Embed Size (px)
Citation preview

POSTGRAD. MED. J. (I961), 37, 276
ALIMENTARY GRANULOMATA ANDTHE IMMUNE RESPONSE
G. SLANEY, M.S., M.B., Ch.B., F.R.C.S.Department of Surgery, Queen Elizabeth Hospital, Birmingham
THE possible i:tiological relationship between thealimentary granulomata and the immune responseis one of the more recent and exciting develop-ments in the sphere of gastroenterology.
General aspectsAlthough the basic features of the antigen-
antibody type of response have been well recog-nized for many years, these processes werehitherto considered to be essentially protective innature and concerned with ensuring survivalunder adverse conditions. Recently, however,there has 'been increasing evidence that undercertain circumstances antigen-antibody reactionsmay play an important etiologlcal role in diseaseswhose pathogenesis was previously obscure andshrouded in medical mystery. Of especial interestare the auto-immune disorders in which an in-dividual tissue becomes antigenic, thus stimulatingthe production of a circulating antibody, thesubsequent reaction resulting in destruction oratrophy of the parent tissue concerned. There isgood evidence that the collagen diseases arise asthe result of such an immune type of response andit has been shown, using fluorescent stainingtechniques, that the tissue lesions in these diseasesare the site of an antigen-antibody reaction(Vazquez and Dixon, 1957). Antibodies tothyroid tissue have been demonstrated in the seraof patients with Hashimoto's disease and chronicthyroiditis (Witebsky, Rose, Terplan, Paine andEgan, 1957; Witebsky, Rose and Shulman, I958).Auto-antibodies have also been demonstrated inthe sera of patients with viral hepatitis, primarybiliary cirrhosis, glomerulo-nephritis and thenephrotic syndrome (Mackay, I958; Gajdusek,I958; Lui and McCrory, 1958).A notable feature is the frequency with which
certain immunological reactions are associatedwith a granulomatous type of response. Thereis now strong experimental and clinical evidenceto indicate that polyarteritis nodosa is caused by animmune-hypersensitivity mechanism. Germuth(I953) showed that giving a large dose of bovineserum intravenously in rabbits produced wide-
spread cardiovascular and renal lesions resemblingthose of rheumatic fever, polyarteritis nodosa andacute glomerulo-nephritis respectively in man;furthermore many of these animals developedwidespread granulomatous lesions. Fulminatingperi-arteritis nodosa with a fatal outcome has beenrecorded following the administration of antiserumand sulphonamides to patients (Rich, 1942); it hasalso occurred in patients with hypersensitivity todrugs such as iodine and arsenic. As in poly-arteritis nodosa it is possible that immunologicalfactors are also involved in sarcoidosis for Refvem(I954) has shown that in animals sensitized tophospholipid an immune response of the Arthustype occurs with the formation of granulomatacontaining giant cells and Schaumann inclusionbodies, the classical histological features of humansarcoidosis. Wegener's granulomatosis is a rarefatal disease characterized by necrotizing granulo-matous lesions in the respiratory tract, generalizedvasculitis and a necrotizing glomerulitis (Wegener,I939); the vascular lesions are identical with thoseof polyarteritis nodosa. Most are agreed that thisdisease is a hypersensitivity state; the initial lesiondevelops in the nose or paranasal sinuses and islater followed by a generalized hypersensitivityreaction and death from respiratory or renal failure.
Alimentary Involvement in Systemic DiseaseThe alimentary tract may be involved in many
of these systemic diseases which arise on an im-munological basis; such involvement, however, isusually secondary though granulomatous ulcera-tion, hkmorrhage and perforation frequentlyresult.
In Wegener's granulomatosis extensive granulo-matous ulceration showing giant cells, fibrosis andcentral necrosis occurs in the mouth, cesophagusand small intestine and multiple granulomata arefrequently present in the liver and spleen (Codmanand Churg, 1954; Walton, I958; Felson andBraunstein, 1958).
