Embed Size (px)
Citation preview

J. clin. Path. (1957), 10, 51.
STARCH GRANULOMATABY
C. G. PAINE AND P. SMITHFrom the Department of Pathology, Jessop Hospital for Women. Sheffield
(RECEIVED FOR PUBLICATION MARCH 20, 1956)
During the years 1933 to 1941 attention wasdrawn in a number of publications to the irritativeeffect of talc, the introduction of which intotissues, particularly the peritoneal cavity, led tothe formation of granulomata and chronic inflam-matory adhesions (Haythorn, 1933; Antopol,1933; Owen, 1936; Fienberg, 1937). The workof Ramsey and Douglass (1940), Byron and Welch(1941), and others made it clear that the use oftalc as a glove powder lubricant was largely respon-sible for such lesions, which developed as a sequelto previous operative procedures, when glovepowder had inadvertently been introduced. Postle-thwait, Howard, and Schanher (1949) consideredthat the implantation of surgical glove lubricantcould occur from unwashed or perforated gloves,spill on to instruments and suture material, and bydirect airborne route. It is probable, as will beshown below, that the introduction of glovepowder into the peritoneal cavity of women is notlimited to these routes.The rejection of talc as a glove lubricant led to
the search for substitutes, and experimental work,mainly upon dogs and rabbits, indicated that suit-able starch preparations could act as serviceablelubricants, and that they produced minimal lesionswithin tissues (Lee and Lehman, 1947; Mac-Quiddy and Tolman, 1948; Postlethwait et al.,1949).
In the above hospltal starch powder was substi-tuted for talc as a glove lubricant in 1952, sincewhen starch-containing lesions have been foundat laparotomy on three occasions. In respect oftalc granulomata there is often a lapse of manyyears between the introduction of the powder andthe recognition of talc lesions; in these thespicules of talc remain apparently unabsorbed,but are enveloped by foreign body and fibroustissue reactions of varying magnitude. It was diffi-cult to believe that starch particles could be simi-larly unabsorbable, and therefore inquiries weremade to determine the method by which theseparticles had been introduced into the peritonealcavity, the nature of the tissue response, and the
probable duration and pathological significance ofthe lesions produced. An account of these investi-gations forms the subject of this communication.
Case ReportsCase 1.-Mrs. Br., aged 39 years, gave a two-day
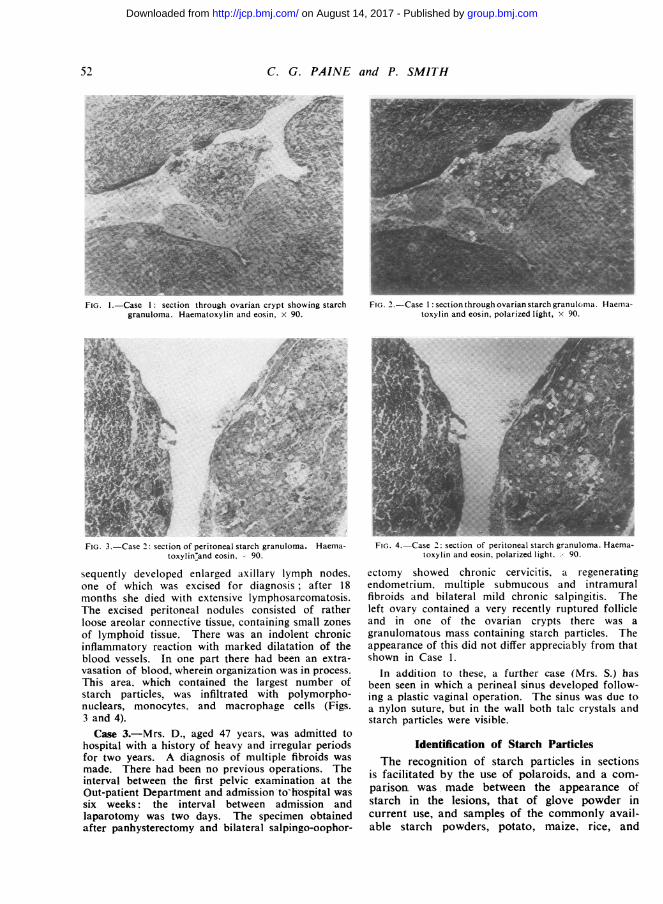
history of lower abdominal pain. On examinationa large tender cystic mass was felt arising from thepelvis. There had been no previous operations, andshe had two normal deliveries, her children being aged16 and 10 years respectively. The duration of timefrom pelvic examination on admission to laparatomywas two days. A panhvsterectomy and doublesalpingo-oophorectomy was performed. The speci-men showed a papillary erosion of the cervix; theendometrium was of normal secretory pattern; oldfibrous adhesions were present on the posterior aspectof the uterus and on the tubes; both ovaries containedareas of endometriosis. In a crypt of the right ovarythere was a proliferation of recent granulation tissuecontaining starch granules and infiltrated by poly-morphonuclear leucocytes, monocytes, and macro-phage cells (Figs. I and 2).Case 2.-Mrs. Ba., aged 65 years, an emaciated old
