Embed Size (px)
Citation preview

Focused Neuro Exam
Loren BellowsNorwalk Hospital – Surgery
Rotation

Comprehensive Neuro Exam Components
• General Appearance– Posture, motor activity, speech
• Mental Status exam• Cranial Nerves• Motor Function
– Atrophy, tone, strength• Sensory
– Vibratory, Position, sharp/dull, temperature• Reflexes• Cerebellar
– Coordination, gait, Romberg’s
Focused Neuro Exam
• Three Exam Classifications– The Comatose Patient
• Unresponsive, Profound state of unconsciousness• Example: Trauma, Neurogenic Shock
– The Patient with Central Neurologic Disorder• Dysarthria, Aphasia, Partial Paralysis• Example: Stroke, Intracranial Bleed
– The Patient with Spinal Cord Disorder• Dysaesthesia, Incontinence, Pain, Weakness• Example: Disk Herniation, Spinal Cord Compression,
Brown-Sequard Syndrome

Focused Exam: The Comatose Patient
• Glasgow Coma Scale6 5 4 3 2 1
Eyes N/A N/A Opens eyes spontaneously
Opens eyes in response to voice
Opens eyes to painful stimuli
Does not open eyes
Verbal N/A Oriented, converses normally
Confused, disoriented
Utters inappropriate words
Incompre-hensible sounds
Makes no sounds
Motor Obeys commands
Localizes painful stimuli
Withdraws from painful stimuli
Decorticate posturing upon painful stimuli
Decerebrate posturing upon painful stimuli
Makes no movements
Interpretation: GCS < 8 = Severe,
GCS 9-12 = Moderate,
GCS > 13 = Minor

Focused Exam: The Comatose Patient (con’t)
• Brain Reflexes– Oculocephalic Reflex (Doll’s eyes)– Babinski– Gag Reflex (CN 9, 10)– Corneal Reflex (CN 5)– Cold Calorics
• Pupillary Response• Response to Pain• DTRs• Gaze (Ping-Pong Gaze)

Focused Exam: Central Neuro Disorder
• CNs• Speech• Coordination• Pronator Drift• Motor• Sensation• Proprioception• Graphesthesia• Stereognosis
Focused Exam: Spinal Cord Disorder
• Sensation• Motor• Hot/Cold• Vibratory Sense• Proprioception• Gait• DTRs• Rectal Tone• Hoffman’s Sign

Motor Function Testing
• Lack of Consistency:– Patient: 90 y/o female vs. 20 y/o male– Examiner
• Motor Weakness helps to pinpoint spinal cord lesion

Keys to the Motor Exam
• Have patient perform movement First!• One side at a time; Compare R vs L• Examiner: Use the same hand throughout
exam• Examiner: Don’t be a wimp! Use full and
consistent strength (unless there is known injury).– Use single muscle group, i.e. don’t use your
body weight to oppose.
• Important to assign a specific response to a set grade
• Test Certain Muscle Groups

Grading Strength
• 5/5: Examiner is unable to overcome patient• 4/5: Examiner is able to overcome patient;
patient demonstrates moderate resistance• 3/5: Patient able to overcome gravity only• 2/5: Patient unable to overcome gravity, but
can move joint• 1/5: Muscle “fires”, but no joint movement• 0/5: No muscle response• May use +/- to differentiate further