Forty per cent. of patients with systemic lupuserythematosis have widespread ulceration in thecesophagus, small bowel and colon due to col-
copyright. on 2 F
ebruary 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.276 on 1 M
ay 1961. Dow
nloaded from

May I96I SLANEY: Alimentary Granulomata and the Immune Response
lagenous degeneration and thrombosis in smallvessels (Dubois, I953). The cesophagus is com-monly involved in scleroderma with resultingcrsophagitis and ulceration due to incompetence ofthe cardia; involvement of the small bowelproduces secondary sacculation and dilatation,and steatorrhcea may be gross (Abrams, Carnesand Eaton, 1954; Hale and Schatzki, I944;Rosenthal, I957). Rarely, colonic changes may beextremely severe resembling fulminating ulcera-tive colitis and frank gangrene has been reported(Lushbaugh, Rubin and Rothman, 1948).
Patients with dermatomyositis have a high in-cidence of stomatitis, glossitis and gastro-intestinalulceration; hwmorrhage and perforation arefrequent (Wainger and Lever,; 1949; Domzalskiand Morgan, I955). There is also a high incidenceof malignant disease, including gastro-intestinalcancer, in this condition; the relationship is soconstant that a continuing search for malignancy isindicated in every patient with dermatomyositis(Curtis, Blaylock and Harrell, 1952; Dowling,'955).
Intestinal involvement occurs in over half thecases of polyarteritis nodosa and symptoms areusually due to ulceration, infarction, perforation orhamorrhage. If ulceration is widespread severesteatorrhcea and malabsorption syndromes result;the mucosa usually shows typical granulomatousulceration with some giant-cell systems (Pugh andStringer, I956; Weinberg, 1946; Mowrey andLundberg, 1954).The alimentary tract is but rarely involved in
generalized sarcoidosis, the commonest site beingthe stomach; the lesion is frequently mistaken fora carcinoma of the linitis plastica type (Orie, VanRijssell and Vanderzwag, 1950; Appell, Pritzkerand Klotz, I95I). Histologically some cases ofCrohn's disease may resemble sarcoidosis butthere is no relationship between the two diseases(McKusick, I953; Phear, 1958).
Experimental AspectsIn the laboratory, typical granulomatous lesions-
can occur as part of an immune response. Ifguinea-pigs or rabbits be sensitized to foreignprotein, subsequent subcutaneous injection of theantigen several days later produces a characteristicgranulomatous response (Figs. i and 2). Histo-logically the lesions show histiocytosis, monocytes,endothelial cells and a giant cell and eosinophilicresponse at the injection site (Goddard, 1947;Goldgraber and Kirsner, I958). Endothelial andperithelial reactions are marked and the cellularreaction around small blood vessels may be i*ntense(Fig. 3). Granulomata produced by these meanscan also be shown to be the site of antibody for-mation (White, Coons and Connolly, I955). This
FIG. I
V-~
41
FIG.2
Sifi
FI G2
FIG. 3
copyright. on 2 F
ebruary 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.276 on 1 M
ay 1961. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
was confirmed by the more precise studies ofAskonas and Humphrey (1955) who studied thegranulomata produced by Freund's adjuvant inrabbits using 14C labelled glycine and showed thatthe cell mass of the granuloma produces some8oO0, of the antibody. There is now very goodevidence that plasma cells are one of the mainsources of antibody (Gell, I959). Fagraeus (I948)has shown that many reticulo-endothelial cellsdevelop into plasma cells and in the course of thisprocess antibodies are formed; the main producersof antibody are immature plasma cells for matureplasma cells apparently lose the power of antibodysynthesis (Oakley, I959).
In clinical practice there is also strong evidenceindicating that certain granulomata arise as a resultof an immune type of response. Shelley andHurley (I957) demonstrated, both experimentallyand clinically, that man can develop granulo-matous lesions as a result of generalized hyper-sensitivity to sodium zirconium lactate. More,McMillan and Duff (1946) reported widespreadgranulomatous lesions in the heart, liver andkidneys in patients sensitive to sulphonamide.Churg and Strauss (I95i) reported I3 cases ofsevere asthma followed by fever and intenseeosinophilia; ii patients subsequently died andwidespread granulomatous lesions were presentthroughout the body with radially arrangedmacrophages and giant cells; arterial lesionsessentially similar to those seen in polyarteritisnodosa were also present.
It will thus be seen that there is strong clinicaland experimental evidence indicating the closecorrelation between the granulomatous responseand immune hypersensitive states generally.