woman, complained of loss of weight and of a bearing-down sensation on walking. A painless mass was feltin the right iliac fossa. A vaginal examination con-firmed the presence of this mass, and a similar butsmaller mass was felt on the left side. The maEseswere considered to be ovarian or intestinal, but abarium enema did not show any interference with thebowel lumen. The patient gave a past history ofpulmonary tuberculosis at age 31 years. There hadbeen no previous operations. The duration in timefrom pelvic examination on admission to laparotomywas nine days. At laparotomy the genital tractappeared normal. The masses were found to involvethe bowel, there being two masses in the small intes-tine 5 and 18 in. from the ileo-caecal valve, and afurther mass in the sigmoid colon. The lesionspresented as soft diffuse thickenings of the intestinalwall without any appreciable narrowing of the gutlumen. No lymph node enlargement was found andthe liver felt normal ; at the reflection of the peri-toneum from the mesentery on to the small intestine,two small nodules were seen. These were removed forbiopsy and the abdomen closed. The patient sub-
group.bmj.com on August 14, 2017 - Published by http://jcp.bmj.com/Downloaded from
C. G. PAINE and P. SMITH
FIG. 1.-Case 1: section through ovarian crypt showing starchgranuloma. Haematoxylin and eosin, x 90.
s-FV -f-,- {..*--r-FIG. 3.-Case 2: section of peritoneal starch granuloma. Haema-
toxylin'and eosin. 90.
sequently developed enlarged axillary lymph nodes.one of which was excised for diagnosis; after 18months she died with extensive lymphosarcomatosis.The excised peritoneal nodules consisted of ratherloose areolar connective tissue, containing small zonesof lymphoid tissue. There was an indolent chronicinflammatory reaction with marked dilatation of theblood vessels. In one part there had been an extra-vasation of blood, wherein organization was in process.This area, which contained the largest number ofstarch particles, was infiltrated with polymorpho-nuclears, monocytes. and macrophage cells (Figs.3 and 4).Case 3.-Mrs. D., aged 47 years, was admitted to
hospital with a history of heavy and irregular periodsfor two years. A diagnosis of multiple fibroids wasmade. There had been no previous operations. Theinterval between the first pelvic examination at theOut-patient Department and admission-tohos-pital wassix weeks: the interval between admission andlaparotomy was two days. The specimen obtainedafter panhysterectomy and bilateral salpingo-oophor-
FIG. 2.-Case 1: section through ovarian starch granuloman Haeniia-toxylin and eosin, polarized light, x 90.
_~~~~~~~~~~~~~~~. -Ny w-xin
FiG. 4.-Case 2: section of peritoneal starch granuloma. Haema-toxylin and eosin, polarized light .x 90.
ectomy showed chronic cervicitis. a regeneratingendometrium. multiple submucous and intramuralfibroids and bilateral mild chronic salpingitis. Theleft ovary contained a very recently ruptured follicleand in one of the ovarian crypts there was agranulomatous mass containing starch particles. Theappearance of this did not differ appreciably from thatshown in Case 1.
In addition to these, a further case (Mrs. S.) hasbeen seen in which a perineal sinus developed follow-ing a plastic vaginal operation. The sinus was due toa nylon suture, but in the wall both talc crystals andstarch particles were visible.
Identification of Starch ParticlesThe recognition of starch particles in sections
is facilitated by the use of polaroids, and a com-parisom was made between the appearance ofstarch in the lesions, that of glove powder incurrent use, and samples of the commonly avail-able starch powders, potato, maize, rice, and
52
I .,
*.
