthey have been observed in several other types ofgranuloma, which have definite and proved aetiolo-gies, suggests that they may play an important rolein initiating the fibrous tissue reactions which is asequel to many of the " foreign body " lesions.
CLINICAL DIAGNOSIS OF MINERAL OIL GRANULOMAAs this is a relatively uncommon condition a
pre-operative diagnosis will probably seldom bemade, particularly as the clinical and radio'ogicalfeatures are so suggestive of a diagnosis of car-cinoma, tuberculosis, or lung abscess. Most ofthe cases described have occurred in the posteriorsegments of the upper lobes and in the apices of thelower lobes, but these sites are also commonlyinvolved in both tuberculosis and lung abscess.At operation the condition can be suspected by firmperibronchial cords radiating to the hilum, whichis singularly free of enlarged glands.Although the diagnosis can be made with cer-
tainty on histological examination, the findingsbear no relation to the duration of any known orsuspected aetiological factor. In Case 1, although
167
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

J. C. WAGNER, D. L ADLER, and D. N. FULLER
the lesion showed marked fibrosis with areas ofnecrosis the history of symptoms was only nineweeks and during that time the patient used nosedrops on rare occasions. It should be noted thatStorrs, McDonald, and Good (1949) found anestablished granuloma 19 days after bronchography.In Case 2, despite nasal drops and a nasal atomizerhaving been used some years previously, exam-ination of this tumour showed less fibrosis andendarteritis than did the first case. In Case 3there is no previous history of the use of " lipiodol "or nasal oil drops, and no communication could bedetected between the sequestrated cyst and thebronchus. Possibly, at the time that the " em-pyema" was drained in 1947 some petroleum oilproduct was used in the wound packs. BothCases 4 and 5 had used oily nose drops regularlyfor years.A history of instillation of oily nose drops would
add weight to a tentative diagnosis of mineral oilgranuloma. Examination of sputa from patientswith suspected oil granulomata of the lung has notbeen helpful. Because of the fibrous nature of thelesions the possibility of liquid paraffin appearingin the sputum is remote. The mere finding of cellscontaining " lipiodol" in the sputum does notindicate an oil granuloma, as these cells can beseen in the sputum for varying periods in patientswho have had a " lipiodol " bronchogram, and donot harbour a granuloma. In two of our patientswho had bronchograms done pre-operatively,although the alveolar phagocytes in the adjacentportion of the lung contained " lipiodol," nonewas found in the granuloma.
THE PATHOGENESIS OF OIL GRANULOMATA IN THELUNGS
On the histopathological and histochemicalevidence from the examination of these cases ofoil granulomata and of cases of lipoid pneumoniain infants, and from a review of literature, thefollowing hypothesis as to the pathogenesis of oilgranuloma in the lungs is suggested. This can bedivided into four consecutive stages (Fig. 18), butany or all of these processes may be present in asingle lesion.
STAGE I.-This stage can be seen in infants whodie of asphyxia following massive inhalation ofmilk. There is altered milk in the bronchi, bron-chioles, and alveoli surrounded by scanty neutro-phils, lymphocytes, and occasional giant cells.STAGE II.-This is the stage of absorption and
foreign body reaction. Numerous alveolar phago-cytes appear in the alveoli and begin absorbing the
fat globules and the oil in the perivascular andperibronchiolar lymphatics (Figs. 4 and 12). Oncethe oil is taken up by the alveolar phagocytes, theneedle-shaped crystals are observed in these cells(Fig. 10). As this stage of foreign-body reactioncontinues, most of the oil is absorbed by thealveolar phagocytes, which now have a distendedfoamy cytoplasm. These, together with numerouslymphocytes, plasma cells, and occasional multi-nucleate giant cells, are present in the alveoli.The alveolar walls now appear thickened and thealveolar epithelium cuboidal. Some of these cellscontain oil and needle-shaped crystals. In thealveolar walls there is an increase of reticulum withnoticeable collagen fibres and occasional fibro-blasts. The lymphatic tissue has become hyper-plastic and lymph nodules with germinal centresare seen. Along the course of the lymphaticsthere are aggregations of lymphocytes aroundglobules of oil and