The Immune Response in the AlimentaryTract
Injection or ingestion of proteins into thestomach of previously sensitized animals producescongestion and cedema followed by induration andnecrosis; similar changes occur in sensitized dogs(Shapiro and Ivy, I926; Thiers and Chevallier,I935). Jahiel and his associates (1952) inducedlocal sensitivity by injecting horse serum into thewall of the stomach and after an interval horseserum was given intravenously; 520/0 of theexperimental animals developed gastric lesionsconsisting of localized areas of mucosal and sub-inucosal crdema with lymphocytes, plasma cellsand a few eosinophils. In a number of animalsactively bleeding lesions with crater formationsurrounded by cedema were produced. TheShwartzman phenomenon can occur in thestomach wall under experimental conditions butdoes not usually produce ulceration (Karsner,Ecker and Jackson, 193 ). If any part of the
alimentary tract of monkeys be passively sensitizeda brisk local reaction occurs when the antigen isgiven either by mouth or intravenously (Walzer,Gray, Straus and Livingston, I938).
In human beings it is common for severeanaphylactic reactions to be accompanied bynausea, vomiting and abdominal pain. In patientswith known gastro-intestinal allergy, ingestion ofthe causative antigen causes an initial hyperaemiaof the alimentary mucous membrane followed bywidespread cedema and a greatly increased pro-duction of mucus; local haemorrhage may occur(Pollard and Stuart, I941). Similar lesions maybe observed on exposed mucous membrane inpatients with an ileostomy or a colostomy if localpassive sensitivity be induced by intramucosalinjection of serum from an allergic individual (Gray,Harten and Walzer, I940). Oral administrationof the antigen is shortly followed by initial pallorin the sensitized area and subsequent hyperxemia,progressive cedema and profuse secretion of mucus.Thus it is clear that the human alimentary tract isquite capable of participating in or being involvedby immune-hypersensitivity reactions.