.;i
group.bmj.com on August 14, 2017 - Published by http://jcp.bmj.com/Downloaded from

STARCH GRANULOMATA
z
usM
IT'
i~ i
FIo. 5.-A comparison of maximum, mean, and minimum particlediameters of starch samples with those of starch in granulo-mata.
wheat. Not only was there a considerable varia-tion in size and shape of starch particles fromdifferent sources, but a wide range of size varia-tion in individual starches was noted. All thestarches examined showed a Maltese cross con-
figuration with polarized light, and it was foundthat the identification of a source of starch was
best accomplished by determining the total rangeof particle size and the mean diameter. Accord-ingly 400 particles were measured in respect ofeach starch sample and of the glove powder, andthe sizes of as many particles as possible (60 to230) in sections of starch lesions. The results ofthese examinations, set out in Fig. 5, show thatthe particle size of the starch in the lesions corre-
sponded closely to that of maize starch and ofglove powder, which, according to the manu-facturers, was prepared from maize starch. Noneof the particles in the lesions showed the ovalforms and contours characteristic of potato starch,and it was therefore concluded that the lesionsformed as a response to the introduction of glovepowder containing maize starch.
Fate of Starch Suspensions InjectedIntraperitoneally into Mice
Attempts were made to produce starch granulo-mata within the peritoneal cavities of mice. Ani-mals killed one week after the intraperitonealinjection of each of the four starch samples, sus-
pended either in saline or in citrated mouse blood,failed to show peritoneal lesions, nor was therehistological evidence from studies of the omentum,
liver, spleen, and lungs of any starch survival ortransportation.
In a second series, 24 mice were given intra-peritoneal injections of 0.5 ml. 4% maize starchsuspensions in saline. The mice were killed inpairs at intervals after inoculation, the peritonealcavity of one of each pair being injected with1.0 ml. Lugol's iodine immediately after death andbefore the peritoneal cavity was opened. At oneand two hours there was a generalized darkeningof the peritoneal wash in the iodine-treatedanimals, and polymorphonuclears with free starchparticles were visible microscopically. No local-ization of the starch was noted, and histologicalexamination of the omentum, intestines, liver,spleen, and lungs confirmed these findings. Micekilled at four hours showed small aggregationsof starch surrounded by polymorphonuclears lyingfree within the peritoneal cavity; the omentumwas stained black with iodine. After eight hoursthe starch no longer remained free within theperitoneum, but it was all immobilized in theomentum. Mice were then killed at 12, 18, 24hours, and daily up to six days; iodine tests failedto show any gross aggregations of starch eitherfree in the peritoneal cavity or within theomentum. Histological studies were made of theomentum, intestines, liver, spleen, and lungs; inno case was starch found in organs other than theomentum, in which it could be detected up tofour days. The omental lesions are shown in Figs.6 and 7.
It was noted that in the omentum of animalskilled at 96 hours, although doubly refractilebodies were still evident, the proportion showingthe Maltese cross configuration was appreciablysmaller than in mice killed earlier. A furtherstudy of particle size in relation to survival timeshowed after eight hours a progressive diminutionin size (Fig. 8).
In the absence of evidence that the injectedstarch was transported elsewhere, and because ofthe diminution in particle size associated withincreasing leucocytic infiltration of the omentum,it was concluded that the disappearance of thestarch was due to local enzymic action by thesurrounding cells.
Fate of Starch Particles Within thePeritoneum of Other Species
No direct observations, comparable with thosein mice, have been made or are possible in humans.The relatively speedy disappearance of starch fromthe peritoneum in mice is paralleled by theobservations of Postlethwait et al. (1949), who
53
group.bmj.com on August 14, 2017 - Published by http://jcp.bmj.com/Downloaded from

C. G. PAINE and P. SMITH
p..~~~~~~~~~~M
FIG. 6-Section of mouse omenum four hours after intrape.-itonealinjection of maize starch suspension. Haematoxylin and eosin,polarized light, 110.
found only minimal adhesions and only on2granulomatous type lesion containing visible starchparticles in a series of four dogs and nine rabbitskilled at intervals of from two hours to 37 daysafter starch had been introduced into the peri-toneal cavity. The cellular response, as describedby these authors, and that in humans and in micedo not differ essentially, and its seems probabletherefore that the mechanism whereby starch dis-appears from the human peritoneal cavity is essen-tially the same as that described here for mice.In reviewing the histology of the human lesions,it will be noted that the starch appeared to havebeen first incarcerated within blood clot, whichprobably protected the starch from early dissolu-tion.