in some of these areas theaggregations are so compact that they resemblelymph nodules. In occasional arterioles andvenules globules of oil can be identified. The lasttwo observations were first made by Pinkerton andMoragues (1940). These globules have a spheritecross (Maltese cross) appearance in polarization(Fig. 11). In addition there is increased perivas-cular fibrous tissue and the internal and externalelastic laminae of the arterioles are grossly contortedand their endothelial cells appear to be swollen.In the bronchi and bronchioles the epithelial cellsswell and fibrous tissue and reticulum fibres in themuscularis increase. The elastic tissue is presentand intact. The alveoli contain lymphocytes,plasma cells, occasional oil-containing alveolarphagocytes, and multinucleate giant cells.STAGE 11.-This is the stage of elastic tissue
degeneration and endarteritis. The alveoli aredistorted and many of them have collapsed. Thelymphocytes and plasma cells have disappearedfrom the alveolar spaces, which now only containcompressed oil-containing phagocytes, occasionalmultinuclear giant cells, and desquamated alveolarepithelial cells. In the alveolar walls there is amarked increase in reticulum and the capillariesare completely replaced by collagen fibres andfibroblasts. In the areas where the alveoli are nolonger discernible, the normal lung structure isobliterated by a loose weave of collagen fibres andfibroblasts, enmeshed in which are oil-containingphagocytes, globules of oil, multinucleate giantcells, and clumps of lymphocytes, plasma cells,and eosinophils. In addition there are occasionalfoci of multinucleated giant cells surrounded by
168
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

GRANULOMATA OF LUNG DUE TO LIQUID PARAFFIN
m;.
EFIG. 18.-This diagram illustrates the four stages in the pathogenesis of these lesions.
palisading epithelioid cells. The appearance ofthese foci is similar to those of proliferating tuber-culosis. The changes in the arterioles are mostsignificant and striking. The fibrosis of the adven-titia has greatly increased and the muscle in themedia has been entirely replaced by fibrous tissue.In all three layers of the walls numerous smallvacuoles are seen. On frozen section these vacuolesare seen to contain oil (Fig. 8) and the needle-shaped negatively birefringent crystals. Whereverthe elastic fibres and elastic laminae come intocontact with these vacuoles, there is disruption ofthe elastic tissues giving the elastic fibres a markedlyfragmented appearance (Fig. 9). The lumina ofthe blood vessels are greatly reduced (Fig. 7). Inthe walls of the bronchi and bronchioles a similarappearance to that of the arterioles is seen with asimilar vacuolation, disruption of elastic fibres,
and fibrous replacement of the muscularis. Thelumina of the bronchi and bronchioles are dilatedand irregular in outline, giving a bronchiectaticappearance. Surrounding the peribronchial lym-phatics lymphoid tissue is markedly hyperplastic,and the aggregations of lymphocytes around theoil globules now appear as mature lymph nodules.These histological features are strikingly similar tothose described by Whitwell (1952) as " follicularbronchiectasis."STAGE IV.-This is the stage of increasing fibrosis.
In it there is an increasing fibrosis with a progressiveendarteritis. The elastic tissue in the arterioles,bronchi, and bronchioles is gradually replaced bya reticulum network (Fig. 6), and the previouslydilated bronchi and bronchioles become collapsedand stenosed by the ever-increasing interstitialfibrosis. The final picture is one of completely
I
II
169
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from

J. C. WAGNER, D. L ADLER, and D. N. FULLER
occluded arterioles and flattened degeneratingbronchi and bronchioles, surrounded by densefibrous tissue in which there are areas of hyalinedegeneration and necrosis. Between the collagenfibres occasional compressed globules of oil areseen (Fig. 5). In any one of these stages secondaryinfection may distort the histological features.
CONCLUSIONS
Oil granulomata of the lung are not rare andshould be considered in the differential diagnosis ofall chronic lung lesions where the more commondiseases such as tuberculosis and carcinoma havebeen excluded. Such cases are preventable, and thewidespread chronic use of oily nasal drops andvapours should not be allowed. Persons occupiedin industry involving the use of oil sprays shouldbe adequately protected.