Goldbraber and Kirsner (1959) have reported anArthus type reaction in the colon of rabbitssensitized to egg albumin. At a subsequentoperation egg albumin was injected subserosallyinto the colon and granulomata and giant cells wererepeatedly observed six and seven days after theeliciting injection; eosinophils were prominent.
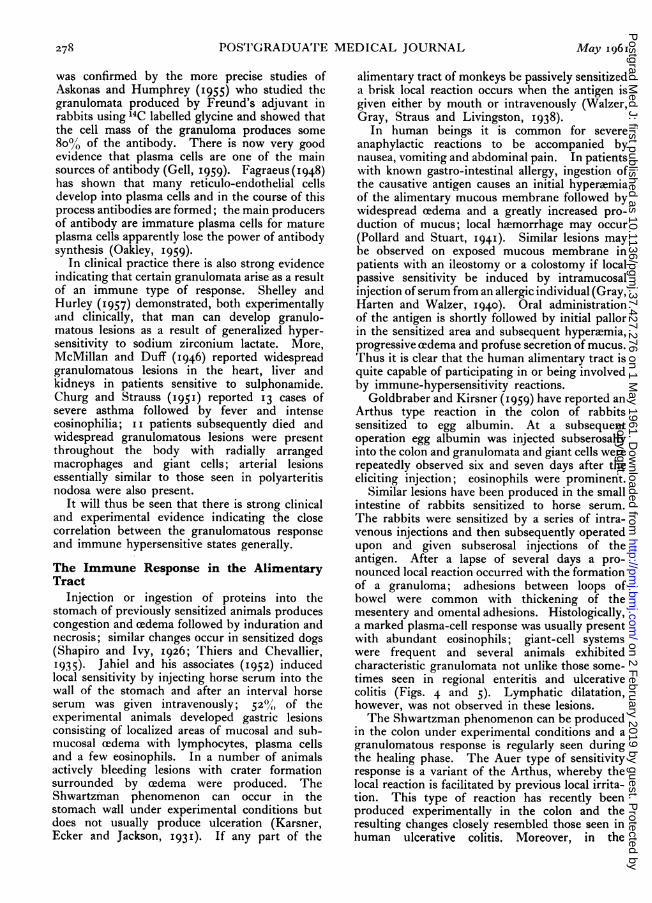
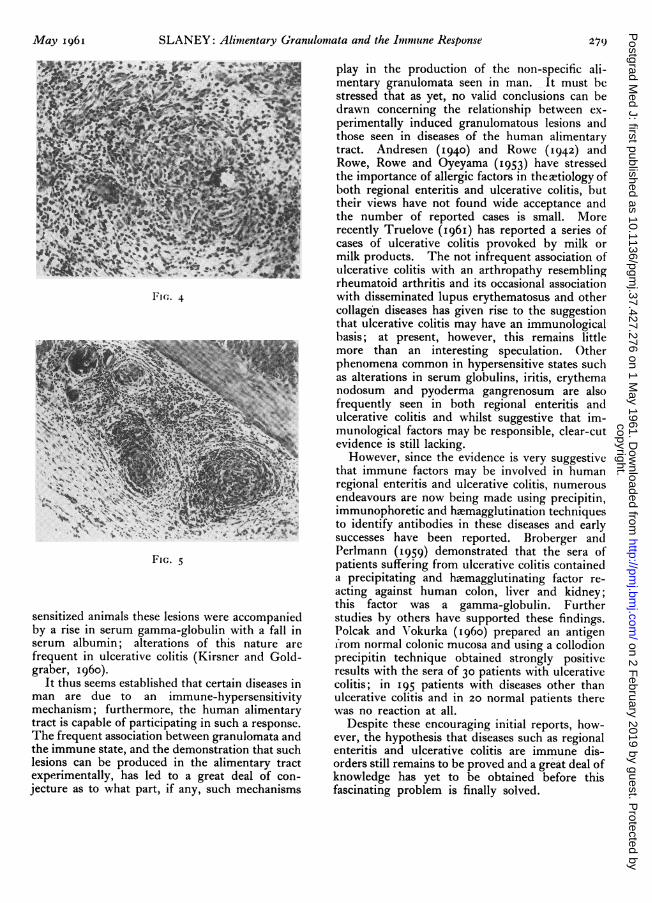
Similar lesions have been produced in the smallintestine of rabbits sensitized to horse serum.The rabbits were sensitized by a series of intra-venous injections and then subsequently operatedupon and given subserosal injections of theantigen. After a lapse of several days a pro-nounced local reaction occurred with the formationof a granuloma; adhesions between loops ofbowel were common with thickening of themesentery and omental adhesions. Histologically,a marked plasma-cell response was usually presentwith abundant eosinophils; giant-cell systemswere frequent and several animals exhibitedcharacteristic granulomata not unlike those some-times seen in regional enteritis and ulcerativecolitis (Figs. 4 and 5). Lymphatic dilatation,however, was not observed in these lesions.The Shwartzman phenomenon can be produced
in the colon under experimental conditions and agranulomatous response is regularly seen duringthe healing phase. The Auer type of sensitivityresponse is a variant of the Arthus, whereby thelocal reaction is facilitated by previous local irrita-tion. This type of reaction has recently beenproduced experimentally in the colon and theresulting changes closely resembled those seen inhuman ulcerative colitis. Moreover, in the
278 May I96Icopyright.
on 2 February 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.427.276 on 1 May 1961. D
ownloaded from
May I96I SLANEY: Alimentary Granulomata and the Immune Response
A.
'.q 44'.J.** .::v **,4'
I"lc,. 4
:,c. N9
'4
fl.'
FIG. 5
sensitized animals these lesions were accompaniedby a rise in serum gamma-globulin with a fall inserum albumin; alterations of this nature arefrequent in ulcerative colitis (Kirsner and Gold-graber, I 960).