Strength Testing: The Muscle Groups• Upper extremities:
Action Nerve Root / Spinal Level
Shoulder Abduction C5
Elbow Flexion C5/C6
Elbow Extension C6/C7/C8
Wrist Extension C6
Wrist Flexion C7
Grip Strength (Finger Flexion)
C8
Interosseous (Finger Ab/Adduction)
T1
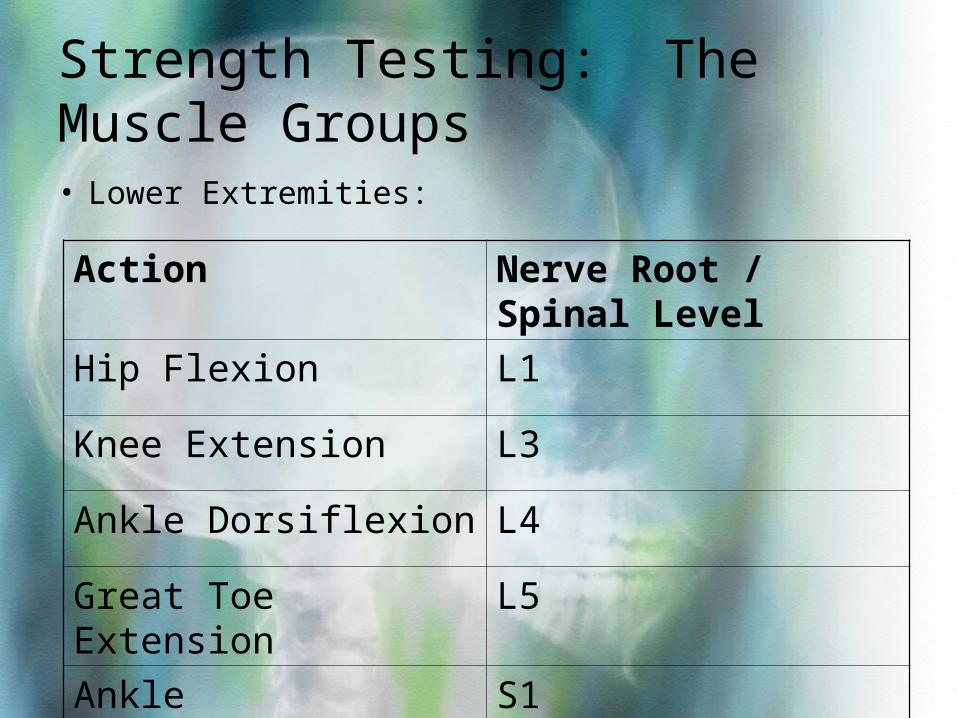
Strength Testing: The Muscle Groups• Lower Extremities:
Action Nerve Root / Spinal Level
Hip Flexion L1
Knee Extension L3
Ankle Dorsiflexion L4
Great Toe Extension L5
Ankle Plantarflexion S1
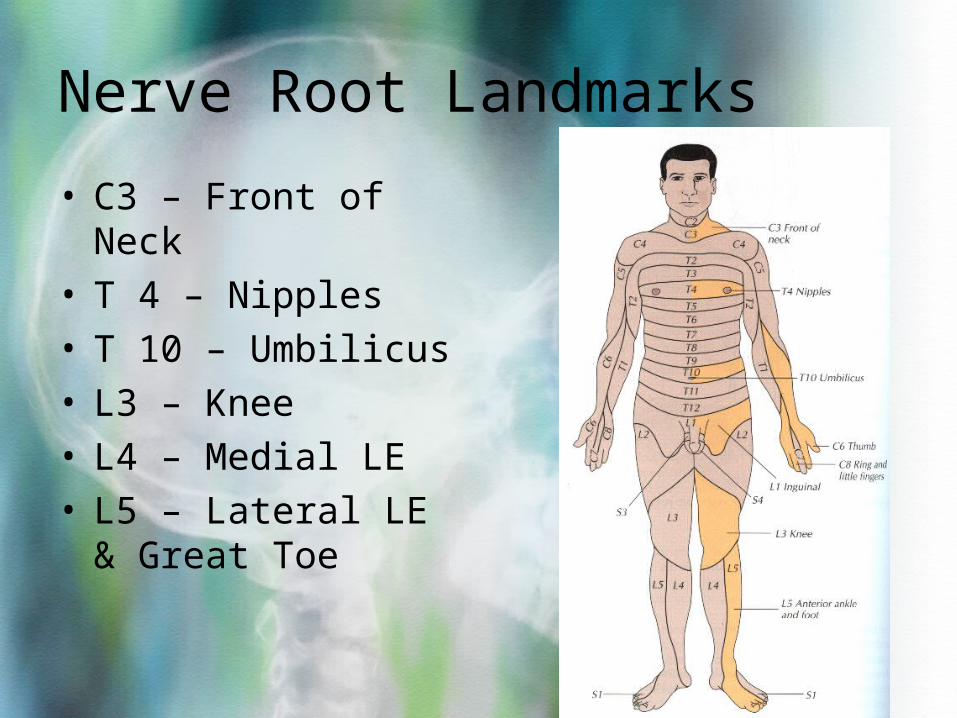
Nerve Root Landmarks
• C3 – Front of Neck• T 4 – Nipples• T 10 – Umbilicus• L3 – Knee• L4 – Medial LE• L5 – Lateral LE &
Great Toe
Questions??