In four of our five cases the granuloma wassituated in the upper lobes, a site in keeping withan inhalation mechanism.The clinical symptomatology and pathological
lesions following inhalation are variable. Two ofour cases presented as a mass indistinguishablefrom bronchogenic carcinoma, one was associatedwith a carcinoma, one presented with atelectasisand obstructive emphysema of an upper lobe, andthe fifth was associated with a previously drainedempyema.
SUMMARY
Five cases of mineral oil granuloma of the lungare presented and the literature is reviewed.
It is suggested that the pathogenesis of mineraloil granulomata of the lung is due to the sclerosingeffect of an endogenous fatty acid to lipoid.The difficulties of pre-operative diagnosis are
discussed
The dangers of using oils internally as a vehiclefor medicaments or radio-opaque substances isstressed.We would like to thank Professor Guy Elliott, Dr.
Sluis Cremer, Dr. Medalie, and Dr. Frack for referringthese cases. Case No. 4 was referred by the late Dr. J.Baynash. We should also like to thank Dr. F. A. Brandtfor the photography, Mr. D. Treumich for preparingthe sections, Mr. H. D. Barnes for the biochemistry,Mr. J. de Bruyn for the diagrams, and Dr. C. Komins,of the Radiological Department of the JohannesburgGeneral Hospital, for the x-ray plates of the specimens.
BIBLIOGRAPHYBaker, J. R. (1946). Quart. J. micr. Sci., 87, 441.Brody, H. (1943). Arch. Path., Chicago, 35, 744.Cain, A. J. (1950). Biol. Rev., 25, 73.Corper, H. J., and Freed, H. (1922). J. Amer. med. Ass., 79, 1739.Daniel, J. W., Frazer, A. C., French, J. M., and Sammons, H. G.
(1953). Biochem. J., 54, xxxvii.Donnelly, L. C., and Hecht, B. P. (1952). Amer. J. clin. Path., 22,449.Fienberg, J. (1953). Ibid., 23, 413.Felton, W. L. (1952). Lab. Invest., 1, 364.-(1953). J. thorac. Surg., 25, 530.Fortner, A. C., and Miles, J. S. (1950). Arch. Path., Chicago, 49,447.Gomori, G. (1952). Microscopic Histochemistry, University of
Chicago Press.Graef, I. (1935). Amer. J. Path., 11, 862.- (1939). Arch. Path., Chicago, 28, 613.Guieysse-Pellissier, A. (1920). C.R. Soc. Biol., Paris, 83, 809.Hastings, E. V. (1950). Arch. Path., Chicago, 49, 453.Ikeda, K. (1937). Ibid., 23, 470.Jacob, O., and Faur6-Fremiet (1917). Rev. Chir., Paris, 54, 221.Jampolis, R. W., McDonald, J. R., and Clagett, 0. T. (1953). Ant.
Abstr., 97, 105.Laughlen, G. F. (1925). Amer. J. Path., 1, 407.Lukens, R. M. (1922). J. Amer. med. Ass., 78, 274.Moran, T. J. (1953). Arch. Path., Chicago, 55, 286.Pearse, A. G. E. (1953). Histochemistry-Theoretical and Applied.
Churchill, London.Pinkerton, H. (1927). Amer. J. Dis. Child., 33, 259.-(1928). Arch. Path., Chicago, 5, 380.-and Moragues, V. (1940). Ibid., 29, 691.Rosenberg, A. (1885). Berl. klin. Wschr., 22, 449.Rubin, I. C. (1939). Radiology, 33, 350.Sabin, F. R., Doan, C. A., and Forkner, C. E. (1930). J. exp. Med.,
52, Suppl. 3.Sicard, J. A., and Forestier, J. (1922). Bull. Soc. med. H6p. Paris,
46, 463.Storrs, R. P., McDonald, J. R., and Good, C. Allen (1949). J.
thorac. Surg., 18, 561.Stryker, W. A. (1941). Arch. Path., Chicago, 31, 670.Waters, C. A., Bayne-Jones, S., and Rowntree, L. G. (1917). Arch.
intern. Med., 19, 538.Whitwell, F. (1952). Thorax, 7, 213.Young, A. M., Applebaum, H. S., and Wasserman, P. B. (1939).
J. Amer. med. Ass., 112, 2406.
170
on April 26, 2021 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.10.2.157 on 1 June 1955. D
ownloaded from