It thus seems established that certain diseases inman are due to an immune-hypersensitivitymechanism; furthermore, the human alimentarytract is capable of participating in such a response.The frequent association between granulomata andthe immune state, and the demonstration that suchlesions can be produced in the alimentary tractexperimentally, has led to a great deal of con-jecture as to what part, if any, such mechanisms
play in the production of the non-specific ali-mentary granulomata seen in man. It must bestressed that as yet, no valid conclusions can bedrawn concerning the relationship between ex-perimentally induced granulomatous lesions andthose seen in diseases of the human alimentarytract. Andresen (1940) and Rowe (1942) andRowe, Rowe and Oyeyama (I953) have stressedthe importance of allergic factors in the etiology ofboth regional enteritis and ulcerative colitis, buttheir views have not found wide acceptance andthe number of reported cases is small. Morerecently Truelove (I96I) has reported a series ofcases of ulcerative colitis provoked by milk ormilk products. The not infrequent association ofulcerative colitis with an arthropathy resemblingrheumatoid arthritis and its occasional associationwith disseminated lupus erythematosus and othercollagen diseases has given rise to the suggestionthat ulcerative colitis may have an immunologicalbasis; at present, however, this remains littlemore than an interesting speculation. Otherphenomena common in hypersensitive states suchas alterations in serum globulins, iritis, erythemanodosum and pyoderma gangrenosum are alsofrequently seen in both regional enteritis andulcerative colitis and whilst suggestive that im-munological factors may be responsible, clear-cutevidence is still lacking.
However, since the evidence is very suggestivethat immune factors may be involved in humanregional enteritis and ulcerative colitis, numerousendeavours are now being made using precipitin,immunophoretic and haemagglutination techniquesto identify antibodies in these diseases and earlysuccesses have been reported. Broberger andPerlmann (i95) demonstrated that the sera ofpatients suffering from ulcerative colitis containeda precipitating and haemagglutinating factor re-acting against human colon, liver and kidney;this factor was a gamma-globulin. Furtherstudies by others have supported these findings.Polcak and Vlokurka (I960) prepared an antigenfrom normal colonic mucosa and using a collodionprecipitin technique obtained strongly positiveresults with the sera of 30 patients with ulcerativecolitis; in I95 patients with diseases other thanulcerative colitis and in 20 normal patients therewas no reaction at all.
Despite these encouraging initial reports, how-ever, the hypothesis that diseases such as regionalenteritis and ulcerative colitis are immune dis-orders still remains to be proved and a great deal ofknowledge has yet to be obtained before thisfascinating problem is finally solved.
copyright. on 2 F
ebruary 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.276 on 1 M
ay 1961. Dow
nloaded from

28o POSTGRADUATE MEDICAL JOURNAL May I96I
REFERENCESABRAMS, H. L., CARNES, W. H., and EATON, J. (I954): Alimentary Tract in Disseminated Scleroderma with Emphasis
on Small Bowel, Arch. intern. Med., 94, 6 i.ANDRESEN, A. F. R. (I940): The Surgeon and Colonic Allergy, Amer. J7. Surg., 50, 28I.APPELL, A. A., PRITZKER, H. G., and KLOTZ, P. G. (I95): Pyloric Obstruction due to Sarcoid of the Stomach, A.M.A.
Arch. Surg., 62, I40.ASKONAS, B. A.. and HUMPHREY, J. H. (1955): Antibody Formation in Slices of Granulomata Produced by Adjuvant,
Biochem. Y. (Lond.), 60, io.BROBERGER, O., and PERLMANN, P. (I959): Auto-antibodies in Human Ulcerative Colitis, J. exp. Med., 110, 657.CHURG, J., and STRAUSS, L. (I95I): Allergic Granulomatosis, Allergic Arteritis and Peri-arteritis Nodosa, Amer.J. Path.
27, 277.CODMAN, G. C., and CHURG, J. (1954): Wegener's Granulomatosis, Arch. Path., 58, 533.CURTIS, A. C., BLAYLOCK, H. C., and HARRELL, E. R. (1952): Malignant Lesions Associated with Dermatomyositis,
J. Amer. med. Ass., iso, 844.DOMZALSKI, C. A., and MORGAN, V. C. (1955): Dermatomyositis, Amer. Y'. Med., 19, 370.DOWLING, G. B. (I955): Scleroderma and Dermatomyositis, Brit. 57. Derm., 67, 275.DUBOIS, E. L. (I953): Effect of the L.E. Cell Test on the Clinical Picture of Systemic Lupus Erythematosus, Ann. intern.