Route of Entry of Starch into the HumanPeritoneal Cavity
In none of the cases recorded here was thereany history of previous laparotomy, as has beenrecorded so frequently in cases of talc granulo-mata. The mechanism of its introduction musttherefore be different, and, in view of the evidencethat starch disappears relatively rapidly, it seems
FIG. 7.-Section of mouse omentum 24 hours after intraperitonealinjection of maize starch suspension. Haematoxylin and eosin,polarized light, x 110.
probable that the starch had been introduced onlya few days before operation. These observations.coupled with the fact that in cervical smear pre-parations, uced in the investigation of sterilitv,
20-
15-
z10-
Zi 8-
6-
4-
2-
I I I0 2 4 8 12 24 96
HOURS AFTER INJECTIONFIG. 8.-Diminution in maximum, mean, and minimum particle
diameters of maize starch after intraperitoneal injection intomice.
54
group.bmj.com on August 14, 2017 - Published by http://jcp.bmj.com/Downloaded from

STARCH GRANULOMATA
starch particles are a common finding, suggestedthat the starch had been introduced at vaginalexamination made at admission, and had traversedthe genital tract to enter the peritoneum. Mc-Cartney and Fraser (1922) showed that a similarmethod of spread operated in primary pneumo-coccal peritonitis, thus accounting for the veryhigh incidence of the disease in young girls ascompared with young males.The number of cases of starch granulomata
was too small to provide any idea of the relativefrequency of occurrence of intra-abdominalgranulomata developing as a response to the intro-duction of foreign particles by routes other thanthat provided by a previous laparotomy. There-fore a series of 50 cases of talc granulomata wasreviewed to determine the case incidence, whereno previous laparotomy could account for theperitoneal seeding; in six of the series there wasno evidence of previous laparotomy, pre-operativeattendances as out-patients, when vaginal examina-tions were made, varying from two to 10 times.
DiscussionThree cases of starch granulomata within the
peritoneal cavity of women have been described,and evidence has been adduced to show that thestarch was derived from the glove powder incurrent use in the hospital. In mice, starch dis-appears from the peritoneal cavity within a fewdays of its introduction, this being accomplishedlargely by digestion by polymorphonuclear leuco-cytes. The absence of previous intraperitonealoperative procedures in the cases described, andthe fact that intraperitoneal talc granulomata canoccur in cases where there had been no previousoperative interference, indicates that the starch
had reached the peritoneal cavity via the genitaltract, and if, as seems probable, the rate of dis-appearance of starch from the human peritoneumis similar to that in mice, the starch was probablyintroduced during vaginal examinations made afew days before operation.
Starch absorption within the peritoneal cavitymay be delayed if the starch is entrapped in bloodclot, and, although it is probable that starchlesions are merely transitory phenomena and un-likely to be of such serious import as talcgranulomata, it would seem desirable to limit thechances of intraperitoneal adhesions from thiscause. Attention is drawn once more to theimportance of a careful peritoneal toilet at the endof intra-abdominal procedures, particular attentionbeing paid to the removal of small fragments ofblood clot, wherein glove powder might be en-trapped. It is desirable also that glove powdershould be removed from gloved hands by washing,both before embarking upon all operative pro-cedures and also before making vaginal examin-ations.We are indebted to Mr. L. B. Patrick and Professor
C. S. Russell for permission to publish notes of theircases, to Mr. H. Dyson for technical assistance, andto Messrs. J. Preston, Ltd., Sheffield, and Messrs.Reckitt & Colman, Ltd., Hull, for starch samples.
REFERENCESAntopol, W. (1933). Arch. Path. (Chicago), 16, 326.Byron, F. X., and Welch, C. S. (1941). Surgery, 10, 766.Fienberg, R. (1937). Arch. Path. (Chicago), 24, 36.Haythorn, S. R. (1933). Amer. J. Path., 9, 725.Lee, C. M., and Lehman, E. P. (1947). Surg. Gynec. Obstet., 84, 689.McCartney, J. E., and Fraser, J. (1922). Brit. J. Surg., 9, 479.MacQuiddy, E. L., and Toliman, J. P. (1948). Surgery, 23, 786.Owen, M. (1936). Texas St. J. Med., 32, 482.Postlethwait, R. W., Howard, H. L., and Schanher, P. W. (1949).
Surgery, 25, 22.Ramsey, T. L., and Douglass, F. M. (1940). J. int. Coll. Surg., 3, 3.
55
group.bmj.com on August 14, 2017 - Published by http://jcp.bmj.com/Downloaded from

Starch Granulomata
C. G. Paine and P. Smith
doi: 10.1136/jcp.10.1.511957 10: 51-55 J Clin Pathol
http://jcp.bmj.com/content/10/1/51.citationUpdated information and services can be found at:
These include:
serviceEmail alerting
the online article. article. Sign up in the box at the top right corner of Receive free email alerts when new articles cite this
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on August 14, 2017 - Published by http://jcp.bmj.com/Downloaded from