Med., 38, I265.FAGRAEUS, A. (I948): Antibody Production in Relation to the Development of Plasma Cells, Acta med. scand. Suppl., 204.FELSON, B., and BRAUNSTEIN, H. (1958): Non-infectious Necrotising Granulomatosis, Radilogy, 70, 326.GAJDUSEK, D. C. (1958): An Auto-immune Reaction against Human Tissue Antigens in Certain Acute and Chronic
Diseases. I. Serological Investigations, Arch. intern. Med., IOl, 9.GELL, P. G. H. (1959): Cytologic Events in Hypersensitivity Reactions, in Cellular and Humoral Aspects of the Hyper-
sensitive States. New York: Hoeber-Harper.GERMUTH, F. G. (1953): A Comparative Histologic and Immunologic Study in Rabbits of Induced Hypersensitivity of
the Serum Sickness Type, J'. exp. Med., 97, 257.GODDARD, J. W. (I947): Granuloma. Characteristic Qualitative Change in Focal Anaphylactic Inflammatio,iU Amer. 5'.
Path., 23, 943.GOLDGRABER, M., KIRSNER, J. B. (1958): Granulomatous Lesions-an Expression of the Hypersensitive State, Arch.
Path., 66, 6i8.I--- (1959): The Arthus Phenomenon in the Colon of Rabbits, Arch. Path., 67, 556.
GRAY, I., HARTEN, M., and WALZER, M. (1940): Studies in Mucous Membrane Hypersensitiveness. IV. The AllergicReaction in the Passively Sensitized Mucous Membranes of the Ileum and Colon in Humaz.s, Ann. intern. Med.,13, 2050.
HALE, C. H., SCHATZKI, R. (I944): The Roentgenological Appearance of the"Gastrointestinal Tract in Scleroderma,Amer. 5'. Roentgenol., 51, 407.
JAHIEL, R., JAHIEL, R., and KRAKAUER, J. (1952): Local Hypersensitiveness of the Rabbit Stomach, Proc. Soc. exp. Biol.(N. Y.), 79, 54.
KARSNER, H. T., ECKER, E. E., and JACKSON, E. L. (I93 I): Shwartzman Phenomenon in the Rabbit Stomach, Proc. Soc.exp. Biol. (N.Y.), 29, 319.
KIRSNER, J. B., and GOLDGRABER, M. B. (I960): Hypersensitivity, Auto-immunity and the Digestive Tract, Gastro-enterology, 38, 536.
LUI, C. T., and MCCRORY, W. W. (1958): Auto-antibodies in Human Glomerulonephritis and Nephrotic Syndrome,5. Immunol., 8I, 492.
LUSHBAUGH, C. C., RUBIN, L., and ROTHMAN, S. (1948): Scleroderma of the Gastro-intestinal Tract; First Report of aFatal Case, Gastroenterology, II, 382.
MACKAY, I. R. (1958): Primary Biliary Cirrhosis Showing a High Titer of Auto-antibody, New Engl. 5'. Med., 258, I85.McKUSICK, V. A. (1953): Boeck's Sarcoid of the Stomach with Comments on the )Etiology of Regional Enteritis,
Gastroenterology, 23, 103.MoRE, J. H., McMILLAN, G. C., and DUFF, G. L. (1946): The Pathology of Sulphonamide Allergy in Man, Amer. 5'.
Path., 22, 703.MOWREY, F. H., and LUNDBERG, E. A. (1954): Clinical Manifestations of Essential Polyangitis, Ann. intern. Med., 40,
1145.OAKLEY, C. L. (1959): The Localisation of Antibody Production, in Modern Trends in Pathology. Ed. Collins, D. H.
London: Butterworth.ORIE, N. G. M., VAN RIJSSEL, T. G., and VANDERZWAG, G. L. (1950): Pyloric Stenosis in Sarcoidosis, Acta med. scand.,
138, I 39.PHEAR, D. N. (1958): The Relationship between Sarcoidosis and Regional Ileitis, Lancet, ii, I250.POLCAK, J. and VOKURKA, V. (I960): Auto-immune Reactions in the Course of Ulcerative Colitis, Amer. 5'. dig. Dis., 5,
395.POLLARD, H. M., and STUART, G. J. (1941): Experimental Reproduction of Gastric Allergy in Human Beings with
Controlled Observations on the Mucosa, 5'. Allergy, 13, 467.PUGH, J. I., and STRINGER, P. (1956): Abdominal Peri-arteritis Nodosa, Brit. 5'. Surg., 44, 303.REFVEM, 0. (1954): Pathogenesis of Boeck's Disease, Acta med. scand. Suppi., 294.RICH, A. R. (1942): Role of Hypersensitivity in Peri-arteritis Nodosa, Bull. J7ohns Hopk. Hosp., 7I, 123.ROSENTHAL, F. D. (1957): Small Intestine Lesions with Steatorrhcea in Diffuse Systemic Sclerosis, Gastroenterology,
32, 332.RowE, A. H. (1942): Chronic Ulcerative Colitis. Allergy in its Aetiology, Ann. intern. Med., 17, 83.
P ROWE, A., and UYEYAMA, K. (1953): Regional Enteritis-its Allergic Aspects, Gastroenterology, 23, 554.SHAPIRO, P. F., and IvY, A. C. (I926): Gastric Ulcer IV. Experimental Production of Gastric Ulcer by Local Ana-
phylaxis, Arch. intern. Med., 38, 237.
copyright. on 2 F
ebruary 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.276 on 1 M
ay 1961. Dow
nloaded from

May x96I SLANEY: Alimentary Granulomata and the Immune Response 281
SHELLEY, W. B., and HURLEY, H. J. (1957): Experimental Evidence for an Allergic Basis for Granuloma Formation inMan, Nature, I8o, io6o.
THIERS, H., and CHEVALLIER, R. (I935): Les Tesions Macroscopiques du Choc Anaphylactique par Ingestion, chez leCobaye Sensibilise par voie Parenterale, C.R. Soc. Biol. (Paris), I2o, IOO9.
TRUELOVE, S. C. (I96I): Ulcerative Colitis Provoked by Milk, Brit. med. J., I, I54.VAZQUEZ, J. J., and DIXON, F. J. (1957): Immuno-histochemical Study of Lesions in Rheumatic Fever, Systemic Lupus
Erythematosus and Rheumatoid Arthritis, Lab. Investigation, 6, 205.WAINGER, C. K., and LEVER, W. F. (1949): Dermatomyositis, Arch. Derm. Syph. (Chicago), 59, 196.WALTON, E. W. (1958): Giant Cell Granuloma of the Respiratory Tract (Wegener's Granulomatosis), Brit. med. J.,
2, 265.WALZFR, M., GRAY, I., STRAUS, H. W., and LIVINGSTON, S. (1938): Studies in Experimental Hypersensitiveness in the
Rhesus Monkey, J. Immunol., 34, 9I.WEGENER, F. (1939): Uber eine eigenartige rhinogene Granulomatose mit besonderer Beteiligung des Arterien systems
und der Nieren, Beitr. path. Anat., 102, 36.WEINBERG, T. (I946): Peri-arteritis Nodosa in Granuloma of Unknown Aetiology, Amer. J. clin. Path., I6, 787.WHITE, R. G., COONS, A. H., and CONNOLLY, J. (1955): Studies on Antibody Production. III. The Alum Granuloma,
J. exp. Med., 102, 73.WITEBSKY, E., ROSE, N. R., TERPLAN, K., PAINE, J. R., and EGAN, R. W. (1957): Chronic Thyroiditis and Auto-
immunisation, J. Amer. med. Ass., 164, I439.and SHULMAN, S. (1958): The Auto-antibody Nature of the Thyroiditis Antibody and the Role of Thyro-
globulin in the Reaction, Lancet, i, 8o8.
copyright. on 2 F
ebruary 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.427.276 on 1 M
ay 1961. Dow
nloaded from


![The Trojan [1960]€¦ · The Trojan I960 SeventhVolume CharlesH.DardenHighSchool Wilson,NorthCarolina](https://img.pdfslide.us/doc/110x75/5f77cccca83936301b071210/the-trojan-1960-the-trojan-i960-seventhvolume-charleshdardenhighschool-wilsonnorthcarolina.jpg)












![March 15, I960 Also present: William Russell, Mlna ^Mrs ...musicrising.tulane.edu/uploads/transcripts/J.Lala 3-15-1960.pdf · JOHNM LALA 1 I [of 5] -Digest -Retyped March 15, I960](https://img.pdfslide.us/doc/110x75/5a790b087f8b9a07628ba8d0/march-15-i960-also-present-william-russell-mlna-mrs-3-15-1960pdfjohnm-lala.jpg)













